")
Back to Journals » Clinical Epidemiology » Volume 15
Large Burden of Stroke Incidence in People with Cardiac Disease: A Linked Data Cohort Study
Authors Robinson K , Katzenellenbogen JM , Kleinig TJ , Kim J, Budgeon CA, Thrift AG , Nedkoff L
Received 30 September 2022
Accepted for publication 28 January 2023
Published 18 February 2023 Volume 2023:15 Pages 203—211
DOI https://doi.org/10.2147/CLEP.S390146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Keira Robinson,1 Judith M Katzenellenbogen,1 Timothy J Kleinig,2 Joosup Kim,3,4 Charley A Budgeon,1 Amanda G Thrift,4 Lee Nedkoff1,5
1School of Population and Global Health, The University of Western Australia, Perth, Western Australia, Australia; 2Department of Neurology, Royal Adelaide Hospital, Adelaide, South Australia, Australia; 3Department of Medicine, The Florey Institute of Neuroscience and Mental Health, The University of Melbourne, Melbourne, Victoria, Australia; 4Department of Medicine, School of Clinical Sciences at Monash Health, Monash University, Melbourne, Victoria, Australia; 5Victor Chang Cardiac Research Institute, Sydney, New South Wales, Australia
Correspondence: Keira Robinson, School of Population and Global Health, The University of Western Australia, M431, 35 Stirling Hwy, Crawley, WA, 6009, Australia, Email [email protected]
Purpose: People with cardiac disease have 2– 4 times greater risk of stroke than the general population. We measured stroke incidence in people with coronary heart disease (CHD), atrial fibrillation (AF) or valvular heart disease (VHD).
Methods: We used a person-linked hospitalization/mortality dataset to identify all people hospitalized with CHD, AF or VHD (1985– 2017), and stratified them as pre-existing (hospitalized 1985– 2012 and alive at October 31, 2012) or new (first-ever cardiac hospitalization in the five-year study period, 2012– 2017). We identified first-ever strokes occurring from 2012 to 2017 in patients aged 20– 94 years and calculated age-specific and age-standardized rates (ASR) for each cardiac cohort.
Results: Of the 175,560 people in the cohort, most had CHD (69.9%); 16.3% had multiple cardiac conditions. From 2012– 17, 5871 first-ever strokes occurred. ASRs were greater in females than males in single and multiple condition cardiac groups, largely driven by rates in females aged ≥ 75 years, with stroke incidence in this age group being at least 20% greater in females than males in each cardiac subgroup. In females aged 20– 54 years, stroke incidence was 4.9-fold greater in those with multiple versus single cardiac conditions. This differential declined with increasing age. Non-fatal stroke incidence was greater than fatal stroke in all age groups except in the 85– 94 age group. Incidence rate ratios were up to 2-fold larger in new versus pre-existing cardiac disease.
Conclusion: Stroke incidence in people with cardiac disease is substantial, with older females, and younger patients with multiple cardiac conditions, at elevated risk. These patients should be specifically targeted for evidence-based management to minimize the burden of stroke.
Keywords: stroke incidence, coronary heart disease, valvular heart disease, atrial fibrillation, cardiac disease, risk factors
Introduction
Stroke remains the second most common cause of death worldwide, accounting for 6.55 million deaths in 2019.1 Although age-standardized death rates and incidence of stroke have declined in high-income countries, an aging global population and a rise in some risk factors has contributed to an increased global burden of stroke, reaching 143 million Disability Adjusted Life Years (DALYs) in the 25 years to 2019. This indicates that improved stroke prevention strategies are required.2–5
Understanding the burden of stroke is essential for informing health service planning and appropriate targeting of risk factors. The INTERSTROKE investigators showed that cardiac diseases including coronary heart disease (CHD), atrial fibrillation (AF) and valvular heart disease (VHD) significantly increase stroke risk in people with these conditions.6 Similar findings are observed in cohort studies with the risk of stroke being two-fold greater in patients with CHD, five-fold in AF, and three-fold in VHD.7–9 However accurate estimates of the population burden of stroke in those with cardiac conditions are limited, and current evidence suggests increasing stroke incidence in young adults within Australia, concurrent with increasing incidence of CHD in young women.10 Therefore, the current study addresses the lack of cohort studies with long-term (five-year) follow-up to investigate stroke burden and multi-cardiac disease. We aimed to determine the burden of stroke in people with major cardiac diseases by measuring the 5-year incidence of stroke among people ever hospitalized with CHD, AF or VHD. Our secondary aims were to compare stroke incidence by age, sex, single versus multiple cardiac conditions and pre-existing versus new cardiac disease.
