Back to Journals » International Journal of General Medicine » Volume 19
Symptom Clusters and Sentinel Symptoms in Heart Failure Patients: A Cross-Sectional Survey
Authors Li Y, Xu M, Jia W, Ma J ![]() , Guo S, Yao L
, Guo S, Yao L
Received 13 March 2026
Accepted for publication 12 June 2026
Published 23 June 2026 Volume 2026:19 607704
DOI https://doi.org/10.2147/IJGM.S607704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Yanran Li,1 Min Xu,1 Wei Jia,1 Jing Ma,1 Shuping Guo,2 Li Yao3
1School of Nursing, Ningxia Medical University, Yinchuan, 750004, People’s Republic of China; 2Nursing Department, The General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China; 3Department of Cardiology, The General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China
Correspondence: Li Yao, Department of Cardiology, The General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China, Email [email protected] Shuping Guo, Nursing Department, The General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China, Email [email protected]
Purpose: To explore the symptom clusters of heart failure (HF) patients, identify the sentinel symptom of each symptom cluster, and provide a basis for the implementation of precise symptom management.
Patients and Methods: The study participants were recruited using convenience sampling from inpatients admitted to the cardiology department between November 2024 and January 2025, including patients admitted for acute HF, chronic HF, and acute decompensation of chronic HF. The General Information Questionnaire and the Memorial Symptom Assessment Scale were used for the survey. Symptom clusters were explored using principal component analysis, sentinel symptoms were explored using the Apriori algorithm.
Results: A total of 354 HF patients participated in the study. Four symptom clusters were identified in HF patients: the nocturnal respiratory distress symptom cluster, the low perfusion symptom cluster, the upper airway irritation symptom cluster, and the gastrointestinal symptom cluster. Three sentinel symptoms were explored: waking up breathless at night, sweating and cough.
Conclusion: HF patients have a variety of symptoms in the form of four symptom clusters, waking up breathless at night, sweating and cough are the sentinel symptoms. Medical staff can take sentinel symptoms as the focus of symptom cluster evaluation and targeted intervention, which can improve the efficiency of symptom cluster management and reduce patients’ symptom burden.
Keywords: heart failure, symptom clusters, sentinel symptoms, nursing
Introduction
Heart failure (HF) is a complex clinical syndrome arising from structural and/or functional abnormalities of the heart that impair ventricular filling and/or ejection function, and it represents the severe and terminal stage of various cardiac diseases,1 which characterised by high prevalence rates, high readmission rates, high mortality rates, multiple coexisting conditions, and an increasingly younger age of onset.2 HF has affected an estimated 64.3 million individuals worldwide,3 with a prevalence of 1.1% in the Chinese population.1 HF is associated with an extremely poor prognosis. Among hospitalized patients with HF, the 1-year mortality rate is as high as 23.6%,4 and the 5-year mortality rate remains close to 50%.5 The annual economic burden attributable to HF is approximately 108 billion,6 and the substantial costs associated with hospitalizations and long-term care for HF patients pose a considerable drain on healthcare systems and the individual households.
Unfortunately, even patients with optimally managed HF experience substantial symptom burden and are trapped in a vicious cycle of symptom exacerbation, remission, and recurrence.7 Patients with HF typically experience with a variety of symptoms, which include dyspnea,8 fatigue,9 edema10 and so on. On average, each patient experiences between 5 and 15 symptoms during the progression of their condition.11 These symptoms often emerge simultaneously rather than in isolation,12 and some of these symptoms interact synergistically, reinforcing one another to form symptom clusters.13 Dodd et al14 first introduced the concept of the “symptom cluster” in 2001, Which refers to 3 or more symptoms that occur simultaneously and are interrelated, yet do not necessarily share the same pathophysiological mechanisms. In 2005, Kim et al15 defined this concept and proposed that a symptom cluster consists of 2 or more interrelated symptoms that occur simultaneously. The correlations among symptoms within one cluster are stronger than those across different clusters, and symptoms in a cluster may or may not share the same etiology. This view has been widely recognized, and the current study adopts this conceptual definition of symptom clusters.
Due to the synergistic effects of symptoms within a cluster, symptom clusters have a more detrimental impact on patients’ physical and mental health and prognosis than do individual symptoms. Although symptom clusters facilitate symptom classification and management, and have improved patients’ quality of life to some extent,16 challenges in managing these clusters remain.If treatment focuses solely on a single symptom without clearly differentiating between primary and secondary factors, the result may be suboptimal management. However, addressing each symptom individually would create additional burden for both medical staff and patients. Therefore, investigating whether a particular symptom within a symptom cluster can influence the onset or progression of other symptoms, and identifying intervention targets, can help address the challenges in managing symptom clusters.
