Back to Journals » Patient Preference and Adherence » Volume 20
Learning Needs in Heart Failure Care Across Patients, Caregivers, and Healthcare Professionals: A Scoping Review of Asian Studies
Authors Sugiharto F ![]() , Trisyani Y
, Trisyani Y ![]() , Nuraeni A
, Nuraeni A ![]() , Abdullah KL
, Abdullah KL ![]()
Received 27 October 2025
Accepted for publication 22 January 2026
Published 4 February 2026 Volume 2026:20 577045
DOI https://doi.org/10.2147/PPA.S577045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Firman Sugiharto,1 Yanny Trisyani,2 Aan Nuraeni,2 Khatijah Lim Abdullah3
1Doctoral Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3School of Nursing, Faculty of Medical and Life Sciences, Sunway University, Bandar Sunway, Malaysia
Correspondence: Yanny Trisyani, Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Fax +620227795596, Email [email protected]
Background: Heart failure (HF) is a significant and growing public health challenge in Asia. Effective HF management relies heavily on sustained self-care and education involving not only patients but also family caregivers and healthcare professionals. However, no previous review has systematically mapped the multidimensional learning needs of patients, family caregivers, and healthcare professionals in this region.
Purpose: This scoping review aimed to identify, categorize, and synthesize existing evidence on learning needs in HF care from the perspectives of patients, caregivers, and healthcare professionals across Asian populations.
Methods: Using the Arksey and O’Malley framework and reported in accordance with PRISMA guidelines, four databases (PubMed, Scopus, EBSCOhost, and Taylor & Francis) and the Google Scholar search engine were searched for Asian studies on August 19, 2025. Sixteen eligible studies published between 2010 and 2025 were included. Data were charted and analysed thematically to identify patterns and variations across three stakeholder perspectives.
Results: A total of 16 studies were included in this review. The thematic analysis identified three perspectives of learning needs. From the patients’ perspective, the key priorities were disease knowledge, medication management, symptom recognition, lifestyle modification, and psychosocial adaptation. Caregivers’ perspective emphasised practical caregiving skills, emotional resilience, and access to guidance and social support. Meanwhile, the healthcare professionals’ perspective highlighted patient-centred communication, consistent educational delivery, and interprofessional coordination.
Conclusion: This review demonstrates a clear need for an integrated and culturally responsive educational framework that aligns the learning priorities of patients, caregivers, and healthcare professionals. Educational interventions should address both clinical and psychosocial dimensions of HF care. Nurses play a crucial role as key educators within multidisciplinary teams and should be empowered to facilitate coherent, continuous, and patient-centered learning across care settings.
Keywords: caregiver, education, heart failure, health professional, learning needs
Introduction
Heart failure (HF) is a global health problem with increasing prevalence and is estimated to affect more than 64 million people worldwide.1 Based on Global Burden of Disease (GBD) data (2019), there were approximately 31.89 million cases of HF in Asia, with an age-standardised prevalence rate of 722.45 per 100,000 population.2,3 This prevalence exceeds that reported in Europe (606.61 per 100,000) but remains slightly lower than in the Americas (810.42 per 100,000).3 Marked regional disparities are evident across Asia, with the highest prevalence observed in East Asia (1,014.06 per 100,000) and the lowest in South Asia (389.97 per 100,000). In addition, HF contributes substantially to the global disability burden, accounting for 5.05 million years lived with disability (YLDs), with East Asia again reporting higher rates (90.93 per 100,000) compared with South Asia (34.41 per 100,000).3 These findings underscore Asia as one of the regions bearing a substantial burden of HF worldwide.
The common causes of high mortality and morbidity rates among HF patients in Asia include poor adherence to medication and dietary recommendations, delayed recognition and response to symptoms, and insufficient knowledge and self-care skills necessary for effective disease management.3 These are known to be factors contributing to clinical decompensation in patients.4 The main priority in the care of patients with heart failure is early detection and symptom management, because delays in intervention can have serious consequences in the form of reduced quality of life, increased morbidity, and risk of death.5
The high prevalence of HF in Asia demands greater attention to long-term care aspects, including the need for patient and caregiver education, which plays a crucial role in disease management.6–8 Previous studies have confirmed that patients with HF require extensive knowledge, ranging from medication management, a low-salt diet, to recognising symptoms that require immediate medical attention.6,9 However, research in Asia still shows limitations. A study in Korea, for example, reported that patients often have low learning needs and are more dependent on medical personnel for their health management.6 Meanwhile, research in Jordan showed differences in educational needs priorities between patients, caregivers, and nurses, where patients placed more emphasis on dietary education, while nurses focused more on medication management and side effects.9 This research gap shows that, despite Asia having a high burden of HF, the literature on patient and caregiver learning needs is still very limited and needs further exploration.
A comprehensive understanding of the educational needs of heart failure patients, caregivers, and healthcare providers is vital for optimizing self-management practices and improving clinical outcomes.8,10,11 Learning needs refer to the identified gaps between existing and desired knowledge, skills, or attitudes required for effective professional performance. These needs are recognised through self-assessment, reflection, peer review, or performance analysis and are used to plan targeted educational interventions. Recent studies from Asia highlight both common and unique educational priorities, emphasising the importance of a culturally sensitive, patient-centred approach.7,9 Additionally, caregivers play a vital role in supporting self-management, but often lack adequate education about HF. Interventions targeting caregiver education have been shown to improve patient self-management and reduce readmission rates.10,12
Self-management plays an essential role in supporting the success of therapy in HF patients.10 Detecting symptoms early is essential to effective self-management.13 In addition, other stages include monitoring changes in conditions, making decisions to act or seek help, implementing management strategies, and re-evaluating the effectiveness of interventions carried out.13 Effective participation in decision-making depends on patients’ and caregivers’ prior understanding of the illness, available therapies, and the relative benefits and risks of each option.14 Efforts to support patients through educational and learning programs have been shown to contribute to improved self-care behaviours, ranging from lifestyle modifications and responses to worsening symptoms to the management of chronic syndromes.15 Ongoing support and continuous education within the home environment are vital components of heart failure care, particularly to ensure a safe and effective transition from hospital to home.10,14,16
At present, no review thoroughly summarizes and synthesizes empirical evidence on learning needs for managing heart failure from the integrated perspectives of patients, caregivers, and healthcare professionals. It is important to understand these three perspectives because the goal of education is to improve patients’ health. A thorough identification of the perspectives of patients, family caregivers, and healthcare providers is anticipated to reveal existing knowledge gaps and differences in perceptions of care requirements.
