Back to Journals » International Journal of Women's Health » Volume 18
Symptoms Experienced by Breast Cancer Patients Before, During and After Chemotherapy: A Systematic Review
Authors Cao Y, Lee K, Yusuf A, Chen ST, Dong X, Li L, Lim PY ![]()
Received 18 September 2025
Accepted for publication 14 January 2026
Published 27 March 2026 Volume 2026:18 568638
DOI https://doi.org/10.2147/IJWH.S568638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yang Cao,1,2 Khuan Lee,1 Azlina Yusuf,3 Seong Ting Chen,4 Xue Dong,2 Lin Li,1 Poh Ying Lim5
1Department of Nursing, Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, Serdang, Selangor, Malaysia; 2Department of Nursing, Changchun University of Chinese Medicine, Changchun, Jilin, People’s Republic of China; 3Nursing Program, School of Health Sciences, Health Campus, Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia; 4Division of Nutrition, Dietetics and Food Science, School of Health Sciences, IMU University, Bukit Jalil, Kuala Lumpur, Malaysia; 5Department of Community Health, Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, Serdang, Selangor, Malaysia
Correspondence: Poh Ying Lim, Email [email protected]
Introduction: Breast cancer is the most prevalent cancer among women worldwide. Chemotherapy remains a key element of treatment for a large proportion of breast cancer patients. Breast cancer patients undergoing chemotherapy often experience multiple symptoms that can impact their quality of life. This systematic review aimed to identify the symptoms experienced by breast cancer patients before, during and after chemotherapy treatment along with associated factors, to provide an evidence base for healthcare providers.
Methods: Five electronic databases were searched from January 2015 to September 2025 encompassing observational studies. Two researchers independently screened the studies and extracted data. The Standard Quality Assessment Criteria for Evaluating Primary Research Papers was used to evaluate the quality of included studies.
Results: Out of 5,588 records, 37 studies met the inclusion criteria. Majority of studies were conducted in Asia and the most common study type was cross-sectional studies (n=18, 48.6%). Anxiety, depression, chemotherapy-induced nausea and vomiting (CINV), fatigue and sleep problems were the most common symptoms observed in these studies. The factors reported were divided into non-modifiable factors (sociodemographic and disease related) and modifiable factors (physiological, psychological, lifestyle, nutritional and other related). Younger age was the most frequently reported risk factor for increased anxiety, depression, fatigue, nausea, and menopausal symptoms, followed by having children, greater number of chemotherapy cycles, higher BMI, lower performance status, and limited social support.
Conclusion: Breast cancer patients undergoing chemotherapy experience a variety of symptoms. These findings underscore the importance of routine symptom screening and baseline risk assessment to enable early identification of high-risk patients and implementation of targeted interventions to optimize quality of life. Future research should prioritize identifying high-risk populations and implementing targeted early preventive interventions to enhance patient quality of life.
Keywords: breast cancer, chemotherapy, symptoms, risk factors, systematic review
Introduction
Breast cancer (BC) was the most prevalent malignancy among women globally. In 2022, 2.3 million women worldwide were diagnosed with breast cancer, comprising 11.6% of all cancer cases.1 Notably, despite constituting a substantial global health burden, breast cancer related mortality represents merely 6.9% of cancer deaths.2,3 The latest clinical research data showed that under a standardized diagnosis and treatment system, the 5-year relative survival rate of breast cancer patients can reach 90% and the 10-year relative survival rate remains above 80%, gradually presenting the characteristics of “chronic disease” management.4
Adjuvant chemotherapy is an important treatment method for breast cancer patients. Neoadjuvant chemotherapy, administered prior to surgery to shrink tumors and improve surgical outcomes, is also a key approach in breast cancer treatment. Although chemotherapy can effectively eliminate malignant cells, it may also have an impact on normal healthy cells, thereby causing side effects and leading to various symptoms in patients during chemotherapy. These can have a negative impact on their quality of life.5
Despite increasing research attention on symptoms experienced by breast cancer patients undergoing chemotherapy, a comprehensive synthesis focusing on individual symptoms remains absent. Although So et al6 and Qi et al7 conducted a systematic review on symptom clusters during chemotherapy, they prioritized concurrent symptoms with shared underlying mechanisms while providing limited insight into the prevalence, severity, symptom changes, as well as demographic, clinical, and psychosocial predictors of individual symptoms. This systematic review fills these gaps by comprehensively appraising individual symptoms across the chemotherapy stages, thereby establishing a robust evidence foundation for precision symptom assessment, timely intervention, and the development of tailored supportive care strategies to improve patient-reported outcomes.
The primary aim of this systematic review is to identify the symptoms experienced by breast cancer patients before, during, and after chemotherapy. The secondary aim is to identify risk factors associated with these symptoms among breast cancer patients. Specifically, this review addresses the following research questions: (1) What symptoms do breast cancer patients experience across chemotherapy stages? (2) What factors are associated with these symptoms among breast cancer patients?
Materials and Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines8 and was registered in PROSPERO (registration number: CRD42024545463) to ensure transparency and minimize duplication.
Search Strategy
A comprehensive literature search was performed across five databases (PubMed, Scopus, Cochrane Library, Embase and ProQuest), from January 2015 to September 2025. No date restrictions were applied initially, but studies published before 2015 were excluded during screening to focus on contemporary chemotherapy regimens. The search strategy combined Medical Subject Headings (MeSH) terms with free-text keywords. Search strategy in PubMed as shown in Table S1. In addition, a hand-search was conducted on the reference lists of related systematic reviews to identify additional relevant studies, thereby reducing publication bias.
Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria: (1) involved adult patients (≥18 years old) diagnosed with breast cancer who received chemotherapy as part of treatment; (2) regardless of breast cancer stage, encompassing both early-stage and metastatic cases; (3) reported symptoms experienced before, during or after chemotherapy; (4) examined factors associated with these symptoms; (5) original research studies, including observational studies (such as cohort, cross-sectional and case-control studies); (6) studies with English version.
Exclusion criteria included: (1) studies focusing solely on non-chemotherapy treatments (such as surgery, radiotherapy alone); (2) pediatric or adolescent populations; (3) studies not reporting symptoms across chemotherapy stages (before, during, and after) or lacking data on associated factors; (4) other type of publications, such as books, government reports, and short communications that lack original data; (5) study that is not available in full text; (6) duplicate publications.
Study Selection
All retrieved records were imported into EndNote for deduplication. Two researchers (YC and LL) screened titles and abstracts for relevance, followed by full-text assessment according to the inclusion and exclusion criteria. Disagreements were resolved through discussion or consultation with a third reviewer (PYL). The selection process was documented using a PRISMA flow diagram.
Data Extraction
Data were extracted independently by two researchers (YC and LL) using a standardized extraction form. Extracted information included: study characteristics (author, year, country, study population, sample size, time of data collection, total time point and study design); symptoms reported at each stage (before, during, and after chemotherapy); prevalence or severity score of symptoms and instrument used for symptom assessment; factors associated with symptoms. Any discrepancies in extraction were resolved by consensus.