Brown et al17 first proposed the concept of sentinel symptoms in 2011. Sentinel symptoms are the earliest indicators of a symptom cluster and can predict the emergence and trend of other symptoms.18 They are also the key triggers of other symptoms within the cluster, characterized by sensitivity, significance, prevalence, and driving properties.19 Because sentinel symptoms can precipitate the onset or worsening of other symptoms, recognizing these early warning signs is crucial for timely identification and effective management of the cluster. Therefore, in clinical practice, sentinel symptoms can serve as a starting point for managing symptom clusters. Thus, they not only help alleviate the onset or progression of related symptoms but also simplify the assessment of symptom clusters and improve efficiency;20 moreover, this approach is of great significance for the implementation of symptom specific nursing care.21
Current research has focused on identifying symptom clusters in HF patients; however, methodological and instrumental heterogeneity across studies has led to variations in the resulting symptom profiles.22,23 Currently, investigations into sentinel symptoms have predominantly been conducted in the context of cancers such as breast,24 lung,25 and gastric cancer,26 while research on sentinel symptoms in HF patients remains in its infancy. This is of great significance for the implementation of symptom-specific nursing care. It is currently unclear whether patients with HF exhibit sentinel symptoms. Therefore, the present study aimed to analyze symptom clusters in patients with HF, to identify sentinel symptoms within each cluster, and to provide a basis for delivering precise treatment and care to HF patients.
Study Design and Patients
This cross-sectional study employed convenience sampling. We recruited patients who were hospitalized in the cardiology department of a tertiary hospital in Ningxia Hui Autonomous Region from November 2024 to January 2025. The study received approval from the Ethics Review Committee of The General Hospital of Ningxia Medical University (No.KYLL-2024-0145) and was performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants prior to the survey. According to the factor analysis sample size estimation method, the sample size should be 10 times the number of entries.27 This study analyzed 32 symptom entries. To account for potential invalid data, an additional 10% was added, setting the final target sample size at 352 participants. In total, 360 questionnaires were distributed, and 354 valid questionnaires were included in this study, with a response rate of 98.3%. The inclusion criteria for participation were as follows: 1. Patients who met the diagnostic criteria in the “Chinese Heart Failure Diagnosis and Treatment Guidelines 2024”,28 2. Age 18 years or older, 3. The ability to complete the questionnaire in written or oral form. The exclusion criteria were as follows: such as severe liver failure,29 severe kidney failure requiring dialysis,30 or advanced malignant tumors.
Measures
Sociodemographic and Clinical Characteristics
The sociodemographic information included gender, age, marital status, residence, education, employment status, household income, smoking history, drinking history and so on. Clinical characteristics included New York Heart Association (NYHA) functional classification,31 annual hospitalization frequency, family history, comorbidities, medication types, the duration of HF diagnosis, left ventricular ejection fraction (LVEF, %) and so on.
Memorial Symptom Assessment Scale, MASAS-HF
The MASAS-HF was utilised to assess the incidence of symptoms and severity by HF patients. This scale was adapted in 2004 by Zambroski et al from the content of the Tumor Assessment Scale.32 Guo et al translated the MASAS-HF into Chinese in 2014.33 This 32-item scale consists of three dimensions: physical (21 items), psychological (6 items), and HF (5 items) symptoms. Likert-type scale ranges from 1 (not at all) to 4 (very much). The higher the entry score, the more severe the subject′s symptoms were for that entry. The Cronbach′ s α coefficient for this scale ranged from 0.807 to 0.946, and its content validity index was 0.712.
Data Collection
The questionnaire was collected by 2 investigators who had undergone standardised training.
Investigators explained to respondents how to complete the questionnaire and the precautions to be taken to ensure that they answered the questionnaire independently and based on a full understanding of it. For patients who were unable to fill in the form on their own, the investigator completed it on their behalf using uniform guidance and asking questions one by one. The Sociodemographic and Clinical Characteristic was filled out by investigators according to the electronic medical record system. The MASAS-HF was completed by participants. After collection of the questionnaires, investigators checked and eliminated the questionnaires that had incomplete information. Data was entered by 2 investigators working in tandem to minimise errors and omissions.
Statistical Analysis
Data analysis was performed using SPSS 28.0 and SPSS modeler 18.0. Firstly, count data were described using frequency and composition ratios; normally distributed data were described using mean ± standard deviation. Non-normal data were presented as medians accompanied by interquartile ranges (P25, P75). Secondly, exploratory factor analysis was performed using the maximum variance method for factor rotation to identify symptom clusters. Symptoms that had an incidence of <30% were excluded from the analysis. The suitability of the data for factor analysis was assessed using the KMO test and Bartlett’s test of sphericity. The criteria for factor selection were as follows: (1) eigenvalue≥ 1; (2) each factor must include at least two symptoms; (3) the symptom loading must be≥ 0.4. Thirdly, in conducting correlation analysis with the Apriori algorithm, support and confidence serve as the standard metrics for evaluating relationships between symptoms.25 The sentinel symptoms were detected based on Apriori algorithm, the support was greater than 40%, confidence was greater than 60% and confidence was greater than support, Which means that there were effective relationships between the two symptoms.34
Results
Characteristics of Heart Failure Patients
A total of 354 patients with HF were recruited in this study, general information is shown in Table 1.
