Back to Journals » Patient Preference and Adherence » Volume 16
Advice from One Patient to Another: Qualitative Analysis of Patients’ Perspectives About Chemotherapy Initiation
Authors Malinowski C ![]() , Paredes E, Housten AJ
, Paredes E, Housten AJ ![]() , Chavez-MacGregor M
, Chavez-MacGregor M
Received 24 August 2022
Accepted for publication 1 December 2022
Published 14 December 2022 Volume 2022:16 Pages 3283—3289
DOI https://doi.org/10.2147/PPA.S385997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Catalina Malinowski,1 Edna Paredes,2 Ashley J Housten,3 Mariana Chavez-MacGregor2,4
1Department of Health Services Research, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 2Department of Health Disparities Research, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 3Division of Public Health Sciences, Washington University School of Medicine, St Louis, MO, USA; 4Department of Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA
Correspondence: Mariana Chavez-MacGregor, 1400 Pressler St Unit 1444, Houston, TX, 77030, USA, Tel +1 713 563 0020, Email [email protected]
Purpose: Although the association between delays in (neo)adjuvant chemotherapy initiation and adverse outcomes is well-documented, patient perspective regarding the lived experience among those with breast cancer delay is sparse. Project Start was a qualitative study designed to assess and identify the multilevel factors contributing to the barriers and facilitators of initiating chemotherapy. This report explores specific responses where patients with breast cancer provide insight and advice for newly diagnosed women on preparing for chemotherapy initiation and informs potential interventions to facilitate timely chemotherapy initiation.
Patients and Methods: Women diagnosed with primary invasive breast cancer who experienced a ≥ 60-day delay in (neo)adjuvant chemotherapy initiation were included. Participants completed semi-structured interviews exploring barriers and facilitators to starting chemotherapy. Interviews were transcribed and coded to identify themes.
Results: We enrolled (N = 22) participants with a median age at diagnosis of 53.5 years (range 27– 70) who identified as Latina (n = 8), Black (n = 5), and non-Latina White (n = 9). Our participants indicated that engaging their medical teams and seeking support earlier were essential to initiate their treatment journeys. They emphasized being proactive and thorough in all aspects of their journey, particularly in processing medical recommendations, communicating with medical personnel, and identifying areas of need. Although explicit insight into chemotherapy delay was rare, participants expressed the importance of beginning treatment promptly. They shared advice on acquiring support (eg, financial, emotional, logistical, spiritual) and suggested connecting with breast cancer survivors to overcome the complex challenges of cancer care.
Conclusion: Patient perspectives regarding barriers and treatment facilitators help provide insight into the lived experience of cancer care journeys that can inform interventions to improve patient support and outcomes. We are using these results to develop a pilot study to test the acceptability and feasibility of a culturally tailored patient navigation intervention to increase self-efficacy and avoid treatment delays.
Keywords: breast cancer, care delivery, chemotherapy, treatment delay, oncology, qualitative, patient perspectives
Plain Language Summary
The use of adjuvant chemotherapy has a dramatic impact decreasing the risk of cancer recurrence and improving survival, however delays in the administration of adjuvant chemotherapy significantly reduce this benefit. Although chemotherapy administration delays are increasing and becoming more common in recent years, documentation of patient perspectives on their cancer care experiences are limited. We designed Project Start to evaluate factors at the operational, medical, and personal/social level, using a semi-structured interview guide, to gain participant insight into their cancer care journeys.
The focus of this analysis is on specific interview guide questions asking participants what they would tell other women upon receiving a breast cancer diagnosis. Participants described seeking support and engaging their medical teams early in their care journey as essential steps to initiate chemotherapy. Being proactive and thorough in all aspects of their care was critical to address and overcome barriers. Participants commonly expressed that beginning treatment promptly was important and discussed what they would have done differently knowing what they know now. Participants also shared advice on how to acquire different types of support (eg, financial, emotional, logistical, spiritual) and suggested connecting with breast cancer survivors to overcome the complex challenges of cancer care.
Findings are helping our research team inform the design of a pilot study to test the acceptability and feasibility of a patient navigation intervention aimed at reducing time to chemotherapy. This information can provide insight for newly diagnosed women on preparing for chemotherapy initiation and inform potential interventions to facilitate chemotherapy initiation. Our objectives are patient-centered and have the potential to improve outcomes and reduce health disparities.
