")
Back to Journals » Patient Preference and Adherence » Volume 16
Pre COVID-19 Pandemic Use of Telemedicine for Adherence Promotion in Patients with Psychotic Disorders: A Literature Review
Authors Edwards AM , Petitt JC, Kumar S, Levin JB, Sajatovic M
Received 4 May 2022
Accepted for publication 12 August 2022
Published 14 September 2022 Volume 2022:16 Pages 2559—2565
DOI https://doi.org/10.2147/PPA.S373309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Alyssa M Edwards,1 Jordan C Petitt,1 Sanjana Kumar,1 Jennifer B Levin,1,2 Martha Sajatovic1,2
1Case Western Reserve University School of Medicine, Cleveland, OH, USA; 2University Hospitals of Cleveland Medical Center, Department of Psychiatry, Cleveland, OH, USA
Correspondence: Martha Sajatovic, University Hospitals of Cleveland Medical Center, Department of Psychiatry, 10524 Euclid Ave, Cleveland, OH, 44106, USA, Email [email protected]
Introduction: Given the increasing use of telepsychiatry and to serve as a reference point informing future research, our team evaluated the literature on the use of telepsychiatry for medication adherence promotion prior to the COVID-19 pandemic among patients with psychotic disorders.
Methods: A search of PubMed, Cochrane, Web of Science, CINAHL, and PsycINFO was conducted using PRISMA guidelines to identify telepsychiatry interventions to enhance medication adherence in patients with primary psychotic disorders. Both quantitative and qualitative data were extracted from the identified articles including study characteristics, interventions, and outcomes.
Results: In total, 230 articles were obtained through electronic literature search, and 4 articles were eventually retained that met inclusion criteria. All 4 articles were randomized controlled trials, were adjuncts to in-person usual care, used telephone platforms and targeted medication adherence. Compared to treatment as usual, 3 out of 4 studies found medication adherence was improved and 2 out of 4 studies found improved medication attitudes. Telepsychiatry appeared to be acceptable to patients with psychotic disorders.
Discussion: In the pre-Covid-19 literature, telepsychiatry appears promising as an adjunct to usual care for increasing medication adherence among individuals with schizophrenia/schizoaffective disorder. However, given the limited number of papers and exclusive use on telephone-only to deliver telepsychiatry, additional research specific to telepsychiatry for patients with psychosis is needed.
Keywords: telemedicine, telehealth, telepsychiatry, remote delivery, virtual delivery, schizophrenia, schizoaffective disorder
Introduction
Schizophrenia is defined by abnormalities which affect quality of life such as delusions, hallucinations, disorganized thinking, grossly disorganized or unusual motor behavior and negative symptoms.1,2 A cornerstone of treatment is antipsychotic medication; however, adherence to medication regimens can be as low as 40%, leading to longstanding negative consequences including hospitalization, incarceration and homelessness.3,4 As such, psychosocial approaches are often important in maintaining adherence and preventing relapse.1
Telepsychiatry, a subset of telemedicine, involves providing psychiatric care from a distance through technology, such as telephone or video conferencing. The range of services includes psychiatric evaluation, psychotherapy, education, and medication management through an interactive technological interface.5,6 Telepsychiatry can improve access to mental health care and contribute to patient satisfaction.5,6
Since the start of the COVID-19 pandemic, there has been a dramatic increase in the use of telemedicine.7,8 For patients with primary psychotic disorders, such as schizophrenia or schizoaffective disorder, telepsychiatry may offer a convenient way to provide clinical service, maintain clinical stability and monitor or improve medication adherence.5 However, there are concerns that using a technological interface could exacerbate psychiatric symptoms, particularly paranoia.5 One paper, which was published prior to the pandemic, reviewed the use of telepsychiatry for the treatment and assessment of schizophrenia and concluded that it was feasible with preliminary evidence of improving outcomes.6 This review did not focus specifically on interventions to promote medication adherence, was focused on schizophrenia alone, and did not limit its inclusion to randomized controlled trials (RCTs).
Considering the poor medication adherence of this patient population, our team was interested in investigating the body of research on the use of telepsychiatry in RCTs for adherence promotion in patients with primary psychotic disorders prior to the start of the COVID pandemic. We elected to focus our review on publications that predated the pandemic to serve as a reference point for future work that is specifically focused on telepsychiatry in the COVID era and beyond. With this literature review, we aimed to evaluate the efficacy of adherence interventions delivered using telepsychiatry on patient outcomes among individuals with psychotic disorders.