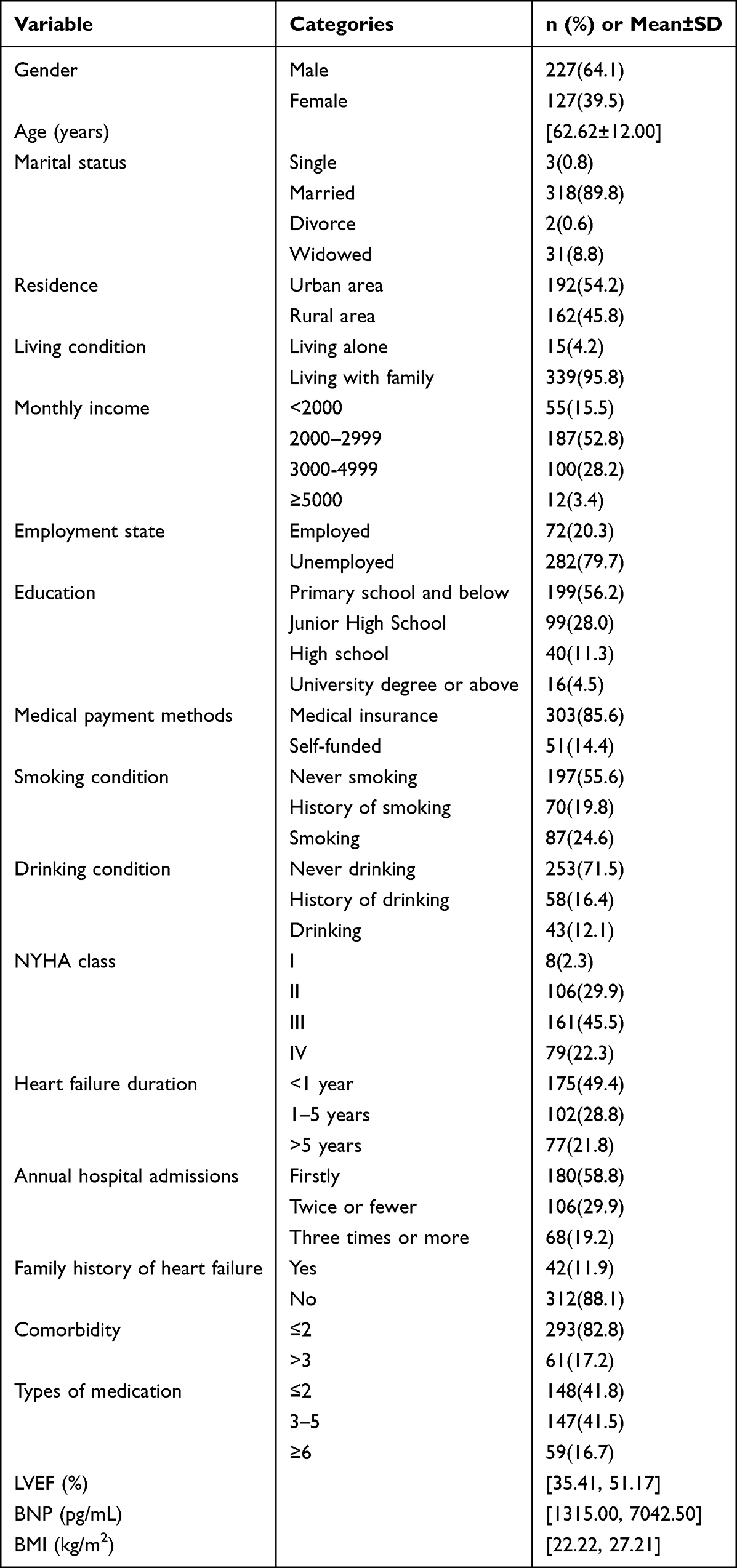 |
Table 1 The General Characteristics of Participants (N=354) |
Symptom Clusters in Heart Failure Patients
The test of applicability showed that this study had a KMO value of 0.624 and Bartlett’s spherical test P <0.01, making it suitable for factor analysis. A total of five factors with eigenvalues >1 were extracted, and the cumulative variance contribution rate was 57.833%. As each factor encompasses at least two symptoms, chest pain has not been included within the symptom cluster. Consequently, four symptom clusters were identified and named respectively as: nocturnal respiratory distress symptom cluster, low perfusion symptom cluster, upper airway irritation symptom cluster and gastrointestinal symptom cluster, which are shown in Table 2.
