Back to Journals » Advances in Medical Education and Practice » Volume 13
“Technology Proficiency” in Medical Education: Worthiness for Worldwide Wonderful Competency and Sophistication
Authors Jain S ![]() , Jain BK, Jain PK, Marwaha V
, Jain BK, Jain PK, Marwaha V
Received 17 June 2022
Accepted for publication 31 October 2022
Published 15 December 2022 Volume 2022:13 Pages 1497—1514
DOI https://doi.org/10.2147/AMEP.S378917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sunil Jain,1 Bhagya Kamal Jain,2 Prem Kamal Jain,3 Vishal Marwaha4
1Department of Paediatrics, Military Hospital Secunderabad, Telangana, India; 2Cloud, Google Inc, Hyderabad, Telangana, India; 3Department of Computational Biology, Indraprastha Institute of Information Technology, New Delhi, India; 4School of Medicine, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Cochin, Kerala, India
Correspondence: Sunil Jain, Department of Paediatrics, Military Hospital Secunderabad, c/o 56 APO, Secunderabad, Telangana, 900 453, India, Tel +91 9651834341, Email [email protected]
Purpose: Advances in bioinformatics, information technology, advanced computing, imaging techniques are changing fundamentally the way physicians define, diagnose, treat, and prevent disease. New disciplines – Artificial Intelligence, Machine Learning, Computational Biology – are improving healthcare. Digital health solutions have immense scope. Education and practice need to keep pace.
Methods: We aimed at assessment of “Technology proficiency” required by medical graduates and its implementation, if found useful. All this in a conceptual framework of “TP” model, having categories (a) proper assessment (b) pertinent treatment (c) progress monitoring (d) prevention applications (e) professional standards. A search of the literature was performed using MedLine & Cochrane Central Register of Controlled Trials databases, for systematic reviews and meta-analysis articles published in the last five years using keyword “technology”. Analysis of those relevant to the role all medical graduates should play. An analysis of worldwide statutory medical institutions guidelines.
Results: Twenty-three systematic studies and meta-analysis were studied. Eighteen show clear evidence for ‘Technology proficiency”, while 5 recommend further studies. The findings are discussed suiting the roles of doctors in the “TP” model. Medical institutions guidelines worldwide diligence suggests need of including “Technology proficiency” as a definite and distinct strategic plan. Medical Council of India mandates “use information technology for appropriate patient care and continued learning”. General Medical Council, UK and Medical Council India have been proactive in technology training. GMC recommends technology use for learning, prescribing, communication, and interpersonal skills. It should be expanding technology proficiency in practice as an essential professional capability.
Conclusion: “Technology proficiency” is found pertinently fruitful. It should be included as a definitive requirement and a distinct strategic plan worldwide. Modern curriculum development is proposed (i) Educational goals and objectives as the proposed Conceptual framework “Technology proficiency” model (ii) Instructional strategies ‘Five Bs’ (iii) Implementation ‘Five Ms’.
Keywords: assessment, treatment, monitoring, prevention, professional standards, curriculum
Plain Language Summary
New technologies for understanding diseases, diagnosis, and treatment are widely available and revolutionizing medical practice. All doctors need to be in tune with the times. Thus, a need for exploring ‘technology proficiency’ as a distinct competency in medical teaching worldwide. We have aimed at assessment of usefulness of ‘technology proficiency’ and to advance its implementation, if found useful. Our methods for this included (i) search of authentic medical literature of best quality with rigorous assessment (ii) analysis of worldwide statutory medical institutions guidelines. Only last five years literature was searched as technology is fast advancing, and old becomes obsolete sooner than later. All this is done in a conceptual framework of proposed ‘TP’ model, encompassing all components of medical practice comprehensively and classified into five categories (a) proper assessment (b) pertinent treatment (c) progress monitoring (d) prevention applications (e) professional standards. We find ‘technology proficiency’ pertinently fruitful based on literature analysis. The worldwide medical institutions guidelines studied suggest need of it’s inclusion in medical education. This should be done as a definite and distinct strategic plan. Benefits and risks need to be balanced for success with safety. We recommend that health professional education for ‘technology proficiency’ should include only those which have passed rigorous health technology assessment as prescribed by the World Health Organization. Our proposed model of ‘technology proficiency’ for modernizing medical curricula for health care covers all aspects, for holistic health of highest standards. Worldwide competency sophistication will result in best care that is futuristic and favourable.
Introduction
Machines taking over men is not new. Machines sophisticated in the art and science of medicine will soon be available for many. New technologies for understanding diseases, diagnosis, and treatment are widely available and revolutionizing the way we practice. It becomes imperative that all doctors should be competent in their use for best practices.
The opening remark in the coveted Harrison's Principles of Internal Medicine is
The practice of medicine has changed in significant ways, The advent of molecular genetics, sophisticated new imaging techniques, robotics, and advances in bioinformatics and information technology have contributed to an explosion of scientific information that has changed fundamentally the way physicians, define, diagnose, treat, and attempt to prevent disease.1
All doctors need to be in tune with the times. This is further justifiably required with new disciplines improving healthcare – The Artificial Intelligence, the Machine Learning, the Data Analytics, the Computational Biology, etc. All these are advancing at an accelerated pace with applications professional in healthcare.
Similarly, the impact of technology in surgery has been phenomenal and best summarised in the Sabiston Textbook of Surgery:
The introduction of digitization, miniaturization, improved optics, novel imaging techniques, and computerized information systems in the operating room have made a dramatic change in surgical care over the past 25 years.2
The results of technology along with other excellence is beautifully summarised by the World Health Organization (WHO) in its “Japan Health System Review” as
Thanks to the overall effectiveness of the health system, socio-economic development and advances in technology, Japan has enjoyed increased life expectancy for many years.3
Importance
The global population is increasing rapidly, and the number of people aged ≥60 years is expected to double by 2050.4,5 A potential shortage of health care professionals is likely.6 Technology is a possible answer, increasing the efficiency and effectiveness of healthcare by doctors.
Digital technologies are now integral to daily life. Digital health can help make health systems more efficient and sustainable, enabling them to deliver good quality, affordable and equitable care. There is immense scope for use of digital health solutions.7 For this utilization, technology proficiency in medical education needs to be explored.
The WHO Global Observatory for eHealth, describing eHealth as the use of Information and Communication Technologies (ICT) for health, commented that it is recognised as one of the most rapidly growing areas in health today.8 Health science education should keep pace with the developments. Weighing pros and cons of advances judiciously is necessary.
Curriculum Development for Medical Education is important. The generic approaches to curriculum development set forth by eminent medical educationists advocated the linking of curricula to health care needs.9 Working modification in the modern world requires incorporating all modalities available for advancing health care, including technology.