The results of this review will furnish a more robust scientific foundation for the formulation of evidence-based educational interventions that are holistic, culturally pertinent to the Asian context, and centered on addressing the genuine learning requirements of individuals with heart failure. This review identifies specific educational deficiencies among patients, caregivers, and healthcare professionals, highlighting critical areas where knowledge gaps directly contribute to inadequate self-management, poor treatment adherence, and frequent hospital readmissions. Using targeted educational strategies to address these gaps, we hope to improve patient outcomes, strengthen family caregiving, and enhance the overall continuity and quality of heart failure care in Asia. This scoping review seeks to systematically delineate and integrate the educational requirements in heart failure management among patients, caregivers, and healthcare professionals within the Asian context, recognizing that learning needs are context-dependent and multifaceted.
Materials and Methods
Study Design
This research adopted a scoping review approach in accordance with the methodological framework outlined by Arksey and O’Malley.17 This Design was considered appropriate due to the fragmented and heterogeneous nature of existing evidence on learning needs in HF management across Asian populations. In response to this gap, a scoping review was adopted to systematically map the scope and diversity of available studies, identify conceptual and methodological variations, and delineate the extent and characteristics of the current evidence base. Scoping reviews are particularly well-suited to exploratory aims, as they facilitate the identification of knowledge gaps, inform future research directions, and provide a robust foundation for the development of contextually relevant educational frameworks in HF care.
Eligibility Criteria
The selection of relevant studies for this review was conducted by three independent reviewers (FS, AN, YT) in accordance with the PRISMA statement. The development of research questions and eligibility criteria was based on the PCC framework (Table 1).
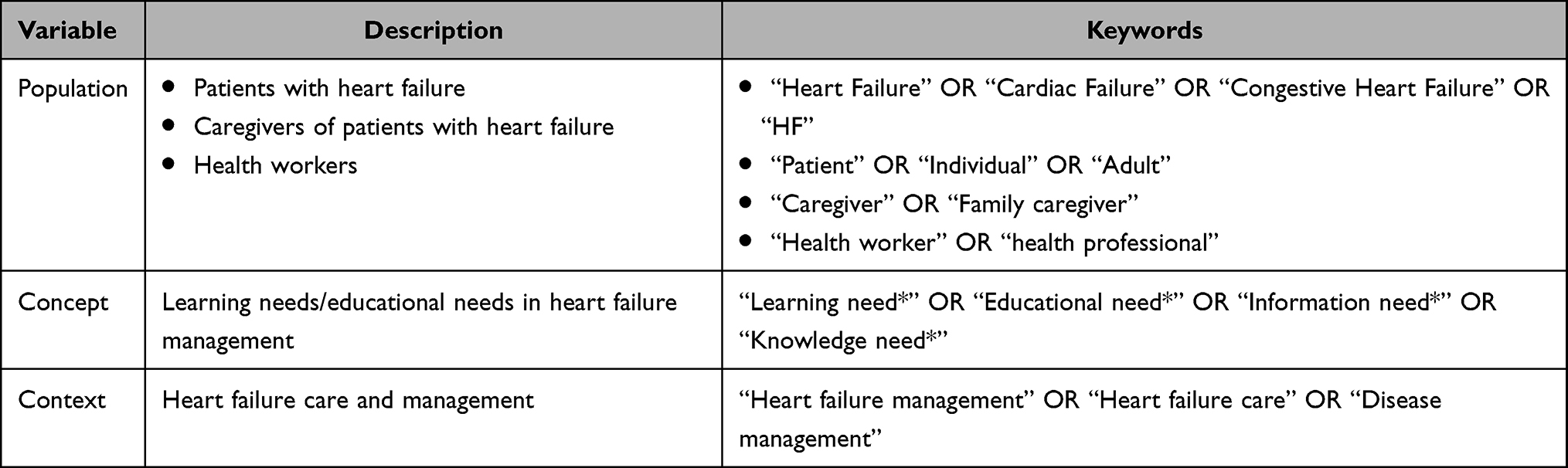 |
Table 1 PCC Framework |
The articles included in this review were selected based on the following inclusion criteria including: (1) publications in English and Indonesia available in full text, (2) studies addressing learning needs, informational needs, or educational needs of patients, caregivers, and health professionals in the context of heart failure care, (3) research employing diverse designs, including qualitative, quantitative, or mixed-methods study, and (4) studies conducted in Asian countries to provide a comprehensive perspective. In contrast, the exclusion criteria encompassed: (1) secondary review articles, editorials, commentaries, or reports that did not present empirical data. No restrictions were placed on the year of publication to ensure the inclusion of all relevant literature.
Search Strategy
The search strategy was conducted systematically across four major databases, including PubMed, Scopus, EBSCOhost, Taylor & Francis, and the search engine: Google Scholar, to ensure comprehensive coverage of relevant studies. The search was performed on August 19, 2025, and included all articles published up to that date. The keywords used were developed using a combination of MeSH and free-text terms, such as: “congestive heart failure[MeSH Terms]” OR “heart failure[MeSH Terms]” OR “cardiac failure[MeSH Terms]” AND (“patient” OR “caregiver” OR “family caregiver” OR “family member” OR “health worker” OR “health professional”) AND (“learning need” OR “educational need[MeSH Terms]” OR “informational need” OR “knowledge need”) AND. (“heart failure management” OR “disease management”).
In addition to the electronic search, manual hand-searching was performed by screening the reference lists of relevant articles, reviewing major cardiology and nursing journals, and examining conference proceedings within the Asian region. This complementary step aimed to identify additional studies that may not have been captured through database searches.
