Back to Journals » Clinical Interventions in Aging » Volume 21
SPISE Index (Single-Point Insulin Sensitivity Estimator): A Long-Term Predictor of Recurrence in Elderly Patients with Atrial Fibrillation After Radiofrequency Ablation
Authors Wang Z ![]() , Qu Y, Wang H, Liu X
, Qu Y, Wang H, Liu X
Received 17 March 2026
Accepted for publication 2 June 2026
Published 12 June 2026 Volume 2026:21 608687
DOI https://doi.org/10.2147/CIA.S608687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Zhen Wang,1,* Yilin Qu,2,* Hua Wang,1,* Xiao Liu1,*
1Cardiology Department, Yantai Yuhuangding Hospital, Affiliated with Qingdao University, Yantai, People’s Republic of China; 2Medical Record Information Department, Yantai Yuhuangding Hospital, Affiliated with Qingdao University, Yantai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao Liu, Email [email protected]
Background: Insulin resistance (IR) plays a significant role in the onset and progression of atrial fibrillation (AF). The single-point insulin sensitivity estimator (SPISE) index is a novel marker for assessing IR. This study aims to investigate the association between the SPISE index and the recurrence of AF following radiofrequency ablation (RFA) in elderly patients.
Methods: A total of 529 elderly patients (aged 65 and above) with AF who underwent RFA treatment were included in the study. The Cox proportional hazards model was employed to assess the association between the SPISE index and AF recurrence after RFA. Within this framework, a restricted cubic spline (RCS) was used to evaluate the nonlinear relationship between SPISE index and AF recurrence. Kaplan-Meier survival analysis was conducted to compare AF recurrence rates among different groups. Additionally, subgroup analyses were performed to assess the heterogeneity of these effects. Receiver operating characteristic (ROC) curve analysis was employed to evaluate the predictive value of the SPISE index for AF recurrence.
Results: After follow-up, a total of 175 patients (33.1%) experienced recurrence. In the fully adjusted Cox proportional hazards model, SPISE index was significantly associated with AF recurrence (HR = 0.661, P < 0.001). The RCS analysis indicated a negative, nonlinear relationship between the SPISE index and the recurrence of AF. In the subgroups defined by early recurrence, AF type, gender, hypertension, diabetes, and coronary heart disease, the association between the SPISE index and AF recurrence remained consistent. Kaplan-Meier survival analysis revealed significant differences in recurrence rates among patients with varying SPISE index levels. Specifically, a higher SPISE index was associated with a lower cumulative incidence of AF recurrence.
Conclusion: A higher SPISE index is associated with a reduced risk of recurrence after RFA in elderly patients with AF.
Keywords: SPISE index, atrial fibrillation, radiofrequency ablation, recurrence
Introduction
The 2019 Global Burden of Disease Study revealed that approximately 59.7 million people worldwide had atrial fibrillation (AF), representing a significant increase compared to data from before 2010.1 The prevalence and incidence of AF gradually increase with age, with higher rates observed in men than in women across all age groups.2 The results of the cross-sectional survey indicated that, after adjusting for age, the prevalence of AF was 0.74% in men and 0.72% in women. Among individuals over 60 years old, the prevalence rates were 1.83% for men and 1.92% for women, respectively.3 Whether it is paroxysmal or persistent AF, radiofrequency ablation (RFA) is recommended as the preferred treatment option.4 However, the recurrence rate after RFA remains relatively high, with approximately 30% to 40% of patients experiencing AF recurrence following the initial ablation procedure.5
Insulin resistance (IR) is a pathological condition characterized by a diminished response to insulin. It is a significant precursor to diabetes, hypertension, metabolic syndrome, and cardiovascular metabolic risks. Previous studies have demonstrated that alternative markers of IR can predict the recurrence of AF after ablation.6,7 The single-point insulin sensitivity estimator (SPISE) index has recently been introduced as an alternative marker for assessing IR. It incorporates triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and body mass index (BMI). SPISE index is negatively correlated with IR and outperforms existing indicators, such as the homeostasis model assessment of insulin resistance (HOMA-IR) and the TG/HDL-C ratio, in predicting metabolic outcomes.8,9 Studies have shown that a higher SPISE index is associated with a reduced risk of cardiovascular disease in middle-aged and elderly individuals, highlighting its value as a tool for assessing cardiovascular disease risk.10 To date, research on the SPISE index has primarily focused on metabolic syndrome, non-alcoholic fatty liver disease, and diabetes. However, there are few studies examining the relationship between the SPISE index and AF recurrence. Therefore, this study aims to investigate the association between the SPISE index and AF recurrence.