Introduction
Over the past few decades, there have been considerable improvements in cancer care treatment. Unfortunately, the increasingly complex and long treatments needed to improve health-related outcomes often involve navigating a challenging healthcare system that can result in delays from diagnosis to treatment initiation. It is known that delays in treatment initiation have a detrimental impact on breast cancer (BC) outcomes.1–4 However, despite this, delays persist. In addition, patient insight to the cancer care journey from BC diagnosis to treatment is limited, with fewer studies incorporating patient perspectives into interventions to reduce delay.
Project START (NCT04087057) was a qualitative study aimed to assess and identify multi-level factors contributing to barriers and facilitators of initiating chemotherapy.5 Our team recruited breast cancer patients to characterize the determinants of delays in starting chemotherapy.5 In this brief report we explore specific responses related to patient perspectives into the breast cancer experience, especially highlighting advice shared for newly diagnosed women on preparing for chemotherapy initiation.
Materials and Methods
We conducted semi-structured, one-on-one interviews lasting approximately 60-minutes in-person or over the phone. Guided by extant literature1,6 and social determinants of health,7 the semi-structured interview guide was developed and pilot tested by research team members with extensive qualitative experience, as previously reported.5 Interviews included a discussion of 1) attitudes and perceptions associated with chemotherapy and 2) barriers to initiation of chemotherapy (Appendix). Questions were designed to probe for the potential impact of multi-level barriers and facilitators at medical, system, and patient-levels. This report, details participant responses to questions 11 and 13 where direct advice and insight into their breast cancer experience was provided for newly diagnosed women.
English- or Spanish-speaking women ages ≥18, diagnosed with primary invasive breast cancer within three years of enrollment were recruited (10/2019-10/2020) at a single academic cancer center. Patients received their first dose of adjuvant chemotherapy ≥60 days after definitive breast cancer surgery or ≥60 days after pathological diagnosis for participants treated with neoadjuvant chemotherapy. Participants were identified via chart review, and those meeting inclusion criteria were approached either in-person or by telephone. A detailed description of the study was provided, and participants signed informed consent. This study was approved by the University of Texas MD Anderson Cancer Center Institutional Review Board (IRB Number: 2018–1133).
Sociodemographic characteristics and relevant clinical information were collected from the medical record. Health literacy, numeracy, physician trust, and social support were assessed using the 3-item-Brief Health Literacy Screener,8 3-item-Subjective Numeracy Scale,9 Interpersonal Trust in a Physician Scale,10 and Berlin Social Support Subscale,11 respectively. Questions were administered and recorded electronically using REDCap.12 Survey items were presented visually on a tablet screen. Interviews were audio-recorded and transcribed verbatim. Professional translation services were used for interviews completed in Spanish.
For the qualitative analysis, we partnered with ResearchTalk (http://www.researchtalk.com/), a leader qualitative methodology and analysis, to use the Sort and Sift, Think and Shift analytic approach.13–15 This rigorous analytic approach incorporates core principles from phenomenology, grounded theory, narrative research, and case study. Specifically, for the “diving in” phase, team members (CM, EP, AJH, MCM, ResearchTalk) independently read four transcripts identifying powerful quotations to develop data summaries. Quotations were reviewed to create a list of core topics to monitor (coding) throughout the analysis of all project transcripts. This list featured deductive topics from the interview guide and inductive topics unearthed during the initial “diving in” phase. We created episode profiles (holistic depictions) for each individual transcript. Team members reviewed and discussed all transcripts and episode profiles, working together to update the core topics to monitor list throughout analysis. During the “stepping back” phase, the team mined codes within the episode profiles. We identified themes specifically related to advice participants would give to other patients to help them initiate BC treatment.
Results
Of 63 potentially eligible patients contacted, 22 consented to participate (median age at diagnosis 53.5 years [range 27–70]). Participants identified as: Black (B; n=5); Hispanic/Latina (H/L; n=8); and non-Latina White (NLW; n=9). Most completed interviews in English (n=15), and over half had lower educational attainment (n=12). Table 1 shows participants characteristics. Our analysis identified that initiating care, completing treatment, and obtaining support were consistent themes across participant advice. This included acquiring support (eg, financial, emotional, logistical, spiritual) and emphasized the importance of “mind-over-matter” to overcome challenges throughout their cancer care journey.
