")
Back to Journals » Cancer Management and Research » Volume 15
Socio-Demographic Factors and Other Predictors of Pap Test Uptake Among Women: A Retrospective Study in Ghana
Authors Mensah KB , Boamah Mensah AB , Yamoah P, Manfo J, Amo R, Wiafe E , Padayachee N, Bangalee V
Received 15 December 2022
Accepted for publication 13 May 2023
Published 12 June 2023 Volume 2023:15 Pages 489—499
DOI https://doi.org/10.2147/CMAR.S398500
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Kofi Boamah Mensah,1 Adwoa Bemah Boamah Mensah,2 Peter Yamoah,3 Jennifer Manfo,4 Richmond Amo,5 Ebenezer Wiafe,6 Neelaveni Padayachee,7 Varsha Bangalee8
1Department of Pharmacy Practice, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 2Department of Nursing, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 3Department of Pharmacy Practice, University of Health and Allied Sciences, Kumasi, Ghana; 4Pharmacy Department, Maternal and Child Health Hospital, Kumasi, Ghana; 5Internal Medicine & Department of Herbal Medicine, University Hospital & Faculty of Pharmacy and Pharmaceutical Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 6Pharmacy Department, Ho Teaching Hospital, Ho, Ghana; 7Department of Pharmacy and Pharmacology, University of the Witwatersrand, Johannesburg, South Africa; 8Discipline of Pharmaceutical Sciences, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
Correspondence: Kofi Boamah Mensah, Email [email protected]
Introduction: The World Health Organization has reported a rise in cervical cancer in Ghana. Ghanaian women predominantly undergo opportunistic Pap smear screening for cervical cancer. Numerous studies have documented differences in the sociodemographic traits of participants undergoing Pap smear testing or screening, which correlates with their screening habits. This study aims to assess sociodemographic variables, including others that determine Pap test utilization at a single center in Ghana.
Methods: A single-center survey was conducted by extracting data from the records of women who walked in for Pap smear testing. A telephone survey was also conducted among these women to document their barriers to utilizing the center. For data analysis, descriptive statistics and chi-square were utilized.
Results: A total of 197 participants’ records were retrieved for the study. Most participants were market women (69.4%) and uneducated (71.4%). Their Pap smear screening records indicate that the majority (86%) had no history of cervical cancer screening, and only 3% tested positive for Pap smear test. Educational level, occupation and family history of cancer significantly correlated with participants’ Pap smear history (p< 0.05). However, most sociodemographic factors were not significant with the Pap test results of the participants (p> 0.05). The perceived barrier identified by most participants was the need for more information (67.40%) on the test.
Conclusion: This study revealed that sociodemographic and gynaecological factors do not correlate with Pap test results. However, education level, occupation, and family history of cancer were significantly associated with the history of Pap smear uptake. The most significant barrier hindering Pap smear services was the need for more information.
Keywords: pap smear, cervical cancer, sociodemographic factors, gynaecological factors, screening, women, Ghana
Introduction
The International Agency for Research on Cancer (IARC) Global Cancer Observatory has reported that over 569,000 new cases of cervical cancer and 311,000 deaths occur annually worldwide.1,2 About 90% of these new cases and deaths globally occur in low- and middle-income countries (LMICs).3 It has been reported to be the most prevalent female reproductive organ cancer in sub-Saharan Africa4 with a record of 20% to 25% of total cancer cases.2 This makes it one of the most significant public health concerns globally. The incidence and mortality of cervical cancer have continued to be high in LMICs due to a lack of structured, regular screening exercises to detect and treat precancerous lesions.4
Cervical cancer estimates in Ghana indicate that 3151 women are diagnosed with the disease and 2119 deaths annually.5 The World Health Organization (WHO) has projected a rise in cervical cancer in the country to approximately 5000 cases and 3300 deaths annually by 2025.6 The projected increase in disease cases and death can be reduced through primary (vaccination) and secondary prevention (screening and precancerous lesions treatment).7 However, there is a lack of national vaccination and screening programme, but like in most LMICs, Ghanaian women predominantly undergo opportunistic Pap smear screening for cervical cancer.7
Numerous studies have reported variations in the sociodemographic characteristics of participants undertaking Pap smear test or screening, which correlates with their screening behavior.8,9 Studies done in North America reported low socioeconomic class, old age, and ethnic group to be associated with poor screening.8–10 A similar study done in Taiwan also reported a strong association between the age of women (below 30 and over 65 years) and their willingness to undergo Pap smear screening.11 In Australia, older women, unmarried and with poor socioeconomic level, are found to be less willing to undergo Pap smear screening.9
In Africa, a study titled “Socio-demographic characteristics and associated factors influencing cervical cancer screening among women attending St. Paul’s Teaching and Referral Hospital, Ethiopia” also reported that middle age women were more likely to undertake Pap smear screening.2 A similar study done in Nigeria also reported that previous awareness of Pap smear screening positively influenced the screening uptake of women.4 To the best of the authors’ knowledge, there is a lack of such studies in Ghana.
