")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Effects of Switching from Dipeptidyl Peptidase-4 Inhibitors to Glucagon-Like Peptide-1 Receptor Agonists on Bone Mineral Density in Diabetic Patients
Authors Huang CF , Mao TY, Hwang SJ
Received 15 September 2022
Accepted for publication 22 December 2022
Published 11 January 2023 Volume 2023:16 Pages 31—36
DOI https://doi.org/10.2147/DMSO.S389964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Chun-Feng Huang,1– 3 Tso-Yen Mao,3 Shinn-Jang Hwang1,2
1Division of Family Medicine, En Chu Kong Hospital, New Taipei City, Taiwan, Republic of China; 2Faculty of Medicine, School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan, Republic of China; 3Department of Leisure Services Management, Chaoyang University of Technology, Taichung, Taiwan, Republic of China
Correspondence: Tso-Yen Mao, Department of Leisure Services Management, Chaoyang University of Technology, 168, Jifeng E. Road, Wufeng District, 413, Taichung, Taiwan, Republic of China, Tel +886 4 23323000 #7453, Fax +886 4 23742363, Email [email protected] Shinn-Jang Hwang, En Chu Kong Hospital, 399, Fuxing Road, Sanxia District, 237, New Taipei City, Taiwan, Republic of China, Tel +886 2 26723456, Fax +886 2 2671-9537, Email [email protected]
Purpose: Diabetes increases the risk of fragility fractures. As a result, when choosing a diabetes treatment, whether the drug affects bone density should be taken into account. The goal of this study was to determine how switching from dipeptidyl peptidase-4 inhibitors (DPP-4i) to glucagon-like peptide-1 receptor agonists (GLP-1RA) influenced bone mineral density (BMD) in diabetic patients.
Patients and Methods: In this retrospective cohort study, diabetic patients with osteoporosis or osteopenia who used DPP-4i but not anti-osteoporosis medications were divided into two groups: those who switched to GLP-1RA (n = 132) and those who did not (control group, n = 133). We compared changes in glycemic control and BMD with and without conversion from DPP-4i to GLP-1RA.
Results: Prior to switching, there was no difference between the groups in terms of age, gender, glycosylated hemoglobin (HbA1c), or BMD. HbA1c was 8.7% in the participants (mean age 62.7 years, 17.4% female). Despite the fact that there was no difference in femoral neck BMD, the GLP-1RA group had a greater decrease in lumbar spine BMD (− 0.028 g/cm2 versus − 0.019 g/cm2, p = 0.041) than the control group. Furthermore, HbA1c levels in the GLP-1RA-treated group were considerably lower than in the control group (7.5% versus 8.0%, p = 0.027).
Conclusion: While switching to GLP-1RA improves glycemic control, it appears to have a less favorable effect on bone density than continuing DPP-4i. More research is needed, however, to determine whether diabetic patients with low bone density should be switched from DPP-4i to GLP-1RA.
