Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Successful Treatment with Secukinumab in a Psoriasis Patient on Hemodialysis
Received 25 April 2025
Accepted for publication 18 July 2025
Published 23 July 2025 Volume 2025:15 Pages 321—325
DOI https://doi.org/10.2147/PTT.S536639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tina Bhutani
Yu Xiao,1– 3 Jingru Sun1– 3
1Department of Dermatology and Venereology, Peking University First Hospital, Beijing, 100034, People’s Republic of China; 2National Clinical Research Center for Skin and Immune Diseases, Beijing, 100034, People’s Republic of China; 3NMPA Key Laboratory for Quality Control and Evaluation of Cosmetics, Beijing, 100034, People’s Republic of China
Correspondence: Jingru Sun, Department of Dermatology and Venereology, Peking University First Hospital, No. 8 Xishiku Street, Xicheng District, Beijing, 100034, People’s Republic of China, Tel +86-10-83573273, Fax +86-10-66551216, Email [email protected]
Abstract: Moderate to severe psoriasis has been reported as an independent risk factor for IgA nephropathy (IgAN). IgAN is characterized by episodic microscopic hematuria, which can progress to end-stage renal disease (ESRD). Managing therapeutic interventions for psoriasis patients requiring dialysis due to ESRD presents significant challenges. We present a case of severe plaque psoriasis in a patient concurrently diagnosed with IgAN who is dependent on hemodialysis. Over the past two months, his condition has worsened without any identifiable triggers. Physical examination revealed generalized scaly plaques on the scalp, trunk, and extremities, resulting in a Psoriasis Area Severity Index (PASI) score of 19.2. Laboratory tests confirmed end-stage renal insufficiency, with no other abnormalities detected. Consequently, the patient was prescribed subcutaneous secukinumab following a standard regimen. He achieved complete resolution of symptoms after eight weeks of treatment and experienced no recurrence during a one-year follow-up. His kidney-related parameters remained stable during secukinumab therapy. To summarize, this case report discusses a patient with severe psoriasis who also has concurrent IgAN and ESRD, successfully treated with secukinumab. It reinforces the rapid efficacy and enduring safety of secukinumab in managing psoriasis in hemodialysis-dependent patients with IgAN comorbidity. Zeno Fratton et al has reported that an interleukin (IL)-17A/F inhibitor effectively treats moderate-to-severe psoriasis in patients with chronic kidney disease (CKD). However, further studies are necessary to develop evidence-based guidelines for biologic selection within this vulnerable population.
Keywords: psoriasis, IgA nephropathy, end-stage renal disease, hemodialysis, secukinumab
Introduction
Psoriasis is a chronic immune-mediated inflammatory disorder characterized by recurrent erythematous plaques. It is also associated with various multiorgan comorbidities, including cardiovascular disorders, gastrointestinal pathologies, and metabolic diseases.1,2 Recent studies have identified severe psoriasis as an independent risk factor for chronic kidney disease (CKD) and end-stage renal disease (ESRD).3,4 The management of psoriasis in patients with impaired renal function presents special challenges due to the nephrotoxic potential of certain treatments and the need for dose adjustments. Although several biologic agents have emerged as viable treatment options for these patients, there is limited real-world evidence regarding the clinical utility of interleukin-17 (IL-17) inhibitors in individuals with CKD or ESRD.5 The efficacy and safety of standard dosing of IL-17 inhibitors in psoriasis patients with concurrent CKD or ESRD require further investigation. Here, we present a case of severe plaque psoriasis concurrently associated with IgA nephropathy (IgAN), successfully managed with secukinumab during maintenance hemodialysis, demonstrating sustained efficacy and an acceptable safety profile over a 12-month follow-up period.
Case Report
A 48-year-old male with a two-decade history of plaque psoriasis was referred to our hospital due to disease exacerbation over the past two months, with no obvious triggers. His medical history included a diagnosis of IgAN at age 33, which progressed to ESRD, necessitating thrice-weekly hemodialysis for the past seven years. The patient reported no pain or swelling in any joints. Physical examination revealed generalized scaly plaques on the scalp, trunk, and extremities (Figure 1A–D), with a Psoriasis Area and Severity Index (PASI) score of 19.2. Laboratory results confirmed end-stage renal insufficiency: serum creatinine of 1182.50 μmol/L (equivalent to 13.36 mg/dL; reference range: 44–133), an estimated Glomerular Filtration Rate (eGFR) of 5.35 mL/min/1.73m², and blood urea nitrogen of 24.35 mmol/L (reference: 1.8–7.1). Complete blood cell counts, liver function tests, and infectious disease screenings (including hepatitis B/C serology, HIV testing, and tuberculosis interferon-gamma release assay) were unremarkable.