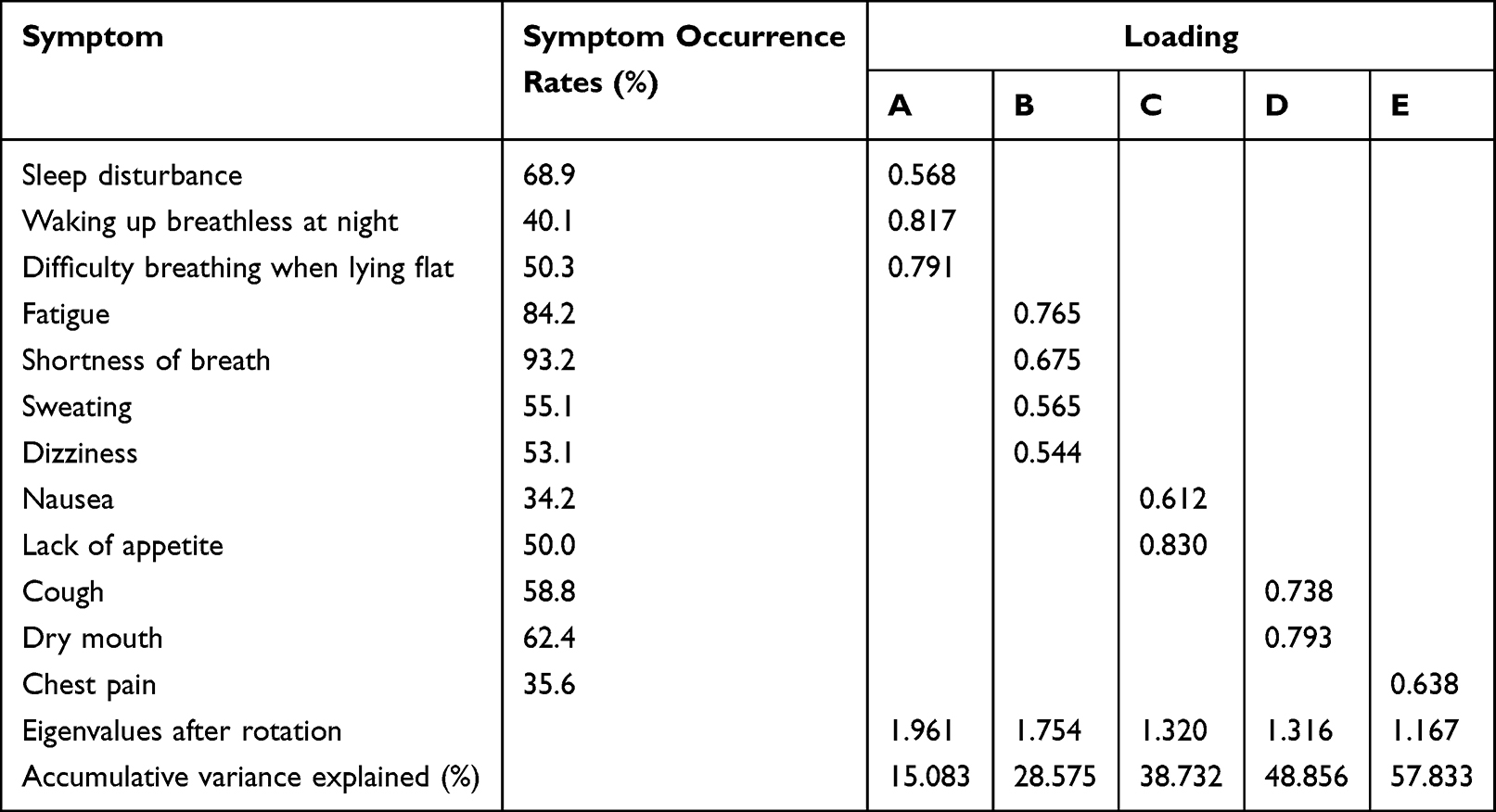 |
Table 2 The Description of Symptoms and Symptom Clusters (N=354) |
Sentinel Symptoms Within 4 Symptom Clusters in Heart Failure Patients
Analysis of fatigue symptom clusters, nocturnal respiratory distress symptom cluster, low perfusion symptom cluster and upper airway irritation symptom cluster using the Apriori algorithm. The results showed that waking up breathless at night was identified as the sentinel symptom of nocturnal respiratory distress symptom cluster, sweating was identified as the sentinel symptom of low perfusion symptom cluster, cough was identified as the sentinel symptom of upper airway irritation symptom cluster. Gastrointestinal symptom cluster was not associated with the sentinel symptom, as shown in Table 3.
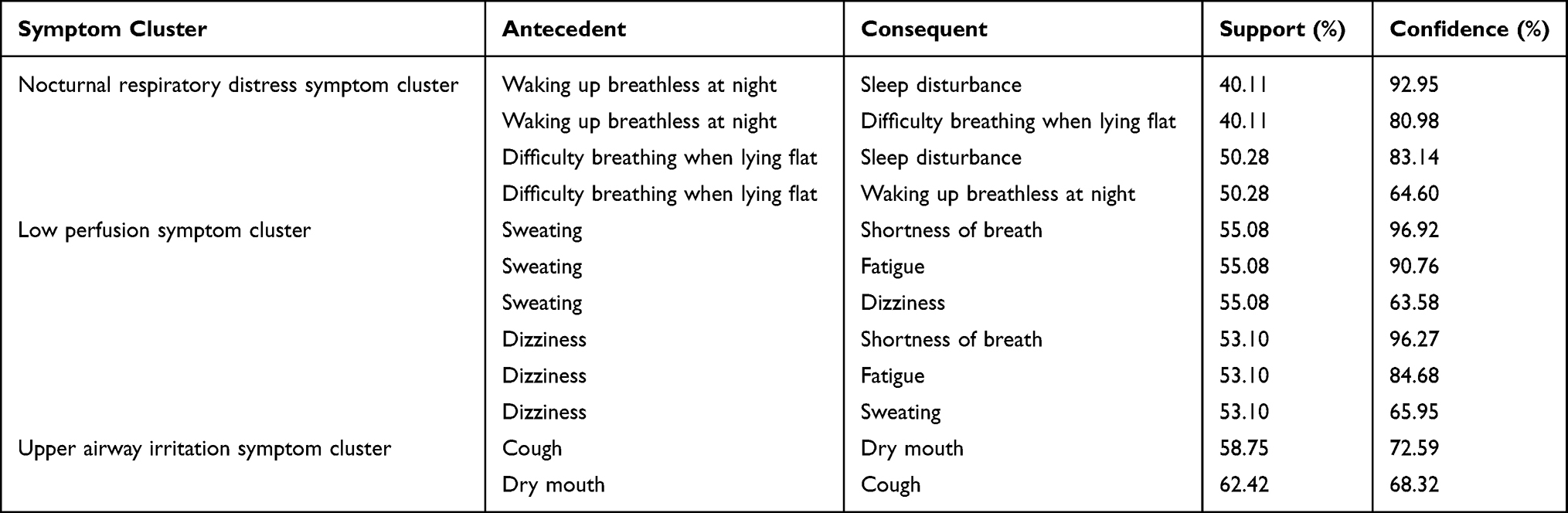 |
Table 3 Apriori Algorithm-Based Association Rules (N=354) |
Discussion
This study identified four symptom clusters in HF patients, designated as nocturnal respiratory distress symptom cluster, low perfusion symptom cluster, upper airway irritation symptom cluster, and gastrointestinal symptom cluster. Waking up breathless at night, sweating, and cough are the corresponding sentinel symptoms, while no sentinel symptoms have yet been identified for gastrointestinal symptom cluster.