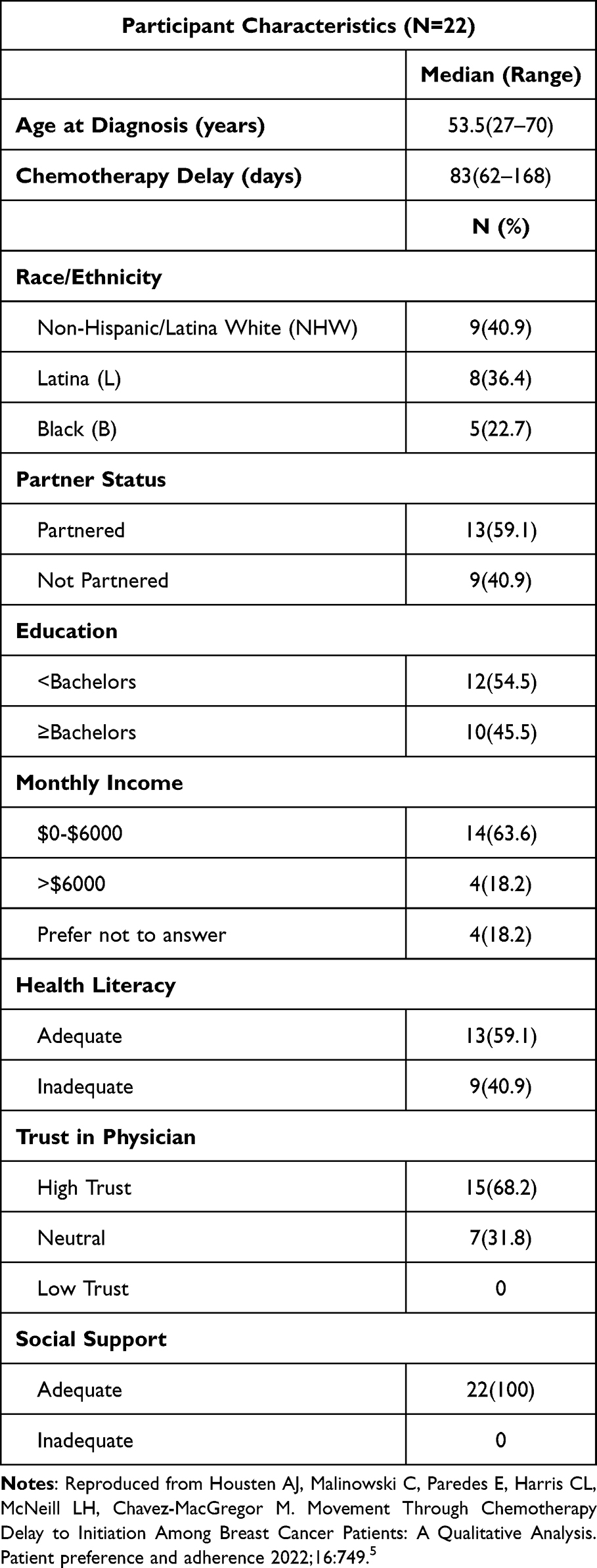 |
Table 1 Sociodemographic Characteristics |
Breast Cancer Survivor Recommendations
During receipt of diagnosis and treatment recommendations, participants recalled experiencing multiple emotions, including shock, disbelief, fear, and denial; yet all participants initiated and completed treatment. When asked what advice participants would give someone about to start chemotherapy, participants urged other women to draw on strength from others and,
… not to be scared because it is all for the better. It got better for me day by day, time by time. And I took it one day at a time, and here I am today, I am still here. (Participant[P]3-H/L-54 years[y])
Patience, “grounding energy”, and drawing strength from faith were suggestions from another participant, who asks women to,
be patient not just with the folks who try to help you but be patient with yourself. It is a process and it advents your life for a little bit, but it’s just for a little bit. If you are a person of faith pray, take a deep breath, and just try to ground yourself and say this too shall pass, and just move on from there. (P18-NHW-60y)
Participants expressed ways to prepare your body, both mentally and physically, and to
be prepared for what your body is going to go through… what I did before was [exercising to] get my strength up and drank a lot of water. I did everything they told me to do, in preparing my body for it, and I do feel like it helped a lot. I felt like because I was told [what was going to happen], I knew how to mentally prepare and deal with it. (P13-H/L-41y)
It is also important to plan for additional support to handle day-to-day tasks by
making a plan that you’re not going to be doing much. Focus on yourself … if you are married and have a spouse, have a significant other, person, or family, someone needs to be with you. I can’t imagine going through this by myself. I know people have done it [alone] … but it made such a difference having family [support]. (P06-NHW-65y)
Importance of planning and organization was also emphasized,
I would definitely say plan as much as you can. To how you plan on getting things done because [chemotherapy] really did wipe me out, as far as physically, with fatigue…definitely [get] help with your meals. I mean most of the time I didn’t want to eat anything anyway; people would have to kind of encourage me to eat but planning everything out. (P20-NHW-52y)
Participants emphasized the importance of engaging medical teams and taking an active role in all aspects of their cancer care journey. When processing medical recommendations,
[women should] research as much possible [about their diagnosis], and just make sure they look at everything, talk to a doctor, and ask a lot of questions. Feel assured, that they are doing the right thing, and that the doctors are choosing the right treatment for them. (P08-H/L-45y)
Communication with medical personnel should continue once treatment is initiated by continued engagement in care throughout the course of treatment by
really communicating with your doctor, [as] they had to try several different medications, to try to manage side effects with me, so communicating with your doctor upfront as soon as you have an issue, so they can try to resolve it before it becomes too complex. (P20-NHW-52y)
Drawing support from others is key at the beginning of the cancer care journey – women should “talk to as many people as you want to or you can and go from there (P13-H/L-41y).” One participant recalled
something someone shared with me is that [tackling chemotherapy] is all about your attitude and it is definitely true. Praying and keeping the faith, [know] that it is going to be all right and that is it. (P23-B-57y)
Connecting with breast cancer survivors before and during treatment was crucial,