Study Selection
The study selection process was carried out independently by three reviewers (FS, AN, YT) following the PRISMA framework. Initially, all identified records from selected databases and additional sources were imported into a reference management software, where automatic and manual procedures were used to detect and remove duplicate entries. Subsequently, the remaining articles’ titles and abstracts were screened to assess their alignment with the predefined research objectives. At this stage, irrelevant records and those that did not meet the broad inclusion criteria were excluded. Full-text versions of the potentially eligible articles were then retrieved and assessed in detail against the established inclusion and exclusion criteria. The evaluation considered study Design, population, intervention or exposure, outcomes, and language requirements. Finally, the studies meeting all criteria were included in the review. Discrepancies during the selection process were resolved through discussion among the reviewers, and when necessary, a third-party adjudicator was consulted to reach consensus. This multi-stage process of identification, screening, eligibility, and inclusion ensured a systematic and transparent selection of studies consistent with PRISMA guidelines.
Data Extraction and Analysis
Two reviewers (FS and AN) independently extracted the included studies into a summary table containing information on study characteristics, participants, cultural or national context, and key findings related to the learning needs of patients and caregivers. Two reviewers performed data extraction, and a third and fourth reviewer subsequently verified the work to ensure consistency and accuracy (YT and KLA). The analysis employed a combination of descriptive, qualitative, and thematic analysis, enabling systematic mapping of study characteristics alongside an in-depth exploration of emerging concepts.
In the first stage, descriptive analysis was used to map and summarise the key attributes of each included study, such as research Design, setting, sample characteristics, and participants’ educational backgrounds. This step provided a structured overview of the scope and distribution of evidence across different Asian countries. Subsequently, thematic analysis was conducted to identify, categorise, and interpret the learning needs of patients, family caregivers, and healthcare professionals. Findings from the various studies were carefully compared and organised into overarching themes that captured both commonalities and contextual distinctions. Data from each stakeholder group were analysed separately to identify within-group themes, which were then compared and contrasted through cross-perspective analysis to reveal areas of convergence, divergence, and complementarity among the three perspectives.
Results
Study Selection
A total of 1.396 records were initially retrieved from four electronic databases (PubMed, EBSCOhost, Scopus, and Taylor & Francis) (see Figure 1). After removing 32 duplicates and one record automatically marked as ineligible, 1.363 records were screened based on titles and abstracts. From this stage, 1.269 records were excluded for not meeting the study objectives, leaving 94 reports for further assessment. Of these, 43 reports could not be retrieved in full text, and the remaining 51 full-text articles were evaluated against the inclusion and exclusion criteria.
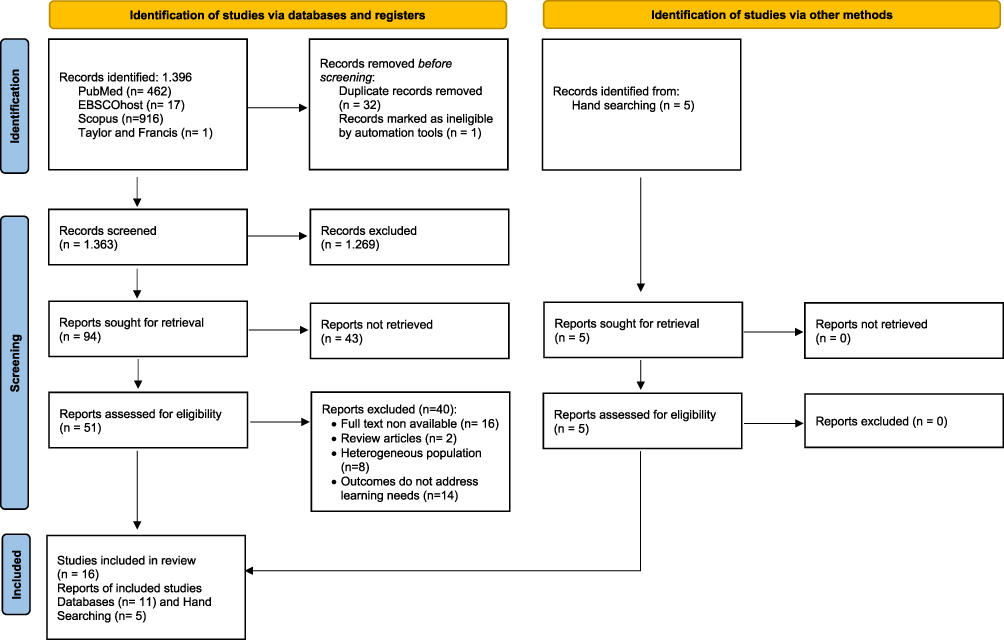 |
Figure 1 PRISMA Flow Diagram adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.18 |
During the eligibility assessment, 40 reports were excluded due to factors such as lack of full text, review article type, heterogeneous populations, or outcomes that did not address learning needs. In addition, five additional studies were identified through manual searching, all of which met the eligibility criteria. Finally, 16 studies were included in the review, comprising 11 studies from databases and 5 from hand searching.
Characteristics of Studies
This review comprised 16 studies conducted across Asia and the Middle East, including China, Korea, Iran, Singapore, Jordan, Indonesia, Turkey, and Japan (see Table 2). Methodologically, the studies employed qualitative designs,19–24 descriptive and cross-sectional surveys,6,9,25–28 and mixed-method approaches.29,30 Two separate qualitative inquiries were also conducted by Yu et al (2016) in China, one with patients and another with healthcare professionals, while Bahrami et al (2014) contributed two distinct caregiver-focused studies in Iran.19,20 This methodological diversity provided both contextual depth and empirical breadth, mapping the spectrum of patient and caregiver learning needs in different healthcare systems.
