Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association Between Hemoglobin Levels and Osteoporosis in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Authors Ye T ![]() , Lu L, Guo L, Liang M
, Lu L, Guo L, Liang M
Received 15 July 2022
Accepted for publication 2 September 2022
Published 14 September 2022 Volume 2022:15 Pages 2803—2811
DOI https://doi.org/10.2147/DMSO.S382480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Tingting Ye, Liujin Lu, Liuqing Guo, Min Liang
Department of Geriatric Endocrinology and Metabolism, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China
Correspondence: Min Liang, Department of Geriatric Endocrinology and Metabolism, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China, Tel +86 13878838907, Email [email protected]
Purpose: To explore the relationship between hemoglobin levels and osteoporosis and the risk factors for osteoporosis in patients with type 2 diabetes mellitus (T2DM).
Patients and methods: A cross-sectional study was conducted in 495 T2DM adults. Medical data were collected from electronic medical records.
Results: T2DM patients with osteoporosis had significant lower hemoglobin levels (P < 0.001). Spearman correlation analysis and logistic regression analysis showed that age, female, body mass index (BMI), smoking, drinking and hemoglobin levels were significantly associated with osteoporosis in T2DM patients (all P < 0.05). After adjustment for BMI, diabetic duration, estimated glomerular filtration rate (eGFR), smoking and drinking, a significant association between hemoglobin levels and osteoporosis was observed in T2DM males aged 50 years and older (odds ratio [OR] = 0.978, 95% confidence interval [CI]: 0.958– 0.998, P = 0.030). Compared to Q3 groups with normal hemoglobin levels, Q1 groups with anemia had an odd of osteoporosis increased 2.9-fold in T2DM men after adjustment for age, BMI, diabetic duration, eGFR, smoking and drinking (P = 0.032).
Conclusion: Hemoglobin levels were associated with the presence of osteoporosis in T2DM men, especially in those aged 50 years and older.
Keywords: type 2 diabetes mellitus, osteoporosis, hemoglobin, bone mineral density
Introduction
Diabetes Mellitus (DM) is one of the most common and fastest growing diseases worldwide, projected to affect 693 million adults by 2045.1,2 Type 2 diabetes mellitus (T2DM) accounts for 90–95% of all diabetes.3 The prevalence of osteoporosis (OP) is increasing as the growth in the aging population and lifestyle changes. As previously reported, the prevalence of osteoporosis in China was 6.46% and 29.13% for men and women aged 50 years and older, respectively.4 As a chronic metabolic disease, T2DM can cause abnormal bone metabolism, microarchitectural deterioration of bone tissue and increased bone fragility, resulting in to the occurrence of diabetic osteoporosis. Compared with individuals without T2DM, an increase in fracture incidence, especially hip fracture, was observed in individuals with T2DM despite normal or even higher bone mineral density (BMD).5 Obesity, poor glycemic control, longer duration and increased risk of falls may contribute to the increased fracture associated with T2DM.6 A cohort study in Spain showed that men and women with T2DM were at a 28% and 57% higher risk of post hip fracture mortality, respectively.7 T2DM patients have high mortality and disability after fracture, resulting in reduced quality of life and heavy burden on society. Therefore, early diagnosis of osteoporosis and prevention of fracture are critical for T2DM patients.
Early evidences indicated that the risk of anemia in patients with DM is 2–3 times higher than that of patients without DM.8 Diabetes-related chronic hyperglycemia can cause hypoxia in the renal interstitium and impaired erythropoietin (EPO) production in peritubular fibroblasts, resulting in anemia.9 Anemia not only increases the risk of diabetes-related microvascular and macrovascular complications, but is also associated with osteoporosis. Several preclinical studies have showed a close association between anemia and bone metabolism. In zebrafish, iron deficiency anemia affected bone formation through the BMPs signaling pathway.10 EPO induced dose-dependent and mostly irreversible bone loss in mice, and anemia is a potent stimulus for EPO production.11 Some authors concluded that increased expression of fetal hemoglobin drove osteoblast bone differentiation in association with decreased inflammatory cytokine release.12 Such possible link has also be reported in clinical studies. Patients with anemia had lower BMD and higher incidence of osteopenia and osteoporosis, while older men with declining hip BMD also had increased risk of anemia.13–16 Hemoglobin has been reported to be genetically associated with femoral neck BMD.17 A cohort study in Pomerania corroborated a close link between anemia and poor bone quality in elderly people.18 Similar results also appeared in a study of elderly people without anemia in South Korea.19 A population-based study concluded that hemoglobin levels <140 g/L in men and <130 g/L in women best predicted osteoporosis.20 However, a significant correlation between hemoglobin levels and BMD was not observed in another study.21 The correlation between hemoglobin levels and osteoporosis is still not clear.
Previous studies on the association between hemoglobin levels and osteoporosis were mostly conducted in the non-DM population. To our knowledge, few studies exist on such relationship in T2DM patients. The aim of this study was to evaluate the relationship between hemoglobin levels and osteoporosis in T2DM patients, and to explore risk factors affecting the occurrence of osteoporosis in T2DM patients.
Materials and Methods
Subjects
A total of 2045 adults with T2DM were consecutively recruited from among hospitalized patients at the Department of Endocrinology and the Department of Geriatric Endocrinology of the First Affiliated Hospital of Guangxi Medical University from July 2020 to June 2021. Type 2 diabetes mellitus was diagnosed according to the American Diabetes Association criteria.22 Inclusion criteria were age ≥18 years and presence of T2DM. Exclusion criteria were as follows: (1) patients with acute diabetic complications, inflammation or tumor; (2) severe heart failure, liver or renal impairments; (3) patients with diseases affecting bone metabolism or hemoglobin, such as hyperthyroidism, hypothyroidism, hyperparathyroidism, hypercortisolism, connective tissue diseases, multiple myeloma. (4) patients taking drugs affecting bone metabolism or hemoglobin, such glucocorticoid use. (5) lack of necessary data. Ultimately, 495 patients (299 men and 196 women) were eligible and included in the study (Figure 1). The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University in accordance with the principles of Helsinki Declaration. Written informed consent was obtained from each subject.
