")
Back to Journals » Patient Preference and Adherence » Volume 17
A Nurse-Led Model of Care with Telemonitoring to Manage Patients with Heart Failure in Primary Health Care: A Mixed-Method Feasibility Study
Authors Longhini J, Canzan F, Zambiasi P, Toccoli S, Gios L, Del Greco M, Sforzin S, Moz M, Fracchetti M, Saiani L, Brolis R, Guarnier A, Soverini M, Maines M, Ambrosi E
Received 22 July 2023
Accepted for publication 7 October 2023
Published 20 October 2023 Volume 2023:17 Pages 2579—2594
DOI https://doi.org/10.2147/PPA.S431865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jessica Longhini,1 Federica Canzan,1 Paola Zambiasi,2 Stefano Toccoli,2 Lorenzo Gios,3 Maurizio Del Greco,2 Simona Sforzin,2 Monica Moz,3 Michela Fracchetti,2 Luisa Saiani,1 Renata Brolis,2 Annamaria Guarnier,2 Mariangela Soverini,2 Massimiliano Maines,2 Elisa Ambrosi1
1Department of Diagnostics and Public Health, University of Verona, Verona, Italy; 2Azienda Provinciale per i Servizi Sanitari, Trento, Italy; 3TrentinoSalute4.0, Competence Center for Digital Health, Trento, Italy
Correspondence: Jessica Longhini, University of Verona, Strada le Grazie 8, Verona, Italy, Tel +393405322936, Email [email protected]
Purpose: To determine whether a nurse-led care model with telemonitoring in primary care for patients with stable heart failure and their caregivers is feasible and acceptable.
Patients and Methods: A mixed-methods feasibility study was conducted. Patients with stable heart failure and their caregivers were consecutively enrolled from March 2021 to April 2022. Participants were managed by nurses in a community health center through education and monitoring with a mobile app. The outcomes were feasibility outcomes, self-care outcomes, and qualitative acceptability and satisfaction. Quantitative and qualitative outcomes were linked to understanding how the model of care might benefit patients.
Results: Twenty-six patients and nine of their caregivers were enrolled. Ten participants used the mobile app. Nineteen patients and eight caregivers were interviewed. Participants who improved their self-care appreciated the help in finding coping strategies, being close to the clinic, and feeling cared for. Participants with fewer improvements in self-care perceived the model of care as useless and were far from the centre. Participants decided to use the app mainly for usefulness prevision, and most of them were satisfied.
Conclusion: The model of care was not successful in recruiting patients, and adjustments are needed to improve the recruitment strategy and to engage people who perceive the model of care as not useful or unable to use the app.
Keywords: nursing, primary care, heart failure, cardiology, general practice
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Wijaya has been published for this article.
Introduction
Throughout decades, the continual increase of chronic conditions in patients has become a major challenge for healthcare systems. Heart failure (HF) is one of the most challenging conditions, with an estimated prevalence of 2–3% across the world.1 However, the prevalence is likely higher because of the large number of undiagnosed cases, especially among those without frequent HF symptomatology.1 Over the years, the models of care and guidelines have mainly focused on acute and complex HF, as well as HF patients with a high risk of rehospitalization. Patients with a low risk of hospitalization and clinical stability are of low interest in health service research1 as they are usually managed by their general practitioners (GPs) or nurse practitioners in primary care. Few experimental studies have tested models of care involving primary care professionals acting as the leaders of HF care pathway, and inconsistent results have been reported in the literature on their effectiveness.2–4 Furthermore, nurse-led interventions for HF patients were mainly experimented in hospital outpatient clinics by recruiting discharged patients, intensive home care services, or transitional care programs.2–4 In addition, in recent decades, telehealth has been introduced to improve the efficiency of models of care5 on health outcomes and hospitalization, and the COVID-19 pandemic has advanced the development of digital health interventions, including mobile apps for remote telemonitoring. As soon as these apps were combined with nurse-led interventions,6 contrasting results on death, hospitalization, lifestyle, and self-care outcomes were found.7,8 However, most studies on telemonitoring focus mainly on complex or decompensated HF patients and on stand-alone telemonitoring interventions with the exclusion of people without internet at home and reaching a population with an average age of less than 75 years.3,7–9 All the issues described above prevent the development of useful recommendations to manage stable HF in primary care by embedding the role of nurses and digital interventions with the purpose to improve self-care abilities and slow the disease progression.
Moreover, few studies tested complex models of care with structured family- or caregiver-targeted interventions by nurses.4 However, scientific statements remark on the critical importance of providing education to families and caregivers, as well as further studies on technological interventions for caregivers.10
Based on these premises, we developed a complex multidisciplinary nurse-led intervention targeted at patients with stable HF in a community health center with a nurse-led telemonitoring service. In this study, we aimed to test the feasibility and acceptability of the nurse-led model of care and evaluate how the model of care might benefit patients and their informal caregivers to develop a protocol for a multicenter randomized control trial.
Materials and Methods
Research Questions
We defined these research questions:
- Quantitative research questions:
- Is this model feasible to recruit patients with stable HF?
- Is this model feasible to manage patients with stable HF with telemonitoring?
- Is this model feasible for improving self-care ability in patients with stable HF?
- Qualitative research questions:
- What is the level of acceptability of the care model in terms of beliefs and qualitative experiences from patients and their caregivers?
- What is the level of acceptability of the mobile app for telemonitoring in terms of beliefs and qualitative experiences of patients and their caregivers?
- Mixed-method research questions:
- How can participants’ and caregivers’ beliefs and experiences about the model of care (qualitative) help explain differences in self-care ability improvement (quantitative)?
- How can participants’ and caregivers’ beliefs and experiences about using the mobile app for telemonitoring (qualitative) explain the rate of adoption and use of the mobile app for telemonitoring (quantitative)?
