Back to Journals » Cancer Management and Research » Volume 17

Identification of Symptom Clusters and Sentinel Symptoms During Radiotherapy in Lung Cancer Patients: A Longitudinal Study
Authors Zhang J, Li S, Wu J, Yang B, Tan X, Zhang G, Zhao X
Received 27 April 2025
Accepted for publication 19 September 2025
Published 7 October 2025 Volume 2025:17 Pages 2307—2318
DOI https://doi.org/10.2147/CMAR.S536992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Jiang Zhang,1,* Song Li,2,* Jiang Wu,1,* Bingkun Yang,1 Xiangxiu Tan,2 Guilan Zhang,3 Xijuan Zhao4
1Department of Radiation Oncology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Peking University Cancer Hospital Yunnan, Kunming, People’s Republic of China; 2Department of Thoracic Surgery I, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Peking University Cancer Hospital Yunnan, Kunming, People’s Republic of China; 3Nursing Department, Kunming Municipal Hospital of Traditional Chinese Medicine, Kunming, People’s Republic of China; 4Department of Oncology, The Second Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guilan Zhang, Nursing Department, Kunming Municipal Hospital of Traditional Chinese Medicine, Kunming, People’s Republic of China, Email [email protected] Xijuan Zhao, Department of Oncology, The Second Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China, Email [email protected]
Purpose: This study longitudinally examined symptom clusters and sentinel symptoms in lung cancer patients across radiotherapy phases, providing a theoretical foundation for targeted symptom management.
Methods: In this prospective longitudinal study, 244 patients were recruited via convenience sampling from a tertiary cancer hospital in Southwest China between January and December 2024. Data were collected using the General Demographic Questionnaire and MD Anderson Symptom Inventory (including the lung cancer module). Assessments occurred at four time points: T1 (one day before radiotherapy), T2 (after 10 sessions), T3 (after 20 sessions), and T4 (at end of radiotherapy). Exploratory factor analysis identified symptom clusters from symptoms with > 20% incidence, while Apriori algorithm modeling analyzed intra-cluster associations to determine sentinel symptoms.
Results: Five symptom clusters emerged: psychological (sadness, distress, sleep disturbance), respiratory (chest tightness, shortness of breath), lung cancer-specific (coughing, expectoration), radiotherapy side-effect (dry mouth, pain, decreased appetite), and perceptual (at T1: pain, numbness, at T2: dry mouth, pain, decreased appetite, numbness, constipation, at T3 and T4: forgetfulness, somnolence, fatigue, nausea, constipation). At T1, distress, shortness of breath, and coughing were sentinel symptoms for the psychological, respiratory, and lung cancer-specific clusters, respectively. Pain was the sentinel for the radiotherapy side-effect cluster at T3, and somnolence for the perceptual cluster at T4.
Conclusion: Lung cancer patients exhibit multiple stable symptom clusters during radiotherapy, with sentinel symptoms varying by phase. These insights offer new perspectives on timed assessments and precision nursing interventions, while providing key theoretical and practical guidance for building early warning models and intelligent symptom management pathways.
Keywords: lung cancer, radiotherapy, symptom clusters, sentinel symptoms, longitudinal study
Introduction
Lung cancer is one of the most prevalent malignancies worldwide, with 2.5 million new cases and 1.8 million deaths reported globally in 2022 according to the latest data from the International Agency for Research on Cancer (IARC).1 In China, lung cancer remains the most common cancer, with 1.0606 million new cases and 73.33 million deaths in 2022 alone, posing a serious threat to human health.2 Radiotherapy is an important treatment and is applicable across all disease stages and performance statuses for lung cancer. It can effectively control tumor progression and significantly prolong patient survival. However, while killing tumor cells, radiation can cause varying degrees of damage to normal lung tissue and adjacent organs.3–5 Consequently, patients experience a series of distressing symptoms such as fatigue, radiation pneumonitis, radiation esophagitis, pain, and anxiety that tend to co-occur and interact.6–9 Symptom clusters are composed of two or more interrelated symptoms, and there may be common causes and mechanisms between these symptoms.10 A symptom cluster is defined as two or more interrelated symptoms that may exist common etiologies and pathophysiologic pathways. Compared with a single symptom, the effect of symptom clusters on patients is enhanced and synergistic, which further affects the treatment effect, physical function, prognosis and quality of life of patients.11,12
Identifying symptom clusters may help healthcare providers develop targeted symptom management plans via the characteristics of the clusters, thereby improving the efficiency of symptom management.13,14 However, there is still no consensus on how to select the most effective symptoms to manage to achieve the best intervention outcomes.15 Sentinel symptoms are early-occurring indicators that both predict the presence of a symptom cluster and act as key drivers for the subsequent emergence of other symptoms within that cluster. Identifying sentinel symptoms simplifies clinical assessment and nursing management of symptom clusters and may serve as an effective entry point for targeted symptom-cluster interventions.16,17 Luo Y et al18 identified sentinel symptoms in 169 lung cancer patients during the first cycle of chemotherapy in a prospective study and reported that sentinel symptoms in lung cancer patients’ symptom clusters appear earlier than other symptoms do and are important indicators for implementing symptom management, potentially alleviating or slowing the progression of other symptoms within the cluster. Brown J et al14 also assessed symptom experiences of 196 women with lung cancer over the past day and past four weeks. The results identified a cluster comprising fatigue, dyspnea, cough, pain, and anorexia as the most prevalent symptoms. Pain was emerged as the sentinel symptom of this cluster, confirming its predictive role for the subsequent appearance of other symptoms and underscoring its potential utility in clinical symptom assessment.
However, these studies are cross-sectional surveys of symptom clusters and sentinel symptoms in lung cancer patients at one or several time points, while ignoring the longitudinal changes of symptom clusters. Moreover, most of the current studies are sentinel symptoms of symptom clusters in lung cancer patients during radiotherapy, and it is not clear whether there are sentinel symptoms in lung cancer patients during radiotherapy. Therefore, it is necessary to clarify the longitudinal changes of symptom clusters and sentinel symptoms in lung cancer patients during radiotherapy, which will be served as the entry point for symptom cluster intervention, further reducing the generation or aggravation of other symptoms in the cluster, and improving the efficiency of symptom cluster intervention. The purpose of this study is to identify the symptom clusters and their internal correlations in different radiotherapy periods by using exploratory factor analysis and Apriori algorithm in a prospective longitudinal study, which provide scientific basis for clinical medical staff to evaluate symptoms and manage symptom clusters, ultimately may reducing the burden of symptoms and improving the quality of life of patients.