Materials and Methods
Study Design and Data Sources
In this retrospective population-based cohort study, we utilized linked health data from the Western Australian (WA) Hospital Morbidity Data Collection, which are systematically linked with the WA Deaths registry using probabilistic matching. Our dataset included all public and private hospitalizations and death records of people admitted with, or dying from, cardiovascular disease (CVD) in WA between 1985 and 2017. The dataset included patient demographics, principal and twenty additional diagnosis fields, in-hospital procedures, date of death, and underlying and associated causes of death. In WA, ICD-9 was in use from 1979, ICD-9-CM from 1988, and ICD-10-Australian modification (AM) from mid-1999.
Cohort Selection
We identified all hospitalizations for CHD, AF and VHD between January 1, 1985 and December 31, 2017 using all diagnosis fields (Supplementary Table 1). Cardiac patients were stratified as pre-existing or new cardiac disease (Figure 1). The accrual periods were selected to enable a 5-year follow-up period to identify incident stroke. People with prior stroke or missing age were excluded. Patients were categorized into mutually exclusive combinations of cardiac sub-groups, including those with single (CHD Only, AF Only or VHD Only) or multiple conditions (Supplementary Table 2). These were consolidated into any CHD, any AF and any VHD for the main analyses.
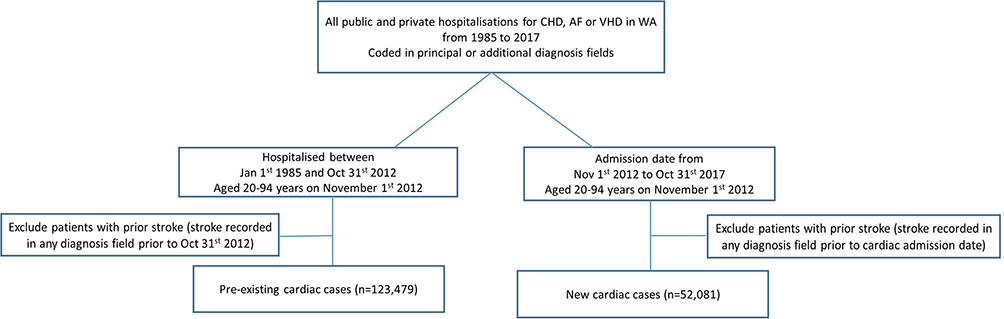 |
Figure 1 Flow diagram showing how the cardiac cohort was identified. |
Outcomes
The primary outcome was first-ever stroke (hospitalization or death) between November 1, 2012 and October 31, 2017. Acute ischemic, hemorrhagic or unspecified hospitalized strokes were identified from the principal diagnosis field (ICD-10-AM code I60, I61, I62.9, I63, I64). Admissions coded as I62.0 and I62.1 (non-traumatic subdural hemorrhage and epidural hematoma respectively) were excluded from the study due to their different etiology, management and prognosis from acute stroke events. Stroke deaths were identified from the underlying or multiple-coded cause of death fields. Non-fatal strokes were those surviving >28 days from admission for stroke. Fatal stroke included any death ≤28 days post-hospitalization for stroke, a death from stroke ≤28 days following a non-stroke hospitalization, or a stroke-coded death with no hospitalization within 28 days of death. The first-ever stroke event date was defined as the date of hospital stroke admission or death from stroke. A subset of new cardiac cases was identified where the first-ever stroke was recorded on the same admission as a first-ever cardiac hospitalization.
Comorbidities and Covariates
Details of age, sex and Aboriginal status were obtained from hospitalization and/or death data. Comorbidities were identified using all diagnosis fields (Supplementary Table 1) from hospitalizations between January 1, 1985 and October 31, 2012 (pre-existing cases), and for those with new cardiac disease, from 1985 to 2017, including the incident cardiac admission. We also identified conditions incorporated into the Charlson Comorbidity Index (congestive heart failure, hypertension, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age, sex) and calculated the CHA2DS2-VASc score.11 Procedures including percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), carotid endarterectomy and AF ablation were identified from any procedure field.