The Medical Council of India (MCI), in its national meet on implementation of reforms in undergraduate and postgraduate medical education “Vision 2015”, had envisioned:
Ensure that community requirements and advancing medical technology are main streamed on an ongoing basis across disciplines.10
However, the pace of advances in technology suggests the need for advanced professionalism. “Technology proficiency” should be explored as a distinct competency in all medical teaching worldwide. An assessment of worldwide worthiness is imperative.
Methods
Aim
Assessment of “Technology proficiency” is required by all medical graduates to advance its implementation, if found useful.
Conceptual Framework
Conceptual frameworks represent ways of thinking about a problem or a study, or ways of representing how complex things work. Conceptual frameworks can come from theories, models or best practices.11
Technology is permeating all aspects of health care, hence the need for a comprehensive multi-faceted perspective and a model. We propose a Technology Proficiency model comprising five categories (Figure 1):
- Technology for proper assessment
- Technology for pertinent treatment
- Technology for progress monitoring
- Technology for prevention applications
- Technology for professional standards
 |
Figure 1 “Technology proficiency” model. |
Evidence and Guidelines Analysis
Proper perspective presentation requires study of latest systematic reviews and meta-analysis for trends and statutory medical institutions guidelines for advancements.
Systematic Reviews and Meta-Analysis
A search of the literature was performed using MedLine & Cochrane Central Register of Controlled Trials databases for systematic reviews and meta-analysis articles published in the last five years. Only last five years literature was searched as technology is fast advancing, and old becomes obsolete sooner than later. Keyword used in search was “technology”. Only systematic reviews and meta-analysis were included, as individual research papers on technology are vast and systematic reviews and meta-analysis filter these on quality, with rigorous assessment. A total of 646 papers