Keywords: bone mineral density, diabetes, dipeptidyl peptidase-4 inhibitor, glucagon-like peptide-1 receptor agonist, osteoporosis
Introduction
Type 2 diabetes mellitus (T2DM) and osteoporosis are chronic metabolic disorders that cause significant morbidity, increased mortality, and higher health-care expenses.1,2 As a result of the general population’s aging, both are soon becoming global epidemics. Although osteoporosis and type 2 diabetes are commonly thought to be separate diseases, mounting evidence suggests that they may be linked by common pathophysiological processes such as insulin resistance, hyperglycemia, oxidative stress, the release of inflammatory agents from visceral fat, and increased bone marrow adiposity.3 Furthermore, fragility fractures caused by diminished bone strength are becoming more well recognized as diabetes-related skeletal disorders. As a result, the potential function of T2DM therapy drugs in abnormal bone metabolism has received a lot of attention recently.4,5
Intestinal hormones enhance glucose absorption by stimulating pancreatic insulin production.6 The finding that enteral feeding triggered a higher insulin secretion response than intravenous sugar infusion supported the existence of incretins as insulin-inducing elements stimulated by dietary glucose. The two principal incretin hormones produced from the intestine in response to glucose or nutrient ingestion are gastric inhibitory polypeptide (GIP) and glucagon-like peptide-1 (GLP-1). These hormones may stimulate insulin production from pancreatic cells. However, both endogenous and exogenous GLP-1 and GIP have limited pharmacologic effects due to their short plasma half-life, as they are rapidly degraded and inactivated by dipeptidyl peptidase-4 (DPP-4), which is widely expressed on cell surfaces and present in the circulation.7
GLP-1 binds to the GLP-1 receptor, increasing insulin synthesis and secretion while suppressing appetite.8 GLP-1 receptor agonists (GLP-1 RA) are peptide analogs of exendin-4 or human GLP-1 that are designed to resist DPP-4 activity and hence have a longer half-life.9 GLP-1RA are widely used as glucose-dependent glucose-lowering treatment in type 2 diabetes. Because the GLP receptor is expressed in osteoblasts, GLP-1RAs may affect bone mineral density (BMD).10 GLP-1RA would improve bone metabolism by enhancing osteoblast proliferation and differentiation while decreasing advanced glycation end products accumulation.11 Although a previous study found that GLP-1RA may benefit BMD, other meta-analyses have found that GLP-1RA does not reduce fractures.12
DPP4 inhibitors (DPP-4i) limit DPP-4 enzymatic activity, hence blocking the breakdown of incretins (GLP-1 and GIP) that trigger insulin release as a means of controlling blood glucose levels.13 DPP-4i may have similar effects on bone as GLP-1RA since it prolongs the effects of GLP-1 by preventing DPP-4 incretin inactivation. As a result, DPP-4i has the potential to improve bone density, bone quality, and bone turnover markers. Furthermore, when compared to other diabetic drugs, DPP-4i is associated with a lower risk of fracture in diabetic patients, according to various studies.14,15
Despite the fact that GLP-1RA is more effective than DPP-4i at lowering blood glucose in persons with poorly managed diabetes, no research has been done to see if the switch affects patients’ BMD. The goal of this study was to see if, rather than focusing solely on good or bad blood glucose control, the effect on BMD of switching to GLP-1RA in diabetic patients who had previously used DPP-4i should be taken into account.
Materials and Methods
Study Design
In this investigation, a retrospective matched-cohort analysis was performed. We retrieved 2218 diabetic patients with concurrent osteoporosis or osteopenia [T-score < −1 by dual-energy X-ray absorptiometry (DXA) (Prodigy; GE Medical Systems Lunar, Madison, WI, USA)] from a patient database at a regional hospital in Yilan County, Taiwan, who were treated with DPP-4i for at least one year between May 2013 and April 2020. After excluding patients taking anti-osteoporosis or alfacalcidol medications (which improve bone mass), hormones (eg, thyroxin facilitates bone turnover), insulin (which increases sugar fluctuation), proton pump inhibitors (which suppress calcium resorption), and antiepileptic drugs (which disrupt vitamin D metabolism), 132 patients (study group) who switched from oral DPP-4i (sitagliptin, linagliptin, and vildagliptin) to GLP-1RA (liraglutide and dulaglutide) injection were matched to 133 patients (control group) who were regularly taking DPP-4i based on age, body mass index (BMI), and glycosylated hemoglobin (HbA1c). DXA was used to assess the study group twice, with the second measurement taking place at least one year following the switch. In addition, the control group underwent two DXA scans (at least two years apart).
