Back to Journals » International Journal of Women's Health » Volume 18
Telehealth Pathways for Cervical Cancer Prevention: A Scoping Review of Strategies to Close the Screening Gap
Authors Solehati T ![]() , Haroen H, Hazmi HB
, Haroen H, Hazmi HB ![]() , Putri YHS
, Putri YHS ![]() , Khoirunnisa K
, Khoirunnisa K ![]() , Sukmawati S
, Sukmawati S ![]() , Purnama D, Kosasih CE
, Purnama D, Kosasih CE ![]()
Received 22 December 2025
Accepted for publication 4 May 2026
Published 9 June 2026 Volume 2026:18 590474
DOI https://doi.org/10.2147/IJWH.S590474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Tetti Solehati,1 Hartiah Haroen,2 Helmy bin Hazmi,3 Yayu Handayani Syaidar Putri,4 Khoirunnisa Khoirunnisa,5 Sukmawati Sukmawati,1 Dadang Purnama,2 Cecep Eli Kosasih6
1Department of Maternity Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Community Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Kota Samarahan, Sarawak, Malaysia; 4Department of Maternity Nursing, STIKep PPNI Jawa Barat, Bandung, West Java, Indonesia; 5Department of Pediatric Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 6Department of Critical Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Tetti Solehati, Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6281224836837, Email [email protected]
Background: Cervical cancer screening faces significant challenges in low- and middle-income countries. Telehealth has emerged as a potential strategy to overcome barriers to cervical cancer screening; however, its role in improving screening uptake and outcomes remains unclear.
Objective: This scoping review aims to map and synthesize evidence on the role of telehealth in enhancing cervical cancer screening.
Methods: A scoping review was conducted following Arksey and O’Malley’s framework. A comprehensive search was conducted across PubMed, Scopus, and CINAHL for studies published between 2015 and 2025. Studies were included if they examined telehealth interventions related to cervical cancer screening.
Results: A total of 13 studies were included, comprising randomized controlled trials, quasi-experimental studies, and one mixed methods study. Four main categories of telehealth interventions were identified: web-based platforms, mobile and app-based services, virtual education programs, and mobile screening services. Overall, these interventions demonstrated potential to improve access, increase screening uptake, and support follow-up care across diverse settings.
Conclusion: Telehealth represents a promising approach to improving cervical cancer screening access, participation, and follow-up, particularly in underserved populations. By focusing on primary quantitative evidence, this review provides a more targeted understanding of how telehealth can support screening implementation. Further research should evaluate long-term effectiveness, user experience, and the integration into healthcare systems.
Keywords: cervical cancer, screening, scoping review, telehealth, telemedicine
Introduction
Cervical cancer remains a major preventable cause of cancer-related morbidity and mortality among women, particularly in low- and middle-income countries (LMICs).1 Persistent infection with high-risk Human Papillomavirus (HPV) is the principal etiological factor in the development of cervical cancer.2 Among the oncogenic HPV types, HPV 16 and 18 are responsible for approximately 70% of cervical cancer cases globally. If persistent and untreated, these infections may induce cervical intraepithelial lesions that can progress to invasive cervical cancer over time.3 Cervical cancer is the fourth leading cause of cancer deaths in women globally.4 In 2022, an estimated 660,000 women were diagnosed with cervical cancer and approximately 350,000 died from the disease, underscoring its substantial global health burden.5
To address this burden, the World Health Organization (WHO) has launched a global strategy to eliminate cervical cancer through vaccination, screening, and treatment.6 Cervical cancer screening refers to the examination of asymptomatic women to detect high-risk HPV infection, precancerous lesions, or early-stage disease before the onset of symptoms.7 Screening is one component of early detection, a broader concept that also includes the timely diagnosis of women presenting with symptoms suggestive of cervical disease. In this context, HPV DNA testing is an important screening modality because it enables the identification of high-risk HPV infection before progression to cervical precancer or cancer.8 Evidence has consistently shown that cervical cancer screening reduces both incidence and mortality.9,10
Despite the availability of preventive methods such as Pap smears, HPV testing, and Visual Inspection with Acetic Acid (VIA), cervical cancer screening remains underutilized, particularly in rural and underserved areas. It is estimated that more than 1.5 billion women worldwide have never been screened for cervical cancer.11 Barriers such as geographic distance, financial constraints, inadequate healthcare infrastructure, and sociocultural stigma continue to prevent many women from accessing timely screening. These challenges contribute substantially to preventable cervical cancer morbidity and mortality.
Telehealth has emerged as a promising strategy to address barriers to cervical cancer screening by facilitating healthcare delivery, communication, education, and follow-up across distance.12 Broadly, telehealth refers to the use of electronic information and telecommunication technologies to support clinical services, health education, public health activities, and administrative functions. Although telehealth adoption in oncology was limited before the COVID-19 pandemic, its use has expanded substantially in recent years.13,14 In the context of cervical cancer prevention, telehealth may support multiple stages of the screening pathway, including patient education, appointment reminders, risk communication, navigation, result delivery, and referral coordination.