the women [who had gone through this] and talk[ed] to me were super important… I would be willing to do anything that I can for women who are going through this or will be going through this…whatever I can do. (P19-H/L-58y)
Discussion
Our findings provide insight for newly diagnosed women on preparing for chemotherapy initiation and how to remain engaged throughout the treatment process. After receiving chemotherapy, participants describe emotional, spiritual, financial, and logistical support as key factors to prepare for and initiate treatment. Participants described the importance of a “mind over matter” attitude to initiate their cancer care – yet while this attitude is an individual accomplishment, various external support may be needed to empower patients. Participants described family, friends, community, and BC survivors as vital sources of support to initiate chemotherapy.
Despite insight into patients’ lived experiences being critical in medical assessment and clinical care,16,17 literature encompassing BC care perspectives remains scarce.18,19 The effectiveness of healthcare extends beyond cancer outcomes to quality of life. Specifically, existing research corroborate psychosocial and socioeconomic burdens play key roles in patients’ medical experiences5 and have been shown to adversely impact outcomes.20–22 These perspectives highlight how women’s needs throughout the BC experience grow in complexity alongside treatment, thus requiring support beyond medical treatment to incorporate factors related to quality of life.
In response to our exploratory research, we have developed a needs assessment checklist to guide a patient navigation pilot, Project Let’s Start. Patient navigation is an effective approach to increase mammography screening and improve adherence among socially marginalized populations23 by reducing barriers and facilitating timely access to care.24 We believe that using both resources together can improve cancer outcomes by empowering patients to engage in their treatment and take active roles in their care.
Empowerment is critical for patient engagement in cancer care25 – many participants described BC as something that was “happening to them”. With the needs assessment checklist, patients can assess their personal needs upon receiving their diagnosis and develop action items for discourse with patient navigators to overcome barriers to care. In this process, patients enhance their self-efficacy and sense of control over their medical diagnoses. Our goal is to test the acceptability and feasibility of a culturally-tailored patient navigation intervention to reduce treatment delays and increase self-efficacy, particularly in lower resource settings.
Limitations
A limitation of our study is that participants were recruited from a single large, academic cancer center. Despite this, approximately half of the participants identified as Black or Latina, roughly half reported less than a college degree, and about 40% had limited health literacy. While none of our participants reported distrust in their physician using the Trust in Physician Scale, this measure has demonstrated ceiling effects and may not adequately reflect the multiple constructs contributing to trust.26 High social support observed in our participant sample may indicate limitations of the measure used. Despite this, our research approach leveraged qualitative methodology to elucidate and capture the depth and complexity of trust and social support. Additionally, participants demonstrated limited insight into their delay, it is possible that delay was not discussed during their clinical care. Recall bias is another potential limitation due to inclusion of patients treated up to three years ago. Future work investigating clinical conversations regarding delay may be warranted.
