Back to Journals » Patient Preference and Adherence » Volume 17
Dietary Behavior and Its Association with Nutrition Literacy and Dietary Attitude Among Breast Cancer Patients Treated with Chemotherapy: A Multicenter Survey of Hospitals in China
Authors Tang H ![]() , Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L
, Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L ![]()
Received 22 March 2023
Accepted for publication 6 June 2023
Published 9 June 2023 Volume 2023:17 Pages 1407—1419
DOI https://doi.org/10.2147/PPA.S413542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Han Tang,1,2 Ruibo Wang,3 Pei Yan,1,4 Wei Zhang,1 Feng Yang,1 Shengjie Guo,3 Ting Li,3 Luanxing Yi,5 Xue Bai,6 Shan Lin,7 Yuhai Zhang,1 Lei Shang1
1Department of Health Statistics, School of Public Health, The Fourth Military Medical University, Xi’an, Shaanxi, 710032, People’s Republic of China; 2Department of Clinical Nursing, School of Nursing, The Fourth Military Medical University, Xi’an, Shaanxi, 710032, People’s Republic of China; 3School of Nursing and Health, Zhengzhou University, Zhengzhou, Henan, 450001, People’s Republic of China; 4Department of Operation Room, Xijing Hospital, The Fourth Military Medical University, Xi’an, Shaanxi, 710032, People’s Republic of China; 5School of Nursing, Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, 350122, People’s Republic of China; 6Puyang Oilfield General Hospital, Puyang, Henan, 457001, People’s Republic of China; 7Department of Neurology, The 900th Hospital of Joint Logistic Support Force, PLA, Fuzhou, Fujian, 350025, People’s Republic of China
Correspondence: Lei Shang, The Fourth Military Medical University, Changle West Road 169#, Xi’an, Shaanxi, People’s Republic of China, Tel +86 029-84774853, Email [email protected]
Background: Chemotherapy often negatively impacts the nutritional status of breast cancer patients, and healthy dietary behaviors are important for patient wellbeing. With the guidance of the “Knowledge, Attitude and Practice model” (KAP model), the objective of this survey was to determine the frequency with which patients engage in healthy dietary behaviors and to explore the association between healthy dietary behaviors and nutrition literacy and dietary attitudes.
Methods: This study included a total of 284 breast cancer patients undergoing chemotherapy from three hospitals spanning three cities in China. Face-to-face interviews were conducted to collect demographic and clinical characteristics as well as the Dietary Nutritional Knowledge, Attitude and Practice Questionnaire (DNKAPQ) and the Nutrition Literacy Measurement Scale for Chinese Adult (NLMS-CA).
Results: Participants exhibited medium to high scores for nutrition literacy, dietary attitude and dietary behavior. Nutrition literacy (r = 0.505, p < 0.001) and dietary attitude (r= 0.326, p < 0.001) scores were both positively correlated with the total dietary behavior score. The total nutrition literacy score was positively correlated with the total dietary behavior score (r = 0.286, p < 0.001). In the univariate analysis, age, body mass index, living environment, education level, monthly family income, work status, menopausal status, number of comorbidities, relapse and endocrine therapy were significantly associated with dietary behavior (p < 0.05). In the multiple linear regression analysis, patients’ dietary behavior was significantly associated with nutrition literacy (β = 0.449, p < 0.001) and dietary attitude (β = 0.198, p < 0.001). These two factors accounted for 28.6% of the variation in the patients’ dietary behavior scores.
Conclusion: There is an important need for targeted dietary and nutritional interventions designed and implemented by health professionals to improve dietary behaviors. Intervention design and content should take the patients’ nutrition literacy and dietary attitudes into consideration. In particular, women who are older, overweight, unemployed, and postmenopausal and live in rural areas, exhibit fewer comorbidities, have a lower family income and education level, have not relapsed and are currently receiving endocrine therapy are in urgent need of diet-specific intervention.
Keywords: attitude, behavior, breast cancer, chemotherapy, dietary, nutrition literacy
Introduction
According to the latest global cancer epidemiological data released by the World Health Organization,1 approximately 2.3 million new cases of female breast cancer were diagnosed in 2020, representing 11.7% of all new cancer cases. Similarly, breast cancer remains the most common cancer in women in China. More than 400,000 new cases of breast cancer are diagnosed each year among Chinese women, and this number is expected to increase further.2 Although the incidence of breast cancer is high, several studies2,3 have confirmed that the 5-year relative survival rate of breast cancer patients is favorable, reaching 40.5% and greater. The proportion of breast cancer survivors is also steadily increasing, which is largely attributed to the development of early diagnosis techniques and improved treatment effects. Among various anticancer therapies, chemotherapy remains one of the most common and effective ways to destroy dividing cancer cells, alleviate tumor burden, improve cancer prognoses, and significantly increase survival rates.4 However, while eliminating tumor cells, chemotherapy will inevitably damage normal cells, resulting in a series of side effects that negatively influence eating and diet, leading to malnutrition.5 A healthy diet may alleviate adverse nutritional outcomes after chemotherapy among breast cancer patients and could improve patient quality of life during long-term treatment and survival.
Nutrition and diet are essential parts of daily life for breast cancer patients.6 Increased metabolic demands in these patients demonstrates the importance of nutrition supplementation and diet intake.7 Moreover, the side effects of chemotherapy, such as nausea and vomiting, loss of appetite and taste change, interfere with normal nutritional intake, food perception and food choice, which is subsequently accompanied by a series of abnormal dietary behaviors.8 This may not only result in weight fluctuations, adverse changes in body composition, and loss of muscle strength9 but also has profoundly negative consequences on quality of life and the psychological status of breast cancer survivors and increases the risk of recurrence. For example, increased BMI after chemotherapy is an important risk factor for breast cancer recurrence.10 In addition, many breast cancer patients in China seek dietary therapy help from traditional Chinese medicine (TCM) after chemotherapy. Because it is thought that edible food and medicine have the same origin, some believe that diet and medicine may similarly treat the disease.11 Given that Chinese female breast cancer patients value the importance of diet, especially after disease and treatment, and in consideration of a long survival period, there is a need to address the nutritional problems after chemotherapy, encourage patients to participate in their own dietary management, promote related healthy behaviors, and adjust and balance healthy dietary behaviors.
Breast cancer patients should engage in healthy dietary behaviors, but the prevalence and performance of such behaviors is unknown. There is little, existing evidence regarding the prevalence of healthy dietary behavior e. A study12 from the US reported that 50.67% of breast cancer survivors engaged in healthy dietary behavior over a 13-year follow-up, but the prevalence of healthy dietary behaviors among Chinese breast cancer patients treated with chemotherapy is unknown. In addition, dietary behavior used to be summarized as “what to eat, how to eat and how much to eat”.13 Several studies of dietary behavior in breast cancer patients have demonstrated that while some participants followed healthy dietary patterns, such as increasing the consumption of fruits and vegetables,14 others tended to eat more dessert and candy to activate the reward system and produce feelings of pleasure and relaxation.15 Chinese females may be influenced by TCM, such as avoiding consumption of any food they perceive as “fawu”, which is believed to lead to allergic disease or relapse, such as onions, leeks, chicken and seafood.16 However, there is no clear evidence that “fawu” is taboo in diet during breast cancer treatment. Additionally, diet-related health management behavior among individuals of different demographics and with clinical conditions may also vary. One study17 demonstrated that younger breast cancer patients were better able to manage their own health, but another18 reported that older adult patients are more willing to invest time and energy in daily health management. Moreover, limited studies19 found significant differences in dietary behavior among pre- and postmenopausal breast cancer patients and among those in different living environments, and the impact of body mass index (BMI) has only gained attention in recent years. There is also a lack of adequate data and verified conclusions regarding the impact of clinical factors on dietary behaviors in this population. One study20 showed that it is difficult to determine the effects of different chemotherapy cycles on patients’ dietary behavior. Furthermore, another study21 reported that breast cancer patients who received no radiotherapy or endocrine therapy may be less likely to adhere to recommended lifestyle guidance.