This broader perspective is important because cervical cancer screening is increasingly evolving beyond a single-test approach. While HPV DNA testing is becoming central to contemporary screening strategies and may eventually serve as a primary standalone method, implementation challenges remain in many settings, including limited laboratory capacity, delayed turnaround times, and uneven service readiness. In such contexts, VIA remains relevant as an accessible, low-cost, and rapid complementary approach, particularly in low-resource settings and as part of follow-up or triage pathways for HPV-positive women. Telehealth may therefore support not only screening uptake, but also the integration of HPV DNA testing and VIA through education, coordination, follow-up, provider training, supervision, and quality assurance.
Although telehealth and other digital interventions have increasingly been used to support cancer prevention and screening, evidence specific to cervical cancer screening remains fragmented. Existing reviews often focus on broader digital health strategies, general oncology care, or heterogeneous intervention types, while relatively few have specifically examined how telehealth supports cervical cancer screening pathways.15 In addition, prior syntheses frequently combine diverse study designs, which can limit clarity regarding intervention effectiveness.13 A more focused synthesis of primary quantitative evidence is therefore needed to better understand how telehealth may improve cervical cancer screening uptake and delivery.
This review takes a more focused approach by specifically examining telehealth interventions relevant to cervical cancer screening pathways, including approaches related to both HPV DNA testing and VIA. Unlike broader reviews of digital health in oncology, this scoping review was intentionally limited to primary quantitative studies, including randomized controlled trials, quasi-experimental studies, and mixed methods studies. Although scoping reviews often include broader evidence types, this restriction was applied to provide a clearer synthesis of measurable intervention outcomes, such as screening uptake, participation, and follow-up, while reducing conceptual heterogeneity. This approach was chosen to better inform future intervention design, implementation planning, and policy development.
Accordingly, this scoping review aims to map and synthesize the existing primary quantitative evidence on the role of telehealth in improving cervical cancer screening. By focusing on telehealth-supported screening pathways involving both HPV DNA testing and VIA, this review seeks to identify the effectiveness, implementation opportunities, and remaining challenges of these interventions across different healthcare settings. The findings are expected to inform future research, policy development, and the design of context-appropriate telehealth-supported cervical cancer screening strategies, particularly in resource-constrained and hard-to-reach settings.
Materials and Methods
Study Design
This study employs a scoping review design to explore and synthesize existing evidence on the selected topic, following the framework proposed by Arksey and O’Malley.16 The review follows a five-stage process: 1) formulating research questions; 2) identifying relevant studies; 3) selecting studies based on inclusion criteria; 4) mapping and interpreting the data; and 5) summarizing and reporting the findings. Additionally, the review aligns with the Preferred Reporting Items for Systematic Reviews and Meta-analyses for Scoping Review (PRISMA-ScR) guidelines.17 The research question in this study is what types of telehealth interventions have been used to increase cervical cancer screening, and what are their characteristics, implementation contexts and effectiveness?
Search Strategy
The search strategy was developed using the PCC framework (Population, Concept, Context). The Population included women of childbearing age; and the Concept focused on telehealth interventions for cervical cancer.
A combination of keywords and controlled vocabulary terms (eg, MeSH in PubMed) was systematically applied across PubMed, Scopus, and CINAHL from May to June 2025. Boolean operators (AND, OR) and truncation techniques were used to refine the results. Titles, abstracts, and index terms of retrieved records were analyzed to identify additional relevant keywords, which were incorporated into subsequent searches. The reference lists of included studies were also screened manually to capture any additional eligible articles. The search was limited to publications from 2015 onward, and all references were managed using EndNote.
The search strategy employed multiple combinations of carefully selected keywords: (“Uterine Cervical Neoplasm” OR “Cervical Neoplasms” OR “Cervical Neoplasm” OR “Uterine Cervical Cancer”) AND (“Early detection of cancer” OR “Cancer Early Detection” OR “Early Diagnosis of Cancer” OR “Cancer Screening” OR “Cancer Screening Test” AND “Telehealth” OR “Virtual Medicine” OR “Mobile Health” OR “mHealth” OR “eHealth” OR “Telecare”) AND (“Papanicolaou test” OR “Papanicolaou Smear” OR “Pap Test” OR “Pap Smear”) AND (“cervical smears” OR “Vaginal Smear”) AND “mass screening” AND (“Visual Inspection of Acetic Acid” OR “Visual Inspection” OR “Acetic Acid”) AND “Cell phone” AND (“Text Messaging” OR “Text Message”) AND (“Mobile applications” OR “Smartphone App”). The research question guiding this review is: What is the role of telehealth in improving cervical cancer screening, including its effectiveness, feasibility, and potential to address barriers to access and uptake?