Awareness of sociodemographic variations and other predictors among the public or population on Pap smear usage is essential. This can help identify the part of the population at risk of underutilizing Pap smear screening for cervical cancer. Since Ghanaian women undertake opportunistic Pap smear screening, it is crucial to identify sociodemographic predictors, including others, that determine utilization of Pap test at a single center in Ghana.
Methodology
Study Design
A retrospective, cross-sectional, descriptive analysis of the screening records of women was carried out using a checklist to retrieve data from the hospital records of females who have undergone Pap smear screening at Kumasi Children’s Home Hospital, located in Kumasi, Ghana.
Study Population and Data Tool
The sample population included women from the suburbs of Kumasi, who utilized the screening center from 2015 to 2020. A purposive sampling method was used because records obtained from the biostatistics office of the hospital indicate a low utilization of the pap smear center. Hence, the researcher and his team decided to include all women who visited the center and meet the inclusion criteria. Therefore, 202 records were obtained. A total of 197 records were included in the study based on the set inclusion and exclusion criteria.
The data capturing tool had two sections. Section A covered the following areas: (1) sociodemographic information (Age, Marital Status, Occupation and Educational background), (2) gynaecological and obstetric history (parity) and (3) history of Pap Smear test, whether the test yielded positive or negative results. The detailed medical history of the participants was not captured on the data capturing sheet since this was a walk-in screening center. Section B contained a list of perceived barriers towards utilization of the Pap smear screening center. The questionnaire was adopted and adapted from Bayu et al12 and Woldetsadik et al2 The researchers conducted a preliminary conversation about the barrier items among five women to get information about their understanding of them. These women deemed these items “difficulty to talk to a provider, do not know where to get the service, and perceived poor quality of service” as not a barrier to general healthcare delivery. Hence, the questionnaire was modified to exclude these items.
Inclusion and Exclusion Criteria
One of the treatment modalities for cervical cancer is hysterectomy, hence all women with no history of hysterectomy were included. Also, women who had taken pap test before were included in the study. The exclusion criteria included women who had undergone complete hysterectomy, pregnant women, incomplete records that had missing information and ages less than 18 and over 70 years.
Data Collection Method and Approach
One of the researchers, a hospital staff member, was responsible for collecting data to check and guarantee consistency. Researchers accessed screening records from the hospital Pap smear center after working hours to ensure privacy. No records were removed from the screening center office. A data capturing sheet with a checklist was used to collect the data, and the records were filled back into their original places by the center clerk. Another member of the researcher's team called the participants on phone to collect data on their perceived barriers towards utilization of the Pap smear screening center. English and Twi where applicable were the languages used by the research member in communication. Confidentiality of the data was ensured by allocating numbers to the document to hide the women’s identities. The data was collected from 1st June to 30th June 2022 because the researcher worked after the closing hours of the center.
Data Analysis
The data were analysed using SPSS software version 25 for windows (Statistical Package for the Social Sciences). The authors used descriptive statistic method to describe and present the data as averages and frequencies. This was then used to make inferences and conclusions about the sample population. The chi-square test was also employed to determine the quantitative measures that tested the results’ consistency, stability and predictability.
