Back to Journals » International Journal of Women's Health » Volume 17
Study on Bone Mineral Density Around the Knee in Postmenopausal Women with Osteoarthritis and Osteoporosis
Authors Guo Z, Mao X, Wang Z, Lu Y, Song F, Chen S ![]() , Di J, Yan Z, Tian Z, Xiang C
, Di J, Yan Z, Tian Z, Xiang C ![]()
Received 1 July 2025
Accepted for publication 25 November 2025
Published 3 December 2025 Volume 2025:17 Pages 5087—5103
DOI https://doi.org/10.2147/IJWH.S550710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Zijian Guo,1,* Xingjia Mao,2,* Zehua Wang,3,* Yao Lu,4 Feipeng Song,4 Shuai Chen,1 Jingkai Di,1 Zehui Yan,1 Zui Tian,1 Chuan Xiang1
1Department of Orthopedic, The Second Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China; 2Department of Basic Medicine Sciences, Zhejiang University School of Medicine, Hangzhou, 310058, People’s Republic of China; 3Department of Orthopaedic Surgery, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China; 4Department of Radiology, The Second Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuan Xiang, Department of orthopedic, The Second Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China, Tel +86-15503637653, Email [email protected]
Background: Osteoporosis (OP) and knee osteoarthritis (KOA) are common comorbidities in postmenopausal women, yet the relationship between OP and localized bone mineral density (BMD) around the knee remains unclear. This study investigated the effect of concomitant OP on periarticular BMD and its associations with the Western Ontario and McMaster University Osteoarthritis Index (WOMAC), radiographic severity, and hip-knee-ankle (HKA) angle in postmenopausal women with KOA.
Methods: In this cross-sectional study, 117 postmenopausal women were classified into a KOA combined with OP group (n=59) and a KOA-only group (n=58) based on dual-energy X-ray absorptiometry (DXA) T-scores. All participants underwent dual-energy computed tomography (DECT) to quantify BMD around the distal femur, proximal tibia, and patella; weight-bearing radiographs to assess Kellgren-Lawrence (K&L) grade and HKA angle; and the WOMAC questionnaire to evaluate pain and joint function.
Results: Patients with KOA combined with OP demonstrated significantly lower knee BMD than those with KOA alone (P < 0.001). This reduction in BMD was more pronounced with increasing OP severity. Notably, even after adjusting for pain levels, BMD remained significantly lower in the KOA combined with OP group (P < 0.05). Furthermore, medial knee BMD in the KOA combined with OP group exhibited an inverted U-shaped relationship with K&L grade, peaking at grade III before declining. In contrast, BMD increased progressively with K&L grade in the KOA group. A significant inverse correlation was also observed between the HKA angle and medial knee BMD in the KOA combined with OP group, suggesting greater bone loss with increasing valgus deformity.
Conclusion: Postmenopausal women with KOA combined with OP have markedly lower periarticular BMD, associated with more severe pain, distinctive radiographic changes, and poorer alignment. These findings highlight the need for active bone preservation and OP management in KOA patients to alleviate symptoms and potentially slow disease progression.
Keywords: bone mineral density, osteoarthritis, osteoporosis, dual-energy computed tomography, subchondral bone
Introduction
Osteoarthritis (OA) and osteoporosis (OP) are two highly prevalent musculoskeletal disorders that disproportionately affect postmenopausal women, contributing significantly to pain, functional disability, and diminished quality of life in this population.1–3 While knee OA (KOA) is characterized by progressive cartilage degradation, osteophyte formation, and subchondral bone sclerosis, OP is defined by systemic reduction in bone mass and deterioration of bone microarchitecture, leading to increased fragility fracture risk.4,5
Historically, OA and OP were considered mutually exclusive due to their opposing pathological features—increased bone formation in OA versus bone loss in OP.6,7 However, a growing body of epidemiological evidence indicates a notable coexistence of KOA and OP in postmenopausal women, suggesting a more complex, bidirectional relationship than previously recognized.8–10 This paradox may be explained by several mechanisms: pain-induced disuse from advanced KOA can accelerate bone loss, precipitating or exacerbating OP.11–13 Research indicates OP-related bone mass reduction, microstructural deterioration, and turnover imbalance may accelerate articular cartilage degeneration in KOA through mechanisms including: weakened subchondral bone biomechanical support, altered stress distribution, exacerbated abnormal remodeling, and pro-inflammatory microenvironments.14,15 Concurrently, KOA progression features pathological bone changes (eg, subchondral sclerosis, microfractures) that further disrupt local bone metabolism.16,17 Moreover, OP significantly complicates total knee arthroplasty (TKA) in KOA patients by compromising prosthesis fixation, increasing perioperative fracture risk, and impeding functional recovery.18–20 Animal studies confirm that coexisting OP and KOA synergistically accelerate joint destruction.21 Collectively, these findings indicate OP substantially influences KOA pathological progression, particularly in periarticular bone tissue.
Local bone mineral density (BMD) around knee—specifically in the distal femur (DF), proximal tibia (PT), and patella—correlates more sensitively and specifically with KOA disease stage, severity, and early subchondral pathological changes than axial BMD measurements (eg, spine or hip).22,23 Consequently, precise periarticular BMD assessment is crucial for understanding KOA pathophysiology and complications. However, dual-energy X-ray absorptiometry (DXA), the gold standard for bone density evaluation, faces limitations when assessing complex anatomical structures like the knee, including superimposition artifacts, positioning challenges, and inability to differentiate cortical from trabecular bone. Dual-energy computed tomography (DECT) addresses these limitations by utilizing X-rays at two distinct energy levels. Through material decomposition techniques (eg, calcium/water or calcium/fat basis pairs), DECT enables accurate quantification of bone mineral content and BMD in specific regions—including complex knee structures—while effectively distinguishing cortical and trabecular bone.24,25
Despite this potential, current literature lacks comprehensive studies that utilize advanced imaging like DECT to directly compare BMD around knee in postmenopausal women with isolated KOA versus those with KOA combined with OP. Key questions remain unanswered: How does concomitant OP alter the localized BMD distribution around the knee in KOA? How are these alterations associated with clinical symptoms (eg, pain), radiographic severity (eg, Kellgren-Lawrence [K&L] grade), and mechanical alignment (eg, hip-knee-ankle [HKA] angle)? Based on this, the present study aims to apply DECT to quantitatively assess and compare BMD in key periarticular regions of the knee in postmenopausal women with KOA alone versus those with KOA combined with OP. Investigate the relationships between periarticular BMD and clinical pain severity, radiographic OA severity, and lower limb alignment. By providing direct, precise imaging evidence of the pathological interactions between OP and KOA, this study seeks to enhance the understanding of their coexistence. Our findings are expected to offer an important objective basis for the early identification of high-risk patients, inform optimized treatment strategies (including the potential role of OP management in slowing KOA progression), and improve preoperative planning for TKA in this complex patient population.
Methods
Study Participants and Inclusion/Exclusion Criteria
This study initially identified 159 postmenopausal women with KOA who presented at Second Hospital of Shanxi Medical University between December 2021 and August 2025. The inclusion criteria were: 1) postmenopausal women aged≥50 years; 2) a diagnosis of KOA meeting the American College of Rheumatology (ACR) clinical and radiographic criteria (K&L grade≥I); 3) for the OP group, a DXA-confirmed diagnosis of OP according to WHO criteria (T-score≤-2.5); and 4) provision of voluntary informed consent and the ability to complete all study assessments, including imaging and questionnaires.
Exclusion criteria comprised: 1) secondary OP (eg, due to hyperparathyroidism, long-term glucocorticoid use, or thyroid dysfunction); 2) secondary OA (eg, post-traumatic, rheumatoid arthritis, or infectious arthritis); 3) other systemic diseases known to severely affect bone metabolism (eg, chronic kidney disease, malignancy, or severe liver disease); 4) a history of knee surgery or intra-articular injections within the past six months; 5) contraindications for or inability to complete DECT scanning, including metallic implants or motion artefacts resulting in suboptimal image quality; 6) concurrent conditions affecting lower limb alignment (eg, severe hip or ankle deformity or neurological disorders); and 7) recent treatment (within one year) with any anti-OP medication (eg, bisphosphonates, SERMs, or teriparatide).
Based on these criteria, 42 patients were excluded. Specific reasons for exclusion included: hyperparathyroidism (n=2), long-term glucocorticoid therapy (n=3), rheumatoid arthritis (n=5), severe chronic kidney disease or cirrhosis (n=6), prior knee arthroscopy (n=7), recent intra-articular injections (n=3), poor DECT image quality (n=6), femoral head necrosis (n=4), congenital hip dysplasia (n=2), and recent anti-OP therapy (n=4). Consequently, 117 patients were ultimately enrolled in the study (Figure 1).
 |
Figure 1 Flow chart of study inclusion and exclusion of patients. |
A post-hoc power analysis was conducted using G*Power software (version 3.1.9.7) to evaluate the statistical power of our study for detecting differences in the primary outcome—BMD around knee. Based on the observed effect size (Cohen’s d = 0.85) for the difference in medial distal femoral BMD between the KOA combined with OP and KOA groups, with a sample size of 117 (n1=59, n2=58), an alpha level of 0.05, and a two-tailed test, the achieved statistical power was calculated to be 0.98. This exceeds the conventional threshold of 0.80, indicating that the final sample size was sufficient to identify statistically significant differences in the primary outcome measure between the two groups.