Study Design
A mixed-methods feasibility study11,12 was conducted as part of a larger study from March 2021 to April 2022. The larger study consisted of a six-month pragmatic single-arm quasi-experimental study embedding the descriptive qualitative design applied as a nested process evaluation12 at three months. In this paper, we present quantitative and qualitative results at three months. The intervention mixed-method approach11,12 was used to understand how the model of care might work. Mixed-method design combines quantitative and qualitative data allowing us to answer our research questions, which could not be fully explained by a standalone qualitative or quantitative study. The reporting guidelines for mixed-method studies13 were adopted.
Setting and Participants
This study was conducted in a community health center placed in a rural-mountain district covering a population of 91.767 citizens. In this area, one hospital is present, and 78 GPs operate alone or in shared outpatient clinics. HF patients and patients with implantable heart devices are managed by cardiologists and nurses of the cardiological outpatient clinic in the hospital, which provide a telemonitoring service through a mobile app. Home care provided by GPs and district nurses is also available for patients with advanced and complex HF not able to reach health services.
We consecutively sampled patients: a) diagnosed with HF in stable conditions (stable NYHA class I–II, no frequent occurrence of HF drug changes or HF symptoms) as judged by cardiologists or GPs; b) in charge of GPs and hospital cardiologists in the district; c) able to reach outpatient services autonomously or accompanied; and d) >18 years. Informal caregivers were included if they contributed to HF self-care of the included patients, for example, helping in managing drugs, daily life activities, and symptoms. Patients were excluded if they were cared for by the hospital outpatient service because of complex heart comorbidities or implantable heart devices or by the home-care nursing service.
The recruitment was conducted in three phases to promote community-based recruitment with the involvement of family and community nurses (FCNs), GPs, and cardiologists of the outpatient hospital HF clinic. Firstly, GPs and cardiologists screened patients during routine visits or through the lists of all patients with HF diagnosis to identify those in stable conditions. Then, potential participants were communicated to FCNs that re-assessed each case for the eligibility criteria and proceeded to the enrolment in the study. In the third phase, FCNs checked the eligibility of caregivers of patients enrolled. The entire recruitment process was supervised by the research team. Considering the feasibility of the study, the sample size was not statistically estimated; however, we considered the need to establish a minimum of 25 patients over a timespan of one year to ensure findings relevant to estimate a parameter for sample size calculation of the next randomized control trial and detect different perspectives of patients’ experience.14
Intervention
The model was developed as a complex intervention comprising multiple interventions based on previous studies, clinical guidelines, and frameworks.1,15,16
Firstly, two mastered FCNs were allocated to a novel outpatient clinic in a community health center and trained on the study processes by the researcher team. The FCNs were registered nurses with post-graduate education and experience in family health and community care.
Then, a multidisciplinary network was established through a shared care pathway including FCNs, GPs, cardiologists, and nurses of the hospital HF outpatient clinic to smooth the HF clinical pathway across primary and secondary services.
The management of the patient consisted of the integration of all these interventions. During the first appointment, the FCN explored the educational and clinical needs of the patients and caregivers. At least two face-to-face follow-up and two phone calls were conducted interchangeably each month; however, the frequency was increased in case of complex needs of patients and their caregivers as judged by FCNs.
During the follow-up, the FNCs adopted the care manager approach and performed patient education through motivational interviewing, goal setting, and action-plan.
Effective communication techniques have been selected from evidence to identify and address patients’ needs and to perform therapeutic patient education. These include the tech-back17 motivational interviewing,18,19 and shared decision-making models20 including an adaption of the recently conceptualized SHERPA model21 to identify and develop a plan of care collegially with patients. Specifically, the teach-back allows to provide information and verify the understanding by the target person in multiple steps. The motivational interview is a counselling style, well established in the literature for its effectiveness in HF self-care.22 It is a collaborative dialogue in a climate of help and acceptance, that is useful to emerge the reasons and resources of the person and strengthen his commitment and motivation to realize a change towards a goal. The main components are reflective listening, open questions aimed at evoking change-oriented statements, sentences of synthesis and support, as well as providing information.
The Sharing Evidence Routine for a Person-centered plan for Action (SHERPA model) is a sharing decision-making approach consisting of three main steps. In Phase 1 (Share), the professional identifies the problems together with the person, including diagnosis, symptoms, emotions, concerns, behaviors, social problems, isolation, poverty, and difficulties in managing the disease. The goal is to develop a framework of problems centered on the person and not on the diagnoses. In Phase 2 (Link), the professional discusses with the patient to connect the problems drawing them on paper inside circles whose size is proportional to the importance of the problems. Pathophysiological links help the person to better understand their situation, while the connections made by the person help the professional to understand non-clinical reasons, values, beliefs, and expectations. In Phase 3 (Plan), the professional and the person explain their priorities, identifying together what to work on, and defining specific objectives, for example, medication reduction, symptom management, change of unhealthy behaviors, or social goals.
Additionally, to promote caregivers’ and families’ engagement and empowerment, the Calgary Family assessment and intervention models23 have been adopted to help caregivers and families in solving issues and developing self-care and resilience abilities. These models allow FCNs to care for families as a unit, thus avoiding focusing attention solely on the patient. FNCs assess families using the genogram to draw important relationships and identify the resources and strengths of that family and the caregiver network.
As for the multidisciplinary network, FCNs contacted the general practitioner or the cardiologist in case of clinical instability. Furthermore, FCNs activated other health professionals according to needs that emerged, such as social workers, dieticians, psychologists, and community lay resources, eg, associations of patients.
Regarding technological interventions, an electronic nursing record and a platform with the related app for patients were adopted.