Conclusion
Patients outlined the benefit of attaining support outside of their medical teams to overcome barriers and initiate treatment promptly. Family, friends, and connecting with BC survivors were vital in achieving activation and supporting quality of life. Patient perspectives regarding barriers and treatment facilitators provide essential insight into cancer care journeys and can inform interventions to support patients and improve outcomes. Patient experiences and advice from BC survivors bring important and practical insight on ways to navigate cancer treatment.
Data Statement
The data that support the findings of this study are available on reasonable request from the corresponding author. The data are not publicly available due to privacy or ethical considerations.
Acknowledgment
Findings from this presentation were presented, in part, at the American Society of Clinical Oncology (ASCO) Quality Care Symposium in September 2022. The authors declare that the procedures were followed according to the regulations established by the Clinical Research and Ethics Committee and to the Helsinki Declaration of the World Medical Association.
Funding
This research was supported by Conquer Cancer, The ASCO Foundation, and NIH/NCI P30CA016672. MCM is supported by Susan G. Komen SAC220221, SAC150061, and BCRF-22-190. AJH is supported by R00MD011485. The funder did not play a role in the design of the study; the collection, analysis, and interpretation of the data; the writing of the manuscript; and the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chavez-MacGregor M, Clarke CA, Lichtensztajn DY, Giordano SH. Delayed initiation of adjuvant chemotherapy among patients with breast cancer. JAMA Oncol. 2016;2:322–329. doi:10.1001/jamaoncol.2015.3856
2. Smith-Graziani D, Lei X, Giordano SH, Zhao H, Karuturi M, Chavez-MacGregor M. Delayed initiation of adjuvant chemotherapy in older women with breast cancer. Cancer Med. 2020;9:6961–6971. doi:10.1002/cam4.3363
3. de Melo Gagliato D, Gonzalez-Angulo AM, Lei X, et al. Clinical impact of delaying initiation of adjuvant chemotherapy in patients with breast cancer. J Clin Oncol. 2014;32:735–744. doi:10.1200/JCO.2013.49.7693
4. Bleicher RJ. Timing and delays in breast cancer evaluation and treatment. Ann Surg Oncol. 2018;25:2829–2838. doi:10.1245/s10434-018-6615-2
5. Housten AJ, Malinowski C, Paredes E, Harris CL, McNeill LH, Chavez-MacGregor M. Movement Through chemotherapy delay to initiation among breast cancer patients: a qualitative analysis. Patient Prefer Adherence. 2022;16:749. doi:10.2147/PPA.S350412
6. de Melo Gagliato D, Lei X, Giordano SH, et al. Impact of delayed neoadjuvant systemic chemotherapy on overall survival among patients with breast cancer. Oncologist. 2020;25:749–757. doi:10.1634/theoncologist.2019-0744
7. Gerend MA, Pai M. Social determinants of Black-White disparities in breast cancer mortality: a review. Cancer Epidemiol Prev Biomark. 2008;17:2913–2923. doi:10.1158/1055-9965.EPI-07-0633
8. Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients with inadequate health literacy; 2004.
9. McNaughton CD, Cavanaugh KL, Kripalani S, Rothman RL, Wallston KA. Validation of a short, 3-item version of the subjective numeracy scale. Medical Decision Making. 2015;35:932–936. doi:10.1177/0272989X15581800
10. Hall MA, Camacho F, Dugan E, Balkrishnan R. Trust in the medical profession: conceptual and measurement issues. Health Serv Res. 2002;37:1419–1439. doi:10.1111/1475-6773.01070
11. Schulz U, Schwarzer R. Soziale Unterstützung bei der Krankheitsbewältigung: die Berliner Social Support Skalen (BSSS). [Social Support in Coping with Illness: the Berlin Social Support Scales (BSSS)]. Diagnostica. 2003;49:73–82. doi:10.1026//0012-1924.49.2.73
12. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381. doi:10.1016/j.jbi.2008.08.010
13. Fryer CS, Passmore SR, Maietta RC, et al. The symbolic value and limitations of racial concordance in minority research engagement. Qual Health Res. 2016;26:830–841. doi:10.1177/1049732315575708
14. Maietta RC. State of the art: integrating software with qualitative analysis. In: Curry L, Shield R, Wetle T, editors. Applying Qualitative and Mixed Methods in Aging and Public Health Research. American Public Health Association and the Gerontological Society of America; 2006.