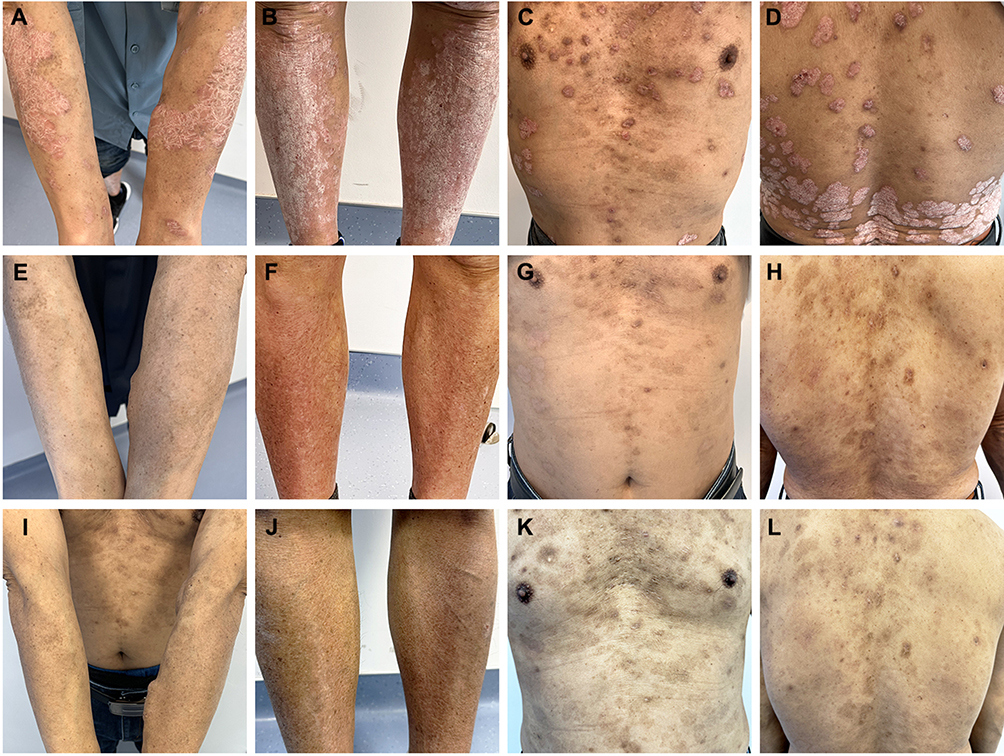 |
Figure 1 (A–D) Clinical presentation of the patient before treatment; (E–H) Image of the patient 8 weeks after initial treatment with secukinumab; (I–L) Photograph of the patient 12 months after secukinumab treatment. |
Following a multidisciplinary consultation, subcutaneous secukinumab was administered according to a standard regimen (300 mg once weekly for weeks 0–4, followed by 300 mg every four weeks). Complete resolution (PASI-100 response) was achieved at week 8 (Figure 1E–H), with sustained PASI 0 during the one-year follow-up (Figure 1I–L). Serial assessments of renal function revealed stable parameters, including a serum creatinine level of 1304 μmol/L (equivalent to 14.74 mg/dL), an eGFR of 5.34 mL/min/1.73 m², and a blood urea nitrogen level of 23.85 mmol/L. These findings are consistent with the patient’s baseline hemodialysis-dependent status. No treatment-related adverse events, including infections, were documented.
Discussion
Recent studies have indicated that a significant number of individuals diagnosed with psoriasis also have secondary IgAN. Emerging evidence suggests that moderate to severe psoriasis may be an independent risk factor for IgAN.6 IgAN is characterized by the accumulation of IgA in the glomerular mesangium, which is manifested by episodic proteinuria and hematuria.6 The mechanisms underlying the association between psoriasis and IgAN remain unclear. One hypothesis posits that IL-17, a key cytokine of psoriasis, stimulates B-cell activation and results in aberrant glycosylation of IgA1. This process may lead to glomerular immune complex deposition in IgAN.7 The pathophysiological overlap between psoriasis and IgAN provides a rationale for IL-17 inhibition in psoriasis patients with comorbid IgAN. Furthermore, previous studies have documented the successful use of IL-17 inhibitors in treating psoriatic patients with IgAN, leading to improvements in both psoriasis and IgAN.7,8 These cases offer valuable insights for developing future treatment strategies for this population.