were identified with this search (615 MedLine systematic reviews and meta-analysis and 31 Cochrane reviews), which question the use of technology in medical practice and are relevant as a role all medical graduates should play. The findings of the most relevant papers, practically suiting the roles of doctors, out of these are presented in Tables 1–5, classified as “Technology proficiency” model five categories.
 |
Table 1 Systematic Review Characteristics and Findings: Technology for Proper Assessment |
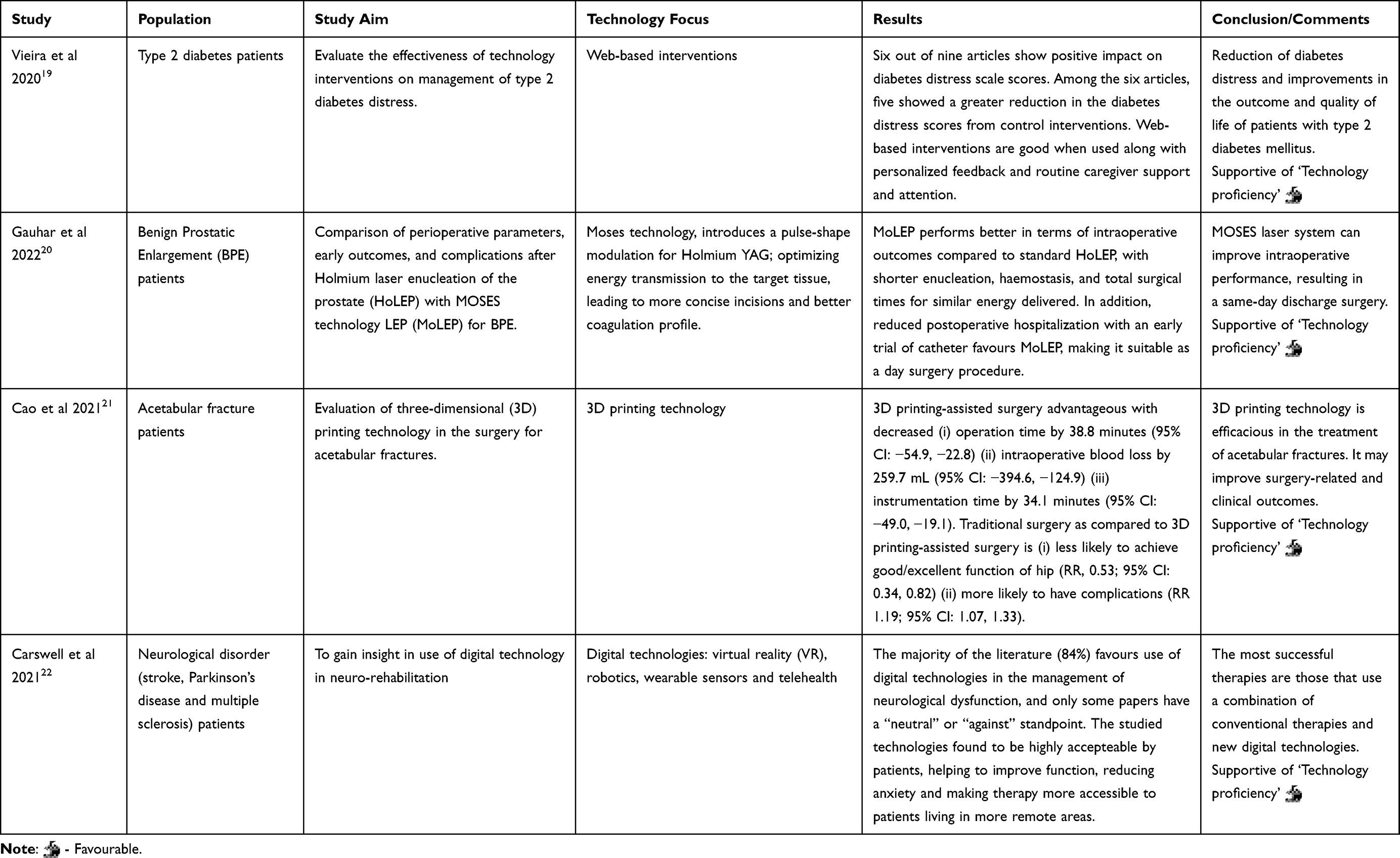 |
Table 2 Systematic Review Characteristics and Findings: Technology for Pertinent Treatment |
 |
Table 3 Systematic Review Characteristics and Findings: Technology for Progress Monitoring |
 |
Table 4 Systematic Review Characteristics and Findings: Technology for Preventive Applications |
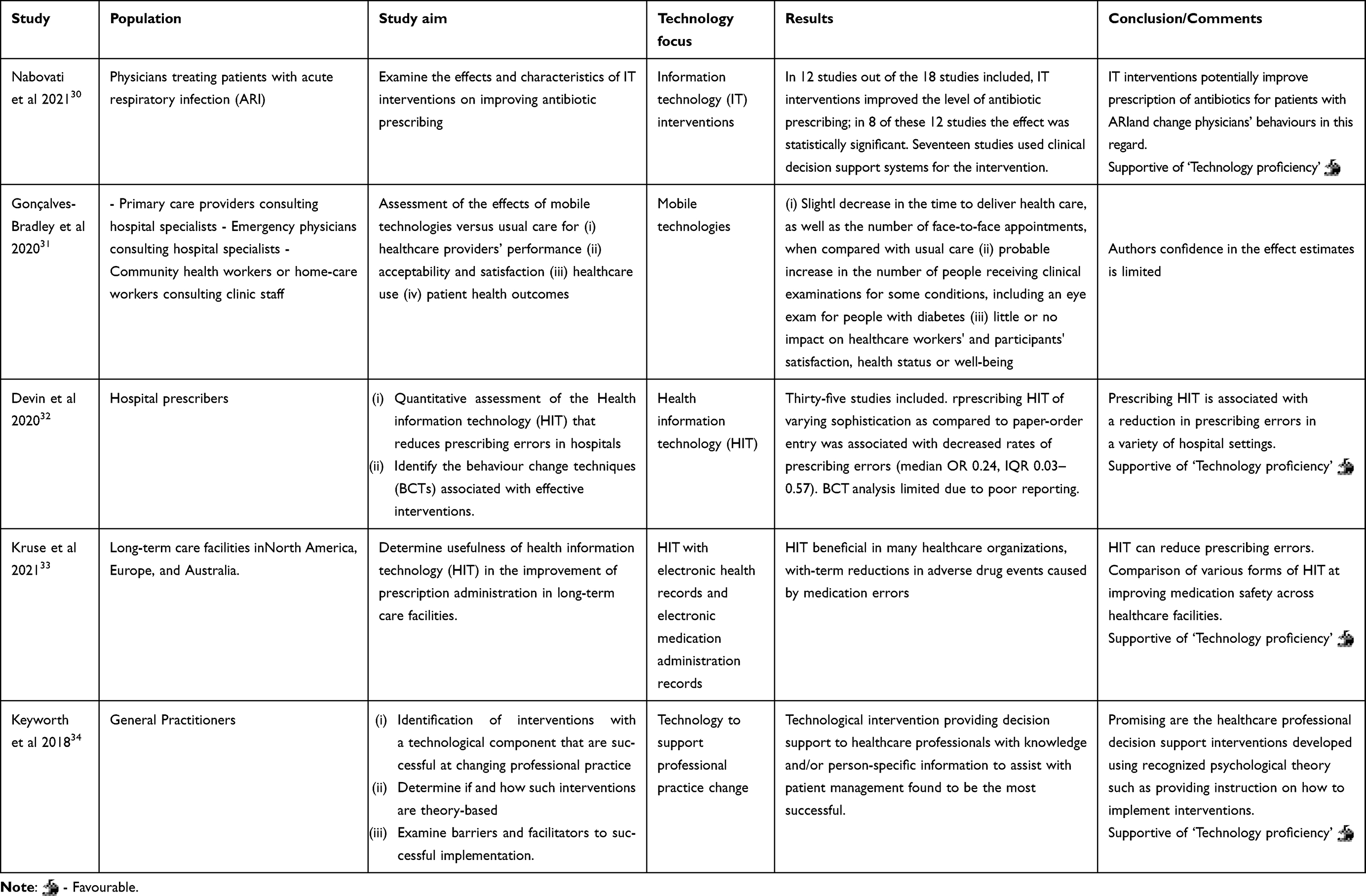 |
Table 5 Systematic Review Characteristics and Findings: Technology for Professional Standards |
The following inclusion criteria were used: 1) Published in peer-reviewed journals and 2) Related to medical professionals. Exclusion criterion was articles not directly relevant to the above five categories were not studied.
Worldwide Medical Institutions
Analysis of worldwide statutory medical institutions guidelines and make recommendations.
Results
(i) The findings and analysis of reviews studied are presented in Tables 1–5. Of the total 23 systematic studies and meta-analysis analysed, 18 have shown clear evidence for “Technology proficiency”. The remaining five have commented (a) Validation: Although promising, there is still a need for large-scale studies for validation.12 (b) Cost-effectiveness: More research on cost-effectiveness is needed to determine the potential for other diseases.13 (c) Clinical acceptance: Further studies are required for leading technologies to clinical acceptance.15 (d) Effectiveness: Stronger primary research on the effectiveness of contact tracing technologies is needed.27 (e) Confidence: Authors confidence in the effect estimates is limited.29
(ii) The findings of statutory medical institutions guidelines worldwide are given in Table 6.