Associations between sociodemographic features and variables were recorded. Responses to questions were coded such that answers with a “yes” were scored one and “no” were scored 0. Age and parity were recorded on the nominal scale. A positive pap smear result was recorded as 1, whereas a negative result was recorded as 0. A positive pap smear indicates the presence of atypical or abnormal cervix cells while a negative test indicates no cell alterations. Regarding marital status, married were given a number of 1, and unmarried was quoted as 0. Women who had a history of pap smear were given one, and those who did not were given a 0 score.
Ethical Consideration
Ethical clearance was obtained from the Committee on Human Research and Publication Ethics, Kwame Nkrumah University of Science and Technology, Ghana (CHRPE), which approved the study with registration number CHRPE\AP\043\22. Each responder was made aware of the goals and parameters of the study during the telephone survey. CHRPE approved the use of verbal informed permission for this study; hence, this was obtained from enrolled study participants. This was necessary because it was a retrospective study. Most participants do not visit the screening site regularly, and they are scattered all over the city, making it challenging to receive written consent but easier to get verbal permission. When study participants indicated their willingness to participate, the data collectors checked the appropriate box on the consent form’s checklist.
Results
Socio-Demographic Characteristics
A total of 197 participants’ records were retrieved for the study. The mean age of the participants was 21.44 years, with most of them in the age group of 31–40 years. There was an almost equal distribution of married participants (53.2%) and unmarried participants (47.7%). Most were uneducated (71.4%) and market women (69.4%) as their job description. Their parity showed that more than half of them (54.3%) had never given birth. Their Pap smear screening records indicate that the majority (86%) had no history of cervical cancer screening, and only 3% tested positive for Pap smear test. Details are presented in Table 1.
 |
Table 1 Socio-Demographic Characteristics of Respondents (n=197) |
Gynaecological and Personal History
The gynaecological and obstetric history of the participants showed that approximately half of them had a history of regular (55%) and irregular (45%) menstrual cycles. The majority (72%) had their menarche at the age of 10–13 years. Also, 11% of them have undergone abortions in the past. Most participants (78%) have no idea of their family history of cervical cancer and past medical history of cervical cancer (72%). Details are presented in Table 2.
 |
Table 2 Gynaecological and Personal History (n=197) |
Perceived Barriers Towards Participation in Pap Smear Test
Participants who fear the outcome of the Pap smear test are less likely to undertake the test [OR = 0.52, 95% CI: (0.24–0.94)] than those who do not fear the outcome of their result. Participants who have adequate information about Pap smear are likely to undertake Pap smear test regularly [OR = 2.84, 95% CI: (1.60–4.52)] compared to participants who require more information about the test. Again, respondents whose residents are far from the screening center are less likely to subsequently visit the center for Pap smear test [OR = 0.57, 95% CI: (0.41–0.82)] as compared to those who live closer to the screening center. Women with a history of obstetrics and gynecology illness were more likely to undertake Pap tests [OR = 4.64, 95% CI: (0.36–2.63)] in comparison to women who felt healthy. Details are presented in Table 3.
 |
Table 3 Correlation Analysis of Perceived Barriers and Pap Smear Test Utilization (n = 197) |
Association Between Pap Smear Result and Sociodemographic Factors
When age, parity, occupation and marital status were analyzed against pap smear results, there was no correlation between the variables and the test results that showed positive Pap smear, as the p-values were more than 0.05%. The details have been provided in Table 4.