Statistical Analyses
All analyses were stratified by cardiac subgroup, and single and multiple cardiac conditions. We calculated age-specific stroke incidence rates and 95% confidence intervals (CIs). Numerators were the number of first-ever strokes in the five-year follow-up period, and denominators, the total number of person-years allocated to each five-year age group until stroke, non-stroke death or the end of the follow-up period, with person-time contribution possible from more than one age group (censored at age 95 years). Age-standardized rates (ASRs) were calculated by the direct method using five-year age groups and the age distribution of all cardiac cases in the study as the standard. Incidence rates are presented per 1000 person-years and stratified by survival status and sex. Incidence rate ratios (IRRs) and 95% CIs comparing age-standardized stroke incidence rates in females versus males by age group and overall, were computed in SAS v9.4 statistical package using the “PROC STDRATE” command.
For patients admitted concurrently for first-ever cardiac hospitalization and stroke (42% of new cardiac cases), we performed a sensitivity analysis to determine appropriate allocation of person-time. Given the likelihood that these cardiac conditions were present pre-stroke, we tested allocating one day, and one, two and five years of person-time to each patient. Analyses were undertaken in STATA v 16.0 and SAS V.9.4.
Results
In total, 175,560 people were included, contributing 801,536 person-years. Within this cohort, 70% had pre-existing cardiac conditions. The CHD Only subgroup comprised the majority (56%), followed by AF Only (23%). The most frequent combination for those with multiple conditions was CHD and AF (9%) (Supplementary Figure 1).
Patient Profiles
Patients with AF were approximately three years older than those with CHD or VHD (Table 1). Females comprised 34.8% of the Any CHD group, 41.4% of the Any AF group, and 46.5% of the Any VHD group. Hypertension was the most common comorbidity in each cardiac group, while Charlson scores were greatest in those with VHD and least in those with CHD. Compared to those with multiple conditions, patients with a single condition were approximately seven years younger, had fewer comorbidities or prior