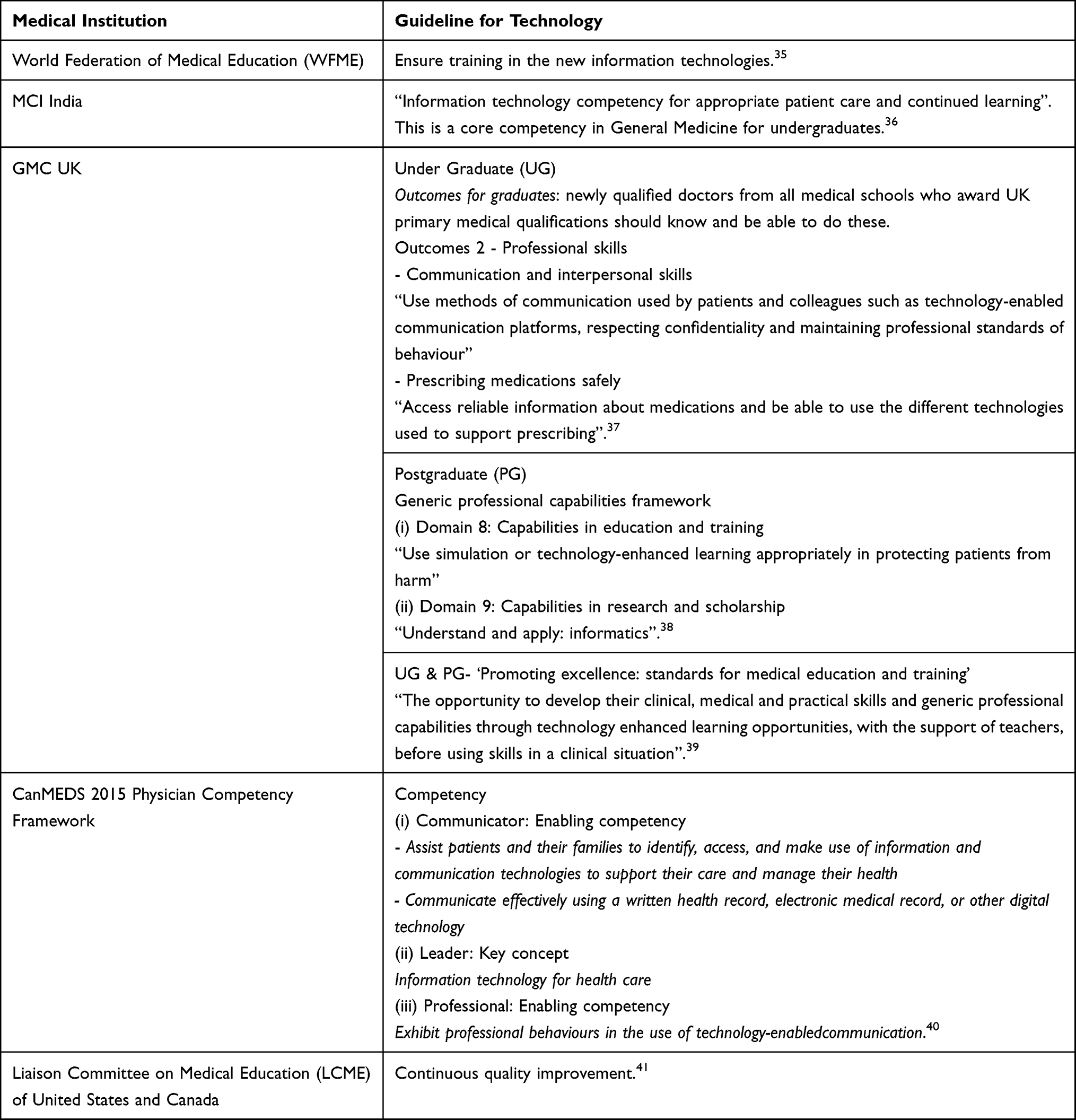 |
Table 6 Statutory Guidelines |
Discussion
Digital transformation of health care is supportive with technologies such as the virtual care, remote monitoring, smart wearables, platforms, tools enabling data exchange and storage and tools enabling remote data capture and the exchange of data and sharing of relevant information across the health ecosystem creating a continuum of care. Technologies enabling all this are Internet of Things, artificial intelligence, big data analytics, blockchain, machine learning, robotics, and advanced computing. All this has proven potential to enhance health outcomes by improving medical diagnosis, data-based treatment decisions, digital therapeutics, clinical trials, self-management of care and person-centred care as well as creating more evidence-based knowledge, skills and competence for professionals to support health care.42
We discuss all this for “Technology proficiency” model comprising five categories.
Technology for Proper Assessment
History taking, clinical examination, investigations are all aided by technology. Telemedicine has evolved for this basic purpose. It increases accessibility to medical services through the Information and Communication Technology (ICT) platform.18 Further face-to-face consultation remotely is possible with video calls, anytime, anywhere, without any waiting and thus useful in emergency also. Clinical examination is also aided. Auscultation with technology is not only possible but can provide diagnosis with standardized technology-based interpretation. This will also aid novice clinicians perfect their skills.
Video clips for paroxysmal disorders is an important case in point, aiding precise diagnosis. Paroxysmal disorders affecting humanity are plenty. Their precise characterization is important for specific management. Descriptions by eye witnesses can be varied and weird. A video recording done by a readily available mobile telephone can help in hitting the bull’s eye in the differential diagnosis list. For example, differentiating epileptic seizures from paroxysmal events that mimic epilepsy, including pseudo-seizures, can be done with a video clip interpretation by an expert.
Telemedicine
The prospect of remote healthcare services is one of the gold standards of telemedicine. It increases accessibility to medical services through the ICT platform.18 It is useful in conditions where distance is a critical factor, making available of experts from anywhere in the world, conveniently and economically.
Competency Tip
In a telephone consultation, it is important to pick up cues such as – pace, pauses, and change in voice intonation.43
Receptive and alert for advanced and real problem solving.
Technology for Pertinent Treatment
Selecting right medications, rightly planned surgeries, right counselling are all benefitted by technology. There is now good evidence that the routine use of ICT will contribute greatly to the use of real-time data to support clinical decisions.44
Computer-generated prescriptions have many benefits, including links to software that highlights risks from drugs or drug–drug combinations.45
3D printing is enabling precision surgery. Virtual surgical planning using information regarding patient anatomy and medical devices to be used in surgery increase confidence and knowledge before surgery for better outcomes. The digital plan is transferred to patient care by way of 3D printed templates, guides, or models.46
Artificial intelligence is making rapid strides. The principle of artificial intelligence is to make machines and programmed computer systems able to work like the human with capacity to learn, interpret, and develop resolutions to a particular issue. Artificial intelligence techniques include machine learning, deep learning, and natural language processing algorithms. AI applications are in diagnostics and making treatment recommendations. Medical professional should have a thorough understanding of AI applications in healthcare for (i) if things go wrong, understanding of what was being done will be a prerequisite for corrective steps and (ii) monitoring effects of AI for advancements. A current example is PAGER (proactive healthcare management), an application that improves patient treatment through making health care recommendations.
Competency Tip
Many trends in the delivery of health care tend to make medical care impersonal. This includes increasing reliance on technological advances and computerization.1 Personal touch with tactful professionalism should be part of “Technology proficiency”.
Compassion and humane understanding of whom you are treating and not only what you are treating is required and better done with doctor oversight.
Technology for Progress Monitoring
Monitoring is required, useful, and remotely done is advantageous. Technology is useful for all this. Fast data transmission for favourable timely actions is the ultimate aim. Tele-critical care (TCC) is useful.18 Remote monitoring is possible and technology provides timely alerts.
Competency Tip
Intricacies and involvement in follow-up for fruitfulness, Energised and simplified with technology for excellence and success.
Technology for Prevention Applications
eHealth
The three prominent but overlapping domains of eHealth are (1) Health in our hands: use eHealth technologies to monitor, track, and inform health for action by self; (2) Interacting for health: use digital technologies to enable health communication among practitioners and between health professionals and patients); and (3) Data enabling health: collecting, managing, and using health data.47 To maximize the likelihood of a successful eHealth intervention, healthcare professionals must acquaint themselves with the tool.48
Doctors have an essential role to play in all three. “Health in our Hands” has to be developed guided by doctors. Its practical and pertinent use has to be motivated by doctors. Proficiency in “Interacting for health” is required and the way forward. Actions on “Data enabling health” is doctors’ duty for larger impacts with prevention applications.