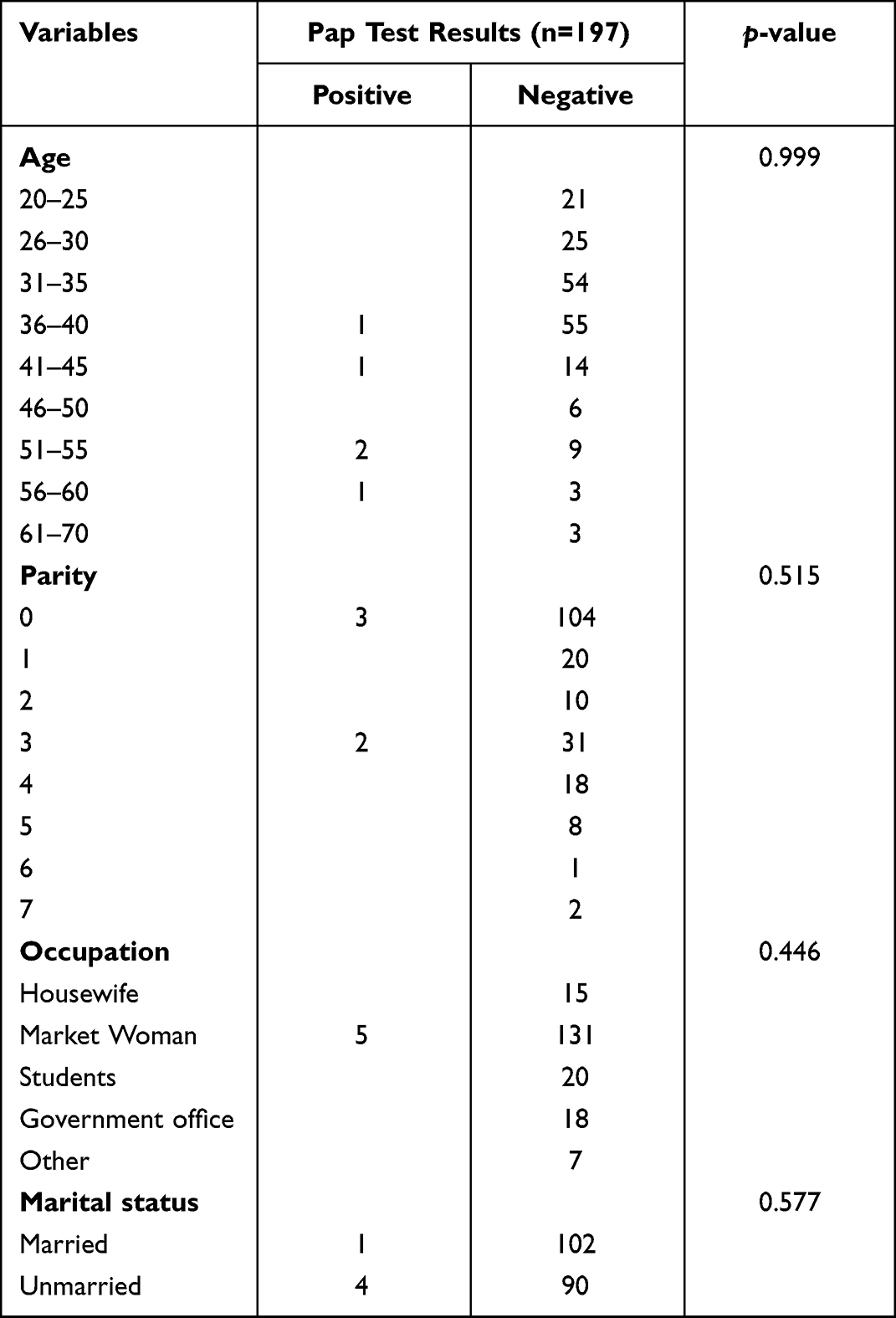 |
Table 4 Correlation Between Pap Smear Results and Sociodemographic Variables |
Association Between Pap Smear Result and Gynaecological Factors
When the gynaecological variables were analyzed against pap smear results, there was no correlation between the variables and the test results that showed positive Pap smear. The details have been provided in Table 5.