cardiac procedures, and had lower CHA2DS2-VASc and Charlson scores. Females with CHD or AF were older than men with the same cardiac condition, and had generally greater prevalence of most comorbidities,including prior MI, heart failure, rheumatic heart disease, and peripheral vascular disease (Supplementary Table 3). Patients with pre-existing cardiac disease were on average three to five years older and had more comorbidities than new cases for each cardiac condition (Supplementary Tables 4 and 5).
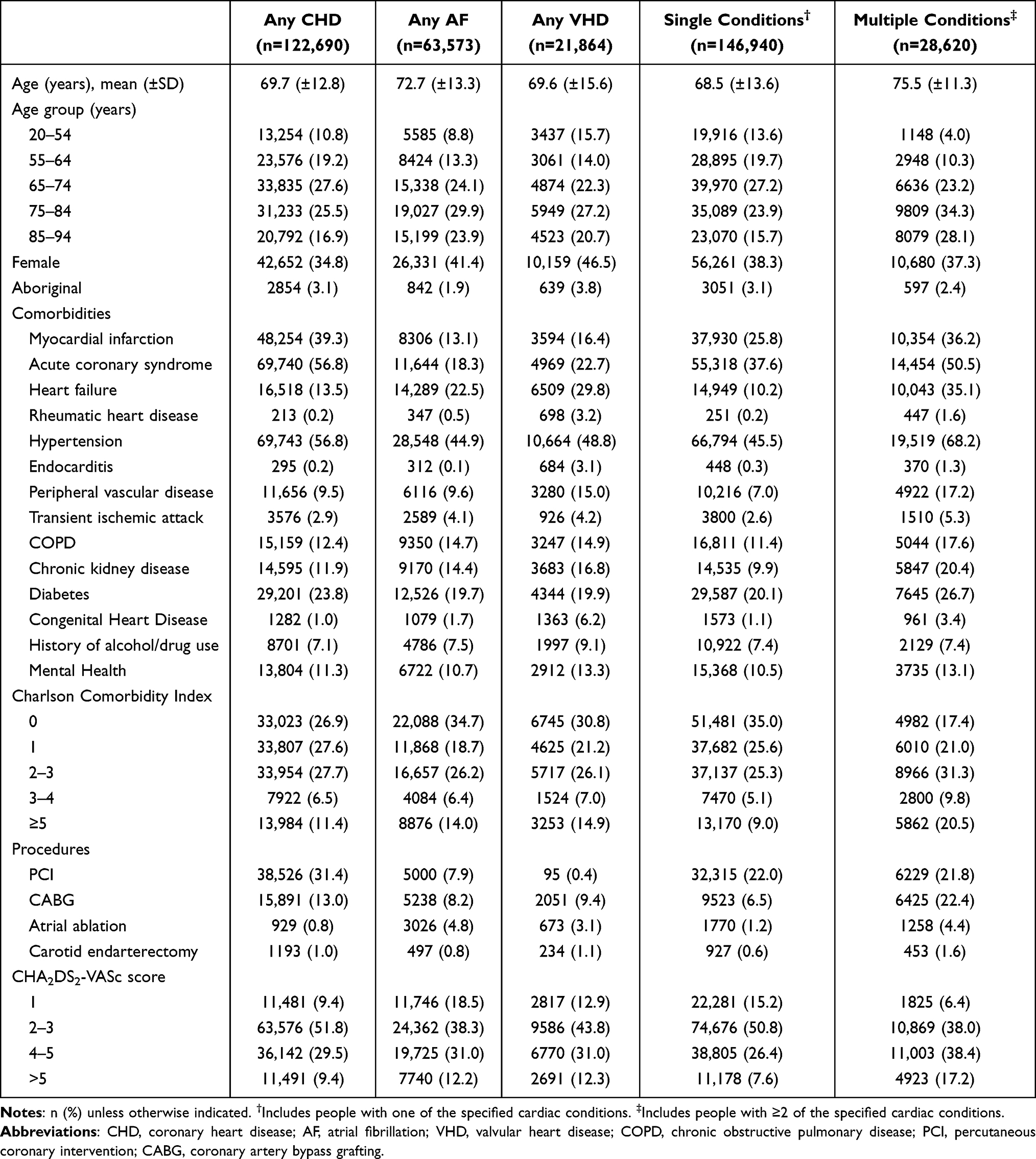 |
Table 1 Baseline Characteristics of the Study Cohort, Stratified by Cardiac Condition |
Concurrent Cardiac Disease and Stroke
In sensitivity analyses determining the appropriate person-time to use for new cases with concurrent cardiac disease and first-ever stroke, allocating five years of person-time resulted in stroke incidence rates that were the least, with the largest incidence rates observed when using one day of person-time (Supplementary Figure 2). As there was little difference between incidence rates when using one-year and two-year person-time durations, one-year of person-time was used to analyse all concurrent cases. Where a patient had a shorter duration of follow-up available than one year, we allocated time from the start of the follow-up period to the start of the cardiac admission.
First-Ever Stroke Events and Incidence Rates
There were 5871 incident strokes (3.3% of total cohort) identified during the follow-up period, with most occurring in those aged ≥75 years (Supplementary Table 6). Stroke incidence was greatest in patients with AF than other cardiac subgroups, ranging from 6.4/1000 person-years in males with CHD, to 18.6/1000 person-years in females with AF, and higher in those with multiple versus single cardiac conditions (Figure 2, Supplementary Table 7). The differential between multiple and single cardiac conditions was greatest in females aged 20–54 years. Total ASRs were greatest in people with AF followed by VHD then CHD. Those aged <84 years mostly had non-fatal strokes, whereas those aged ≥85 years predominantly had fatal strokes. Incidence rates were between 1.2 and 2.4 times greater in new cardiac cases than pre-existing cases (Supplementary Figure 3, Supplementary Tables 8 and 9).