The nocturnal respiratory distress symptom cluster consisted of sleep disturbance, waking up breathless at night, difficulty breathing when lying flat and consistent with previous studies.13,35 This cluster can be physiologically explained by the fact that pulmonary congestion and edema resulting from HF are the primary mechanisms underlying dyspnoea, which in turn contributes to sleep difficulties to a certain extent.36 The low perfusion symptom cluster consisted of sweating, shortness of breath, fatigue and dizziness, whereas the studies by Li et al37 and Wu et al38 classify them as distinct symptom clusters. This may be due to differences between the criteria for identifying symptom clusters and the statistical methods used. The upper airway irritation symptom cluster consisted of cough and dry mouth, which is consistent with the findings of Li et al37 The gastrointestinal symptom cluster consisted of nausea and lack of appetite, which is essentially similar to the studies by Son35 and Yi.39 This can be explained by impaired venous return, which causes systemic congestion and reduced cardiac output, ultimately leading to visceral ischemia and hypoxia. It is noteworthy that, in contrast to previous studies, this research did not identify an emotion-related symptom cluster. This may be related to the advanced age of the patients in this study. Influenced by China’s traditional social and cultural context, older adults tend to express their emotions in a more restrained manner and rarely reveal negative emotions to others.40 Therefore, medical staff should complement pharmacological treatment with psychological interventions, encouraging patients to openly express their negative emotions and providing individualized psychological support. In addition, the symptoms experienced by HF patients are complex and exhibit cumulative and synergistic effects. Therefore, medical staff can adopt comprehensive management strategies to monitor symptom clusters holistically, thereby alleviating the burden on the healthcare system, improving the efficiency of symptom management, and ultimately enhancing HF patients’ quality of life.
Waking up breathless at night was the sentinel symptom of the nocturnal Respiratory distress symptom cluster. This may be due to elevated left atrial pressure, leading to fluid leakage into the interstitial and alveolar spaces, which disrupts gas exchange, causing respiratory symptoms.41 Several studies have demonstrated that approximately 50% of HF patients experience waking up at night due to sleep disordered breathing, including apnea, paroxysmal nocturnal dyspnoea, orthopnoea, and cough.42,43 These symptoms disturbances consequently contribute to sleep disruption and poor sleep quality in the majority of HF patients.44 Importantly, waking up breathless at night and difficulty breathing when lying flat frequently co-occur, and the former serves as a clinical marker of worsening HF.16,45 Therefore, medical staff should closely monitor the nighttime sleep patterns of HF patients. This can be achieved using wearable devices that continuously record sleep related breathing patterns.46 Notably, if a patient wakes up breathless at night, this may indicate worsening of their condition, and prompt medical attention should be sought.45 Medical staff can use cognitive behavioral therapy, auricular acupressure with beans, and traditional Chinese medicine to alleviate waking up breathless at night, thereby reducing other symptoms within this symptom cluster and improving HF patients’ quality of life.47,48
Sweating was the sentinel symptom of the low perfusion symptom cluster. Excessive activation of the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system (SNS) contributes to the progression of HF through multiple mechanisms. Specifically, during HF episodes, RAAS overactivation promotes sodium and water retention, whereas SNS activation stimulates eccrine sweat gland secretion. Together, these two mechanisms lead to increased sweating.49 Beyond fluid and sweat disturbances, elevated aldosterone levels also cause myocardial thickening and stiffening, impairing cardiac pumping and reducing cardiac output.50 This results in hypoperfusion of organs and tissues, accompanied by compensatory tachycardia, which subsequently contributes to fatigue and shortness of breath. HF Patients require long-term treatment with angiotensin converting enzyme inhibitors to slow disease progression; however, these medications may cause dizziness and fatigue as side effects.51 Therefore, medical staff should pay attention to the symptom of sweating in patients, as it may help impede the development of other symptoms and prevent synergistic effects within the cluster. Waon therapy can be used to induce sweating, which in turn causes peripheral vasodilation and consequently reduces both the preload and afterload on the heart.52 This treatment has been proven to be a comfortable and safe therapy that improves clinical symptoms and enhances cardiac function.53
Cough was the sentinel symptom of the upper airway irritation symptom cluster. Among the serious conditions associated with cough, HF represents the most prevalent extra-pulmonary etiology.54 Specifically, HF can lead to pulmonary congestion, which in turn irritates the airways and triggers the cough.41 Consequently, to alleviate symptoms of congestion, patients require long term diuretic therapy, which can lead to fluid loss and subsequent dry mouth; moreover, the side effects of these medications may also directly induce dry mouth.39,55 Medical staff should pay closer attention to assessing patients’ cough symptoms to avoid missed or delayed diagnosis in the early stages.56 In terms of cough management, patients may adopt a sitting or semi recumbent position to relieve coughing. Furthermore, for those with frequent cough, respiratory exercises may be recommended, and appropriate cough suppressants can be prescribed as needed to reduce symptoms.