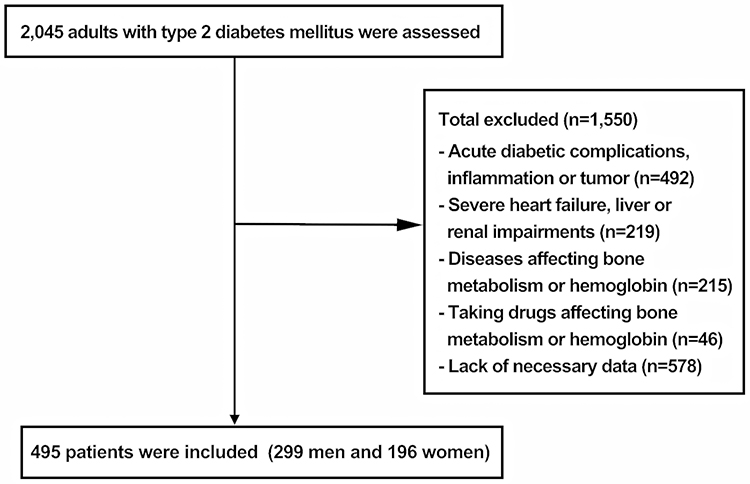 |
Figure 1 Flow diagram of the subjects selection process. |
Methods
General Data
Demographic characteristics (age and gender), medical history, anthropometric data (height and weight), personal habits (smoking and drinking) were collected from electronic medical records. Body mass index (BMI) was calculated as the ratio of weight (kg) to height2 (m2).
Determination of Biochemical Indices
Laboratory data including fast blood glucose (FBG), glycated hemoglobin A1c (HbA1c), red blood cell (RBC), hemoglobin (HGB), platelets (PLT), albumin (ALB), 25(OH)D and serum creatinine were collected. All laboratory parameters were determined by venous blood samples following fasting for 8 to 12 hours, and measured by professional medical laboratory researchers of the First Affiliated Hospital of Guangxi Medical University. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation.23
Hemoglobin Levels Measurement
Hemoglobin levels was measured by colorimetric assay with an automatic analyzer (Hitachi P800). Since the sex difference in hemoglobin levels in adults, we classified men and women into three groups by their hemoglobin levels: for men, Q1: <120 g/L, Q2: 120–140g/L, Q3: ≥140g/L; for women, Q1: <110 g/L, Q2: 110–130g/L, Q3: ≥130g/L. According to World Health Organization (WHO) hemoglobin cutoffs, anemia was defined as hemoglobin <130 g/L in men and hemoglobin <120 g/L in women.24 Patients in the Q1 groups met the criteria for anemia.
Bone Mineral Density Measurement
BMD was measured by dual energy X-ray absorptiometry (Hologic, USA). The measured areas included the lumbar spine and the hip areas. The diagnosis of osteoporosis in this study was based on the diagnostic criteria recommended by WHO.25
Statistical Analysis
Kolmogorov–Smirnov test was used to test normal distribution of data. Continuous variables with or without normal distribution were expressed as mean ± SD or median (interquartile range), respectively. We compared the differences of the means used two-sample t-test or one-way analysis of variance (ANOVA). Comparison of the medians between groups used Mann–Whitney U-test. Categorical variables were shown as numbers and percentages. The χ2 test was used to compare categorical variables according groups. Spearman correlation was used to perform the correlation of variables with BMD and osteoporosis. To assess odds ratios (ORs) and 95% confidence interval (CIs) for related variables according to the occurrence of osteoporosis, we used logistic regression analysis. Furthermore, we used logistic regression analysis to evaluate the association between hemoglobin levels with osteoporosis according to age and gender. All analyses were performed using SPSS 26.0. The P-values of all results were bilateral, and the significance level was set at P < 0.05.
Results
Baseline Characteristics of the Study Participants
Baseline characteristics of study participants are shown in Table 1. Among the study population (n = 495) ranged in age from 30 to 95 years, the mean age was 60.37±11.41 years, and 299 (60.40%) patients were male. Patients were divided into two groups based on the prevalence of osteoporosis: an OP group (OP, n = 165) and a non-OP group (NOP, n = 330). In participants with osteoporosis, BMI, RBC, hemoglobin levels, femoral neck (FN) BMD, total hip (TH) BMD, lumbar spine (LS) BMD were lower, whereas age and ALB were higher than those in participants without osteoporosis (all P < 0.05). No differences were observed for diabetic duration, FBG, HbA1c, PLT, 25(OH)D and eGFR between the two groups. Q3 had higher FN BMD than Q1 and Q2. TH BMD increased significantly in line with increase in hemoglobin levels (P = 0.001) (Table 2).