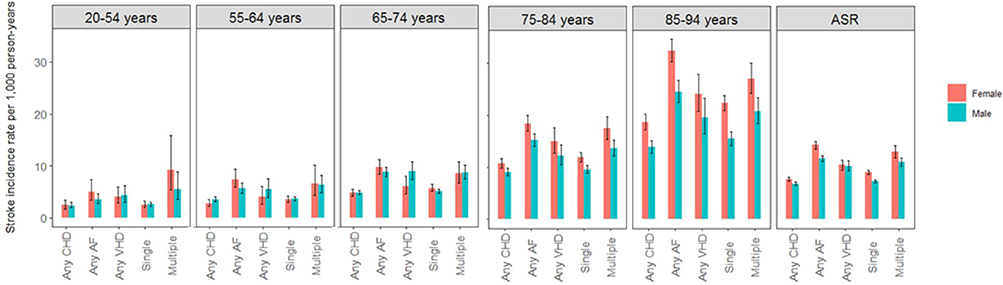 |
Figure 2 Age-specific stroke incidence rates and age standardized rates (95% confidence intervals) in all cardiac cases, stratified by sex and cardiac condition. |
Among those aged ≥75 years, stroke incidence was at least 20% greater in females than males in each cardiac subgroup, in those with single and multiple cardiac conditions, and in pre-existing cases (Figure 3, Supplementary Figure 4). The sex differential extended to all age groups for AF although was not significant at a younger age. In people with VHD, there was a trend towards lesser stroke incidence in females than males aged <74 years although this was only statistically significant in those aged 65–74 years (IRR 0.67, 95% CI 0.47, 0.94).
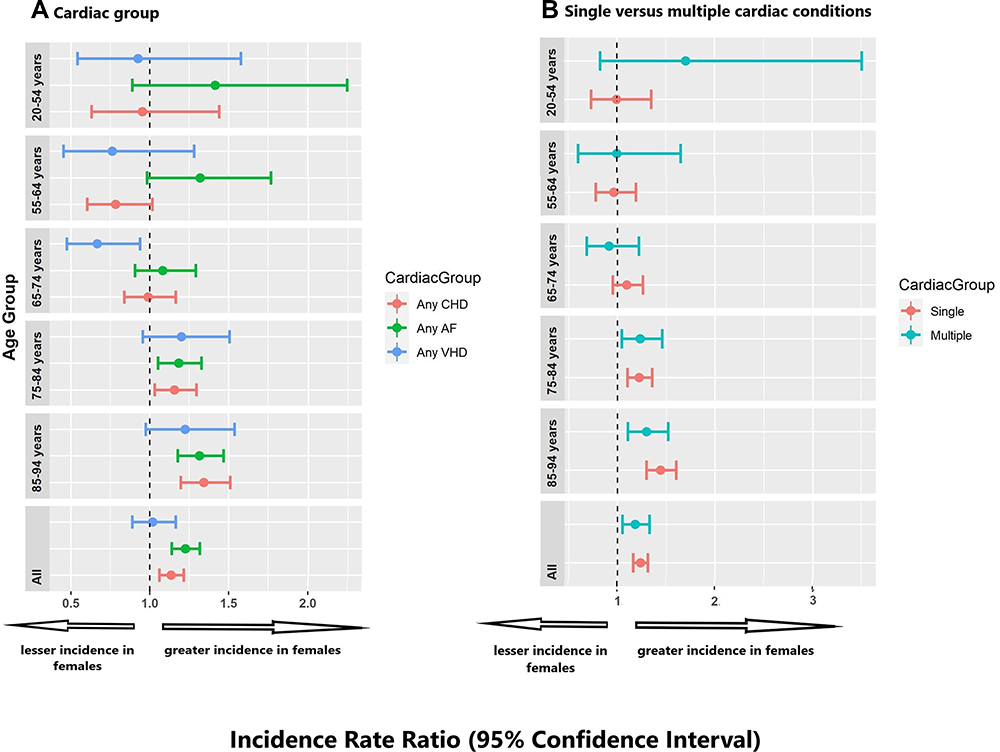 |
Figure 3 Age-standardized stroke incidence rate ratios in females versus males in (A) each cardiac group and (B) single and multiple cardiac conditions. |
Discussion
This whole-population linked data study provides contemporary insights into the population-burden of stroke incidence in people with cardiac disease. Our study demonstrated that stroke incidence was greatest in patients with AF, and in those newly hospitalized with a cardiac condition. Importantly, we showed that female patients aged ≥75 years had a greater incidence of stroke than their age-matched male counterparts, irrespective of the underlying cardiac disease. This disparity extended to all age groups in people with AF. Stroke was more common in people with multiple cardiac conditions, this difference being greatest in females aged 20–54 years.