Although IgAN can progress to CKD and ESRD, other conditions such as nephrotic syndrome, diabetic nephropathy, atherosclerosis, and hypertension may also contribute to CKD and ESRD in psoriasis patients with comorbidities.4 Managing psoriasis in patients with ESRD who require dialysis is particularly challenging, as appropriate psoriasis treatments must be selected carefully. While acitretin has been reported to be effective and safe in these patients, the improvement of skin lesions is limited, and monitoring of alkaline phosphatase and bilirubin levels is necessary.9 Consequently, alternative therapies are warranted for these individuals. Given that several case reports have documented the successful and safe use of biologic therapy for patients on hemodialysis, we selected secukinumab for our patient.10,11 Secukinumab, a fully human IgG1-κ monoclonal antibody targeting interleukin-17A (IL-17A), is particularly promising because it is not removed by hemodialysis and its metabolism is unaffected by renal function.
We summarized the clinical information and outcomes of previous reports concerning psoriasis patients undergoing hemodialysis who received biological therapy, as presented in Table 1.10–22 TNF-α inhibitors typically require a duration of 8–24 weeks to achieve PASI-100 response in hemodialysis patients.14 Moreover, IL-12/23 blockade (ustekinumab) demonstrates PASI-90 or PASI-100 response by week 16.15,21 Although limited case reports show complete clearance of skin lesions at week 4, a retrospective study in plaque‐type psoriasis with CKD reports that about 50% patients achieved PASI-100 response at week 16 after treatment with bimekizumab, an interleukin (IL)-17A/F inhibitor.5,20,22 Additionally, ixekizumab, another IL-17 inhibitor, has achieved complete clearance within 1 to 3 months.17,19 According to previous case reports, secukinumab can achieve a PASI-100 clearance as early as 8 weeks.16,18 Our case establishes secukinumab’s superior efficacy in terms of rapidity, suggesting a class-specific therapeutic advantage. Although no serious infections or other adverse events were noted in these patients, routine monitoring remains essential due to their immunocompromised status.
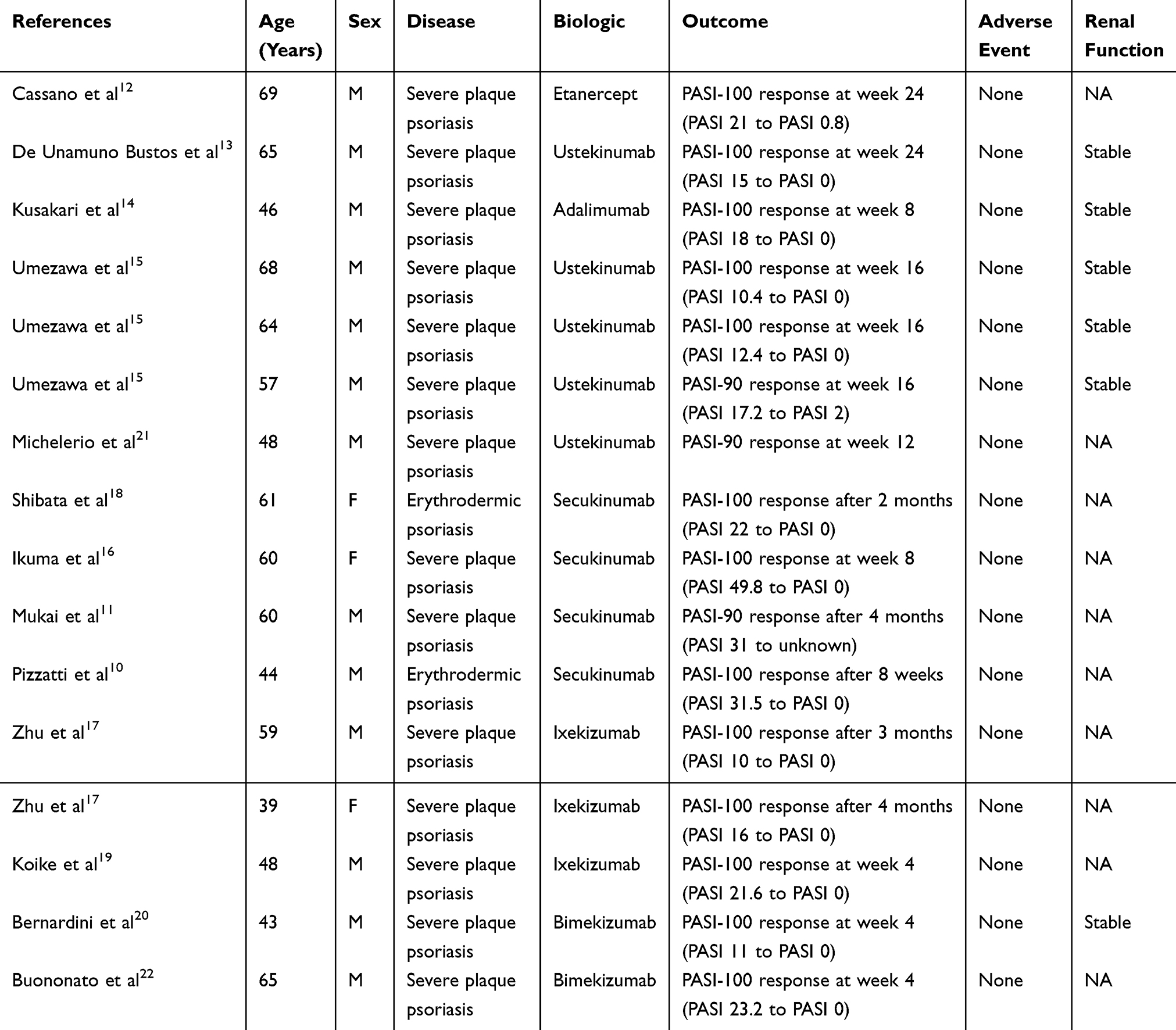 |
Table 1 Reported Cases with Biologic Therapy in Psoriatic Patients Undergoing Hemodialysis |
In conclusion, this case substantiates the rapid efficacy and durable safety of secukinumab in managing psoriasis for hemodialysis-dependent patients with IgAN comorbidity. Prospective multicenter studies are warranted to establish evidence-based guidelines for biologic selection in this vulnerable population.
Abbreviations
CKD, chronic kidney disease; ESRD, end-stage renal disease; IgAN, IgA nephropathy; PASI, Psoriasis Area and Severity Index.
Ethical Statements
The patient has given consent to publish his case details and picture. No institutional approval was required to publish this case.
Disclosure
The authors declare no conflict of interest.
References
1. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
2. Bu J, Ding R, Zhou L, Chen X, Shen E. Epidemiology of psoriasis and comorbid diseases: a narrative review. Front Immunol. 2022;13:880201. doi:10.3389/fimmu.2022.880201
3. Conti A, Giovannini L, Mandel VD, et al. Chronic kidney disease in psoriasis: a cohort study. JDDG. 2020;18(5):438–445. doi:10.1111/ddg.14087
4. Lee E, Han JH, Bang CH, et al. Risk of end-stage renal disease in psoriatic patients: real-world data from a nationwide population-based cohort study. Sci Rep. 2019;9(1):16581. doi:10.1038/s41598-019-53017-4
5. Fratton Z, Balato A, Bighetti S, et al. Real-world experience using bimekizumab in a patient cohort with plaque-type psoriasis and chronic kidney disease: a 48-week retrospective multicentre study. Int J Dermatol. 2025;64(6):1095–1097. doi:10.1111/ijd.17657
6. Grewal SK, Wan J, Denburg MR, Shin DB, Takeshita J, Gelfand JM. The risk of IgA nephropathy and glomerular disease in patients with psoriasis: a population-based cohort study. Br J Dermatol. 2017;176(5):1366–1369. doi:10.1111/bjd.14961
7. Ochi M, Toyama T, Ando M, et al. A case of secondary IgA nephropathy accompanied by psoriasis treated with secukinumab. CEN Case Rep. 2019;8(3):200–204. doi:10.1007/s13730-019-00393-5
8. Kulaklı S, Akagün T. A case of psoriasis with IgA nephropathy successfully treated with secukinumab. Int J Dermatol. 2024;63(2):e35–e37. doi:10.1111/ijd.16903
9. Shim PJ, Quintos JL, Faraz K, et al. A report on the safety of Acitretin use in patients with renal failure on haemodialysis. Clin Exp Dermatol. 2024;49(9):1052–1055. doi:10.1093/ced/llae093
10. Pizzatti L, Mugheddu C, Sanna S, Atzori L, Rongioletti F. Erythrodermic psoriasis in a dialyzed patient successfully treated with Secukinumab. Dermatol Ther. 2020;33(3):e13348. doi:10.1111/dth.13348
11. Mukai M, Kurihara Y, Ito Y, et al. Successful treatment with secukinumab of three psoriatic patients undergoing dialysis. J Dermatol. 2020;47(1):e26–e28. doi:10.1111/1346-8138.15132
12. Cassano N, Vena GA. Etanercept treatment in a hemodialysis patient with severe cyclosporine-resistant psoriasis and hepatitis C virus infection. Int J Dermatol. 2008;47(9):980–981. doi:10.1111/j.1365-4632.2008.03619.x
13. de Unamuno Bustos B, Sánchez RB, Martínez VO, Carazo JL. Efficacy and safety of ustekinumab in a patient with chronic renal failure on hemodialysis. Int J Dermatol. 2014;53(4):e299–301. doi:10.1111/ijd.12163
14. Kusakari Y, Yamasaki K, Takahashi T, et al. Successful Adalimumab treatment of a psoriasis vulgaris patient with hemodialysis for renal failure: a case report and a review of the previous reports on biologic treatments for psoriasis patients with hemodialysis for renal failure. J Dermatol. 2015;42(7):727–730. doi:10.1111/1346-8138.12901
15. Umezawa Y, Hayashi M, Kikuchi S, et al. Ustekinumab treatment in patients with psoriasis undergoing hemodialysis. J Dermatol. 2015;42(7):731–734. doi:10.1111/1346-8138.12903
16. Ikuma D, Oguro M, Hoshino J, et al. Efficacy of Secukinumab for plaque psoriasis in a patient on hemodialysis. CEN Case Rep. 2020;9(1):55–58. doi:10.1007/s13730-019-00426-z
