Back to Journals » International Journal of Women's Health » Volume 14
Knowledge, Barriers and Motivators to Cervical Cancer Screening in Rwanda: A Qualitative Study
Authors Gafaranga JP ![]() , Manirakiza F
, Manirakiza F ![]() , Ndagijimana E, Urimubabo JC, Karenzi ID, Muhawenayo E, Gashugi PM, Nyirasebura D, Rugwizangoga B
, Ndagijimana E, Urimubabo JC, Karenzi ID, Muhawenayo E, Gashugi PM, Nyirasebura D, Rugwizangoga B ![]()
Received 17 May 2022
Accepted for publication 25 August 2022
Published 1 September 2022 Volume 2022:14 Pages 1191—1200
DOI https://doi.org/10.2147/IJWH.S374487
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Jean Pierre Gafaranga,1,2 Felix Manirakiza,3,4 Emmanuel Ndagijimana,5 Jean Christian Urimubabo,6 Irénée David Karenzi,7 Esperance Muhawenayo,6 Phophina Muhimpundu Gashugi,8 Dancilla Nyirasebura,6 Belson Rugwizangoga3,4
1Department of Psychiatry, School of Medicine and Pharmacy, University of Rwanda, Kigali, Rwanda; 2Department of Psychiatry, University Teaching Hospital of Kigali, Kigali, Rwanda; 3Department of Clinical Biology, School of Medicine and Pharmacy, University of Rwanda, Kigali, Rwanda; 4Department of Pathology, University Teaching Hospital of Kigali, Kigali, Rwanda; 5Department of Epidemiology and Biostatistics, School of Public Health, University of Rwanda, Kigali, Rwanda; 6Department of Surgery, University Teaching Hospital of Kigali, Kigali, Rwanda; 7Department of Surgery, Ruhengeri Referral Hospital, Musanze, Rwanda; 8Department of Physical Rehabilitation, University Teaching Hospital of Kigali, Kigali, Rwanda
Correspondence: Jean Pierre Gafaranga, Department of Psychiatry, University of Rwanda, Kigali, Rwanda, Department of Psychiatry, University Teaching Hospital of Kigali, Kigali, Rwanda, Tel +250788224864, Email [email protected]; [email protected]
Background: Cervical cancer is a global public health problem with marked geographical disparity. High morbidity and mortality rates in developing countries are associated with low screening rates. In 2020, in Rwanda, 3.7 million women aged 15– 59 years were at risk of developing cervical cancer, the most commonly diagnosed female cancer in Rwanda. Despite Rwanda being the first African country to vaccinate against human papilloma virus with a three-dose regimen vaccination coverage of nearly 93% in the target population of girls aged < 15 years, and having established cervical cancer screening program, recent studies have found low screening rates. Our study sought to determine knowledge, motivators and barriers of cervical cancer screening.
Methods: We conducted a qualitative descriptive study; using focus group interview in an urban health facility (Muhima district hospital) and a rural health center (Nyagasambu health center) offering cervical screening services in Rwanda. Participants were women seeking these services and other women attending the health facility for any reason, and female staff working in these facilities. Interviews were recorded and transcribed, and data were analyzed using content analysis.
Results: Thirty women participated in focus group interview, with an average age of 39 years. Many of women showed knowledge about cervical cancer existence and prevention methods. However, fear for pain, lack of knowledge about screening, how and where the screening was done, and concern for privacy were recurring subthemes. Some participants also mentioned lack of health insurance as a barrier for cervical cancer screening.
Conclusion: Barriers to uptake cervical cancer screening services in Rwanda are related to poor information about cervical cancer and the importance of screening as well as non-adherence to medical insurance. Population sensitization through campaign and community outreach activities could have a positive impact on increasing the usage of cervical cancer screening in Rwanda.