Quality Assessment
The quality of the included studies was assessed using The Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields developed by Kmet et al,9 which is suitable for evaluating studies of various designs. The specific items assessed are presented in Table S2. This tool comprises 14 items scored independently (2 points for “yes”, 1 for “partial”, and 0 for “no”), with the total score calculated as a percentage of applicable items. The studies were categorized according to Lee et al’s guidelines,10 with classifications ranging from limited (50%) to adequate (50–70%), good (70–80%) and strong (80%). Two researchers (YC and LL) independently assessed the quality of the included studies and crosschecked their evaluation results. Discussed the inconsistencies with the third reviewer (PYL) until a consensus reached.
Results
Study Selection
A total of 5,588 records were initially identified through systematic literature searches across five electronic databases. Of these, 526 duplicates were removed, leaving 5,062 records for title and abstract screening. Following this, 117 records were selected for full-text evaluation. Records were excluded for the following reasons: six that lacked full-text availability, four that were not published in English, 18 that involved irrelevant study populations, 15 that did not report symptom prevalence or scores, 10 that did not report associated factors, 13 that were not observational studies and 14 that were not related to chemotherapy. Ultimately, 37 studies met the inclusion criteria and were included in the review, as illustrated in Figure 1.
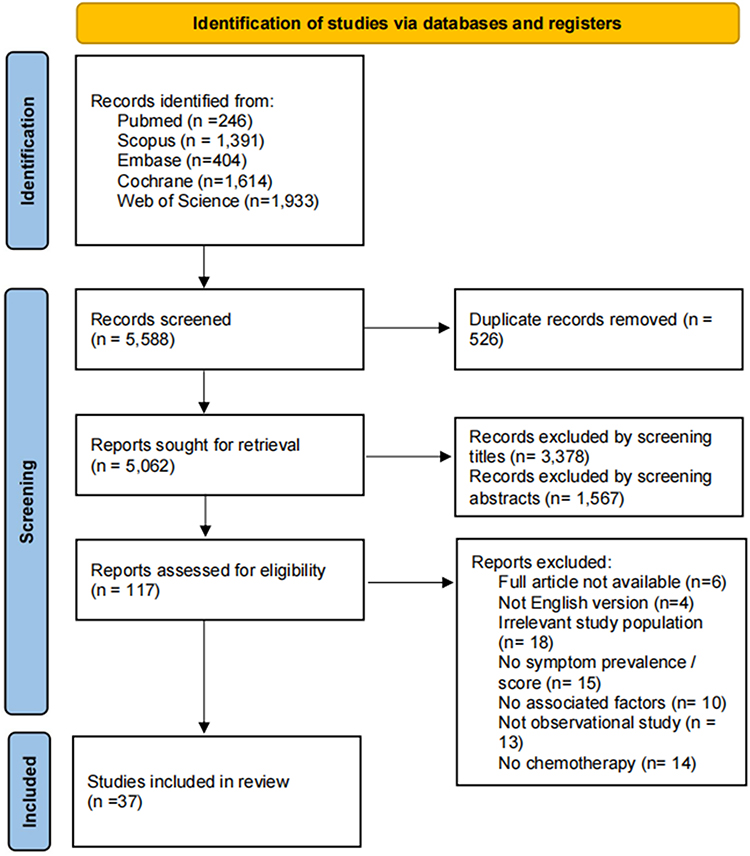 |
Figure 1 Flowchart of the systematic review process. |
Quality of Studies
The present review encompassed exclusively observational studies. Items 5 to 7 and item 9 are applicable solely to randomized controlled trials (RCTs) and were therefore designated as “NA (not applicable).” Item 12 pertains only to specific types of cohort studies, for studies to which it is not applicable, it was marked as “NA.” The quality scores of the included studies ranged from 11 to 19, with corresponding percentage scores ranging from 61.1% to 95.0%. Thirty-one studies were assessed as strong, five studies were rated as good, one study was considered adequate and no study was assessed as limited. The quality assessment of the included studies is shown in Table 1.
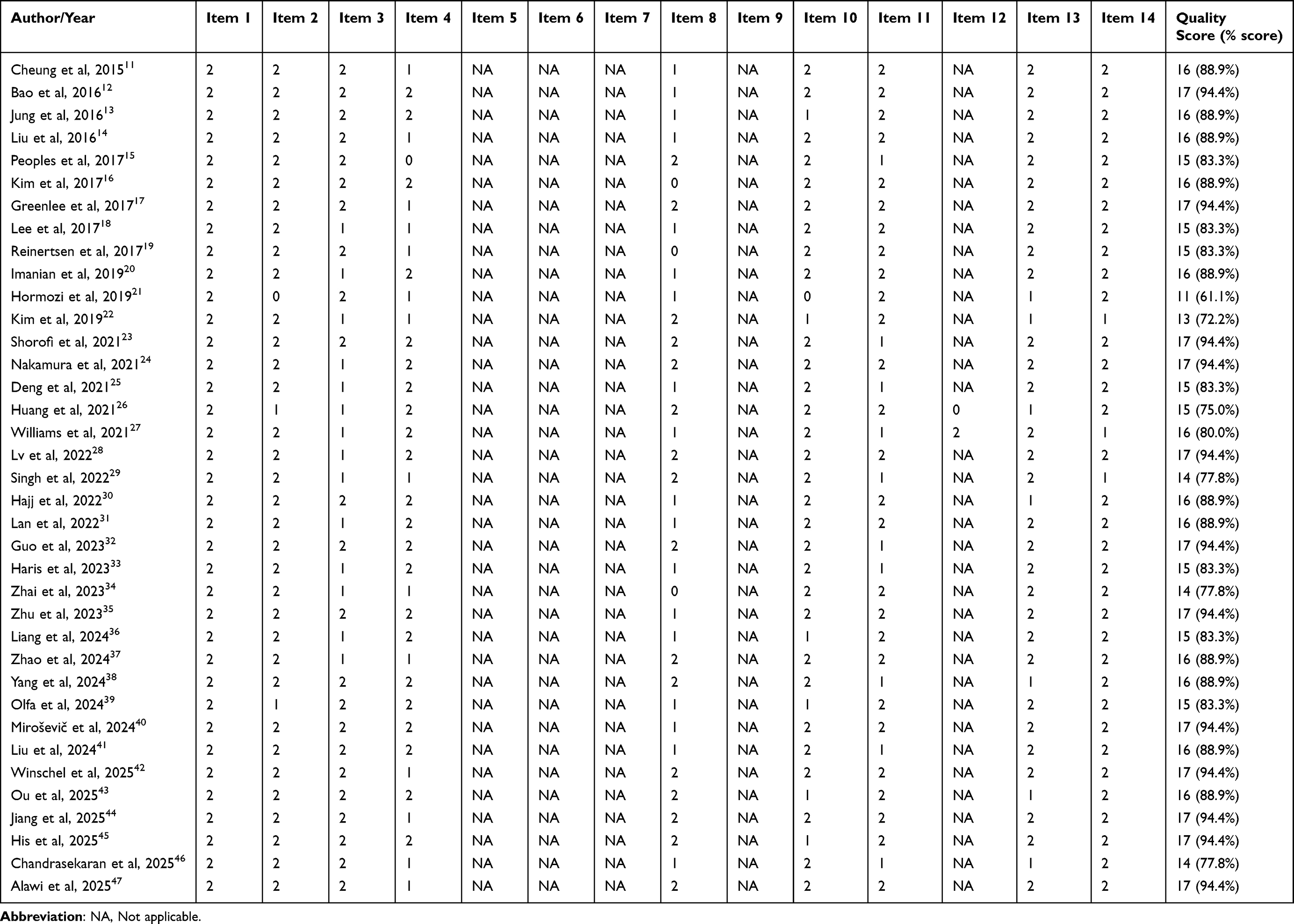 |
Table 1 The Result of Quality Assessment of the Included Studies (n=37) |
Study Characteristics
A total of 37 studies met the inclusion criteria and were incorporated into this systematic review. These studies were published between 2015 and 2025, with the majority (n=25) appearing from 2021 onward, reflecting a growing interest in symptom experiences among breast cancer patients undergoing chemotherapy. Geographically, studies originated predominantly from Asia (n=26, 70.3%),11,13,14,16,18,20–23,25,26,28,30–38,41,43,44,46,47 including China (n=12),14,26,28,31,32,34–37,41,43,44 Korea (n=5),13,16,18,22,38 Iran (n=3),20,21,23 India (n=1),46 Indonesia (n=1),33 Singapore (n=1),11 The Sultanate of Oman (n=1),47 Lebanon (n=1),30 and Taiwan (n=1).25 North America contributed seven studies (18.9%), all from the United States.12,15,17,24,27,29,42 Europe accounted for three studies (8.1%, France, Norway and Slovenia),19,40,45 while one from Africa (2.7%, Tunisia),39 and other regions had minimal representation.