Materials and Methods
Study Population
This study included 529 elderly patients with AF. All patients underwent RFA treatment at Yantai Yuhuangding Hospital, affiliated with Qingdao University, from December 2020 to December 2025. The diagnosis and classification of AF were conducted in accordance with the 2024 European Society of Cardiology (ESC) guidelines.4 The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of Yantai Yuhuangding Hospital, affiliated with Qingdao University (No. K2026-155). All patients signed informed consent forms. All personal information has been encrypted. The research flowchart is shown in Figure 1.
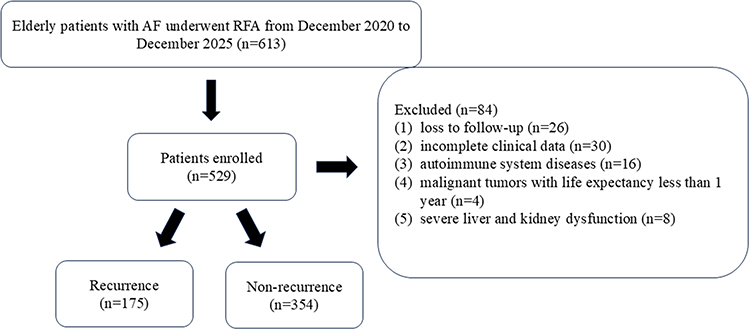 |
Figure 1 The flowchart of our research. |
Data Collection and Definition
The clinical data of the participants were obtained from the case database. Demographic information included age, gender, BMI, AF duration, and CHA2DS2-VASc score. Comorbidities recorded were atrial flutter (AFL), hypertension, diabetes, coronary heart disease (CHD), chronic heart failure (CHF), chronic obstructive pulmonary disease (COPD), and ischemic stroke (IS). Laboratory indicators comprised leukocyte count, hemoglobin, platelets, neutrophils, monocytes, lymphocytes, alanine aminotransferase (ALT), glucose, uric acid, albumin, creatinine, total cholesterol (TC), TG, low-density lipoprotein cholesterol (LDL-C), HDL-C, and B-type brain natriuretic peptide (BNP). Imaging indicators included left atrial diameter (LAD), left ventricular end-diastolic diameter (LVEDD), and left ventricular ejection fraction (LVEF). The drug usage included Sodium-Glucose Cotransporter 2 inhibitor (SGLT-2 inhibitor) and Glucagon-Like peptide-1 Receptor Agonist (GLP-1 RA). The neutrophil-to-lymphocyte ratio (NLR) was calculated as neutrophil count (×109/L) divided by lymphocyte count (×109/L). BMI was calculated as weight (kg) divided by height (m) squared. The SPISE index was calculated as 600 × HDL-C0.185 / (TG0.2 × BMI1.338).9 The SPISE index is categorized into tertiles as follows: T1 < 5.25, 5.25 ≤ T2 < 6.68, and T3 ≥ 6.68.
Radiofrequency Ablation
All patients received anticoagulant therapy with rivaroxaban or dabigatran during the perioperative period. Prior to the RFA, transesophageal echocardiography or enhanced computed tomography (CT) angiography of the left atrium was performed to assess for left atrial thrombus. During catheter ablation, fentanyl was administered for pain relief and midazolam for sedation. After two punctures of the femoral vein, atrial septal puncture was performed under X-ray guidance. Immediately following the atrial septal puncture, systemic heparinization was initiated. Three-dimensional electroanatomic mapping (CARTO3, Biosense Webster) was used to reconstruct the atrial geometry. The specific ablation strategy can be found in our previous research.11
Follow-Up and Outcome
After ablation, all patients received oral anticoagulants for at least three months. If there were no contraindications, they were also prescribed anti-arrhythmic drugs to prevent recurrence and scheduled for outpatient monitoring. The system-based follow-up assessment included clinical evaluation and either a dynamic electrocardiogram or a standard electrocardiogram conducted quarterly (at 3, 6, 9, and 12 months). Recurrence was defined as AF, AFL, or atrial tachycardia lasting more than 30 seconds after ablation. A recurrence occurring within three months was classified as an early recurrence (ER).