Methods
Literature Search
With collaboration from a university research librarian and following Prisma guidelines,9 five electronic databases (PubMed, Cochrane, PsychInfo, Web of Science, CINAHL) were searched for original research articles on the utilization of telepsychiatry in patients with psychotic disorders. Our search strategy included combinations of the following words (and other equivalent terminology): telemedicine, telehealth, telepsychiatry, remote delivery, virtual delivery, serious mental illness, schizophrenia, schizoaffective disorder, psychotic disorders, adherence, compliance, medication, treatment.
Inclusion and Exclusion Criteria
The inclusion of articles were based upon the following criteria: (1) all ages; (2) original research reports published up until April 2020; (3) English language peer-reviewed literature; (4) must have a primary psychotic psychiatric disorder defined as schizophrenia, schizoaffective disorder or schizophrenia spectrum – the basis of the psychiatric diagnosis could be based on self-report, clinical evaluation, standardized diagnostic interview, or medical record diagnosis; (5) telepsychiatry/telemedicine consists of a behavioral intervention or treatment to improve treatment adherence, where the delivery of the intervention is done remotely by a clinician using technology and in which health professionals and patients interact in real-time. Interventions must be entirely or substantively delivered remotely; (6) studies could compare some type of experimental telehealth vs some other type of intervention (such as in-person intervention or treatment as usual); (7) studies have at least 1 patient-level outcome and patient acceptability can be considered an outcome, (8) longitudinal studies.
Exclusion criteria were as follows: (1) papers focused only on clinical evaluation comparing in-person vs remote; (2) interventions that are primarily automated therapies or apps; (3) studies where the technology was simple notifications delivered by phone, text or email (eg, appointment reminders); (4) other psychiatric diagnoses including bipolar disorder; (5) interventions where the primary focus is on substance use/abuse or other non-psychotic condition (premenstrual dysphoric disorder, etc.), and (6) opinion pieces, other literature reviews, case studies, or book chapters.
Analytical Strategies
The first 3 authors screened and rated all abstracts for relevance of inclusion and exclusion criteria. When there was disagreement among the 3 raters, the full article was reviewed, and if needed, the other authors weighed in. Study variables were extracted including author, year, study design, sample description, control group, intervention, outcome, measurement, and results.
A quality analysis was performed using the adapted Methodological Quality Rating Scale (MQRS).10 The MQRS is a widely used tool to evaluate the quality of studies based on the following components: study design, replicability, baseline characteristics, quality control, follow-up length, intervention dosage, collateral and objective verification, dropouts and attrition, statistical power, independent outcome assessment, statistical analyses, and number of study sites. Scores on the MQRS range from 0 (poorer quality) to 17 (higher quality).
Results
Study Selection
As demonstrated in Figure 1, the literature search initially returned a total of 230 articles. Each publication underwent title and abstract screening. The remaining 29 articles underwent full-text screening and data extraction and 4 articles eventually met inclusion criteria.
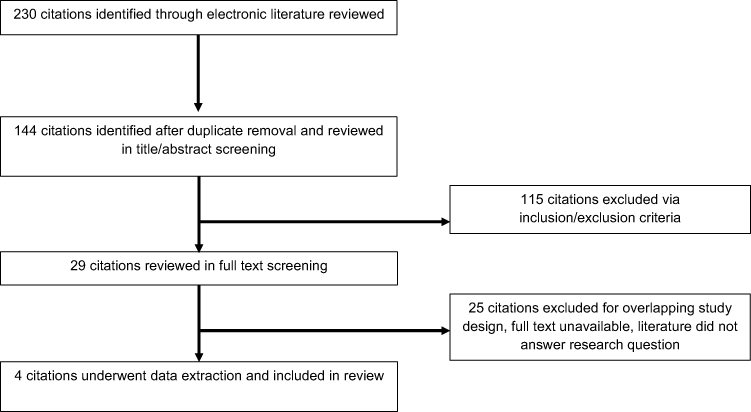 |
Figure 1 CONSORT diagram. |
Study Characteristics
Collectively, the studies included a total of 1076 patients with schizophrenia or schizophrenia spectrum disorders, with a mean or median age ranging from 38.9−52 years. Female participants comprised 34.8–58.7% of study samples. Study characteristics including sample description, study design, outcomes and quality ratings were extracted from the included studies (Table 1).
 |
Table 1 Study Characteristics – Sample, Design, Outcomes, Results, and Quality |
Three studies investigated patients with schizophrenia, while 1 study investigated patients with schizophrenia spectrum disorders (defined as schizophrenia, schizophreniform disorder, and schizoaffective disorders).