Inclusion and Exclusion Criteria
This review followed the PRISMA Extension for Scoping Reviews (PRISMA-ScR) to guide the identification and selection of evidence on the role of telehealth in improving cervical cancer screening (Figure 1). Specific inclusion and exclusion criteria were established to determine study eligibility.
 |
Figure 1 PRISMA Flow Diagram. |
Studies were included if they: (1) were published between 2015 and 2025; (2) were peer-reviewed and published in English; (3) focused on telehealth interventions aimed at improving cervical cancer screening; (4) used a randomized controlled trial, quasi-experimental, or mixed methods design; (5) were primary studies evaluating an intervention and reported outcomes related to screening uptake, access, participation, follow-up, or patient-related outcomes. Studies were excluded if they: (1) were study protocols; (2) lacked full-text availability; (3) did not focus on cervical cancer screening; (4) did not involve telehealth interventions; (5) were reviews, meta-analyses, editorials, opinion pieces, letters, conference proceedings, dissertations, or theses; (6) constituted secondary analyses or did not involve a primary empirical evaluation relevant to the review objective.
The eligibility criteria were developed to ensure the inclusion of studies directly relevant to the review objective and telehealth-supported cervical cancer screening pathways. These criteria were intended to support a more focused mapping of the available evidence and facilitate interpretation of intervention characteristics and outcomes across studies.
Data Extraction
To extract data, the author uses a table that organizes key information, including the author and year, country, study purpose, population/sample size, age, methodology, study setting, type of screening, intervention components, results, obstacles, and opportunities. This approach facilitates a more efficient analysis of the screened articles.
Quality Appraisal
Although quality appraisal is not a mandatory component of scoping reviews, the authors opted to conduct a methodological assessment to enhance the transparency and rigor of the evidence synthesis. Given the heterogeneity of study designs included in this review, appraisal was deemed necessary to provide context for interpreting the findings and to inform future research recommendations. The appraisal was conducted using the Joanna Briggs Institute (JBI) critical appraisal tool18,19 and the Mixed Methods Appraisal Tool (MMAT) version 2018,20 depending on the study design (Table 1). For quantitative studies, the JBI tool was applied, comprising 13 items for randomized controlled trials and 9 items for quasi-experimental studies, each rated as Yes, No, Unclear, or Not applicable. A score of 1 was assigned for each “Yes” response, while “No” and “Unclear” responses received a score of 0. Studies scoring below 75% were considered low quality and would have been excluded; however, all included quantitative studies met this threshold.
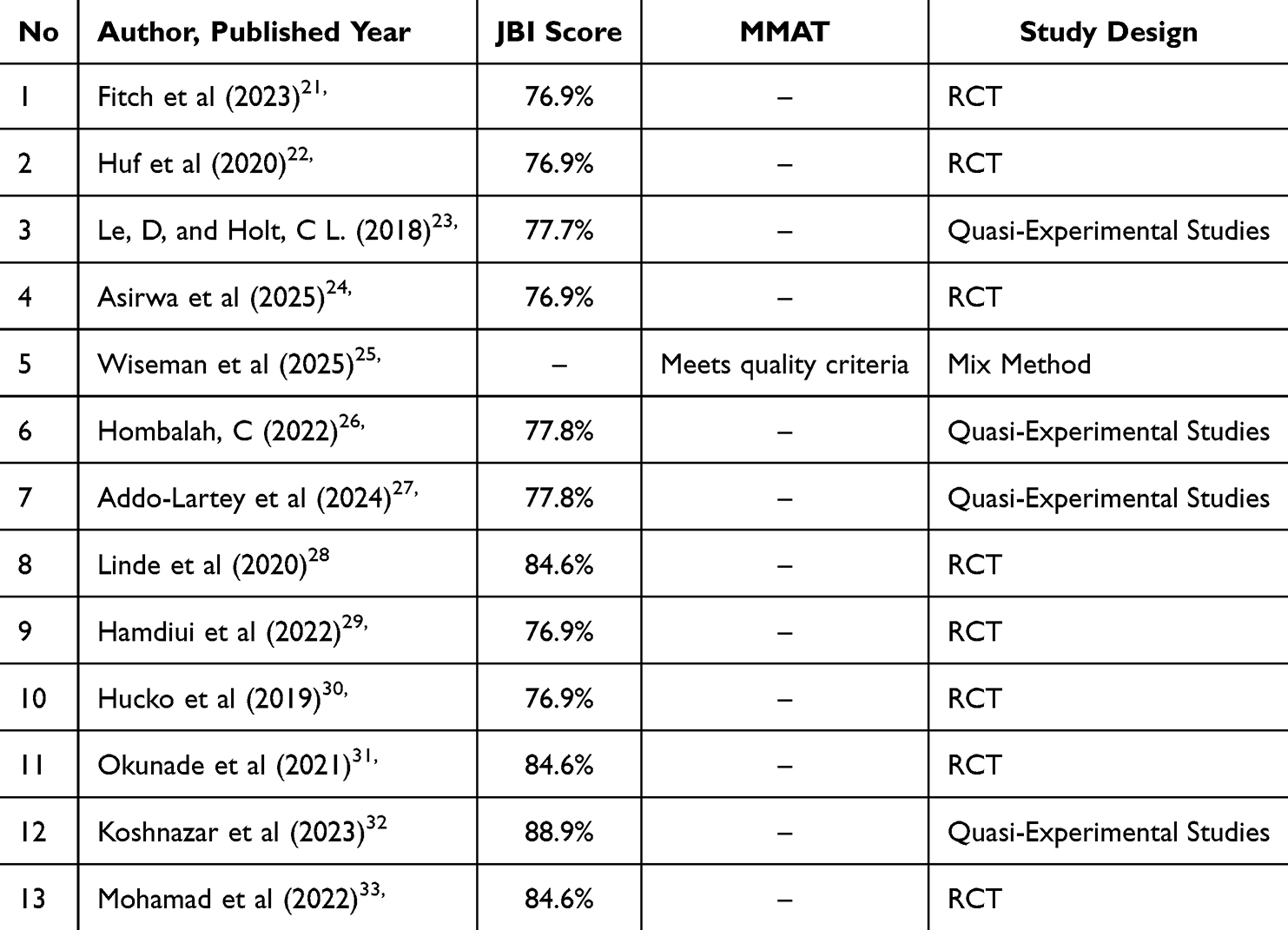 |
Table 1 Critical Appraisal Tool |
For the mixed methods study, the MMAT 2018 was applied to assess the quality of both the qualitative and quantitative components and the extent to which they were effectively integrated. Each criterion was rated as Yes, No, or Cannot tell, and the findings were reported narratively without calculating a total score, in accordance with MMAT guidelines. The mixed methods study included in this review met all applicable quality criteria, indicating satisfactory methodological quality (Table 1).