Statistical Analysis
SPSS 27.0, GraphPad Prism 8.0, and Z Stats (https://www.medsta.cn/) were used for data analysis and visualization. The sample size for the survival analysis was calculated using the Log rank test, assuming a hazard ratio of 0.6, 90% power, two-sided α = 0.05, and 25% anticipated censoring. We required 162 events across both groups, corresponding to a total sample size of 215 participants.12 Measurement data were assessed for normality using the Shapiro–Wilk test. The results showed that all continuous variables were non-normally distributed. These data are reported as the median with the first and third quartiles. Inter-group comparisons were performed using the Mann–Whitney U-test and the Kruskal-Walk test. Categorical variables are presented as frequencies and percentages, with inter-group comparisons conducted using the chi-square test or Fisher’s exact test. ROC curve analysis was employed to evaluate the predictive value of the SPISE index for AF recurrence. We assessed the predictive value of the SPISE index in both paroxysmal and persistent AF, as well as its predictive accuracy at 1, 3, and 5 years post-AF ablation. A multivariate Cox regression model was used to examine the relationship between the SPISE index and AF recurrence. SPISE index levels were categorized into quartiles and included in the multivariate Cox regression analysis. Model 1 was unadjusted; Model 2 was adjusted for age, gender, hypertension, diabetes, CHD, and CHF; Model 3 included all covariates in Model 2 plus CHA2DS2-VASc score, LAD, AF type, glucose, LVEF, NLR, cardioversion, and ER. In Model 3, all independent variables were subjected to collinearity diagnostics. The results showed that the variance inflation factor (VIF) values for all independent variables in the Cox regression model ranged from 1.04 to 1.89 (all below 5), and the tolerance values ranged from 0.53 to 0.96 (all above 0.1), indicating no significant multicollinearity among the variables. RCS were applied based on Models 1–3 to assess the nonlinear association between the SPISE index and AF recurrence. Additionally, subgroup analyses were performed to evaluate the robustness of the SPISE index-AF recurrence relationship in elderly patients, with stratification by gender, AF type, hypertension, diabetes, CHD, CHF, and ER. Kaplan-Meier survival analysis was used to compare recurrence rates across groups with different SPISE index levels. Survival analyses were also conducted within subgroups defined by ER, AF type, gender, hypertension, diabetes, CHD, and CHF to compare the predictive value of the SPISE index for AF recurrence. Spearman correlation analysis assessed associations between variables. The DeLong test was used to compare areas under different ROC curves. A threshold analysis was conducted to evaluate the threshold effect of the SPISE index and the association with recurrence. Statistical significance was set at P < 0.05 for all analyses.
Results
Baseline Data of the Recurrence and Non-Recurrence Groups
There were significant differences between the recurrence and non-recurrence groups regarding AF type, BMI, diabetes, CHF, glucose, albumin, HDL-C, triglycerides, leukocytes, neutrophils, monocytes, NLR, LAD, LVEF, cardioversion, ER, SGLT-2 inhibitors and GLP-1 RAs (all P < 0.05). The SPISE index level in the recurrence group was significantly lower than that in the non-recurrence group (P < 0.001). See Table 1 and Figure 2.