Except for the conversion of DPP-4i to GLP-1RA, no other additions or deletions to the individual’s prescription of oral diabetes medications occurred between DXA exams in our chosen patients (In Taiwan, sodium-glucose cotransporter 2 inhibitors cannot be combined with DPP-4i or GLP-1RA due to health insurance reimbursement restrictions). The variations in BMD and HbA1c between the study and control groups were then compared. Figure 1 depicts the research design as well as the data gathering process that was used.
 |
Figure 1 Flow chart for study subject selection. Abbreviations: DPP-4i, dipeptidyl peptidase-4 inhibitors; DXA, dual-energy X-ray absorptiometry; GLP-1RA, glucagon-like peptide-1 receptor agonists. |
Ethics
This study was approved by the Institutional Review Board (IRB) of the National Yang-Ming University Hospital (YMUH2020A023) in accordance with the Declaration of Helsinki. The study involves no prospectively collected data so there is no access to patients or opportunity to seek informed consent. A waiver of consent was approved by IRB as re-contacting this number of patients to obtain informed consent would be impracticable. The study is no greater than minimal risk and will have no direct impact on patient’s rights and clinical care. Finally, we guarantee the confidentiality of all patient data.
Statistical Analysis
Descriptive statistics were used to summarize the basic characteristics. IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, N.Y., USA) was used to conduct formal statistical studies. Differences between means were tested by independent-samples t-test using Levene’s test for equality of variances. The paired t-test was used to determine