Nutrition literacy refers to a special type of health literacy related to nutrition and food, reflected as an individual’s ability to obtain, process and understand basic nutritional information and make correct nutrition-related decisions.22 Compared to knowledge, nutrition literacy is a more comprehensive concept that consists of not only the acquisition of nutritional knowledge but also the application of knowledge, which assesses whether an individual is able to help themselves solve nutrition problems independently. Studies on nutrition literacy of patients primarily focus on healthy adults,23 children’s parents24 or pregnant women.25 Research26 related to breast cancer patients demonstrated that their nutritional knowledge was inadequate, with only 30% improving their diet after treatment. However, the study did not state how the patients applied their knowledge or modified their dietary behaviors. In addition, dietary attitude primarily includes patients’ views and thoughts on food and diet in terms of disease and treatment. Some studies10,27 indicate that cancer patients expressed surprise and concern associated with changes to weight after chemotherapy; patients were reported as being aware of the importance of diet in recovery, but only 33.2% of participants wanted to go to nutrition clinics when they had questions about diet. Evidence on dietary attitudes among breast cancer patients is insufficient.
There is a need to explore the levels of nutrition literacy, dietary attitude and dietary behavior in breast cancer patients treated with chemotherapy and the factors that influence these levels. With the guidance of the “Knowledge, Attitude and Practice model” (KAP model),28 this study aims to determine whether nutrition literacy and dietary attitude influence dietary behavior.
Materials and Methods
Study Design, Subjects and Setting
This was a cross-sectional study and was conducted using convenience sampling. Participants were enrolled from three general hospitals distributed in three cities (Zhengzhou, Fuzhou, Puyang) in mainland China. A total of twenty-four variables, including twenty-two variables from the demographic and clinical characteristics questionnaire as well as two variables, nutrition literacy and dietary attitude, were included and analyzed in this research. According to a previous study,29 the sample size should be at least 5 to 10 times the number of variables. Thus, the number of participants should not be less than 120 to 240 subjects, and a 20% loss to follow-up rate should also be considered. Therefore, 288 Chinese breast cancer patients were contacted.
The inclusion criteria were as follows: (a) age 18 or older; (b) pathologic diagnosis of malignant breast cancer; (c) informed of the cancer diagnosis; (d) undergoing neoadjuvant or adjuvant chemotherapy, with or without other treatments; (e) able to eat by mouth independently; and (f) able to express one’s own thoughts autonomously and communicate with barrier-free obstacles. The exclusion criteria were as follows: (a) unstable mental state or physical condition that prevented completion of the questionnaire; and (b) involvement or previous involvement in other similar investigations.
The data were collected from June to September 2022 using paper questionnaires generated by the research members and then typed in the 2016 version of Microsoft Excel. All of the instruments used are publicly available for scientific research. The specific data collection process was as follows. The research group consisted of a researcher, a doctor, two medical students and three nurses. Before the survey, the researcher introduced the purpose, content, methods and precautions to the group members. Given that the clinics we enrolled had not only breast cancer inpatients but also patients with other kinds of cancer, the group members first looked through the patient’s electronic medical record system to broadly exclude patients with other diseases. Then, the members approached the patients. The patients were informed of the purpose and process of the study and were asked to sign an informed consent form. After that, an independent questionnaire was completed by the patients. Questionnaires were distributed and returned on the spot. The team members checked whether there were any missing items or unclear identification; if there were, the participants were asked to complete the information. The study was approved by the Ethics Committee of the Affiliated Hospital of Zhengzhou University (Project identification code: 2020-KY-220).
Instruments
All instruments were self-report questionnaires. The dependent variable was dietary behavior, which was measured by one of the dimensions (dietary practice) of the Dietary Nutritional Knowledge, Attitude and Practice Questionnaire (DNKAPQ). The independent variables included demographic and clinical characteristics, dietary attitude and nutrition literacy. Dietary attitude was measured by one of the dimensions (dietary attitude) of the DNKAPQ, and nutrition literacy was assessed by the Nutrition Literacy Measurement Scale for Chinese Adult (NLMS-CA). In addition, a self-designed demographic and clinical characteristics questionnaire was used to evaluate demographic, disease and treatment characteristics among Chinese breast cancer patients treated with chemotherapy.
Questionnaire of Demographic and Clinical Characteristics
There were three main aspects of the demographic and clinical characteristics questionnaire. Demographic information included age, BMI, marital status, number of children, living environment, nationality, religion, education level, monthly family income per capita, work status and menopausal status. With respect to disease characteristics, variables included the number of comorbidities, cancer stage, unilateral or bilateral breast cancer and relapse. The last category included treatment information, which included whether chemotherapy was administered for the first time, the type of chemotherapy, number of cycles of chemotherapy, and whether patients also underwent surgery, radiotherapy, endocrine therapy or targeted therapy.
Dietary Nutritional Knowledge, Attitude and Practice Questionnaire (DNKAPQ)
The Dietary Nutritional Knowledge, Attitude and Practice Questionnaire (DNKAPQ) was developed by Xu30 from China in 2021 to assess the level of nutritional knowledge, dietary attitudes and dietary practices in patients with malignant tumors undergoing chemotherapy treatment. This 32-item scale has 3 dimensions: nutritional knowledge (14 items), dietary attitude (7 items) and dietary practice (11 items). The development of this questionnaire was based on the concept of the KAP model. We only adopted two of the dimensions to measure the dietary attitude and dietary behavior, and the assessment of nutrition knowledge was performed using specific nutrition literacy-related tools. The dietary attitude dimension was used to quantify the dietary attitude. Each item is rated on a 5-point Likert scale ranging from 1 point (strongly disagree) to 5 points (strongly agree), and the total score is the sum of the scores for all items. A higher total score indicates a more positive attitude towards a healthy diet after disease and treatment. The Cronbach’s α coefficient of this dimension in this study was 0.843. The dietary practice dimension was used to quantify the dietary behavior. Each item is rated on a 5-point Likert scale ranging from 1 point (never) to 5 points (always), and the total score is the sum of the scores for all items. A higher total score indicates a higher frequency of engaging in positive healthy diet behaviors. The Cronbach’s α coefficient of this dimension in this study was 0.829.
Nutrition Literacy Measurement Scale for Chinese Adult (NLMS-CA)
The NLMS-CA was designed by Zhang31 from China in 2021 to evaluate the level of nutrition literacy in Chinese adults. The development of this scale refers to the three-factor model (functional, interactive and critical) of nutrition literacy from Velardo,32 comprising 6 dimensions and 43 items: knowledge reserve (7 items), knowledge understanding (5 items), skills of acquisition (5 items), skills of application (11 items), skills of interaction (9 items) and skills of criticism (6 items). The items are scored on a 5-point scale (1 point = strongly disagree to 5 points = strongly agree), and the total score is the sum of the scores for all the items. A higher total score indicates a higher degree of nutrition literacy. The Cronbach’s α coefficient of this scale in this study was 0.949.