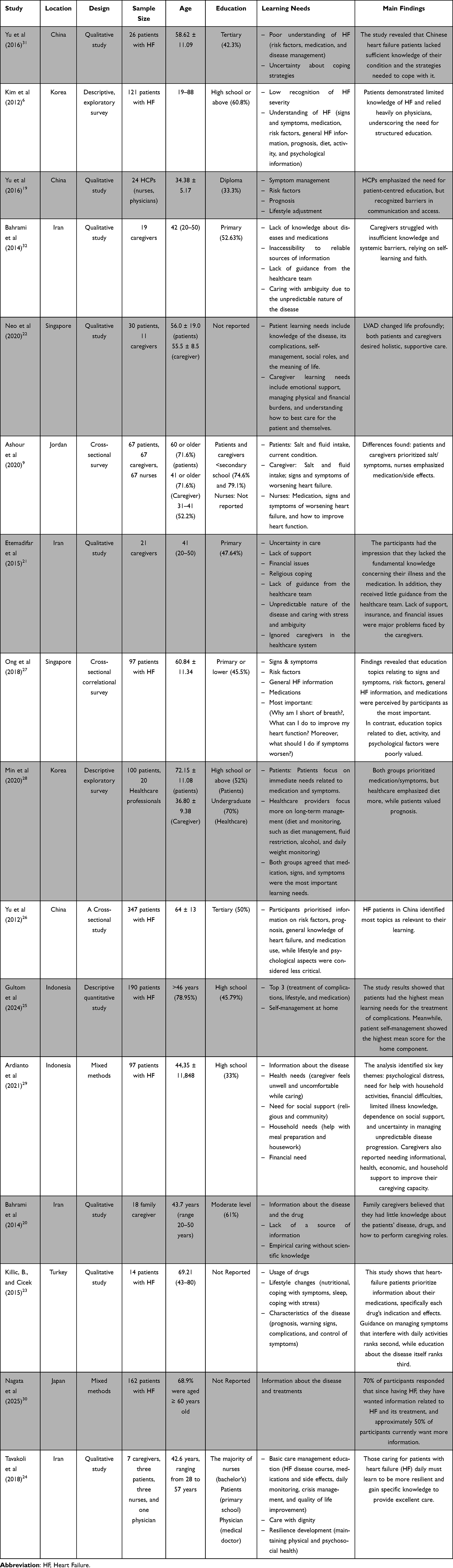 |
Table 2 Characteristic of Studies and Participants |
Geographically, the studies spanned multiple regions, enhancing the cultural representativeness of findings. Research conducted in East Asia,6,19,26,28,30 Southeast Asia,22,27 the Middle East,9,24 and South Asia,25,29 revealed both convergences and divergences in heart failure education priorities. Collectively, the geographical and methodological diversity reflects the multifaceted nature of learning needs in heart failure care while simultaneously highlighting disparities that call for tailored, context-sensitive educational interventions.
Characteristics of Participants
Participants consisted of HF patients, caregivers, and healthcare professionals (nurses and physicians). Patients were generally middle-aged to older adults, with mean ages mostly 50–70 years, while caregivers were often 30–50 years old (see Table 2). The youngest participant was 19, and the oldest was 88.6 In terms of education, there was considerable diversity. Many patients had at least a high school education (eg, 60.8% in Korea with a high school or higher education). By contrast, caregivers in some settings, particularly in Iran, were predominantly educated at the primary school level. Healthcare professionals were mainly holders of a diploma or a bachelor’s degree.
Analysis of Learning Needs
The thematic analysis in this review was categorized into three distinct yet complementary perspectives: patients, families or caregivers, and healthcare professionals (see Figure 2). These themes depict a complex, interconnected spectrum of learning needs in the context of heart failure management. Each perspective demonstrates a unique area of focus. These differences indicate that educational processes cannot be understood in isolation from a single viewpoint but must instead be regarded as part of an integrative learning ecosystem. Accordingly, synthesising these three perspectives provides an essential foundation for analysing how diverse learning needs can be harmonised into collaborative, contextually grounded, and evidence-based educational strategies.
 |
Figure 2 Thematic Analysis of Learning Needs. |
Category I: Patients’ Perspective
From the patient’s perspective, it consists of six main themes, such as (I) Knowledge and severity understanding, (II) Symptom management and response, (III) Medication knowledge and adherence, (IV) Lifestyle and daily self-management, (V) Complication crisis management, and (VI) Psychosocial adaptation. Patients expressed an urgent demand for fundamental information on heart failure, including risk factors, prognosis, and available treatment options.6,19,26,27,30 Moreover, recognizing warning signs and knowing the appropriate actions to take during symptom exacerbations were identified as critical elements in fostering self-reliance.6,23,26,27
Another emphasised aspect is patients’ understanding of pharmacological therapy, which includes drug indications, therapeutic effects, potential side effects, and adherence strategies. Previous studies highlighted persistent challenges patients face in independently managing their medication regimens.6,23,26,27,31 Lifestyle modifications, such as dietary control, salt and fluid restriction, physical activity, sleep regulation, and coping strategies, were also identified as key learning needs to ensure effective home-based self-management.6,9,23,25,27 Further learning requirements include strategies for managing complications, particularly acute exacerbations or crises.22,25,27 In addition, patients require psychosocial support in coping with uncertainty, adjusting to social role changes, and reinterpreting the meaning of life while living with a chronic illness.6,22,31
Category II: Caregiver Perspective
From the caregivers’ perspective, six significant learning themes are needed, which include: (I) Disease and treatment knowledge, (II) Symptom monitoring and daily care, (III) Guidance and system support, (IV) Physical, psychological, and emotional support, (V) Financial and resource needs, and (VI) Care with dignity. The learning needs primarily centre on disease knowledge, practical caregiving skills, and psychological well-being. Caregivers frequently encounter information gaps regarding the course of the disease, medication regimens, and their daily patient care responsibilities.9,20,21,32 They also require enhanced skills in symptom monitoring, dietary management, particularly in salt and fluid restriction, and crisis response.9,24
Another significant challenge is the limited guidance and support from healthcare providers. Many caregivers reported feeling overlooked within the healthcare system, contributing to knowledge gaps and increased psychological burden.20,21 Consequently, there is a substantial demand for physical, emotional, and spiritual support. Evidence suggests that caregivers benefit from coping strategies, stress management interventions, and religious coping mechanisms to sustain psychosocial resilience.21,22,24
Beyond psychological needs, financial burdens are also prevalent due to treatment costs and limited insurance coverage. Caregivers emphasized the necessity of access to sufficient supportive and financial resources.21,22 Moreover, caregivers consistently highlighted the importance of dignified care, ensuring that patients’ integrity and self-respect are preserved throughout the caregiving process.24
Category III: Healthcare Perspective
For healthcare professionals, there are five learning needs themes, namely: I) Disease knowledge and symptom management, (II) Long-term management and lifestyle adjustment, (III) Treatment and medication, (IV) Patient-centered care and communication, and (V) Coordinated care and barriers.