Keywords: cervical cancer, screening, fear for pain, qualitative, acceptance, Rwanda
Background
Cancer incidence, morbidity and mortality is still a major global public health challenge.1–3 Particularly, cervical cancer is a deadly disease, the fourth most common cancer in women worldwide with more than 604,127 new cases and 341,831 deaths in 2020.1 Arbyn et al reported that cervical cancer is among the top three cancers affecting women <45-year-old in 79% of 185 countries.4 Furthermore, according to GLOBOCAN 2020, cervical cancer is the most commonly diagnosed cancer in 23 countries and the leading cause of cancer-related deaths in 36 countries.1
The disparity in cervical cancer incidence and mortality between developed and low- and middle-income countries (LMICs) is highlighted by noting that 70% to 90% of cervical cancer cases and deaths occur in LMICs.1,4,5 Although considered a deadly disease, cervical cancer is one of the most easily managed forms of female cancers through screening, early detection and treatment.1,6,7 However, screening rates are low in LMICs, especially in sub-Saharan Africa, compared to developed countries.8 East African countries, where the Rwanda is located, have a high number of cervical cancer cases and deaths.4,9–11 In addition, the majority of women at risk for cervical cancer disease who reside in rural communities in LMICs may not have access to cervical cancer prevention programmes;11 thus, only 0.4–14% of rural women are screened, compared to >20% of their urban counterparts.12
In Rwanda, 3.7 million women aged 15–59 years, representing approximately 30% of the total population in 2020,13 were at risk of developing cervical cancer.9 This is the most commonly diagnosed female cancer in Rwanda,14,15 with a high incidence rate of 42 cases per 100,000 women per year.15 A national program for cervical cancer prevention exists and the country has been the first African country to initiate a nationwide program to prevent cervical cancer through vaccination against Human papillomavirus (HPV).15 The program started in 2011 when girls in primary school grade six (approximately 12 years old) were vaccinated with quadrivalent (HPV16/18/6/11) HPV vaccine.15 The three-dose vaccination coverage was estimated at 93% of the target population.16
Furthermore, Rwanda has introduced low-cost methods for cervical cancer screening including visual inspection of cervix with acetic acid (VIA) and HPV-DNA test for women aged ≥35 years with a repeat screening at 7 years for those with a negative result.14 Women with positive results are followed by colposcopy and biopsy.10
Unfortunately, cervical cancer screening rate are still low among Rwandan women. The reasons are not known.14 Different studies about cervical cancer screening in Rwanda reported a participation rate ranging from 2.6% to 28.3%.15,17–19 For example, Mukanyangezi et al19 reported that only 7% in HIV-negative women and 27% in HIV-positive women have ever participated in cervical cancer screening. The aim of this study was to elucidate knowledge, barriers and motivators that may affect Rwandan women in using cervical cancer screening services, in order to improve the overall utilization of this program and thus contribute to the prevention of cervical cancer.
Methods
Study Design and Settings
We used a qualitative descriptive study20 approach to elucidate knowledge about cervical cancer, and identify barriers and motivators for Rwandan women to use cervical cancer screening services.
The study was conducted in one urban (Muhima district hospital) and one rural health facility (Nyagasambu health center) which provided cervical cancer screening. It involved women aged 30 to 59 years. These sites were selected among urban and rural health facilities providing cervical screening services.
Muhima district hospital is located in Kigali city, the capital city of Rwanda. As a hospital serving women and children in an urban area, the hospital is committed to improve the health outcomes of women, children and families from its catchment area, including providing cervical cancer screening services. On the other hand, Nyagasambu health center is a primary health facility located in Rwamagana district, Eastern province of Rwanda. The center provides high-quality primary health care services including maternal healthcare. Its services are used by ordinary citizens with a rural life style. The participants were recruited from the women who came to these sites for cervical cancer screening and for work-related activities, and women who accompanied patients to the sites.
Study Participants
We did interview in five focus groups for a total of 30 women (14 urban and 16 rural). Group one (n=7, urban), group two (n=7, urban), group three (n= 5, rural), group four (n=5, rural) and group five (n=6, rural). Hennink et al21 stated that the combination of different parameters influencing data saturation has to be used to determine the number of focus groups. As the purpose of the study was to identify core issues, with simple codes, themes saturation, 90% as the degree of saturation, and absence of stratification; Given that each of the parameters requires 4 to 6 focus groups, we estimated 5 focus groups as the sample size of the study.
Study Procedure
In focus group interview, we used a semi-structured interview guide22 with 9 open ended questions with possibility of probing as needed (Supplementary Material S1) and conducted face-to-face interview with recording of voices. The choice for focus group interview was based on the fact that most of existing qualitative research related to cervical cancer screening in Rwanda have used structured questionnaires or questions with yes/no answers18,23,24 therefore, to be able to collect in depth subjective opinions22,25 from primordial potential beneficiary of cervical screening we opted for focus group interview. One team of facilitators conducted interview for all five focus groups. The team was composed by experienced healthcare personnel including 2 female nurses and one male medical doctor.
