Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
The Need for Speed: A Qualitative Study on Nurse Recruitment and Management Amidst the COVID-19 Pandemic in Indonesia
Authors Efendi F ![]() , Aurizki GE
, Aurizki GE ![]() , Auwalin I, McKenna L
, Auwalin I, McKenna L ![]()
Received 21 April 2022
Accepted for publication 15 August 2022
Published 27 August 2022 Volume 2022:15 Pages 1809—1817
DOI https://doi.org/10.2147/JMDH.S370758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ferry Efendi,1,2 Gading Ekapuja Aurizki,1,2 Ilmiawan Auwalin,3 Lisa McKenna4
1Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia; 2Community, Family and Gerontological Nursing Research Group, Universitas Airlangga, Surabaya, Indonesia; 3Faculty of Economics and Business, Universitas Airlangga, Surabaya, Indonesia; 4School of Nursing and Midwifery, La Trobe University, Melbourne, Victoria, Australia
Correspondence: Ferry Efendi, Faculty of Nursing, Universitas Airlangga, Campus C Mulyorejo, Surabaya, East Java, 60115, Indonesia, Tel +62 31 591 3754, Email [email protected]
Introduction: Nursing workforce is a pivotal element in tackling the COVID-19 pandemic. However, this has not been comprehensively discussed, particularly in Indonesia. This study aimed to explore stakeholders’ perspectives on Indonesian nursing workforce recruitment and management during the COVID-19 pandemic.
Methods: This study employed a qualitative design with an exploratory descriptive approach. Stakeholders who recruited and managed nursing resources in Indonesia were involved. In-depth interviews and focus group discussions with stakeholders representing eight different institutions were undertaken. Data were analysed using thematic analysis. Eight key stakeholders were interviewed.
Results: Three themes emerged, namely uncertain recruitment system, nursing labour market situation, and workforce management dynamics. COVID-19 caused reduced workforce capacity and increased demands for health professionals, especially nurses.
Conclusion: Uncertainty and volatility happened at the recruitment and management of nursing human resources during the pandemic. Stakeholders were not convinced of overall quality of local nurses recruited to care for COVID-19 patients given workforce was dominated by new graduates and nurses without specialistic qualifications. Employers gave new staff more training to ease their deployment to COVID-19 units to make up for the nurses’ lack of expertise and experience.
Keywords: adaptive management, COVID-19, health worker, labour market, pandemic, personnel management
Introduction
COVID-19 has had unprecedented impacts on global health workforce.1 Despite a significant reduction in general healthcare utilisation during the pandemic, demand for health professionals to manage and treat COVID-19 patients increased.2 International health systems have needed to expand workforce capacity to minimise the negative impact of lack of workforce3 while working to protect existing workers from infection and death. Since the pandemic started, countless health care workers (HCWs) have died or suffered physical and psychological issues and undoubtedly hindered surge capacity.4,5
However, the pandemic has provided opportunities to build sustainable and long-term-oriented health workforces.6,7 One study proposed to meet nursing surge capacity amid the pandemic using standardised staffing ratios based on patient needs and recruiting additional intensive care unit (ICU) staff from internal/external sources, team-based approaches, and training models for ICU-tiered staffing.8 Individual countries have employed strategies to expand health workforce, such as reassigning existing staff to COVID-19 units, involving medical or nursing students, redeploying retired or inactive health professionals, employing foreign-trained health professionals, and recruiting volunteers and others (eg, private or military).9–11
Nurses, the largest group of HCWs globally, are considered the health care system’s backbone12 and vital in overcoming COVID-19.13 International data show countries with high concentrations of nurses are more likely to have lower mortality risk. For every additional nurse per 1000 nurses, a country’s COVID-19-related mortality decreased by 1.98 per 1,000,000 people.14 Nevertheless, many countries still struggle to fill nursing vacancies because of pre-existing global shortages,15,16 impacting efforts to combat the pandemic. Moreover, current situations could affect people’s future interest in entering the nursing profession.17
Among the worst pandemic-affected countries, Indonesia’s workforce capacity was considered inadequate to manage the surge of COVID-19 cases. Health professionals to population ratios are still below standard and unequally distributed across the country’s regions.18 Moreover, Indonesia’s health professional mortality during the pandemic has been among the highest worldwide. By 10 December 2021, this was around 1435 per 100,000 COVID-19-related deaths. Of 2066 HCWs who died, 670 (32.4%) were nurses.19
Amidst the global nursing shortage, Indonesia is one of the few countries to report a nursing excess.20 In 2018, around 250,000 Indonesian nurses were reportedly job searching; however, to achieve ideal nurse-to-population ratios, less than 30,000 were needed. Therefore, the net excess was estimated at 220,000 nurses.21 Production of nurses has been high, at >350,000 per year, but the domestic market lacks capacity to absorb all graduates.21,22
Extensive nursing unemployment is problematic in normal circumstances; however, during COVID-19 has been advantageous for Indonesia. Health facilities benefited from oversupply and opened nursing vacancies for short durations to acquire required numbers as potential applicant numbers were vast. Moreover, in 2021, the Indonesian government allocated nearly IDR 6 trillion (around US$400 million) towards financial incentives for every HCW taking care of COVID-19 patients, including those working in private health facilities,23 allowing facilities to recruit additional HCWs, especially nurses.