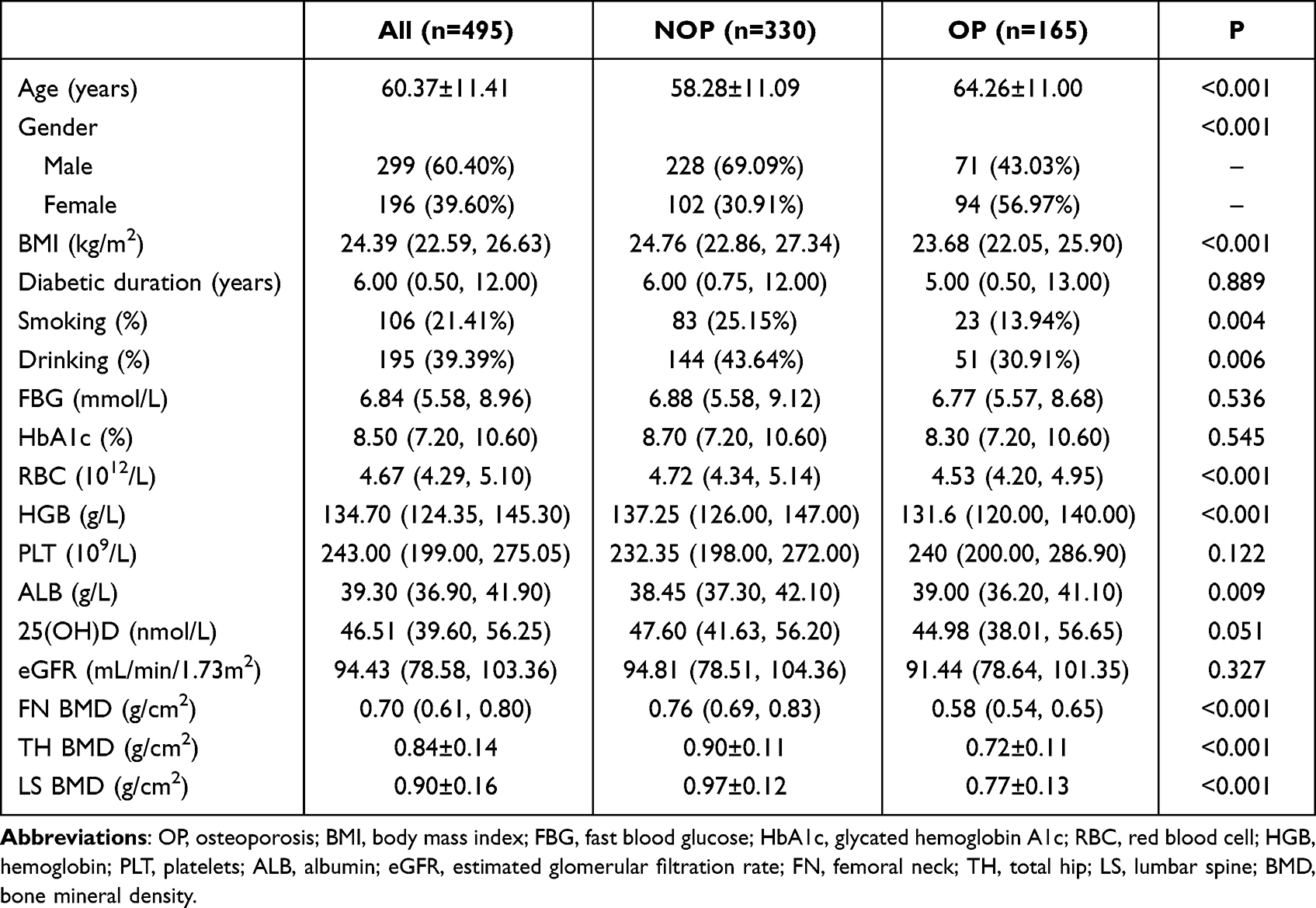 |
Table 1 Characteristics of the Study Population Stratified by the Prevalence of Osteoporosis |
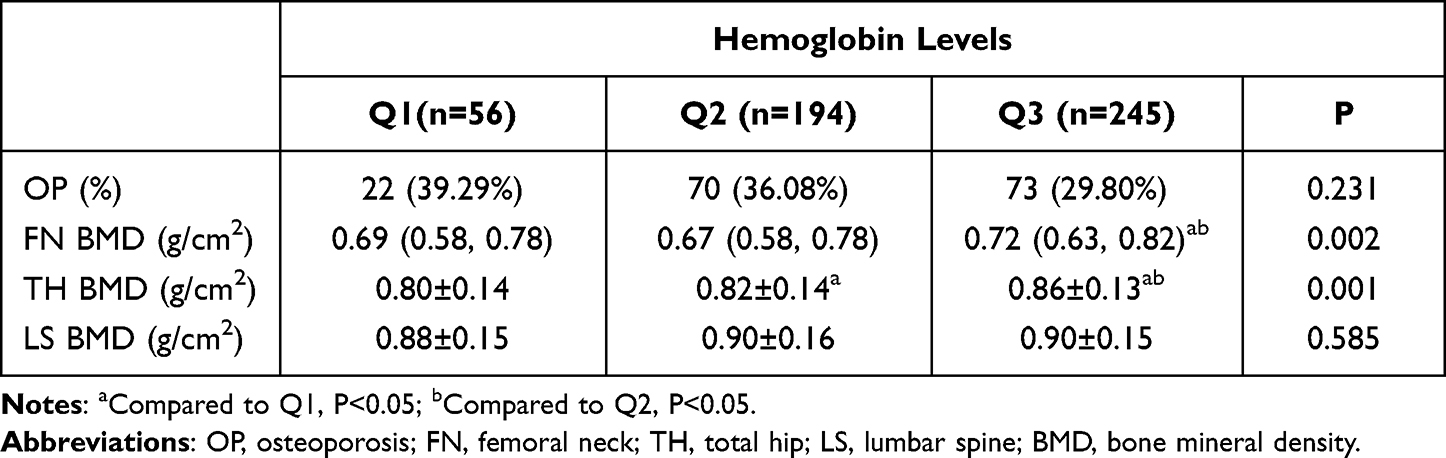 |
Table 2 The Prevalence of Osteoporosis and BMD Grouped by Hemoglobin Levels |
Association of Risk Factors with BMD and Osteoporosis
Spearman correlation analysis showed that the prevalence of osteoporosis was positively associated with age and female, and negatively associated with BMI, smoking, drinking, RBC and hemoglobin levels. FN BMD, TH BMD and LD BMD were positively associated with BMI, smoking, drinking, RBC and hemoglobin levels, and inversely associated with age and female (all P < 0.05) (Table 3). Logistic regression analysis showed that age, gender, BMI, smoking, drinking and hemoglobin levels were significantly associated with osteoporosis (all P < 0.05) (Table 4).