Regarding the app, when patients or caregivers had a good level of digital literacy and accept to use the app, the Trec_Cardio app was downloaded on their smartphone. The TreC_Cardio app is designed to provide medical and lifestyle recommendations and to allow the patient to record disease-related information, ie, vital parameters, weight, symptoms, etc. The app includes also messaging and teleconference systems to facilitate communication between the patients and healthcare staff. In our study, FCNs prescribed routine tasks with notification alerts (ie, measuring blood pressure on Monday and Thursday at 8 in the morning), called patients or caregivers and cardiologists by video calls, and chatted with patients by attaching files and images. Patients or caregivers recorded the blood pressure, heart rate, oxygen saturation, weight, and symptoms according to a schedule fixed with the FCN. FCNs monitored patients’ data on the Trec_Cardio online platform daily, contacting the patient when data are not properly recorded or changes in clinical stability were observed. The online platform could be accessed also by cardiologists. In case the digital literacy of the patients or caregivers was low, or the participant did not accept the app, paper-based educational materials were provided with a written self-monitoring diary. The FCN monitored the clinical stability of the participants without the app during phone calls and face-to-face visits with the help of the self-reported monitoring diary.
FCNs reported all the activities conducted in the electronic nursing records, called @Home, developed before this study for home nursing care, which allowed accessing drug prescriptions and hospital reports.
Study Variables
Quantitative Outcomes
The quantitative outcomes investigated were the feasibility outcomes and self-care outcomes.
The feasibility outcomes were the number of patients enrolled and that completed the study, the number of participants accepting to use the app, and that use the app regularly in agreement with the FCN (Table 1). Feasibility outcomes, as the progression criteria for a randomized control trial,12 were evaluated according to pre-defined cut-off as a traffic light system24 (Table 1).
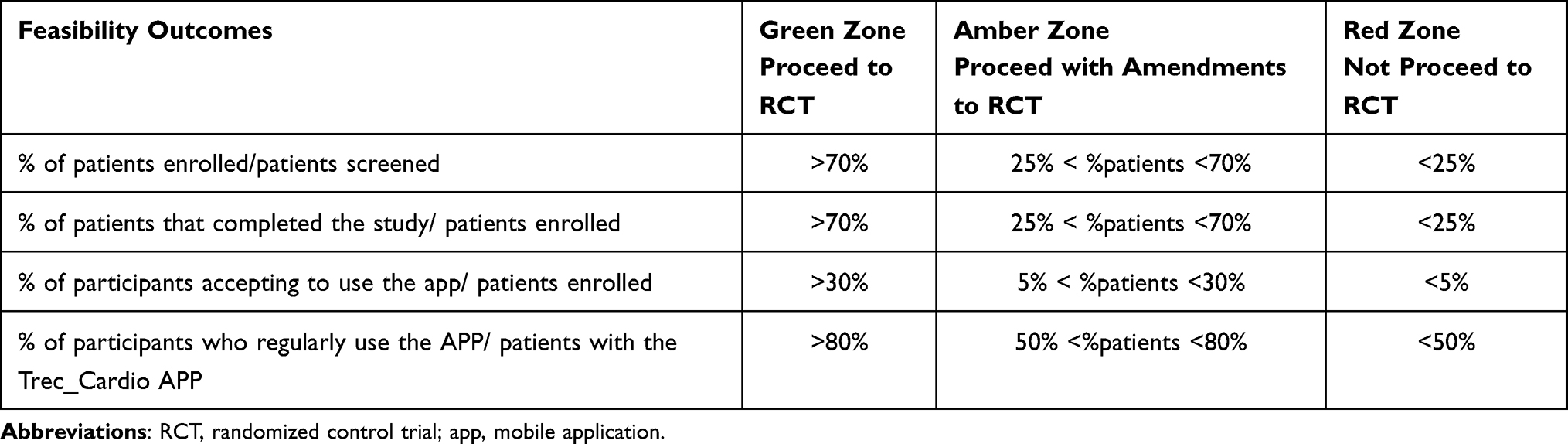 |
Table 1 Traffic Light System for Feasibility Outcomes Evaluation |
The self-care outcomes referred to the potential impact on self-care ability measured with self-report questionnaires: a) the Self-Care of Heart Failure Index (SCHFI) 7.2 Italian version25 for patients and b) the Caregiver Contribution to Self-care of Heart Failure Index (CC-SCHFI) 2 Italian version26 for informal caregivers. Both versions consist of 29 items grouped into three domains: self-care maintenance, monitoring, and management, with standardized points ranging from 0 to 100, where 100 is the best self-care. The tools have been validated in Italian, with good reliability and validity.25,26
Qualitative Outcomes
As qualitative data, patients’ and informal caregivers’ beliefs and experiences regarding the model of care were collected through qualitative semi-structured face-to-face interviews.
Data Collection
Demographics, comorbidities, and lifestyles were collected at the baseline. Feasibility outcomes were collected throughout the study period up to three months and self-care questionnaires were administered to patients and caregivers at the baseline and at three months after having received three months of intervention. All the data were collected by the FCNs as part of the care provided. Therefore, data were available for all participants. All patients and caregivers completed the questionnaires.
Qualitative data were collected by a trained researcher after the first three months of intervention in a dedicated space at the FCN clinic. The researcher followed a semi-structured guide (Supplementary File 1), piloted on one patient and one informal caregiver. These two interviews, judged relevant by the researchers, were included in the data analysis. The interviews lasted from 5 to 30 minutes, and participants were interviewed until data saturation was reached.