In Indonesia, nurses can be recruited through several paths, namely public (ie, civil servant, contract worker, and special assignment) and private (ie, permanent and contract staff).24 The public recruitment is organised by the government agencies in the national, provincial, and district/municipality levels. Despite the levels, these agencies have non-hierarchical relationship and their own areas of authority to recruit health care workers.25 The training and recruitment process of nurses have been described in the previous study by the authors using a nursing labor market framework.26
Some articles discussed nursing management during COVID-19 pandemic from the nurse manager’s perspective.27–31 However, only one Iranian study was located discussing the recruitment aspect.32 The study identified three themes: recruitment of volunteer and non-volunteer workforces; flexible work arrangements and rearrangements; and retention strategies employing preventive and motivational measures, and psychological supports.32 Given the uniqueness of the Indonesian nursing labour market, this study sought to explain how nursing workforce has been managed and how key stakeholders, including government and health care facilities, met requirements and perceived nursing quantity and quality available during the pandemic.
Objective
To explore key stakeholders’ perspectives on recruiting and managing nursing workforce during the COVID-19 pandemic.
Materials and Methods
An exploratory descriptive approach33 was used to investigate nursing workforce recruitment and management practices during the pandemic from stakeholders’ perspectives. This approach is suitable for new or rarely discussed topics.33 Twenty-two health care institutions that carried out nursing recruitment during the COVID-19 pandemic were invited by mail, email, phone and personal correspondence. The institutions were asked to be represented by their nurse managers, human resource managers or institution heads who understand nursing management and the recruitment process. Some invited institutions refused to participate, did not answer the invitation, or could not attend the scheduled sessions. The response rate is quite low as most of them are busy managing human resources for health at their institution. Only eight agreed to participate, including five hospitals, one central government ministry, one COVID-19 task force and one human resource development institute.
Data were collected by focus group discussions (FGDs) and in-depth interviews in Bahasa Indonesia. The FGD durations were around 2–3 hours, while the interviews were between 30 and 60 minutes. The FGD was led by one team member, while individual interviews were conducted by two team members with nursing backgrounds. A set of semi-structured questions was developed that focused on six aspects: 1) planning for nursing personnel; 2) nurse availability in labour markets; 3) strategies to attract nurses; 4) recruitment processes; 5) selection processes; and 6) deployment. Semi-structured questions asked during the interviews and FGDs were described in Appendix 1. All were contextualised to the pandemic situation. FGDs and interviews were audio-recorded and transcribed verbatim with field notes kept. Data organisation, coding and analysis was assisted by NVivo. The author names and information were removed from the transcript to protect their privacy. All data were kept by the research team and cannot be accessed by unauthorised individuals in a restricted cloud service.
Data collection was conducted from June to October 2021. Two FGDs in Surabaya involved two and three participants respectively, followed by three individual in-depth interviews in Surabaya, Jakarta and Bali. Between July and September, research activities were postponed due to significant COVID-19 cases and central government’s implementation of Community Activities Restrictions Enforcement.
Data were analysed using thematic analysis informed by Vaismoradi et al, suitable for identifying, analysing and reporting patterns on qualitative data with low interpretation levels.34 Transcripts were read and re-read and data imported into NVivo to identify codes. Codes addressing similar topics were grouped into sub-themes and themes. A series of team discussions on themes were held until consensus was reached. Conclusions were returned to participants to ensure original meanings were captured.
Ethical approval was obtained from the Health Research Ethics Committee of the Faculty of Nursing, Universitas Airlangga (Certificate Number: 2292-KEPK). Participants provided written consent after being fully informed about the research and participation was voluntary. All of the responses were anonymised to protect the privacy of participants.
Results
Eight key stakeholders were interviewed representing eight institutions. Public and private organisations were equally represented (Table 1). Three themes emerged, namely uncertain recruitment system, nursing labour market situation, and workforce management dynamics, and nine sub-themes.