 |
Table 5 Correlation Between Pap Smear Results and Gynaecological Variables |
Association Between Pap Smear History and Sociodemographic Factors
The association between the education of the participants and Pap smear test history was analyzed to see whether different levels of education influence the number of people who underwent frequent Pap smear tests. Using a chi-square test, a p-value of 0.00 (p=<0.05) was obtained for educational level and past pap smear history. Hence, the correlation was significant, and an association was seen between the two parameters. Similarly, when the occupation was tabulated against Pap smear history, and the chi-square test was run, the p-value was again 0.00 (p<0.05), showing a significant correlation, which indicates an association between occupation and pap smear history. Similarly, for the variable, history of cancer, the p-value obtained indicates a correlation between this variable and Pap test history. The findings are summarized in Table 6.
 |
Table 6 Correlation Between Pap Smear Test History, Sociodemographic and Gynaecological Factors |
Discussion
Pap smear test in an asymptomatic population is intended to identify and reduce mortality from cervical cancer. This is the first study that describes sociodemographic determinants associated with the utilization of cervical cancer screening in Ghana. The findings reveal that uneducated people utilized or are more likely to undergo Pap smear screening than educated people. Studies have reported that the low level of utilization of Pap smear screening is due to insufficient knowledge or awareness and service availability.13,14 Our study did not measure knowledge; however, the availability of the service might have increased the utilization of Pap smear screening in the uneducated population. Again, maternal, family planning and child health-care services are integrated at the hospital where the screening center is located. Hence, many women visit the hospital for their health-care needs and are provided with cervical cancer information, which might have also accounted for the increased test utilization in the uneducated population. This study’s results are similar to others in Addis Ababa and Bangladesh which reported increased uptake of cervical screening services due to the availability of the services and provision of cervical cancer information at the health facility.14,15
More than half of the percentage of women who utilized the Pap smear screening test were between 31 and 40 years old. The WHO has also reported that the target age group in low-resource countries should be between 30 and 49 years old since the disease is uncommon in females under 30.16 This might have informed the screening centre’s health-care staff, hence focusing on or encouraging this age group to take the test. The highest female population in Ghana is in the age range of 30–39 years, constituting 13.45%.17 This might also explain why this population was the most significant group utilizing the screening center. Every woman should have one Pap smear before age 45 to reduce cervical cancer risk.18 Most participants who utilized the screening center were below this recommended age, hence a positive initiative by these women towards cervical cancer prevention.
Majority of the females who utilized the center were market women. The largest open market in West Africa, the Kejetia market,19 is very close to the hospital, making it easy for market women to seek healthcare, thereby utilizing the screening center. This indicates that proximity is a motivator in increasing the screening uptake. This study is consistent with one conducted in Mexico, which reported that greater accessibility increases cervical cancer screening uptake.20 Related studies done in Uganda21 and Nepal22 have also indicated that proximity is crucial to the uptake of cervical cancer screening tests such as Pap smear.
The study indicates nulliparous women took Pap smear test more than multiparous women. This is contrary to studies that reported nulliparous women are associated with low cervical cancer screening.2,23 Nulliparity is associated with an increased risk of endometrial cancer. Therefore, this group utilizing or participating more in Pap test has a positive attitude towards preventing gynaecological cancers.
This study found that the age, parity, occupation and marital status of women who utilized the Pap center have no significant association with the positive Pap smear results. Hence, the demographic characteristics of women do not determine their Pap test results. However, there was an association between Pap smear history and some demographic characteristics, namely education level and occupation. Women with lower education levels have taken Pap smears or had a Pap test history. The hypothesis is that the hospital is a public facility. Most uneducated women in Ghana have low socioeconomic status,24 hence utilize public services more often than educated people. Health-care staff at this facility more frequently recommended the Pap smear. Thus, this might be why uneducated women had a previous history of pap tests. Education is one of the most frequently mentioned independent factors in the literature.25 Numerous earlier studies revealed a favourable correlation between a high level of education and Pap smear utilization.26–28 However, other studies reported no correlation29–31 and a recent one done in Brazil,25 reported that women with a low level of schooling perform Pap smear test more than educated women.