The included studies encompassed a total of 11,461 participants, with sample sizes ranging from 30 to 1,237 (median=256). The majority of studies focused on patients with early-stage or non-metastatic breast cancer undergoing adjuvant or neoadjuvant chemotherapy, often involving taxane-based or anthracycline-based chemotherapy regimens. Study designs varied, with cross-sectional studies being the most common (n=18, 48.6%),12,16,20,23,25,29,30,32,33,35,37–42,46,47 followed by prospective observational studies (n=8, 21.6%),13–15,18,24,28,34,36 as well as cohort studies (n=6, 16.2%),11,17,19,26,27,31 longitudinal studies (n=3, 8.1%),21,22,45 and other designs such as case-control (n=1, 2.7%)43 or retrospective observational studies (n=1, 2.7%).44 Data collection timing relative to chemotherapy included assessments before treatment (n=10),11,13,19,21,22,24,27,28,31,35 during cycles (n=32),11–21,23–26,28–39,41,43,44,46,47 and after completion (n=13).11,12,17,19,21,22,27,31,35,38,40,42,45 The measurement time points of these studies ranged from one to five.
Symptom assessment utilized a diverse array of validated instruments. The common instruments included Pittsburgh Sleep Quality Index (PSQI, n=4),20,22,23,35 Brief Fatigue Inventory (BFI, n=3),15,20,25 Hospital Anxiety and Depression Scale (HADS, n=3)28,31,40 and Functional Assessment of Cancer Therapy-Cognitive Function (FACT-Cog, n=2).11,41 Some studies relied on medical records,44,45 WHO grades,39,43 and physicians’ judgments for the measurement of symptoms.46 Four studies reported multiple symptoms.33,37,39,47 Symptoms measured were multifaceted, with anxiety (n=8),22,24,27,28,31,32,40,47 depression (n=8),22–24,28,31,32,37,40 chemotherapy-induced nausea and vomiting (CINV, n=7),13,14,18,26,29,39,44 fatigue (n=7),15,19,20,25,27,30,47 and sleep problems (sleep disturbance and drowsiness, n=6),20,22,23,35,37,47 which were the top five symptoms reported. Characteristics of included studies are shown in Table 2.
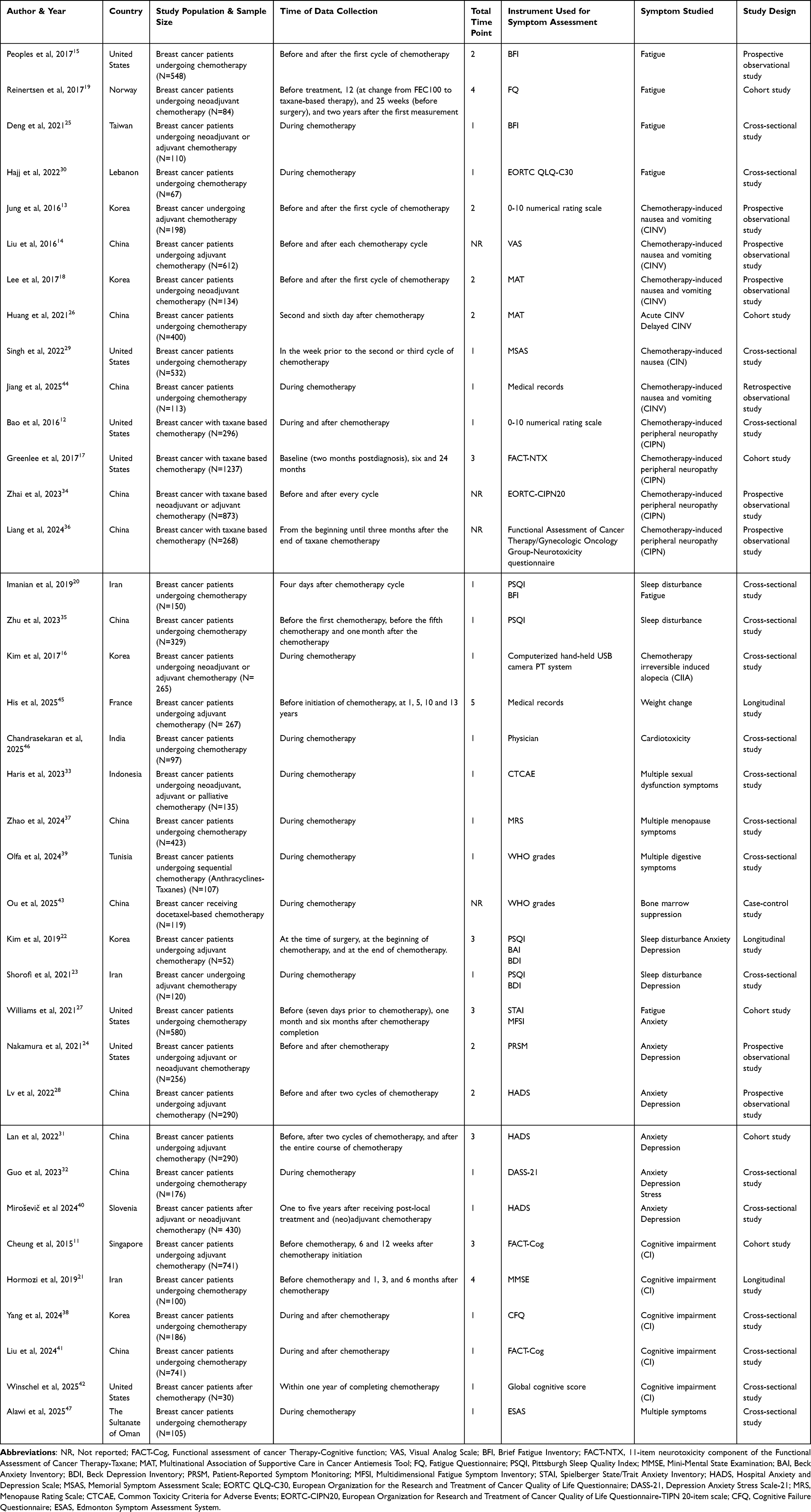 |
Table 2 Characteristics of Included Studies (n=37) |
Prevalence and Severity of Symptoms
Symptoms reported in the 37 studies can be classified into physical (such as fatigue, chemotherapy-induced nausea and vomiting [CINV], chemotherapy-induced peripheral neuropathy [CIPN], sleep problems, alopecia, digestive issues, menopausal/sexual symptoms, bone marrow suppression, weight change, and cardiotoxicity), psychological (such as anxiety, depression, and stress), and cognitive domains (such as cognitive impairment [CI]). Due to heterogeneity in timing, regimens and reporting formats, meta-analysis was not performed. Instead, a systematic review was employed, focusing on prevalence and severity scores.