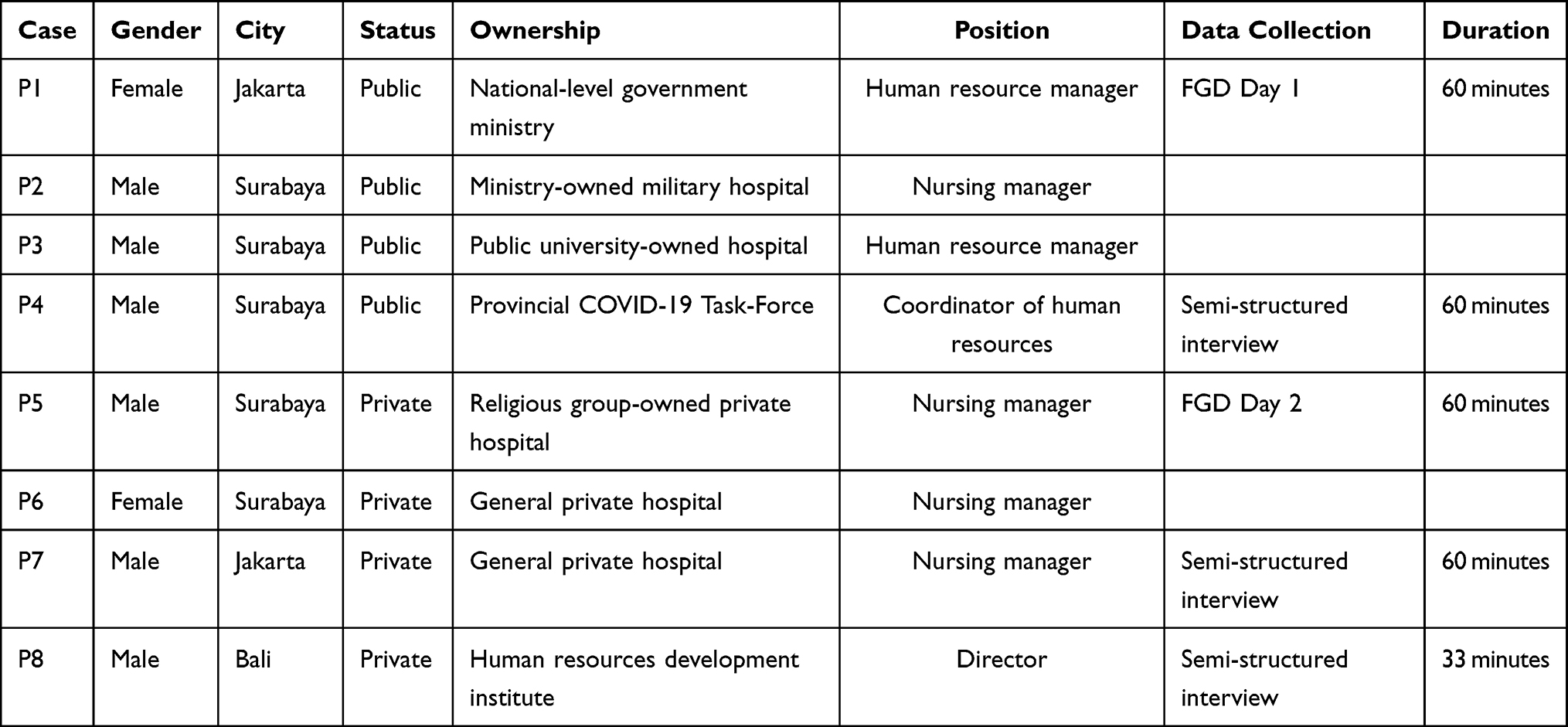 |
Table 1 Participant Characteristics |
Theme 1: Uncertain Recruitment System
Need to recruit quickly within non-ideal labour market situations led nursing recruitment to become uncertain. Employers reported being forced to compromise quality to fulfil demand. As recruits were mostly new graduates and generalists, employers faced dilemmas about where to place them, and offered short-term contracts assuming the pandemic was temporary.
Recruiting Fast, Compromising Quality
Several hospital stakeholders revealed having no choice but accept underqualified applicants to meet needs. Often set selection processes just became formalities.
When the situation is in crisis, we’ll immediately choose whoever can work immediately after being asked to come tomorrow. That’s what we have done so far. Sure, sometimes it sacrifices quality because all cannot be screened completely. At least, for field hospitals like us, if they can do swabs and basic care that is enough. (P4)
Now it is not easy to get volunteers. It’s different from the first and second waves as then we could make rigorous selections. Right now, we cannot be that selective. They only need to have a registration certificate, sign the contract and pass a medical check-up. The test is just a formality. (P2)
Short-Term Employment Contracts
Several hospital stakeholders stated new recruits or volunteers were only offered short-term contracts because they felt the COVID-19 peak would not last long.