Data Analysis
The language used in focus group interview was Kinyarwanda which was the mother tongue of the participants. The recorded sessions were translated into English language, transcribed and verified for fidelity to the recording with two different investigators. In case of a difference in translation, these investigators made a consensus on the final translation with assistance of principal investigator. As our study design was a qualitative descriptive study, we adopted content analysis method (firstly quantitative content approach followed by manifest qualitative content approach).26 We preferred content analysis as the approach that use a lower level of interpretation of data to be able to try to convey the message as was transmitted by the participants.26,27 The data were hand coded and we identified recurrent themes.
During data analysis we followed the six steps described by Creswell:28
Step 1: Data organization and preparation for analysis, during this step the audio recordings from interviews were transcribed into word document transcripts then translated into English.
Step 2: Reading through the data. Three investigators compiled the overall meaning to gain the general sense of the information and ideas that the participants provided.
Step 3: Start the coding process: To achieve this, sentences with similar meaning were colored with one marker and annotated using # number and rural or urban were added to each sentence to be able to know from which participant is coming from.
Step 4: Use the coding process to generate a description of the setting or people as well as categories or themes for analysis. At this step we grouped similar subthemes under a one theme.
Step 5: Advance how the description and themes will be represented in the qualitative narrative. We decided to use narrative passage to be able to transmit the point view/feelings from our respondents. Each narrative was annotated by the assigned # number of the respondent, her living area (rural or urban) and her age.
Step 6: The final step consisted in interpreting our results by comparing our findings to the currently available data about cervical cancer screening and other healthcare related issues.
The findings of this study were reported according to the standards for reporting qualitative research (SRQR) recommendations.29 The final report was reanalyzed, verified and validated by all researchers.
Ethical Consideration
Our study was approved by the institutional review board (IRB) of the University of Rwanda College of Medicine and Health Sciences (IRB Notice No 524/CMHS IRB/2019).
Results
Participant Characteristics
Thirty women (14 urban and 16 rural) participated in the interview. Fifteen were at the site of interview specifically for cervical cancer screening, while the others came for other reasons (2 working in the cleaning company, 2 women working as accountant, 6 women were accompanying their patients, 5 were there for other health reasons). The mean age was 39 years.
Knowledge About Cervical Cancer and Motivators/Barriers for Attending Screening Services
Qualitative data were classified into 3 different themes: knowledge about cervical cancer, barriers to the use or adoption of screening services and motivation to use screening services. Each theme had subthemes as summarized in Table 1.
 |
Table 1 Study Themes |
For 30 women who participated into focus group interview, 25 women (83%) have some knowledge or are aware of cervical cancer, 5 women (17%) do not know cervical cancer. Any knowledge for the prevention of cervical was expressed by 17 women (57%). However, the majority of the interviewed women (77%, 23/30) have some knowledge of or have heard how cervical cancer is screened (Table 2)
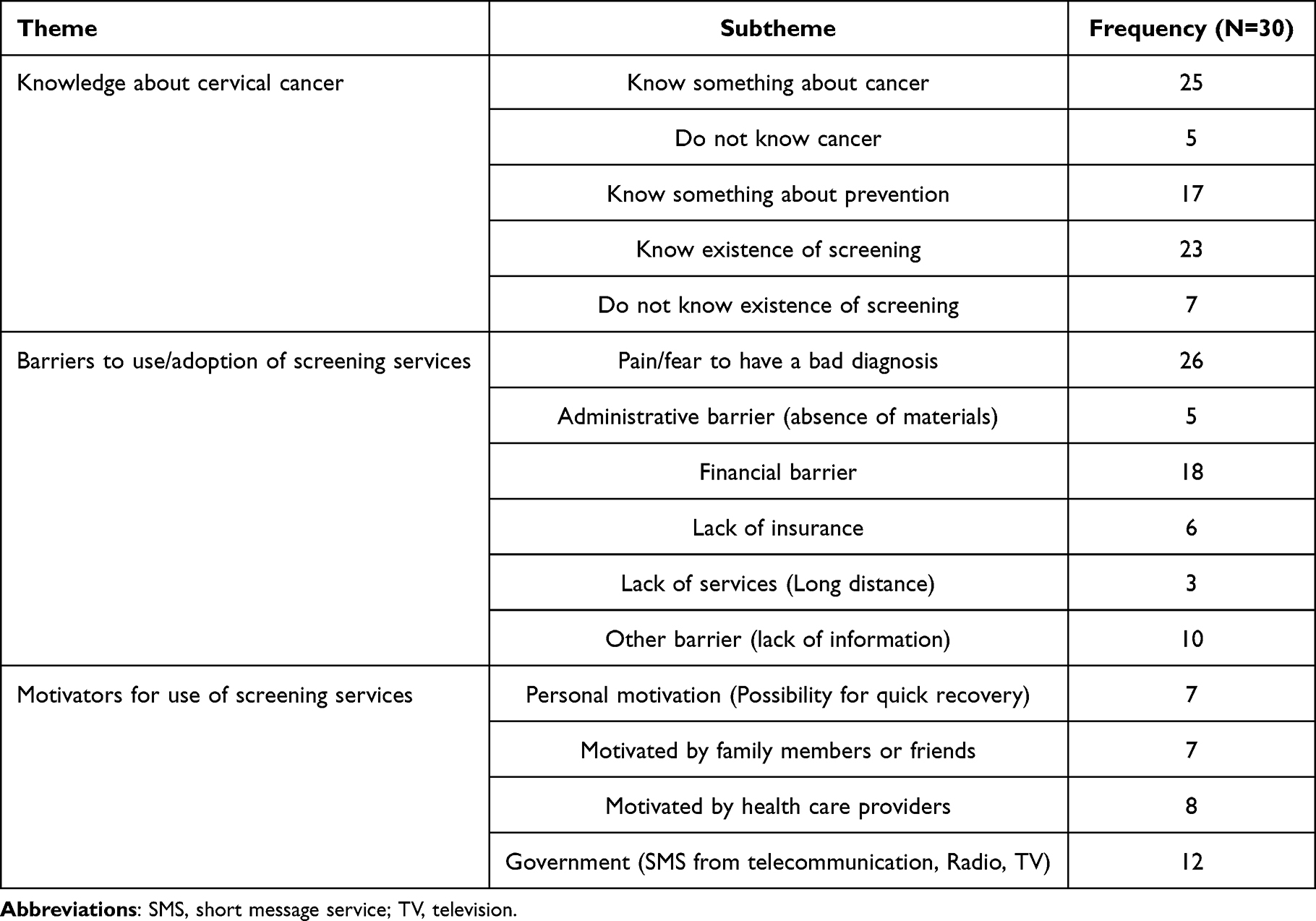 |
Table 2 Characteristics of Findings According to Themes and Sub-Theme |