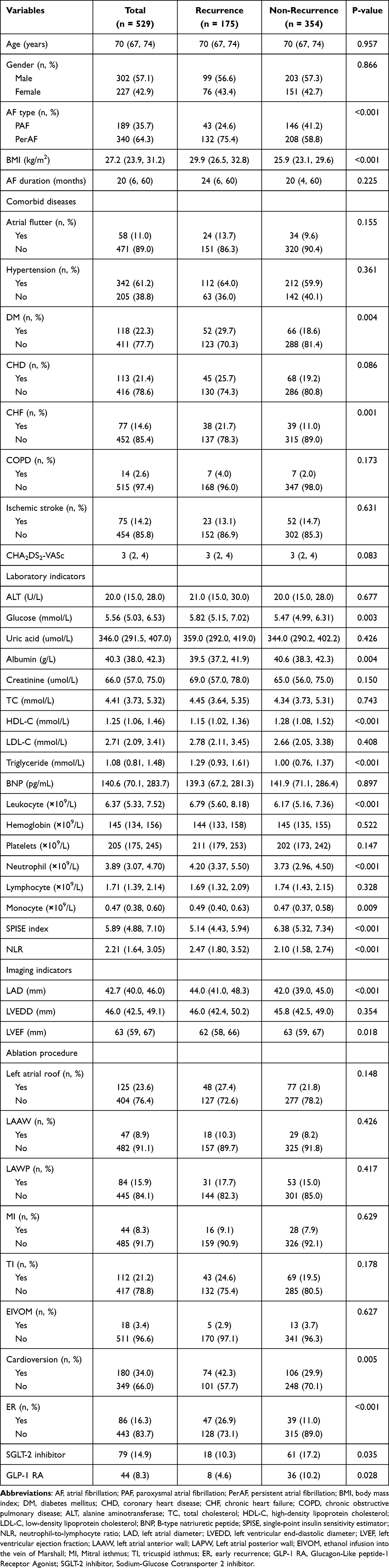 |
Table 1 Comparison of Baseline Data Between the Recurrence Group and the Non-Recurrence Group |
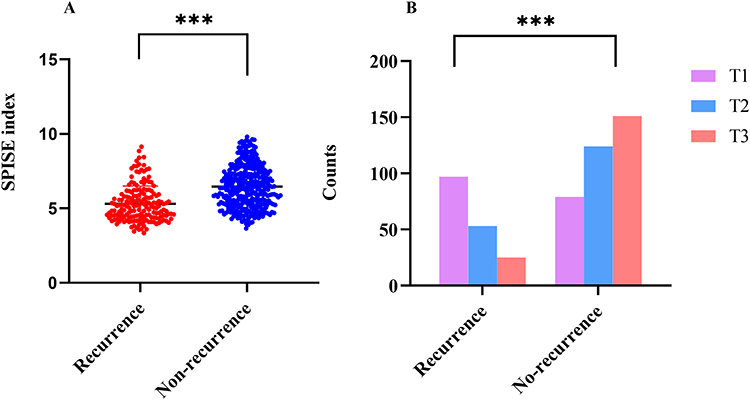 |
Figure 2 Comparison of SPISE index between the recurrence group and the non-recurrence group (A) and distribution of patients across SPISE tertiles (T1, T2, T3) according to recurrence status (B). ***P < 0.001. |
Baseline Data Across Different SPISE Index Groups
There were significant differences among the various SPISE index groups regarding BMI, diabetes, ischemic stroke, glucose, HDL-C, triglycerides, platelets, lymphocytes, LAD, recurrence, SGLT-2 inhibitors and GLP-1 RAs (all P < 0.05). See Table 2.