Anxiety was reported in eight studies.22,24,27,28,31,32,40,47 Before chemotherapy, the prevalence ranged from 21.0% to 35.0% and severity scores ranged from 6.00 ± 3.60 to 36.00 ± 10.16. During treatment, the prevalence varied from 21.9% to 60.2%, while the scores ranged from 1.76 ± 2.51 to 10.64 ± 8.06, indicating a peak during the treatment period. After chemotherapy, the prevalence and severity scores varied from 29.3% to 34.2% and from 5.80 ± 3.60 to 32.91 ± 10.62, respectively.
Depression was reported in eight studies.22–24,28,31,32,37,40 Pre-chemotherapy prevalence was ranged from 12.0% to 20.0% and severity scores ranged from 4.00 ± 3.60 to 9.86 ± 8.61. During chemotherapy, the prevalence and scores ranged from 25.2% to 52.3% and from 0.80 ± 1.00 to 13.40 ± 6.51, respectively. This indicated moderate escalation. Post-treatment, the prevalence ranged from 24.8% to 30.2% and severity scores ranged from 4.90 ± 3.60 to 8.97 ± 7.31.
CINV (including nausea/vomiting, acute/delayed) was assessed in seven studies.13,14,18,26,29,39,44 Before chemotherapy, limited data from one study showed low prevalence, with nausea at 11.1% and vomiting at 13.6%. During treatment, the prevalence was notably higher. The overall prevalence ranging from 23.0% to 92.2% and no severity scores were reported. After chemotherapy, no specific data for CINV were available.
Fatigue was one of the most commonly reported symptoms, assessed in seven studies.15,19,20,25,27,30,47 Before chemotherapy, prevalence was reported in one study at 8.0%, with a severity score of 9.42 ± 8.31 in another, indicating generally low baseline levels. During chemotherapy, prevalence ranged from 11.0% to 75.0%, with scores varying from 2.50 ± 2.61 (for tiredness) to 5.59 ± 1.67, reflecting moderate severity. After chemotherapy, the prevalence ranging from 13.0% to 36.0% and severity scores ranging from 9.19 ± 9.05 to 17.70 ± 8.83, respectively. This indicates an ongoing burden in a subset of patients.
Sleep problems, encompassing sleep disturbance and drowsiness, were reported in six studies.20,22,23,35,37,47 Before chemotherapy, prevalence was reported in one study at 27.0%, with severity scores between 5.66 ± 3.21 and 6.38 ± 4.24 in another, indicating mild to moderate sleep problems at baseline. During chemotherapy, prevalence increased, ranging from 27.6% to 50.8%, with severity scores from 1.05 ± 1.00 to 14.06 ± 3.06, reflecting a significant escalation in sleep problems. One study specifically reported drowsiness during chemotherapy, with a prevalence of 27.6% and a severity score of 1.95 ± 2.21, suggesting a related but distinct manifestation of sleep problems. Post-chemotherapy, prevalence was 39.2% and severity score was 6.21 ± 3.70, indicating persistent sleep issues in a notable proportion of patients.
Cognitive impairment (CI, n=5) was reported with a prevalence of 18.2% in one study and a severity score of 25.02 ± 4.02 in another before chemotherapy.11,21 The prevalence reported was 23.6% in one study, with severity scores from 23.60 ± 16.32 to 97.21 ± 23.75 during treatment, highlighting worsening cognitive function during treatment.11,21,38,41 After chemotherapy, prevalence was reported 15.0% in one study, with the scores of 0.15 ± 0.54 to 23.60 ± 16.32, implying the impact on some patients is still ongoing.11,21,38,42
Chemotherapy-induced peripheral neuropathy (CIPN, n=4) showed the prevalence ranging from 31.7% to 58.4% during chemotherapy, with severity scores ranging from 24.80 ± 4.80 to 39.50 ± 5.20.12,17,34,36 Post-chemotherapy, the scores were 33.80 ± 8.30 to 35.50 ± 7.70, suggesting persistent effects.12,17
Other symptoms, including stress, permanent chemotherapy-induced alopecia, menopausal symptoms, sexual dysfunction, digestive issues, bone marrow suppression, cardiotoxicity and weight change, were less consistently reported but typically emerged or intensified during chemotherapy, with some persisting post-treatment. Prevalence and severity scores of symptoms included in the study are shown in Table 3.