Methods
Patients and Setting
This prospective longitudinal study measured symptom clusters and sentinel symptoms in lung cancer patients at four time points: one day before radiotherapy, after 10 sessions, after 20 sessions, and at the end of radiotherapy. Patients were recruited from the radiotherapy departments of two tertiary general hospitals in Kunming, Yunnan Province, China, via convenience sampling. The inclusion criteria were as follows: (1) pathological or cytological diagnosis of lung cancer requiring radiotherapy with more than 20 sessions,19 (2) age over 18 years and voluntary signing of the informed consent form, (3) no cognitive or consciousness disorders and ability to complete the questionnaire, (4) undergoing intensity-modulated radiotherapy and completing at least 20 sessions. The exclusion criteria were as follows: (1) patients who had undergone lung cancer surgery within the past 3 months and received concurrent chemotherapy, (2) patients with severe heart, liver, or kidney failure or bone marrow dysfunction, (3) patients with other serious physical or mental health conditions. This study adheres to the ethical principles of the Declaration of Helsinki, ensuring informed consent and privacy protection for all participants. Additionally, this study was approved by the Ethics Committee of Yunnan Cancer Hospital (Approval No. SLKYLX2023-031).
Procedures
When patients initiated their initial radiotherapy cycle, the investigator explained the purpose and methods of the study to them. If patients agreed to participate, they completed the general demographic and disease-related questionnaires, as well as the initial MD Anderson Symptom Inventory. The scores of the MD Anderson Symptom Inventory were recorded after 10 or 20 sessions and after radiotherapy. The questionnaires were collected face-to-face, and the completeness of the responses was reviewed onsite. For those who could not complete the questionnaires independently, the researchers assisted the patients in completing the form. The participants were assured that all personal information would remain confidential and would only be used for research purposes.
Instruments
Sociodemographic and Clinical Characteristics
The questionnaire collected demographic data (age, sex, occupation, place of residence, education level, medical payment method, and family average income) and disease-related information (lung cancer cell type, disease duration, TNM stage, metastasis, number of radiotherapy sessions, comorbidities, and treatment history).
MD Anderson Symptom Inventory – Revised Lung Cancer Module
The MD Anderson Symptom Inventory was developed by Cleeland et al at the University of Texas M. D. Anderson Cancer Center in 2000.20 In 2011, a lung cancer-specific module was developed on the basis of this inventory.21 Zang Yu et al22 revised the MD Anderson Symptom Inventory and the lung cancer module to adapt them to the Chinese context. The revised inventory includes 19 symptom items: the former 13 items are common cancer core symptoms, including pain, shortness of breath, forgetfulness, etc., and the last 6 items are lung cancer-specific symptoms, including chest tightness, cough, hemoptysis, etc. The occurrence of symptoms was calculated on the basis of whether the symptoms were present and the severity of symptoms was rated on an 11-point Likert scale, with 0 indicating “no symptoms” and increasing incrementally to 10 indicating “the most severe degree perceivable”. The Cronbach’s α coefficient of the inventory is 0.925,22 and it is widely used for symptom assessment in Chinese lung cancer patients. The Cronbach’s α coefficients for the four measurements in this study were 0.744, 0.805, 0.852, and 0.874, respectively.
Data Analysis
The data were analyzed via SPSS 29.0 and SPSS Modeler 18.0. Categorical variables are presented as frequencies and percentages. Continuous variables with a normal distribution are described as mean ± standard deviation. Non-normally distributed data are reported as median and quartile ranges (M (P25, P75)). Exploratory factor analysis (EFA) was performed on symptoms whose incidence exceeded 20% at each study time-point.23 Principal component analysis (PCA) was used to extract common factors (ie, symptom clusters), followed by varimax orthogonal rotation. Internal consistency of the clusters was assessed with Bartlett’s test of sphericity (P < 0.05) and the Kaiser-Meyer-Olkin (KMO) measure. Factors were retained according to the following criteria: eigenvalue ≥ 1, individual symptom loadings ≥ 0.5 on the respective factor, and assignment of cross-loading symptoms (≥ 0.5 on two or more factors) to the factor with the highest loading. Each factor had to contain at least two symptoms. Symptom clusters were named on the basis of their constituent symptoms, existing literature, and clinical expertise. Statistical significance was set at α = 0.05 (P < 0.05).
After symptom clusters were established, the Apriori algorithm was employed to identify sentinel symptoms within each cluster. As the most widely used association-rule mining technique in data science, Apriori efficiently uncovers fundamental patterns and latent relationships among variables.18,24 In this study, items from the M. D. Anderson Symptom Inventory–Lung Cancer Module (MDASI-LC) were transferred into binary variables (“symptom present = 1 / absent = 0”). The analysis was restricted to the 244 patients who completed all assessments at the end of radiotherapy (T4). Separate Apriori models were run for each of the four time points (T1–T4) and within each symptom cluster to identify sentinel symptoms.
A symptom was designated as sentinel if it fulfilled all of the following criteria: (1) support ≥ 40% when serving as the antecedent, (2) confidence ≥ 60% for the rule, (3) confidence of the rule exceeded the support of the antecedent. Only symptoms that repeatedly appeared as antecedents and demonstrated strong associative linkages with subsequent symptoms were retained as sentinel symptoms,25 thereby minimizing spurious co-occurrences while balancing prevalence and association strength. Data-processing workflow: (1) import symptom data at each time point (present = 1, absent = 0), (2) set variables as binary, (3) connect Apriori node with parameters: minimum support = 40%, minimum confidence = 60%, minimum rule length = 2, (4) execute the model to generate association rules, (5) filter rules meeting all three sentinel-criteria and whose confidence exceeds the antecedent’s support, (6) export the final rule report.