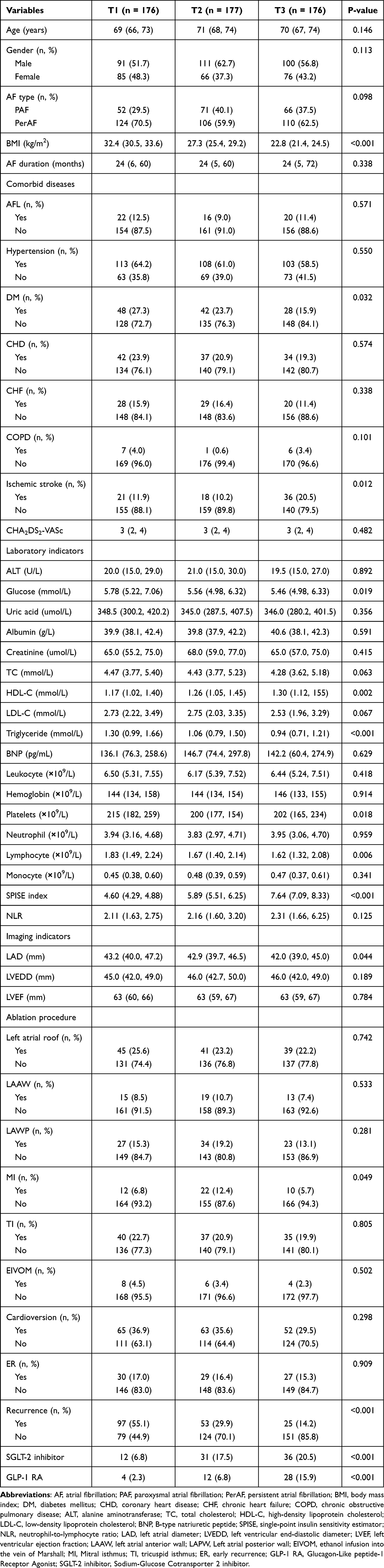 |
Table 2 Comparison of Basic Clinical Data Among Different SPISE Index Groups |
Relationship Between SPISE Index and Atrial Fibrillation Recurrence
After adjusting for all covariates-including age, gender, hypertension, diabetes, CHD, CHF, CHA2DS2-VASc score, LAD, AF type, glucose, LVEF, NLR, cardioversion, and ER-we found that a higher SPISE index was associated with a lower risk of AF recurrence in the elderly after RFA, demonstrating a negative correlation (HR = 0.661, 95% CI: 0.579–0.755, P < 0.001). Compared with the T3 group, participants in the T1 group had a higher AF recurrence rate (HR = 3.414, 95% CI: 2.181–5.344, P < 0.001). See Table 3.
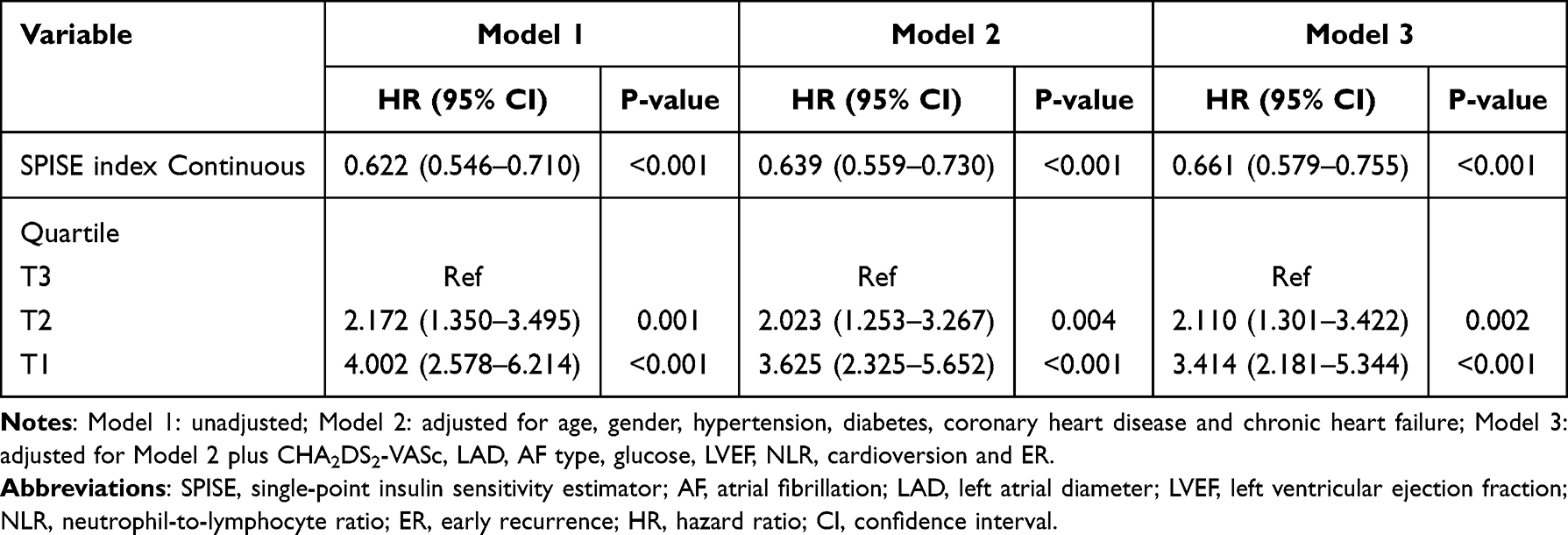 |
Table 3 Multivariate Cox Regression Analysis Model |
The ROC curve demonstrated that the SPISE index had the highest predictive value for AF recurrence, with an area under the curve (AUC) of 0.74 (95% CI: 0.70–0.79). One year after RFA, the predictive value of the SPISE index for AF recurrence was an AUC of 0.84 (95% CI: 0.77–0.91), while the 3-year AUC was 0.75 (95% CI: 0.70–0.81). For paroxysmal AF, the SPISE index had a predictive value of 0.75 (95% CI: 0.67–0.83), and for persistent AF, the AUC was 0.74 (95% CI: 0.68–0.79). The DeLong test indicated that the SPISE index had significantly better predictive value for AF recurrence compared to the LAD (Z = 3.35, P < 0.001). Similarly, compared with the components (triglycerides, HDL-C and BMI), the SPISE index had a better predictive value (Figure 3 and Table 4).