Based on the World Health Organisation diagnostic criteria and the Chinese Practice Guidelines for OP Patients, patients were grouped and degrees of OP were defined based on their DXA results’ T-score.26,27 T-score≥-1.0 indicates normal bone mass, −2.5<T-score<-1.0 denotes reduced bone mass, T-score≤-2.5 signifies OP, and T-score≤-2.5 with fragility fractures constitutes severe OP. In this study, T-scores were compared against data from white female subjects. Patients all voluntarily signed the informed consent form. This study were approved by the Clinical Research Ethics Committee of the Second Hospital of Shanxi Medical University (approval No.(2020)YXNO.131).
Demographic Data and Questionnaire Data
Demographic data (age, weight, height) were recorded for all patients and bone mass index (BMI) was calculated. Additionally, clinical data pertaining to alcohol and tobacco usage, as well as The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) were documented. WOMAC (version 3.1) comprises three scales: 1) pain severity during different postures or movements, 2) the severity of joint stiffness, and 3) difficulty in performing activities of daily living. Each item is scored using a visual analogue scale, and a total score is calculated to assess the severity of the patient’s OA and pain level. Higher scores are associated with more severe pain, worse quality of life, and poorer joint function. Mild < 80, moderate 80–120, severe > 120.
Radiographic Data
For each patient, standardized anteroposterior, lateral, and weight-bearing knee radiographs were obtained. Two specialized musculoskeletal radiologists independently assessed KOA severity using the K&L grading system. Discrepancies of one grade were resolved by accepting the higher-ranking radiologist’s assessment; differences exceeding one grade underwent third radiologist arbitration, with the final diagnosis determined by consensus with the third reviewer. Consequently, the inter-rater reliability among the three physicians was quantified using Fleiss’ kappa, yielding a value of 0.773 (p<0.001, 95% CI: 0.711–0.835), which indicates excellent agreement. Additionally, we measured the HKA angle from bilateral lower extremity full-length radiographs.
BMD Measurement
The patient’s medial and lateral DF BMD, medial and lateral PT BMD, and patella BMD were scanned using a Revolution CT instrument (GE Medical Systems, Waukesha, WI, USA). The reconstructed 1.25 mm thin-layer CT images after DECT scanning were transferred to an advanced workstation (ADW4.7; GE Medical Systems, Waukesha, WI, USA) using the “MD analysis” function in the Gemstone Spectral Imaging (GSI) viewer software (GE Healthcare, USA). The principle of this method is that the X-ray attenuation of each substance can be represented by two “base substances”, of which water and iodine are the two most commonly used base substances, and bone minerals are represented by hydroxyapatite; therefore, the quantitative determination of hydroxyapatite is key to the diagnosis of OP. DECT scan with hydroxyapatite-water as the substrate pair has good accuracy and high application value in the clinical diagnosis of OP.28 Therefore, in this study, MD images were obtained using HAP-water as the substrate pair, and hydroxyapatite-water values of knee were measured. Additionally, DXA and DECT were utilized to obtain BMD measurements at the ipsilateral femoral neck to evaluate the accuracy of DECT-based BMD assessment.
The patient will be measured in a supine position as well as in a comfortable lower extremity curvature, which will minimize artifacts and errors associated with swaying during the examination due to pain.29,30 We chose coronal images for data measurements and the measurement plane will be set at the center of the knee, where the intercondylar spine is located. The investigator will measure three consecutive images to reduce measurement errors. The data will also be collected independently by two specialized physicians, and if the error is greater than 20 (mg/cm3) then a third physician will perform the measurement and take the result with an error of less than 20 (mg/cm3) with the third physician and take the average of the two as the final measurement value (Figure 2).
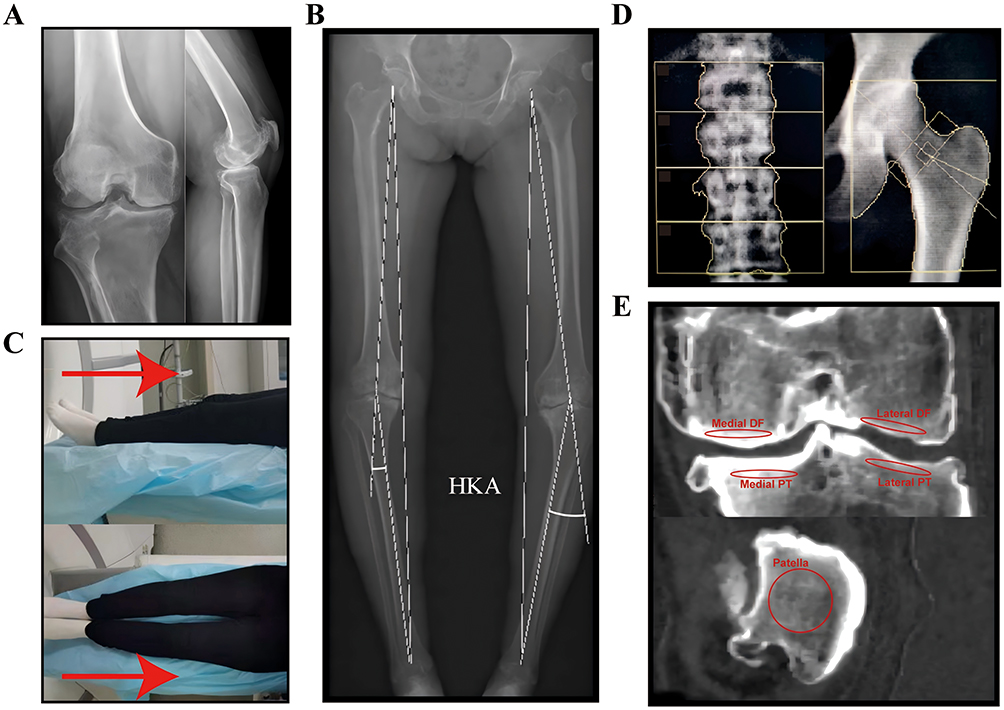 |
Figure 2 Schematic diagram of radiographic data acquisition for patients. (A) Frontal and lateral X-ray diagram of the knee. (B) Full-length diagram of the patient’s bilateral lower extremities and a schematic diagram of the HKA angle measurements. (C) Diagram of the patient’s position for DECT. The red arrow indicates the patient’s head position during the examination. (D) Lumbar spine and femoral neck BMD test chart. The yellow box represents the region of interest during DXA testing. (E) Schematic diagram of the patient’s BMD around knee measured by GSI View software. The red circle denotes the region of interest selected during measurement around the knee and the patella. Abbreviations: BMD, bone mineral density; HKA, hip-knee-ankle angle; DXA, dualenergy X-ray absorptiometry; DECT, dual-energy computed tomography; GSI, gemstone spectral imaging; DF, distal femur, PT, proximal tibia. |
Statistic Analysis
Categorical variables are expressed as percentages. Normally distributed continuous variables are reported as mean ± standard deviation (SD), while non-normally distributed continuous variables are presented as median and interquartile range (IQR). Normality was assessed using the Shapiro–Wilk test for sample sizes smaller than 50 and the Kolmogorov–Smirnov test for larger samples. For comparisons between two independent groups, independent samples t-tests were used for normally distributed data and Mann–Whitney U-tests for non-normally distributed data. Differences in categorical variables were assessed using chi-square tests. For comparisons across more than two independent groups with normally distributed data, one-way analysis of variance (ANOVA) was applied; if variances were equal, post-hoc LSD tests were used, otherwise, Tamhane’s T2 test was employed. All statistical analyses were performed using SPSS software version 26.0 (IBM, Armonk, NY, USA). We utilized Pearson’s correlation analysis to assess the relationship between the HKA and BMD around knee, reporting the strength of the association using the correlation coefficient (r). Graphical representations were created using GraphPad Prism version 8.0.1 for Windows (GraphPad Software, Boston, MA, USA; www.graphpad.com). A two-sided p-value of less than 0.05 was considered statistically significant for all tests.
Results
The DECT-Based Method Demonstrated Favorable Accuracy for Evaluating BMD
DECT and DXA were utilized to quantify BMD within an identical region of interest in the femoral neck. The results indicated a strong positive correlation between the two modalities (Pearson’s r = 0.920, P < 0.001), confirming that the DECT-based assessment provides an accurate reflection of BMD (Table 1).
 |
Table 1 Correlation Between DECT and DXA Measurements of Femoral Neck BMD |
Baseline Data on KOA Patients Combined with or without OP and BMD Around Knee
A total of 59 menopausal patients diagnosed with KOA and OP, and 58 menopausal patients diagnosed with KOA, were enrolled in this investigation. Table 2 contains the pertinent demographic and clinical information for the participant pool. There was no significant difference between the KOA combined with or without OP group in terms of age, height, weight, BMI, risk of AUDIT, and risk of smoking. And there was no significant difference between the two groups in terms of WOMAC grading and K&L grading (p>0.05).