This study has several limitations. First, as a single-center study conducted exclusively in tertiary hospitals within the Ningxia Hui Autonomous Region, the findings may not be generalizable to other settings or regions in China. Therefore, future large-scale, multi-center trials with subgroup analyses are warranted to facilitate more precise medical care for patients. Second, the cross-sectional design precluded investigation of the dynamic trajectory of sentinel symptoms over time; future longitudinal studies could be conducted to elucidate how these symptoms change over time. Lastly, this study did not record detailed information about the medications the patients were taking nor did it examine the relationship between biological markers and sentinel symptoms, issues that need to be further explored in the future.
Conclusion
This study found that HF patients have multiple symptoms in the form of four symptom clusters, and identified three sentinel symptoms: waking up breathless at night, sweating and cough. Such findings provide novel evidence to facilitate personalized cluster targeted symptom management and strengthen early symptom screening capacity. Future research can develop tailored interventions centered on these sentinel symptoms to improve quality of life in HF populations.
Ethics Approval and Informed Consent
Prior to commencement of the study, written informed consent was obtained from all participants. Participants’ privacy and confidentiality were rigorously protected throughout the entire research process, and they were entitled to withdraw from the study at any time without prejudice. This study received approval from the Ethics Review Committee of The General Hospital of Ningxia Medical University (No.KYLL-2024-0145) and was performed in accordance with the Declaration of Helsinki.
Acknowledgment
The authors sincerely thank all heart failure patients who participated in this study. We also wish to express our sincere gratitude for the financial support provided by the School of Nursing, Ningxia Medical University.
Funding
The research was supported by Key Incubation Project for First-Class Disciplines School of Nursing Ningxia Medical University (NYHLZD202402).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang H, Chai K, Du M, et al. Prevalence and incidence of heart failure among urban patients in china: a national population-based analysis. Circ Heart Fail. 2021;14(10):e008406. doi:10.1161/CIRCHEARTFAILURE.121.008406
2. Lecoeur E, Domeng O, Fayol A, et al. Epidemiology of heart failure in young adults: a French nationwide cohort study. Eur Heart J. 2023;44(5):383–9. doi:10.1093/eurheartj/ehac651
3. Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020;5:15. doi:10.21037/amj.2020.03.03
4. Wang H, Liu YJ, Yang JF. Epidemiology of heart failure. J Clin Cardiol. 2023;39(04):243–247.
5. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
6. Bragazzi NL, Zhong W, Shu J, et al. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prev Cardiol. 2021;28(15):1682–1690. doi:10.1093/eurjpc/zwaa147
7. Alpert CM, Smith MA, Hummel SL, et al. Symptom burden in heart failure: assessment, impact on outcomes, and management. Heart Fail Rev. 2017;22(1):25–39. doi:10.1007/s10741-016-9581-4
8. Luiso D, Villanueva JA, Belarte-Tornero LC, et al. Surface respiratory electromyography and dyspnea in acute heart failure patients. PLoS One. 2020;15(4):e0232225. doi:10.1371/journal.pone.0232225
9. Danziger J, Chen K, Cavender S, et al. Admission peripheral edema, central venous pressure, and survival in critically ill patients. Ann Am Thorac Soc. 2016;13(5):705–711. doi:10.1513/AnnalsATS.201511-737OC
10. Kataoka H. Clinical significance of bilateral leg edema and added value of monitoring weight gain during follow-up of patients with established heart failure. ESC Heart Fail. 2015;2(4):106–115. doi:10.1002/ehf2.12043
11. Goldberg RJ, Spencer FA, Szklo-Coxe M, et al. Symptom presentation in patients hospitalized with acute heart failure. Clin Cardiol. 2010;33(6):E73–80. doi:10.1002/clc.20627
12. Park J, Moser DK, Griffith K, et al. Exploring symptom clusters in people with heart failure. Clin Nurs Res. 2019;28(2):165–181. doi:10.1177/1054773817729606
13. Song EK, Moser DK, Rayens MK, et al. Symptom clusters predict event-free survival in patients with heart failure. J Cardiovasc Nurs. 2010;25(4):284–291. doi:10.1097/JCN.0b013e3181cfbcbb
14. Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status of patients with cancer. Oncol Nurs Forum. 2001;28(3):465–470.