Results
A total of 13 studies met the inclusion criteria, representing diverse geographical contexts, including high-income countries (United States, United Kingdom, Canada) and low- and middle-income countries (Zambia, India, Tanzania, Nigeria). Study designs included randomized controlled trials, quasi-experimental studies, and one mixed methods study. Overall, four main categories of telehealth interventions were identified: web-based platforms, mobile and app-based strategies, virtual education programs, and mobile screening services (Table 2). Methodological quality of quantitative studies ranged from 76.9% to 100% based on JBI appraisal, while the mixed methods study met all MMAT quality criteria (Table 1).
 |
Table 2 Extraction Data |
Web-Based Telehealth
One RCT evaluated the effectiveness of a web-based educational intervention designed to improve women’s knowledge, attitudes, and intentions to undergo cervical cancer screening.29 The intervention was delivered through an interactive website over a four-week period, providing multimedia educational materials covering reproductive anatomy, cervical cancer risk factors, the importance of Pap smear screening, and HPV vaccination. Results demonstrated that the web-based intervention significantly improved participants’ knowledge and attitudes toward cervical cancer screening compared to the control group (p < 0.001), as well as a significant increase in intention to undergo Pap smear screening (p < 0.05).
Mobile and App-Based Telehealth
Multiple studies examined mobile-based strategies to enhance cervical cancer screening participation, including remote guidance for HPV self-sampling, SMS and telephone-based delivery of test results and reminders, culturally adapted educational messages, and integrated telehealth platforms. Most participants were women of reproductive age from underserved or rural settings. Web-based and video-supported guidance for HPV self-sampling was generally well received, with participants reporting confidence in performing the procedure independently.21–23
Mobile-based strategies using SMS or telephone calls achieved wide reach and sustained engagement. Interventions incorporating personalized communication, particularly messages delivered by trusted healthcare providers or grounded in behavioral theory, were associated with notable improvements in screening participation and follow-up rates. Culturally and spiritually tailored educational messages effectively improved knowledge, attitudes, and perceived social norms; however, improved awareness alone did not always translate to higher screening uptake, as financial constraints and limited access to services remained significant barriers. Comprehensive telehealth applications combining education, result notification, follow-up guidance, and reminders demonstrated broader benefits including improved preventive behaviors. Notably, interventions blending face-to-face education with continued digital support consistently yielded the highest screening uptake, highlighting the value of multimodal approaches.26–28,30,31,33
Virtual Education-Based Telehealth
One study examined the effect of online education based on the Health Belief Model (HBM) on cervical cancer screening behaviors among middle-aged women.32 The intervention was delivered through a virtual platform over a three-week period and consisted of interactive sessions addressing key HBM components, including cervical cancer susceptibility, severity, perceived benefits and barriers to Pap smears, and self-efficacy for preventive action. Educational methods included interactive lectures, group discussions, infographics, and educational videos, supplemented by reminder messages during a two-month follow-up period. Findings revealed that HBM-based virtual education significantly improved participants’ knowledge, risk perception, perceived benefits, and confidence in undergoing Pap smears, while perceived barriers to screening decreased significantly.
Mobile Screening Service-Based Telehealth
One mixed methods study assessed an integrated mobile screening program designed to expand access to cervical and colorectal cancer screening in rural and remote areas of northern Canada.25 The program involved nurse practitioners delivering Pap tests alongside existing mammography services, supported by community mobilization coordinators who assisted with outreach, appointment scheduling, and coordination with local health workers. Between December 2020 and December 2021, the mobile service reached 36 communities across Northern Alberta, screening a total of 653 participants. Program acceptability was high, with 98% of participants willing to participate again and 100% of health workers expressing support for program continuation, underscoring its relevance for populations with limited access to healthcare facilities.