Results
Sociodemographic and Clinical Characteristics
Between January and October 2024, a total of 244 patients with lung cancer who were receiving radiotherapy completed the study. Six patients had their radiotherapy interrupted, and 10 patients withdrew from the study and were excluded. Among the remaining participants, 198 were male (81.15%), and 46 were female (18.85%). The age distribution was as follows: 129 patients (52.87%) were under 60 years old, and 115 patients (47.13%) were 60 years old or older. The educational level was as follows: 119 patients (48.77%) had an elementary school education or lower, 70 patients (28.69%) had a junior high school education, 28 patients (11.48%) had a high school or vocational school education, and 27 patients (11.07%) had a college education or higher. The marital status was as follows: 232 patients (95.08%) were married, and 12 patients (4.92%) were unmarried. The occupational status was as follows: 152 patients (62.30%) were manual laborers, 16 patients (6.56%) were civil servants or employees of public institutions, and 76 patients (31.15%) were unemployed or retired. The places of residence were as follows: 55 patients (22.54%) lived in cities, 25 patients (10.25%) lived in counties or towns, and 164 patients (67.21%) lived in rural areas or towns. The monthly household income was as follows: 57 patients (23.36%) had an income of less than 2000 RMB, 62 patients (25.41%) had an income between 2000 and 3999 RMB, 33 patients (13.52%) had an income between 4000 and 5999 RMB, and 92 patients (37.70%) had an income of 6000 RMB or more. The medical payment method was as follows: 69 patients (28.28%) had employee medical insurance, and 175 patients (71.72%) had resident medical insurance. The disease duration was as follows: 142 patients (58.20%) had a duration of less than 12 months, 45 patients (18.44%) had a duration between 12 and 24 months, and 57 patients (23.36%) had a duration of 24 months or more. The cell type distribution was as follows: 70 patients (28.69%) had squamous cell carcinoma, 110 patients (45.08%) had adenocarcinoma, 49 patients (20.08%) had small cell lung cancer, and 15 patients (6.15%) had other types. The disease stage was as follows: 131 patients (53.69%) were in stage III, and 113 patients (46.31%) were in stage IV. The degree of metastasis was as follows: 126 patients (51.64%) had local metastasis, and 118 patients (48.36%) had distant metastasis. The previous treatment history was as follows: 27 patients (11.07%) had no treatment, 6 patients (2.46%) had targeted or immunotherapy, 104 patients (42.62%) had chemotherapy, 46 patients (18.85%) had chemotherapy combined with targeted or immunotherapy, 10 patients (4.10%) had surgery, and 51 patients (20.90%) had surgery combined with chemotherapy or targeted therapy or immunotherapy (Table 1).
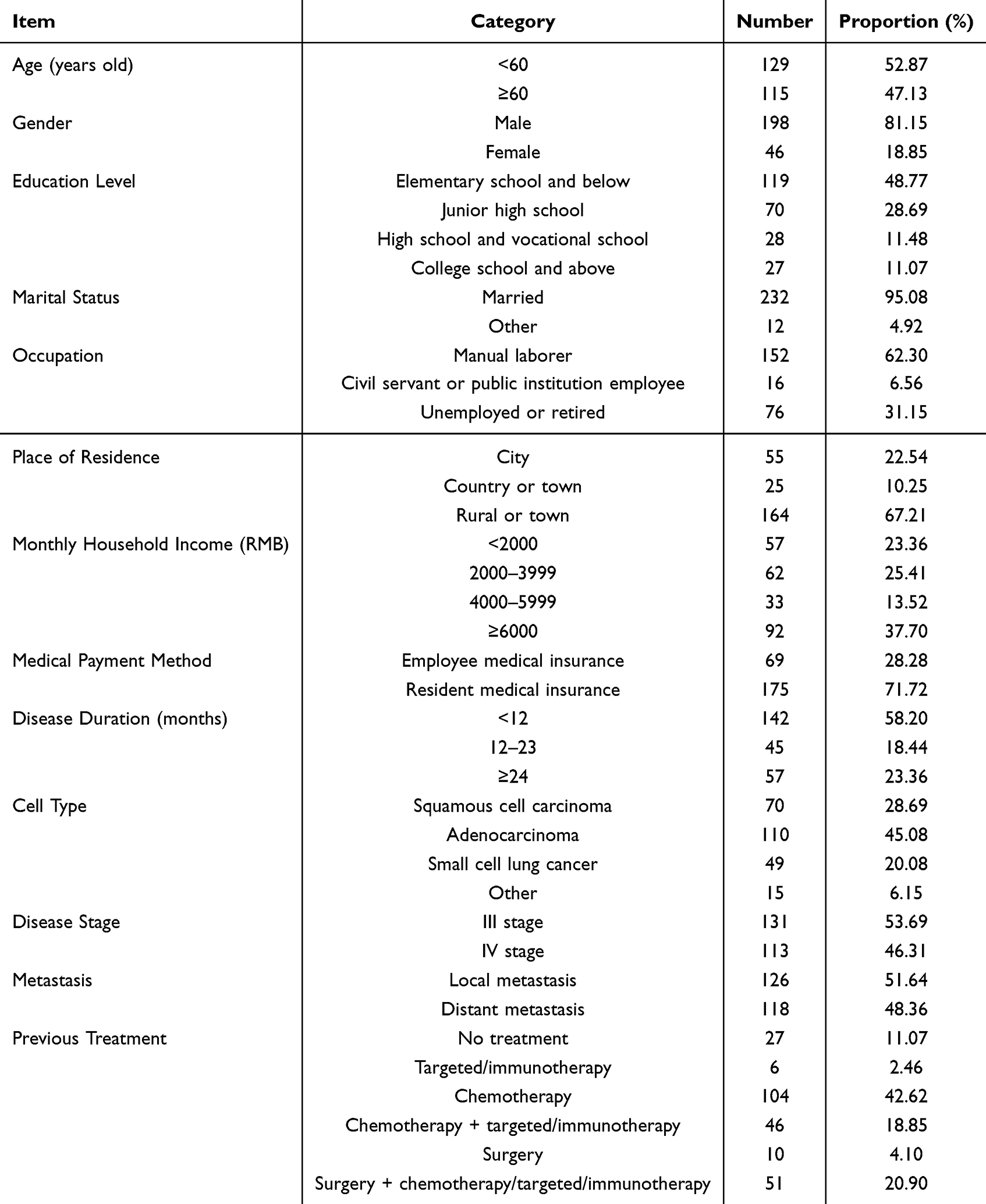 |
Table 1 Sociodemographic and Clinical Characteristics of the Participants (n = 244) |
Characteristics of Individual Symptoms at Different Time Points During Radiotherapy in Middle-aged and Elderly Lung Cancer Patients
Before radiotherapy, coughing and expectoration had the highest incidence rates. After 10 sessions of radiotherapy, the incidence rates of coughing and expectoration did not increase significantly, but the incidence rates of dry mouth and pain increased significantly. After 20 sessions of radiotherapy, the incidence rates of coughing, expectoration, dry mouth, and pain, and fatigue were high. At the end of radiotherapy, the incidence rates of all symptoms except chest tightness, shortness of breath, and hemoptysis were high (Table 2).