15. Kim HJ, Mcguire DB, Tulman L, et al. Symptom clusters: concept analysis and clinical implications for cancer nursing. Cancer Nurs. 2005;28(4):
16. Yao Q, Luo J, Song B, et al. The effect of heart failure symptom clusters on quality of life: the moderating effect of self-care behaviours. J Clin Nurs. 2025;34(7):2766–2778. doi:10.1111/jocn.17475
17. Brown JK, Cooley ME, Chernecky C, et al. A symptom cluster and sentinel symptom experienced by women with lung cancer. Oncol Nurs Forum. 2011;38(6):E425–35. doi:10.1188/11.ONF.E425-E435
18. Kirkova J, Aktas A, Walsh D, et al. Consistency of symptom clusters in advanced cancer. Am J Hosp Palliat Care. 2010;27(5):342–346. doi:10.1177/1049909110369869
19. Jim HS, Jacobsen PB, Phillips KM, et al. Lagged relationships among sleep disturbance, fatigue, and depressed mood during chemotherapy. Health Psychol. 2013;32(7):768–774. doi:10.1037/a0031322
20. Lu X, Geng W, Liu F, et al. Symptom clusters and sentinel symptoms in breast cancer survivors based on self-reported outcomes:A cross-sectional survey. J Clin Nurs. 2025;34(3):1072–1080. doi:10.1111/jocn.17383
21. Skerman HM, Yatesp M, Battistutta D. Identification of cancer-related symptom clusters:anempiricalcomparisonofex-ploratoryfactoranalysismethods. J Pain Sympt Manage. 2012;44(1):10–22. doi:10.1016/j.jpainsymman.2011.07.009
22. Huang TY, Moser DK, Hwang SL. Identification, associated factors, and prognosis of symptom clusters in taiwanese patients with heart failure. J Nurs Res. 2018;26(1):60–67. doi:10.1097/JNR.0000000000000199
23. Hu Y, Jiang J, Xu L, et al. Symptom clusters and quality of life among patients with chronic heart failure: a cross-sectional study. Jpn J Nurs Sci. 2021;18(1):e12366. doi:10.1111/jjns.12366
24. Liang M, Zhong T, Knobf MT, et al. Sentinel and networked symptoms in patients with breast cancer undergoing chemotherapy. Eur J Oncol Nurs. 2024;70:102566. doi:10.1016/j.ejon.2024.102566
25. Molassiotis A, Lowe M, Blackhall F, et al. A qualitative exploration of a respiratory distress symptomcluster in lung cancer: cough, breathlessness and fatigue. Lung Cancer. 2011;71(1):94–102. doi:10.1016/j.lungcan.2010.04.002
26. Wei L, Lv F, Luo C, et al. Study on sentinel symptoms and influencing factors of postoperative chemotherapy in patients with gastric cancer. Eur J Oncol Nurs. 2023;64:102318.
27. Wu ML. Practical Questionnaire Statistical Analysis: SPSS Operation and Application. Chongqing: Chongqing University Press; 2009:207–208.
28. Cardiovascular Disease Branch of Chinese Medical Association, Cardiovascular Internal Medicine Physicians Branch of Chinese Medical Doctor Association, Heart Failure Professional Committee of Chinese Medical Doctor Association, et al. Chinese guidelines for the diagnosis and treatment of heart failure 2024. Chin J Cardiol. 2024;52(3):235–275.
29. Chinese Society of Infectious Diseases, Severe Liver Disease and Artificial Liver Group, Chinese Medical Association; Chinese Society of Hepatology, Severe Liver Disease and Artificial Liver Group, Chinese Medical Association. Guidelines for the Diagnosis and Treatment of Liver Failure (2024 Edition). Chin J Hepatol. 2025;33(1):18–33. doi:10.3760/cma.j.cn501113-20241206-00614
30. Levey AS, De Jong PE, Coresh J, et al. The definition, classification, and prognosis of chronic kidney disease: a KDIGO Controversies Conference report. Kidney Int. 2011;80(1):17–28. doi:10.1038/ki.2010.483
31. Caraballo C, Desai NR, Mulder H, et al. Clinical Implications of the New York Heart Association Classification. J Am Heart Assoc. 2019;8(23):e014240. doi:10.1161/JAHA.119.014240
32. Zambroski CH, Moser DK, Bhat G, et al. Impact of symptom prevalence and symptom burden on quality of life in patients with heart failure. Eur J Cardiovasc Nurs. 2005;4(3):198–206. doi:10.1016/j.ejcnurse.2005.03.010
33. Guo JY, Lyu R, Zhang J, et al. Evaluation of the reliability and validity of the Chinese version of the heart failure symptom assessment scale. Chin J Nurs. 2014;49:1448–1452.
34. Ma J, Li L, Du J, et al. The quantification and clinical analysis of depression and anxiety in patients undergoing Da Vinci robot-assisted radical gastrectomy and open radical gastrectomy. Eur J Cancer Prev. 2021;30(6):442–447. doi:10.1097/CEJ.0000000000000653
35. Son YJ, Won MH. Symptom clusters and their impacts on hospital readmission in patients with heart failure: a Cross-Sectional Study. Res Theory Nurs Pract. 2018;32(3):311–327. doi:10.1891/1541-6577.32.3.311
36. Coniglio AC, Mentz RJ. Sleep breathing disorders in heart failure. Cardiol Clin. 2022;40(2):183–189. doi:10.1016/j.ccl.2021.12.006
37. Li RR, Wang M, Chen SS, et al. Network analysis of symptom clusters and bridge symptoms in elderly patients with chronic heart failure. Chin Nurs Manage. 2025;25(1):37–41.