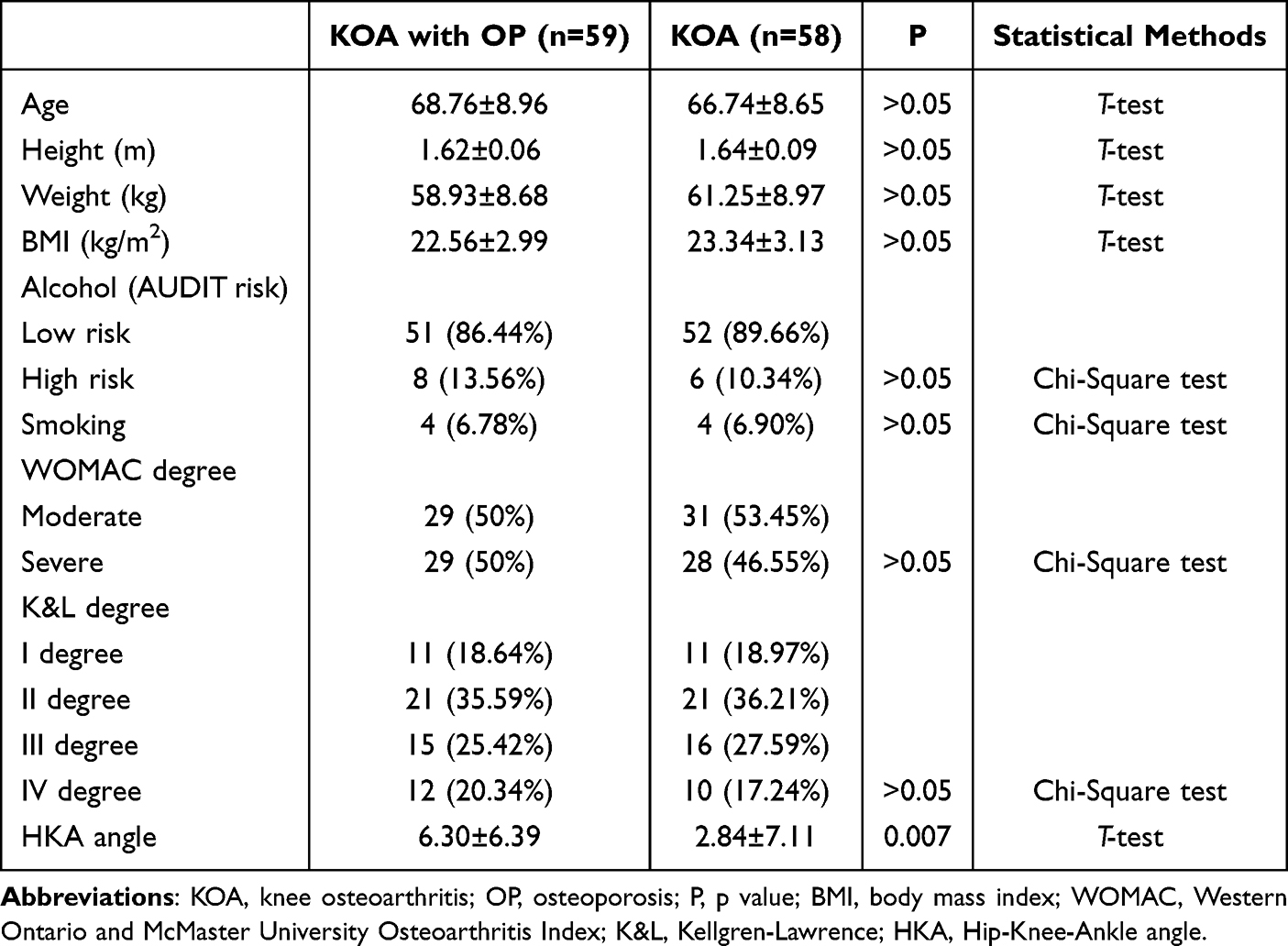 |
Table 2 Baseline Characteristics of Patients and Characteristics of OA and WOMAC Degree |
Table 3 presented the variations in BMD around knee of patients with KOA combined with or without OP. The results indicate that in KOA combined OP patients, the medial and lateral DF BMD, medial and lateral PT BMD, and the patellofemoral BMD were considerably lower than those in KOA patients (p<0.001). Conversely, the values of medial/lateral (M/L) PT BMD were significantly higher in KOA combined with OP patients compared to KOA patients (p<0.05). The higher M/L BMD ratio in the KOA combined with OP group, despite lower absolute BMD values, suggests that concomitant OP may exacerbate the mechanical-driven disparity in bone loss between compartments, further disturbing the load distribution and biomechanical environment of the knee. Furthermore, the HKA angle exhibited a statistically significant decrease in KOA combined with OP patients compared to KOA patients (p<0.01), indicating greater degrees of genu valgum in the former group.
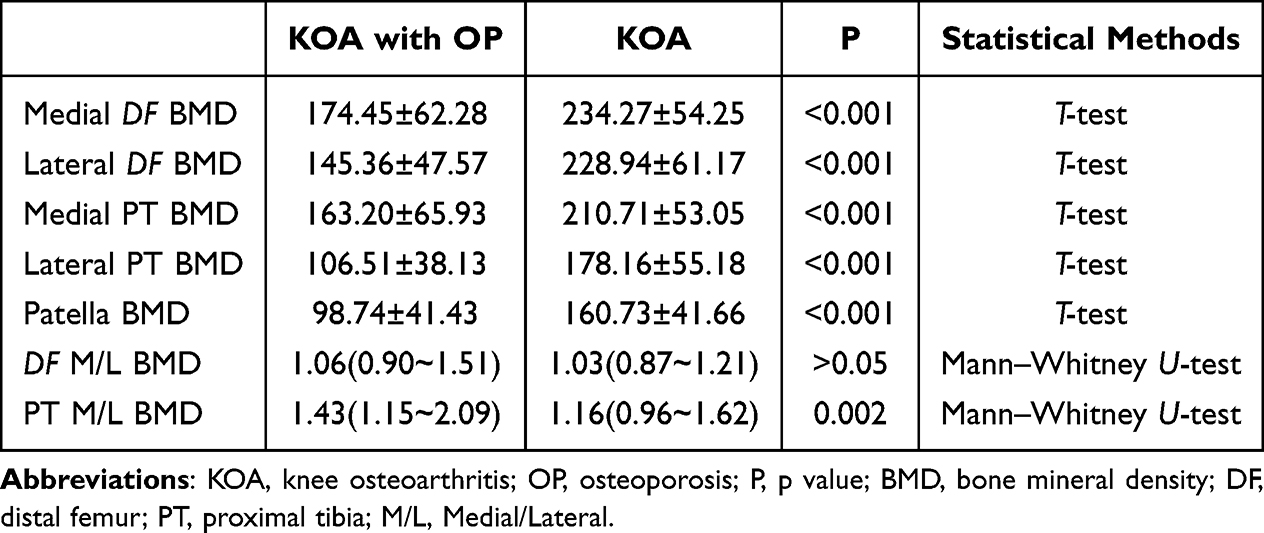 |
Table 3 BMD Around Knee in Patients with KOA Combined with or Without OP |
Relationship Between BMD Around Knee and OP
Patients were categorized into four categories based on their mid-axis bone BMD examination and T values: normal bone mass, reduced bone mass, OP, and severe OP. Overall, BMD around knee was inversely correlated with OP severity. The most pronounced reduction in BMD was observed in the OP group compared to the reduced bone mass and normal bone density groups. However, no significant difference was found between the OP and severe OP groups, a finding likely constrained by the limited sample size of severe OP patients in our cohort. (Figure 3).
 |
Figure 3 Histogram of BMD around knee with OP grade. (A) Histogram of BMD of the medial DF with OP grade. (B) Histogram of BMD of the lateral DF with OP grade. (C) Histogram of BMD of the medial PT with OP grade. (D) Histogram of BMD of the lateral PT with OP grade. (E) Histogram of BMD of the patella with OP grade. *p<0.05; **p<0.01; ***p<0.001. Abbreviations: OP, osteoporosis; BMD, bone mineral density; DF, distal femur; PT, proximal tibia; M/L, medial/Lateral. |
Relationship Between BMD Around Knee and WOMAC Degree
Tables 4 and 5 present the statistical results for BMD around knee across different WOMAC degree. In the severe patient group, there were notable dissimilarities in BMD around knee among KOA combined with or without OP patients. Additionally, PT M/L BMD was significantly greater in KOA combined with OP patients than in KOA patients (p<0.05). Similarly, a parallel occurrence was found in the moderate patient group, except for the absence of significant differences in DF and PT M/L BMD. There was no significant variation found in BMD around knee between the varying degrees of WOMAC degree in KOA patients with OP. However, among patients with KOA, the severe group demonstrated significantly higher BMD in the medial PT compared to the moderate group (p<0.05).