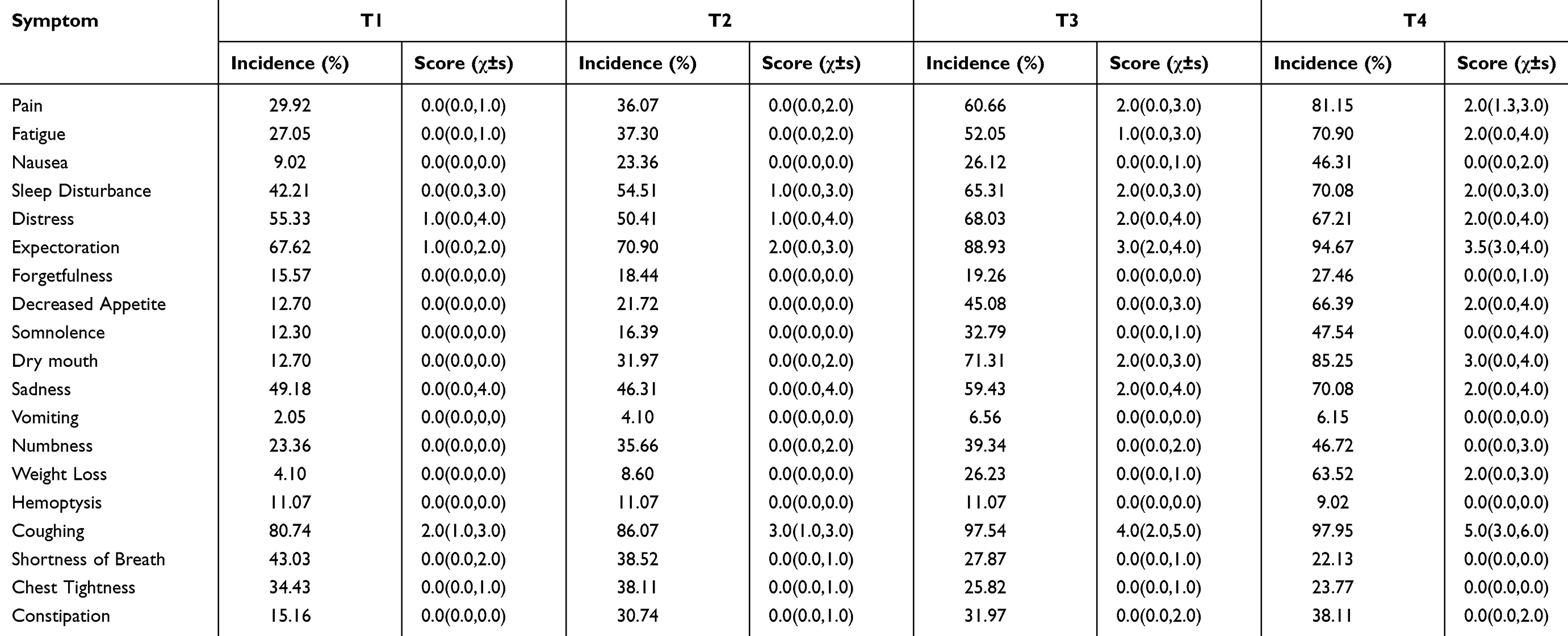 |
Table 2 Incidence and Severity of Symptoms at Different Time Points During Radiotherapy in Lung Cancer Patients (n = 244) |
Symptom Clusters in Lung Cancer Patients During Different Periods of Radiotherapy
After extracting the symptoms with an incidence of more than 20% during radiotherapy, factor analysis was performed on the data at each time point. The KMO values for T1, T2, T3, and T4 were 0.602, 0.703, 0.772, and 0.806, respectively, and Bartlett’s test of sphericity (all P < 0.001) indicated that the conditions for factor analysis were met. At T1, 10 symptoms had an occurrence rate more than 20%, and four common factors were extracted: the psychological symptom cluster, respiratory symptom cluster, perceptual symptom cluster, and lung cancer-specific symptom cluster. At T2, 14 symptoms had an occurrence rate more than 20%, and four common factors were extracted: the psychological symptom cluster, respiratory symptom cluster, perceptual symptom cluster, and lung cancer-specific symptom cluster. At T3, 16 symptoms had an occurrence rate more than 20%, and five common factors were extracted: the psychological symptom cluster, the perceptual symptom cluster, the lung cancer-specific symptom cluster, the respiratory symptom cluster, and the radiotherapy side-effect symptom cluster. At T4, 17 symptoms had an occurrence rate more than 20%, and five common factors were extracted: the psychological symptom cluster, the perceptual symptom cluster, the lung cancer-specific symptom cluster, the respiratory symptom cluster, and the radiotherapy side-effect symptom cluster (Table 3).
 |
Table 3 Rotated Factor Loadings of Symptoms in Lung Cancer Patients During Different Periods of Radiotherapy |
Sentinel Symptoms in Different Symptom Clusters During Different Periods of Radiotherapy
The Apriori algorithm was used to explore the existence of sentinel symptoms within each symptom cluster. At T1, six valid association rules were extracted for the psychological symptom cluster, which were mainly constructed around symptoms such as “distress”, “sleep disturbance”, and “sadness”. These three symptoms repeatedly appeared as antecedents, each demonstrating support > 40% and confidence > 60%. Consequently, “distress” was identified as the sentinel symptom occupying the pivotal node within this cluster. In the respiratory symptom cluster, a single valid association rule was extracted, linking “dyspnea” and “chest tightness”, both exceeding the 40% support and 60% confidence thresholds. The pattern indicates that “dyspnea” functions as the pivotal node within this cluster and is therefore designated as its sentinel symptom. Two valid association rules were extracted within the lung-cancer-specific symptom cluster, both centering on “cough” and “sputum production.” Both indicators met the required support and confidence standard, suggesting that “cough” acts as the pivotal node in this cluster and is therefore designated its sentinel symptom. At T3, four valid association rules were extracted from the radiotherapy-side-effect symptom cluster. These rules primarily involved “pain”, “dry mouth”, and “decreased appetite”. All three symptoms repeatedly served as antecedents, with both support and confidence surpassing the preset thresholds. Among them, “pain” demonstrated the strongest associative link and was therefore designated the sentinel symptom of this cluster. At T4, four valid association rules were extracted within the sensory symptom cluster, centering on “drowsiness”, “constipation”, and “fatigue”. These three symptoms repeatedly appeared as antecedents across the rules, each satisfying the required support and confidence thresholds. The pattern indicates that “drowsiness” occupies the pivotal node in this cluster and is therefore designated its sentinel symptom (Table 4).