Two studies were based in the United States (n = 2, 50%), while Spain (n = 1, 25%) and Turkey (n = 1, 25%) were the locations for the other 2 studies.
Three of 4 studies were set in community health centers (n = 3, 75%), while one was set in an inpatient psychiatric unit (n = 1, 25%). Study duration ranged from 2 to 4 months [median = 3 months]. All 4 studies were prospective randomized controlled trials (RCTs) comparing telepsychiatry as an adjunct to usual care vs treatment as usual (TAU).
Technology Platforms
Studies used direct communication between provider and patient in a real-time digital media platform. All 4 studies used a telephone-based intervention (n = 4, 100%). Three of 4 studies used the Telephone Intervention Problem Solving (TIPS) application.11–13 TIPS is a telephone nursing intervention that provides weekly support to increase positive medication attitudes and reduce psychiatric hospitalizations.12 TIPS is grounded in planned behavior theory and is used to support daily life problems, using weekly interviews that help patients cope with problems, such as sub-optimal medication adherence.12,13
Outcomes
Patient Level Outcomes
Patient-level outcomes assessed included medication adherence (N = 4, 100%) and medication attitudes (N = 4, 100%). All 4 studies investigated medication adherence as an outcome when comparing telephone-based nursing support as an adjunct to routine care versus TAU.11–14 Three of 4 studies found higher adherence to psychiatric medications with telepsychiatry vs TAU. Uslu et al found that patients receiving telepsychiatry had a higher belief in the necessity of medication (p = 0.008) and higher voluntary medication continuation (p < 0.001).12 The Drug Attitude Inventory (DAI), used in Monte’s study to identify subjective attitude towards antipsychotic medication, was significantly better in the telehealth group.13 Furthermore, Montes found that improved adherence led to a reduction in psychopathology, mainly in positive symptoms.7 Unlike in the other 3 studies, Beebe did not find a statistically significant difference in adherence or medication taking self-efficacy with TIPS vs TAU.11
Acceptability of Telehealth Interventions
Acceptability often refers to how well an intervention is received within the target population and is a critical aspect of generalizability of the treatment. None of the 4 reports specifically reported on perceived acceptability of the adherence promotion interventions at the patient level. However, attrition rates to study participation by intervention arm (see Table 1) may provide at least some proxy indication for program acceptability. Montes reported overall low attrition rates ranging from 10.3% (experimental intervention) to 7.2% (controls).13 Beebe similarly reported relatively low attrition rates of 13% for the experimental arm (TIPS) vs a Control attrition rate 7%.14 Uslu found a 12% attrition rate with experimental intervention and 0% attrition with controls.12 In contrast to the other 3 reports, a later report by Beebe reported an attrition rate of approximately 24% for a project that tested TIPS but did not report attrition rates differentially comparing experimental intervention vs controls.11
Study Quality Assessment
MQRS scores (Table 1) for the included studies ranged from 10 to 14 and averaged 11.5 ± 1.66. Strengths in the study quality included the fact that they were RCTs (n = 4) and inclusion of baseline to post-intervention follow-up (n = 4). Limitations included relatively short follow-up (≤4 months) and no discussion of dropouts.