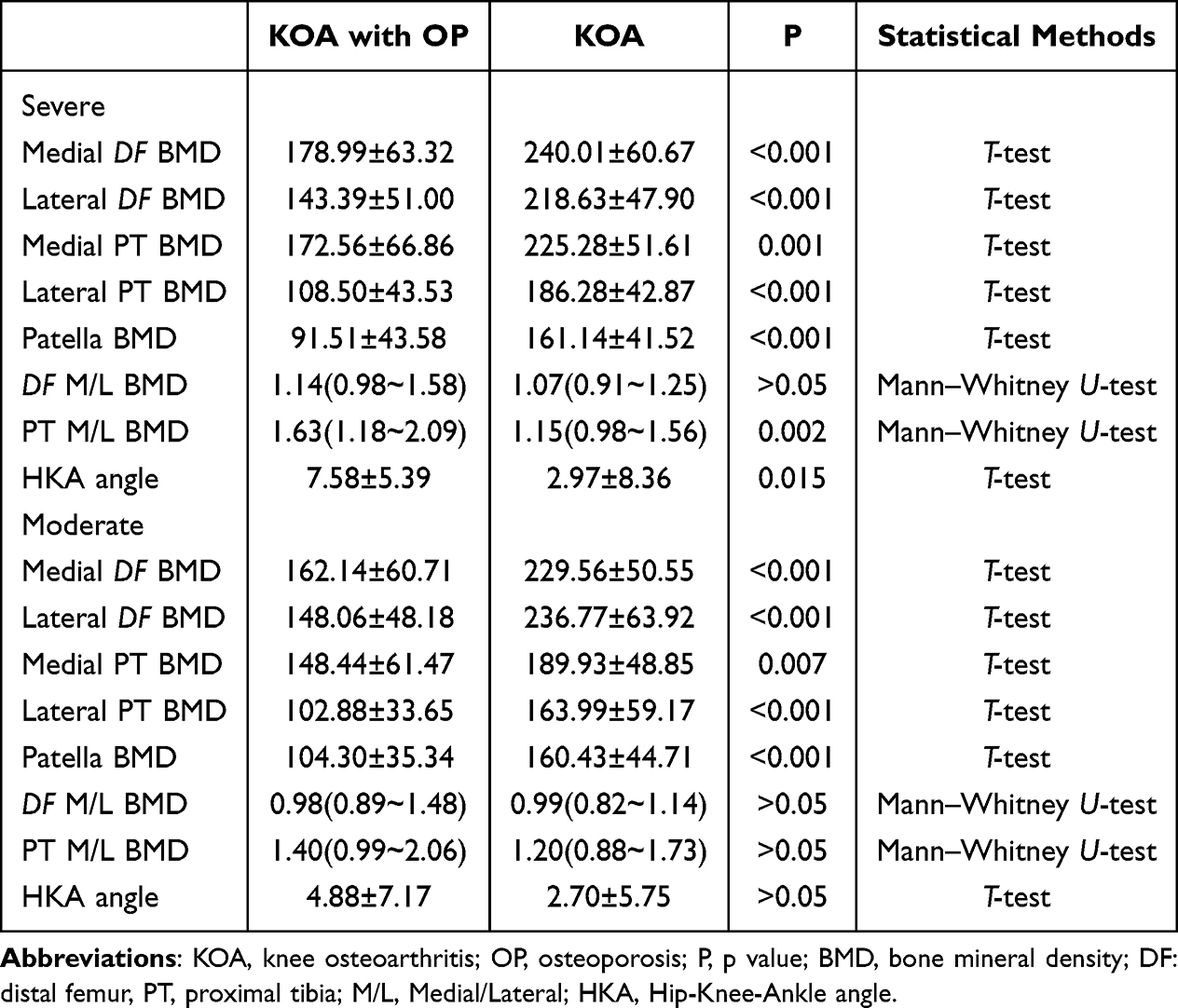 |
Table 4 BMD Around Knee Between the Two Groups with Different Degrees of WOMAC Index |
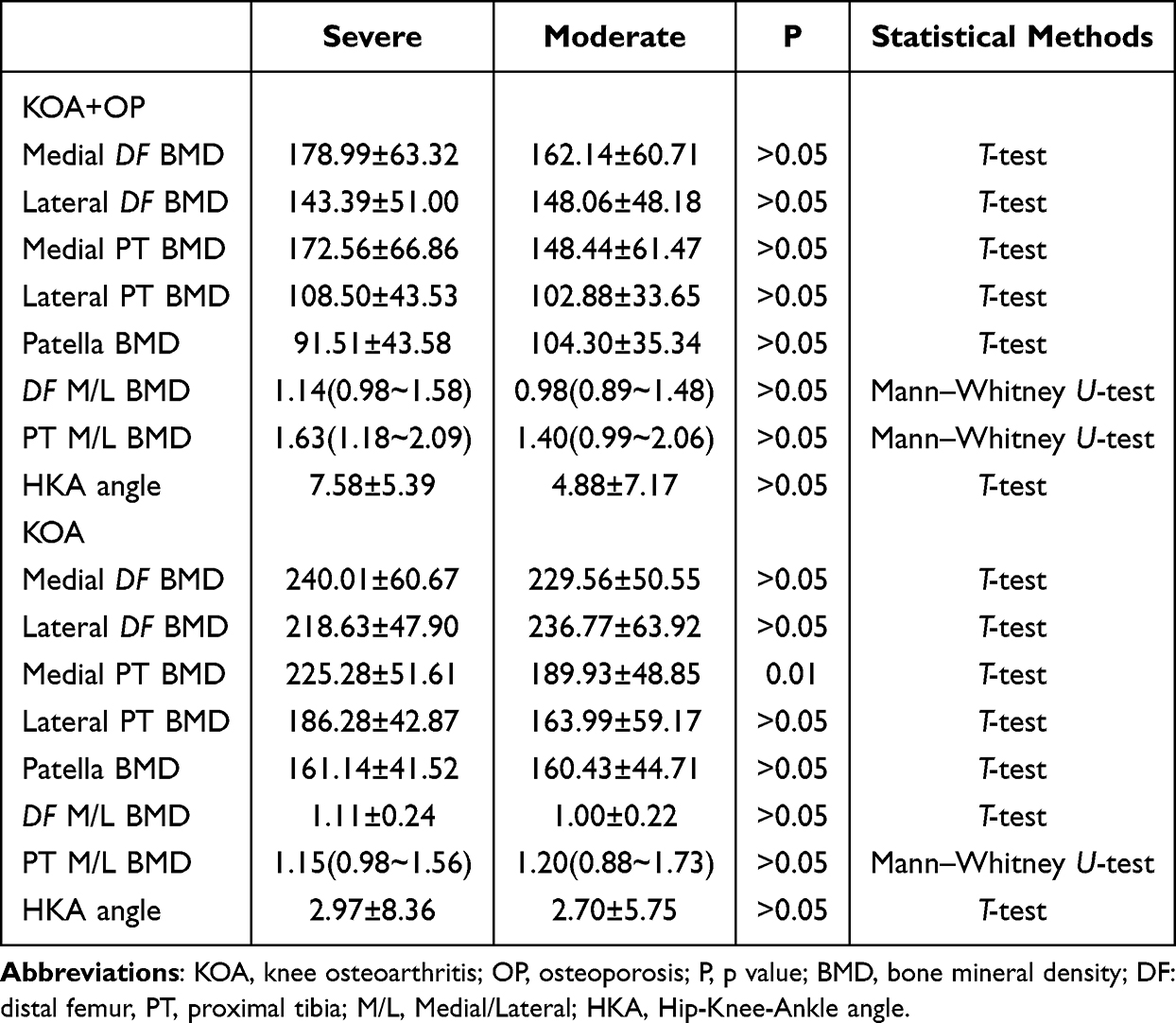 |
Table 5 BMD Around Knee in Patients with Different Degrees of WOMAC Index in the Two Groups |
Relationship Between BMD Around Knee and K&L Grading
K&L grading was devised to evaluate patients’ radiographic results objectively. As displayed in Table 6, patients with KOA combined with OP had notably lower BMD around knee than those with only KOA at K&L grades II and IV (P<0.05). Interestingly, at K&L grade I, significant differences in medial BMD were observed between the groups. Patients with KOA combined with OP exhibited significantly lower BMD in the medial DF and PT compared to those with KOA alone. Conversely, at K&L grade III, significant differences were noted in the lateral compartment, where BMD for the lateral DF, PT, and patella were significantly lower in the KOA with OP group than in the KOA group. In patients with KOA combined with OP, BMD around knee demonstrated an initial increase with advancing K&L grade, peaking at grade III, followed by a decline at grade IV. This inversely U-shaped pattern was most pronounced in the medial PT and was also evident in the lateral PT and DF. In contrast, the trend was less distinct in the medial DF and patella BMD. (Figures 4 and 5).