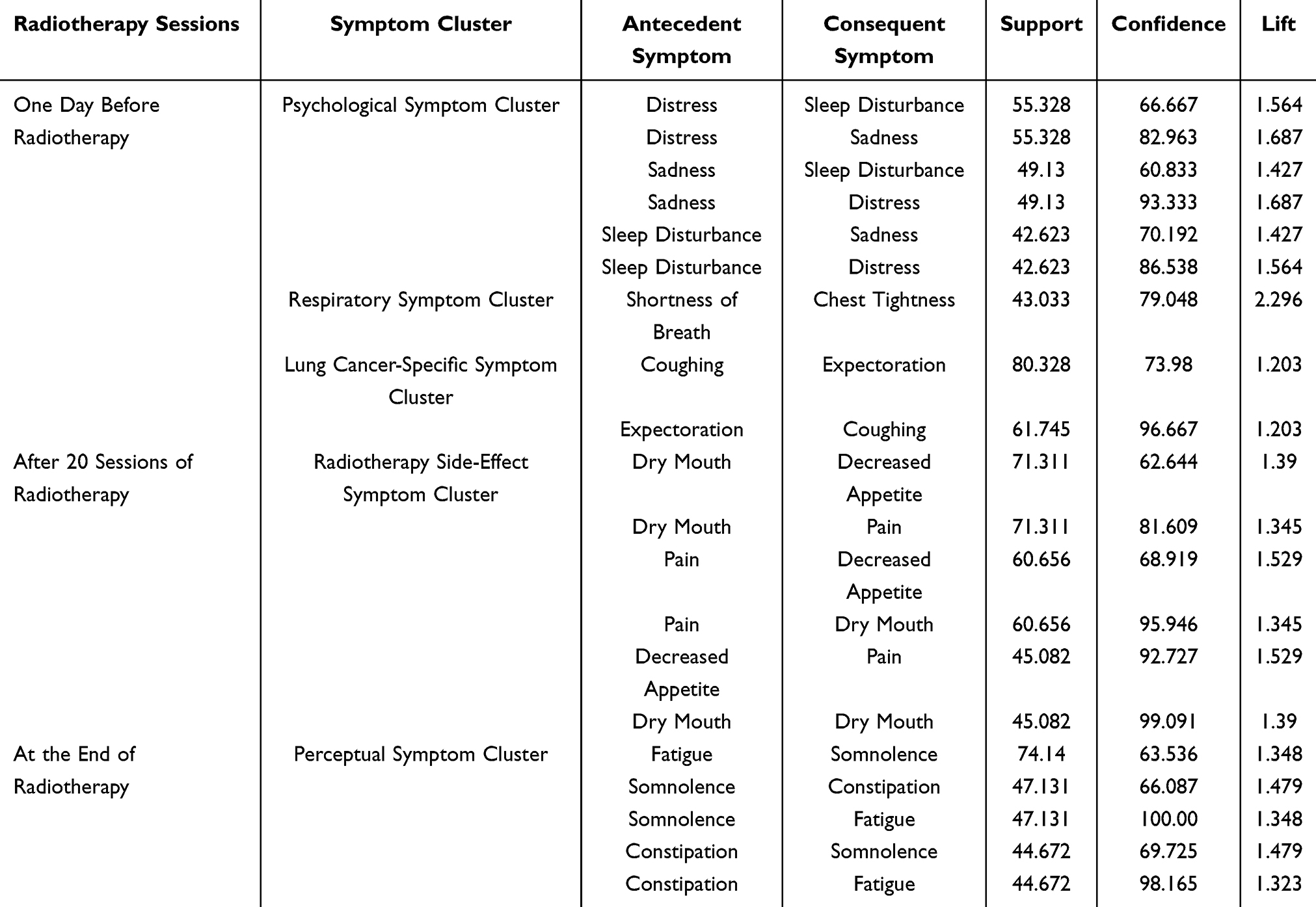 |
Table 4 Apriori Algorithm Results for Symptom Associations in Lung Cancer Patients Before Radiotherapy (N = 244) |
Discussion
This is the first study to investigate symptom clusters and sentinel symptoms in lung cancer patients during radiotherapy. We found that five symptom clusters exist during radiotherapy, with psychological, respiratory, and lung cancer-specific symptom clusters persisting from one day before radiotherapy to the end of treatment. These results are consistent with those of Li JJ et al26 and Ju X et al13 in lung cancer patients during the perioperative period and the first cycle of chemotherapy. Notably, the perceptual symptom cluster and the radiotherapy side effect symptom cluster were identified for the first time in lung cancer patients receiving radiotherapy and exhibited specificity in terms of the composition and onset time of symptoms. Ultimately, our study identified distress, shortness of breath, and coughing as sentinel symptoms for the psychological, respiratory, and lung cancer-specific symptom clusters, respectively. Pain was identified as the sentinel symptom for the radiotherapy side-effect symptom cluster after 20 sessions of radiotherapy, and somnolence was identified as the sentinel symptom for the perceptual symptom cluster at the end of radiotherapy. These findings provide new insights for symptom monitoring and management in lung cancer patients, potentially improving quality of life and treatment outcomes.