Discussion
Overall, the included studies suggest that telehealth interventions have promising potential to improve cervical cancer screening participation, particularly when used to support patient education, reminders, navigation, and follow-up. Across intervention types, simpler and more accessible strategies—such as mobile messaging, app-based reminders, and web-based education appeared to show more consistent benefits in screening uptake. In contrast, more complex interventions involving integrated service delivery or mobile screening initiatives demonstrated important feasibility and reach, but their effectiveness appeared to be more dependent on implementation context, infrastructure, and local health system capacity.
The synthesis of the reviewed studies highlights that telehealth interventions have emerged as a promising strategy to improve cervical cancer screening participation across diverse contexts. Although the studies varied in design, population, and delivery mode, a consistent trend suggests that digital health technologies can bridge geographical, social, and informational barriers that have long hindered access to preventive services, particularly among women in low-resource or rural settings.
Web-based platforms have proven effective in enhancing women’s knowledge and attitudes toward health screening. Their success can be attributed to flexible, self-paced learning environments that enable repeated engagement with educational materials, fostering deeper understanding and retention of health information. However, many telehealth initiatives conclude once the research phase ends and fail to be integrated into routine clinical practice. To address these challenges, Murray et al (2012) recommend applying the Medical Research Council (MRC) framework to guide the development, evaluation, and implementation of complex interventions. This framework underscores the importance of a solid theoretical foundation, a clearly defined mechanism of action, alignment between evaluation methods and the proposed mechanisms, and early consideration of implementation strategies throughout the development process.24
Mobile and app-based interventions demonstrated the broadest potential due to their accessibility and scalability. Evidence suggests that short message service (SMS) and mobile applications can effectively deliver educational messages, reminders, and even facilitate self-sampling processes. SMS text messages and telephone calls are the most frequently used telehealth technologies to boost cancer screening participation. These interventions were effective in enhancing participants’ knowledge about screening and were widely accepted.34 However, results were not universally positive—some interventions failed to increase participation despite high message reach, indicating that knowledge alone does not always translate into action. Socioeconomic barriers, logistical challenges, and personal health beliefs remain influential determinants of screening behaviour. Studies such as Poulsen et al (2024) reinforce the importance of culturally adapted and context-sensitive digital designs,35 particularly in low- and middle-income countries25 where access and affordability are central concerns.
Virtual education programs based on behavioural frameworks, such as the Health Belief Model, have proven particularly effective in improving psychological readiness and intention to undergo screening. These interventions enhance knowledge, boost self-efficacy, increase perceived susceptibility, and reduce perceived barriers, key cognitive factors associated with preventive health behaviours, as demonstrated by Khoshnazar et al.32 Furthermore, research by Bhochhibhoya et al (2021) suggests that mHealth interventions are a promising strategy for improving cervical cancer screening uptake among women. To ensure that women attend their next appointment, however, barriers such as transportation costs, inaccessibility, and difficulties with walk-in appointments must be addressed in mobile phone-based interventions, alongside reminders.2 Similarly, Bhardwaj et al (2023) found that text messaging interventions are effective in increasing Pap smear uptake, especially among populations most affected by health disparities.36
Meanwhile, mobile screening service–based telehealth interventions address a more structural gap by bringing healthcare directly to remote communities. The integration of nurse-led outreach and digital coordination mechanisms ensures that screening opportunities reach those least likely to access facility-based care. The findings from northern Canada underscore the value of hybrid telehealth models that combine mobile units with local engagement to deliver equitable screening access. Similar success has been reported in Uganda, where comparable programs have increased service uptake and improved patient experiences.37 According to research by Degife et al (2023), mobile medical clinics have demonstrated their global effectiveness in boosting screening uptake. This model could be adapted locally to improve screening accessibility across various healthcare settings.38
In addition to the promising effects, telehealth offers opportunities for equity-oriented innovations in cervical cancer screening. Given the persistent disparities in screening coverage across socio-economic and geographic lines, digital-enabled strategies can help reach hard-to-access populations, provided that issues of connectivity, cost, language, and trust are addressed. The systematic review of mobile health applications for cervical cancer (eg, in India) emphasized the need for user-centered design, cultural adaptation, and continuous usability evaluation.39
The findings of this review are particularly relevant in the context of Indonesia’s national cervical cancer screening policy. Following a Health Technology Assessment submitted by INASGO in 2021, a Ministerial Decree (KMK) issued in May 2023 established both HPV DNA testing and Visual Inspection with VIA as official national screening methods.40,41 Currently, HPV DNA testing faces implementation challenges, including limited laboratory capacity and quality assurance issue.42 In this context, VIA serves as a faster complementary approach, particularly for triaging women who test positive for HPV. Telehealth offers a strategic opportunity to integrate these two modalities within a coordinated screening pathway. It can support HPV DNA testing through remote result delivery, patient education, follow-up coordination, and referral navigation, while simultaneously enhancing the reach, consistency, and objectivity of VIA through digital decision-support tools and remote supervision. As HPV DNA infrastructure continues to expand, telehealth-enabled self-sampling approaches hold strong potential as a primary screening strategy. Therefore, future telehealth models should adopt an integrated approach that accommodates both HPV DNA testing and VIA, ensuring alignment with national policy and responsiveness to local health system capacity.43
Across the four telehealth intervention categories identified in this review, mobile and app-based strategies demonstrated the most consistent improvements in screening participation, particularly SMS-based reminders delivered in low-resource settings across sub-Saharan Africa and South Asia. Interventions incorporating personalized or culturally tailored messaging, as well as those grounded in behavioral theories such as the Health Belief Model or Social Cognitive Theory, were associated with stronger and more sustained effects on both knowledge and screening uptake. Virtual education programs showed the strongest impact on psychological readiness, including self-efficacy, perceived susceptibility, and reduction of perceived barriers, though their translation into actual screening behavior varied across contexts. Web-based interventions were effective in enhancing knowledge and attitudes, particularly among populations with adequate digital literacy, but their direct impact on screening uptake was less consistent. Mobile screening services, while demonstrating high acceptability and reach, were more dependent on implementation context, infrastructure, and community engagement. Overall, the evidence suggests that no single telehealth modality is universally superior; rather, multimodal approaches combining digital education, reminders, and direct service delivery consistently yielded the highest screening participation rates.