For volunteers, since July last year, we’ve recruited as many as 22. When in March the cases decreased, we laid them off. We contracted the nurses for six months last year. Right now, we have opened it again to add 13 volunteers so the total will be around 30 volunteers. However, it’s tough … past volunteers, maybe because they’ve already had experience, have been recruited elsewhere … days ago we called 12, but only five came. (P5)
Finally, the volunteers, when COVID-19 was slightly decreasing … were terminated or no longer available … we recruited contract employees … from the hospital budget. Right now, we have non-permanent employees for COVID. They’re contracted with a particular scheme, which was for a three-month period. (P3)
Deployment Dilemma
Employers reported dilemmas in placing their new recruits because most were new graduates and without special skills. These employers had expected new staff could be immediately deployed to crucial posts such as COVID-19 wards or critical care units.
… we were extremely overwhelmed with where to place the workforce to synergise them with the volunteers. That’s where we were a bit troubled. Because they’re coming from a new program and not experienced yet. Though they have already had many experiences, working mechanisms in other hospitals may be different from ours. (P2)
I notice in nursing alone, it’s slightly … difficult to arrange placement. As there were a lot of new graduates, for us to allocate the person-in-charge (PIC) for the ward, especially nurses, was difficult. One PIC could handle five or six nurses in one shift. If there were five nurses on duty, the PIC was only one, the rest were new graduates. (P7)
Theme 2: Nursing Labour Market Situation
Stakeholders described problems faced managing nursing workforce during the pandemic. These were mainly around lack of hospital staff capacity, while COVID-19 cases were rising increased demand for nurses. Hospital managements responded to surging demand by recruiting additional workforce but determined that available nurses in the market did not meet expectations in terms of experience and skills.
Reduced Capacity and Surging Demand
Some stakeholders revealed that staff capacity in hospitals was severely insufficient as many workers were infected by COVID-19 whilst cases quickly escalated. This precipitated surging demand for nurses.
Many institutions made requests to the Ministry of Health for volunteer help because their health workers had already … collapsed. [The workers] had already been exposed to COVID so could not work and they needed extra workers. Thousands were proposed to the Ministry of Health. (P1)
We added [new employees] by calculating who were positive; that must be calculated. If they were already positive, for two to three weeks they cannot be utilised because they should be in self-isolation. So, we had to strategise at that moment. That makes our jobs very dynamic. (P3)
Abundant Quantity but Varying Quality
Most stakeholders believed the numbers of nurses available in the domestic market was abundant. However, qualities among nurses varied greatly and many were ineligible for employment.
I cannot predict the exact number, but in principle there are plenty. As an illustration, on two different occasions, which were coincidentally close, December and January, we needed so many, applicants were around three times the number of vacancies. (P2)
It’s neither easy nor difficult to recruit nurses. When we opened applications, there were lots of nurses applying … But in the middle of the selection process, they usually failed the test and interview phases. That’s the tricky aspect for me. As of today, there are ten nurse applicants, but the ‘Okay’, who passes based on qualifications, we expect, is only one. (P7)
New Graduate and Nurse Generalist Dominance
Most stakeholders expected experienced and skilled nurses, but candidates who applied to their institutions were mostly new graduates or nurses without specialist skills. Stakeholders reported that recruiting nurses with special qualifications (eg ICU, anaesthetics, scrub nurses, haemodialysis) was difficult as they were rare in the market. They resorted to sending generalist nurses to undertake continuing education and guaranteed tuition.
We want to be like other hospitals which are able to recruit work-ready nurses who are medical-surgical experts, have ICU backgrounds or may be haemodialysis or chemotherapy nurses … Nurses who applied for our jobs were mostly new graduates or generalist nurses. (P2)
Regarding ICU, we were sending our nurses to training programmes, not recruiting new. The difficult ones are the likes of instrument nurses, anaesthesia and haemodialysis. If there’s any, we will give them offers as these nurses are rare. (P5)
Theme 3: Workforce Management Dynamics
The pandemic made human resource management very dynamic. Since COVID-19 was an unprecedented phenomenon, health workers needed additional knowledge and skills. In addition, management agility and leadership became more important to support staff health, both physically and psychologically.
Need for Additional Training
Stakeholders reported concerns about quality of nurses, expressing that additional training was needed to enhance their knowledge and skills to enable appropriate patient care during the pandemic.
The infection prevention and control team taught nurses how to wear personal protective equipment [PPE] properly. Because in COVID rooms there are some people who need high-level PPE, or basic PPE when they do not make contact with patients, we did it gradually. However, we did socialisation or learning processes really quick. Because this is a new situation compared to before when COVID-19 didn’t exist. There’s a lot online learning and we sent the nurses videos on steps and methods for wearing PPE in COVID rooms. (P7)
In the past, we had one week for orientation. There was theoretical orientation, followed by field orientation; the model was purposefully designed like that. However, now, the process is modified to become quicker. In the morning, there’s theoretical orientation, covering the likes of handwashing, quality, infection prevention and control, more about accreditation, and so on. Of course, field orientation is also carried out, but now it becomes quicker because the need is urgent … Sometimes we give other materials, but most importantly we make Zoom meetings at night. This means that ‘training by doing’ appears now. (P3)
Leadership and Management Agility
Some stakeholders identified bureaucratically pandemic handling was quite slow, but lower-level management always had ways to overcome problems faced. They reported being able to redeploy human resources from less urgent to more crucial units. In some cases, they closed non-COVID-19 units.