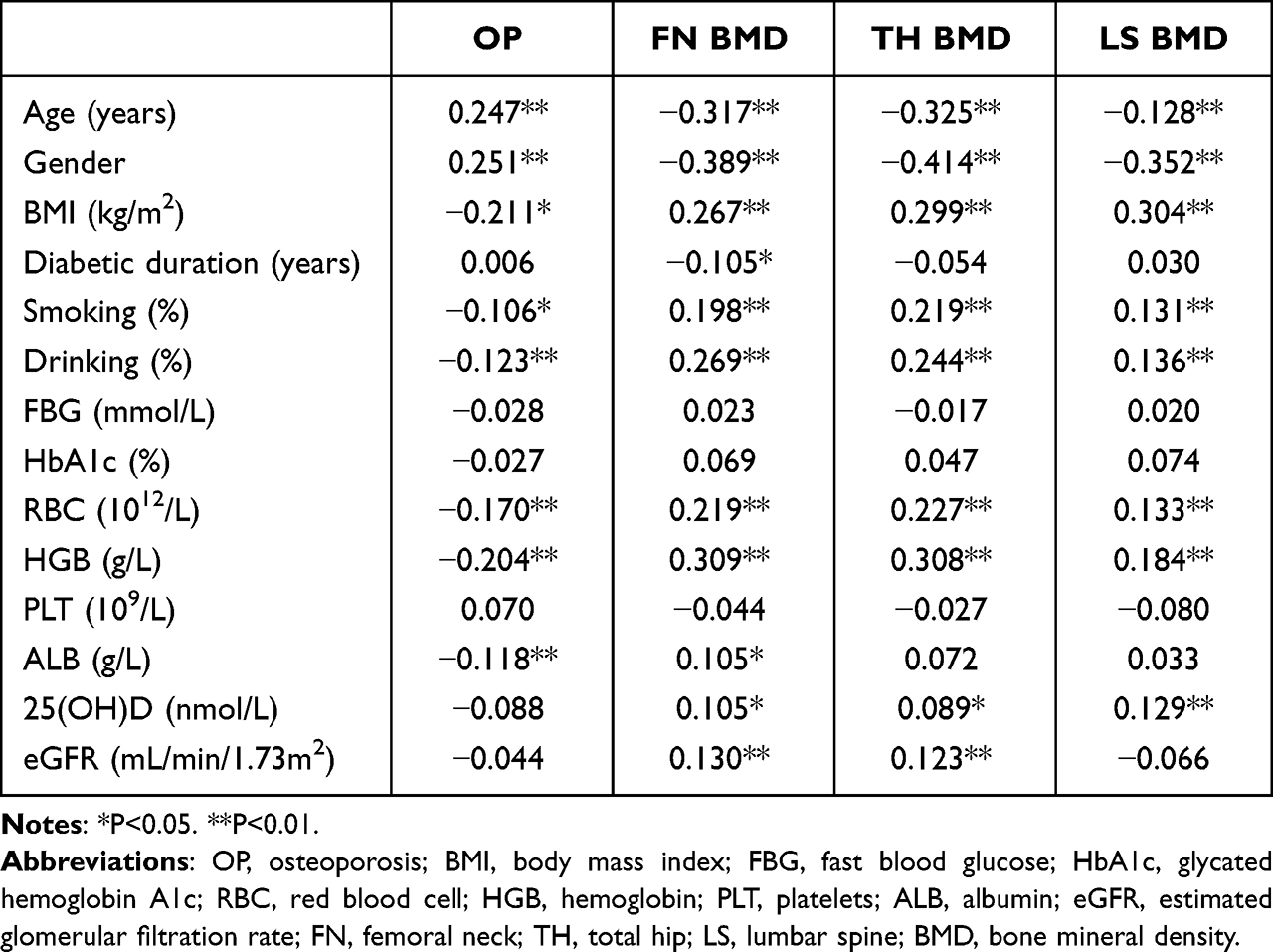 |
Table 3 Spearman Correlation Analysis on Associations of Risk Factors with BMD and Osteoporosis |
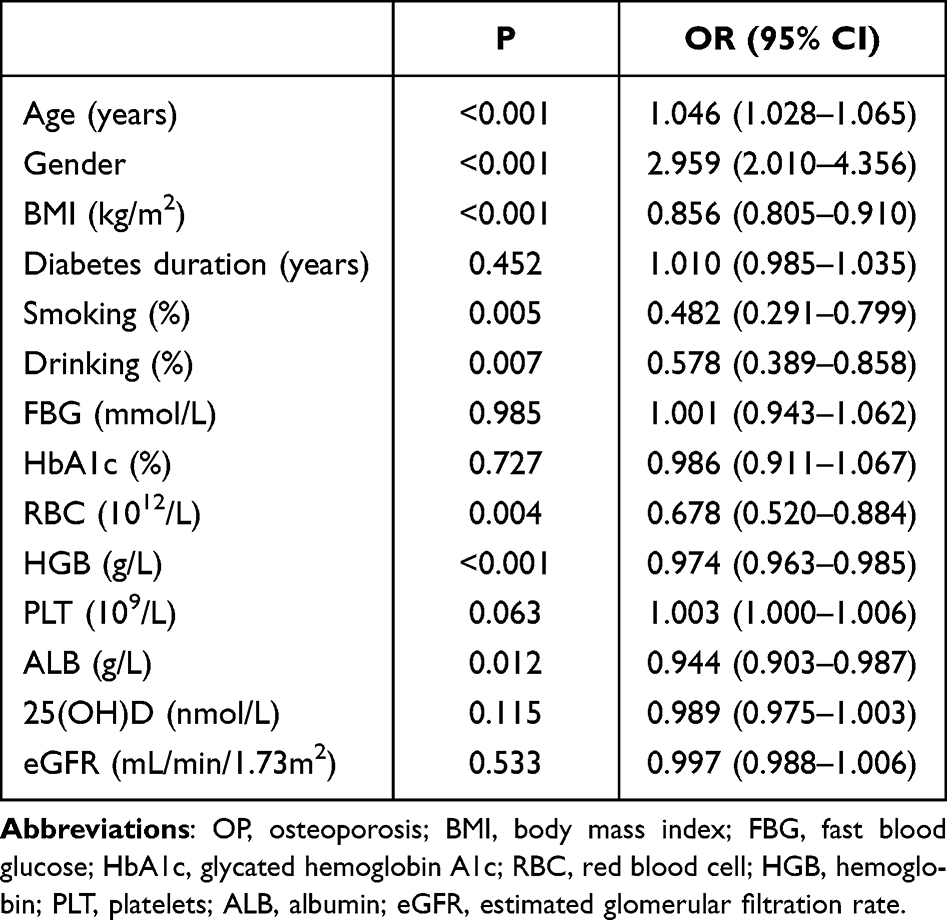 |
Table 4 Logistic Regression Analysis of Osteoporosis Risk Factors in Patients with T2DM |
Association Between Hemoglobin Levels and Osteoporosis
The association between hemoglobin levels and osteoporosis in T2DM patients was shown in Tables 5 and 6. In the model 1 (adjusted for age, BMI, diabetic duration and eGFR) and model 2 (adjusted for smoking and drinking based on model 1), we observed that hemoglobin levels were inversely associated with incident osteoporosis in T2DM males (P < 0.05). The OR (95% CI) was 0.976 (0.956–0.995) for both model 1 and model 2. We performed further logistic regression analysis after classifying T2DM males by age. After adjustment for BMI, diabetic duration, eGFR, smoking and drinking, hemoglobin levels were still associated with osteoporosis in T2DM males aged 50 years and older (P = 0.030). The OR (95% CI) was 0.978 (0.958–0.998).