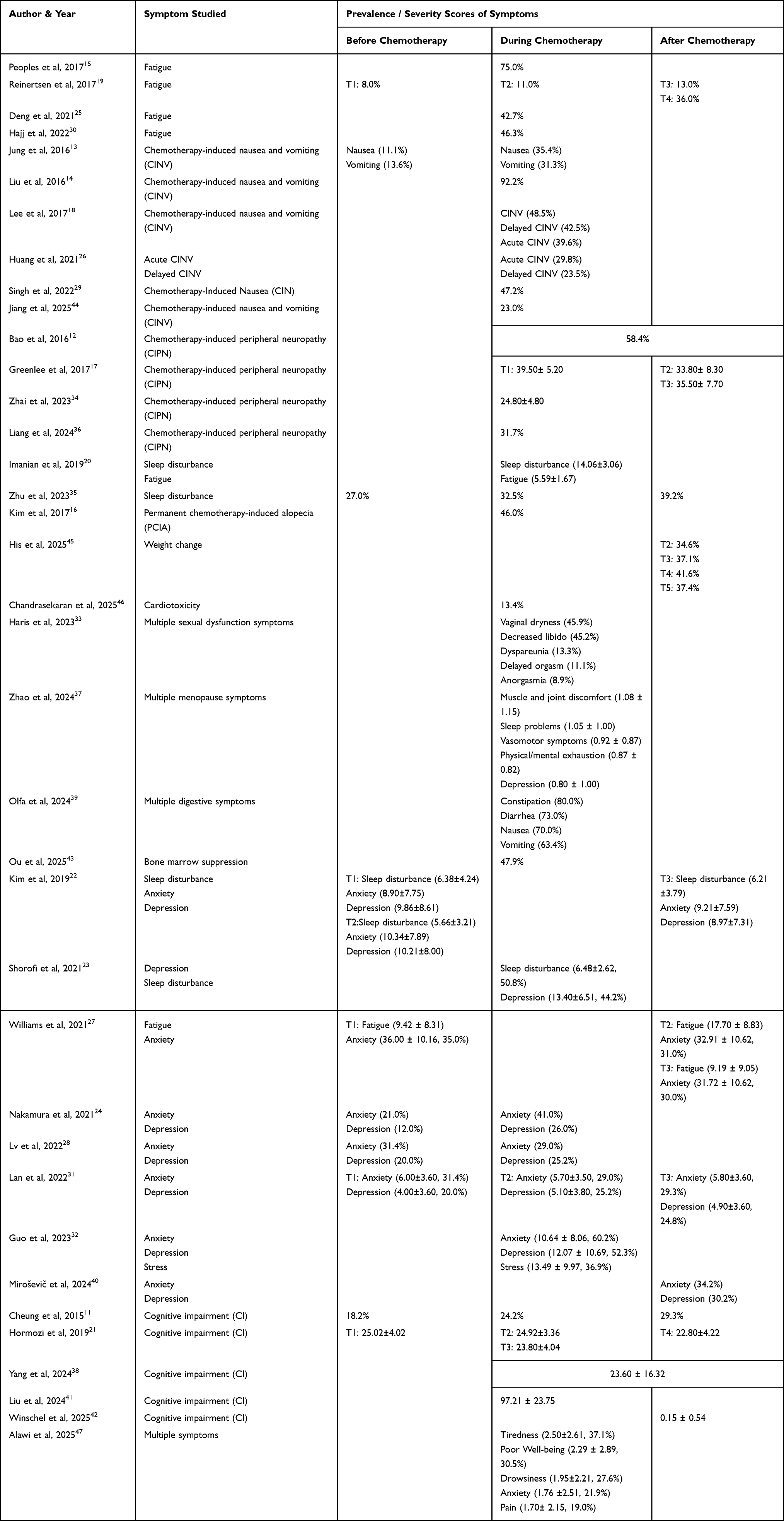 |
Table 3 Prevalence and Severity Scores of Symptoms Included in the Study (n=37) |
Factors Associated with Each Symptom
All factors associated with symptoms were divided into seven categories, including sociodemographic factors, disease related factors, physiological factors, psychological factors, lifestyle factors, nutritional factors and other related factors. Based on the seven categories of reported factors, associated factors for the reported symptoms were categorized into non-modifiable (sociodemographic and disease related) and modifiable (physiological, psychological, lifestyle, nutritional, and other related factors) domains, as detailed in Table 4. Several factors recurred across multiple symptoms. Younger age was associated with increased anxiety, depression, fatigue, nausea, and menopausal symptoms.15,23,29,37,40 Having children was associated with increased fatigue, pain, and anxiety.31,47 A higher number of chemotherapy cycles was associated with worsened fatigue, CINV, sleep disturbances, CIPN, menopausal symptoms, sexual dysfunction, and CI.23,25,30,41,44 Higher body mass index (BMI) was associated with increased fatigue and CIPN.27,36 Lower Karnofsky Performance Status (KPS) score were associated with increased nausea, anxiety, and depression,24,29 whereas limited social support was associated with heightened anxiety and depression.24,31,40 These findings underscore the complex interplay between patient characteristics and symptom burden, highlighting the importance of targeted risk stratification and personalized symptom management in clinical practice.
 |
Table 4 Factors Associated with Each Symptom |
Discussion
This systematic review of 37 studies synthesizes evidence on the dynamic symptom burden experienced by breast cancer patients across chemotherapy stages. The included studies encompassed both early-stage and metastatic disease, as well as adjuvant, neoadjuvant, and palliative treatment settings, thereby providing healthcare providers with a comprehensive overview of multiple symptoms prevalence, severity, and duration across chemotherapy phases. Our findings reveal that symptoms are generally mild or infrequent at baseline, escalate significantly during chemotherapy phase and often persist into the post-treatment. The most commonly reported symptoms including anxiety, depression, CINV, fatigue and sleep problems, which align with established symptom clusters among breast cancer chemotherapy patients, such as fatigue-sleep disturbance cluster and psychological cluster.7 Associated factors can be classified into non-modifiable and modifiable factors. This review enables healthcare providers to more accurately identify high-risk patient groups prone to severe or persistent symptoms. Ultimately, these insights can guide the development of personalized, evidence-based interventions, such as tailored symptom management protocols, supportive care strategies and multidisciplinary approaches, thereby enhancing treatment adherence, improving quality of life and reducing long-term morbidity risks in breast cancer survivors.
The prevalence of common symptoms during chemotherapy was notably high, with fatigue affecting up to 75.0% of patients, sleep problems up to 50.8%, CINV up to 92.2%, and psychological symptoms like anxiety and depression ranging from 21.9% to 60.2% and 25.2% to 52.3%, respectively. These findings align with previous studies, which identify fatigue as one of the most prevalent and impactful symptoms among cancer patients, persisting in 30% to 50% of breast cancer survivors.48,49 Similarly, CINV, despite advancements in antiemetic therapies, continues to affect 50–60% of cancer patients.50 The significant increase in symptom prevalence during chemotherapy reflects the toxicological mechanisms of chemotherapeutic agents, such as the disruption of the central nervous system, gastrointestinal tract and autonomic nervous system by cytotoxic drugs.51 Some symptoms, including anxiety (29.3–34.2%), fatigue (13.0–36.0%) and sleep problems (39.2%), persist even after the completion of chemotherapy. These symptoms significantly impair patients’ daily functioning and treatment adherence.52,53 For high-risk patients, mitigation strategies should be prioritized for these symptoms to improve long-term quality of life.54
Beyond the five common symptoms mentioned above, other symptoms are equally noteworthy. CI commonly referred to as “chemo brain,” persists throughout the chemotherapy process,11,21 manifesting as declines in memory, attention, and executive function post-chemotherapy.55 These cognitive deficits can persistently impair patients’ daily decision-making abilities and work efficiency, thereby reducing their quality of life and social engagement.56 CIPN remains highly severe post-chemotherapy,17 often presenting as numbness, tingling and sensory abnormalities, which lead to difficulties in walking, impaired fine motor skills, and an increased risk of falls, significantly affecting patients’ functional independence and sense of safety.12 Additionally, some patients experience sexual dysfunction due to the disease or chemotherapy, such as vaginal dryness (45.9%) and decreased libido (45.2%).33 These symptoms not only compromise patients’ sexual quality of life but may also trigger strained intimate relationships and psychological distress, particularly among younger patients.57,58 The breadth and persistence of these symptoms underscore the complex supportive care needs of breast cancer patients undergoing chemotherapy, necessitating multidisciplinary interventions to comprehensively address their physiological, psychological and social impacts.