Data Analysis
For quantitative data, the distribution was tested by visualizing the quantile–quantile plot and Shapiro–Wilk test. Self-care outcomes were analyzed using the Wilcoxon signed-rank test. The level of significance was set at p < 0.05. According to a relevant positive change of 8 points in the SCHFI and CC-SCHFI domains,27 patients were grouped into eight self-care categories (eg, “No changes in all self-care domains”). Data analysis was performed using R statistical software version 4.1.2.
Regarding qualitative data, the interviews were transcribed verbatim, and content analysis was performed according to the preparation, organizing, and reporting phases.28 The unit of analysis was identified, and an open coding system was created by analyzing five interviews. Categories and themes were identified by applying and adapting the coding systems to other interviews. Three themes were identified, namely “Input”, including categories expressing the reasons to adhere to the model of care, “Process”, gathering categories related to strategies and perceived experience in being cared for, and “Outcomes” collecting categories expressing the results as perceived by the participants. Specifically, coded narratives in the “Outcomes” category were further categorized according to the self-care maintenance, monitoring, and management dimensions of SCHI-FI.25
To address the mixed-method research questions, integration of data occurred in data analysis. Quantitative and qualitative data were merged by linking the qualitative data to quantitative self-care outcomes through the patient’s identification code, according to the eight self-care categories identified by the analysis of quantitative self-care outcomes. Then, we have created a joint display to show the confirmation, discordance, and expansion meta-inferences drawn from the data linking.11,29
Results
Feasibility Outcomes
Twenty-six patients (out of 137, 19%) and nine of their caregivers were enrolled (Figure 1), not reaching the feasibility cut-off. The median age was 72 years (63.7–80.7, IQR) and 50.5 years (43–55.2 IQR) for patients and informal caregivers, respectively (Supplementary File 2). Of the 26 patients enrolled, 25 patients and eight caregivers completed the three months of intervention, satisfying the feasibility cut-off of the green zone. Regarding the mobile app, 10 participants accepted using the app (out of 26, 38.5%), meeting the green zone feasibility cut-off, of which six were caregivers. Two patients and three caregivers (5 out of 10, 50%) regularly used the app for the entire study period, partially satisfying the amber zone feasibility cut-off, whereas others used the app inconstantly or interrupted its use.
 |
Figure 1 Flowchart of the study. |
Self-Care Outcomes
Patients reported the highest median score in self-care monitoring activities (78.2, 65–83.2 IQR), while caregivers reported the best support abilities in self-care maintenance (79, IQR 73.5–84.5) (66.4, IQR 56.8–76.8). We found statistically significant improvements in all three self-care dimensions in patients, with the highest difference in monitoring (IQR 5.5–12.3, p < 0.001) (Table 2).
 |
Table 2 Self-Care Abilities in Patients and Caregivers |
Qualitative results on Model of Care Beliefs and Experience
A total of 19 patients and seven of their informal caregivers were interviewed. From the analysis, six themes and 18 categories emerged (Figure 2).
 |
Figure 2 Participants’ experiences regarding the model of care. |
Theme: Input as Adhering to the Model of Care
The patients described three main processes in adhering to the care model. First, patients reported to be compliant with the indication received from their GP, who emphasized the value of the FCNs’ service. Other participants adhered to the model because they felt that they needed to be checked, helped, and taken in charge. Some patients reflected before accepting to attend the model of care, drawing positive conclusions on potential advantages in participating, including usefulness, more time dedicated compared to GP, and ease in accessing GP and services.
Because it [FCNs’ clinic] was the only service still active during pandemic, you could not go to the hospital... all the difficulties... so in short, it will remain only the nurses. (int.18)
The general practitioner maybe can order you the antibiotic or what you need... but he spends less time on you as compared to what nurses do. (int.12-Caregiver)
Theme: Processes
Category: Finding Strategies to Develop Self-Care Skills
Participants found strategies by themselves to act self-care abilities, including following the nurses’ suggestions, strategies to lose weight, and increasing their own willingness. However, few participants encountered difficulties in finding strategies, such as finding time and supporting relatives in self-care abilities.
I often leave early in the morning when he [the father] still sleep, and I let him sleep it’s not that I feel like waking him up to measure his blood pressure. I know it is important but… we only can figure it out when I am at home on Saturday (int.25-Caregiver)
Participants valued help from nurses in promoting their self-care abilities. Examples included agreeing upon the timing of self-monitoring, helping to find strategies to cope with healthy lifestyles, giving instructions, being present with home visits, and taking appointments. Few experiences were reported in not considering the innovative suggestions received by the FCN and perceiving the conversation as chitchats.
Category: Feeling Being Cared for
Participants felt free to unload and perceived that the FNC listened to their needs compared with the GP’s visit or family members.
They [nurses] listen and believe me, others like family members at home don’t believe me so much. (Int.14)
Participants appreciated the interest of FCNs expressed by frequent calls to assess the situation, the availability to deepen problems, and thinking about future steps in planning care.
Because when you feel alone, you let yourself go... if I know that someone is monitoring me, then I try harder too. (Int.2)
In addition, the participants considered it important to be assessed and monitored by competent professionals. Patients and informal caregivers felt engaged in care and safety and helped with the FNC’s expertise.
I feel helped by the human relationship with people who have skills that we do not have. So, the possibility of calling them and say that maybe something is getting worse... because we can clearly help him [parent], but we don’t have any kind of medical expertise. (Int.1-Caregiver)
Category: Filling the Gap Between Services
Participants appreciated the facilitated access to health services and having a direct channel with specialist clinicians. Participants valorized the role of FCNs’ clinics in filling a deficit among services, especially regarding the building of new networks, acting as a filter to other services, and supporting and taking charge patients when no other services do it.