whether the variables differed before and after the switch. Furthermore, an analysis of covariance (ANCOVA) adjusted for confounding factors was used to investigate the relationship between switching from DPP4-i to GLP-1RA and BMD in the control and study groups. The minimum total sample size in this study is 88, with at least 44 subjects for each independent variable, for an effect size of d = 0.5, power = 0.8, and α = 0.05.
Results
When the baseline parameters of the patients were compared, such as gender, age, weight, HbA1c, BMD, and other biochemical markers, there were no statistically significant differences between the study and control groups, as shown in Table 1.
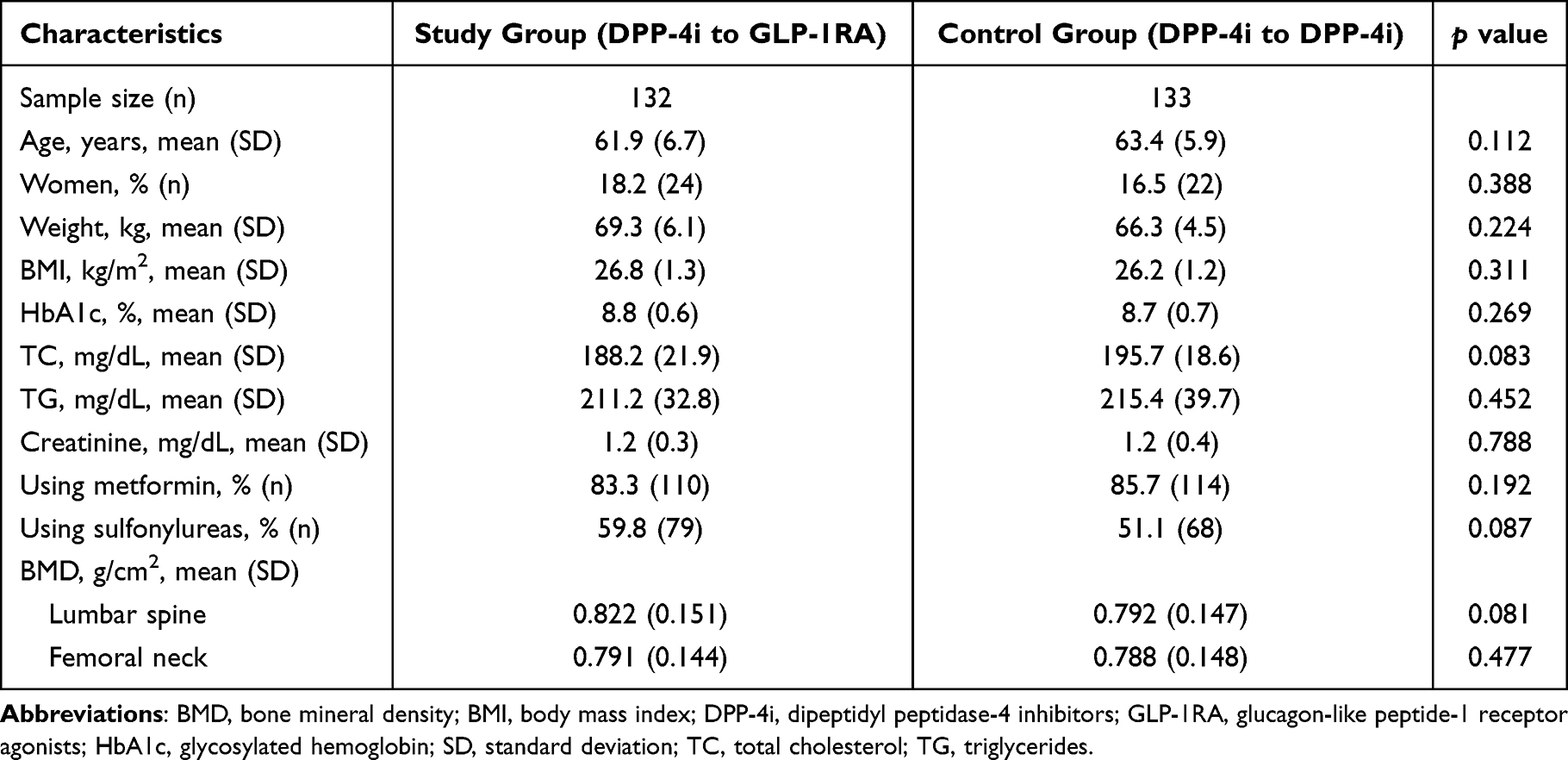 |
Table 1 Baseline Characteristics of Subjects |
The duration between two DXA tests in the GLP-1RA group was 3 ± 0.4 years and 3.3 ± 0.6 years in the control group. The average transition time from DPP4-I to GLP-1RA was 1.8 ± 0.3 years. When compared to baseline, the GLP-1RA group had a decrease in lumbar spine BMD but not in femoral neck BMD. The BMD of the lumbar spine and femoral neck, on the other hand, did not change appreciably in the control group (Table 2). Notably, while the body weight of the GLP-1RA group decreased significantly compared to the baseline (−2.25 ± 0.68 kg, p = 0.012) but not the control group (−0.81 ± 0.56 kg, p = 0.168), the ANCOVA analysis with age and BMI adjustment still discovered that the lumbar spine BMD decreased significantly in the GLP-1RA group. Furthermore, when compared to baseline, HbA1c declined substantially in both the GLP-1RA and control groups, though the reduction was more pronounced in the GLP-1RA group (Table 2).