38. Wu JY, Yu M, Qiu AH, et al. Identification of symptom clusters, core symptoms and bridge symptoms in patients with chronic heart failure. Chin General Pract Nurs. 2025;23(19):3640–3645.
39. Yi YF, Yuan Y, Song HX, et al. Relationship between symptom cluster and quality of life in patients with heart failure.The. J Nurs. 2018;25(1):10–13.
40. Zeng Z, Deng Y, Liu J, et al. Chinese cancer patients’ attitudes toward psychotherapy and their willingness to participate in clinical trials of psychotherapy. Cancer Control. 2022;29:10732748221112664. doi:10.1177/10732748221112664
41. Mocan D, Jipa R, Jipa DA, et al. Unveiling the systemic impact of congestion in heart failure: a narrative review of multisystem pathophysiology and clinical implications. J Cardiovasc Dev Dis. 2025;12(4). doi:10.3390/jcdd12040124
42. Zuurbier LA, Luik AI, Leening MJ, et al. Associations of heart failure with sleep quality: the Rotterdam Study. J Clin Sleep Med. 2015;11(2):117–121. doi:10.5664/jcsm.4454
43. Dos Santos MA, Guedes Ede S, Barbosa RL, et al. Sleeping difficulties reported by patients with heart failure. Rev Lat Am Enfermagem. 2012;20(4):644–650. doi:10.1590/S0104-11692012000400003
44. Gharaibeh B, Al-Absi I, Abuhammad S, et al. Dimensions of sleep characteristics and predictors of sleep quality among heart failure patients: a STROBE compliant cross-sectional study in Jordan. Medicine. 2022;101(52):e32585. doi:10.1097/MD.0000000000032585
45. Mahmood A, Ray M, Dobalian A, et al. Insomnia symptoms and incident heart failure: a population-based cohort study. Eur Heart J. 2021;42(40):4169–4176. doi:10.1093/eurheartj/ehab500
46. Heidenr Eich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of. Cardiology. 2022;145(18):e895–1032.
47. Tang RX, Li M, Liu XC, et al. Effects of auricular point pressing combined with external counterpulsation on sleep quality, quality of life and psychological status in patients with chronic heart failure. Chin Nurs Res. 2021;35(5):901–904.
48. Li YY, Li ML, Fang JB. Research progress on non-pharmacological interventions to improve sleep quality in patients with heart failure. J Nurs Train. 2022;37(5):412–415,429.
49. Maryam, Varghese TP,BT. Unraveling the complex pathophysiology of heart failure: insights into the role of renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system (SNS). Curr Probl Cardiol. 2024;49(4):102411. doi:10.1016/j.cpcardiol.2024.102411
50. Alfarano M, Marchionni G, Costantino J, et al. Aldosterone-Related cardiovascular disease and benefits of mineralocorticoid receptor antagonists in clinical practice. JACC Adv. 2025;4(6 Pt 1):101762. doi:10.1016/j.jacadv.2025.101762
51. Butzner M, Riello RJ, Sarocco P, et al. Adverse drug effects across patients with heart failure: a systematic review. Am J Manag Care. 2022;28(3):e113–e20.
52. Tei C, Imamura T, Kinugawa K, et al. Waon therapy for managing chronic heart failure- results from a multicenter prospective randomized WAON-CHF study. Circ J. 2016;80(4):827–834. doi:10.1253/circj.CJ-16-0051
53. Miyata M, Kihara T, Kubozono T, et al. Beneficial effects of Waon therapy on patients with chronic heart failure: results of a prospective multicenter study. J Cardiol. 2008;52(2):79–85. doi:10.1016/j.jjcc.2008.07.009
54. Emilsson ÖI. The burden and impact of chronic cough in severe disease. Curr Opin Support Palliat Care. 2022;16(4):183–187. doi:10.1097/SPC.0000000000000623
55. Yao L, Chen YM, Wu YT, et al. Efficacy and safety evaluation of low-dose tolvaptan in extremely elderly patients with chronic heart failure[J]. Chin J Evid Based Cardiovasc Med. 2019;11(12):1517–1519.
56. Xiong X, Liu L, Xue B. Misdiagnosis analysis of early atypical heart failure in the elderly presenting mainly with cough[J]. Clin Misdiagnosis Misther. 2019;32(4):9–13.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nurse-Led Model of Care with Telemonitoring to Manage Patients with Heart Failure in Primary Health Care: A Mixed-Method Feasibility Study
Longhini J, Canzan F, Zambiasi P, Toccoli S, Gios L, Del Greco M, Sforzin S, Moz M, Fracchetti M, Saiani L, Brolis R, Guarnier A, Soverini M, Maines M, Ambrosi E
Patient Preference and Adherence 2023, 17:2579-2594
Published Date: 20 October 2023
Identification of Symptom Clusters and Sentinel Symptoms During Radiotherapy in Lung Cancer Patients: A Longitudinal Study
Zhang J, Li S, Wu J, Yang B, Tan X, Zhang G, Zhao X
Cancer Management and Research 2025, 17:2307-2318
Published Date: 7 October 2025
Learning Needs in Heart Failure Care Across Patients, Caregivers, and Healthcare Professionals: A Scoping Review of Asian Studies
Sugiharto F, Trisyani Y, Nuraeni A, Abdullah KL
Patient Preference and Adherence 2026, 20:577045
Published Date: 4 February 2026