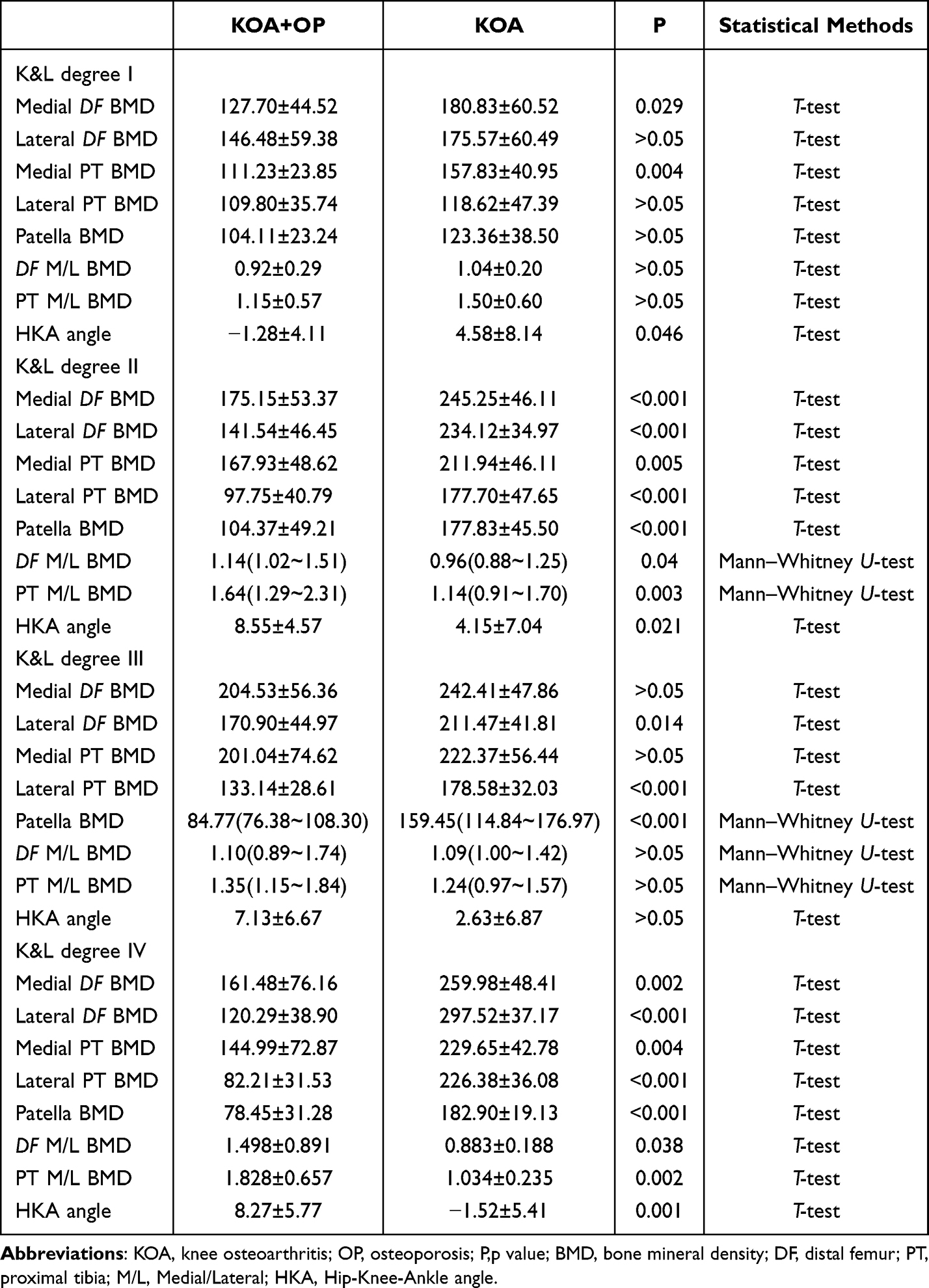 |
Table 6 BMD Around Knee in Two Groups of Patients with Different K&L Grades |
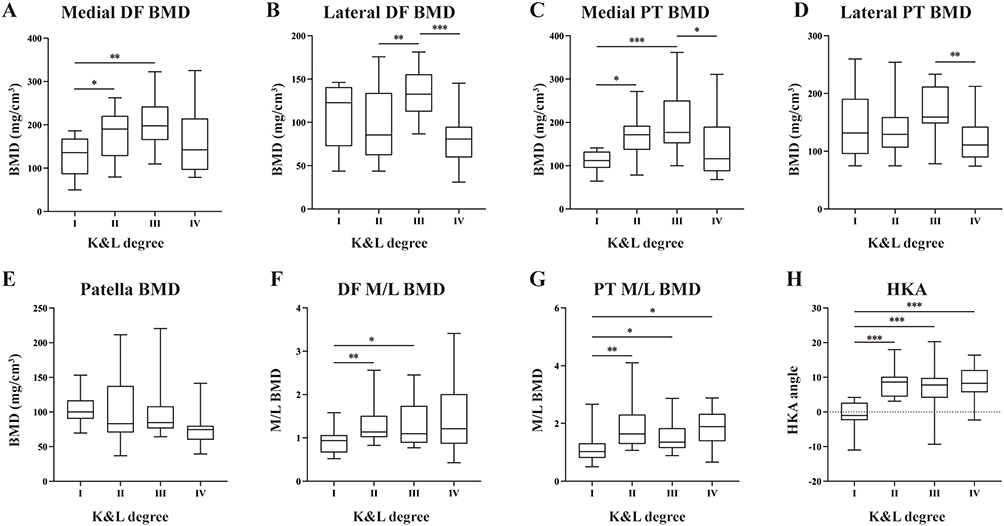 |
Figure 4 Statistical chart of the change in BMD around knee with K&L grade in patients with KOA combined with OP. (A) Histogram of BMD of the medial DF with K&L grade. (B) Histogram of BMD of the lateral DF with K&L grade. (C) Histogram of BMD of the medial PT with K&L grade. (D) Histogram of BMD of the lateral PT with K&L grade. (E) Histogram of BMD of the patella with K&L grade. (F) Histogram of medial/lateral BMD of the DF with K&L grade. (G) Histogram of medial/lateral BMD of the PT with K&L grade. (H) Histogram of HKA angle with K&L grade. *p<0.05;**p<0.01;***p<0.001. Abbreviations: KOA, knee osteoarthritis; OP, osteoporosis; BMD, bone mineral density; DF, distal femur; PT, proximal tibia; M/L, Medial/Lateral; HKA, Hip-Knee-Ankle angle. |
 |
Figure 5 Statistical chart of the change in BMD around knee with K&L grade in patients with KOA. (A) Histogram of BMD of the medial DF with K&L grade. (B) Histogram of BMD of the lateral DF with K&L grade. (C) Histogram of BMD of the medial PT with K&L grade. (D) Histogram of BMD of the lateral PT with K&L grade. (E) Histogram of BMD of the patella with K&L grade. (F) Histogram of medial/lateral BMD of the DF with K&L grade. (G) Histogram of medial/lateral BMD of the PT with K&L grade. (H) Histogram of HKA angle with K&L grade. *p<0.05;**p<0.01;***p<0.001. Abbreviations: KOA, knee osteoarthritis; BMD, bone mineral density; DF, distal femur; PT, proximal tibia; M/L, Medial/Lateral; HKA, Hip-Knee-Ankle angle. |
Relationship Between BMD Around Knee and HKA Angle
With increasing HKA angle, there was a significant correlation between medial DF BMD (r=0.491, P<0.001) and medial PT BMD (r=0.426, P<0.001) in patients with KOA combined with OP. In patients with KOA combined with OP, medial knee BMD demonstrates an positive correlation with the HKA angle. At the same time, a statistically significant trend was observed between DF (r=0.464, P<0.001) and PT (r=0.436, P<0.001) M/L BMD and HKA (Figure 6). On the contrary, patients with KOA exhibited opposing BMD trends around knee. Lateral DF BMD (r=−0.380, P<0.01), lateral PT BMD (r=−0.281, P<0.05) and patella BMD (r=−0.304, P<0.05) all decreased with the HKA angle increasing. Conversely, PT M/L BMD decreased as the HKA angle increased in KOA group (r=0.338, P<0.05) (Figure 7).
 |
Figure 6 Scatter plot of BMD around knee with HKA angle in patients with KOA combined with OP. (A) Scatter plot of BMD of the mineral DF with HKA angle. (B) Scatter plot of BMD of the lateral DF with HKA angle. (C) Scatter plot of BMD of the medial PT with HKA angle. (D) Scatter plot of BMD of the lateral PT with HKA angle. (E) Scatter plot of BMD of the patella with HKA angle. (F) Scatter plot of medial/lateral BMD of the DF with HKA angle. (G) Scatter plot of medial/lateral BMD of the PT with HKA angle. ***p<0.001. Abbreviations: KOA, knee osteoarthritis; OP, osteoporosis; BMD, bone mineral density; DF, distal femur; PT, proximal tibia; M/L, Medial/Lateral; HKA, Hip-Knee-Ankle angle. |
 |
Figure 7 Scatter plot of BMD around knee with HKA angle in patients with KOA. (A) Scatter plot of BMD of the medial DF with HKA angle. (B) Scatter plot of BMD of the lateral DF with HKA angle. (C) Scatter plot of BMD of the medial PT with HKA angle. (D) Scatter plot of BMD of the lateral PT with HKA angle. (E) Scatter plot of BMD of the patella with HKA angle. (F) Scatter plot of medial/lateral BMD of the DF with HKA angle. (G) Scatter plot of medial/lateral BMD of the PT with HKA angle. *p<0.05;**p<0.01. Abbreviations: KOA, knee osteoarthritis; BMD, bone mineral density; DF, distal femur; PT, proximal tibia; M/L, Medial/Lateral; HKA, Hip-Knee-Ankle angle. |
Discussion
In this study, we measured the changes in BMD around knee in postmenopausal women with KOA combined with or without OP, and measured the HKA, WOMAC degree and the degree of K&L grading to evaluate the difference of BMD around knee in postmenopausal women between KOA combined with OP patients and KOA patients. It was found that the BMD around knee in postmenopausal women with KOA combined with OP was significantly lower than that in patients with KOA, and a higher proportion of patients with KOA combined with OP had severe WOMAC degree than that in patients with KOA. The difference in the BMD around knee between patients with KOA combined with or without OP was not eliminated after adjustment for WOMAC degree. As the K&L classification increased, the medial knee BMD of the KOA combined with OP patients tended to increase and then decrease. And the OA group as a whole showed an increasing trend. Meanwhile, PT medial BMD and DF medial BMD in patients with KOA combined with OP showed a significant negative correlation with the HKA angle.This trend was also observed for DF and PT M/L BMD, indicating that the medial BMD around knee decreased significantly with the increase of the angle. This is also contrary to the data measured in patients with KOA alone, suggesting that OP significantly influences the effect brought about by HKA on BMD around knee.