Similarly, market women have a history of Pap tests compared to other occupations, such as those working in government organizations and students. Market women are self-employed and will have enough time to participate in screening exercises compared to government workers and students whose time is restricted due to their activities and who may need more time to engage in screening activities. These results are comparable to other studies done in Ethiopia2 and Greece32, which also reported that self-employed women were more engaged in cervical cancer screening activities than government staff and probably due to negligence and tight work schedule of these government staff. A family history of cancer was associated with a history of Pap testing. This might be due to awareness of cancer among family members, hence encouraging members to take the opportunity of screening services available. A study done in Indonesia reported that women with a family history of cervical cancer had undergone Pap testing due to awareness of the disease.33 Another study done among African American and white women also reported a unique perspective on the history of Pap test uptake and a family history of cervical cancer. Women with relatives of any cancer have undergone Pap tests in the past and this predicts their behaviour of Pap screening.34
The study showed that barriers such as “need more information”, “clinic far from home” and “no history of cervical illness” were the barriers identified by most participants towards utilization of the screening center. Another study in Ghana’s Central region also reported variables such as ‘screening sites being too far away, ‘limited information on cervical cancer’ and ‘absence of health education programs as the most dominant barriers.35 This result is in resonance with our study results. Other studies in other regions have also documented similar results, especially a need for more information about Pap smear screening.2,12,36 There was also a significant association between some variables: fear of the outcome, adequate information about Pap smear and distance between the screening center with the uptake of Pap test. Women who fear test outcome of the screening are less likely to undertake or utilize cervical screening. Those who are unaware of the disease are less likely to utilize the screening center. Lastly, the far away the participant is from the screening center, the less likely the participant will utilize the screening center. These barriers need to be addressed to increase cervical cancer screening.
There are some drawbacks to this study. Due to the small sample size, statistical power and generalization may be compromised. Part of the data collection was done using a telephone survey, which can lead to loss of anonymity, a rise in social desirability bias, and the interviewer’s mood, all of which have the potential to skew responses.
Conclusion
The purpose of this study was to ascertain the impact of sociodemographic and associated factors on women’s Pap smear test uptake. Based on our study findings, age, parity, occupation, and marital status have no significant association with positive Pap smear results. Also, gynaecological variables, age at menarche, family history of cancer, menstrual type, and abortion have no significant association with positive Pap smear results. However, education level, occupation, and family history of cancer were significantly associated with the history of Pap smear uptake. The most significant barrier hindering Pap smear services was the need for more information. Women form majority of the workforce in Ghana and contribute significantly to the country’s development. As a result, we recommend paying close attention to strengthening the healthcare system by giving due attention to education and follow-up on families with a history of gynaecological cancers. Policies should be drawn to address the perceived barriers women encounter to promote their health. This will improve Pap smear screening uptake.
Data Sharing Statement
The content contains the information that backs up this study’s results.
Ethical Considerations
The authors confirm that the study complies with the Declaration of Helsinki. The Institutional Ethics Review Board on Human Research and Publication Ethics, Kwame Nkrumah University of Science and Technology, Ghana, granted approval for the study.
Acknowledgments
We want to forward our respectful gratitude to the participants who took part in the study for their cooperation in giving us important information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study received no funding.
Disclosure
In this paper, the authors declare no conflicts of interest.
References
1. International Agency for Research on Cancer. Global Cancer Observatory. Geneva: World Health Organization; 2019.
2. Woldetsadik AB, Amhare AF, Bitew ST, Pei L, Lei J, Han J. Socio-demographic characteristics and associated factors influencing cervical cancer screening among women attending in St. Paul’s Teaching and Referral Hospital, Ethiopia. BMC Womens Health. 2020;20(1):1–9. doi:10.1186/s12905-020-00927-5
3. Shrestha AD, Neupane D, Vedsted P, Kallestrup P. Cervical cancer prevalence, incidence and mortality in low and middle income countries: a systematic review. APJCP. 2018;19(2):319. doi:10.22034/APJCP.2018.19.2.319
4. Okunade KS, John-Olabode S, Adejimi AA, et al. Predictors of pap smear testing uptake among women in Lagos, Nigeria. ecancermedicalscience. 2022;16. doi:10.3332/ecancer.2022.1368
5. Bray F, Ferlay J, Soerjomataram I, Siegel R, Torre L, Jemal A. Erratum: global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca Cancer J Clin. 2020;70(4):313.