Data Analysis
We used SPSS version 21.0 software (IBM Corporation, Armonk, NY) to analyze all included data. All variables, including independent and dependent variables, were reported in detail. Demographic and clinical characteristics, patient dietary behaviors, dietary attitudes and nutrition literacy are presented as the means ± standard deviations (SD) if they are continuous variables. For categorical variables, frequency counts and percentages were used. Independent t-tests were used to assess the differences in dependent variables (dietary behavior) between two groups of variables (eg, marital status, relapse). One-way ANOVA was used to measure differences in dietary behavior for more than two groups of variables (eg, age, BMI, cancer stage). Pearson’s correlation analyses were conducted to determine the correlations between patients’ dietary behavior and dietary attitudes and nutrition literacy. The total dietary attitude and nutrition literacy scores were included in a multiple linear regression to further explore their influence on patients’ dietary behaviors.
Results
Approximately 288 breast cancer patients were initially contacted. Ultimately, 284 (recruitment rate = 98.61%) subjects were recruited and analyzed for this survey. The demographic and clinical characteristics of the Chinese breast cancer patients are presented in Table 1. All participants were female. With respect to demographic information, the mean age and BMI of the participants were 47.21±10.46 years and 23.58±3.39 kg/m2, respectively. A total of 94.0% of participants were married. Additionally, 62.3% and 37.7% of patients lived in rural and urban areas, respectively. With respect to educational level, most participants had at least a junior high school (31.7%) or senior high school (20.4%) level of education. The monthly family income per capita distribution was relatively even at 1000–2999 yuan (31.0%), 3000–5000 yuan (32.4%) and more than 5000 yuan (23.6%). Most patients were unemployed (66.2%), including farmers and freelancers. In addition, most females were premenopausal (48.9%) or postmenopausal (39.8%). With respect to disease characteristics, 65.5% of patients reported no comorbidities, and 21.5% of patients reported one comorbidity. Most of the participants were at cancer stage II (59.2%) or III (26.1%). The vast majority of participants had unilateral breast cancer (94.4%) and had no relapse (85.2%). Approximately 91.9% of patients received primary chemotherapy, and 73.2% of participants received adjuvant chemotherapy. Most patients were undergoing the first to sixth cycle of chemotherapy (82.8%). Among the other treatments, 71.5% of participants underwent surgery, 25.0% of participants received radiotherapy, and 26.8% and 17.3% of patients received endocrine therapy and targeted therapy, respectively.
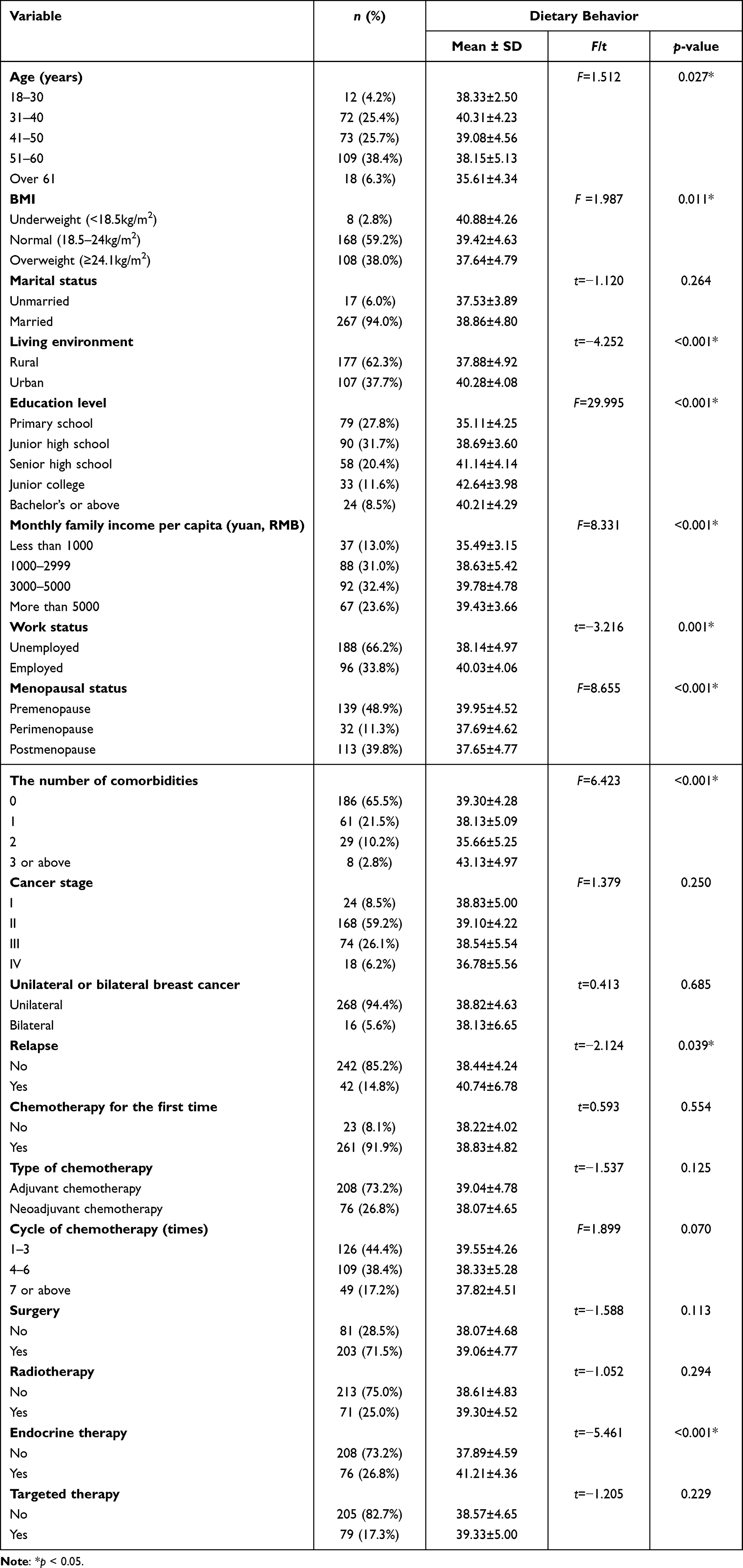 |
Table 1 Dietary Behavior of Different Sample Characteristics (n = 284) |
The dietary behavior, nutrition literacy and dietary attitude scores are presented in Table 2. The total average dietary behavior score was 38.78 ± 4.76 points, which reflected more than 70% of the total possible score (total possible score range: 11 to 55 points). The average item score (total average score divided by the total number of items) was 3.53 ± 0.43 points, which was higher than the median item score (3 points). With respect to nutrition literacy, the total average score was 156.69 ± 18.30 points, which also reflected more than 70% of the total possible score (total possible score range: 43 to 215 points). The average item score was 3.64 ± 0.43 points, which was slightly higher than the score for dietary behavior. Additionally, the average item score of each of the six dimensions from NLMS-CA from high to low were knowledge reserve (4.19 ± 0.48 points), skills of application (3.84 ± 0.46 points), skills of interaction (3.79 ± 0.47 points), skills of criticism (3.33 ± 0.55 points), skills of acquisition (3.18 ± 0.58 points) and knowledge understanding (3.02 ± 0.71 points). Furthermore, the three highest average item scores among the six dimensions were higher than the total average score for nutrition literacy, and the remaining three lowest average item scores were lower than the total average score for nutrition literacy. The total average score for dietary attitude was 27.46 ± 2.70 points, which was more than 70% of the total possible score (total score range: 7 to 35 points). The average item score was 3.92 ± 0.39 points, which was higher than those for dietary behavior and nutrition literacy.