A series of epidemiologic studies have shown that OA and OP, two diseases with opposite pathologic features, can occur in the same patient, the exact mechanism of which has not been clarified.31 With the advancement of imaging technology and the deepening of basic research, more and more evidence suggests that the subchondral bone is the primary target organ of OA.32 Lesions and changes in BMD in the subchondral region are correlated with cartilage loss in cases of OA.33 Systemic or joint localized OP can accelerate the development of OA by exacerbating damage to subchondral bone and cartilage.14 The relationship between KOA and OP has been investigated by many researchers, and a large number of studies have demonstrated that systemic BMD is a predictor of OA progression, plays a key role in the onset and progression of OA, and is associated with increased progression of medial and lateral cartilage defects in the tibiofemoral and accelerated degradation of tibiofemoral lateral cartilage volume.34,35 Recent studies have found that BMD around knee reflects early pathological changes in KOA, as evidenced by dense thickening of the subchondral bone and reduced bone mineralisation and elasticity, leading to increased BMD but no improvement in bone quality.36,37 Therefore, it is necessary to explore in detail the different clinical features of KOA with or without OP.
Abnormal subchondral bone activity and remodelling are crucial mechanisms in the development of OA pain.38 A study of tibial plateau specimens from patients with KOA found that increased local bone remodelling led to degradation of subchondral bone cysts and structural changes in the cyst region accelerated the destruction of the overlying cartilage.39 Furthermore, incorrect stress stimulation led to microfractures of the subchondral bone, bone marrow oedema and increased pain.40,41 The WOMAC scale is the most widely utilized instrument for evaluating joint pain and functional status in KOA. Its pain subscale demonstrates high internal consistency and provides a validated measure of perceived pain severity.42,43 In this study, we found that in patients with KOA, the BMD of the patella and lateral DF was significantly higher in patients with severe WOMAC degree than the moderate patients. This is similar to the findings of Burnett et al44 and Lo GH et al.45 Patients with high levels of pain had more pronounced reductions in BMD in the medial and total knee epiphysis and metaphysis, and patients with mild OA had significantly lower trabecular thickness than patients with severe OA.46 Some studies have also suggested that PT BMD is an independent risk factor for pain in patients with OA, with patients with low BMD tending to exhibit higher levels of pain.47 This is also consistent with our previous findings. Therefore, it is important to pay attention to changes in BMD in patients with KOA and to prevent the development of OP, especially for patients’ quality of life and pain levels.
The results of most studies have shown that the medial knee BMD in KOA patients was significantly higher than the lateral knee BMD in normal and OP patients.48 In the present study, our overall BMD around knee in the KOA combined with OP group was significantly lower than that of KOA patients. Interestingly, there was no significant difference in medial knee BMD between the two groups at K&L classification III, whereas there was still a significant difference in lateral BMD values between the two groups.The medial knee BMD in KOA combined OP patients tended to increase first with increasing K&L classification, and then decreased at K&L classification IV. In patients with KOA, knee BMD tended to increase with increasing K&L classification. Similarly, Kim YH et al found an inverted U-shaped relationship between hip BMD and hip OA K&L grading in patients with OP after adjusting for age and gender.49 The underlying pathophysiology can be conceptualized as follows: in early to mid-stage OA, persistent mechanical stress stimulates compensatory subchondral bone sclerosis to maintain joint stability, thereby increasing BMD. In contrast, concomitant OP compromises bone microarchitecture and repair capacity. In late-stage disease, this impaired state may prevent the subchondral bone from sustaining abnormal loads, leading to accumulated microfractures, expanded necrotic areas, and failed pathological remodeling, ultimately manifesting as a decline in BMD. This hypothesis integrates the localized sclerosis of OA with the systemic fragility of OP, providing a pathophysiological model for their co-existence. Several studies have shown that medial knee BMD is significantly higher in KOA patients than lateral knee BMD in OP patients, and the ratio of medial to lateral tibial BMD (M/L-BMD) is greater than.50,51 This performance is similar to similar results observed in this study in the group of KOA combined with OP patients versus the group of KOA patients, and we also observed that patella BMD was also significantly lower in KOA combined with OP patients than in KOA patients, and that the medial DF BMD as well as the medial PT BMD in KOA combined with OP patients increased with increasing K&L grading. This also suggests that OP appears to counteract the sclerotic effect of OA on the medial and subchondral patella of the knee, but the sclerosis still increases with increasing OA severity. This effect is not evident on the lateral side of the knee.
HKA is critical not only for the severity and pathogenesis of KOA, but also for knee degeneration. Improvement of knee valgus deformity can greatly slow down the rate of joint degeneration and is the key to preventing and treating severe KOA. Genu varum or valgum deformity may be caused by congenital anatomical and developmental abnormalities or secondary to cartilage wear and narrowing of the medial joint space following tibiofemoral subluxation.52 A previous study of BMD around knee in patients with KOA found that medial knee BMD was proportional to the severity of intra-articular dislocation of the knee.53 Similarly, medial knee BMD was higher than lateral BMD in KOA patients with internal derangement.54,55 This is similar to what we observed in the OA group of patients. In addition to our DF of interest, we also found that patella BMD was positively correlated with HKA. In contrast, in KOA patients with OP and medial knee BMD were negatively correlated with HKA. During the development of KOA, decreased remodeling of the subchondral bone of the medial malleolus and an imbalance between bone resorption and bone production lead to increased thickness and sclerosis of the subchondral bone plate. Studies have shown a 15% increase in subchondral bone density and a 30% increase in bone mass in patients with OA.56,57 The concomitant presence of OP significantly compromises the mechanical properties of subchondral bone, thereby accelerating the progression and severity of KOA. In patients with both conditions, the weakened subchondral bone, combined with abnormal stress, can lead to subsidence of the medial PT. This exacerbates cartilage degradation and contributes to internal knee derangement. Our findings demonstrate a significant negative correlation between the HKA angle and medial knee BMD, which partially supports this proposed mechanism. An increasing varus alignment (decreasing HKA angle) heightens stress on the medial compartment, further accelerating cartilage wear and establishing a vicious cycle. This finding aligns with existing literature, which suggests that concomitant OP may contribute to accelerated OA progression and exacerbated joint deformity.58 Consequently, maintaining normal BMD in KOA patients may help mitigate the progression of varus deformity.
Despite the novel findings of this study, several limitations should be acknowledged. First, the sample size, although sufficient for the primary outcome as confirmed by the post-hoc power analysis, was relatively modest. This was particularly evident in the subgroup analyses, such as for patients with severe OP or specific K&L grades, where the limited number of cases may have reduced the statistical power to detect significant differences. Second, as a single-center study conducted at a tertiary hospital, our cohort primarily consisted of patients with moderate to severe symptoms seeking specialized care. This inherent selection bias limits the generalizability of our findings to the broader community-based population of postmenopausal women with KOA, which likely includes a larger spectrum of disease severity, including many with mild or asymptomatic OA. Third, the cross-sectional nature of our study cannot establish causality or elucidate the temporal sequence of the observed changes. For instance, we cannot definitively conclude whether OP leads to changes in periarticular BMD that accelerate KOA progression, or if the progression of KOA and its associated disuse and pain ultimately contribute to bone loss. Fourth, we did not measure several key biochemical markers and hormone known to influence bone metabolism, such as serum vitamin D (25-(OH)D3), parathyroid hormone and estradiol. Vitamin D deficiency and secondary hyperparathyroidism are highly prevalent in postmenopausal women and represent significant, independent risk factors for reduced bone mass and OP. Our inability to account for these variables precluded a more detailed investigation into the pathophysiological interplay between OP and KOA from an endocrine-metabolic perspective. Future studies should incorporate these key serum biomarkers to facilitate multivariable analyses and statistically adjust for their potential confounding effects. Despite these limitations, this study provides valuable insights using advanced imaging technology. Future prospective, longitudinal, and multi-center studies incorporating comprehensive serological testing are warranted to confirm our findings and better understand the complex temporal relationship and pathophysiological mechanisms linking OP and periarticular bone changes in KOA.