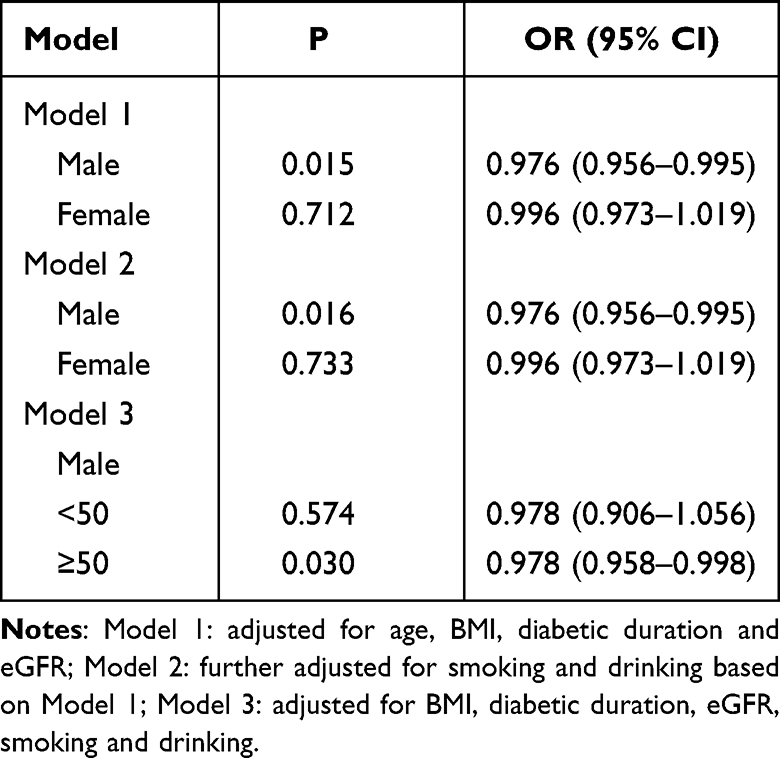 |
Table 5 Logistic Regression Models for the Association Between Hemoglobin Levels and Osteoporosis Stratified by Gender and Age |
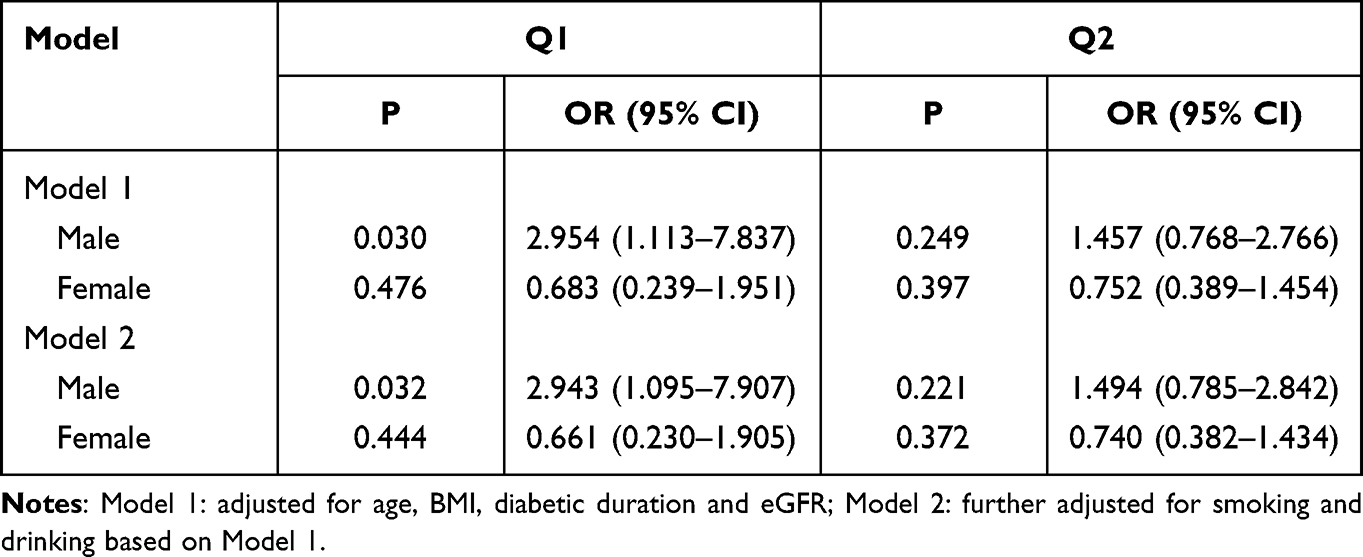 |
Table 6 The Association Between Hemoglobin at Three Levels and Osteoporosis Stratified by Gender |
We identified the correlation between different hemoglobin levels and osteoporosis by logistic regression, with osteoporosis as the dependent variable and hemoglobin at three levels (Q1, Q2 and Q3) as the independent variable. Q3 was set as the reference group. Compared to Q3, Q1 had an odd of osteoporosis increased 2.9-fold in men in both model 1 and model 2 (P < 0.05). No significant difference was found between Q2 and Q3. No significant association between hemoglobin levels and osteoporosis was detected in T2DM women.