Limitations and Future Directions
While the reviewed studies are encouraging, limitations remain: many were short-term, used self-reported outcomes, varied in design and quality, and lacked long-term follow-up or clinical endpoints. Future research should focus on: 1) longitudinal and large-scale effectiveness trials that evaluate the actual screening uptake, follow-up compliance, and clinical outcomes; 2) Future studies should also conduct cost-effectiveness analyses in various settings, with a particular emphasis on low- and middle-income countries (LMICs); and 3) Implementation science studies evaluating integration with health systems, sustainability, digital literacy, and equity impacts.
This review also has methodological limitations that should be acknowledged. The search was conducted across four databases and was restricted to peer-reviewed studies published in English, which may have resulted in the omission of relevant studies published in other languages or disseminated through non-indexed channels, particularly from low- and middle-income countries. Additionally, this review is subject to potential publication bias, as studies reporting statistically significant or positive findings are more likely to be published than those with null or negative results, which may lead to an overestimation of telehealth effectiveness in the synthesized evidence.
Conclusion
In conclusion, telehealth represents a strategic innovation with significant potential to improve cervical cancer screening participation. This review identified four main categories of interventions—web-based platforms, mobile and app-based strategies, virtual education programs, and mobile screening services—each addressing distinct informational, behavioral, and access-related barriers. To achieve sustainable impact, telehealth interventions must go beyond information delivery and be theory-informed, context-sensitive, culturally tailored, and integrated with service delivery within health systems. Such an approach is essential to effectively close screening gaps and advance women’s health outcomes globally.
Data Sharing Statement
The corresponding author can provide the datasets created and/or examined during the current investigation upon reasonable request.
Acknowledgments
We would like to express our gratitude to Universitas Padjadjaran and the Indonesian Endowment Fund for Education (LPDP). This publication charge is funded by Universitas Padjadjaran through LPDP on behalf of the Indonesian Ministry of Higher Education, Science and Technology, and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this study.
References
1. World Health Organization. Global cervical cancer elimination forum 2025. 2025. Available from: https://www.who.int/cancer/prevention/diagnosis-screening/cervical-cancer/en/.
2. Bhochhibhoya S, Dobbs PD, Maness SB. Interventions using mHealth strategies to improve screening rates of cervical cancer: a scoping review. Prev Med. 2021;143:106387. doi:10.1016/j.ypmed.2020.106387
3. World Health Organization. Human Papillomavirus (HPV) and cervical cancer. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/humanpapillomavirus-hpv-and-cervical-cancer.
4. International Agency for Research on Cancer (IARC). Cervical Cancer Awareness Month 2021: Questions and Answers (Q&A). 2022. Available from: https://www.iarc.who.int/faq/cervical-cancer-awareness-month-2021-qa/.
5. World Health Organization. Cervical cancer. 2025. Available from: https://www.who.int/cancer/prevention/diagnosis-screening/cervical-cancer/en/.
6. Das M. WHO launches strategy to accelerate elimination of cervical cancer. Lancet Oncol. 2021;22(1):20–12. doi:10.1016/S1470-2045(20)30729-4
7. Salmani H, Ahmadi M, Shahrokhi N. The impact of mobile health on cancer screening: a systematic review. Cancer Inform. 2020;19:1176935120954191. doi:10.1177/1176935120954191
8. Liu X, Ning L, Fan W, Jia C, Ge L. Electronic health interventions and cervical cancer screening: systematic review and meta-analysis. J Med Internet Res. 2024;26:e58066. doi:10.2196/58066
9. Chen THH, Yen AMF, Fann JCY, et al. Clarifying the debate on population-based screening for breast cancer with mammography. Medicine. 2017;96(3):e5684. doi:10.1097/MD.0000000000005684
10. Tokosi TO, Fortuin J, Douglas TS. The impact of mhealth interventions on breast cancer awareness and screening: systematic review protocol. JMIR Res Protoc. 2017;6(12):e246. doi:10.2196/resprot.8043
11. Bedell SL, Goldstein LS, Goldstein AR, Goldstein AT. Cervical cancer screening: past, present, and future. Sex Med Rev. 2020;8(1):28–37. doi:10.1016/j.sxmr.2019.09.005
12. HealthIT.gov. Office of the national coordinator for health information technology. Available from: https://www.healthit.gov/faq/what-telehealth-how-telehealth-different-telemedicine.