Conclusion
This study describes the changes in BMD around knee in postmenopausal female KOA patients combined with or without OP. Overall, BMD around knee was lower and more painful in KOA combined OP postmenopausal female patients compared to KOA patients. Meanwhile, with increasing the severity of OA, medial BMD in KOA combined with OP patients tended to increase at first, and then decrease. As the angle of the knee valgus increases, the BMD around knee in the two groups of patients showed an opposite trend, with a increasing trend in patients with KOA combined with OP and an decreasing trend in patients with KOA. As the degree of OP increased, the BMD around knee became lower. Consequently, our results highlight the imperative for clinicians to actively screen for and manage OP in postmenopausal KOA patients. Interventions aimed at preventing bone loss and treating established OP may not only reduce fracture risk but also represent a promising strategy to alleviate pain, improve joint biomechanics, and potentially modify the progression of KOA, thereby enhancing the overall quality of life for this patient population.
Abbreviations
BMD, Bone Mineral Density; OA, Osteoarthritis; KOA, Knee Osteoarthritis; OP, Osteoporosis; TKA, Total Knee Arthroplasty; DF, Distal Femur; PT, Proximal Tibia; DXA, Dual-Energy X-ray Absorptiometry; DECT, Dual-Energy Computed Tomography; WOMAC, Western Ontario and McMaster University Osteoarthritis Index; GSI, Gemstone Spectral Imaging; BMI, Body Mass Index; M/L, Medial/Lateral; K&L, Kellgren-Lawrence; HKA, Hip-Knee-Ankle angle.
Data Sharing Statement
The data from the review are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University. In addition to this, we confirm that all methods were performed in accordance with the relevant guidelines and regulations. We made each patient sign a patient informed consent form at the time of the examination. Regarding informed consent, the “Patient Informed Consent Form” was approved by the Ethics Committee of the Second Hospital of Shanxi Province. This study complies with the Declaration of Helsinki.
Acknowledgments
We acknowledge the support provided by the Shanxi Provincial Key Laboratory of Bone and Soft Tissue Repair for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from Central-led Local Science and Technology Development Funds (YDZJSX20231A062), Shanxi Provincial Scientific, Technological Achievement Transformation Guidance Special Programme (202204021301067) and Postgradute Education Innovation Program of Shanxi Province (2025SJ016).
Disclosure
The authors declared that there is no conflicts of interest in this work.
References
1. Hu Y, Chen X, Wang S, Jing Y, Su J. Subchondral bone microenvironment in osteoarthritis and pain. Bone Res. 2021;9(1):20. doi:10.1038/s41413-021-00147-z
2. Tang S, Zhang C, Oo WM, et al. Osteoarthritis. Nat Rev Dis Primers. 2025;11(1):10. doi:10.1038/s41572-025-00594-6
3. Minnig M, Golightly YM, Nelson AE. Epidemiology of osteoarthritis: literature update 2022-2023. Curr Opin Rheumatol. 2024;36(2):108–112. doi:10.1097/BOR.0000000000000985
4. Johnston CB, Dagar M. Osteoporosis in older adults. Med Clin North Am. 2020;104(5):873–884. doi:10.1016/j.mcna.2020.06.004
5. Walker MD, Shane E. Postmenopausal Osteoporosis. N Engl J Med. 2023;389(21):1979–1991. doi:10.1056/NEJMcp2307353
6. Deng ZH, Zeng C, Li YS, et al. Relation between phalangeal bone mineral density and radiographic knee osteoarthritis: a cross-sectional study. BMC Musculoskelet Disord. 2016;17:71. doi:10.1186/s12891-016-0918-x
7. Yokota S, Ishizu H, Miyazaki T, Takahashi D, Iwasaki N, Osteoporosis ST. Osteoarthritis, and Subchondral Insufficiency Fracture: recent Insights. Biomedicines. 2024;12(4). doi:10.3390/biomedicines12040843
8. Soininvaara TA, Harju KA, Miettinen HJ, Kröger HP. Periprosthetic bone mineral density changes after unicondylar knee arthroplasty. Knee. 2013;20(2):120–127. doi:10.1016/j.knee.2012.10.004
9. Im GI, Kim MK. The relationship between osteoarthritis and osteoporosis. J Bone Miner Metab. 2014;32(2):101–109. doi:10.1007/s00774-013-0531-0
10. Kim D, Pirshahid AA, Li Y, Varghese T, Pope JE. Prevalence of osteoporosis in osteoarthritis: a systematic review and meta-analysis. Osteoporos Int. 2022;33(8):1687–1693. doi:10.1007/s00198-022-06376-0
11. Bellido M, Lugo L, Roman-Blas JA, et al. Subchondral bone microstructural damage by increased remodelling aggravates experimental osteoarthritis preceded by osteoporosis. Arthritis Res Ther. 2010;12(4):R152. doi:10.1186/ar3103
12. Setty N, Leboff MS, Thornhill TS, Rinaldi G, Glowacki J. Underestimated fracture probability in patients with unilateral Hip osteoarthritis as calculated by FRAX. J Clin Densitom. 2011;14(4):447–452. doi:10.1016/j.jocd.2011.06.001
13. Hahn MH, Won YY. Bone mineral density changes after total knee replacement in women over the age of 65. J Bone Metab. 2013;20(2):105–109. doi:10.11005/jbm.2013.20.2.105
14. Wada H, Aso K, Izumi M, Ikeuchi M. The effect of postmenopausal osteoporosis on subchondral bone pathology in a rat model of knee osteoarthritis. Sci Rep. 2023;13(1):2926. doi:10.1038/s41598-023-29802-7
15. Zhang J, Hu W, Li Y, et al. MAGI1 attenuates osteoarthritis by regulating osteoclast fusion in subchondral bone through the RhoA-ROCK1 signaling pathway. J Orthop Translat. 2025;52:167–181. doi:10.1016/j.jot.2025.04.007
16. Cui Z, Wu H, Xiao Y, et al. Endothelial PDGF-BB/PDGFR-β signaling promotes osteoarthritis by enhancing angiogenesis-dependent abnormal subchondral bone formation. Bone Res. 2022;10(1):58. doi:10.1038/s41413-022-00229-6
17. Su S, Tian R, Jiao Y, et al. Ubiquitination and deubiquitination: implications for the pathogenesis and treatment of osteoarthritis. J Orthop Translat. 2024;49:156–166. doi:10.1016/j.jot.2024.09.011
18. Jeray KJ, Williams SA, Wang Y, et al. Bone health management in elective orthopaedic surgery: a claims-based observational study. Geriatr Orthop Surg Rehabil. 2023;14:21514593231216553. doi:10.1177/21514593231216553
19. Kang KH, Kim MS, Kim JJ, In Y. Risk factors and preventive strategies for perioperative distal femoral fracture in patients undergoing total knee arthroplasty. Medicina. 2023;59(2). doi:10.3390/medicina59020369
20. Kato M, Warashina H, Kataoka A, Ando T, Mitamura S. Calcaneal insufficiency fractures following ipsilateral total knee arthroplasty. Injury. 2021;52(7):1978–1984. doi:10.1016/j.injury.2021.05.008
21. Calvo E, Castañeda S, Largo R, Fernández-Valle ME, Rodríguez-Salvanés F, Herrero-Beaumont G. Osteoporosis increases the severity of cartilage damage in an experimental model of osteoarthritis in rabbits. Osteoarthritis Cartilage. 2007;15(1):69–77. doi:10.1016/j.joca.2006.06.006
22. Lo GH, Tassinari AM, Driban JB, et al. Cross-sectional DXA and MR measures of tibial periarticular bone associate with radiographic knee osteoarthritis severity. Osteoarthritis Cartilage. 2012;20(7):686–693. doi:10.1016/j.joca.2012.03.006
23. LaValley MP, Lo GH, Price LL, Driban JB, Eaton CB, McAlindon TE. Development of a clinical prediction algorithm for knee osteoarthritis structural progression in a cohort study: value of adding measurement of subchondral bone density. Arthritis Res Therapy. 2017;19(1):95. doi:10.1186/s13075-017-1291-3
24. Vetter JR, Perman WH, Kalender WA, Mazess RB, Holden JE. Evaluation of a prototype dual-energy computed tomographic apparatus. II. Determination of vertebral bone mineral content. Med Phys. 1986;13(3):340–343. doi:10.1118/1.595951
25. Wesarg S, Kirschner M, Becker M, Erdt M, Kafchitsas K, Khan MF. Dual-energy CT-based assessment of the trabecular bone in vertebrae. Methods Inf Med. 2012;51(5):398–405. doi:10.3414/ME11-02-0034
26. Kanis JA, Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos Int. 1994;4(6):368–381. doi:10.1007/BF01622200
27. Qiu ML, Xie Y, Wang XH, et al. Practice guideline for patients with osteoporosis. Zhonghua Nei Ke Za Zhi. 2020;59(12):953–959. doi:10.3760/cma.j.cn112138-20200904-00792
28. Mu S, Wang J, Gong S. Application of medical imaging based on deep learning in the treatment of lumbar degenerative diseases and osteoporosis with bone cement screws. Comput Math Methods Med. 2021;2021:2638495. doi:10.1155/2021/2638495
29. Lobos S, Cooke A, Simonett G, Ho C, Boyd SK, Edwards WB. Assessment of bone mineral density at the distal femur and the proximal tibia by dual-energy x-ray absorptiometry in individuals with spinal cord injury: precision of protocol and relation to injury duration. J Clin Densitom. 2018;21(3):338–346. doi:10.1016/j.jocd.2017.05.006
30. Boudenot A, Pallu S, Toumi H, Loiseau Peres S, Dolleans E, Lespessailles E. Tibial subchondral bone mineral density: sources of variability and reproducibility. Osteoarthritis Cartilage. 2013;21(10):1586–1594. doi:10.1016/j.joca.2013.07.009
31. Rizou S, Chronopoulos E, Ballas M, Lyritis GP. Clinical manifestations of osteoarthritis in osteoporotic and osteopenic postmenopausal women. J Musculoskelet Neuronal Interact. 2018;18(2):208–214.