Discussion
The use of technology for intervention delivery is increasingly in demand among patients with psychosis.15 This systematic literature review, which evaluated the efficacy of adherence interventions delivered using telepsychiatry on patient outcomes among individuals with psychotic disorders, had several key findings that may help to inform future research. This review may also serve as a useful reference point with respect to the pre-COVID use of telepsychiatry to help inform delivering mental health care in the COVID/post-COVID era.15
First, our review yielded a limited number of publications with a rather narrow use of telehealth delivery modes. The technology platform used in these 4 studies was telephone and evaluated 2 different adjunct adherence interventions. In 3 of 4 studies, the intervention was Telephone Intervention Problem Solving or TIPS. In contrast, a recent set of recommendations on the use of telepsychiatry in the COVID era suggests that digital platforms that include video assessments are an important component of care.16
Second, the findings broadly suggest that telehealth for patients with schizophrenia may improve medication adherence and medication attitudes. In 2 of the 3 TIPS studies, medication adherence was better in the intervention groups vs controls. An additional point worth noting is that TIPS was delivered by nursing staff to support adherence behaviors in all the selected studies. While the findings are potentially generalizable to team-based care and/or care delivered by other specialty mental health clinicians, it is not clear if the medication adherence patterns seen in these reports would have also occurred if telepsychiatry had been delivered by prescribing clinicians such as psychiatrists or advanced practice nurses with prescribing authority.
Finally, the acceptability of telepsychiatry for patients with psychosis in our review of pre-COVID interventions, based on study attrition rates, appeared to be relatively good with roughly 80–90% of individuals being able to continue participation in programs. However, important caveats are that in all 4 studies identified in our review, telepsychiatry was an adjunct to in-person care, and acceptability was not assessed at the patient level in any of the reports. It is not possible to conclude how useful these interventions might be as a stand-alone treatment for people with psychotic conditions. A recent set of recommendations for clinicians on the delivery of telepsychiatry provides some specific examples of special populations which may have specific or unique needs within the telepsychiatry model, including older adults, children/adolescents and groups that may have specific cultural considerations.16 The recommendations did not note the need for any special accommodations for patients with psychosis. Future studies testing telepsychiatry acceptability should include patient-level specific questions regarding perceived satisfaction with interventions.
During the COVID pandemic, travel and safety restrictions have severely limited the ability of psychiatric patients to receive in-person care. Continuing areas that need additional focus include issues of information governance, consent and confidentiality as well as modifications to in-person assessment that may be appropriate for implementing digital technologies.16
Our review findings, based on delivery of phone telepsychiatry delivered by nurses, did not find that patients with schizophrenia had difficulty receiving or benefitting from services. During the COVID era, telepsychiatry delivered via videoconference provides an ability to see the patient’s home environment, which can be helpful in treatment planning. For patients with psychosis, physical presence or video observation could facilitate the assessment of personal hygiene, other basic functions, and extrapyramidal signs.12 Telepsychiatry may also help with resource limitations and may improve care access.
However, there are also potential disadvantages to telepsychiatry. Lack of visibility of symptoms via telephone or video screen can lead to an underestimation of symptom severity and in turn may negatively impact treatment decision and patient outcomes.17 In rural communities, telepsychiatry may be limited by a lack of broadband service.18 Taken together, future studies need to investigate the benefits and burdens of telepsychiatry more specifically for people with psychosis.
Limitations of this review include the small number of studies, exclusive reliance on audio-only delivery of telepsychiatry, the fact that telepsychiatry interventions did not have an attentional control, the short duration of study designs as well as the limited focus on treatment outcomes beyond medication adherence. In addition to the need for future studies specific to telepsychiatry in patients with psychosis using newer digital technologies, there is a need for a head-to-head comparison of current remote technologies to one another (phone vs videoconferencing) and to in-person care.
Conclusion
This review of pre-COVID pandemic publications of studies using adjunct telepsychiatry in patients with schizophrenia suggests that interventions are acceptable to patients and may be promising to improve medication adherence and attitudes toward medications. Future studies are needed to establish 1) utility of telepsychiatry as a stand-alone treatment; 2) assessment of newer remote technologies, and 3) assessing telepsychiatry on a broader array of treatment outcomes. Due to the limited selection of included articles, these findings should be considered preliminary.
Disclosure
Dr Martha Sajatovic reports grants from National Institute of Mental Health, during the conduct of the study; grants from Nuromate, Otsuka, International Society for Bipolar Disorders (ISBD), National Institutes of Health (NIH), Centers for Disease Control and Prevention (CDC), Patient-Centered Outcomes Research Institute (PCORI), personal fees from Alkermes, Otsuka, Sunovion, Janssen, Lundbeck, Teva, Clinical Education Alliance, Health Analytics, other from Springer Press, Johns Hopkins University Press, Oxford Press, UpToDate, other from American Physician’s Institute (CMEtoGo), Psychopharmacology Institute, Novus, American Epilepsy Society, American Society of Clinical Psychopharmacology, American Academy of Child and Adolescent Psychiatry, Neurocrine, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Schizophrenia. WHO/OMS; 2022.