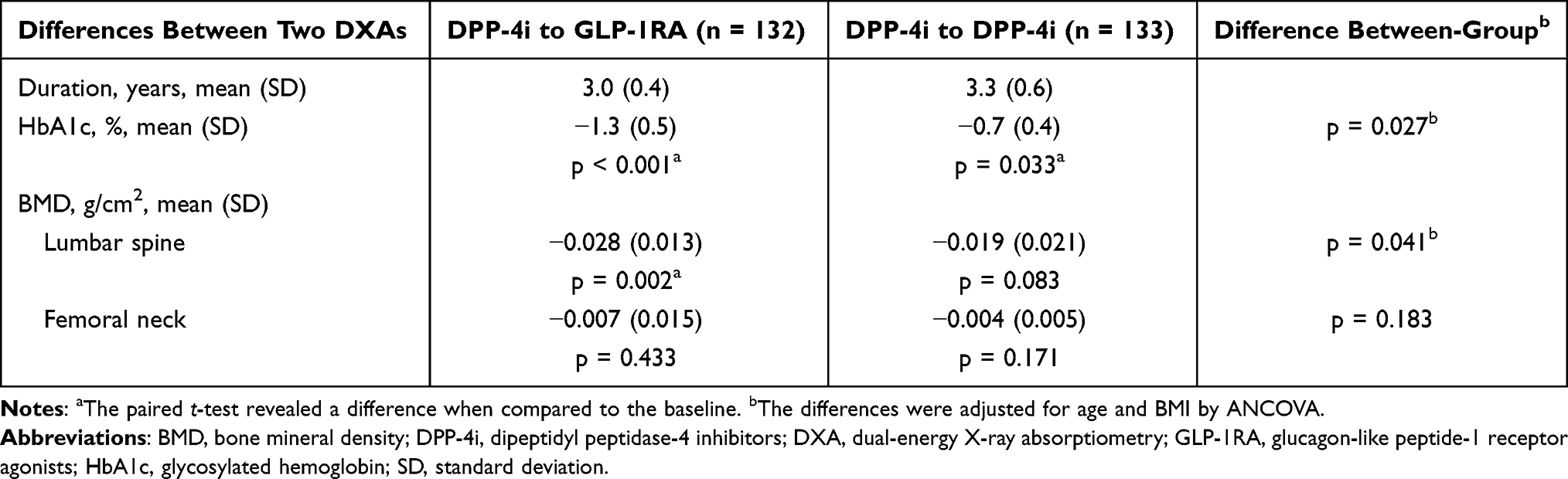 |
Table 2 Clinical Data Comparison with and without Switching from DPP-4i to GLP-1RA |
Discussion
The study discovered that switching from DPP-4i to GLP-1RA reduced lumbar spinal bone density in diabetics with untreated osteoporosis or osteopenia.
Previous study has discovered that diabetes-related hyperglycemia or insulin insufficiency may contribute to a deterioration in bone quality.3 The imbalance of the advanced glycation end product accumulation axis directly affects osteoblast activity by lowering their numbers and function.16 Furthermore, hyperglycemia impairs bone quality by interfering with osteocalcin production and the Wnt signaling pathways through an imbalance in osteoblast/osteoclast activity. However, switching from DPP-4i to GLP-1RA improved blood sugar control but had no discernible effect on BMD in our study. Blood glucose control may not be a determinant in BMD changes.
Among the hypoglycemic medications currently available are biguanides, sulfonylureas, thiazolidinediones, GLP-1RA, DPP-4i, and insulin, which may have varying effects on BMD.4 Metformin did not affect bone density in a clinical trial, and sulfonylureas had no effect on bone metabolism or BMD in a meta-analysis. Thiazolidinediones, on the other hand, have been linked to bone loss. Previous research has discovered that both DPP-4i and GLP-1RA have bone-protective properties, but the effect of GLP-1RA on fracture prevention is debatable.12 Our findings suggest that GLP-1RA have a better effect on blood sugar control than DPP-4i, but they may increase the consequences of bone fragility after switching from DPP-4i, resulting in a significant BMD decrease in lumbar spine. Trabecular bone dominates the lumbar spine, while cortical bone dominates the femoral neck. Trabecular bone is more vulnerable to pharmacological effects than cortical bone because it has a faster rate of bone turnover.