Internet of things (IoT) is a useful technology for preventive applications. Computer scientists stimulated IoT systems have the capability to provide public data on health matters accessible to the general population. Proficient doctors can guide actions based on the data for communities and populations.
Competency Tip
As a general rule, the most successful man in life is the man who has the best information. Health information provides reliable, relevant, up-to-date, adequate, timely, and reasonably complete information.49 Actions need to be advanced from these.
Data diligence for distinctive delight,
professional advice pragmatically advanced with technology right.
Technology for Professional Standards
Attainment, maintaining, and improvement of professional standards is all possible with technology. Technology proficiency will make these efficient. Progressive attitude required for professional standards is best summarised as
The challenges of contemporary surgical practice not only necessitate attention to the lessons of the past but also contemplation of the future. Reflection, self-assessment, and deliberation about what it means to be a good surgeon are essential.50
Reflection, self-assessment, and deliberation aid in attaining the highest professional standards. Reflection along with worldwide evidence and practices; self-assessment for improvements of best abilities and correction of weak areas; deliberations with colleagues, seniors, and juniors, at bedside, in classrooms, conference rooms, etc, lead to professional standards. Technology aids all these, subjectively and objectively.
Progress in technological applications for healthcare are contributing to advancements for high standards. Excellent examples for “Professional standards” are
Programmable Actual Leads
Pharmacogenomics research and precision medicine practice is making useful progress, and its utilization in prescribing is professional standards par excellent. Bringing the knowledge contained in biomedical literature to be of use practically on particular clinical situations and improving patient care requires “Technology proficiency”. GeneDive is a web application for pharmacogenomics researchers and precision medicine practitioners. It makes gene, disease, and drug interactions data easily accessible and usable. A superb advantage of this is that the interactive search-visualization loop enables relationship discoveries between diseases, genes, and drugs. These are most useful practically and might not be explicitly described in literature but are emergent from the source medical corpus and deductive reasoning.51
Pointing Advantageous Leads
Treatment regimens for many prevalent complex diseases are frequently ineffective. Technology is enabling in selection of best treatment choices. Han et al have developed a novel “NetPTP – a Network-based Personalized Treatment Prediction framework” for making personalized drug ranking. The framework captures and models measured drug effects from gene expression data and applies them to patient samples to generate personalized ranked treatment lists.52 The ability to use all these useful developments with “Technology proficiency” will ensure highest professional standards.
Progressive Advanced Leads
Clinical practices are dynamically evolving. Incorporating a continuous stream of new data is advantageous. It is required as historical data does not predict new therapeutics or diseases. Constantly updated latest data allows automated methods to rapidly detect and adapt to shifting practice changes and alert authors to dynamic areas in need of additional decision support. Automatic data-mining of clinical practice patterns from electronic health records (EHR) can enable prediction of future practices as a form of clinical decision support (CDS).53
Google Flu Trends has been shown to detect local flu activity more rapidly than conventional methods.54 Similar advances for many more affections are favourably possible for practical applications with “Technology proficiency”.
Precision at Large
Clinical wisdom of years and machine learning: Experience in clinical practice leads to the realization that patients with a shared diagnosis often fall into subsets that “look” the same. These often respond to similar treatment strategies. These are not described in standard texts and are usually recognized only after years of experience. The best clinical teachers convey these distinctions to their trainees.55 Machine learning simplifies these classifications and categorizations.
A great deal of knowledge and skill is required to practise as a doctor.56 Anything facilitating, simplifying, and contributing to this is a welcome step, and “Technology proficiency” will advance this.
Another example is gene-based supervised machine learning classification models. These have been widely used to (i) differentiate disease states, (ii) predict disease progression, and (iii) determine effective treatment options. However, for complex, heterogeneous diseases, these classifiers are limited by not being able to capture varying combinations of genes that lead to the same phenotype. Advancement to this is pathway-based classification. This overcomes these challenges by using robust, aggregate features to represent biological mechanisms. A recent work has used a novel pathway-based approach, PRObabilistic Pathway Score. It has been used successful to differentiate the two types of inflammatory bowel disease, ulcerative colitis (UC) and Crohn’s disease (CD).57 Future appears exciting for many more complexities, for diagnostic, prognostic, and therapeutic precision.
Competency Tip
Sayings of the great continue to inspire and motivate highest professional standards. Sir Stanley Davidson, the renowned educator and a particularly gifted teacher at the bedside, remains an inspiration. At the bedside he taught
Everything has to be questioned and explained.58
We have done exactly the same, questioned and explained the use of technology, at bedside and beyond. Overall, professional standards may be attained with
Practice, analyse, labour, improve, learn, advance, & perfect.
Medical Institutions Worldwide
Medical institutions, public and statutory, play an important role. The General Medical Council (GMC) UK helps protect patients and improve UK medical education and practice by supporting students, doctors, educators and healthcare providers. The Medical Council of India (MCI), now National Medical Commission of India, establishes uniform and high standards of medical education in India.
WHO along with World Federation of Medical Education (WFME) had importantly highlighted, way back in 2004, in its report on technical meeting on “Accreditation of medical education institutions”:
Training in the new information technologies in order to help doctors cope with the explosion in medical and scientific knowledge and technology, is expected to be ensured.35
Now, definitely with many advantageous and meritorious advancements, time has come to take definitive steps with “Technology proficiency” made an essential clinical competency worldwide.
MCI India has been proactive in training on technology. The MCI Competency-based Undergraduate curriculum for the Indian medical graduates requires the following core competency:
Demonstrate adequate knowledge and use of information technology that permits appropriate patient care and continued learning.36
The GMC UK views are to keep up to date, with medical education keeping up with developments in the technologies used to diagnose, treat and manage illness. It specifies UGs to have professional skills to be able to (i) use technology-enabled communication platforms as part of “Communication and interpersonal skills” outcome and (ii) use the different technologies used to support prescribing as part of “Prescribing medications safely” outcome.37 For PGs, it recommends in its “Generic professional capabilities framework” in information and technology domains for only learning and research.38 For both UGs & PGs in the “Promoting excellence: standards for medical education and training”, it recommends
The opportunity to develop their clinical, medical and practical skills and generic professional capabilities through technology enhanced learning opportunities, with the support of teachers, before using skills in a clinical situation.39
Soon, GMC UK should be including technology proficiency in actual practice, in its proven aspects, with all its advanced professional abilities, as an essential professional capability. Informatics applications should also be boosted, broadening its applications to evidence-based healthcare practices.
CanMEDS 2015 Physician Competency Framework has recommendations for use of digital technology for effective communication and IT for leadership. It envisions integrating eHealth throughout in all competencies.40 However, we recommend introducing “Technology proficiency” as a distinct competency based on the findings of this study.