Discussion
By analyzing hemoglobin, our study revealed that there could be a significant association between hemoglobin levels and osteoporosis in patients with T2DM. First, patients with osteoporosis had lower hemoglobin levels. Second, TH BMD tended to be higher in patients with higher hemoglobin levels, indirectly supporting the relationship between hemoglobin levels and osteoporosis. Furthermore, after adjusting for confounding factors, hemoglobin levels were also identified to be significantly associated with osteoporosis by logistic regression analysis.
Anemia is common in patients with T2DM. In a study of 2889 diabetic patients, male, older age, low eGFR, poor glycemic control and longer duration of illness were found to be contributing factors for the development of anemia in diabetic patients.26 The significant association of eGFR and diabetic duration with osteoporosis in T2DM patients was not detected in this study. However, previous studies have shown that both eGFR and diabetic duration are associated with osteoporosis and anemia in T2DM patients,6,26,27 so these variables were also included in the logistic regression models in this study. Hemoglobin can cause fluctuation of HbA1c, so HbA1c was not included in the models to prevent bias. In our study, BMI was positively correlated with BMD in T2DM patients. Previous evidence also suggested that increasing BMI was associated with higher BMD for non-obese men (BMI <30), but not associated with BMD for obese men (BMI >30).28 Increased BMI within a range is a protective factor for osteoporosis.
Hemoglobin levels have been reported to be associated with osteoporosis in the normal glycemic population. A retrospective study in Turkey showed that anemia was an independent predictor of low bone mass for spine in postmenopausal women.29 A study of male adults not only revealed a positive correlation between hemoglobin levels and BMD, but also found a negative association of hemoglobin levels with both hip fracture risk and major osteoporotic fracture risk assessed by FRAX.30 Another also suggested low and high hemoglobin values were associated with increased hip fracture risk.31 The conclusions of the above studies are generally consistent with the results of this study. Conversely, a longitudinal study in older adults did not support the hypothesis that hemoglobin levels are associated with BMD,21 possibly due to differences in race, age, inclusion and exclusion criteria.
Both hemoglobin levels and osteoporosis may be affected by gender and age, and we therefore investigated the association between hemoglobin levels and osteoporosis in males and females separately. A significant negative correlation between hemoglobin levels and osteoporosis was observed in males, while no such association was observed in females. A possible explanation for the absence of the association in females might be the small sample size for females. We further analyzed the relationship between hemoglobin levels and osteoporosis in T2DM males stratified by age. After adjustment for BMI, diabetic duration, eGFR, smoking and drinking, the significant correlation between hemoglobin levels and osteoporosis still existed in T2DM men aged 50 years and older, but not in T2DM men aged <50 years. Since the cut-off points for anemia in Chinese men and women were 120 g/L and 110 g/L, respectively, we divided patients into three groups according to their hemoglobin levels. We found that anemia was significantly associated with the occurrence of osteoporosis in T2DM men after adjustment for age, BMI, diabetic duration, eGFR, smoking and drinking. The results of subgroup analyses thus suggested the need to pay particular attention to T2DM males aged 50 years and older or T2DM males with anemia, in order to prevent osteoporosis. A retrospective study in Taiwan also found that anemia were related to lower BMD and a higher percentage of osteoporosis in T2DM patients.32 But the study was only performed in men above 50 years of age and postmenopausal women. Our study included a broader age range of patients aged 30–95 years with T2DM, and performed age-stratified analyses. We think that this study is the first to evaluate the association between hemoglobin levels and osteoporosis by age-stratified analyses in T2DM men, and the first to show that the results of this relationship are different in T2DM men of different ages. There is no doubt that osteoporosis mainly affects postmenopausal women. Although osteoporosis in women has a higher frequency than the male counterpart, osteoporosis in men is not at all rare, and there are more complications and higher mortality after osteoporotic fractures in men.33 However, there is currently a prevalence of underscreening, underdiagnosis and undertreatment of osteoporosis in men.
Although no clear mechanism of the relationship between hemoglobin levels and osteoporosis has been established, there are several possible explanations. First, on the one hand, relative hypoxia caused by decreased hemoglobin may increase the differentiation and activity of osteoclasts by increasing the expression of hypoxia-inducible factors and osteoclast-specific factors and the formation of extracellular acidic environment, resulting in increased bone resorption29,30,34–37 On the other hand, the effects of hypoxia on osteoblasts, including inhibition of proliferation and differentiation and alteration of bone mineralization, suppress bone formation.38 Second, we learned that the interaction between bone cells and hematopoietic cells has been observed in animal models.39 Blood loss stimulates the proliferation of hematopoietic cells, including osteoclasts, leading to increased bone resorption.40 Third, some have postulated that low hemoglobin levels are a reflection of poor general health, rather than a direct risk factor.41 Low hemoglobin levels share many risk factors with osteoporosis, such as chronic inflammation, renal insufficiency, and nutrient deficiencies.42 T2DM can not only lead to osteoporosis through its associated obesity, microvascular complications and accumulation of advanced glycation end products, but also indirectly through anemia caused by impaired erythropoietin production in peritubular fibroblasts.6,9
Bone loss in T2DM patients occurs invisibly and is initially asymptomatic. Osteoporosis is usually not diagnosed until the first clinical fracture has occurred. Therefore, early assessment of osteoporosis risk in T2DM patients is important to prevent fractures. Further study on the relationship between bone metabolism and hemoglobin levels and its possible mechanisms may be of great clinical significance, as measuring hemoglobin levels would be a simple and inexpensive way to assess bone health.