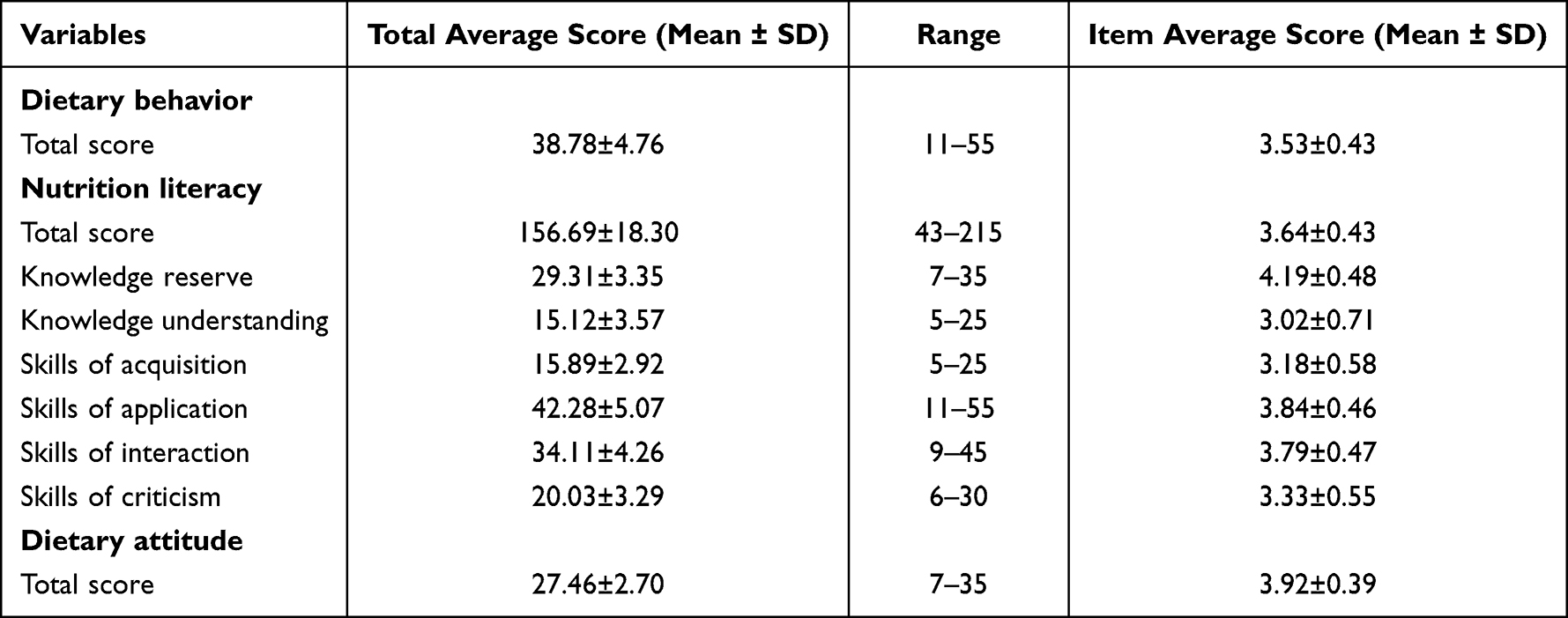 |
Table 2 Scores of Nutrition Literacy, Dietary Attitude and Dietary Behavior (n =284) |
The correlations between nutrition literacy, dietary attitude and dietary behavior among the Chinese breast cancer patients are presented in Table 3. The total nutrition literacy (r = 0.505, p < 0.001) and dietary attitude (r = 0.326, p < 0.001) scores were both positively correlated with the total dietary behavior score. In addition, the total scores of the six dimensions of nutrition literacy were all positively correlated with the total dietary behavior score (r ranged from 0.364 to 0.460, p < 0.001). Furthermore, the total nutrition literacy score was positively correlated with the total dietary attitude score (r = 0.286, p < 0.001), including the total scores of the six dimensions of nutrition literacy, which were all positively correlated with the total dietary attitude score (r ranged from 0.158 to 0.276, p < 0.01).
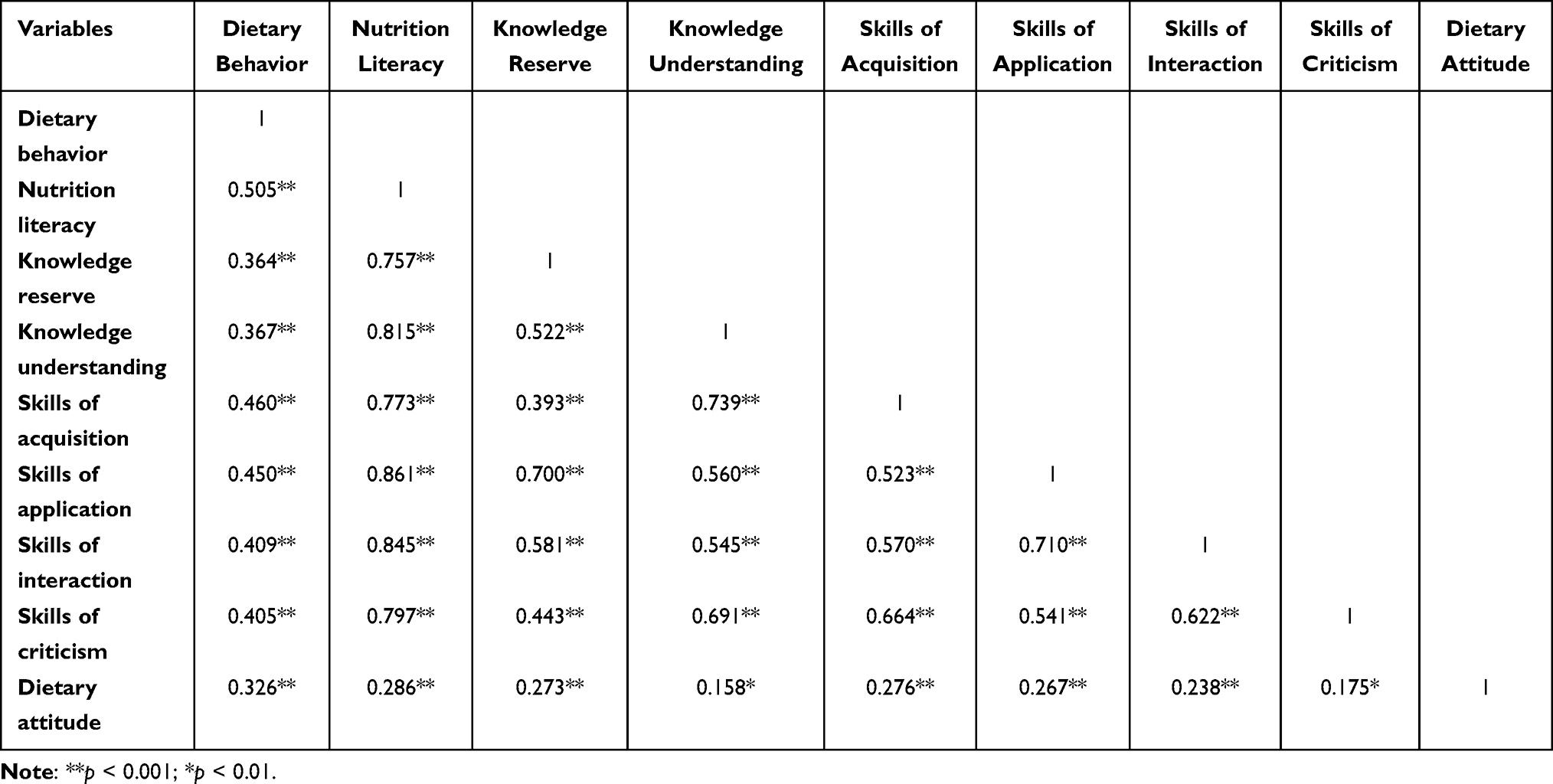 |
Table 3 Pearson’s Correlation Between Nutrition Literacy, Dietary Attitude and Dietary Behavior (n =284) |
In the univariate analysis, demographic and clinical characteristics that were significantly associated with dietary behavior were age, BMI, living environment, education level, monthly family income per capita, work status, menopausal status, number of comorbidities, relapse and endocrine therapy (p < 0.05), which are presented in Table 1.