The Liaison Committee on Medical Education (LCME) of the United States and Canada Element 1.1 requires medical schools to engage in strategic planning and continuous quality improvement (CQI).41 We suggest including “Technology proficiency” as a distinct strategic plan for continuous quality improvements.
Curriculum Development for Medical Education
Our positive findings should contribute to modern curriculum development, incorporating “Technology Proficiency”. Medical educators “benefit from learning a practical, generic, and timeless approach to curriculum development that can address today’s as well as tomorrow’s needs”59
The six-step approach to curriculum development proposed by Kern et al is very useful and the best.9 It represents a model comprising a series of components that were derived overall from systems theory applied to curriculum development.11 The detailed application based on this for “Technology Proficiency” is given in Table 7.
 |
Table 7 Six-Step Approach to Curriculum Development |
Limitations
New interventions and technologies are constantly being developed and refined. Their impacts on health, and implications for health systems, are not always clear. This is an important limitation. However, the solution is also there, as health technology assessment (HTA). A systematic and multidisciplinary evaluation of the properties of health technologies and interventions covering both their direct and indirect consequences is done in HTA.64 This includes 1) Safety, 2) Clinical effectiveness, 3) Economic considerations, 4) Budget impact analysis, 5) Organization impact, 6) Equity issues, 7) Ethical issues, 8) Feasibility considerations, 9) Acceptability to health care providers, and 10) Acceptability to patients. Evidence-based medicine is best, and similarly HTA evidence-based use of technology needs to be promoted. Also, the World Health Assembly had resolved in 2014 for the promotion of HTA within national frameworks, including health professional education.65 Also, health professional education for “Technology proficiency” should include only those which have passed HTA.
Physicians have an important role to play in ensuring that the powerful technologies and sources of new information, like epigenetics, microbiomics, metagenomics, metabolomics, exposomics, etc, are applied judiciously to patient care.1 “Technology proficiency” will ensure weighing pros and cons of advances judiciously.
In Lighter Vein
The philosophical dilemma “which came first: the chicken or the egg?” Progressive perspective is education for practice, practice for experience, and all for excellence.
A systematic review for “Factors determining the success and failure of eHealth interventions” has importantly pointed that for eHealth interventions to be successful, future research must ensure a positive impact in the quality of care, with particular attention given to improved diagnosis, clinical management, and patient-centered care.66 All these three attributes should be essential components of “Technology proficiency”.
It is important to recognize that while technology and innovations can enhance health service capabilities, human interaction remains a key element to patients’ well-being.67
Conclusion
“Technology proficiency” is need of the hour with technology progress in healthcare at a fast pace and pertinently found fruitful. Our proposed model of “Technology Proficiency” for Modern medical curricula for modern health care covers all aspects comprehensively. Results of systematic reviews and meta-analysis have provided the necessary evidence for excellence. It should be made a recommended requirement as a distinct strategic plan by all statutory Medical Institutions worldwide.
Fast pace technology progress, Present & future perfect favourable Technology proficiency for success.
Worldwide competency sophistication worth fullness is summarised as
Better competency standards, better technology proficiency, best care,
Futuristic & favourable.
Acknowledgments
The authors are thankful to the creators of all references cited as well as the formulators of all regulatory policies and guidelines.
Disclosure
The authors report no conflicts of interest in this work.
References
1. The Editors. The practice of medicine. In: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo D, Loscalzo J, editors. Harrison’s Principles of Internal Medicine.
2. Mueller CL, Fried GM. Emerging technology in surgery: informatics, robotics, electronics. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice.
3. Sakamoto H, Rahman M, Nomura S, et al. Japan Health System Review. New Delhi: World Health Organization, Regional Office for South- East Asia; 2018.
4. World Populations Prospects. United Nations; 2017. Available from: https://esa.un.org/unpd/wpp/Publications/Files/WPP2017_KeyFindings.pdf.
5. Global Aging Institute. About global aging. Available from: http://www.globalaginginstitute.org/about-gai/about-global-aging.html.
6. Rauwerdink A, Kasteleyn MJ, Chavannes NH, Schijven MP. Successes of and lessons from the first joint eHealth program of the Dutch university hospitals: evaluation study. J Med Internet Res. 2021;23(11):e25170. PMID: 34842536; PMCID: PMC8663485. doi:10.2196/25170
7. WHO Health Topics. Digital health; 2022. Available from: https://www.who.int/health-topics/digital-health.
8. World Health Organization. WHO Global Observatory for eHealth. Available from: https://www.who.int/observatories/global-observatory-for-eHealth.
9. Kern DE. Overview: a six-step approach to curriculum development. In: Thomas PA, Kern DE, Hughes MT, Chen BY, editors. Curriculum Development for Medical Education: A Six-Step Approach.
10. Medical council of India, Vision 2015; 2011:27. Available from: https://www.niti.gov.in/writereaddata/files/mci1.pdf.