GLP-1RA has previously been shown to protect against bone mineral content loss and increase levels of bone formation indicators (procollagen type 1 N-terminal peptide and osteocalcin).17 GLP-1RA may stimulate osteogenic differentiation of bone marrow stromal cells by regulating β-catenin signal transduction and increasing the expression of osteoprotegerin genes, thereby influencing nuclear factor-κB ligand-receptor activator to reverse bone mass loss and boost bone formation. Furthermore, the GLP-1 receptor is present on the surface of osteocytes, where it inhibits the synthesis of sclerostin, a protein known to limit osteoblastic activity while increasing catabolic activity on bone. GLP-1 receptors are also located on the surface of thyroid C cells, where they increase calcitonin, reducing osteoclast activity and preventing calcium from being released into the bloodstream. Our study, on the other hand, discovered that GLP-1RA impacts both body weight and lumbar spine BMD at the same time. Because bone loss is commonly associated with weight loss, GLP-1RA’s positive effect on bone density may be partially reversed.18
DPP-4i has the potential to enhance serum 25 (OH)-D levels, which could lead to an increase in bone mass.19 Furthermore, because adiponectin inhibits pre-osteoclast development and decreases osteoclastic bone resorption, DPP-4i may promote bone formation while inhibiting bone resorption inhibition by reducing the drop in adiponectin receptor expression in diabetics. GIP receptor activation upon GIP binding can increase intracellular Ca2+ and cAMP concentrations, as well as alkaline phosphatase activity and type I collagen mRNA expression in osteoblasts.20 DPP-4i, in addition to inhibiting GLP-1 degradation by selectively cleaving alanine and proline, can also inhibit GIP degradation, suggesting that it may have a stronger potential to prevent bone fragility.13 In this study, the average duration of DPP-4i use in the control group was 3.3 years. Even though aging is the most significant risk factor for bone loss, there was no significant reduction in BMD in the control group, demonstrating DPP-4i’s potential benefit on bone.
For the first time, the research suggests that while switching to GLP-1RA improves glycemic control, it appears to have a less favorable effect on bone density than continuing DPP-4i. However, this retrospective cohort study has some limitations, including the fact that it recruited more men and that postmenopausal women are often the primary population affected by osteoporosis. It is unknown whether switching from DPP-4i to GLP-1RA is associated with an increase in spinal fragility fractures, even in patients with lower BMD. Furthermore, Clinicians may have switched therapy for a presumably medically motivated reason related to bone density. Also, GLP-1RA are only considered as a valid alternative for patients in generally worse health conditions. In addition, the inability to provide information on comorbidity status and other drug use associated with osteoporosis, including proportion and subgroups analysis, is a potential confounding factor. Finally, the study was limited to a single hospital, the sample size was small, and it used a retrospective observational design, making it difficult to confirm causality.
Conclusion
The study first demonstrates that prescription changes in diabetes may influence BMD in specific bones. Aside from blood sugar control, patients switching from DPP-4i to GLP-1RA should be aware of the less favorable effect on BMD in the lumbar spine, and clinicians should regularly assess bone quality change in these patients.
Acknowledgments
The authors thank the Department of Information Management at National Yang Ming Chiao Tung University Hospital in Yilan for collecting clinical data and providing administrative support, as well as Dr. Po-Wen Hsu for sparking the idea for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