Responding to current cases … sometimes regulations are not as fast to respond to existing conditions such as this pandemic, everything is all of a sudden. It’s so fast. Sometimes regulations must be tossed around. It can’t widely give an immediate response to what happens. It always takes time. That’s what sometimes makes the implementation like it is … stuttering. It’s not that smooth. (P1)
The problem now is that when COVID rises again, it rises really fast. From an occupancy of about 20-30% yesterday, suddenly it was 80 or even 90%, sometimes 100%. Such increase cannot be followed by our recruitment speed and bureaucracy … finally what can be done is moving human resources … like nurses from surgical wards which may not be too productive, where there are not many patients. (P4)
Prioritising Employees’ Health and Wellbeing
Employers reported enacting policies to place staff with comorbidities in “green zone”, non-COVID-19 units. They provided supplementary nutrition for nurses and other employees, psychological assessment, and rewards. All hospital stakeholders also reported carrying out routine employee check-ups.
We put nurses with comorbidities in the green zone. Nurses who are pregnant, breastfeeding, elderly, or who have comorbid diseases are not allowed to work in COVID areas. So, we distinguish between green and red areas. (P5)
At the beginning of the pandemic, there was a suggestion those to receive additional feeding and vitamins should be nurses in isolation rooms. After that, everyone had extra work as well, including nutritionists, pharmacists, and so on. Finally, they all got supplements, including the Board of Directors. (P6)
Discussion
This study found the nursing labour market in Indonesia was uncertain and volatile. The pandemic increased health workforce demand, especially nursing. Yet, the labour market appeared unprepared for increasing cases and number of health workers needing to be sidelined due to being COVID-19 infected, leading many institutions to quickly recruit. A similar situation was described in one private hospital in Depok, West Java, Indonesia. The hospital’s recruitment sequence was reportedly changed to respond to the situation and standard operating procedures were not fully adhered, so recruitment outcomes did not meet users’ expectations.35 Similarly, Keeley et al in 2020 reported that staffing strategy to expand health workforce in New York City was done in a rapid and uncoordinated manner.36 Despite limited evidence specifically discussing health personnel recruitment during the pandemic, both studies illustrated that in extraordinary situations, services cannot recruit ordinarily. However, success or failure of new recruitment strategies is dependent on several factors, including labour market situation. Short-employment nursing contracts can be a quick fix strategy to meet demand, resulting in short assignments and leading to new unemployment phenomena among recruits, which can be observed following COVID-19 surge cases in Indonesia.
In Indonesia particularly, the existing nursing labour market seemed unable to meet stakeholders’ expectations as it was dominated by new graduates lacking experience, and nurse generalists without specialist skills. However, because of the urgency, employers needed to accept applicants, regardless of quality. Almost all stakeholders perceived nurses were widely available but simultaneously were concerned about shortages of nurses with special skills. This concurs with a policy paper by the Indonesian Ministry of Health highlighting the paradox of surplus and shortage.20 Limited availability of specialised nurses in the market, especially ICU nurses, is a stumbling block for many hospitals in providing optimal services during the pandemic. Although the impact of availability and workload of ICU nurses on mortality rates shows varying results,13 stakeholders assessed that ICU-certified nurses had crucial roles, concurring with Schwerdtle et al in 2020 that the presence of nurses with special skills could make the difference of whether institutions collapsed or survived and numbers of lives lost.37 Moreover, an African study revealed employers preferred specialist over non-specialist candidates.11 Despite the context, the authors believed that their results could be generalised to wider contexts.