11. Bordage G. Conceptual frameworks to illuminate and magnify. Med Educ. 2009;43(4):312–319. PMID: 19335572. doi:10.1111/j.1365-2923.2009.03295.x
12. Clark CCT, Bisi MC, Duncan MJ, Stagni R. Technology-based methods for the assessment of fine and gross motor skill in children: a systematic overview of available solutions and future steps for effective in-field use. J Sports Sci. 2021;39(11):1236–1276. PMID: 33588689. doi:10.1080/02640414.2020.1864984
13. Huang G, Wei X, Tang H, Bai F, Lin X, Xue D. A systematic review and meta-analysis of diagnostic performance and physicians’ perceptions of artificial intelligence (AI)-assisted CT diagnostic technology for the classification of pulmonary nodules. J Thorac Dis. 2021;13(8):4797–4811. PMID: 34527320; PMCID: PMC8411165. doi:10.21037/jtd-21-810
14. Nazarian S, Lam K, Darzi A, Ashrafian H. Diagnostic accuracy of smartwatches for the detection of cardiac arrhythmia: systematic review and meta-analysis. J Med Internet Res. 2021;23(8):e28974. PMID: 34448706; PMCID: PMC8433941. doi:10.2196/28974
15. Versluis A, Schnoor K, Chavannes NH, Talboom-Kamp EP. Direct access for patients to diagnostic testing and results using eHealth: systematic review on eHealth and diagnostics. J Med Internet Res. 2022;24(1):e29303. PMID: 35019848; PMCID: PMC8792777. doi:10.2196/29303
16. Bortolani S, Brusa C, Rolle E, et al. Technology outcome measures in neuromuscular disorders: a systematic review. Eur J Neurol. 2021. PMID: 34962693. doi:10.1111/ene.15235
17. Mennella C, Alloisio S, Novellino A, Viti F. Characteristics and applications of technology-aided hand functional assessment: a systematic review. Sensors. 2021;22(1):199. PMID: 35009742; PMCID: PMC8749695. doi:10.3390/s22010199
18. Alhasan M, Hasaneen M. Digital imaging, technologies and artificial intelligence applications during COVID-19 pandemic. Comput Med Imaging Graph. 2021;91:101933. PMID: 34082281; PMCID: PMC8123377. doi:10.1016/j.compmedimag.2021.101933
19. Vieira P, Kobayasi R, Pereira F, Zaia IM, Sasaki SU. Impact of technology use in type 2 diabetes distress: a systematic review. World J Diabetes. 2020;11(10):459–467. PMID: 33133393; PMCID: PMC7582117. doi:10.4239/wjd.v11.i10.459
20. Gauhar V, Gilling P, Pirola GM, et al. Does MOSES technology enhance the efficiency and outcomes of standard holmium laser enucleation of the prostate? results of a systematic review and meta-analysis of comparative studies. Eur Urol Focus. 2022:S2405–4569. PMID: 35105516. doi:10.1016/j.euf.2022.01.013
21. Cao J, Zhu H, Gao C. A systematic review and meta-analysis of 3D printing technology for the treatment of acetabular fractures. Biomed Res Int. 2021;2021:5018791. PMID: 34458367; PMCID: PMC8387177. doi:10.1155/2021/5018791
22. Carswell C, Rea PM. What the tech? The management of neurological dysfunction through the use of digital technology. Adv Exp Med Biol. 2021;1317:131–145. PMID: 33945135. doi:10.1007/978-3-030-61125-5_7
23. Dawes AJ, Lin AY, Varghese C, Russell MM, Lin AY. Mobile health technology for remote home monitoring after surgery: a meta-analysis. Br J Surg. 2021;108(11):1304–1314. PMID: 34661649. doi:10.1093/bjs/znab323
24. Doshi H, Hsia B, Shahani J, Mowrey W, Jariwala SP. Impact of technology-based interventions on patient-reported outcomes in asthma: a systematic review. J Allergy Clin Immunol Pract. 2021;9(6):2336–2341. PMID: 33548519. doi:10.1016/j.jaip.2021.01.027
25. Marthick M, McGregor D, Alison J, Cheema B, Dhillon H, Shaw T. Supportive care interventions for people with cancer assisted by digital technology: systematic review. J Med Internet Res. 2021;23(10):e24722. PMID: 34714246; PMCID: PMC8590193. doi:10.2196/24722
26. Jameel L, Valmaggia L, Barnes G, Cella M. mHealth technology to assess, monitor and treat daily functioning difficulties in people with severe mental illness: a systematic review. J Psychiatr Res. 2021;145:35–49. PMID: 34856524. doi:10.1016/j.jpsychires.2021.11.033
27. Botene PHR, de Azevedo AT, de Arruda Ignácio PS. Blockchain as an enabling technology in the COVID-19 pandemic: a systematic review. Health Technol. 2021;11(6):1369–1382. PMID: 34513552; PMCID: PMC8421063. doi:10.1007/s12553-021-00593-z
28. Navidad L, Padial-Ruz R, González MC. Nutrition, Physical activity, and new technology programs on obesity prevention in primary education: a systematic review. Int J Environ Res Public Health. 2021;18:10187. doi:10.3390/ijerph181910187
29. Anglemyer A, Moore THM, Parker L, et al. Digital contact tracing technologies in epidemics: a rapid review. Cochrane Database Syst Rev. 2020;(8):CD013699. doi:10.1002/14651858.CD013699
30. Nabovati E, Jeddi FR, Farrahi R, Anvari S. Information technology interventions to improve antibiotic prescribing for patients with acute respiratory infection: a systematic review. Clin Microbiol Infect. 2021;27(6):838–845. PMID: 33813115. doi:10.1016/j.cmi.2021.03.030
31. Gonçalves-Bradley DC, Maria J, Ricci-Cabello I, et al. Mobile technologies to support healthcare provider to healthcare provider communication and management of care. Cochrane Database Syst Rev. 2020;8:CD012927. doi:10.1002/14651858.CD012927
32. Devin J, Cleary BJ, Cullinan S. The impact of health information technology on prescribing errors in hospitals: a systematic review and behaviour change technique analysis. Syst Rev. 2020;9(1):275. PMID: 33272315; PMCID: PMC7716445. doi:10.1186/s13643-020-01510-7
33. Kruse CS, Mileski M, Syal R, MacNeil L, Chabarria E, Basch C. Evaluating the relationship between health information technology and safer-prescribing in the long-term care setting: a systematic review. Technol Health Care. 2021;29(1):1–14. PMID: 32894257. doi:10.3233/THC-202196
34. Keyworth C, Hart J, Armitage CJ, Tully MP. What maximizes the effectiveness and implementation of technology-based interventions to support healthcare professional practice? A systematic literature review. BMC Med Inform Decis Mak. 2018;18(1):93. PMID: 30404638; PMCID: PMC6223001. doi:10.1186/s12911-018-0661-3
35. WHO-WFME Task Force on Accreditation. Accreditation of medical education institutions: report of a technical meeting. Copenhagen, Denmark: Schaeffergården; 2004. Available from: https://www.who.int/hrh/documents/WFME_report.pdf.
36. Medical Council of India. Competency based undergraduate curriculum for the Indian medical graduate; 2018:104. Available from: https://www.nmc.org.in/wp-content/uploads/2020/01/UG-Curriculum-Vol-II.pdf.
37. General Medical Council. Outcomes for graduates; 2018. Available from: https://www.gmc-uk.org/education/standards-guidance-and-curricula/standards-and-outcomes/outcomes-for-graduates/outcomes-for-graduates.
38. General Medical Council. Generic professional capabilities framework. Available from: https://www.gmc-uk.org/-/media/documents/generic-professional-capabilities-framework--2109_pdf-70417127.pdf.
39. General Medical Council. Promoting excellence: standards for medical education and training. Available from: https://www.gmc-uk.org/-/media/documents/promoting-excellence-standards-for-medical-education-and-training-2109_pdf-61939165.pdf.
40. Frank JR, Snell L, Sherbino J. CanMEDS 2015 Physician Competency Framework. Ottawa: Royal College of Physicians and Surgeons of Canada; 2015.
41. Liaison Committee on Medical Education. Functions and structure of a medical school: standards for accreditation of medical education programs leading to the MD Degree. Available from: http://lcme.org/publications/.