[…] also, because the general practitioner is good and checks you, but she is too busy, so this service is useful for relieving general practitioners. (Int.22)
Theme: Outcomes
Category: Perceiving Changes in Health Outcomes
Some participants reported general improvement in their health status. Other outcomes were categorized according to self-care theory, comprising self-care maintenance, monitoring, and management abilities. Regarding maintenance, most improvements were in changing eating habits, reducing salt intake, increasing physical activity, being more adherent to follow-up, and sleeping better. However, some participants did not modify their daily activities.
As for diet, there are some foods that are not good for me, but I have made some changes compared to before, in fact my GP has seen it on the blood exams. (Int.22)
With regard to monitoring, participants improved their monitoring of the parameters and symptoms, especially by using the written diary. Others, differently, reported to be not constant in measuring blood pressure or weight due to the absence of symptoms or do not have modified habits in monitoring because of good abilities already acquired.
Yes, it seems to me that nurses have helped me to manage health problems better... yes... in the measurements of blood pressure, blood sugar, weight. I do more regularly and write in the diary. (Int.26)
As for self-management, some participants explained that they were more confident in making decisions to manage problems related to HF, in particular, referring to when calling the physicians or nurses to prevent major negative events.
[…] but if I see that there is something is getting worse, I take and go to the emergency department, or if I see weight change, I start with furosemide or whatever has [the parent] as diuretics. (Int.12-Caregiver)
Theme: Perceiving Satisfaction on the Model of Care
Participants had a good experience with the model of care, perceiving it as useful, and attending it gladly. Satisfaction was highly related to the organization, with no suggested areas for improvement in most cases. Few needs were expressed concerning the possibility of having a visit with the cardiologist or making an electrocardiogram in the FCNs’ clinic. Furthermore, the participants appreciated the proximity of the FCNs’ clinic to their homes. Negative considerations emerged among those living far from the FCNs’ clinic, highlighting the difficulties in reaching the service in cases of lack of driving license or elderly. Some participants raised doubts about the appropriateness of the FCNs’ clinic, judging it as useless for the clinical stability condition.
The last time I was there I said it was useless to come if I don’t have symptoms or something changes... if the situation remains the same. (Int.18)
Mixed-Method Analysis Results
Integrating Self-Care Outcomes with Participants’ Experiences of the Care Model
By merging the data (Table 3), most of the qualitative data on health outcomes confirmed the relevant changes observed in the SCHFI and CC-SCHFI scores. Few incongruences have emerged, mainly regarding self-care maintenance and monitoring. We found that the lack of relevant changes in SCHFI and CC-SCHFI scores could be explained by previous good self-care, the distance of the service from home, work duties, or perceiving visits with FCNs such as chatting and not relevant for their stable condition, thus not perceiving benefits from this model of care. When relevant changes in at least two self-care dimensions were observed, participants frequently reported feeling supported, engaged, free to vent, and converse fearlessly, and appreciating the mutual agreement with FCNs on self-care and coping strategies. In addition, these participants appreciated FNCs’ help in booking appointments and physical closeness to the FCN clinic (Table 3).
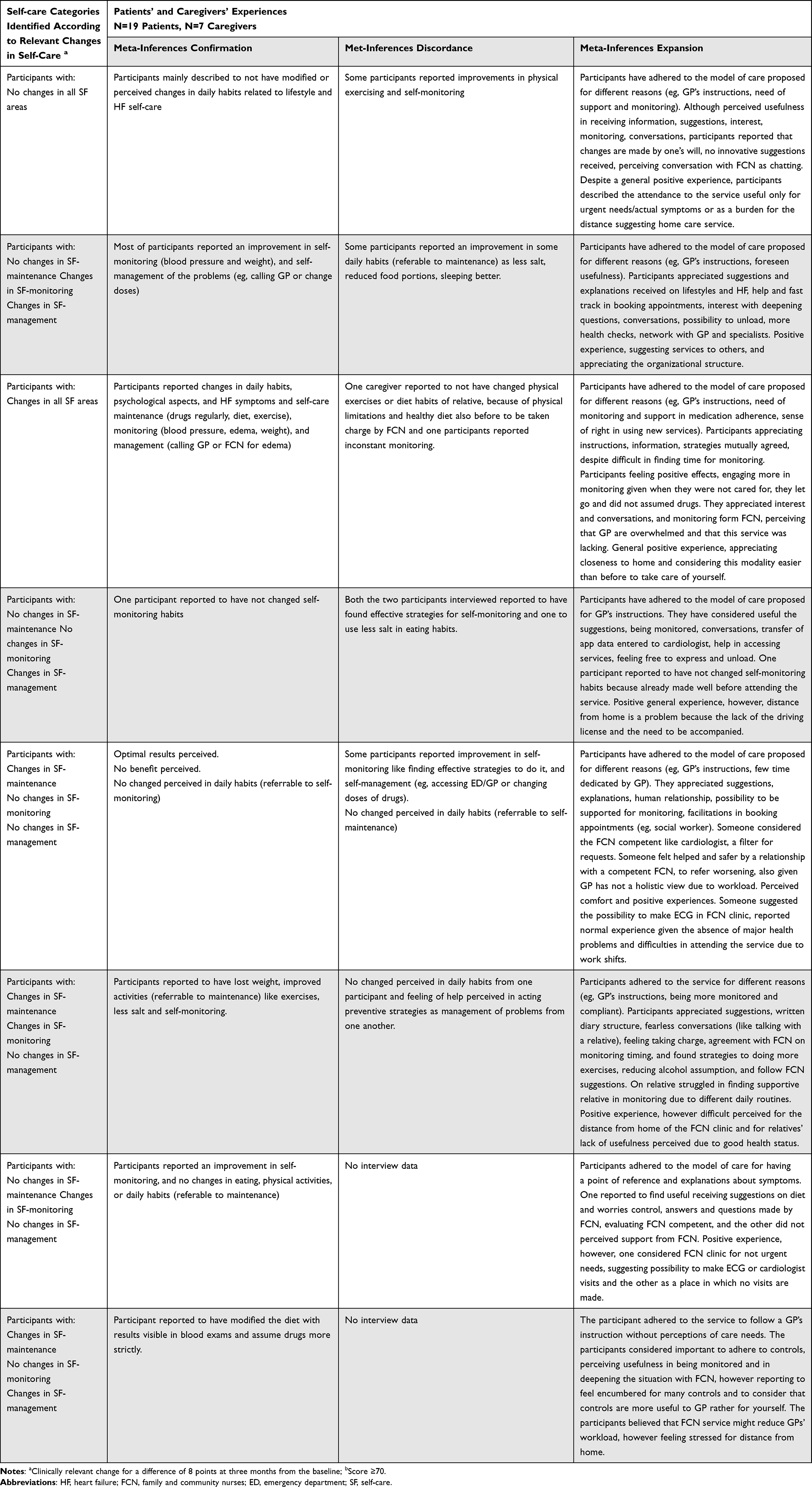 |
Table 3 Joint Display. Integrating Data on Self-Care Outcomes and Participants’ Experiences with the Model of Care |
Integrating Data on App Use and Participants’ Experiences of the App
Among the 16 patients (out of 26, 61.5%) and three caregivers (33.3%) that did not accept the app, 14 patients and three caregivers were interviewed given the reached data saturation. Reasons for not accepting the app mainly relied on the perceived inability to use the mobile phone (eg, for visual impairment) or app-related functions and the lack of a mobile phone. Other participants reported different reasons, such as lack of time to insert data or to take care of the relative, wishing not to complicate the relative’s caregiving, preferring the written diary, or thinking that telemedicine means having a remote relationship with a stranger.