Stakeholders reported moving quickly and trying various strategies to overcome the crisis, adapting with emerging situations and available resources. One study revealed an adaptive strategy and investment in health human resources data and research were vital in the midst of the changing and ongoing pandemic.3 A review suggested that adaptive management was needed to manage case spikes amidst infectious disease pandemics.38 Human resources (staff), bed capacity (space), facilities and infrastructure (stuff), and governance (system) all require adaptive management. Managers need to consider how to allocate employees, accommodate choices to withdraw from burdensome roles, anticipate employee shortages, and pay attention to their welfare.38 Furthermore, flexible and situational approaches are needed to recruiting, arranging, and retaining workforce, as well as considering strategies to fill shortages.32
Transfer of nurses into or out of COVID-19 units is one adaptive policy to increase staff and protect employees. However, due to shortages, generalist nurses are often forced into ICU, not only having an impact on services but also on nurses themselves. A Singaporean study revealed generalist nurses working in general wards experienced anxiety and stress when considering high exposure and risks in caring for critically ill patients. Despite challenges, nurses remained committed to their duties wherever they were placed.39 Organisational factors are pivotal to maintaining nurses’ resilience and wellbeing.40 Some stakeholders in this study explained that supports were materialised in regular check-ups, nutritional supplements, and psychosocial motivation and encouragement, corresponding with strong management recommendations to initiate staff surveillance41 and create supportive workplaces.42
Before deployment to new units, nurses need to receive clear messages about what they need to do as well as adequate briefing.39 Non-critical care nurses should receive ICU-focused hands-on training and refresher courses using online materials and instructional videos.41 Simulation-based education can also be utilised to upskill non-ICU nurses for deployment to critical care units.43 Such strategies have been adopted in urgent situations where nurses were untrained to handle COVID-19 patients with demand to immediately utilise available personnel. Moreover, as this study found, COVID-19-related knowledge among Indonesian health professionals was still low.44 One participant raised “training by doing”, as nurses had insufficient time to learn prior, and learning when deployed. This approach is similar to the Training Model for ICU Tiered Staffing Strategy proposed by Al Mutair et al (2020), where two reassigned nurses work directly under an ICU-trained nurse supervision as part of training.8 Amidst many limitations, management must facilitate provision of additional training for nurses ensuring they are capable to undertake new roles.
Limitations
This study included participants from major cities especially Surabaya area, which may not represent the geographical challenges of Indonesia’s rural areas. It is recommended that future research explores the representativeness of rural areas of Indonesia.
Conclusion
COVID-19 surges and lack of health worker capacity due to infection cause increased demand for nurses. Stakeholders reported taking quick action to address shortages by transferring nurses from other areas to work in COVID-19 units and quickly recruiting new employees. However, concerns existed, particularly readiness of reassigned nurses and new recruit quality. Despite the number of nurses in the Indonesian domestic labour market, stakeholders were not convinced of overall quality. To compensate for nurses’ lack of experience and skills, employers provided additional training for new and non-ICU employees to facilitate deployment to COVID-19 units. Nurse managers play critical roles in ensuring a sufficient nursing workforce to meet patient care needs. This is particularly challenging during the COVID-19 pandemic. Adaptive planning strategies should be implemented to meet nursing workforce needs during critical situations, such as pandemics.
Abbreviations
COVID-19, Coronavirus Disease 2019; FGDs, Focus Group Discussions; HCWs, Health Care Workers; ICUs, Intensive Care Units; PPE, Personal Protective Equipment.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Funding
This work was supported by Kementerian Pendidikan dan Kebudayaan, Riset dan Teknologi Republik Indonesia, through Penelitian Dasar Unggulan Perguruan Tinggi (PDUPT) [8/E1/KPT/2021; 4/E1/KP.PTNBH/2021; 546/UN3.15/PT/2021]. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare no conflicts of interest.
References
1. World Health Organization. Health Workforce Policy and Management in the Context of the COVID-19 Pandemic Response. World Health Organization; 2020.
2. Moynihan R, Sanders S, Michaleff ZA, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open. 2021;11(3):e045343. doi:10.1136/bmjopen-2020-045343
3. Gupta N, Balcom SA, Gulliver A, Witherspoon RL. Health workforce surge capacity during the COVID-19 pandemic and other global respiratory disease outbreaks: a systematic review of health system requirements and responses. Int J Health Plann Manage. 2021;36(December2020):26–41. doi:10.1002/hpm.3137
4. Sant’Ana G, Imoto AM, Amorim FF, et al. Infection and death in healthcare workers due to COVID-19: a systematic review. ACTA Paul Enferm. 2020;33:1–9. doi:10.37689/ACTA-APE/2020AO0107
5. Şahin MK, Aker S, Şahin G, Karabekiroğlu A. Prevalence of Depression, Anxiety, Distress and Insomnia and Related Factors in Healthcare Workers During COVID-19 Pandemic in Turkey. J Community Health. 2020;45(6):1168–1177. doi:10.1007/s10900-020-00921-w
6. Rees GH, Peralta Quispe F, Scotter C. The implications of COVID-19 for health workforce planning and policy: the case of Peru. Int J Health Plann Manage. 2021;36(December2020):190–197. doi:10.1002/hpm.3127
7. Bourgeault IL, Maier CB, Dieleman M, et al. The COVID-19 pandemic presents an opportunity to develop more sustainable health workforces. Hum Resour Health. 2020;18(1):1–8. doi:10.1186/s12960-020-00529-0
8. Al Mutair A, Amr A, Ambani Z, Al SK, Schwebius D. Nursing Surge Capacity Strategies for Management of Critically Ill Adults with COVID-19. Nurs Reports. 2020;10(1):23–32. doi:10.3390/nursrep10010004
9. Williams BGA, Maier CB, Scarpetti G, et al. What strategies are countries using to expand health workforce surge capacity during the COVID-19 pandemic? Eurohealth. 2020;26(2):51–57.