Knowledge About Cervical Cancer
Existence of Cervical Cancer
Existence of cervical cancer was reported in all focus groups. Women showed awareness of risk factors, symptoms and treatment options by the following expressions:
Cervical cancer can mostly affect women in childbearing age…., or those who start having sex at an earlier age, among symptoms Iknow that someone may have persistent menses [#4, urban, age 45]
Cervical cancer may be caused by becoming pregnant at an earlier age or by having too many babies, [#1, urban, age 36]
My friend had cervical cancer and told me that it is the most painful disease. [#12, urban, age 33]
Examples of lack of knowledge about cervical cancer were expressed in statements such as:
I did not know that cervical cancer is related to having sexual intercourse,… Iwas thinking that it could be adisease like the most common disease. [#2, urban, age 40]
Lack of knowledge can also be detected in such questions as:
Does cervical cancer have signs/symptoms that we can recognize and go for screening? [#29, rural, age 37]
Knowledge About Cervical Cancer Prevention and Screening
Some women exhibited some knowledge related to cervical cancer screening (23/30) or how cervical cancer could be prevented (17/30). They gave examples including the use of HPV vaccines, use of condoms and limitation of number of sex partners
You can do prevention by not involving in prostitution, or by going for consultation as earlier as possible [#21, rural, age 46]
You can use condoms when having sexual intercourse, [#7, urban, age 34]
Yet, some women also expressed lack of important information as in the following example:
I knew, through radio and television broadcast, that screening for cervical cancer is being done but I did not know where to go for screening. [#9, urban, age 39]
Barriers to Cervical Cancer Screening
As for barriers to the use or adoption of screening services, the major barriers found are the fear for pain or fear to have a cancer as diagnosis (26 women) and financial barriers (18 women). The majority think that the screening is too painful and it involves exposing private parts of a lady. Then, especially for girls (not yet married female) they choose to secure their privacy. These barriers come out as:
Fear for Pain Related to the Procedure
I thought about going to screening many times, but I always had fear of pain, … even in past time I went to screening area where campaign for cervical cancer screening were being done but because of fear of pain I did not yet participate in screening [#13, urban, age 40]
I always had fear of pain even though today I came for screening, I come with reluctance because of fear for pain [#6, urban, age 38]
I thought about going for screening but once I heard that it is painful, I decided not to go [#19, rural, age 36]
I know nothing about cervical cancer screening but those who went for it told me that the procedure is painful. [#2, urban, age 40]
Concerning fear for the pain two women suggested that:
I can suggest the use of anesthesia during screening because the procedure is painful, even though I do not know if it is possible to use anesthesia [#10, urban, age 39]
I am afraid that the procedure is painful and I am asking myself if there are no other way of screening for cervical cancer, for example by using imaging tool or ultrasound [#17 rural, age 46]
Privacy Concerns, Especially Discomfort with Exposure of Private Parts During the Procedure
Let’s consider a not yet married female (a girl) with no prior experience of giving childbirth, she is very concerned with her privacy, she may have shyness, … There is no other way of doing screening without exposing private part of body? [#26, rural, age 58]
Another woman asked about alternative procedures that would not require exposure.