Out of the 10 participants who agreed to use the app, four caregivers (out of six managing the app) and four patients (out of four managing the app) were interviewed. Furthermore, one patient was interviewed even if the app was managed by the caregiver, given the caregiver, even though accepting to manage the app, did not contribute to HF self-care of the relative and thus was not enrolled in the study. Three categories emerged from the narration about the use of the app.
Firstly, the category “Reasons for accepting the app use” referred to the expected usefulness in preventing negative events, registering data to obtain FNCs’ feedback, and monitoring the relative’s health status. The second and third categories are the “Modalities of app use” and “Satisfaction with the app”. The five participants who regularly used the app reported good functionality and highlighted the need to enter data regularly to maintain the ability to use the app. These participants considered the app useful for managing health problems and appreciated the ease of entering the data. However, some of these five patients highlighted the importance of receiving feedback from health professionals, even when there were no health issues:
Giving an answer on the app as feedback of parameters entered is important for me… the oxygen saturation is always good but why am I so breathless? So, a nurse who answers the fatigue you have is due to the mask you put on your mouth “for example... it serves... because I enter the pressure every day and then I don’t have an answer when I am fine... then it means that I report it just for me”.
Participants who used the app inconstantly (5, 50%, two patients, and three caregivers) considered it useful and easy; however, they missed entering data because of forgetfulness, lack of time, or not measuring parameters:
I have no difficulties, the app is well done, intuitive. I should be more diligent in measuring the pressure, I rarely do it, but I should do it more often. It’s not that I don’t use the app, but that I don’t use the tool for blood pressure…
In addition, caregivers expressed issues in reporting timely in the app the data collected from relatives in the written diary, especially when they did not live in the same house.
Discussion
In this study, we tested a community-based nurse-led model of care to manage patients with stable HF with GPs, cardiologists, and digital interventions.
Starting from enrolment, we did not reach the feasibility cut-off. Only 19% of the screened patients were enrolled, failing to intercept the target population of outpatients with stable HF, mostly because screened patients did not meet the HF inclusion criteria. Patients could be recruited during visits with the GP or cardiologist; therefore, there was the likelihood of both a high level of complexity when accessing a cardiologist and no HF diagnosis when visiting a GP. In the last case, it might happen that GP considers stable patients who have symptoms referrable to HF or, for example, diuretic therapy prescriptions without a diagnostic examination to confirm the diagnosis, especially in the elderly. Both explanations may explain why the 51 patients did not meet the HF inclusion criteria. A recent experience demonstrated similar difficulties in recruitment in hospitals for a home care program in which only 37% of dyads were included, mostly due to lack of HF diagnosis or caregivers.30 However, most participants said that they adhered to the GP’s instructions. This suggests that keeping the GPs involved in recruitment might have a positive impact on the participants’ decision to adhere to the model of care. However, the recruitment strategy should be improved by adding other possibilities for recruitment, such as hospital discharge.
Differently from the recruitment, the retention of participants was successful.
Regarding self-care abilities, the care model significantly improved self-care scores across all dimensions, with a higher impact on self-care monitoring. As for caregivers, we noticed an increase in all self-care dimensions, with the largest increase in self-maintenance. These results were confirmed by several studies that tested nurse-led interventions on self-care, reflecting the difficulties in improving self-management.3,18,31 Low pre-post self-management abilities might be explained by the condition of stability, which does not allow patients and caregivers to experience symptoms and, therefore, not learn from experience.