10. Waitzberg R, Hernández-Quevedo C, Bernal-Delgado E, et al. Early health system responses to the COVID-19 pandemic in Mediterranean countries: a tale of successes and challenges. Health Policy (New York). 2021;12:18. doi:10.1016/j.healthpol.2021.10.007
11. Mkenda V, Woolhouse M, Mutapi F, Banda G. Recruiting students for the COVID-19 emergency response: lessons from eight African countries. AAS Open Research. 2020;3:42. doi:10.12688/aasopenres.13115.1
12. WHO. State of the World’s Nursing 2020: Investing in Education, Jobs and Leadership. World Health Organization; 2020.
13. Wynne R, Davidson PM, Duffield C, Jackson D, Ferguson C. Workforce management and patient outcomes in the intensive care unit during the COVID-19 pandemic and beyond: a discursive paper. J Clin Nurs. 2021;1(April):1–10. doi:10.1111/jocn.15916
14. Padula WV, Davidson P. Countries with High Registered Nurse (RN) Concentrations Observe Reduced Mortality Rates of Coronavirus Disease 2019 (COVID-19). SSRN Electron J. 2020;2019:548. doi:10.2139/ssrn.3566190
15. Marć M, Bartosiewicz A, Burzyńska J, Chmiel Z, Januszewicz P. A nursing shortage – a prospect of global and local policies. Int Nurs Rev. 2019;66(1):9–16. doi:10.1111/inr.12473
16. Drennan VM, Ross F. Global nurse shortages - The facts, the impact and action for change. Br Med Bull. 2019;130(1):25–37. doi:10.1093/bmb/ldz014
17. Mannino JE, Watters P, Cotter E, et al. The Future Capacity of the Nursing Workforce. Nurse Educ. 2021;6:342–348. doi:10.1097/nne.0000000000001078
18. Mahendradhata Y, Andayani NLPE, Hasri ET, et al. The Capacity of the Indonesian Healthcare System to Respond to COVID-19. Front Public Heal. 2021;9(July):1–9. doi:10.3389/fpubh.2021.649819
19. Lapor Covid-19. Pusara Digital Tenaga Kesehatan. Published 2021. Accessed December 9, 2021. https://nakes.laporcovid19.org/statistik
20. Kurniati A, Astari LD, Efendi F, et al. Analisis Kebijakan Pemenuhan Pasar Kerja Tenaga Kesehatan Di Tingkat Global. Badan Pengembangan dan Pemberdayaan SDMK Kemenkes RI; 2020.
21. Ministry of Manpower. Analisis Pasar Kerja: Ketersediaan Dan Kebutuhan Tenaga Kerja Perawat. Kementerian Ketenagakerjaan Republik Indonesia; 2019.
22. Ministry of Health. Human Resources for Health Country Profiles: Indonesia. Kemenkes; 2019.
23. Ministry of Health. Kemenkes Telah Bayarkan Insentif Nakes Pusat Tahun 2021 Sebesar Rp 5865 Triliun. Sehat Negeriku; 2021.
24. Efendi F. The Situational Analysis of Nursing Education and Workforce in Indonesia. Malaysian J Nurs. 2018;9:20–29.
25. Mahendradhata Y, Trisnantoro L, Listyadewi S, et al. The Republic of Indonesia Health System Review. Vol 7.; 2017. Accessed September 6, 2018. http://apps.who.int/iris/bitstream/handle/10665/254716/9789290225164-eng.pdf;jsessionid=433D7EB61E6C8DDB4F75C6675AAB13BF?sequence=1
26. Efendi F, Aurizki GE, Auwalin I, et al. The Paradox of Surplus and Shortage: a Policy Analysis of Nursing Labor Markets in Indonesia. J Multidiscip Healthc. 2022;15:
27. White JH. A Phenomenological Study of Nurse Managers’ and Assistant Nurse Managers’ Experiences during the COVID-19 Pandemic in the United States. J Nurs Manag. 2021;29(6):1525–1534. doi:10.1111/jonm.13304
28. Kagan I, Shor R, Ben Aharon I, et al. A Mixed-Methods Study of Nurse Managers’ Managerial and Clinical Challenges in Mental Health Centers During the COVID-19 Pandemic. J Nurs Scholarsh. 2021;53(6):663–670. doi:10.1111/jnu.12685
29. Moyo I, Mgolozeli SE, Risenga PR, et al. Experiences of Nurse Managers during the COVID-19 Outbreak in a Selected District Hospital in Limpopo Province, South Africa. Healthc. 2022;10:1. doi:10.3390/healthcare10010076
30. Jackson J, Nowell L. ‘The office of disaster management’ nurse managers’ experiences during COVID-19: a qualitative interview study using thematic analysis. J Nurs Manag. 2021;29(8):2392–2400. doi:10.1111/jonm.13422
31. Gab Allah AR. Challenges facing nurse managers during and beyond COVID-19 pandemic in relation to perceived organizational support. Nurs Forum. 2021;56(3):539–549. doi:10.1111/nuf.12578
32. Poortaghi S, Shahmari M, Ghobadi A. Exploring nursing managers’ perceptions of nursing workforce management during the outbreak of COVID-19: a content analysis study. BMC Nurs. 2021;20(1):27. doi:10.1186/s12912-021-00546-x
33. Hunter DJ, Mccallum J, Howes D. Defining Exploratory-Descriptive Qualitative (EDQ) research and considering its application to healthcare. J Nurs Heal Care. 2019;4:1.
34. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405.
35. Kawedhar W. Analisis Sistem Rekrutmen Dan Seleksi Tenaga Kesehatan Di Rumah Sakit Permata Depok. Universitas Pembangunan Nasional Veteran Jakarta; 2021.
36. Keeley C, Jimenez J, Jackson H, et al. Staffing Up For The Surge: expanding The New York City Public Hospital Workforce During The COVID-19 Pandemic. Health Aff. 2020;39(8):1426–1430. doi:10.1377/hlthaff.2020.00904
37. Nayna Schwerdtle P, Connell CJ, Lee S, et al. Nurse Expertise: a Critical Resource in the COVID-19 Pandemic Response. Ann Glob Heal. 2020;86(1):49. doi:10.5334/aogh.2898
38. Anesi GL, Lynch Y, Evans L. A Conceptual and Adaptable Approach to Hospital Preparedness for Acute Surge Events Due to Emerging Infectious Diseases. Crit Care Explor. 2020;2(4):e0110. doi:10.1097/cce.0000000000000110
39. Tang CJ, Lin YP, Chan E. ‘From Expert to Novice’, Perceptions of General Ward Nurses on Deployment to Outbreak Intensive Care Units during the COVID‐19 Pandemic: a Qualitative Descriptive Study. J Clin Nurs. 2021;1(December 2020):1–13. doi:10.1111/jocn.16029
40. Jo S, Kurt S, Bennett JA, et al. Nurses’ resilience in the face of coronavirus (COVID-19): an international view. Nurs Health Sci. 2021;23(3):646–657. doi:10.1111/NHS.12863
41. Goh KJ, Wong J, Tien JCC, et al. Preparing your intensive care unit for the COVID-19 pandemic: practical considerations and strategies. Crit Care. 2020;24(1):1–12. doi:10.1186/s13054-020-02916-4
42. Vizheh M, Qorbani M, Arzaghi SM, Muhidin S, Javanmard Z, Esmaeili M. The mental health of healthcare workers in the COVID-19 pandemic: a systematic review. J Diabetes Metab Disord. 2020;19(2):1–12. doi:10.1007/s40200-020-00643-9
43. Almomani E, Sullivan J, Hajjieh M, Leighton K. Simulation-based education programme for upskilling non-critical care nurses for COVID-19 deployment. BMJ Simul Technol Enhanc Learn. 2021;7(5):319–322. doi:10.1136/bmjstel-2020-000711
44. Jamil K, Winardi W, Yufika A, et al. Knowledge of coronavirus disease 2019 (COVID-19) among healthcare providers: a cross-sectional study in Indonesia. Asian Pac J Trop Med. 2020;13(9):402–408. doi:10.4103/1995-7645.290584
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Suicide and Suicide Attempts Among Patients Attending Primary Health Care Facilities in Uganda: A Medical Records Review
Kaggwa MM, Rukundo GZ, Wakida EK, Maling S, Sserumaga BM, Atim LM, Obua C
Risk Management and Healthcare Policy 2022, 15:703-711
Published Date: 19 April 2022
COVID-19 Pandemic and Physician Burnout: Ramifications for Healthcare Workforce in the United States
Bhardwaj A
Journal of Healthcare Leadership 2022, 14:91-97
Published Date: 13 June 2022
Behavioural Response To Self-Medication Practice Before and During Covid-19 Pandemic in Western Uganda
Dare SS, Eze ED, Echoru I, Usman IM, Ssempijja F, Bukenya EE, Ssebuufu R
Patient Preference and Adherence 2022, 16:2247-2257
Published Date: 20 August 2022
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023
Effectiveness of Drug Repurposing and Natural Products Against SARS-CoV-2: A Comprehensive Review
Velásquez PA, Hernandez JC, Galeano E, Hincapié-García J, Rugeles MT, Zapata-Builes W
Clinical Pharmacology: Advances and Applications 2024, 16:1-25
Published Date: 4 January 2024