6. Gyamfua AA, Nkrumah I, Ibitoye BM, et al. The level of knowledge and associated socio-demographic factors on cervical cancer among women: a cross-sectional study at Kenyase Bosore community, Ghana. Pan Afr Med J. 2019;34. doi:10.11604/pamj.2019.34.44.19471
7. Effah K, Tekpor E, Wormenor CM, et al. A revolution in cervical cancer prevention in Ghana; 2022.
8. Kim J, Dove MS, Dang JH. Sociodemographic factors associated with HPV awareness/knowledge and cervical cancer screening behaviors among caregivers in the US. BMC Women's Health. 2022;22(1):1–9. doi:10.1186/s12905-022-01918-4
9. Siahpush M, Singh GK. Sociodemographic predictors of pap test receipt, currency and knowledge among Australian women. Prev Med. 2002;35(4):362–368. doi:10.1006/pmed.2002.1086
10. Johnson NL, Head KJ, Scott SF, Zimet GD. Persistent disparities in cervical cancer screening uptake: knowledge and sociodemographic determinants of Papanicolaou and human papillomavirus testing among women in the United States. Public Health Rep. 2020;135(4):483–491. doi:10.1177/0033354920925094
11. Wang P, Lin R. Sociodemographic factors of pap smear screening in Taiwan. Public Health. 1996;110(2):123–127. doi:10.1016/S0033-3506(96)80059-X
12. Bayu H, Berhe Y, Mulat A, Alemu A, Grce M. Cervical cancer screening service uptake and associated factors among age eligible women in Mekelle Zone, Northern Ethiopia, 2015: a community based study using health belief model. PLoS One. 2016;11(3):e0149908. doi:10.1371/journal.pone.0149908
13. Abiodun O, Fatungase O, Olu-Abiodun O, Idowu-Ajiboye B, Awosile J. An assessment of women’s awareness and knowledge about cervical cancer and screening and the barriers to cervical screening in Ogun State, Nigeria. IOSR J Dent Med Sci. 2013;10(3):52–58. doi:10.9790/0853-1035258
14. Abu SH, Woldehanna BT, Nida ET, Tilahun AW, Gebremariam MY, Sisay MM. The role of health education on cervical cancer screening uptake at selected health centers in Addis Ababa. PLoS One. 2020;15(10):e0239580. doi:10.1371/journal.pone.0239580
15. Nessa A, Hussain MA, Ur Rashid MH, Akhter N, Roy JS, Afroz R. Role of print and audiovisual media in cervical cancer prevention in Bangladesh. Asian Pac J Cancer Prev. 2013;14(5):3131–3137. doi:10.7314/APJCP.2013.14.5.3131
16. World Health Organization. The Global Health Observatory: Cervical Cancer Screening. Geneva; 2022.
17. Statistics Times. Demographics of Ghana. Available from: https://statisticstimes.com/demographics/country/ghana-demographics.php.
18. Umarani M, Gayathri M, Kumar R. Study of cervical cytology in Papanicolaou (Pap) smears in a tertiary care hospital. Indian J Pathol Oncol. 2016;3(4):679–683. doi:10.5958/2394-6792.2016.00126.5