The psychological symptom cluster consists of sadness, distress, and sleep disturbance and persists throughout the radiotherapy period. One day before radiotherapy, the incidence rates of sadness, distress, and sleep disturbance were all close to 50%, and by the end of radiotherapy, these rates approached 70%. It shows that the psychological burden of patients is significantly increased with the process of radiotherapy. These results are similar to those of Luo Y et al18 in lung cancer patients during the first cycle of chemotherapy, confirming that the psychological symptom cluster is both highly prevalent and fluctuates across the different phases of radiotherapy in lung cancer patients. Notably, the present study identified “distress” as the sentinel symptom of this cluster, which differs from Luo et al’s report that “sadness” occupied the sentinel role.18 This discrepancy may be attributable to disease-specific factors, symptom burden, individual coping styles, social support, and intrusive thoughts.27–30 In mainland China, most patients referred for radiotherapy have either lost the opportunity for surgery or have relapsed after surgery, chemotherapy, targeted therapy, or immunotherapy. In our study, 88.93% had previously received other treatments. Before radiotherapy, most patients showed psychological distress such as worry, helplessness and distress due to economic pressure and poor early treatment. During radiotherapy, patients often show negative emotions such as tension, anxiety and distress when they have discomfort symptoms due to concerns about the efficacy and related side effects of radiotherapy, which affects patients’ cognition of disease and treatment, and reduces their compliance and cooperation with treatment. Studies have shown that long-term psychological distress can affect the autonomic nervous system and endocrine function, inhibit the immune system function, reduce the body ‘s tolerance to tumors and treatment-related adverse reactions, aggravate physical symptoms, and lead to adverse outcomes such as tumor metastasis, deterioration, and recurrence.27 Therefore, medical service providers need to carry out psychological assessment and management for sentinel symptoms such as distress, sadness and sleep disorders as soon as possible. Before radiotherapy, they can help patients reduce psychological distress and establish treatment confidence by means of distraction and positive motivation. Radiotherapy-related side effects and treatment effects were evaluated during and after radiotherapy to reduce the psychological burden of patients, improving radiotherapy tolerance and compliance and optimizing the treatment effect.
In our study, chest tightness and dyspnea formed the respiratory symptom cluster, with dyspnea identified as the sentinel symptom. The findings are basically consistent with those of Luo et al18 in Chinese patients during the first cycle of chemotherapy. However, there are still differences in the incidence of chest tightness and dyspnea between the two studies. Specifically, prevalence was similar before treatment, but as radiotherapy progressed, our patients reported markedly lower rates than those reported by Luo et al. The reasons may be as follows. Before radiotherapy, lung tumor, pleural effusion or hilar lymphadenopathy may compress the airway or lung, resulting in symptoms such as chest tightness and shortness of breath.31,32 During radiotherapy, radiotherapy can accurately irradiate the patient ‘s lung tumor and enlarged lymph nodes. According to the biological effects of radiotherapy, the tumor or metastatic lymph nodes may be significantly reduced after about 20 sessions of radiotherapy, thereby significantly alleviating the patient ‘s chest tightness and dyspnea.33 Combined with the changes of sentinel symptoms, chest tightness and dyspnea, it is suggested that medical providers should early evaluate the respiratory function of patients, and urge and encourage patients to carry out respiratory function exercise to alleviate the distress of respiratory symptoms.
The lung-cancer-specific symptom cluster is composed of cough and expectoration. Cough is regarded as the sentinel symptom of this symptom group. With the increase of radiotherapy times, the incidence of cough and expectoration is on the rise. In patients with lung cancer after surgery or chemotherapy, cough and expectoration are mostly attributed to respiratory symptom clusters.15,16,18 However, radiotherapy is different from the above treatment methods. Radiotherapy directly acts on lung tumors or lymph nodes via ray, and may also affect the normal tissue structure when killing tumor cells. In the middle and late stages of radiotherapy, patients may have cough and expectoration symptoms due to damage to tracheal mucosa and lung tissue.34,35 Combined with the particularity of sentinel symptoms and radiotherapy, it is suggested that medical providers should strengthen the supervision and health education of patients, persuade patients to quit smoking and increase daily drinking water to relieve cough symptoms. Meanwhile, patients are encouraged to carry out moderate aerobic exercise, endurance training and respiratory function exercise to slow down the loss of lung function. In view of the climatic characteristics of Yunnan, China, which is located in the plateau and has a large temperature difference between day and night, it is recommended that patients should keep warm and wear masks to reduce the impact of cold air stimulation on the respiratory tract, thereby reducing symptoms such as cough.
Perceptual symptom clusters and radiotherapy-related side effects symptom clusters are the first symptom clusters identified in patients with lung cancer radiotherapy. The perceptual symptom cluster was composed of pain and numbness on the day before radiotherapy. With the increase of the sessions of radiotherapy, the composition of the perceptual symptom cluster expanded to include dry mouth, pain, loss of appetite, numbness and constipation at 10 sessions of radiotherapy, and remained unchanged at 20 times of radiotherapy. The symptom cluster of radiotherapy-related side effects appeared for the first time and the 20th session of radiotherapy and remained stable This phenomenon may be related to the following factors: the patients receiving radiotherapy are mostly middle and late patients who have lost the chance of surgery or after surgery. All the patients were stage III and IV, and most of them were accompanied by lymph node metastasis and bone metastasis in this study. The surrounding normal nerves were susceptible to tumor compression, resulting in pain and numbness.36 Therefore, before radiotherapy, the patient ‘s perceptual symptom clusters were mainly pain and numbness. With the sessions of radiotherapy, radiotherapy-related side effects gradually appear and the degree is aggravated until 10 sessions of radiotherapy. Symptoms such as pain, dysphagia, fatigue and loss of appetite caused by radiation esophagitis may occur,6,18,37–39 making the perception symptom cluster items change accordingly, and the radiotherapy side effect symptom cluster appears. According to the Apriori algorithm, pain was identified as the sentinel symptom of the radiotherapy side-effect symptom cluster after 20 sessions of radiotherapy, and drowsiness was identified as the sentinel symptom of the perceived symptom cluster at the end of radiotherapy. Therefore, it is recommended that medical service providers should evaluate radiotherapy-related side effects every week for patients who have received radiotherapy more than 10 times, and timely relieve adverse reactions. Meanwhile, preventive use of esophageal, gastric mucosal protective agents, and skin protective agents can reduce the incidence of radiation esophagitis and dermatitis, and prevent symptom distress caused by radiotherapy-related side effects.