The results of multiple linear regression used to explore the influence of nutrition literacy and dietary attitude on the dietary behaviors of breast cancer patients are presented in Table 4. The univariable analysis revealed a statistically significant association between dietary behavior and nutrition literacy (β = 0.505, p < 0.001); nutrition literacy accounted for 25.3% of the variation in the patients’ dietary behavior scores. Additionally, dietary attitude (β = 0.326, p < 0.001) accounted for 10.3% of the variation in the patients’ dietary behavior scores. In the multivariable analysis, dietary behaviors were significantly associated (p < 0.001) with nutrition literacy (β = 0.449, p < 0.001) and dietary attitude (β = 0.198, p < 0.001). In particular, each 1-point increase in nutrition literacy and dietary attitude resulted in a 0.117-point and 0.349-point increase, respectively, in the dietary behavior of Chinese cancer patients treated with chemotherapy. These two factors accounted for 28.6% of the variation in the patients’ dietary behavior scores.
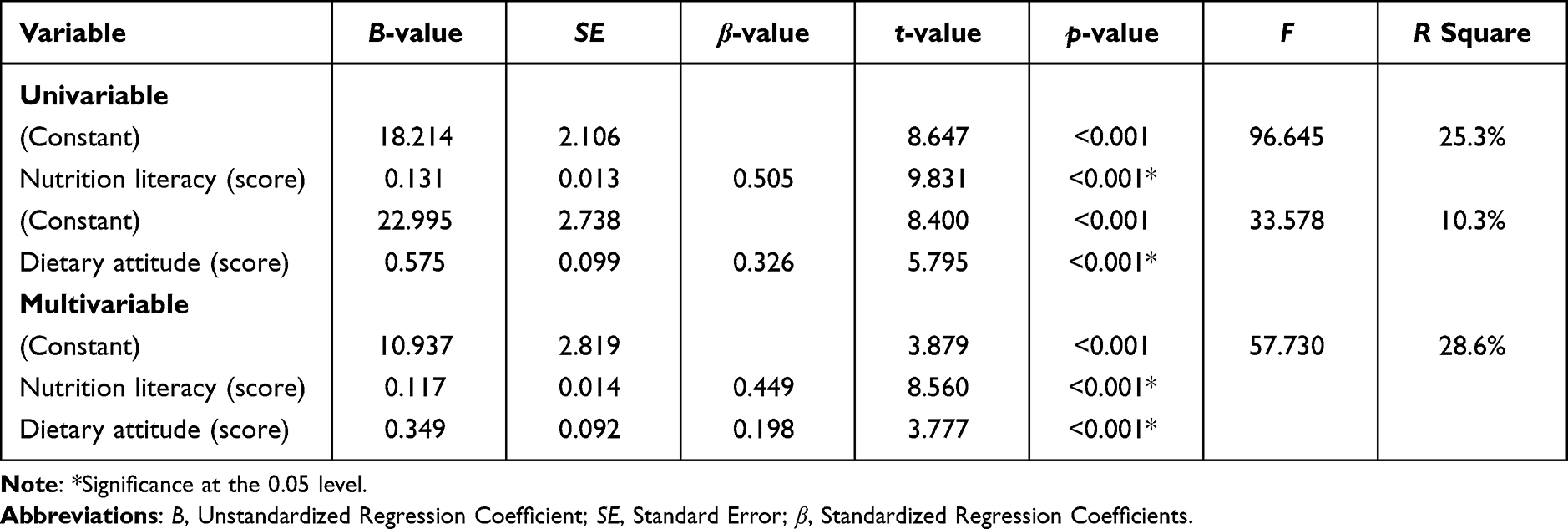 |
Table 4 Multiple Linear Regression Analysis of the Dietary Behavior Among Breast Cancer Patients Treated with Chemotherapy (n =284) |
Discussion
This study aims to explore the dietary behaviors among Chinese cancer patients treated with chemotherapy and to determine whether nutrition literacy and dietary attitude influence dietary behaviors with the guidance of the KAP model. To our knowledge, this is the first study to provide a direct assessment of dietary behaviors in such a specific cultural background and treatment condition without intervention.
The average dietary behavior score in this study was over 70% of the total possible score, demonstrating a high frequency of adopting a healthy diet. This finding is consistent with a previous study among Filipino cancer patients receiving chemotherapy, in which patients’ self-care strategies most often employed diet/nutrition/lifestyle change.33 The instrument to assess the level of dietary behavior primarily focuses on three elements: what to eat, how to eat and how much to eat. With respect to the type of foods, some items of the DNKAPQ assessed the diversity of food intake, and the score in this study demonstrated that participants had a high frequency of eating a variety of foods, which was different from another American survey targeting breast cancer survivors who completed chemotherapy, which found that 55.78% of patients did not eat sufficient fruits or vegetables.34 These differences in “what to eat” suggest that the intake of various healthy foods should be emphasized not only while breast cancer patients are undergoing chemotherapy but also during the survival period. Furthermore, the items of the DNKAPQ related to how to eat, including eating slowly, drinking more water, and gargling after eating, also revealed a high frequency of these behaviors, which was similar to other studies from Japan,35 Filipino33 and Australia.36 These similarities in “how to eat” seem to be generally recognized globally. With respect to how much to eat, the results demonstrated that most participants would force themselves to eat even if they had lost their appetite, which was in contrast to a previous study from Brazil reporting that only 41.8% of breast cancer patients were able to eat meals throughout the entire chemotherapy cycle, even when affected by chemotherapy-induced appetite loss.37 The primary reason for this difference may be that Chinese people attach great importance to diet, especially for cancer patients, where food plays a more active role in their disease recovery.16 Influenced by TCM, Chinese patients believe that “medicine and food homology” and daily foods can exert a large effect on regulating body function; thus family caregivers encourage Chinese patients to eat adequate food during chemotherapy to maintain the therapeutic effect and nutritional status. Thus, it is important for health professionals to educate Chinese breast cancer patients and their caregivers on the appropriate amounts of food intake, ensuring that the daily nutrient intake is up to the standard.