When we merged quantitative and qualitative data to assess the underlying mechanism of model functioning, confirming meta-inference emerged as the most frequent, while discordant meta-inferences emerged to a lesser extent. Discrepancies between qualitative and quantitative measures were mainly related to self-maintenance and self-monitoring, which might be explained by the specificity of the SCHFI items in relation to HF, while participants during the interviews reported changes in daily habits to a larger extent beyond HF. Experience did not differ significantly between participants with relevant changes and those with no relevant changes in self-care. However, we found that participants with relevant changes in self-care reported that more strategies appreciated as useful, including the emphasis on facilitating access to care, the quality of the relationship with FCNs, and support received to be more engaged. The absence of relevant changes in at least two self-care dimensions seems to be related to the discomfort of the distance from home, the absence of symptoms, and the perception that the service is useful only for urgent needs or actual symptoms. This suggests the need to ensure the proximity of the FCN clinic to patients’ homes and include home visits by the FCN, similar to other effective studies.3 In addition, effective engagement strategies should be identified for patients perceiving their situation of clinical stability as normal and considering conversation with FCN as chatting rather than motivational conversation. As suggested by previous studies, motivational interviewing might be ineffective in some patients, including those with high self-care at baseline or those taking few medications.32
Regarding the mobile app, we reached the feasibility cut-off for the green zone for the number of participants who accepted to use the app, and the amber zone for the number of participants who regularly used the app. The proportion of patients who agreed to use the app was low compared to other available studies.33 However, we considered this result acceptable for two reasons. First, we foresaw the possibility of choosing to be taken in charge with or without the app at the discretion of patients or caregivers. Second, we should consider that elderly have difficulties in using m-health, especially when an active role is required to enter data. Reasons for not accepting the use of the app were mainly related to the lack of mobile phones or low self-efficacy in using it, similar to available evidence.34 Due to the low rate of app use, we were unable to draw conclusions on the impact of the app on self-care. However, evidence supports the use of telemonitoring systems and m-health to improve self-care among community-dwelling HF patients,8 demonstrating an additional improvement in self-care when added to a home-care nurse-led specific HF program.3
This study had several limitations. First, we adopted different screening strategies, both by GPs and cardiologists, which might have different knowledge and perspectives regarding patients and families. However, the second step of FCNs screening controlled for potential errors in recruitment. Second, the SCHFI was completed autonomously or with the help of an FCN, given that a relevant number of patients were older and lived alone, thus leading to a potential bias in the answers. However, the FCNs were trained to prevent answer-induction or patients’ perceptions of judgment. Third, the sample was small, given that as a feasibility study, we did not foresee a large sample, and no control group was included, preventing the possibility of identifying specific patterns and associations between self-care outcomes and experiences. Therefore, our results may not be considered in terms of the efficacy of the model and should be interpreted with caution. However, the aim was not to test the efficacy of the model, but rather to test its feasibility. Patients with complex HF are usually managed by specialized services as a reactive model of care after hospitalization or acute events. We tried to shift the focus to patients with stable HF to keep them aware of the importance of performing self-care, even when they feel good to prevent and manage early acute decompensation, with a proactive approach.
Conclusion
In conclusion, this model could be a solution for managing patients with stable HF outside the hospital, fostering the role of primary care health professionals, although it was not feasible in recruiting. Changes and improvements are needed to reinforce the recruitment strategies, adding home visits, engaging those that perceive worthless the regular monitoring, and educational strategies to improve self-management, such as clinical cases, simulation, or role-playing, to stimulate reflection and decision-making. The m-health intervention might be improved by adding support for caregivers in using the app and devices that transmit directly to the app, thus also encouraging patients with low self-efficacy in using the mobile phone or app. The relationship between different interventions and outcomes should be deeply investigated with larger mixed-method studies, especially regarding the use of m-health in stable and low-risk patients.
Ethical Statement
The study was performed in accordance with the Declaration of Helsinki, and the study protocol was approved by the Local Ethics Committee of the Local Healthcare Trust (Comitato etico per le Sperimentazioni Cliniche, Azienda Provinciale per i Servizi Sanitari, Provincia autonoma di Trento, n.130951304). Signed informed consent including the authorization to publish anonymized responses was obtained from all participants.
Acknowledgments
The authors are grateful to the participating GPs, cardiologists, nurses, managers, and tech experts involved in this research.
Author Contributions
All authors meet the following criteria:
- Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
- Have drafted or written, or substantially revised or critically reviewed the article.
- Have agreed on the journal to which the article will be submitted.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Funding
The authors did not receive fundings for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
2. Son YJ, Choi J, Lee HJ. Effectiveness of nurse-led heart failure self-care education on health outcomes of heart failure patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(18):1–14. doi:10.3390/ijerph17186559
3. Jiang Y, Koh KWL, Ramach S, et al. The effectiveness of a nurse-led home-based heart failure self-management programme (the HOM-HEMP) for patients with chronic heart failure: a three-arm stratified randomized controlled trial. Int J Nurs Stud. 2021;122:104026. doi:10.1016/j.ijnurstu.2021.104026
4. Longhini J, Canzan F, Mezzalira E, Saiani L, Ambrosi E. Organisational models in primary health care to manage chronic conditions: a scoping review. Health Soc Care Community. 2022;30(3):e565–e588. doi:10.1111/hsc.13611
5. World Health O. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; 2019.
6. Krzesiński P, Jankowska EA, Siebert J, et al. Effects of an outpatient intervention comprising nurse-led non-invasive assessments, telemedicine support and remote cardiologists’ decisions in patients with heart failure (AMULET study): a randomised controlled trial. Eur J Heart Fail. 2021;24(3):565–577. doi:10.1002/ejhf.2358
7. Kitsiou S, Vatani H, Paré G, et al. Effectiveness of Mobile Health Technology Interventions for Patients With Heart Failure: systematic Review and Meta-analysis. Canadian J Cardiol. 2021;37(8):1248–1259. doi:10.1016/j.cjca.2021.02.015
8. Nick JM, Roberts LR, Petersen AB. Effectiveness of telemonitoring on self-care behaviors among community-dwelling adults with heart failure: a quantitative systematic review. JBI Evidence Synthesis. 2021;19(10):2659–2694. doi:10.11124/JBIES-20-00329
9. Drews TEI, Laukkanen J, Nieminen T. Non-invasive home telemonitoring in patients with decompensated heart failure: a systematic review and meta-analysis. ESC Heart Failure. 2021;8(5):3696–3708. doi:10.1002/ehf2.13475
10. Kitko L, McIlvennan CK, Bidwell JT, et al. Family Caregiving for Individuals with Heart Failure: a Scientific Statement from the American Heart Association. Circulation. 2020;141(22):e864–e878. doi:10.1161/CIR.0000000000000768