The study had several limitations. First, it was a cross-sectional study, the causal relationship between hemoglobin levels and osteoporosis could not be determined, and there is a need for prospective studies. Second, although some confounding factors were adjusted in the regression model, but possible confounders (such as dietary habit, physical activity, antidiabetic drugs and diabetic complications) were not considered in this study. Third, the majority of patients with anemia excluded common causes of anemia such as thalassemia, iron deficiency anemia, folic acid and vitamin B12 deficiency, but failed to complete all tests for anemia-related causes.
Conclusion
In summary, our study suggested that lower hemoglobin levels were related to higher percentages of osteoporosis in T2DM men, especially in those aged 50 years and older. Regular monitor of serum hemoglobin and BMD may be necessary in T2DM men aged 50 years and older. Since fractures can occur at higher BMD levels in T2DM patients, further studies are warranted to directly evaluate the relationship between hemoglobin levels and osteoporotic fractures in T2DM patients.
Acknowledgments
The authors gratefully appreciated the team of the Department of Geriatric Endocrinology and Metabolism of The First Affiliated Hospital of Guangxi Medical University for their work in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
2. Cole JB, Florez JC. Genetics of diabetes mellitus and diabetes complications. Nat Rev Nephrol. 2020;16(7):377–390. doi:10.1038/s41581-020-0278-5
3. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl1):S15–S33. doi:10.2337/dc21-s002
4. Zeng Q, Li N, Wang Q, et al. The prevalence of osteoporosis in China, a nationwide, multicenter DXA survey. J Bone Miner Res. 2019;34(10):1789–1797. doi:10.1002/jbmr.3757
5. Lecka-Czernik B. Diabetes, bone and glucose-lowering agents: basic biology. Diabetologia. 2017;60(7):1163–1169. doi:10.1007/s00125-017-4269-4
6. Compston J. Type 2 diabetes mellitus and bone. J Intern Med. 2018;283(2):140–153. doi:10.1111/joim.12725
7. Tebé C, Martínez-Laguna D, Carbonell-Abella C, et al. The association between type 2 diabetes mellitus, Hip fracture, and post-Hip fracture mortality: a multi-state cohort analysis. Osteoporos Int. 2019;30(12):2407–2415. doi:10.1007/s00198-019-05122-3
8. Sahay M, Kalra S, Badani R, et al. Diabetes and anemia: International Diabetes Federation (IDF) - Southeast Asian Region (SEAR) position statement. Diabetes Metab Syndr. 2017;11(Suppl 2):S685–S695. doi:10.1016/j.dsx.2017.04.026
9. Singh DK, Winocour P, Farrington K. Erythropoietic stress and anemia in diabetes mellitus. Nat Rev Endocrinol. 2009;5(4):204–210. doi:10.1038/nrendo.2009.17
10. Bo L, Liu Z, Zhong Y, et al. Iron deficiency anemia’s effect on bone formation in zebrafish mutant. Biochem Biophys Res Commun. 2016;475(3):271–276. doi:10.1016/j.bbrc.2016.05.069
11. Kolomansky A, Hiram-Bab S, Ben-Califa N, et al. Erythropoietin mediated bone loss in mice is dose-dependent and mostly irreversible. Int J Mol Sci. 2020;21(11):E3817.
12. Kos O, Alexander C, Brandenburg K, et al. Regulation of fetal hemoglobin expression during hematopoietic stem cell development and its importance in bone metabolism and osteoporosis. Int Immunopharmacol. 2018;57:112–120.
13. Eskiocak Ö, Yılmaz MÖ, Ilhan G. Metabolic bone diseases in sickle cell anemia patients and evaluation of associated factors. Am J Med Sci. 2022;363(6):490–494.
14. Shi L, Lin CL, Su CH, et al. The risk of developing osteoporosis in hemolytic anemia-what aggravates the bone loss? J Clin Med. 2021;10(15):3364. doi:10.3390/jcm10153364
15. Kharroubi A, Karmi B, Shamasneh W, et al. Bone mineral density among Palestinian patients suffering from hemoglobinopathy disorders. Arch Osteoporos. 2020;15(1):181. doi:10.1007/s11657-020-00853-x
16. Valderrábano RJ, Lui LY, Lee J, et al. Bone density loss is associated with blood cell counts. J Bone Miner Res. 2017;32(2):212–220. doi:10.1002/jbmr.3000
17. Liang X, Du Y, Wen Y, et al. Assessing the genetic correlations between blood plasma proteins and osteoporosis: a polygenic risk score analysis. Calcif Tissue Int. 2019;104(2):171–181. doi:10.1007/s00223-018-0483-4
18. Hannemann A, Nauck M, Völzke H, et al. Interactions of anemia, FGF-23, and bone in healthy adults-results from the Study of Health in Pomerania (SHIP). J Clin Endocrinol Metab. 2021;106(1):e288–e299. doi:10.1210/clinem/dgaa716
19. Kim HS, Park HM, Lee HS, et al. Hemoglobin levels and low bone mineral density in non-anemic older adults: secondary analysis of the Korean National Health and Nutrition Examination Survey. Exp Gerontol. 2019;126:110706. doi:10.1016/j.exger.2019.110706
20. Laudisio A, Marzetti E, Pagano F, et al. Haemoglobin levels are associated with bone mineral density in the elderly: a population-based study. Clin Rheumatol. 2009;28(2):145–151. doi:10.1007/s10067-008-0998-6
21. Valderrábano RJ, Buzkova P, Chang PY, et al. Association of bone mineral density with hemoglobin and change in hemoglobin among older men and women: the cardiovascular health study. Bone. 2019;120:321–326. doi:10.1016/j.bone.2018.11.010
22. Chamberlain JJ, Rhinehart AS, Shaefer CF, et al. Diagnosis and management of diabetes: synopsis of the 2016 American Diabetes Association Standards of medical care in diabetes. Ann Intern Med. 2016;164(8):542–552. doi:10.7326/m15-3016
23. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
24. World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. In: Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization; 2011.