The primary learning needs revolve around patient-centred communication, clinical knowledge, and interprofessional coordination. Barriers in communication with patients and caregivers often diminish the effectiveness of education, emphasizing the necessity for healthcare providers to deliver information with greater clarity and empathy.19 From the perspective of healthcare professionals, patients also need to improve their competence in symptom management, including understanding risk factors, prognosis, and recognizing early warning signs.9,28 In addition, lifestyle adjustment strategies, particularly dietary regulation, fluid restriction, and weight monitoring, are critical to supporting patients in the long-term management of heart failure.28
In terms of medical treatment, professionals identified the need for a deeper understanding of pharmacotherapy, including medication effects, adverse reactions, and strategies to improve patients’ functional outcomes.9,28 Nonetheless, systemic barriers in coordination across healthcare teams remain a persistent issue. Multiple studies have emphasized the importance of establishing more integrated services to enhance the accessibility and effectiveness of patient care.19
Discussion
This review is the first to synthesize learning needs in HF care across patients, caregivers, and healthcare professionals in Asia, revealing a significant misalignment in priorities between families and healthcare professionals. These variations in perspective are not merely differences in the list of topics to be taught but rather reflect the distinct roles, identities, and motivations of each group within the heart failure care system. Such differences further underscore the importance of contextually grounded educational frameworks that integrate patients’, caregivers’, and professionals’ perspectives to achieve cohesive, culturally responsive heart failure self-care education.
Patients primarily focus their learning on self-management, which includes disease knowledge, recognizing warning signs, adhering to medication regimens, and modifying their lifestyles to gain greater control and independence in their daily lives.6,23,26,27 Caregivers prioritize practical competencies (symptom monitoring, diet, crisis response) that go hand in hand with psychosocial resilience (coping strategies, spiritual/social support) to maintain continuity of home care and prevent burnout.21,22,24,32 Meanwhile, healthcare professionals view learning needs through a system-centred lens, focusing on effective empathetic communication, evidence-based lifestyle counselling, and coordination to bridge care transitions and ensure consistency of educational messages.9,19,28 These differences in learning needs align with the Situation Specific Theory of Heart Failure Self Care, with its three core concepts: self-care maintenance, confidence, and management.33,34 The three core concepts highlighted the interaction of patient, caregiver, and contextual factors. In this case, the healthcare professionals influence health failure self-care decisions on management.33,34
These three perspectives, although with different focuses, complement each other and form a unified whole to ensure continuity of care. These findings indicate that most of the patient’s learning needs have been covered by the caregiver and healthcare worker perspectives. However, both caregivers and health workers still have learning or informational needs that require special attention. Differences in perception among patients, caregivers, and healthcare workers reflect variations in focus and perspective on learning needs, depending on role. Therefore, a comprehensive analysis from all three perspectives is necessary to identify areas that need improvement and harmonization. For patients and caregivers, strengthening intensive communication and integration with healthcare professionals is key to ensuring consistent education and care. If these mismatched perceptions are not aligned, the continuum of care risks becoming suboptimal. Therefore, these three perspectives need to be synergistically integrated to create a learning and care system that is sustainable, adaptive, and capable of improving the quality of life and overall well-being of patients.
Understanding learning needs from the caregiver perspective is a crucial issue that must be comprehensively identified. In addition to assisting patients with daily care, families act as co-providers, maintaining therapy continuity, monitoring symptoms, and ensuring adherence to treatment regimens. This care is long-term, so the family, as caregivers, is at risk of experiencing burden.35–38 Previous reviews reported that most caregivers from 30 studies analyzed experienced high burdens both physically, psychologically, and socially.37 This gap has a direct impact on the effectiveness of patient care, as the caregiver’s inability to understand danger signs or implement dietary and fluid management can worsen the patient’s clinical condition.
In the context of caring for heart failure patients, families also experience several perceived obstacles.21,39 Major barriers include ineffective communication between patients, families, and healthcare professionals, fragmented care, and poorly structured care plans.39–42 In addition, other barriers include a lack of support, limited knowledge about patient care, and limited access to needed health resources and services.39,43,44 These barriers may increase the burden on the family, ultimately reducing the quality of care provided to the patient.45,46
Understanding patients’ learning needs from a family perspective significantly impacts treatment outcomes. Targeted education enables patients to recognize symptoms early, seek prompt medical help, and practice effective self-care.47,48 For families, adequate understanding increases self-confidence in accompanying patients and reduces anxiety in caring for them at home.24,32 Thus, mapping educational needs is one of the preventive strategies in heart failure management. In Asian settings, family-centered decision-making and cultural norms such as respect for authority and limited patient autonomy profoundly shape communication and caregiving.49,50 Families often serve as key mediators between patients and healthcare providers, influencing how health information is understood and acted upon.49,50 Thus, mapping educational needs represents not only a preventive strategy in heart failure management,51 but also a culturally attuned effort that recognizes the family’s central role in sustaining self-care.
The role of nurses in educating patients and their families is crucial.52 As healthcare professionals who interact most directly with patients, nurses are strategically positioned to convey health information effectively and consistently.53,54 To optimize this role, nurses need empathetic communication training and the ability to adapt educational approaches to patients’ individual needs.55 The results of this review also confirmed that the primary needs reported by healthcare professionals focused on patient-centered communication and interprofessional coordination,9,19,28 Because communication barriers between healthcare workers, patients, and families often reduce the effectiveness of the educational process, healthcare providers need to ensure that information is delivered clearly, consistently, and with empathy so that patients and their families can truly understand and apply the learning. Structural barriers within healthcare systems, including time constraints, fragmented care transitions, and the lack of caregiver inclusion, may also reinforce misalignments between healthcare professionals and patients and their family members.