11. Creswell JW, Clark VL. Designing and Conducting Mixed Methods Research.
12. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061–n2061. doi:10.1136/bmj.n2061
13. O’Cathain A, Murphy E, Nicholl J. The quality of mixed methods studies in health services research. J Health Serv Res Policy. 2008;13(2):92–98. doi:10.1258/jhsrp.2007.007074
14. Billingham SAM, Whitehead AL, Julious SA. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom Clinical Research Network database. BMC Med Res Methodol. 2013;13(1):104. doi:10.1186/1471-2288-13-104
15. Bodenheimer T, Wagner EH, Grumbach K. Improving Primary Care for Patients With Chronic IllnessThe Chronic Care Model, Part 2. JAMA. 2002;288(15):1909–1914. doi:10.1001/jama.288.15.1909
16. Bodenheimer T, Wagner EH, Grumbach K. Improving Primary Care for Patients With Chronic Illness. JAMA. 2002;288(14):1775–1779. doi:10.1001/jama.288.14.1775
17. Bodenheimer T. Teach-back: a simple technique to enhance patients’ understanding. Fam Pract Manag. 2018;25(4):20–22.
18. Vellone E, Rebora P, Ausili D, et al. Motivational interviewing to improve self-care in heart failure patients (MOTIVATE-HF): a randomized controlled trial. ESC Heart Failure. 2020;7(3):1309–1318. doi:10.1002/ehf2.12733
19. Miller W, Rollnick S. Motivational Interviewing: Helping People Change.
20. Backman WD, Levine SA, Wenger NK, Harold JG. Shared decision-making for older adults with cardiovascular disease. Clin Cardiol. 2020;43(2):196–204. doi:10.1002/clc.23267
21. Jack E, Maskrey N, Byng R. SHERPA: a new model for clinical decision making in patients with multimorbidity. Lancet. 2018;392(10156):1397–1399. doi:10.1016/S0140-6736(18)31371-0
22. Ghizzardi G, Arrigoni C, Dellafiore F, Vellone E, Caruso R. Efficacy of motivational interviewing on enhancing self-care behaviors among patients with chronic heart failure: a systematic review and meta-analysis of randomized controlled trials. Heart Fail Rev. 2022;27(4):1029–1041. doi:10.1007/s10741-021-10110-z
23. Wright LM, Leahey M. A Guide to Family Assessment. Int J Med. 2013. doi:10.1016/j.ijnurstu.2012.10.009
24. Avery KNL, Williamson PR, Gamble C, et al. Informing efficient randomised controlled trials: exploration of challenges in developing progression criteria for internal pilot studies. BMJ Open. 2017;7(2):e013537–e013537. doi:10.1136/bmjopen-2016-013537
25. Vellone E, De Maria M, Iovino P, et al. The Self-Care of Heart Failure Index version 7.2: further psychometric testing. Res Nurs Health. 2020;43(6):640–650. doi:10.1002/nur.22083
26. Vellone E, Barbaranelli C, Pucciarelli G, Zeffiro V, Alvaro R, Riegel B. Validity and Reliability of the Caregiver Contribution to Self-Care of Heart Failure Index Version 2. J Cardiovasc Nurs. 2020;35(3):280–290. doi:10.1097/JCN.0000000000000655
27. Riegel B, Lee CS, Dickson VV, Carlson B. An update on the self-care of heart failure index. J Cardiovasc Nurs. 2009;24(6):485–497. doi:10.1097/JCN.0b013e3181b4baa0
28. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
29. Younas A, Pedersen M, Durante A. Characteristics of joint displays illustrating data integration in mixed-methods nursing studies. J Adv Nurs. 2020;76(2):676–686. doi:10.1111/jan.14264
30. Irani E, Niyomyart A, Dolansky MA, et al. A pilot randomized clinical trial of a teamwork intervention for heart failure care dyads. Heart Lung. 2021;50(6):877–884. doi:10.1016/j.hrtlng.2021.07.008
31. Sahlin D, Rezanezad B, Edvinsson ML, Bachus E, Melander OLLE, Gerward S. Self-care Management Intervention in Heart Failure (SMART-HF): a Multicenter Randomized Controlled Trial. J Card Fail. 2022;28(1):3–12. doi:10.1016/j.cardfail.2021.06.009
32. Stawnychy MA, Zeffiro V, Iovino P, Vellone E, Riegel B. Characteristics of Patients Who Do Not Respond to Motivational Interviewing for Heart Failure Self-care. J Cardiovasc Nurs. 2021;37(5):E139–E148. doi:10.1097/JCN.0000000000000840
33. Chew HSJ, Sim KLD, Choi KC, Chair SY. Effectiveness of a nurse-led temporal self-regulation theory-based program on heart failure self-care: a randomized controlled trial. Int J Nurs Stud. 2021;115:103872. doi:10.1016/j.ijnurstu.2021.103872
34. Cajita MI, Hodgson NA, Lam KW, Yoo S, Han H-R. Facilitators of and Barriers to mHealth Adoption in Older Adults With Heart Failure. Comput Inform Nurs. 2018;36(8):376–382. doi:10.1097/CIN.0000000000000442
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.