15. Maietta R, Mihas P, Swartout K, Petruzzelli J, Hamilton AB. Sort and Sift, think and shift: let the data be your guide an applied approach to working with, learning from, and privileging qualitative data. Qualitative Report. 2021;26:16.
16. Zanini C, Sarzi-Puttini P, Atzeni F, Di Franco M, Rubinelli S. Doctors’ insights into the patient perspective: a qualitative study in the field of chronic pain. Biomed Res Int. 2014;2014:1–6. doi:10.1155/2014/514230
17. McKinley SK, Boland GM. The patient speaks: importance of patient perspectives in clinical decision-making. Ann Surg Oncol. 2019;26:2665–2666. doi:10.1245/s10434-019-07575-6
18. Binkley JM, Harris SR, Levangie PK, et al. Patient perspectives on breast cancer treatment side effects and the prospective surveillance model for physical rehabilitation for women with breast cancer. Cancer. 2012;118:2207–2216. doi:10.1002/cncr.27469
19. Prakash A, Sardar M, Shaikh N, et al. The perspective of a breast cancer patient: a survey study assessing needs and expectations. Cureus. 2020;12:e9171.
20. Willis L, Goodwin J, Lee K-O, et al. Impact of psychosocial factors on health outcomes in the elderly: a prospective study. J Aging Health. 1997;9:396–414. doi:10.1177/089826439700900307
21. Coughlin SS. Social determinants of breast cancer risk, stage, and survival. Breast Cancer Res Treat. 2019;177:537–548. doi:10.1007/s10549-019-05340-7
22. Unger JM, Moseley AB, Cheung CK, et al. Persistent disparity: socioeconomic deprivation and cancer outcomes in patients treated in clinical trials. J Clin Oncol. 2021;39:1339–1348. doi:10.1200/JCO.20.02602
23. Nelson HD, Cantor A, Wagner J, et al. Effectiveness of patient navigation to increase cancer screening in populations adversely affected by health disparities: a meta-analysis. J Gen Intern Med. 2020;35:3026–3035. doi:10.1007/s11606-020-06020-9
24. Baik SH, Gallo LC, Wells KJ. Patient navigation in breast cancer treatment and survivorship: a systematic review. J Clin Oncol. 2016;34(30):3686–3696. doi:10.1200/JCO.2016.67.5454
25. Joergensen C, Thomsen TG, Ross L, et al. What facilitates” patient empowerment” in cancer patients during follow-up. Acta oncologica. 2017;56(2):156–165. doi:10.1080/0284186X.2016.1267402
26. Müller E, Zill JM, Dirmaier J, Härter M, Scholl I. Assessment of trust in physician: a systematic review of measures. PLoS One. 2014;9:e106844. doi:10.1371/journal.pone.0106844
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test in Node-Negative Early Breast Cancer
Berdunov V, Millen S, Paramore A, Griffin J, Reynia S, Fryer N, Brown R, Longworth L
ClinicoEconomics and Outcomes Research 2022, 14:619-633
Published Date: 19 September 2022
Identifying Recurrences Among Non-Metastatic Colorectal Cancer Patients Using National Health Data Registries: Validation and Optimization of a Registry-Based Algorithm in a Modern Danish Cohort
Nors J, Mattesen TB, Cronin-Fenton D, Mailhac A, Bramsen JB, Gotschalck KA, Erichsen R, Andersen CL
Clinical Epidemiology 2023, 15:241-250
Published Date: 27 February 2023
Dietary Behavior and Its Association with Nutrition Literacy and Dietary Attitude Among Breast Cancer Patients Treated with Chemotherapy: A Multicenter Survey of Hospitals in China
Tang H, Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L
Patient Preference and Adherence 2023, 17:1407-1419
Published Date: 9 June 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test from a US Societal Perspective
Berdunov V, Cuyun Carter G, Laws E, Luo R, Russell CA, Campbell S, Abdou Y, Force J
ClinicoEconomics and Outcomes Research 2024, 16:471-482
Published Date: 4 June 2024