17. Zhu X, Pan X, Dong Z. Plaque psoriasis with renal dysfunction successfully treated with ixekizumab. Hemodial Int. 2025;29(1):126–129. doi:10.1111/hdi.13185
18. Shibata T, Muto J, Takama H, Yanagishita T, Ito T, Watanabe D. Case of psoriatic erythroderma induced by the discontinuation of the chronic use of topical steroid after dialysis initiation and successfully treated with secukinumab. J Dermatol. 2019;46(4):e119–e120. doi:10.1111/1346-8138.14649
19. Koike Y, Fujiki Y, Higuchi M, Fukuchi R, Kuwatsuka S, Murota H. An interleukin-17 inhibitor successfully treated a complicated psoriasis and psoriatic arthritis patient with hepatitis B virus infection and end-stage kidney disease on hemodialysis. JAAD Case Rep. 2019;5(2):150–152. doi:10.1016/j.jdcr.2018.11.016
20. Bernardini N, Ambrosio L, Tolino E, Proietti I, Skroza N, Potenza C. Successful treatment with Bimekizumab of a psoriatic patient undergoing hemodialysis: a case report and review of the literature. J Clin Med. 2024;13(8):2250. doi:10.3390/jcm13082250
21. Michelerio A, Ciolfi C, Rotatore G, Grosjean F, Brazzelli V. Successful ustekinumab treatment of severe refractory psoriasis vulgaris in a hemodialysis patient. Ital J Dermatol Venerol. 2021;156(4):510–511. doi:10.23736/S2784-8671.20.06789-9
22. Buononato D, Tancredi V, Di Brizzi EV, Argenziano G, Balato A. A case of severe psoriasis successfully treated with bimekizumab in a hemodialysis patient with end-stage renal disease. Ital J Dermatol Venerol. 2024;159(5):585–586. doi:10.23736/S2784-8671.24.07920-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiology of End-Stage Renal Disease in Mogadishu, Somalia: First Report at a Tertiary Care Hospital
Mohamed AH, Jeele MOO
International Journal of General Medicine 2022, 15:6259-6267
Published Date: 21 July 2022
Drug Survival Outcomes Associated with the Real-World Use of Ixekizumab, Secukinumab, Guselkumab, and Adalimumab for the Treatment of Plaque Psoriasis in China: A 52-Week Single-Center Retrospective Study
Li Y, Lu JJ, Zhong XY, Yu YY, Yu N, Wang Y, Yi XM, Ding YF, Shi YL
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2245-2252
Published Date: 20 October 2022
Interleukin-17A Inhibitor Secukinumab Treatment in HIV-Positive Psoriasis Patient: A Case Report
Gong J, Wu W, Qiu L, Wang X, Bao J, Wang J, Cheng L, Fu Z, Hu F
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2949-2956
Published Date: 30 December 2022
Prevention of Intradialytic Hypotension in Hemodialysis Patients: Current Challenges and Future Prospects
Hamrahian SM, Vilayet S, Herberth J, Fülöp T
International Journal of Nephrology and Renovascular Disease 2023, 16:173-181
Published Date: 1 August 2023
Prevalence of Depression and Its Associated Factors Among Hemodialysis Patients in Hodeida City, Yemen
Alkubati SA, Al-Sayaghi KM, Salameh B, Halboup AM, Ahmed WAM, J. Alkuwaisi M, Zoromba MA
Journal of Multidisciplinary Healthcare 2024, 17:689-699
Published Date: 13 February 2024