Can you use other technics for screening like ultrasound or by testing through blood? [#6, urban, age 38]
Financial Issues Which Prevented Them from Screening, Such as the Lack of Health Insurance, Unaffordable Consultation Fees and Other Medical Expenses
I had a desire for screening but because of lack of health insurance, I waited until I got it [#11, urban, age 41]
Other Barriers
Other barriers include long distance from the testing site, lack of services nearby, inadequate information about the location of screening services, and other administrative problems such as not having enough testing materials and confusion about screening eligibility
When I reached at the screening service, they told me that the screening tools were not available and they advised me to come back at another time [#23, rural, age 35]
I had a desire for cervical cancer screening for a long time but I could not know where I can get screening services [#9, urban, age 39]
I came for cervical cancer screening in past time but nurses told me that they can not do screening for me because I was less than 30 years old. Now as I have reached 30 years, I am back at health center and am happy that now they will do a screening for me![#22, rural, age 30]
Another woman was afraid that she might be too old because she was 59 years old, but was reassured by the nurse that she was eligible to be screened.
None of women expressed religious belief or familial reasons as barriers for attending cancer screening services. However, one female insisted that she would not attend cervical cancer screening because she was a widow:
Because I do not have a husband … and as are the males who bring the cancer to the females … and I had my own way I do prevention (abstinence?) myself [The Kinyarwanda -The national language- word used by the women may have both meaning prevention or abstinence], therefore I think that there is no reason that I have to go for screening, but in case I have signs/symptoms I will go for consultation. [#30, rural, age 46]
Motivators for Use of Cervical Cancer Screening Services
Government and Healthcare Providers’ Role
The current study found that the main motivator cited for using screening services was from government promotion through different channels including mobile phones, radios and television broadcasts, and local leaders. Individual health care providers also helped.
Even today I received an SMS (short message service) advertising for cervical cancer screening [24, rural, age 42]
When we come for antenatal care or for health of our children, nurses sensitize us about cervical cancer screening, [#7, urban, age 34]
Friends and Family Members or Familial History of Cancer
Women whose family members or relatives or friends had previously been screened for cervical cancer or had a history of cancer were motivated to seek screening services.
I come because I had my grand sister who had cervical cancer [# 25, rural, age 42]
My friend had many times advised me to go for cervical cancer screening. [#10, urban, age 39]
My daughter has cervical cancer, before she did not know that it was cancer and she was seriously ill weighing like 20 kg but after we consult different hospitals, she received treatment and she is doing well with about more than 50 kg, she is now healthy. [# 26., rural, age 58]
After my mother died of cervical cancer, I thought about cervical cancer screening but I did not yet come because I did not have insurance. [#18, rural, age 36]
Personal Reason: Early Treatment and Quick Recovery
A few women reported that they took the decision to go for cervical cancer screening on their own without any external motivators. They thought that they were increasing the recovery chances if results were positive.
When you go for screening if you are diseased, they will treat you as earlier as possible and you will be cured. And if they find that you do not have cancer, they will teach you more about how to do prevention [# 5, urban, age 46]
Discussion
In this qualitative study, most women in the focus groups had some knowledge about cervical cancer and the screening methods used. Prior studies done in different part of Rwanda, although they used different study design to ours, they have reported varying degree of knowledge related to cervical cancer existence, its prevention and screening methods.17,18,23 However, none of them has reported health promotion efforts such as the use of SMS, radio station broadcasts, and other telecommunication tools, as possible motivators or sources of information and knowledge related to cervical cancer screening.