2. Clynes MA, Harvey NC, Curtis EM, Fuggle NR, Dennison EM, Cooper C. The epidemiology of osteoporosis. Br Med Bull. 2020;133(1):105–117. doi:10.1093/bmb/ldaa005
3. Wang J, You W, Jing Z, Wang R, Fu Z, Wang Y. Increased risk of vertebral fracture in patients with diabetes: a meta-analysis of cohort studies. Int Orthop. 2016;40(6):1299–1307. doi:10.1007/s00264-016-3146-y
4. Gilbert MP, Pratley RE. The impact of diabetes and diabetes medications on bone health. Endocr Rev. 2015;36(2):194–213. doi:10.1210/er.2012-1042
5. Zhang YS, Zheng YD, Yuan Y, Chen SC, Xie BC. Effects of anti-diabetic drugs on fracture risk: a systematic review and network meta-analysis. Front Endocrinol. 2021;12:735824. doi:10.3389/fendo.2021.735824
6. Rosenberg J, Jacob J, Desai P, Park J, Donovan L, Kim JY. Incretin hormones: pathophysiological risk factors and potential targets for type 2 diabetes. J Obes Metab Syndr. 2021;30(3):233–247. doi:10.7570/jomes21053
7. Meier JJ, Nauck MA, Kranz D, et al. Secretion, degradation, and elimination of glucagon-like peptide 1 and gastric inhibitory polypeptide in patients with chronic renal insufficiency and healthy control subjects. Diabetes. 2004;53(3):654–662. doi:10.2337/diabetes.53.3.654
8. Gutzwiller JP, Drewe J, Göke B, et al. Glucagon-like peptide-1 promotes satiety and reduces food intake in patients with diabetes mellitus type 2. Am J Physiol. 1999;276(5):R1541–R1544. doi:10.1152/ajpregu.1999.276.5.R1541
9. Meier JJ. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat Rev Endocrinol. 2012;8(12):728–742. doi:10.1038/nrendo.2012.140
10. Pacheco-Pantoja EL, Ranganath LR, Gallagher JA, Wilson PJ, Fraser WD. Receptors and effects of gut hormones in three osteoblastic cell lines. BMC Physiol. 2011;11:12. doi:10.1186/1472-6793-11-12
11. Odawara M, Miyagawa J, Iwamoto N, Takita Y, Imaoka T, Takamura T. Once-weekly glucagon-like peptide-1 receptor agonist dulaglutide significantly decreases glycated haemoglobin compared with once-daily liraglutide in Japanese patients with type 2 diabetes: 52 weeks of treatment in a randomized Phase III study. Diabetes Obes Metab. 2016;18(3):249–257. doi:10.1111/dom.12602
12. Su B, Sheng H, Zhang M, et al. Risk of bone fractures associated with glucagon-like peptide-1 receptor agonists’ treatment: a meta-analysis of randomized controlled trials. Endocrine. 2015;48(1):107–115. doi:10.1007/s12020-014-0361-4
13. Demuth HU, McIntosh CH, Pederson RA. Type 2 diabetes--therapy with dipeptidyl peptidase IV inhibitors. Biochim Biophys Acta. 2005;1751(1):33–44. doi:10.1016/j.bbapap.2005.05.010
14. Dombrowski S, Kostev K, Jacob L. Use of dipeptidyl peptidase-4 inhibitors and risk of bone fracture in patients with type 2 diabetes in Germany-A retrospective analysis of real-world data. Osteoporos Int. 2017;28(8):2421–2428. doi:10.1007/s00198-017-4051-y
15. Yang J, Huang C, Wu S, et al. The effects of dipeptidyl peptidase-4 inhibitors on bone fracture among patients with type 2 diabetes mellitus: a network meta-analysis of randomized controlled trials. PLoS One. 2017;12(12):e0187537. doi:10.1371/journal.pone.0187537
16. Yamamoto M, Sugimoto T. Advanced glycation end products, diabetes, and bone strength. Curr Osteoporos Rep. 2016;14(6):320–326. doi:10.1007/s11914-016-0332-1
17. Iepsen EW, Lundgren JR, Hartmann B, et al. GLP-1 receptor agonist treatment increases bone formation and prevents bone loss in weight-reduced obese women. J Clin Endocrinol Metab. 2015;100(8):2909–2917. doi:10.1210/jc.2015-1176
18. Shapses SA, Riedt CS. Bone, body weight, and weight reduction: what are the concerns? J Nutr. 2006;136(6):1453–1456. doi:10.1093/jn/136.6.1453
19. Barchetta I, Cimini FA, Bloise D, Cavallo MG. Dipeptidyl peptidase-4 inhibitors and bone metabolism: is vitamin D the link? Acta Diabetol. 2016;53(5):839–844. doi:10.1007/s00592-016-0882-9
20. Bollag RJ, Zhong Q, Phillips P, et al. Osteoblast-derived cells express functional glucose-dependent insulinotropic peptide receptors. Endocrinology. 2000;141(3):1228–1235. doi:10.1210/endo.141.3.7366
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.