The differences found among patients, caregivers, and healthcare professionals indicate a misalignment in learning priorities, potentially hindering the continuum of care. An effective continuum of care requires integration across perspectives. The differences in understanding among patients, who focus on practical aspects and self-adaptation; caregivers, who emphasize emotional support and the burden of care; and healthcare professionals, who focus on clinical education and team coordination, need to be bridged through a collaborative educational approach. Thus, all three parties must complement each other cross-sectionally and work synergistically to ensure consistent and continuous educational messages.
Implication for Practice
This study has several notable strengths. Unlike previous reviews that focused only on patient self-care education, this review uniquely incorporates caregiver and healthcare professional perspectives, revealing misalignment that may contribute to poor continuity of care. First, unlike previous reviews that focused only on patient self-education, this review uniquely incorporates caregiver and healthcare professional e-learning needs in Asia, enabling a more holistic analysis of educational dynamics within the context of heart failure management. Another strength lies in its emphasis on cultural aspects, which are often underexplored in similar studies, thereby adding practical relevance and contextual depth to the Asian setting.
Overall, this scoping review provides an essential contribution to understanding the learning needs of patients with heart failure, their families, and healthcare professionals within the Asian context. The mapping demonstrates that educational programs should adopt a comprehensive approach that encompasses medical, lifestyle, and psychosocial dimensions while being sensitive to cultural values. By integrating these components, educational strategies are expected to enhance treatment adherence, reduce hospital readmissions, and ultimately improve patients’ quality of life. Hence, the present findings provide a strong basis for designing evidence-based, patient- and family-centred educational interventions that promote holistic and sustainable heart failure management.
Strengths and Limitations of the Study
This study has several strengths. First, the review was conducted systematically using a scoping review approach, which enabled mapping of diverse literature and provided a comprehensive overview of the learning needs of patients, families, and healthcare professionals in Asia. Second, this review focused on multiple perspectives, enabling a more holistic analysis of educational dynamics within the context of heart failure management. Another strength lies in its emphasis on cultural aspects, which are often underexplored in similar studies, thereby adding practical relevance and contextual depth to the Asian setting.
However, this study also has certain limitations. Most of the included literature originated from a few East Asian countries, which may limit the representativeness of findings across the wider Asian region. Additionally, several studies employed cross-sectional designs, which restrict the ability to infer causal relationships. These factors suggest that the results of this review should be interpreted with caution and may not be fully generalizable to all populations across Asia.
Conclusion
This scoping review identified and analyzed 16 relevant articles addressing learning needs in HF care across Asian settings. The synthesis revealed that these learning needs can be categorized into three primary perspectives. First, patients require a comprehensive understanding of the disease, medication regimens, lifestyle modification, and the ability to recognize signs of deterioration. Second, families emphasize the need for both practical and emotional support in daily caregiving. Third, healthcare professionals focus on ensuring consistency in education, clinical monitoring, and effective communication to facilitate structured and coordinated care. The analysis highlighted distinct priorities among these three perspectives, which may lead to practice gaps if left unaddressed. Therefore, educational programs should be designed to be integrated, continuous, and evidence-based, ensuring alignment among patients, families, and healthcare professionals to optimize outcomes in heart failure management.
In conclusion, this review emphasizes the necessity for an integrative educational framework that aligns the learning requirements and instructional methodologies of patients, caregivers, and healthcare practitioners. Educational interventions must go beyond generic instruction and develop into person-centered, culturally sensitive, and psychosocially integrated strategies that respond to the actual experiences of individuals and families impacted by heart failure. Crucially, nurses must be positioned as the central agents of transformative learning, equipped with advanced communication competencies and empowered through interprofessional collaboration to sustain coherent and compassionate education across settings.
Acknowledgement
The Article Processing Charge (APC) for this article was funded by Universitas Padjadjaran through the Padjadjaran Doctoral Program Scholarship, under Contract No. 2650/UN6.3.1/PT.00/2025.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020;5(Ci):2–15. doi:10.21037/amj.2020.03.03
2. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
3. Feng J, Zhang Y, Zhang J. Epidemiology and burden of heart failure in Asia. JACC Asia. 2024;4(4):249–264. doi:10.1016/j.jacasi.2024.01.013
4. Verdu-Rotellar JM, Vaillant-Roussel H, Abellana R, et al. Precipitating factors of heart failure decompensation, short-term morbidity and mortality in patients attended in primary care. Scand J Prim Health Care. 2020;38(4):473–480. doi:10.1080/02813432.2020.1844387
5. Reeder KM, Ercole PM, Peek GM, Smith CE. Symptom perceptions and self-care behaviors in patients who self-manage heart failure. J Cardiovasc Nurs. 2015;30(1):E1. doi:10.1097/JCN.0000000000000117
6. Kim SS, Ahn JA, Kang SM, Kim G, Lee S. Learning needs of patients with heart failure a descriptive, exploratory study. J Clin Nurs. 2012;22(5–6):661–668. doi:10.1111/j.1365-2702.2012.04075.x
7. Cha ES, Clark PC, Reilly CM, et al. Educational needs for improving self-care in heart failure patients with diabetes. Diabetes Educ. 2012;5(38):673–684. doi:10.1177/0145721712450923
8. Leung PB, Silva AF, Cho J, et al. Eliciting the educational priorities of home care workers caring for adults with heart failure. Gerontol Geriatr Educ. 2020;43(2):1–11.