32. Li X, Roemer FW, Cicuttini F, MacKay JW, Turmezei T, Link TM. Early knee OA definition-what do we know at this stage? An imaging perspective. Ther Adv Musculoskelet Dis. 2023;15:1759720X231158204. doi:10.1177/1759720X231158204
33. Wang H, Yuan T, Wang Y, et al. Osteoclasts and osteoarthritis: novel intervention targets and therapeutic potentials during aging. Aging Cell. 2024;23(4):e14092. doi:10.1111/acel.14092
34. Teichtahl AJ, Wang Y, Wluka AE, et al. Associations between systemic bone mineral density and early knee cartilage changes in middle-aged adults without clinical knee disease: a prospective cohort study. Arthritis Res Ther. 2017;19(1):98. doi:10.1186/s13075-017-1314-0
35. Qu Y, Chen S, Han M, et al. Osteoporosis and osteoarthritis: a bi-directional Mendelian randomization study. Arthritis Res Ther. 2023;25(1):242. doi:10.1186/s13075-023-03213-5
36. Bertoldi I, Frediani B. Osteoarthritis and osteoporosis: correlations between two clinical entities. Reumatismo. 2013;65(2):51–54. doi:10.4081/reumatismo.2013.51
37. Hannani MT, Thudium CS, Karsdal MA, et al. From biochemical markers to molecular endotypes of osteoarthritis: a review on validated biomarkers. Expert Rev Mol Diagn. 2024;24(1–2):23–38. doi:10.1080/14737159.2024.2315282
38. Zhang M, Hu W, Cai C, Wu Y, Li J, Dong S. Advanced application of stimuli-responsive drug delivery system for inflammatory arthritis treatment. Mater Today Bio. 2022;14:100223. doi:10.1016/j.mtbio.2022.100223
39. Tong H, Chen R, Yin H, et al. Mesenteric lymph duct ligation alleviating lung injury in heatstroke. Shock. 2016;46(6):696–703. doi:10.1097/SHK.0000000000000660
40. Liu SY, Song JC, Mao HD, Zhao JB, Song Q. Expert consensus on the diagnosis and treatment of heat stroke in China. Mil Med Res. 2020;7(1):1. doi:10.1186/s40779-019-0229-2
41. Coaccioli S, Sarzi-Puttini P, Zis P, Rinonapoli G, Varrassi G. Osteoarthritis: new insight on its pathophysiology. J Clin Med. 2022;11(20):6013. doi:10.3390/jcm11206013
42. Bliddal H, Bays H, Czernichow S, et al. Once-weekly semaglutide in persons with obesity and knee osteoarthritis. N Engl J Med. 2024;391(17):1573–1583. doi:10.1056/NEJMoa2403664
43. Bideshki MV, Jourabchi-Ghadim N, Radkhah N, et al. The efficacy of curcumin in relieving osteoarthritis: a meta-analysis of meta-analyses. Phytother Res. 2024;38(6):2875–2891. doi:10.1002/ptr.8153
44. Burnett WD, Kontulainen SA, McLennan CE, et al. Knee osteoarthritis patients with severe nocturnal pain have altered proximal tibial subchondral bone mineral density. Osteoarthritis Cartilage. 2015;23(9):1483–1490. doi:10.1016/j.joca.2015.04.012
45. Lo GH, Schneider E, Driban JB, et al. Periarticular bone predicts knee osteoarthritis progression: data from the Osteoarthritis Initiative. Semin Arthritis Rheum. 2018;48(2):155–161. doi:10.1016/j.semarthrit.2018.01.008
46. Wen L, Shin MH, Kang JH, et al. The relationships between bone mineral density and radiographic features of hand or knee osteoarthritis in older adults: data from the dong-gu study. Rheumatology. 2016;55(3):495–503. doi:10.1093/rheumatology/kev377
47. Burnett WD, Kontulainen SA, McLennan CE, et al. Proximal tibial trabecular bone mineral density is related to pain in patients with osteoarthritis. Arthritis Res Therapy. 2017;19(1):200. doi:10.1186/s13075-017-1415-9
48. Shakoor N, Dua A, Thorp LE, et al. Asymmetric loading and bone mineral density at the asymptomatic knees of patients with unilateral Hip osteoarthritis. Arthritis Rheum. 2011;63(12):3853. doi:10.1002/art.30626
49. Kim YH, Lee JS, Park JH. Association between bone mineral density and knee osteoarthritis in Koreans: the Fourth and Fifth Korea National Health and Nutrition Examination Surveys. Osteoarthritis Cartilage. 2018;26(11):1511–1517. doi:10.1016/j.joca.2018.07.008
50. Omoumi P, Babel H, Jolles BM, Favre J. Quantitative regional and sub-regional analysis of femoral and tibial subchondral bone mineral density (sBMD) using computed tomography (CT): comparison of non-osteoarthritic (OA) and severe OA knees. Osteoarthritis Cartilage. 2017;25(11):1850. doi:10.1016/j.joca.2017.07.014
51. Thorp LE, Wimmer MA, Block JA, et al. Bone mineral density in the proximal tibia varies as a function of static alignment and knee adduction angular momentum in individuals with medial knee osteoarthritis. Bone. 2006;39(5):1116–1122. doi:10.1016/j.bone.2006.05.001
52. Akamatsu Y, Kobayashi H, Mitsuhashi S, Kusayama Y. Bone mineral density around the knee after open wedge high tibial osteotomy measured up to 24 months in 51 patients. Knee Surg Sports Traumatol Arthrosc. 2023;31(11):4910–4919. doi:10.1007/s00167-023-07539-0
53. Zhang C, Zhuang Z, Chen X, et al. Osteoporosis is associated with varus deformity in postmenopausal women with knee osteoarthritis: a cross-sectional study. BMC Musculoskelet Disord. 2021;22(1):694. doi:10.1186/s12891-021-04580-3
54. Rougereau G, Villard A, Langlais T, Delord M, Boisrenoult P, Pujol N. Femoral condyle bone mineral density in osteoarthritis differs significantly between knees with valgus vs. varus deformity. Orthop Traumatol Surg Res. 2023;109(5):103584. doi:10.1016/j.otsr.2023.103584
55. Ishii Y, Noguchi H, Sato J, Ishii H, Todoroki K, Toyabe SI. Association between bone mineral density distribution and various radiographic parameters in patients with advanced medial osteoarthritis of the knee. J Orthop Sci. 2019;24(4):686–692. doi:10.1016/j.jos.2018.12.019
56. Arden NK, Griffiths GO, Hart DJ, Doyle DV, Spector TD. The association between osteoarthritis and osteoporotic fracture: the Chingford Study. Br J Rheumatol. 1996;35(12):1299–1304. doi:10.1093/rheumatology/35.12.1299
57. Hannan MT, Anderson JJ, Zhang Y, Levy D, Felson DT. Bone mineral density and knee osteoarthritis in elderly men and women. The Framingham Study. Arthritis Rheum. 1993;36(12):1671–1680. doi:10.1002/art.1780361205
58. Linde KN, Puhakka KB, Langdahl BL, et al. Bone mineral density is lower in patients with severe knee osteoarthritis and attrition. Calcif Tissue Int. 2017;101(6):593–601. doi:10.1007/s00223-017-0315-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Hemoglobin Levels and Osteoporosis in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Ye T, Lu L, Guo L, Liang M
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2803-2811
Published Date: 14 September 2022
Clinical Utility of Romosozumab in the Management of Osteoporosis: Focus on Patient Selection and Perspectives
Lim SY, Bolster MB
International Journal of Women's Health 2022, 14:1733-1747
Published Date: 15 December 2022
The Effects of Switching from Dipeptidyl Peptidase-4 Inhibitors to Glucagon-Like Peptide-1 Receptor Agonists on Bone Mineral Density in Diabetic Patients
Huang CF, Mao TY, Hwang SJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:31-36
Published Date: 11 January 2023
The Relationship Between Serum 25-Hydroxyvitamin D Levels and Osteoporosis in Postmenopausal Women
Wang D, Yang Y
Clinical Interventions in Aging 2023, 18:619-627
Published Date: 18 April 2023
Causal Effects of Female Reproductive and Hormonal Factors on Osteoporosis, Bone Mineral Density, and Osteoarthritis: A Two-Sample Mendelian Randomization Study
Li G, Shen W, Chen J, Dai Y, Mo G, Wang S, Wang X
International Journal of Women's Health 2026, 18:574318
Published Date: 7 May 2026