2. Harrison G, Hopper K, Craig T, et al. Recovery from psychotic illness: a 15- and 25-year international follow-up study. Br J Psychiatry. 2001;178:506–517. doi:10.1192/bjp.178.6.506
3. Velligan DI, Lam YW, Glahn DC, et al. Defining and assessing adherence to oral antipsychotics: a review of the literature. Research support, N.I.H., extramural review. Schizophr Bull. 2006;32(4):724–742. doi:10.1093/schbul/sbj075
4. Sajatovic M, Levin J, Ramirez LF, et al. Prospective trial of customized adherence enhancement plus long-acting injectable antipsychotic medication in homeless or recently homeless individuals with schizophrenia or schizoaffective disorder. J Clin Psychiatry. 2013;74(12):1249–1255. doi:10.4088/JCP.12m08331
5. Association AP. Telepsychiatry. American Psychiatric Association. Available from: https://www.psychiatry.org/psychiatrists/practice/telepsychiatry.
6. Kasckow J, Felmet K, Appelt C, Thompson R, Rotondi A, Haas G. Telepsychiatry in the assessment and treatment of schizophrenia. Clin Schizophr Relat Psychoses. 2014;8(1):21–27A. doi:10.3371/CSRP.KAFE.021513
7. Anthony Jnr B. Use of telemedicine and virtual care for remote treatment in response to COVID-19 pandemic. J Med Syst. 2020;44(7):132. doi:10.1007/s10916-020-01596-5
8. Bokolo AJ. Exploring the adoption of telemedicine and virtual software for care of outpatients during and after COVID-19 pandemic. Ir J Med Sci. 2021;190(1):1–10. doi:10.1007/s11845-020-02299-z
9. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–1012. doi:10.1016/j.jclinepi.2009.06.005
10. Miller WR, Wilbourne PL. Mesa Grande: a methodological analysis of clinical trials of treatments for alcohol use disorders. Addiction. 2002;97(3):265–277. doi:10.1046/j.1360-0443.2002.00019.x
11. Beebe LH, Smith K, Phillips C. Effect of a telephone intervention upon self-reported medication adherence and self-efficacy in outpatients with Schizophrenia Spectrum Disorders (SSDs). Issues Ment Health Nurs. 2016;37(10):708–714. doi:10.1080/01612840.2016.1214855
12. Uslu E, Buldukoglu K. Randomized controlled trial of the effects of nursing care based on a telephone intervention for medication adherence in schizophrenia. Perspect Psychiatr Care. 2020;56(1):63–71. doi:10.1111/ppc.12376
13. Montes JM, Maurino J, Diez T, Saiz-Ruiz J. Telephone-based nursing strategy to improve adherence to antipsychotic treatment in schizophrenia: a controlled trial. Int J Psychiatry Clin Pract. 2010;14(4):274–281. doi:10.3109/13651501.2010.505343
14. Beebe LH, Smith K, Crye C, et al. Telenursing intervention increases psychiatric medication adherence in schizophrenia outpatients. J Am Psychiatr Nurses Assoc. 2008;14(3):217–224. doi:10.1177/1078390308318750
15. Santesteban-Echarri O, Piskulic D, Nyman RK, Addington J. Telehealth interventions for schizophrenia-spectrum disorders and clinical high-risk for psychosis individuals: a scoping review. J Telemed Telecare. 2020;26(1–2):14–20. doi:10.1177/1357633X18794100
16. Smith K, Ostinelli E, Macdonald O, Cipriani A. COVID-19 and telepsychiatry: development of evidence-based guidance for clinicians. JMIR Ment Health. 2020;7(8):e21108. doi:10.2196/21108
17. Brewer WJ, Edwards J, Anderson V, Robinson T, Pantelis C. Neuropsychological, olfactory, and hygiene deficits in men with negative symptom schizophrenia. Biol Psychiatry. 1996;40(10):1021–1031. doi:10.1016/0006-3223(95)00594-3
18. St Clair M, Murtagh D. Barriers to telehealth uptake in rural, regional, remote Australia: what can be done to expand telehealth access in remote areas? Stud Health Technol Inform. 2019;266:174–182. doi:10.3233/SHTI190791
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.