The classification of factors associated with these symptoms into modifiable and non-modifiable categories facilitates targeted interventions for modifiable risks while enabling risk stratification to identify high-risk individuals for enhanced monitoring and prevention strategies. Researchers can identify high-risk groups through known non-modifiable factors and develop comprehensive interventions to mitigate symptom occurrence. For instance, screening younger patients for anxiety and depression could prompt early referral to evidence-based mitigation strategies, including cognitive-behavioral therapy, supportive care programs, or physical activity interventions to alleviate psychological distress.59–61 For modifiable factors, tailored approaches can enhance the applicability and effectiveness of nursing interventions. For instance, addressing modifiable factors like low Karnofsky Performance Status or inadequate adherence to healthful diets (such as Mediterranean or MIND patterns) through relevant interventions, such as multidisciplinary supportive care or exercise programs, could reduce persistent post-treatment symptom burden and improve quality of life.42,62,63
Strengths and Limitations
This systematic review provides a comprehensive synthesis of observational studies encompassing multiple symptom domains, chemotherapy phases, and associated factor categories. By adopting this broad scope, it offers a holistic perspective on symptom experiences in breast cancer patients undergoing chemotherapy, which is lacking in prior reviews focused on narrower aspects, such as cardiotoxicity alone.
Several limitations should be acknowledged. Firstly, the reliance on self-reported data may introduce recall bias and subjective bias, potentially affecting the accuracy of symptom prevalence and severity estimates. Secondly, the exclusion of non-English language studies limits the inclusion of diverse global perspectives, possibly underrepresenting variations in symptom profiles across cultural or regional contexts. Finally, substantial heterogeneity among the included studies arising from differences in chemotherapy regimens (such as adjuvant versus neoadjuvant settings), assessment timing (before, during, and after chemotherapy), and measurement instruments. This poses challenges for data standardization and quantitative synthesis. Future research should prioritize standardized protocols for regimens, timing, and tools to facilitate meta-analyses and improve clinical applicability.
Conclusion
Breast cancer patients undergoing chemotherapy experience a variety of symptoms. The most common symptoms identified in this review include anxiety, depression, CINV, fatigue, and sleep problems. The factors reported were divided into non-modifiable and modifiable factors. Younger age was the most frequently reported risk factor for increased anxiety, depression, fatigue, nausea, and menopausal symptoms, followed by having children, greater number of chemotherapy cycles, higher BMI, lower performance status, and limited social support. These findings highlight the necessity of early symptom screening in clinical practice, particularly baseline assessments to identify high-risk patients and inform comprehensive management strategies that optimize outcomes and quality of life. Future research should prioritize identifying high-risk groups, developing personalized interventions to enhance treatment adherence, and validating standardized symptom assessment tools alongside patient-directed approaches to address current evidence gaps.
Statement of Ethics Approval
As this is a systematic review, ethical approval was not required.
Consent to Participate Declaration
This systematic review does not require a consent to participate declaration, as it analyzes data from published studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors acknowledge Universiti Putra Malaysia for funding the article processing fees.
Disclosure
The authors declare no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA CANCER J CLIN. 2024;74:229–20. doi:10.3322/caac.21834
2. McDonald ES, Clark AS, Tchou J, Zhang P, Freedman GM. Clinical diagnosis and management of breast cancer. J Nucl Med. 2016;57:9S–16S. doi:10.2967/jnumed.115.157834
3. Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: an independent review. The Lancet. 2012;380:1778–1786. doi:10.1016/S0140-6736(12)61611-0
4. Nardin S, Fm V, Ar V, et al. Breast cancer survivorship, quality of life, and late toxicities. Front Oncol. 2020;10. doi:10.3389/fonc.2020.00864
5. Mokhtari-Hessari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health and quality of life outcomes. Health Qual Life Outcomes. 2020;18. doi:10.1186/s12955-020-01591-x
6. WKW S, Law BMH, MSN N, et al. Symptom clusters experienced by breast cancer patients at various treatment stages: a systematic review. Cancer Med. 2021;10:2531–2565. doi:10.1002/cam4.3794
7. Qi Y, Li H, Guo Y, Cao Y, Wong CL. Symptom clusters in breast cancer patients receiving adjuvant chemotherapy: a systematic review. Journal of Clinical Nursing. 2024;33:4554–4567. doi:10.1111/jocn.17479
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
9. Kmet L, Lee R, Cook L. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. 2004 [Cited May 6, 2024]. Available from: https://www.ihe.ca/advanced--search/standard--quality--assessment--criteria--for--evaluating--primary--research--papers--from--a--variety--of--fields.