25. Genant HK, Cooper C, Poor G, et al. Interim report and recommendations of the World Health Organization task-force for osteoporosis. Osteoporos Int. 1999;10(4):259–264. doi:10.1007/s001980050224
26. Adane T, Getawa S. Anaemia and its associated factors among diabetes mellitus patients in Ethiopia: a systematic review and meta-analysis. Endocrinol Diabetes Metab. 2021;4(3):e00260. doi:10.1002/edm2.260
27. Paschou SA, Dede AD, Anagnostis PG, et al. Type 2 diabetes and osteoporosis: a guide to optimal management. J Clin Endocrinol Metab. 2017;102(10):3621–3634. doi:10.1210/jc.2017-00042
28. Shen J, Nielson CM, Marshall LM, et al. The association between BMI and QCT-derived proximal hip structure and strength in older men: a cross-sectional study. J Bone Miner Res. 2015;30(7):1301–1308. doi:10.1002/jbmr.2450
29. Korkmaz U, Korkmaz N, Yazici S, et al. Anemia as a risk factor for low bone mineral density in postmenopausal Turkish women. Eur J Intern Med. 2012;23(2):154–158. doi:10.1016/j.ejim.2011.11.009
30. Chuang MH, Chuang TL, Koo M, et al. Low hemoglobin is associated with low bone mineral density and high risk of bone fracture in male adults: a retrospective medical record review study. Am J Mens Health. 2019;13(3):1557988319850378. doi:10.1177/1557988319850378
31. Looker AC. Hemoglobin and Hip fracture risk in older non-Hispanic white adults. Osteoporos Int. 2014;25(10):2389–2398. doi:10.1007/s00198-014-2769-3
32. Cui R, Zhao Z, Fei Z, et al. Anemia is related to osteoporosis in Chinese type 2 diabetic patients. Arch Osteoporos. 2021;16(1):161. doi:10.1007/s11657-021-01030-4
33. Rinonapoli G, Ruggiero C, Meccariello L, et al. Osteoporosis in men: a review of an underestimated bone condition. Int J Mol Sci. 2021;22(4):2105. doi:10.3390/ijms22042105
34. Sun KT, Chen MYC, Tu MG, et al. MicroRNA-20a regulates autophagy related protein-ATG16L1 in hypoxia-induced osteoclast differentiation. Bone. 2015;73:145–153. doi:10.1016/j.bone.2014.11.026
35. Yu X, Jiang H, Cheng G, et al. High levels of HIF-1ɑ in hypoxic dental pulps associated with teeth with severe periodontitis. J Mol Histol. 2020;51(3):265–275. doi:10.1007/s10735-020-09878-5
36. Arnett TR, Gibbons DC, Utting JC, et al. Hypoxia is a major stimulator of osteoclast formation and bone resorption. J Cell Physiol. 2003;196(1):2–8. doi:10.1002/jcp.10321
37. Dimai HP, Domej W, Leb G, et al. Bone loss in patients with untreated chronic obstructive pulmonary disease is mediated by an increase in bone resorption associated with hypercapnia. J Bone Miner Res. 2001;16(11):2132–2141. doi:10.1359/jbmr.2001.16.11.2132
38. Tan JK, Mohamad Hazir NS, Alias E. Impacts of hypoxia on osteoclast formation and activity: systematic review. Int J Mol Sci. 2021;22(18):10146. doi:10.3390/ijms221810146
39. Panaroni C, Tzeng YS, Saeed H, et al. Mesenchymal progenitors and the osteoblast lineage in bone marrow hematopoietic niches. Curr Osteoporos Rep. 2014;12(1):22–32.
40. Gurevitch O, Slavin S. The hematological etiology of osteoporosis. Med Hypotheses. 2006;67(4):729–735.
41. Merchant AA, Roy CN. Not so benign haematology: anaemia of the elderly. Br J Haematol. 2012;156(2):173–185.
42. Chaparro CM, Suchdev PS. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann N Y Acad Sci. 2019;1450(1):15–31. doi:10.1111/nyas.14092
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors for Nonalcoholic Fatty Liver Disease in Postmenopausal Women with Type 2 Diabetes Mellitus and the Correlation with Bone Mineral Density at Different Locations
Du YJ, Liu NN, Zhong X, Pan TR
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1925-1934
Published Date: 21 June 2022
Clinical Utility of Romosozumab in the Management of Osteoporosis: Focus on Patient Selection and Perspectives
Lim SY, Bolster MB
International Journal of Women's Health 2022, 14:1733-1747
Published Date: 15 December 2022
Association Between Coronary Artery Calcium Score and Bone Mineral Density in Type 2 Diabetes Mellitus with Different Visceral Fat Area
Yang Y, Li L, Zhang Y, Yang H, Bai J, Lv H, Fu S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3949-3960
Published Date: 16 December 2022
The Effects of Switching from Dipeptidyl Peptidase-4 Inhibitors to Glucagon-Like Peptide-1 Receptor Agonists on Bone Mineral Density in Diabetic Patients
Huang CF, Mao TY, Hwang SJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:31-36
Published Date: 11 January 2023
The Relationship Between Serum 25-Hydroxyvitamin D Levels and Osteoporosis in Postmenopausal Women
Wang D, Yang Y
Clinical Interventions in Aging 2023, 18:619-627
Published Date: 18 April 2023