Limitations
This study has some limitations. First of all, the follow-up time extends to the end of the patient ‘s radiotherapy, and does not cover the long-term symptom distress after discharge. Secondly, this study only uses the Apriori association rule algorithm to explore the co-occurrence and sentinel symptoms of symptoms in different radiotherapy periods, and it is still unable to reveal the causal relationship between symptoms and effect prediction. In the future, it is suggested to carry out multi-center, large-sample longitudinal research, and integrate big data and artificial intelligence technology to construct a more accurate longitudinal change model of frailty symptoms to optimize the symptom identification and management in the process of radiotherapy and further improve the quality of life of lung cancer patients.
Conclusion
The study systematically identified the symptom clusters and sentinel symptoms of lung cancer patients during radiotherapy via prospective longitudinal analysis. Psychological, respiratory, and lung-cancer-specific clusters remained stable throughout the entire course of treatment. Perceptual symptom clusters and radiotherapy side effect symptom clusters are gradually emerging during the radiotherapy process. In different radiotherapy periods, the sentinel symptoms of each symptom group also showed phased changes: distress, dyspnea and cough were the main symptoms before radiotherapy, while pain and drowsiness were the main symptoms in the middle and late stages of radiotherapy. These sentinel symptoms have significant linkage and indicative significance within their respective symptom clusters, which can be used as an important reference for clinical symptom management. This study not only provides theoretical support for symptom assessment and precise nursing intervention during radiotherapy, but also lays a foundation for the establishment of subsequent early warning models and the development of intelligent intervention pathways.
Data Sharing Statement
The authors will provide all the raw data that support the conclusions of this paper upon request by the first author (Email: [email protected]).
Ethics Approval
This study adheres to the ethical principles of the Declaration of Helsinki, ensuring informed consent and privacy protection for all participants. Additionally, this study was approved by the Ethics Committee of Yunnan Cancer Hospital (Approval No. SLKYLX2023-031).
Acknowledgments
The authors thank the patients with lung cancer and the caregivers who agreed to participate in this study.
Author Contributions
All authors contributed significantly to the work reported whether in the conception, study design, execution, data acquisition, analysis and interpretation, or in multiple of these areas. Each author participated in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and accepts responsibility for all aspects of the work.
Funding
This study was supported by the Scientific Research Fund of the Yunnan Provincial Department of Education (2023Y0757 and 2024J0363) and the Chinese Nursing Association’s 2023 Established Scientific Research Project (ZHKYQ202312).
Disclosure
Jiang Zhang, Song Li and Jiang Wu are co-first authors for this study. The authors have no conflicts of interest to disclose in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Wang SM, Zheng RS, Han BF. Analysis of age characteristics of cancer incidence and mortality in Chinese population in 2022. Cancer Chin. 2024;33(03):165–174. doi:10.11735/j.issn.1004-0242.2024.03.A001
3. Li Y, Wang Q, Liu C, et al. Symptom clusters and their impact on quality of life among Chinese patients with lung cancer: a cross-sectional study. Eur J Oncol Nurs. 2023;67(102465):102465. doi:10.1016/j.ejon.2023.102465
4. Chen Z, He G, Zhao Y, et al. Symptom burden and emotional distress in advanced lung cancer: the moderating effects of physicians’ communication skills and patients’ disease understanding. Support Care Cancer. 2022;30(11):9497–9505. doi:10.1007/s00520-022-07323-9
5. Sharbafchi MR, Naji F, Ghaderi S, et al. Evaluating the prevalence of somatization symptoms in the family of cancer patients. Sci Rep. 2025;15(1):22583. doi:10.1038/s41598-025-85474-5
6. Fan G, Hadi S, Chow E. Symptom clusters in patients with advanced-stage cancer referred for palliative radiation therapy in an outpatient setting. Support Cancer Ther. 2007;4(3):157–162. doi:10.3816/SCT.2007.n.010
7. Wang Y, Fang L, Zhou K, et al. Symptom burden and clusters during chemotherapy in patients with lung cancer. World J Surg Oncol. 2024;22(1):309. doi:10.1186/s12957-024-03594-0
8. Chan CW, Richardson A, Richardson J. An investigation of a symptom cluster in Chinese patients with lung cancer receiving radiotherapy. Contemp Nurse. 2013;45(2):164–173. doi:10.5172/conu.2013.45.2.164
9. Grendarova P, Yannitsos D, Ahmed S, et al. Experience of individuals with lung and gastrointestinal cancers undergoing radiation therapy: a qualitative study. Support Care Cancer. 2024;33(1):51. doi:10.1007/s00520-024-09103-z
10. Kim HJ, McGuire DB, Tulman L, et al. Symptom clusters: concept analysis and clinical implications for cancer nursing. Cancer Nurs. 2005;28(4):270–82;quiz283–4. doi:10.1097/00002820-200507000-00005
11. Koyama N, Matsumura C, Tahara Y, et al. Symptom clusters and their influence on prognosis using EORTC QLQ-C15-PAL scores in terminally ill patients with cancer. Support Care Cancer. 2021;30(1):135–143. doi:10.1007/s00520-021-06380-w
12. Yang X, Bai J, Zhang J, et al. Symptom clusters and their impacts on the quality of life of patients with lung cancer receiving immunotherapy: a cross-sectional study. J Clin Nurs. 2024;34(5):1725–1740. doi:10.1111/jocn.17321
13. Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status of patients with cancer. Oncol Nurs Forum. 2001;28(3):465–470. PMID: 11338755.