Fear for pain or to be worried about pain and having cancer as a diagnosis, concern about lack of privacy and financial costs were major barriers cited for not coming forward for cervical cancer screening. Fear of pain, which can also be coupled with shyness or uncertainty for privacy has been previously reported in our country and in other African countries, especially Tanzania which is a neighbouring country of Rwanda.30,31 Niyonsenga et al18 in a study done in selected urban hospital of Kigali, Rwanda, reported the barriers for screening to be feeling pain during screening (15.8%), embarrassing to go for screening (34.7) and to feel worry (54.2%). As there is increasing evidence of the effectiveness and acceptability of self-sampling in cervical cancer screening and diagnostic testing of diseases of female genital tract30,32 this might be a remedy for both the concern of lack of privacy, embarrassment and pain as barriers for attending cervical cancer screening.
The inability to cover the expenses of cervical cancer screening in rural African settings, was reported as a major finding in the systematic literature review by Rahman et al.31 In our study, participants reported that health insurances did not cover some of the costs related to screening services. Other women noted that they waited until they had health insurance before attendance at screening services. Barrier related to health insurance was previously reported in Rwanda by Niyonsenga et al18 where 54% of women agreed that lack of health insurance was a barrier for uptake of screening. In the same study,18 16.6% of participant agreed that there is much money needed for treatment although we can not be sure if they were referring to treatment of cancer or referring to screening cost as the item was described under barrier to cervical cancer screening.
While someone may expect familial and religious reasons to be among barriers,31 in our study none of the women raised these. Long distance as a barrier has been reported by other authors;31 hence, community outreach and/or use of community health workers may be needed to address this problem. We suggest involving community health workers because they are playing a considerable role in healthcare system in Rwanda33 and have been used in different roles for cervical cancer screening elsewhere.34
Community outreach activities were mentioned by some women as the source of information about cervical cancer as one way of increasing coverage for cancer screening. We therefore think that community outreach aiming at sensitization, teaching and screening for cervical cancer should be considered as a remedy for both long distance, lack of information and procrastination. Additionally, community outreach has been found to increase the cervical cancer screening rate in the United States of America.35,36
Limitation
Our study has some limitations, which further research may be able to address. First of all, the majority of our respondents came from the ones who had access to health services. We did not go out to women in the community in either urban or rural settings. Future research might involve the women who are using herbal medicine or religious approach to keep themselves safe. In addition, poverty is well known to interfere with healthcare seeking behaviour37–39 and we only interviewed women who had come to a health center.
Conclusion
This study has found fear for pain or for a diagnosis of cancer, privacy concerns and health insurance limitation as major barriers for not coming for cervical cancer screening. Additionally, lack of information and misinformation may be contributing to low rate of participation in this program. On the other hand, the use of government sensitization campaigns, health workers recommending and community outreach activities could have a positive impact on increasing the uptake of cervical cancer screening.
Abbreviations
CMHS, College of medicine and health sciences; DNA, Deoxyribonucleic acid; HPV, Human papillomavirus; IRB, Institutional review board; LMICs, Low- and middle-income countries; SMS, Short message service; SRQR, Standards for reporting qualitative research recommendations; TV, Television; VIA, Visual inspection of cervix with acetic acid; WHO, World health organization.
Data Sharing Statement
The audio data that support the findings of this study are not publicly available due to the fact that they contain information that could compromise research participants’ privacy/consent. The transcribed and translated data are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Our study was approved by the institutional review board (IRB) of the University of Rwanda College of Medicine and Health Sciences (IRB Notice No 524/CMHS IRB/2019). All participants were informed about the purpose of the study and publication of anonymized responses and they signed an informed consent form before participation in the study. The study was conducted in accordance to Rwandan national regulations and Helsinki declaration.
Acknowledgments
We acknowledge Micro Research Project/Dalhousie University, IWK Health Centre, 5850/5980 University Ave, Halifax, Nova Scotia, B3K 6R8, Canada. MicroResearch International (www.microresearch.ca) for providing mentorship in the development and writing up of the findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study has received a grant (MR 18N RWA 02) from Micro Research Project/Dalhousie University, IWK Health Centre, 5850/5980 University Ave, Halifax, Nova Scotia, B3K 6R8, Canada.
Disclosure
The authors declare that they have no competing interests
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. World Health Organization. Global status report on noncommunicable diseases 2014; 2014.
3. World Health Organisation (WHO). Non-communicable diseases country profiles 2018. Geneva; 2018.
4. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob. Heal. 2020;8:e191–e203. doi:10.1016/S2214-109X(19)30482-6
5. Chuang LT, Temin S, Camacho R, et al. Management and care of women with invasive cervical cancer: American society of clinical oncology resource-stratified clinical practice guideline. J Glob Oncol. 2016;2(5):311–340. doi:10.1200/JGO.2016.003954
6. World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva; 2020.
7. World Health Organization. WHO Technical guidance and specifications of medical devices for screening and treatment of precancerous lesions in the prevention of cervical cancer. Geneva; 2020.