9. Ashour A, Al-Rawashdeh S, Alwidyan M, Al-Smadi A, Alshraifeen A. Perceived learning needs of patients with heart failure in jordan: perspectives of patients, caregivers, and nurses: a cross-sectional survey. J Cardiovasc Nurs. 2020;35(3):273–279. doi:10.1097/JCN.0000000000000681
10. Ferguson C, William S, Allida S, et al. A qualitative exploration of the educational needs of people living with heart failure: BANDAIDD-Explore study. PLoS One. 2025;20(2 February):1–17. doi:10.1371/journal.pone.0314059
11. Ivynian SE, Newton PJ, DiGiacomo M. Patient preferences for heart failure education and perceptions of patient–provider communication. Scand J Caring Sci. 2020;34(4):1094–1101. doi:10.1111/scs.12820
12. Clements L, Frazier SK, Lennie TA. Improvement in heart failure self-care and patient readmissions with caregiver education: a randomized controlled trial. West J Nurs Res. 2022;45(5):402–415. doi:10.1177/01939459221141296
13. White MF, Kirschner J, Hamilton MA. Self-care guide for the heart failure patient. Circulation. 2014;129(3):e293–4. doi:10.1161/CIRCULATIONAHA.113.003991
14. Strömberg A. The crucial role of patient education in heart failure. Eur J Heart Fail. 2005;7(3):363–369. doi:10.1016/j.ejheart.2005.01.002
15. Riegel B, Dickson VV, Vellone E. The situation-specific theory of heart failure self-care: an update on the problem, person, and environmental factors influencing heart failure self-care. J Cardiovasc Nurs. 2022;37(6):515–529. doi:10.1097/JCN.0000000000000919
16. Allida S, Du H, Xu X, et al. mHealth education interventions in heart failure. Cochrane Database Syst Rev. 2020;7(7):CD011845. doi:10.1002/14651858.CD011845.pub2
17. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 2005;8(1):19–32. doi:10.1080/1364557032000119616
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
19. Yu M, Chair SY, Chan CW, Choi KC. Information needs of patients with heart failure: health professionals’ perspectives. Int J Nurs Pract. 2016;22(4):348–355. doi:10.1111/ijn.12442
20. Bahrami M, Etemadifar S, Shahriari M, Farsani AK. Caregiver burden among Iranian heart failure family caregivers: a descriptive, exploratory, qualitative study. Iran J Nurs Midwifery Res. 2014;19(1):56–63.
21. Etemadifar S, Bahrami M, Shahriari M, Farsani AK. Family caregivers’ experiences of caring for patients with heart failure: a descriptive, exploratory qualitative study. J Nurs Res. 2015;23(2):153–161. doi:10.1097/JNR.0000000000000076
22. Neo SHS, Ku JSM, Wong GCS, et al. Life beyond heart failure—what are the long-term challenges, supportive care needs, and views toward supportive care of multiethnic asian patients with left ventricular assist device and their caregivers? J Pain Symptom Manage. 2020;60(3):577–587.e1. doi:10.1016/j.jpainsymman.2020.03.022
23. Kiliç B, Sütçü Çiçek H. Assessment of educational needs of heart failure patients in intensive care units: qualitative study. Intensive Care Med Exp. 2015;3(Suppl 1):2197. doi:10.1186/2197-425X-3-S1-A208
24. Tavakoli A, Ilkhani M, Ashktorab T, Rohani C. The educational needs of iranian family caregivers of patients with advanced heart failure: a qualitative study. Int J Cardiovasc Res. 2018;12(4):148–153.
25. Chris Veronica Gultom E, Natalia Watania L, Pailak H, et al. Identification of learning needs and self-management of terminal renal failure patients undergoing hemodialysis at tangerang hospital [Identifikasi Kebutuhan Belajar Dan Manajemen Diri Pasien Gagal Ginjal Terminal Yang Menjalani Hemodialisis Di Rumah Saki. J Keperawatan Suaka Insa. 2024;9(2):123–130. doi:10.51143/jksi.v9i2.641
26. Yu M, Chair SY, Chan CWH, Li X, Choi KC. Perceived learning needs of patients with heart failure in China: a cross-sectional questionnaire survey. Contemp Nurse. 2012;41(1):70–77. doi:10.5172/conu.2012.41.1.70
27. Ong SF, Foong PPM, Seah JSH, Elangovan L, Wang W. Learning needs of hospitalized patients with heart failure in singapore: a descriptive correlational study. J Nurs Res. 2018;26(4):250–259. doi:10.1097/jnr.0000000000000239
28. Min D, Park JS, Choi EY, Ahn JA. Comparison of learning needs priorities between healthcare providers and patients with heart failure. PLoS One. 2020;15(9 September):1–10. doi:10.1371/journal.pone.0239656
29. Ardianto Pangastuti HS, Alim S. Family caregiver needs for post-hospitalization heart failure patients in indragiri hulu district [Kebutuhan family caregiver penderita gagal jantung post hospitalisasi di kabupaten indragiri hulu]. Syntax Lit J Ilm Indones. 2021;6(1):51–66.
30. Nagata S, Shiki K, Yagi N, Sato N. How do Japanese patients with chronic heart failure view their disease, self-care, and support? Adv Ther. 2025;42(7):3207–3222. doi:10.1007/s12325-025-03203-w
31. Yu MM, Chair SY, Chan CWH, Choi KC. Information needs of older people with heart failure: listening to their own voice. J Geriatr Cardiol. 2016;13(5):435–438. doi:10.11909/j.issn.1671-5411.2016.05.012
32. Bahrami M, Etemadifar S, Shahriari M, Farsani AK. Informational needs and related problems of family caregivers of heart failure patients. J Educ Health Promot. 2014;3(1):1–6. doi:10.4103/2277-9531.127541
33. Riegel B, Dickson VV. A situation-specific theory of heart failure self-care. J Cardiovasc Nurs. 2008;23(3):190–196. doi:10.1097/01.JCN.0000305091.35259.85
34. Riegel B, Dickson VV, Faulkner KM. The situation-specific theory of heart failure self-care: revised and updated. J Cardiovasc Nurs. 2016;31(3):226–235. doi:10.1097/JCN.0000000000000244
35. Lahoz R, Proudfoot C, Fonseca AF, et al. Caregivers of patients with heart failure: burden and the determinants of health-related quality of life. Patient Prefer Adherence. 2021;15:1153–1164. doi:10.2147/PPA.S297816
36. Durante A, Younas A, Cuoco A, et al. Burden among informal caregivers of individuals with heart failure: a mixed methods study. PLoS One. 2023;18(11 November):1–13. doi:10.1371/journal.pone.0292948
37. Suksatan W, Tankumpuan T, Davidson PM. Heart failure caregiver burden and outcomes: a systematic review. J Prim Care Community Heal. 2022;13.
38. Ghasemi M, Arab M, Shahrbabaki PM. Relationship between caregiver burden and family functioning in family caregivers of older adults with heart failure. J Gerontol Nurs. 2020;46(6):25–33.