19. Wikipedia. Kejetia Market; 2022. Available from: https://en.wikipedia.org/wiki/Kejetia_Market.
20. McDonald YJ, Goldberg DW, Scarinci IC, et al. Health service accessibility and risk in cervical cancer prevention: comparing rural versus nonrural residence in New Mexico. J Rural Health. 2017;33(4):382–392. doi:10.1111/jrh.12202
21. Ndejjo R, Mukama T, Musabyimana A, Musoke D. Uptake of cervical cancer screening and associated factors among women in rural Uganda: a cross sectional study. PLoS One. 2016;11(2):e0149696. doi:10.1371/journal.pone.0149696
22. Ranabhat S, Tiwari M, Dhungana G, Shrestha R. Association of knowledge, attitude and demographic variables with cervical Pap smear practice in Nepal. Asian Pac J Cancer Prev. 2014;15(20):8905–8910. doi:10.7314/APJCP.2014.15.20.8905
23. Wongwatcharanukul L, Promthet S, Bradshaw P, Jirapornkul C, Tungsrithong N. Factors affecting cervical cancer screening uptake by Hmong hilltribe women in Thailand. Asian Pac J Cancer Prev. 2014;15(8):3753–3756. doi:10.7314/APJCP.2014.15.8.3753
24. Nkansah JN. The future of education in Ghana: critical education for socio-economic development. Int Interdiscip J Educ. 2021;10(SI):57–78.
25. Açucena Vieira Alves S, Schiaveto de Souza A, Weller M, Pires Batiston A. Differential impact of education level, occupation and marital status on performance of the Papanicolaou test among women from various regions in Brazil. APJCP. 2019;20(4):1037–1044. doi:10.31557/APJCP.2019.20.4.1037
26. Chang HK, Myong J-P, Byun SW, et al. Factors associated with participation in cervical cancer screening among young Koreans: a nationwide cross-sectional study. BMJ open. 2017;7(4):e013868. doi:10.1136/bmjopen-2016-013868
27. Farzaneh E, Heydari H, Shekarchi AA, Kamran A. Breast and cervical cancer-screening uptake among females in Ardabil, northwest Iran: a community-based study. Onco Targets Ther. 2017;10:985. doi:10.2147/OTT.S125344
28. Kelly DM, Estaquio C, Léon C, Arwidson P, Nabi H. Temporal trend in socioeconomic inequalities in the uptake of cancer screening programmes in France between 2005 and 2010: results from the cancer barometer surveys. BMJ open. 2017;7(12):e016941. doi:10.1136/bmjopen-2017-016941
29. Al Rifai R, Nakamura K. Differences in breast and cervical cancer screening rates in Jordan among women from different socioeconomic strata: analysis of the 2012 population-based household survey. Asian Pac J Cancer Prev. 2015;16(15):6697–6704. doi:10.7314/APJCP.2015.16.15.6697
30. Albuquerque CL, Costa P, Nunes FM, et al. Knowledge, attitudes and practices regarding the Pap test among women in northeastern Brazil. Sao Paulo Med J. 2014;132:3–9. doi:10.1590/1516-3180.2014.1321551
31. Salem MR, Amin TT, Alhulaybi AA, Althafar AS, Abdelhai RA. Perceived risk of cervical cancer and barriers to screening among secondary school female teachers in Al Hassa, Saudi Arabia. APJCP. 2017;18(4):969. doi:10.22034/APJCP.2017.18.4.969
32. Vakfari A, Gavana M, Giannakopoulos S, Smyrnakis E, Benos A. Participation rates in cervical cancer screening: experience in rural Northern Greece. Hippokratia. 2011;15(4):346.
33. Sumarmi S, Hsu -Y-Y, Cheng Y-M, Lee S-H. Factors associated with the intention to undergo Pap smear testing in the rural areas of Indonesia: a health belief model. Reprod Health. 2021;18(1):1–10. doi:10.1186/s12978-021-01188-7
34. Williams KP, Reiter P, Mabiso A, Maurer J, Paskett E. Family history of cancer predicts Papanicolaou screening behavior for African American and white women. Cancer. 2009;115(1):179–189. doi:10.1002/cncr.23994
35. Ebu NI, Mupepi SC, Siakwa MP, Sampselle CM. Knowledge, practice, and barriers toward cervical cancer screening in Elmina, Southern Ghana. Int J Womens Health. 2015;7:31. doi:10.2147/IJWH.S71797
36. Nigussie T, Admassu B, Nigussie A. Cervical cancer screening service utilization and associated factors among age-eligible women in Jimma town using health belief model, South West Ethiopia. BMC Womens Health. 2019;19(1):1–10. doi:10.1186/s12905-019-0826-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.