8. Lemp JM, De Neve J-W, Bussmann H, et al. Lifetime prevalence of cervical cancer screening in 55 low-and middle-income countries. JAMA. 2020;324(15):1532–1542. doi:10.1001/jama.2020.16244
9. Aweke YH, Ayanto SY, Ersado TL. Knowledge, attitude and practice for cervical cancer prevention and control among women of childbearing age in Hossana Town, Hadiya zone, Southern Ethiopia: community-based cross-sectional study. PLoS One. 2017;12(7):1–18. doi:10.1371/journal.pone.0181415
10. Binagwaho A, Ngabo F, Wagner CM, et al. Integration of comprehensive women’s health programmes into health systems: cervical cancer prevention, care and control in Rwanda. Bull World Health Organ. 2013;91(9):697–703. doi:10.2471/BLT.12.116087
11. LaVigne AW, Triedman SA, Randall TC, Trimble EL, Viswanathan AN. Cervical cancer in low and middle income countries: addressing barriers to radiotherapy delivery. Gynecol Oncol Rep. 2017;22:16–20. doi:10.1016/j.gore.2017.08.004
12. Onyenwenyi AOC, Gugu GM. Strategies for the prevention and control of cervical cancer in rural communities: a Nigerian perspective. J Community Med Prim Heal Care. 2016;28(2):77–93.
13. National Institute of Statistics of Rwanda. Fourth Population and Housing Census, Rwanda, 2012. Thematic Report. Population Projections; 2014.
14. Ruzigana G, Bazzet-Matabele L, Rulisa S, Martin AN, Ghebre RG. Cervical cancer screening at a tertiary care center in Rwanda. Gynecol Oncol Rep. 2017;21:13–16. doi:10.1016/j.gore.2017.05.005
15. Umulisa MC, Franceschi S, Baussano I, et al. Evaluation of human-papillomavirus testing and visual inspection for cervical cancer screening in Rwanda. BMC Womens Health. 2018;18(1):1–8. doi:10.1186/s12905-018-0549-5
16. Ngabo F, Franceschi S, Baussano I, et al. Human papillomavirus infection in Rwanda at the moment of implementation of a national HPV vaccination programme. BMC Infect. Dis. 2016;16(1):1–10. doi:10.1186/s12879-016-1539-6
17. Ndateba I, Kabatsinda A, Ndabarora E. Uptake of cervical cancer screening and associated factors among women attending outpatient services in Rwamagana Hospital, Rwanda. Rwanda J Med Heal Sci. 2021;4(3):387–397. doi:10.4314/rjmhs.v4i3.8
18. Niyonsenga G, Gishoma D, Sego R, et al. Knowledge, utilization and barriers of cervical cancer screening among women attending selected district hospitals in Kigali - Rwanda. Can Oncol Nurs J. 2021;31(3):266–274. doi:10.5737/23688076313266274
19. Mukanyangezi MF, Sengpiel V, Manzi O, et al. Screening for human papillomavirus, cervical cytological abnormalities and associated risk factors in HIV-positive and HIV-negative women in Rwanda. HIV Medicine. 2018;19(2):152–166. doi:10.1111/hiv.12564
20. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Heal Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
21. Hennink MM, Kaiser BN, Weber MB. What influences saturation? Estimating sample sizes in focus group research. Qual Health Res. 2019;29(10):1483–1496. doi:10.1177/1049732318821692
22. Then KL, Rankin JA, Ali E. Focus group research: what is it and how can it be used? Can J Cardiovasc Nurs. 2014;24(1):16–22.
23. Izuwayo G, Habtu M, Marete O, Mochama M, Rutayisire E, Dida O G. A mixed method study to assess women’s knowledge on cervical cancer screening and associated factors in Gakenke District, Rwanda. J Oncol Res Treat. 2021;S5(004):45.
24. Nkurunziza C, Ghebre R, Magriples U, Ntasumbumuyange D, Bazzett-Matabele L. Healthcare provider challenges to early detection of cervical cancer at primary healthcare level in Rwanda. Gynecol Oncol Rep. 2021;37:100810. doi:10.1016/j.gore.2021.100810
25. McIntosh MJ, Morse JM. Situating and constructing diversity in semi-structured interviews. Glob Qual Nurs Res. 2015;2:34.