With respect to the level of participants’ reported nutrition literacy, the average nutrition literacy score in this study was over 70% of the total possible score, which was lower than that in a previous study of American breast cancer survivors, in which patients’ average nutrition literacy score was over 80% of the total possible score.38 However, differences in the assessment tool may lead to heterogeneity in the results. The latter study used the Nutrition Literacy Assessment Instrument for Breast Cancer Patients (NLit-BCa),39 and in this study, we adopted the NLMS-CA instrument, which was developed specifically for adult Chinese patients. In addition, the latter study focused on breast cancer survivors who had finished over 6 months of treatments, and such patients may be more familiar with nutritional knowledge during the long disease and treatment period, as they have formed and applied their own set of eating habits. Nevertheless, most of the participants enrolled in this study were primarily undergoing their first time of chemotherapy (91.9%), which led to unfamiliarity and fear. Moreover, Chinese patients are interested in complex TCM knowledge related to food contraindications and diet therapy, and breast cancer patients are also required to command extra knowledge about phytoestrogens.40 All of these factors increase the difficulty of achieving a high level of nutrition literacy. In addition, the results of the six dimensions of nutrition literacy demonstrated that the lowest average item score was content knowledge understanding, which was similar to a Polish study.41 An analysis of breast cancer patients’ understanding of educational materials revealed that only 46.1% passed a knowledge test relating to the content of the brochures. In addition, a study from Poland41 also reported that 60% of patients received educational materials in hospitals and that more than 2/3 of the respondents took the materials home, which could explain our result that the highest item average score among the six dimensions was knowledge reserve. The nutrition literacy results suggest that health professionals should pay more attention to providing Chinese breast cancer patients who are undergoing their first round of chemotherapy with targeted diet education and nutritional knowledge, especially information about TCM and phytoestrogens, with the use of plain language and videos to help them truly understand.
The average dietary attitude score was more than 70% of the total possible score, and the average item score was also higher than that of dietary behavior and nutrition literacy, which indicated a relatively positive attitude toward seeking a scientific diet after breast cancer disease and chemotherapy. These results were consistent with but may be statistically lower than those of a previous study from China that assessed patients with multiple cancer types who were undergoing chemotherapy, which reported that 95.2% of participants recognized that a scientific diet is important for cancer patients.27 Female breast cancer patients cooked for families or others, cared more about the nutritional intake and food preferences of their husbands and children, and sometimes ignored themselves even if they were diagnosed or receiving chemotherapy.42 Influenced by Confucian culture, Chinese females are more focused on the dedication to care for the daily needs of the, and their dietary attitude is easily influenced by families. The discrepancy suggest that although most Chinese breast cancer patients have a positive attitude toward a healthy diet during chemotherapy, health professionals and their families should also stimulate patients’ awareness of their own preferences and express thoughts about the relationship between diet and clinical factors.
Overall, participants’ dietary behaviors were positively influenced by their nutrition literacy and dietary attitudes according to the multiple linear regression analysis. The KAP model is widely applied in clinical conditions and research. Although several previous surveys have demonstrated the positive impact of health knowledge and attitudes on health behavior, the population and health topics were not focused on cancer patients’ diet and nutrition but rather teenagers’ nutrition KAP,43 KAP about therapeutic lifestyle changes in patients with hypertension,44 and KAP toward cancer prevention in the public population.45 In addition, some intervention studies38,46 have tested the effect of lifestyle-related education on breast cancer survivors’ knowledge and behaviors after they have finished all the treatments. Our study demonstrated that participants’ nutrition literacy and dietary attitudes may positively influence their dietary behaviors while on inpatient chemotherapy, which was consistent with another study that demonstrated that patients had a higher level of need for supportive care during treatment compared with long-term survivorship.47 One reason for this could be that patients suffer from more severe side effects during chemotherapy, which leads to a poor nutritional status,48 so they have a strong demand for nutrition knowledge and think highly of the effect of diet, further prompting patients to create coping strategies to eat well. The positive effects of patients’ nutrition literacy and dietary attitudes on dietary behaviors suggest that health professionals should emphasize breast cancer patients’ nutrition literacy and dietary attitudes during chemotherapy as well as during survivorship after the end of treatments, and education about dietary behavior improvement can be designed and applied to promote patients’ nutrition literacy and dietary attitude.
Additionally, several demographic and clinical characteristics exhibited significant differences with respect to dietary behavior. Patients between 31 and 40 years old had higher dietary behavior scores than patients of other ages. This result was similar to a study17 from the UK in which breast cancer patients under 40 years of age reported greater interest in cancer-related information. The probable reason may be that middle-aged breast cancer patients tend to have a greater ability and willingness to manage their own diet and health. Furthermore, overweight patients exhibited lower dietary behavior scores. Studies on the influence of BMI on health management have not attracted much attention until recent years, with little verified data and few conclusions. We hypothesize that overweight participants may exhibit a limited desire for healthy food and greater cravings for palatable food.49 Females who lived in urban areas exhibited higher dietary behavior scores. This result was consistent with another study50 from China that assessed cancer patients’ self-management behaviors after chemotherapy; however, the latter study did not provide significant information on specific dietary-related practices. The reason may be that large hospitals and high-quality medical resources in China are primarily concentrated in cities, and women who live in urban areas find it easier to obtain comprehensive and continuous health care. Furthermore, participants with a higher family income and higher educational level may exhibited better dietary behaviors. High-income Chinese breast cancer patients can easily obtain various sources of nutrition information and expensive supplements, such as ginseng, deer antler, Ejiao, turtle soup and other nutritional products promoted in TCM.51 This access may provide more options for them to engage in healthy dietary management. Patients with a higher educational level more easily mastered scientific dietary knowledge, and it is easier for such patients to take action and apply their knowledge to daily dietary practices, which has been recognized by a previous study.27 Employed patients exhibited better dietary behaviors than unemployed patients, possibly because working women had the intention to return to work after disease52 and were more eager to cooperate with disease treatment and lifestyle management. Premenopausal women also exhibited higher dietary behavior scores, which was consistent with results according to age. These participants were young and needed to consider foods that may affect estrogen levels.53 In addition, patients who had 3 or more comorbidities exhibited higher dietary behavior scores. Most of the existing literature54 focuses on the relationship between comorbidities and breast cancer risk, and we assumed that patients with many comorbidities may be more cautious of dietary management because many chronic diseases, such as diabetes and hypertension, have certain dietary requirements, and it is easier for these patients to develop healthy eating habits in daily life. Compared with patients who have not relapsed, patients who have relapsed exhibited better dietary behaviors. Although the survival rate of breast cancer is improving, there remains a high five-year recurrence rate. Patients who relapse may have a longer disease duration, have a better understanding of dietary knowledge and are more experienced in practice. Last, participants who received endocrine therapy exhibited better dietary behaviors, which may be explained by another similar study21 demonstrating that breast cancer patients who received endocrine therapy were less likely to adhere to recommended lifestyle guidelines. These findings suggest that health professionals should pay more attention to the dietary behavior of breast cancer patients who are older, overweight, unemployed, postmenopausal, live in rural areas, have fewer comorbidities, have a lower family income and education level, have not experienced disease relapse and have not had endocrine therapy; these patients should be offered targeted nutritional intervention.
Several limitations existed in this survey. Given its cross-sectional design, causal relationships cannot be firmly inferred. Furthermore, due to limited time and manpower, this survey only included three centers and primarily spanned central and southern China. Different geographical locations may have slightly different dietary habits and concepts, which may interfere with the representativeness of the results, and further studies should expand the survey scope and sample size. This is the first step in a series of studies. We initially intended to test whether nutrition literacy and dietary attitudes could influence dietary behavior. The specific factors associated with nutrition literacy and dietary attitudes will be further explored in the future. Moreover, the coefficient of association between dietary attitudes and nutrition literacy was small, which may limit further internal validation or pathway analysis. The relationship between the three variables will be examined in the future after expanding the sample size and sources. Last, the questionnaire-based survey may lead to patients who are not able to freely express their thoughts because the items are fixed and the assessment content is the same for each patient. Qualitative studies will be employed in the future to comprehensively explore breast cancer patients’ diet experiences and associated factors.