10. Lee L, Packer TL, Tang SH, Girdler S. Self‐management education programs for age‐related macular degeneration: a systematic review. Australas J Ageing. 2008;27:170–176. doi:10.1111/j.1741-6612.2008.00298.x
11. Cheung YT, Ng T, Shwe M, et al. Association of proinflammatory cytokines and chemotherapy-associated cognitive impairment in breast cancer patients: a multi-centered, prospective, cohort study. Annals of Oncology. 2015;26:1446–1451. doi:10.1093/annonc/mdv206
12. Bao T, Basal C, Seluzicki C, Li S, Ad S, Mao J. Long-term chemotherapy-induced peripheral neuropathy among breast cancer survivors: prevalence, risk factors, and fall risk. Breast Cancer Res Treat. Breast Cancer Res Treat. 2016;159:327–333. doi:10.1007/s10549-016-3939-0
13. Jung D, Lee K-M, Kim W-H, et al. Longitudinal association of poor sleep quality with chemotherapy-induced nausea and vomiting in patients with breast cancer. Psychosom Med. 2016;78:959–965. doi:10.1097/PSY.0000000000000372
14. Liu Y, Pan T, Zou W, et al. Relationship between traditional Chinese medicine constitutional types with chemotherapy-induced nausea and vomiting in patients with breast cancer: an observational study. BMC Complement Alternat Med. 2016;16. doi:10.1186/s12906-016-1415-3
15. Peoples AR, Roscoe JA, Block RC, et al. Nausea and disturbed sleep as predictors of cancer-related fatigue in breast cancer patients: a multicenter NCORP study. Support Care Cancer. 2017;25:1271–1278. doi:10.1007/s00520-016-3520-8
16. Kim GM, Kim S, Park HS, et al. Chemotherapy-induced irreversible alopecia in early breast cancer patients. Breast Cancer Res Treat. 2017;163:527–533. doi:10.1007/s10549-017-4204-x
17. Greenlee H, Hershman DL, Shi Z, et al. BMI, lifestyle factors and taxane-induced neuropathy in breast cancer patients: the pathways study. JNCI J Natl Cancer Inst. 2017;109:djw206. doi:10.1093/jnci/djw206
18. Lee K-M, Jung D-Y, Hwang H, et al. Late chronotypes are associated with neoadjuvant chemotherapy-induced nausea and vomiting in women with breast cancer. Chronobiol Int. 2017;34:480–491. doi:10.1080/07420528.2017.1295978
19. Reinertsen KV, Engebraaten O, Loge JH, et al. Fatigue during and after breast cancer therapy—a prospective study. J Pain Sympt Manage. 2017;53:551–560. doi:10.1016/j.jpainsymman.2016.09.011
20. Imanian M, Imanian M, Karimyar M. Sleep quality and fatigue among breast cancer patients undergoing chemotherapy. Int J Hematol Oncol Stem Cell Res. 2019;13:196–200. doi:10.18502/ijhoscr.v13i4.1894
21. Hormozi M, Hashemi S-M, Shahraki S. Investigating relationship between pre- and post- chemotherapy cognitive performance with levels of depression and anxiety in breast cancer patients: a cross-sectional study. Asian Pac J Cancer Prev Thailand. 2019;20:3831–3837. doi:10.31557/APJCP.2019.20.12.3831
22. Kim JH, Paik H-J, Jung YJ, et al. A prospective longitudinal study about change of sleep, anxiety, depression, and quality of life in each step of breast cancer patients. Oncol. Switzerland. 2019;97:245–253. doi:10.1159/000500724
23. Shorofi SA, Nozari-Mirarkolaei F, Arbon P, Bagheri-Nesamie M. Depression and sleep quality among iranian women with breast cancer. Asian Pac J Cancer Prev. 2021;22:3433–3440. doi:10.31557/APJCP.2021.22.11.3433
24. Nakamura ZM, Deal AM, Nyrop KA, et al. Serial assessment of depression and anxiety by patients and providers in women receiving chemotherapy for early breast cancer. Oncologist. 2021;26:147–156. doi:10.1002/onco.13528
25. Deng S-M, Chiu A-F, Wu S-C, et al. Association between cancer-related fatigue and traditional Chinese medicine body constitution in female patients with breast cancer. J Tradit Complement Med. 2021;11:62–67. doi:10.1016/j.jtcme.2020.08.005
26. Huang X, Li X, Li J, et al. Chemotherapy-Induced nausea and vomiting in breast cancer patients: a multicenter prospective observational study. Asia Pac J Oncol Nurs United States. 2021;8:433–437. doi:10.4103/apjon.apjon-2120
27. Williams ALM, Khan CP, Heckler CE, et al. Fatigue, anxiety, and quality of life in breast cancer patients compared to non-cancer controls: a nationwide longitudinal analysis. Breast Cancer Res Treat. 2021;187:275–285. doi:10.1007/s10549-020-06067-6
28. Lv D, Lan B, Zhang L, Sun X, Yang M, Ma F. Association between depression and anxiety status of breast cancer patients undergoing adjuvant chemotherapy and chemotherapy-induced adverse events. Cancer Med. 2022;12:4794–4800. doi:10.21203/rs.3.rs-1186049/v1
29. Singh KP, Kober KM, Ernst B, et al. Multiple gastrointestinal symptoms are associated with chemotherapy-induced nausea in patients with breast cancer. Cancer Nurs. 2022;45:181–189. doi:10.1097/NCC.0000000000000976
30. Hajj A, Chamoun R, Salameh P, et al. Fatigue in breast cancer patients on chemotherapy: a cross-sectional study exploring clinical, biological, and genetic factors. BMC Cancer. 2022;22:16. doi:10.1186/s12885-021-09072-0
31. Lan B, Lv D, Yang M, Sun X, Zhang L, Ma F. Psychological distress and quality of life in Chinese early-stage breast cancer patients throughout chemotherapy. J Nat Canc Cent. 2022;2:155–161. doi:10.1016/j.jncc.2022.06.002
32. Guo Y-Q, Qing-Mei J, You M, Liu Y, Azlina Y, Lean Keng S. Depression, anxiety and stress among metastatic breast cancer patients on chemotherapy in China. BMC Nurs. 2023;22:1–11. doi:10.1186/s12912-023-01184-1
33. Haris I, Hutajulu SH, Astari YK, et al. Sexual dysfunction following breast cancer chemotherapy: a cross-sectional study in Yogyakarta, Indonesia. Cureus. 2023. doi:10.7759/cureus.41744
34. Zhai J, Sun X, Zhao F, et al. Serum sodium ions and chloride ions associated with taxane-induced peripheral neuropathy in Chinese patients with early-stage breast cancer: a nation-wide multicenter study. Breast. 2023;67:36–45. doi:10.1016/j.breast.2022.12.034
35. Zhu W, Li W, Gao J, Wang L, Guo J, Yang H. Factors associated with the sleep disturbances of people with breast cancer during chemotherapy in China: a cross-sectional study. Nurs Open. 2023;10:5453–5461. doi:10.1002/nop2.1784
36. Liang C, Zhang Y, Chen QY, Chen WF, Chen MZ. Risk factors for taxane‐induced peripheral neuropathy in patients with breast cancer. Asia-Pac J Clncl Oncology. 2024;20:220–227. doi:10.1111/ajco.13923
37. Zhao D, Ma Q, Li G, Qin R, Meng Y, Li P. Treatment-induced menopause symptoms among women with breast cancer undergoing chemotherapy in China: a comparison to age- and menopause status–matched controls. Menopause. 2024;31:145–153. doi:10.1097/GME.0000000000002296
38. Yang Y, Han J, Monroe TB, Kim S. Pain and cognition of breast cancer survivors treated with chemotherapy: the mediating role of depression. Seminar Oncol Nurs. 2024;40:151693. doi:10.1016/j.soncn.2024.151693
39. Olfa B, Salma M, Othman Rym B, et al. Impact of nutritional status on chemotherapy related digestive toxicity in women with breast cancer. Nutr Metab Insights. 2024;17:11786388241297142. doi:10.1177/11786388241297142
40. Miroševič Š, Prins J, Bešić N, et al. Symptoms of anxiety and depression among slovenian breast cancer survivors post-treatment during the COVID-19 pandemic: a cross-sectional study. Slovenian J Public Health. 2024;63:55–62. doi:10.2478/sjph-2024-0008
41. Liu Y, Liu J-E, Shi T-Y, et al. Factors associated with perceived cognitive function in breast cancer patients treated with chemotherapy: a multicenter cross-sectional study. Eur J Oncol Nurs. 2024 doi:10.1016/j.ejon.2024.102623.