13. Shaffer KM, Turner KL, Siwik C, et al. Digital health and telehealth in cancer care: a scoping review of reviews. Lancet Digit Health. 2023;5(5):e316–e327. doi:10.1016/S2589-7500(23)00049-3
14. Rittberg R, Mann A, Desautels D, Earle CC, Navaratnam S, Pitz M. Canadian cancer centre response to COVID-19 pandemic: a national and provincial response. Current Oncol. 2020;28(1):233–251. doi:10.3390/curroncol28010026
15. Vargas-Cardona HD, Rodriguez-Lopez M, Arrivillaga M, et al. Artificial intelligence for cervical cancer screening: scoping review, 2009–2022. Int J Gynecol Obstet. 2024;165(2):566–578. doi:10.1002/ijgo.15179
16. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
17. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
18. Barker TH, Stone JC, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid Synth. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430
19. Barker TH, Habibi N, Aromataris E, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for quasi-experimental studies. JBI Evid Synth. 2024;22(3):378–388. doi:10.11124/JBIES-23-00268
20. Hong QN, Pluye P, Fàbregues S, et al. Mixed methods appraisal tool (MMAT). 2018.
21. Fitch K, Bohn JA, Emerson JB, Boniface ER, Bruegl A. Acceptability of human papillomavirus self-collection and the role of telehealth: a prospective, randomized study stratified by menopausal status. Int J Gynecol Cancer. 2023;34(1):19–27. doi:10.1136/ijgc-2023-004935
22. Huf S, Kerrison RS, King D, et al. Behavioral economics informed message content in text message reminders to improve cervical screening participation: two pragmatic randomized controlled trials. Prev Med. 2020;139:106170. doi:10.1016/j.ypmed.2020.106170
23. Le D, Holt CL. CervixCheck: a spiritually-based text messaging intervention to promote cervical cancer awareness and pap test screening intention among African-American women. J Health Commun. 2018;23(9):842–853. doi:10.1080/10810730.2018.1528317
24. Asirwa FC, Bresnahan BW, Yego F, Duncan D, Karichu JK, Garrison LP. A prospective model of the potential clinical and economic impact of cervical cancer screening supported by a mobile phone app. PLoS One. 2025;20(1 January):e0316001. doi:10.1371/journal.pone.0316001
25. Wiseman J, Patterson K, Kliewer G, et al. Integrated access to cancer screening: expanding access for cervical and colorectal cancer screening in rural and remote Northern Alberta, Canada using a mobile service to bring cancer screening closer to home. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-12392-7
26. Hombaiah C, Madhu B, Gopi A, Murthy MRN. Effects of mobile Health (mHealth) application on cervical cancer prevention knowledge and screening among women social support groups with low-socioeconomic status in Mysuru city, Southern India. PLoS One. 2022;17(9 September):e0273070. doi:10.1371/journal.pone.0273070
27. Addo-Lartey AA, Bonful HA, Sefenu RS, et al. Effectiveness of a culturally tailored text messaging program for promoting cervical cancer screening in Accra, Ghana: a quasi-experimental trial. BMC Womens Health. 2024;24(1). doi:10.1186/s12905-023-02867-2
28. Linde DS, Andersen MS, Mwaiselage J, Manongi R, Kjaer SK, Rasch V. Effectiveness of one-way text messaging on attendance to follow-up cervical cancer screening among human papillomavirus-positive Tanzanian women (Connected2Care): parallel-group randomized controlled trial. J Med Internet Res. 2020;22(4):e15863. doi:10.2196/15863
29. Hamdiui N, Stein ML, van Steenbergen J, et al. Evaluation of a web-based culturally sensitive educational video to facilitate informed cervical cancer screening decisions among Turkish- and Moroccan-Dutch women aged 30 to 60 years: randomized intervention study. J Med Internet Res. 2022;24(10):e35962. doi:10.2196/35962
30. Huchko MJ, Saduma I, Blat C, Oketch S, Bukusi EA. How providing cervical cancer screening results via cell phone affects patient follow-up rates in Western Kenya. J Glob Oncol. 2019;5:1–8. doi:10.1200/JGO.18.00264
31. Okunade KS, Soibi-Harry A, John-Olabode S, et al. Cancer prevention and control original reports impact of mobile technologies on cervical cancer screening practices in Lagos, Nigeria (mHealth-Cervix): a randomized controlled trial. JCO Global Oncol. 2021;7(7):1418–1425. doi:10.1200/GO.21