Conclusions
The findings demonstrate a moderate uptake of healthy dietary behaviors among Chinese breast cancer patients treated with chemotherapy. Among different demographic and clinical characteristics, patients who are older, overweight, unemployed, postmenopausal, live in rural areas, have fewer comorbidities, have a lower family income and education level, have not experienced disease relapse, and have not had endocrine therapy are inclined to engage in fewer healthy dietary behaviors. Additionally, patients’ nutrition literacy and dietary attitudes were found to positively influence their dietary behaviors. Targeted dietary and nutritional interventions to improve dietary behaviors should be designed and provided by health professionals to breast cancer patients treated with chemotherapy. To ensure the quality and specificity of future interventions, interventions should consider the nutrition literacy and dietary attitudes of patients during the intervention design period. Within our population, females who are older, overweight, unemployed, postmenopausal, live in rural areas, have fewer comorbidities, have a lower family income and education level, have not experienced disease relapse and have not received endocrine therapy are in urgent need of diet-specific interventions.
Data Sharing Statement
Data can be acquired by corresponding author’ permission. However, the whole work about this project has not yet been completed, data in this study may not shared.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the affiliated hospital of Zhengzhou University (Project identification code: 2020-KY-220).
Acknowledgments
We are especially grateful to all breast cancer patients and health professionals for their cooperation in the multicenter survey.
Funding
This work was supported by the National Natural Science Foundation of China (grant numbers 82173627), and only used as paper-based questionnaire printing and publication fees.
Disclosure
The authors declare no conflict of interest.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Wen D, Wen X, Yang Y, et al. Urban rural disparity in female breast cancer incidence rate in China and the increasing trend in parallel with socioeconomic development and urbanization in a rural setting. Thorac Cancer. 2018;9(2):262–272. doi:10.1111/1759-7714.12575
3. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J (Engl). 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
4. Ghafouri SN, Nayeri RW, McAndrew NP, et al. Chemotherapy regimen choice and patient outcomes in early-stage triple-negative breast cancer: a retrospective analysis. Ther Adv Med Oncol. 2022;14:7469708. doi:10.1177/17588359221085556
5. Yazbeck V, Alesi E, Myers J, et al. An overview of chemotoxicity and radiation toxicity in cancer therapy. Adv Cancer Res. 2022;155:1–27.
6. de Kruif AJ, Westerman MJ, Winkels RM, et al. Exploring changes in dietary intake, physical activity and body weight during chemotherapy in women with breast cancer: a Mixed-Methods Study[J]. J Hum Nutr Diet. 2021;34(3):550–561. doi:10.1111/jhn.12843
7. Marcelo CESI, Lúcia PLC. Health-related quality of life in women with breast cancer undergoing chemotherapy in Brazil. Int J Gen Med. 2021;14:10265–10270. doi:10.2147/IJGM.S343804
8. Phoosuwan N, Lundberg PC. Psychological distress and health-related quality of life among women with breast cancer: a descriptive cross-sectional study. Support Care Cancer. 2022;30(4):3177–3186. doi:10.1007/s00520-021-06763-z
9. Nguyen V, Chen J, Lord R, et al. The impact of multidisciplinary weight management on body weight and body mass composition in women with breast cancer post-adjuvant chemotherapy: a retrospective chart review. Oncology. 2022;100(6):344–353. doi:10.1159/000524519
10. Kwok A, Palermo C, Boltong A. Dietary experiences and support needs of women who gain weight following chemotherapy for breast cancer. Support Care Cancer. 2015;23(6):1561–1568. doi:10.1007/s00520-014-2496-5
11. Leng JCF, Gany F. Traditional Chinese medicine use among Chinese immigrant cancer patients. J Cancer Educ. 2014;29(1):56–61. doi:10.1007/s13187-013-0542-5
12. Parada HJ, Sun X, Tse CK, et al. Lifestyle patterns and survival following breast cancer in the Carolina breast cancer study. Epidemiology. 2019;30(1):83–92. doi:10.1097/EDE.0000000000000933
13. Bu T, Tang D, Liu Y, et al. Trends in dietary patterns and diet-related behaviors in China. Am J Health Behav. 2021;45(2):371–383. doi:10.5993/AJHB.45.2.15
14. Ceccatto V, Faria DPP, Nogueira PA, et al. Brazilian healthy eating index revised (BHEI-R) of women before and during adjuvant treatment for breast cancer. Nutr Hosp. 2014;30(5):1101–1109.
15. Harvie MN, Campbell IT, Baildam A, et al. Energy balance in early breast cancer patients receiving adjuvant chemotherapy. Breast Cancer Res Treat. 2004;83(3):201–210. doi:10.1023/B:BREA.0000014037.48744.fa
16. Cai YJ, Masaki H, Shi TY. Supportive care needs of Chinese women with newly diagnosed breast cancer prior to adjuvant chemotherapy. Oncol Nurs Forum. 2021;48(3):341–349. doi:10.1188/21.ONF.341-349
17. Melhem SJ, Nabhani-Gebara S, Kayyali R. Informational needs and predictors of Jordanian breast and colorectal cancer survivors: a national cross-sectional study. Support Care Cancer. 2022;30(8):6827–6837. doi:10.1007/s00520-022-07110-6
18. Krok-Schoen JL, Naughton MJ, Noonan AM, et al. Perspectives of survivorship care plans among older breast cancer survivors: a pilot study. Cancer Control. 2020;27(1):1073274820917208. doi:10.1177/1073274820917208
19. Adams N, Gisiger-camata S, Hardy CM, et al. Evaluating survivorship experiences and needs among rural African American breast cancer survivors. J Cancer Educ. 2017;32(2):264–271. doi:10.1007/s13187-015-0937-6
20. Kenne SE, Browall M, Gaston-Johansson F. Symptom burden clusters: a challenge for targeted symptom management. A longitudinal study examining symptom burden clusters in breast cancer. J Pain Symptom Manage. 2014;47(4):731–741. doi:10.1016/j.jpainsymman.2013.05.012
21. Ruddy KJ, Herrin J, Sangaralingham L, et al. Follow-up care for breast cancer survivors. J Natl Cancer Inst. 2020;112(1):111–113.
22. Krause C, Sommerhalder K, Beer-Borst S, et al. Just a subtle difference? Findings from a systematic review on definitions of nutrition literacy and food literacy. Health Promot Int. 2018;33(3):378–389. doi:10.1093/heapro/daw084
23. Zhang Y, Zhang Z, Xu M, et al. Development and validation of a food and nutrition literacy questionnaire for Chinese adults. Nutrients. 2022;14:9.
24. Maheri M, Bidar M, Farrokh-Eslamlou H, et al. Evaluation of anthropometric indices and their relationship with maternal nutritional literacy and selected socio-economic and demographic variables among children under 5 years old. Ital J Pediatr. 2022;48(1):137. doi:10.1186/s13052-022-01327-1
25. Zhou Y, Lyu Y, Zhao R, et al. Development and validation of nutrition literacy assessment instrument for Chinese pregnant women. Nutrients. 2022;14(14):2863. doi:10.3390/nu14142863
26. Costanzo ES, Lutgendorf SK, Roeder SL. Common-sense beliefs about cancer and health practices among women completing treatment for breast cancer. Psychooncology. 2011;20(1):53–61. doi:10.1002/pon.1707
27. Cong M, Wang J, Fang Y, et al. A multi-center survey on dietary knowledge and behavior among inpatients in oncology department. Support Care Cancer. 2018;26(7):2285–2292. doi:10.1007/s00520-018-4057-9
28. Cleland J. A critique of KAP studies and some suggestions for their improvement. Stud Fam Plann. 1973;4(2):42–47. doi:10.2307/1964829
29. Ni P, Chen J, Liu N. The sample size estimation in quantitative nursing research. Chin J Nurs. 2010;45(4):378–380.
30. Xu X. Development and Preliminary Application of Dietary Nutritional Knowledge, Attitude and Practice Questionnaire in Maligant Tumor Patients with Chemotherapy [dissertation]. Hengyang, China: University of South China; 2012.