26. Bengtsson M. How to plan and perform a qualitative study using content analysis. NursingPlus Open. 2016;2:8–14. doi:10.1016/j.npls.2016.01.001
27. Vaismoradi M, Jones J, Turunen H, Snelgrove S. Theme development in qualitative content analysis and thematic analysis. J Nurs Educ Pract. 2016;6(5):54.
28. Creswell JW. Research Design. Qualitative, Quantitative and Mixed Methods Approaches.
29. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
30. Bakiewicz A, Rasch V, Mwaiselage J, Linde DS. “The best thing is that you are doing it for yourself” - Perspectives on acceptability and feasibility of HPV self-sampling among cervical cancer screening clients in Tanzania: a qualitative pilot study. BMC Womens Health. 2020;20(1):1–9. doi:10.1186/s12905-020-00917-7
31. Rahman R, Clark MD, Collins Z, et al. Cervical cancer screening decentralized policy adaptation: an African rural-context-specific systematic literature review. Glob Health Action. 2019;12(1):1–14. doi:10.1080/16549716.2019.1587894
32. Ndayisaba G, Verwijs MC, van Eeckhoudt S, et al. Feasibility and acceptability of a novel cervicovaginal lavage self-sampling device among women in Kigali, Rwanda. Sex Transm Dis. 2013;40(7):552–555. doi:10.1097/OLQ.0b013e31828e5aa5
33. Lauren C. Rwanda’s community health worker program; 2014.
34. O’Donovan J, O’Donovan C, Nagraj S. The role of community health workers in cervical cancer screening in low-income and middle-income countries: a systematic scoping review of the literature. BMJ Glob Heal. 2019;4(3):1–8.
35. Castle PE, Rausa A, Walls T, et al. Comparative community outreach to increase cervical cancer screening in the Mississippi Delta. Prev Med (Baltim). 2011;52(6):452–455. doi:10.1016/j.ypmed.2011.03.018
36. Levano W, Miller JW, Leonard B, et al. Public education and targeted outreach to underserved women through the national breast and cervical cancer early detection program. Cancer. 2014;120(SUPPL. 16):2591–2596. doi:10.1002/cncr.28819
37. Oduro Appiah J, Agyemang-Duah W, Fordjour AA, Adei D. Barriers to formal healthcare utilisation among poor older people under the livelihood empowerment against poverty programme in Ghana. BMC Public Health. 2019;19(1):1–12. doi:10.1186/s12889-018-6343-3
38. Masiye F, Kaonga O. Determinants of healthcare utilisation and out-of-pocket payments in the context of free public primary healthcare in Zambia. Int J Heal Policy Manag. 2016;5(12):693–703. doi:10.15171/ijhpm.2016.65
39. Ponsar F, Tayler-Smith K, Philips M, et al. No cash, no care: how user fees endanger health-lessons learnt regarding financial barriers to healthcare services in Burundi, Sierra Leone, Democratic Republic of Congo, Chad, Haiti and Mali. Int Health. 2011;3(2):91–100. doi:10.1016/j.inhe.2011.01.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Economic Evaluations of HPV Vaccination in Targeted Regions of Low- and Middle-Income Countries: A Systematic Review of Modelling Studies
Frianto D, Setiawan D, Diantini A, Suwantika AA
International Journal of Women's Health 2022, 14:1315-1322
Published Date: 12 September 2022
Socio-Demographic Factors and Other Predictors of Pap Test Uptake Among Women: A Retrospective Study in Ghana
Mensah KB, Boamah Mensah AB, Yamoah P, Manfo J, Amo R, Wiafe E, Padayachee N, Bangalee V
Cancer Management and Research 2023, 15:489-499
Published Date: 12 June 2023
Screening of Depression Among Medical Outpatients Visiting the University Teaching Hospital of Kigali, Rwanda
Gafaranga JP, Bitunguhari L, Mudenge C, Manirakiza F, Kelly B, Gatabazi P
Neuropsychiatric Disease and Treatment 2024, 20:845-854
Published Date: 8 April 2024
Principles for Service Delivery: Best Practices for Cervical Screening for Women with Disabilities
Kuper H, Andiwijaya FR, Rotenberg S, Yip JL
International Journal of Women's Health 2024, 16:679-692
Published Date: 18 April 2024
“Barriers and Advantages of Self-Sampling Tests, for HPV Diagnosis: A Qualitative Field Experience Before Implementation in a Rural Community in Ecuador”
Vega-Crespo B, Neira VA, Maldonado - Rengel R, López D, Delgado-López D, Guerra Astudillo G, Verhoeven V
International Journal of Women's Health 2024, 16:947-960
Published Date: 28 May 2024