14. Chen E, Nguyen J, Cramarossa G, et al. Symptom clusters in patients with lung cancer: a literature review. Expert Rev Pharm Out. 2011;11(4):433–439. doi:10.1586/erp.11.56
15. Ju X, Bai J, She Y, et al. Symptom cluster trajectories and sentinel symptoms during the first cycle of chemotherapy in patients with lung cancer. Eur J Oncol Nurs. 2023;63(102282):102282. doi:10.1016/j.ejon.2023.102282
16. Brown JK, Cooley ME, Chernecky C, et al. A symptom cluster and sentinel symptom experienced by women with lung cancer. Oncol Nurs Forum. 2011;38(6):E425–35. doi:10.1188/11.ONF.E425-E435
17. Donovan HS, Hagan TL, Campbell GB, et al. Nausea as a sentinel symptom for cytotoxic chemotherapy effects on the gut-brain axis among women receiving treatment for recurrent ovarian cancer: an exploratory analysis. Support Care Cancer. 2016;24(6):2635–2642. doi:10.1007/s00520-015-3071-4
18. Luo Y, Mao D, Zhang L, et al. Identification of symptom clusters and sentinel symptoms during the first cycle of chemotherapy in patients with lung cancer. Support Care Cancer. 2024;32(6):385. doi:10.1007/s00520-024-08600-5
19. Health Commission of the People’s Republic Of China N. National guidelines for diagnosis and treatment of lung cancer 2022 in China (English version). Chinese J Cancer Res. 2022;34(3):176–206. doi:10.21147/j.issn.1000-9604.2022.03.03
20. Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer Am Cancer Soc. 2000;89(7):1634–1646. doi:10.1002/1097-0142(20001001)89:7<1634::aid-cncr29>3.0.co;2-v
21. Mendoza TR, Wang XS, Lu C, et al. Measuring the symptom burden of lung cancer: the validity and utility of the lung cancer module of the M. D. Anderson symptom inventory. Oncologist. 2011;16(2):217–227. doi:10.1634/theoncologist.2010-0193
22. Zhang LL, Zang Y. Revision and evaluation of lung cancer module of MD Anderson symptom inventory. Cancer. 2013;33(05):434–438. doi:10.3781/j.issn.1000-7431.2013.05.009
23. Harris CS, Kober KM, Conley YP, et al. Symptom clusters in patients receiving chemotherapy: a systematic review. BMJ Support Palliat. 2021;12(1):10–21. doi:10.1136/bmjspcare-2021-003325
24. Ma J, Xu H, Liu S, et al. An investigation of symptom clusters and sentinel symptoms during the first 2 cycles of postoperative chemotherapy in patients with lung cancer. Cancer Nurs. 2022;45(6):488–496. doi:10.1097/NCC.0000000000001058
25. Wei L, Lv F, Luo C, et al. Study on sentinel symptoms and influencing factors of postoperative chemotherapy in patients with gastric cancer. Eur J Oncol Nurs. 2023;64:64102318. doi:10.1016/j.ejon.2023.102318
26. Li JJ, Li JR, Wu JM, et al. Change in symptom clusters perioperatively in patients with lung cancer. Eur J Oncol Nurs. 2021;55(102046):102046. doi:10.1016/j.ejon.2021.102046
27. Lv XQ, Wang BQ, Tong HH, et al. Predictive model of psychological distress in patients with lung cancer: a cross-sectional study. Cancer Nurs. 2022;45(1):E59–E67. doi:10.1097/NCC.0000000000000837
28. Tian X, Li H, Li F, et al. Development and validation of a web-based calculator for determining the risk of psychological distress based on machine learning algorithms: a cross-sectional study of 342 lung cancer patients. Support Care Cancer. 2024;33(1):63. doi:10.1007/s00520-024-09127-5
29. Rose S, Boyes A, Kelly B, et al. Lung cancer stigma is a predictor for psychological distress: a longitudinal study. Lung cancer stigma is a predictor for psychological distress. Psycho-Oncology. 2021;30(7):1137–1144. doi:10.1002/pon.5665
30. Fang M, Hu W, Xie Z. Dyadic effects of social support on psychological distress in patients with advanced lung cancer and spousal caregivers: the mediating role of sense of coherence. Geriatr Nurs. 2024;60:686–692. doi:10.1016/j.gerinurse.2024.09.006
31. Muruganandan S, Mishra E, Singh B. Breathlessness with pleural effusion: what do we know? Semin Resp Crit Care. 2023;44(4):502–508. doi:10.1055/s-0043-1769098
32. Shin J, Kober KM, Wong ML, et al. Distinct shortness of breath profiles in oncology outpatients undergoing chemotherapy. J Pain Symptom Manag. 2022;65(3):242–255. doi:10.1016/j.jpainsymman.2022.11.010
33. Baskar R, Lee KA, Yeo R, et al. Cancer and radiation therapy: current advances and future directions. Int J Med Sci. 2012;9(3):193–199. doi:10.7150/ijms.3635
34. Lu X, Wang J, Zhang T, et al. Comprehensive pneumonitis profile of thoracic radiotherapy followed by immune checkpoint inhibitor and risk factors for radiation recall pneumonitis in lung cancer. Front Immunol. 2022;13:918787. doi:10.3389/fimmu.2022.918787
35. Jia W, Guo H, Jing W, et al. An especially high rate of radiation pneumonitis observed in patients treated with thoracic radiotherapy and simultaneous osimertinib. Radiother Oncol. 2020;152:96–100. doi:10.1016/j.radonc.2020.07.051
36. Snijders RAH, Brom L, Theunissen M, et al. Update on prevalence of pain in patients with cancer 2022: a systematic literature review and meta-analysis. Cancers. 2023;15(3). doi:10.3390/cancers15030591
37. Temiz G, Cankaya G, Ozturk A, et al. Acute side effects and health care requirements in breast cancer patients treated with radiotherapy. Saudi Med J. 2024;45(2):199–204. doi:10.15537/smj.2024.45.2.20230438
38. Petri S, Berthelsen CB. Lived experiences of everyday life during curative radiotherapy in patients with non-small-cell lung cancer: a phenomenological study. Int J Qual Stud Heal. 2015;10(29397). doi:10.3402/qhw.v10.29397
39. Soni PD, Boonstra PS, Schipper MJ, et al. Lower incidence of esophagitis in the elderly undergoing definitive radiation therapy for lung cancer. J Thorac Oncol. 2017;12(3):539–546. doi:10.1016/j.jtho.2016.11.2227
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Albumin-Modified Gold Nanoparticles as Novel Radiosensitizers for Enhancing Lung Cancer Radiotherapy
Chen Y, Liu S, Liao Y, Yang H, Chen Z, Hu Y, Fu S, Wu J
International Journal of Nanomedicine 2023, 18:1949-1964
Published Date: 11 April 2023
Perioperative Symptom Trajectories and a Risk Prediction Model for Cervical Cancer: A Prospective Longitudinal Study
Zhang Y, Wu Y, Wang Y, Yang J, Chen L, Xu C
International Journal of Women's Health 2026, 18:613006
Published Date: 16 June 2026
Symptom Clusters and Sentinel Symptoms in Heart Failure Patients: A Cross-Sectional Survey
Li Y, Xu M, Jia W, Ma J, Guo S, Yao L
International Journal of General Medicine 2026, 19:607704
Published Date: 23 June 2026