31. Zhang Y Development and Evaluation of Nutrition literacy Measurement Scale for Chinese Adults: a pilot study in Anhui province [dissertation]. Bengbu, China: Bengbu Medical College; 2021.
32. Velardo S. Nutrition literacy for the health literate. J Nutr Educ Behav. 2017;49(2):183. doi:10.1016/j.jneb.2016.07.018
33. Williams PD, Balabagno AO, Manahan L, et al. Symptom monitoring and self-care practices among Filipino cancer patients. Cancer Nurs. 2010;33(1):37–46. doi:10.1097/NCC.0b013e3181b0f2b4
34. Twiss JJ, Gross GJ, Waltman NL, et al. Health behaviors in breast cancer survivors experiencing bone loss. J Am Acad Nurse Pract. 2006;18(10):471–481. doi:10.1111/j.1745-7599.2006.00165.x
35. Saito H, Watanabe Y, Sato K, et al. Effects of professional oral health care on reducing the risk of chemotherapy-induced oral mucositis. Support Care Cancer. 2014;22(11):2935–2940. doi:10.1007/s00520-014-2282-4
36. Terranova CO, Lawler SP, Spathonis K, et al. Breast cancer survivors’ experience of making weight, dietary and physical activity changes during participation in a weight loss intervention. Support Care Cancer. 2017;25(5):1455–1463. doi:10.1007/s00520-016-3542-2
37. Marinho ED, Custo Dio IDD, Ferreira IB, et al. Impact of chemotherapy on perceptions related to food intake in women with breast cancer: a prospective study. PLoS One. 2017;12(11):e0187573. doi:10.1371/journal.pone.0187573
38. Parekh N, Jiang J, Buchan M, et al. Nutrition literacy among cancer survivors: feasibility results from the healthy eating and living against breast cancer (HEAL-BCa) study: a pilot randomized controlled trial. J Cancer Educ. 2018;33(6):1239–1249. doi:10.1007/s13187-017-1238-z
39. Gibbs HD, Ellerbeck EF, Befort C, et al. Measuring nutrition literacy in breast cancer patients: development of a novel instrument. J Cancer Educ. 2016;31(3):493–499. doi:10.1007/s13187-015-0851-y
40. Li Y, Li S, Meng X, et al. Dietary natural products for prevention and treatment of breast cancer. Nutrients. 2017;9:7.
41. Kostecka M. The potential influence of dietary counseling on nutritional status and dietary supplement consumption in breast cancer patients: a pilot study. Nutr Cancer. 2019;71(5):749–755. doi:10.1080/01635581.2018.1531138
42. De Kruif AJ, Chrifou R, Langeslag GL, et al. Perceptions of non-Western immigrant women on having breast cancer and their experiences with treatment-related changes in body weight and lifestyle: a qualitative study. PLoS One. 2020;15(7):e0235662. doi:10.1371/journal.pone.0235662
43. Hamulka J, Wadolowska L, Hoffmann M, et al. Effect of an education program on nutrition knowledge, attitudes toward nutrition, diet quality, lifestyle, and body composition in polish teenagers. The ABC of healthy eating project: design, protocol, and methodology. Nutrients. 2018;10(10):1439. doi:10.3390/nu10101439
44. Abdalla AA. Knowledge, attitude and practice towards therapeutic lifestyle changes in the management of hypertension in Khartoum State. Cardiovasc J Afr. 2021;32(4):198–203. doi:10.5830/CVJA-2021-011
45. Karadeniz H, Cetinkaya F. Knowledge levels and attitudes of adult individuals about cancer and its risk factors. Niger J Clin Pract. 2020;23(11):1607–1614. doi:10.4103/njcp.njcp_434_19
46. Lisevick A, Cartmel B, Harrigan M, et al. Effect of the lifestyle, exercise, and nutrition (Lean) study on long-term weight loss maintenance in women with breast cancer. Nutrients. 2021;13(9):3265. doi:10.3390/nu13093265
47. Ktistaki P, Alevra N, Voulgari M. Long-term survival of women with breast cancer. overview supportive care needs assessment instruments. Adv Exp Med Biol. 2017;989:281–284.
48. Custódio I, Franco FP, Marinho E, et al. Prospective analysis of food consumption and nutritional status and the impact on the dietary inflammatory index in women with breast cancer during chemotherapy. Nutrients. 2019;11(11):2610. doi:10.3390/nu11112610
49. Salwa A, Zvolensky MJ, Kauffman B. The association between anxiety sensitivity and food cravings among individuals seeking treatment for weight-related behaviors. Eat Behav. 2023;48:101684. doi:10.1016/j.eatbeh.2022.101684
50. Lou Y, Yates P, Mccarthy A, et al. Self-management of chemotherapy-related nausea and vomiting: a cross-sectional survey of Chinese cancer patients. Cancer Nurs. 2014;37(2):126–138. doi:10.1097/NCC.0b013e318291b6f5
51. Lee MM, Shen JM. Dietary patterns using traditional Chinese medicine principles in epidemiological studies. Asia Pac J Clin Nutr. 2008;17(Suppl 1):79–81.
52. Schmidt ME, Scherer S, Wiskemann J, et al. Return to work after breast cancer: the role of treatment-related side effects and potential impact on quality of life. Eur J Cancer Care (Engl). 2019;28(4):e13051. doi:10.1111/ecc.13051
53. Filippone A, Rossi C, Rossi MM, et al. Endocrine disruptors in food, estrobolome and breast cancer. J Clin Med. 2023;12(9):3158. doi:10.3390/jcm12093158
54. Dalmartello M, Vermunt J, Parazzini F, et al. Comorbidity patterns, family history and breast cancer risk: a latent class analysis. J Epidemiol Community Health. 2022;16:219279.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test in Node-Negative Early Breast Cancer
Berdunov V, Millen S, Paramore A, Griffin J, Reynia S, Fryer N, Brown R, Longworth L
ClinicoEconomics and Outcomes Research 2022, 14:619-633
Published Date: 19 September 2022
Advice from One Patient to Another: Qualitative Analysis of Patients’ Perspectives About Chemotherapy Initiation
Malinowski C, Paredes E, Housten AJ, Chavez-MacGregor M
Patient Preference and Adherence 2022, 16:3283-3289
Published Date: 14 December 2022
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Comprehensive Knowledge, Attitudes, Behaviors, and Associated Factors of HIV/AIDS in Gondar City Public Health Facilities Among HIV Testing and Counselling Service Users, Northwest Ethiopia, 2022; an Ordinal Logistic Regression Analysis
Terefe B, Techane MA, Assimamaw NT
HIV/AIDS - Research and Palliative Care 2023, 15:713-726
Published Date: 7 December 2023
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test from a US Societal Perspective
Berdunov V, Cuyun Carter G, Laws E, Luo R, Russell CA, Campbell S, Abdou Y, Force J
ClinicoEconomics and Outcomes Research 2024, 16:471-482
Published Date: 4 June 2024