39. Trivedi RB, Slightam C, Nevedal A, et al. Comparing the barriers and facilitators of heart failure management as perceived by patients, caregivers, and clinical providers. J Cardiovasc Nurs. 2019;34(5):399–409. doi:10.1097/JCN.0000000000000591
40. Browne S, Macdonald S, May C, Macleod U, Patient MF. Carer and professional perspectives on barriers and facilitators to quality care in advanced heart failure. PLoS One. 2014;9:e93288. doi:10.1371/journal.pone.0093288
41. Jose P, Ravindranath R, Joseph L, et al. Patient, caregiver, and health care provider perspectives on barriers and facilitators to heart failure care in Kerala, India: a qualitative study. Wellcome Open Research [Internet]. 2020. Available from: https://consensus.app/papers/patient-caregiver-and-health-care-provider-perspectives-harikrishnan-rhodes/5a5708ff4c695e2ebfd5b2075c4cdb10/.
42. Kim E, Oh S, Son Y. Caring experiences of family caregivers of patients with heart failure: a meta-ethnographic review of the past 10 years. Eur J Cardiovasc Nurs. 2020;19:473–485. doi:10.1177/1474515120915040
43. Babygeetha A, Devineni D. Social support and adherence to self-care behavior among patients with coronary heart disease and heart failure: a systematic review. Eur J Psychol. 2024;20(1):63–77. doi:10.5964/ejop.12131
44. Shahriari M, Ahmadi M, Babaee S, Mehrabi T, Sadeghi M. Effects of a family support program on self-care behaviors in patients with congestive heart failure. Iran J Nurs Midwifery Res. 2013;18(2):152.
45. Bidwell JT, States U, Vellone E, et al. Caregiver determinants of patient clinical event risk in heart failure. Eur J Cardiovasc Nurs. 2018;16(8):707–714. doi:10.1177/1474515117711305
46. Buck HG, Harkness K, Wion R, et al. Caregivers’ contributions to heart failure self-care: a systematic review. Eur J Cardiovasc Nurs. 2015;14(1):79–89. doi:10.1177/1474515113518434
47. Pereira Sousa J, Neves H, Lobao C, Goncalves R, Santos M. The effectiveness of education on symptoms recognition in heart failure patients to manage self-care: a systematic review protocol. Prof Inferm. 2019;72(1):50–54. doi:10.7429/pi.2019.721050
48. Philip A, Shastry CS, Unnikrishnan MK, Utagi B. Empowering self-care through patient education in heart failure patients: a multimodal approach comprising of P-PILs, videos, and personalized advice. J Educ Health Promot. 2024;13(1). doi:10.4103/jehp.jehp_1797_23
49. Corrigan PW, Lee EJ. Family-centered decision making for east asian adults with mental illness. Psychiatr Serv. 2021;72(1):114–116. doi:10.1176/appi.ps.201900570
50. Thojampa PhD RNS, Gunda BSN, K RN. Patient and family centered care from a South East Asian cultural perspective: a discussion. Int J Caring Sci. 2019;12(2):1–4.
51. Sugiharto F, Trisyani Y, Nuraeni A, Abdullah K. Comparative Systematic Review of Telehealth Delivery Models, Intervention Content, and Outcomes in Heart Failure Care. Patient Prefer Adherence. 2025;19:4335–4352. doi:10.2147/PPA.S568141
52. Sugiharto F, Haroen H, Alya F, et al. Health Educational Methods for Improving Self-Efficacy Among Patients with Coronary Heart Disease: A Scoping Review. J Multidiscip Healthc. 2024;17:779–792. doi:10.2147/JMDH.S455431
53. Sugiharto F, Nuraeni A, Trisyani Y, Melati Putri A, Aghnia Armansyah N. Nursing interventions for improving quality of life among patients with coronary heart disease after percutaneous coronary intervention: A scoping review. J Kep Padjadjaran. 2024;12(1):86–97. doi:10.24198/jkp.v12i1.2294
54. Kwame A, Petrucka P. A literature-based study of patient-centered care and communication in nurse-patient interactions: barriers, facilitators, and the way forward. BMC Nurs. 2021;20. doi:10.1186/s12912-021-00684-2
55. Kerr D, Ostaszkiewicz J, Dunning T, Martin P. The effectiveness of training interventions on nurses’ communication skills: a systematic review. Nurse Educ Today. 2020;89:104405. doi:10.1016/j.nedt.2020.104405
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Nursing-Home Care Quality Perceived Levels from Patients and Caregivers: An Explanatory Study
Vitale E, Mea R, Chang YC
Patient Preference and Adherence 2023, 17:1237-1245
Published Date: 9 May 2023
A Two-Pronged Educational Intervention for Caregivers to Prevent Residential Pesticide Exposure Among Thai Young Children Living in Agricultural Area
Muenchamnan N, Naksen W, Ong-Artborirak P
Journal of Multidisciplinary Healthcare 2023, 16:2339-2350
Published Date: 15 August 2023
A Nurse-Led Model of Care with Telemonitoring to Manage Patients with Heart Failure in Primary Health Care: A Mixed-Method Feasibility Study
Longhini J, Canzan F, Zambiasi P, Toccoli S, Gios L, Del Greco M, Sforzin S, Moz M, Fracchetti M, Saiani L, Brolis R, Guarnier A, Soverini M, Maines M, Ambrosi E
Patient Preference and Adherence 2023, 17:2579-2594
Published Date: 20 October 2023
Stakeholder Recommendations for Sports-Focused Undergraduate Nursing Curriculum: A Qualitative Study
Yusuf A, Aditya RS, Sulistyorini A, Rahmatika QT, Sunaryo EYAB, Masfi A, Afiani N, Widjayanti Y, Ramadhan MP, Evi N, AlMutairi RI, Al Razeeni DM
Advances in Medical Education and Practice 2024, 15:1-13
Published Date: 3 January 2024
Importance-Performance Analysis of Patient-Safety Nursing in the Operating Room: A Cross-Sectional Study
Shin J, Kim NY
Risk Management and Healthcare Policy 2024, 17:715-725
Published Date: 26 March 2024