42. World Health Organization. Global strategy on digital health 2020–2025. Geneva: World Health Organization; 2021. Available from: https://www.who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf.
43. Car J, Aziz S. Telephone consultations. BMJ. 2003;326:966–969. doi:10.1136/bmj.326.7396.966
44. Keane FBV, Mealy K. Human factors, patient safety, and quality improvement. In: Williams N, O’connell PR, McCaskie AW, editors. Bailey & Loves Short Practice of Surgery.
45. Trent RJ. Omics. In: Trent RJ, editor. Molecular Medicine.
46. Chepelev L, Wake N, Ryan J, et al. RSNA special interest group for 3D printing. radiological society of North America (RSNA) 3D printing Special Interest Group (SIG): guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print Med. 2018;4(1):11. PMID: 30649688; PMCID: PMC6251945. doi:10.1186/s41205-018-0030-y
47. Shaw T, McGregor D, Brunner M, Keep M, Janssen A, Barnet S. What is eHealth (6)? development of a conceptual model for eHealth: qualitative study with key informants. J Med Internet Res. 2017;19(10):e324. PMID: 29066429; PMCID: PMC5676031. doi:10.2196/jmir.8106
48. Hickson R, Talbert J, Thornbury WC, Perin NR, Goodin AJ. Online medical care: the current state of “eVisits” in acute primary care delivery. Telemed J E Health. 2015;21(2):90–96. doi:10.1089/tmj.2014.0022
49. Park K. Health information and basic medical statistics. In: Park’s Textbook of Preventive & Social Medicine.
50. Vaiani CE, Brody H. Ethics and professionalism in surgery. In: Townsend CM, Beauchamp JRD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice.
51. Wong M, Previde P, Cole J, et al. Search and visualization of gene-drug-disease interactions for pharmacogenomics and precision medicine research using GeneDive. J Biomed Inform. 2021;117:103732. PMID: 33737208. doi:10.1016/j.jbi.2021.103732
52. Han L, Sayyid ZN, Altman RB. Modeling drug response using network-based personalized treatment prediction (NetPTP) with applications to inflammatory bowel disease. PLoS Comput Biol. 2021;17(2):e1008631. PMID: 33544718; PMCID: PMC7891788. doi:10.1371/journal.pcbi.1008631
53. Chen JH, Goldstein MK, Asch SM, Altman RB. dynamically evolving clinical practices and implications for predicting medical decisions. Pac Symp Biocomput. 2016;21:195–206. PMID: 26776186; PMCID: PMC4719775. doi:10.1142/9789814749411_0019
54. Ginsberg J, Mohebbi MH, Patel RS, Brammer L, Smolinski MS, Brilliant L. Detecting influenza epidemics using search engine query data. Nature. 2009;457(7232):1012–1014. PMID: 19020500. doi:10.1038/nature07634
55. Altman RB, Ashley EA. Using “big data” to dissect clinical heterogeneity. Circulation. 2015;131(3):232–233. PMID: 25601948. doi:10.1161/CIRCULATIONAHA.114.014106
56. Cooper N, Cracknell AL. Clinical decision-making. In: Ralston SH, Penman ID, Strachan MWJ, Hobson RP, editors. Davidson’s Principles and Practice of Medicine.
57. Han L, Maciejewski M, Brockel C, et al. A probabilistic pathway score (PROPS) for classification with applications to inflammatory bowel disease. Bioinformatics. 2018;34(6):985–993. PMID: 29048458; PMCID: PMC5860179. doi:10.1093/bioinformatics/btx651
58. Ralston SH. Sir Stanley Davidson (1894–1981). In: Penman ID, Strachan MWJ, Hobson RP, editors. Davidson’s Principles and Practice of Medicine.
59. Thomas PA, Kern DE, Hughes MT, Chen BY. Preface. In: Thomas PA, Kern DE, Hughes MT, Chen BY, editors. Curriculum Development for Medical Education: A Six-Step Approach.
60. Simpson D, Fincher RM, Hafler JP, et al. Advancing educators and education by defining the components and evidence associated with educational scholarship. Med Educ. 2007;41(10):1002–1009. PMID: 17822412. doi:10.1111/j.1365-2923.2007.02844.x
61. Ericsson KA, Krampe RT, Tesch-Ro¨mer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100:363–406. doi:10.1037/0033-295X.100.3.363
62. Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(Suppl):70–81. doi:10.1097/00001888-200410001-00022
63. Kaufman DM. Applying educational theory in practice. In: Cantillon P, Wood D, editors. ABC of Learning and Teaching in Medicine.
64. WHO HTA 2022 WHO Health Topics. Health technology assessment; 2022. Available from: https://www.who.int/health-topics/health-technology-assessment.
65. World Health Assembly, 67. Health intervention and technology assessment in support of universal health coverage; 2014. Available from: https://apps.who.int/iris/handle/10665/162870.
66. Granja C, Janssen W, Johansen MA. Factors determining the success and failure of eHealth interventions: systematic review of the literature. J Med Internet Res. 2018;20(5):e10235. PMID: 29716883; PMCID: PMC5954232. doi:10.2196/10235
67. WHO 71st World Health Assembly; 2018. Geneva, Switzerland. Resolution WHA71. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_R7-en.pdf?ua=1.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Strategies to Improve Outcomes of Bullous Pemphigoid: A Comprehensive Review of Clinical Presentations, Diagnosis, and Patients’ Assessment
Ruggiero A, Megna M, Villani A, Comune R, Fabbrocini G, di Vico F
Clinical, Cosmetic and Investigational Dermatology 2022, 15:661-673
Published Date: 14 April 2022
Prevention and Treatment of Neuraxial Morphine-Induced Pruritus: A Scoping Review
Becker LM, Teunissen AJW, Koopman JSHA
Journal of Pain Research 2022, 15:1633-1645
Published Date: 4 June 2022
New Developments and Challenges in Antibody-Based Therapies for the Respiratory Syncytial Virus
Diethelm-Varela B, Soto JA, Riedel CA, Bueno SM, Kalergis AM
Infection and Drug Resistance 2023, 16:2061-2074
Published Date: 8 April 2023
Moral Injuries in Healthcare Workers: What Causes Them and What to Do About Them?
Rabin S, Kika N, Lamb D, Murphy D, AM Stevelink S, Williamson V, Wessely S, Greenberg N
Journal of Healthcare Leadership 2023, 15:153-160
Published Date: 16 August 2023
Managing Opioid Withdrawal Symptoms During the Fentanyl Crisis: A Review
Weber AN, Trebach J, Brenner MA, Thomas MM, Bormann NL
Substance Abuse and Rehabilitation 2024, 15:59-71
Published Date: 10 April 2024