32. Khoshnazar MS, Tarrahi MJ, Shahnazi H. Impact of virtual education based on health belief model on cervical cancer screening behavior in middle-aged women: a quasi-experimental study. Cancer Rep. 2024;7(4):e2058. doi:10.1002/cnr2.2058
33. Mohammad Z, Ahmad N, Baharom A. The effects of theory-based educational intervention and whatsapp follow-up on papanicolaou smear uptake among postnatal women in Malaysia: randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(6):e32089. doi:10.2196/32089
34. Schliemann D, Tan MM, Hoe WMK, et al. mHealth interventions to improve cancer screening and early detection: scoping review of reviews. J Med Internet Res. 2022;24(8):e36316. doi:10.2196/36316
35. Poulsen A, Hickie IB, Alam M, et al. Overcoming barriers to mHealth co-design in low- and middle-income countries: a research toolkit. Inf Technol Dev. 2024;30(3):542–561. doi:10.1080/02681102.2023.2295480
36. Bhardwaj N, Herndon AT, Kuo YF, Porterfield LR. Text messaging intervention for Pap smear uptake: a single-institution study. Mhealth. 2023;9:34. doi:10.21037/mhealth-23-11
37. Kabukye JK, Namugga J, Mpamani CJ, et al. Implementing smartphone-based telemedicine for cervical cancer screening in Uganda: qualitative study of stakeholders’ perceptions. J Med Internet Res. 2023;25:e45132. doi:10.2196/45132
38. Degife EA, Oliveira CR, Znamierowski E, Meyer JP, Sheth SS. Uptake of cervical cancer screening among female patients using a mobile medical clinic. Am J Prev Med. 2023;65(5):835–843. doi:10.1016/j.amepre.2023.05.013
39. Purohit R, Singh S, Vaishampayan D, Sane Y, Pande J, Devi S. A systematic review of cervical cancer mobile applications and a future directions for developers. Asian Pac J Cancer Prev. 2024;25(10):3429–3437. doi:10.31557/APJCP.2024.25.10.3429
40. Ministry of Health of The Republic of Indonesia. Implementation of a pilot program for early detection of cervical cancer with HPV DNA testing and visual inspection with acetic acid (Co-Testing). Ministry of Health of The Republic of Indonesia; 2023.
41. Utami TW, Nuranna L, Rahman SA, et al. A decade data of HPV genotypes in metropolitan regions of Indonesia: paving the way for a national cervical cancer elimination strategy. J Gynecol Oncol. 2025;36(6). doi:10.3802/jgo.2025.36.e85
42. Aurora WID, Dwiza M. HPV DNA testing in cervical cancer screening: challenges, opportunities, and future directions. Scientific Environm Health Dis. 2024;4(1):42–53. https://online-journal.unja.ac.id/e-sehad/article/view/41351. Accessed May 18, 2026.
43. Ekawati FM, Listiani P, Idaiani S, Thobari JA, Hafidz F. Cervical cancer screening program in Indonesia: is it time for HPV-DNA tests? Results of a qualitative study exploring the stakeholders’ perspectives. BMC Womens Health. 2024;24(1):125. doi:10.1186/s12905-024-02946-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Barriers and Motivators to Cervical Cancer Screening in Rwanda: A Qualitative Study
Gafaranga JP, Manirakiza F, Ndagijimana E, Urimubabo JC, Karenzi ID, Muhawenayo E, Gashugi PM, Nyirasebura D, Rugwizangoga B
International Journal of Women's Health 2022, 14:1191-1200
Published Date: 1 September 2022
Economic Evaluations of HPV Vaccination in Targeted Regions of Low- and Middle-Income Countries: A Systematic Review of Modelling Studies
Frianto D, Setiawan D, Diantini A, Suwantika AA
International Journal of Women's Health 2022, 14:1315-1322
Published Date: 12 September 2022
Pre COVID-19 Pandemic Use of Telemedicine for Adherence Promotion in Patients with Psychotic Disorders: A Literature Review
Edwards AM, Petitt JC, Kumar S, Levin JB, Sajatovic M
Patient Preference and Adherence 2022, 16:2559-2565
Published Date: 14 September 2022
Socio-Demographic Factors and Other Predictors of Pap Test Uptake Among Women: A Retrospective Study in Ghana
Mensah KB, Boamah Mensah AB, Yamoah P, Manfo J, Amo R, Wiafe E, Padayachee N, Bangalee V
Cancer Management and Research 2023, 15:489-499
Published Date: 12 June 2023
Healthcare Providers’ Experience with Saudi Arabia’s 937 Virtual Medical Call Centers and Telehealth
Al-Wathinani AM, Dhafar YO, Aljarallah SA, Alqahtani MS, Alamri FA, Aljohani AO, Alanazi MD, Arbaein TJ, Zaidan AM, Aljuaid M, Goniewicz K
Journal of Multidisciplinary Healthcare 2024, 17:2949-2960
Published Date: 22 June 2024