Stroke incidence appears to be much greater in people with major cardiac diseases than in the general population as shown by the Global Burden of Disease estimates.12 Authors measuring the risk of stroke following ACS have reported incidence of 2–4% over a 1–2 year period, which although not directly comparable to our population measures, is likely larger in our cohort as we did not restrict the sample to acute CHD events and we had a longer-term follow-up in our cohort.13–15 Additionally, these studies have provided evidence that stroke incidence is lower in ACS patients without AF than in those with AF.13,15 Furthermore, in another cohort of people with mitral valve regurgitation and AF, the incidence of stroke was comparable to the age standardized stroke incidence rate for VHD that we report in our study.16 When compared to a study of people with aortic stenosis, we identified similar age-specific stroke incidence in those aged between 55 and 84 years with VHD,17 but considerably larger stroke incidence among younger people. This may reflect the large proportion of Aboriginal people with RHD in the <55-year age group in our population, a group with 60-fold the prevalence of RHD than non-Aboriginal Australians.18
Stroke incidence in people with AF in our study was considerably lower across all age groups than reported from registry studies.19,20 This may be due to low or no anticoagulant use in these studies or inclusion of patients with a prior history of stroke. The rates of stroke in younger adults with AF in our study were similar or greater than stroke incidence in the other cardiac groups, highlighting that younger patients with AF also carry an elevated risk of stroke, although this may be due to lower usage of oral anticoagulant drugs in younger AF patients. This group should therefore be a critical target for anticoagulation therapy in a clinical setting, irrespective of having a lower CHA2DS2-VASc score because of their younger age.
Women with cardiac disease appear to have greater stroke incidence than males with cardiac disease. This contrasts with findings from stroke incidence studies conducted within the general population where the incidence of stroke predominates in males, highlighting that the presence of cardiac disease imposes a considerable burden of stroke among females.21 A similar disparity between females and males was also notable in people with single and multiple cardiac conditions and this disparity increased with age. The cumulative effect of additional cardiovascular risk factors in females associated with increasing age, and the greater adverse effect of conditions such as diabetes, smoking and metabolic syndrome in females, all contributes to greater stroke incidence in elderly females.22 A trend towards greater stroke incidence in 20–54 year old women with multiple cardiac conditions was also observed; this may reflect the large proportion of Aboriginal people with multiple cardiac conditions in this age group (15% versus 7% with single cardiac conditions) and risk factors for stroke compared with non-Aboriginal people.23 Additionally, physician hesitation to prescribe oral anticoagulants for female patients with AF may be due to documented risk of hemorrhage from anti-coagulation therapy in this population.24–26
Stroke incidence is greater in people with new versus pre-existing AF or VHD. This difference was particularly marked in those with AF and probably reflects long-term implementation of evidence-based treatment strategies in people with longstanding AF and the inclusion of AF survivors in the pre-existing cohort. Our finding that 42% of strokes occur concurrently with the first cardiac hospitalization, together with prior findings that strokes in patients with AF occur within the first year of AF diagnosis,19 further highlights the importance of screening for AF, and early treatment once diagnosed.
Strengths and Limitations
Our study addresses the gap in the literature for a cohort study with long-term (five-year) follow-up to investigate the burden of stroke in a population comprised of both prevalent and incident cardiac cases. A major strength of this study is access to three decades of whole-population high-quality linked health data, enabling investigation of long-term stroke and cardiac history. Most studies of stroke incidence in cardiac disease are conducted in single cardiac disease populations. In contrast, investigating three major cardiac conditions enabled us to demonstrate important differences and interactions in stroke burden according to cardiac disease type and the presence of multiple diseases. There are also some limitations. Hospital administrative data comprise cardiac events treated in hospital thereby missing lesser severity or stable conditions diagnosed and treated exclusively in primary care. It is estimated that between 50% and 70% of people with AF are managed in primary care, although it is not clear what percentage of these patients are not captured in hospitalization data.27 Therefore, our results may be only generalizable to patients with more severe AF or AF with concurrent conditions necessitating hospitalization, however this most likely would not affect the interpretation of the results for VHD and CHD. In addition, we did not have data on individual drug treatment; our AF cohort would have had variable exposure to oral anticoagulants which would reduce the risk of stroke, and we could not determine whether differences across population groups were attributable to differences in drug adherence. Furthermore, for the 42% of people with a first cardiac admission and concurrent stroke, the assumptions of person-year time may have resulted in some over-estimate of stroke incidence.