42. Winschel TR, Weinhold K, Schnell PM, et al. The association of the MIND diet and its components with cognitive function in postmenopausal breast cancer survivors. Support Care Cancer. 2025;33:736. doi:10.1007/s00520-025-09789-9
43. Ou H, Tan Z, Shen A, et al. Development of a machine learning-based risk prediction model and analysis of risk factors for docetaxel-induced bone marrow suppression in breast cancer patients. Int J Clin Pharm. 2025. doi:10.1007/s11096-025-01989-x
44. Jiang T, Wang X, Zheng L, Ren T, Li Y, Li J. Risk factors of nausea and vomiting in patients with breast cancer undergoing chemotherapy: a retrospective study. Medicine. 2025;104(e41067). doi:10.1097/MD.0000000000041067
45. His M, Baggio I, Chabaud S, et al. Long-term weight change among breast cancer patients treated with chemotherapy: a longitudinal study over 13 years. Breast Cancer Res. 2025;27:117. doi:10.1186/s13058-025-02079-6
46. Chandrasekaran SH, Inban P, Maharjan R, et al. Investigation of chemotherapy-induced cardiac dysfunction in breast cancer. J Chemotherapy. 2025:1–11. doi:10.1080/1120009X.2025.2466278
47. Alawi KA, Fahdi AA, Chan MF, Sumri HA, Al-Azri M. Evaluating symptom burden among omani women newly diagnosed with breast cancer: a cross-sectional study. Curr Oncol. 2025;32:9. doi:10.3390/curroncol32020059
48. Kang Y-E, Yoon J-H, Park N-H, Ahn Y-C, Lee E-J, Son C-G. Prevalence of cancer-related fatigue based on severity: a systematic review and meta-analysis. Sci Rep. 2023;13:12815. doi:10.1038/s41598-023-39046-0
49. Ma Y, He B, Jiang M, et al. Prevalence and risk factors of cancer-related fatigue: a systematic review and meta-analysis. Int J Nurs Stud. 2020;111:103707. doi:10.1016/j.ijnurstu.2020.103707
50. Sun Y, Zheng Y, Yang X, et al. Incidence of chemotherapy-induced nausea and vomiting among cancer patients receiving moderately to highly emetogenic chemotherapy in cancer centers in Sichuan, China. J Cancer Res Clin Oncol. 2021;147:2701–2708. doi:10.1007/s00432-021-03554-1
51. Tao G, Huang J, Moorthy B, et al. Potential role of drug metabolizing enzymes in chemotherapy-induced gastrointestinal toxicity and hepatotoxicity. Expert Opin Drug Metab Toxicol. 2020;16:1109–1124. doi:10.1080/17425255.2020.1815705
52. Hendy A, Ibrahim RK, Darwish A, et al. Sleep disturbance, cancer-related fatigue, and depression as determinants of quality of life among breast cancer patients undergoing chemotherapy: a cross-sectional study. BMC Cancer. 2025;25:1122. doi:10.1186/s12885-025-14538-6
53. Rashidi A, Thapa S, Kahawaththa Palliya Guruge WS, Kaur S. Patient experiences: a qualitative systematic review of chemotherapy adherence. BMC Cancer. 2024;24:658. doi:10.1186/s12885-024-12353-z
54. Sibeoni J, Picard C, Orri M, et al. Patients’ quality of life during active cancer treatment: a qualitative study. BMC Cancer. 2018;18:951. doi:10.1186/s12885-018-4868-6
55. Vearncombe KJ, Rolfe M, Wright M, Pachana NA, Andrew B, Beadle G. Predictors of cognitive decline after chemotherapy in breast cancer patients. J Int Neuropsychol Soc. 2009;15:951–962. doi:10.1017/S1355617709990567
56. Yang Y, Von Ah D. Cancer-related cognitive impairment: updates to treatment, the need for more evidence, and impact on quality of life-a narrative review. Ann Palliat Med. 2024;13:1265–1280. doi:10.21037/apm-24-70
57. Chang C-P, Ho TF, Snyder J, et al. Breast cancer survivorship and sexual dysfunction: a population-based cohort study. Breast Cancer Res Treat. 2023;200:103–113. doi:10.1007/s10549-023-06953-9
58. Jankowska M. Sexual functioning in young women in the context of breast cancer treatment. Rep Pract Oncol Radiother. 2013;18:193–200. doi:10.1016/j.rpor.2013.04.032
59. Kostecka M. The potential influence of dietary counseling on nutritional status and dietary supplement consumption in breast cancer patients: a pilot study. Nutr Cancer. 2019;71:749–755. doi:10.1080/01635581.2018.1531138
60. Kwekkeboom K, Zhang Y, Campbell T, et al. Randomized controlled trial of a brief cognitive‐behavioral strategies intervention for the pain, fatigue, and sleep disturbance symptom cluster in advanced cancer. Psycho-Oncology. 2018;27:2761–2769. doi:10.1002/pon.4883
61. Park S, Sato Y, Takita Y, et al. Mindfulness-Based cognitive therapy for psychological distress, fear of cancer recurrence, fatigue, spiritual well-being, and quality of life in patients with breast cancer—a randomized controlled trial. Journal of Pain and Symptom Management. 2020;60:381–389. doi:10.1016/j.jpainsymman.2020.02.017
62. Chen G, Leary S, Niu J, Perry R, Papadaki A. The role of the mediterranean diet in breast cancer survivorship: a systematic review and meta-analysis of observational studies and randomised controlled trials. Nutrients. 2023;15:2099. doi:10.3390/nu15092099
63. Li L, Wang Y, Cai M, Fan T. Effect of different exercise types on quality of life in patients with breast cancer: a network meta-analysis of randomized controlled trials. The Breast. 2024;78:103798. doi:10.1016/j.breast.2024.103798
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test in Node-Negative Early Breast Cancer
Berdunov V, Millen S, Paramore A, Griffin J, Reynia S, Fryer N, Brown R, Longworth L
ClinicoEconomics and Outcomes Research 2022, 14:619-633
Published Date: 19 September 2022
Advice from One Patient to Another: Qualitative Analysis of Patients’ Perspectives About Chemotherapy Initiation
Malinowski C, Paredes E, Housten AJ, Chavez-MacGregor M
Patient Preference and Adherence 2022, 16:3283-3289
Published Date: 14 December 2022
Dietary Behavior and Its Association with Nutrition Literacy and Dietary Attitude Among Breast Cancer Patients Treated with Chemotherapy: A Multicenter Survey of Hospitals in China
Tang H, Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L
Patient Preference and Adherence 2023, 17:1407-1419
Published Date: 9 June 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Analysis of Cardiotoxicity and Risk Factors of Breast Cancer Chemotherapy Drugs: A Five-Year Single-Centre Retrospective Study in Early Breast Cancer
Ju F, Gu H, Yu L, Zhao G, Liu Y, Yin D, Niu J, Xue T, Yin C, Jiao L, Li C, Wu J, Ji Y
Drug Design, Development and Therapy 2025, 19:6505-6517
Published Date: 30 July 2025