Implications and Future Directions
Our study highlights the need for early detection of AF across age- and sex-groupings to ensure early initiation of guideline-directed treatment. Older women with major cardiac diseases, in particular, should be targeted for prevention of stroke. The high-risk period following a first cardiac hospitalization demonstrates the need for ensuring continuation of care following discharge from hospital to reduce stroke risk. Further studies linking Australian Pharmaceutical Benefits Scheme data to determine the proportion of the cardiac cohort on relevant drug therapy and effects of changing patient management on stroke incidence would provide an opportunity to better understand the interplay between various risk factors and impact of treatment in large populations of patients with the three cardiac conditions. Primary care data would also be of interest to investigate any differences between people with community-managed cardiac diseases relative to those admitted to hospital for these conditions.
Conclusion
This study demonstrates the considerable stroke burden in people with one or more of AF, CHD or VHD, particularly in older females, and thus people with these conditions are important targets for reducing stroke incidence. The large incidence of stroke among people admitted to hospital with new onset cardiac disease highlights the importance of prompt, optimal clinical management following diagnosis of cardiac conditions to reduce the risk of stroke. Our findings demonstrated higher than expected rates of stroke in young people with AF, indicating that current guidelines advising drug therapy based on the CHA2DS2-VASc score (which weights age heavily) should be re-visited. Because nearly half of all people at stroke onset were newly diagnosed with a cardiac condition, regular screening for these conditions may be required to improve the prevention of stroke.
Data Sharing Statement
Data for this study are provided by the WA Department of Health and are not able to be shared with external parties due to governance restrictions.
Ethics Approval
The study was conducted after approval by the WA Department of Health Human Research Ethics Committee (2014/55). Use of the data was approved under a waiver of informed consent. The data accessed was de-identified (anonymized) and complied with the data protection and privacy regulations relevant to WA. No other approvals were required for data access.
Acknowledgments
We thank the following for data: WA Data Linkage Branch and WA Department of Health data custodians for Hospital Morbidity Data Collection and Death Registrations data; the Australian Co-ordinating Registry, the Registries of Births, Deaths and Marriages, the Coroners, the National Coronial Information System and the Victorian Department of Justice and Community Safety, for enabling use of cause of death data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is funded by a National Health and Medical Research Council of Australia Synergy grant # 1182071.
Disclosure
LN and JK are funded by National Heart Foundation of Australia Future Leader Fellowships. The authors report no other conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
2. Petersen P, Godtfredsen J. Risk factors for stroke in chronic atrial fibrillation. Eur Heart J. 1988;9(3):291–294. doi:10.1093/oxfordjournals.eurheartj.a062499
3. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. J Am Heart Assoc. 1991;22:983–988.
4. Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991;22(3):312–318. doi:10.1161/01.STR.22.3.312
5. Odutayo A, Wong CX, Hsiao AJ, Hopewell S, Altman DG, Emdin CA. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and meta-analysis. BMJ. 2016;354:i4482. doi:10.1136/bmj.i4482
6. O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–775. doi:10.1016/S0140-6736(16)30506-2
7. Steg PG, Bhatt DL, Wilson PW, et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA. 2007;297(11):1197–1206. doi:10.1001/jama.297.11.1197
8. Yiin GS, Howard DP, Paul NL, et al. Age-specific incidence, outcome, cost, and projected future burden of atrial fibrillation-related embolic vascular events: a population-based study. Circulation. 2014;130(15):1236–1244. doi:10.1161/CIRCULATIONAHA.114.010942
9. Zeymer U, Senges J, Parhofer KG, Rother J. Risk factors and event rates in patients with atherothrombotic disease in Germany: results of the REACH registry. Dtsch Arztebl Int. 2008;105(45):769–775. doi:10.3238/arztebl.2008.0769
10. Sarink D, Nedkoff L, Briffa T, et al. Trends in age- and sex-specific prevalence and incidence of cardiovascular disease in Western Australia. Eur J Prev Cardiol. 2018;25(12):1280–1290. doi:10.1177/2047487318786585
11. Mitchell LB, Southern DA, Galbraith D, et al. Prediction of stroke or TIA in patients without atrial fibrillation using CHADS 2 and CHA 2 DS 2 -VASc scores. Heart. 2014;100(19):1524–1530. doi:10.1136/heartjnl-2013-305303
12. Feigin VL, Stark BA, Johnson CO; Global Burden of Disease Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
13. Cordero A, Rodriguez-Manero M, Garcia-Acuna JM, et al. Incidence and predictors of stroke in patients discharged with the diagnosis of acute coronary syndrome. Int J Cardiol. 2019;276:20–25. doi:10.1016/j.ijcard.2018.10.082
14. Hurskainen M, Tynkkynen J, Eskola M, Hernesniemi J. Incidence of stroke and mortality due to stroke after acute coronary syndrome. J Stroke Cerebrovasc Dis. 2022;31(12):106842. doi:10.1016/j.jstrokecerebrovasdis.2022.106842
15. Petersen JK, Butt JH, Yafasova A, et al. Incidence of ischaemic stroke and mortality in patients with acute coronary syndrome and first-time detected atrial fibrillation: a nationwide study. Eur Heart J. 2021;42(44):4553–4561. doi:10.1093/eurheartj/ehab575
16. Raposeiras-Roubin S, Dominguez-Erquicia P, Abu-Assi E, et al. Effect of mitral regurgitation on stroke risk in patients with non-rheumatic atrial fibrillation. Arch Cardiovasc Dis. 2022;115(8–9):448–456. doi:10.1016/j.acvd.2022.05.006
17. Andreasen C, Gislason GH, Kober L, et al. Incidence of ischemic stroke in individuals with and without aortic valve stenosis: a Danish retrospective cohort study. Stroke. 2020;51(5):1364–1371. doi:10.1161/STROKEAHA.119.028389
18. Katzenellenbogen JM, Bond-Smith D, Seth RJ, et al. Contemporary incidence and prevalence of rheumatic fever and rheumatic heart disease in Australia using linked data: the case for policy change. J Am Heart Assoc. 2020;9(19):e016851. doi:10.1161/JAHA.120.016851
19. Son MK, Lim NK, Kim HW, Park HY. Risk of ischemic stroke after atrial fibrillation diagnosis: a national sample cohort. PLoS One. 2017;12(6):e0179687. doi:10.1371/journal.pone.0179687
20. Suzuki S, Yamashita T, Okumura K, et al. Incidence of ischemic stroke in Japanese patients with atrial fibrillation not receiving anticoagulation therapy--pooled analysis of the Shinken Database, J-RHYTHM Registry, and Fushimi AF Registry. Circ J. 2015;79(2):432–438. doi:10.1253/circj.CJ-14-1131
21. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American heart association. Circulation. 2021;143(8):e254–e743. doi:10.1161/CIR.0000000000000950
22. Haast RA, Gustafson DR, Kiliaan AJ. Sex differences in stroke. J Cereb Blood Flow Metab. 2012;32(12):2100–2107. doi:10.1038/jcbfm.2012.141
23. Nedkoff L, Kelty EA, Hung J, Thompson SC, Katzenellenbogen JM. Differences in stroke risk and cardiovascular mortality for Aboriginal and other Australian patients with atrial fibrillation. Med J Aust. 2020;212(5):215–221. doi:10.5694/mja2.50496
24. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139(11):893–900. doi:10.7326/0003-4819-139-11-200312020-00007
25. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351–358. doi:10.4330/wjc.v3.i11.351
26. Yong CM, Tremmel JA, Lansberg MG, Fan J, Askari M, Turakhia MP. Sex differences in oral anticoagulation and outcomes of stroke and intracranial bleeding in newly diagnosed atrial fibrillation. J Am Heart Assoc. 2020;9(10):e015689. doi:10.1161/JAHA.120.015689
27. Wakai A, O’Neill JO. Emergency management of atrial fibrillation. Postgrad Med J. 2003;79(932):313–319. doi:10.1136/pmj.79.932.313
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.