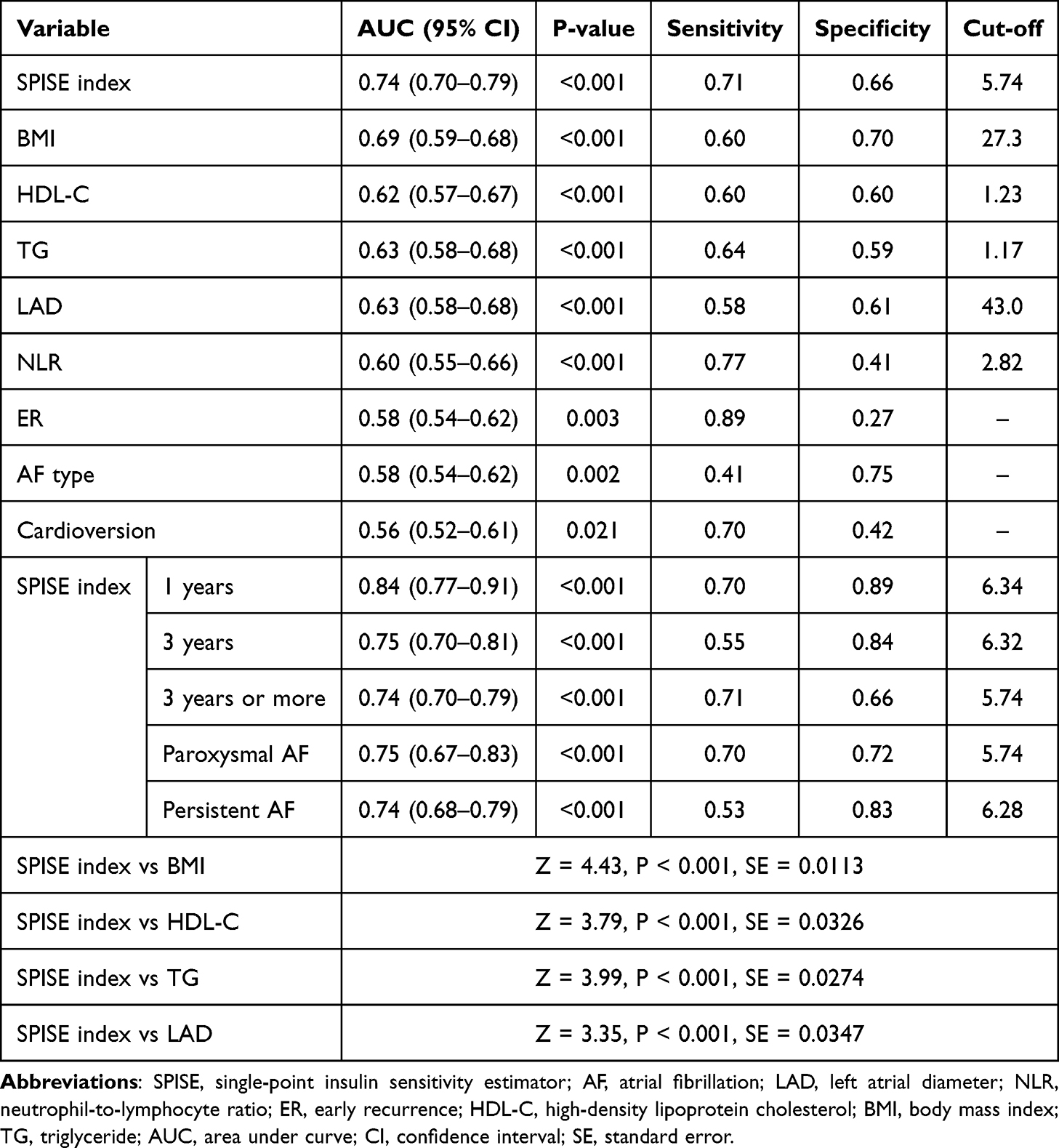 |
Table 4 Receiver Operating Characteristic Curve of Risk Factors for AF Recurrence |
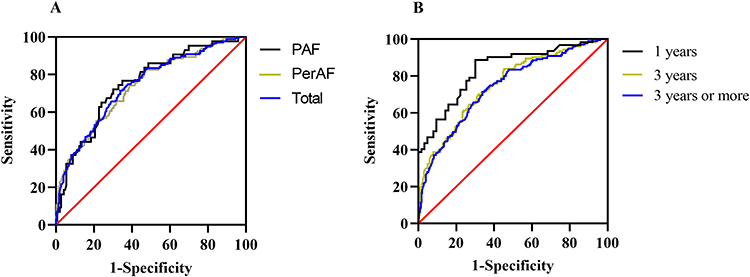 |
Figure 3 Receiver operating characteristic curve (ROC) for evaluating the predictive value of SPISE index for AF recurrence. ROC curves stratified by AF type (A); ROC curves stratified by follow-up duration (B). |
Based on Model 3, we found a nonlinear association between the SPISE index and the recurrence of AF (P for overall < 0.001, P for nonlinear = 0.011) (Figure 4).
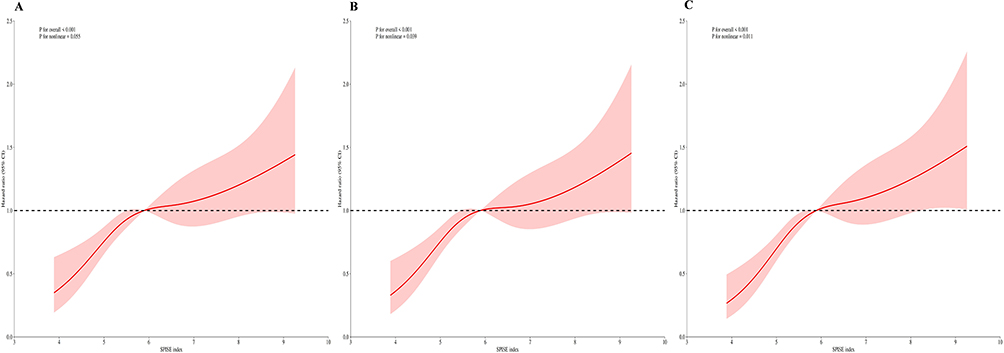 |
Figure 4 The restricted cubic splines analysis between the SPISE index and AF recurrence. (A) Model 1: unadjusted; (B) Model 2: adjusted for age, gender, hypertension, diabetes, coronary heart disease and chronic heart failure; (C) Model 3: adjusted for Model 2 plus CHA2DS2-VASc, LAD, AF type, glucose, LVEF, NLR, cardioversion and ER. Abbreviations: SPISE, single-point insulin sensitivity estimator; AF, atrial fibrillation; LAD, left atrial diameter; LVEF, left ventricular ejection fraction; NLR, neutrophil-to-lymphocyte ratio; ER, early recurrence; HR, hazard ratio. |
Subgroup Analysis
We conducted a subgroup analysis to evaluate potential interaction factors between the SPISE index and the recurrence of AF in elderly patients (Figure 5). We observed that this association remained consistent across various subgroups (all P for interaction > 0.05), such as gender, ER, AF type, hypertension, diabetes and CHD. However, in elderly patients with CHF, the SPISE index was not associated with the recurrence of AF (P > 0.05).
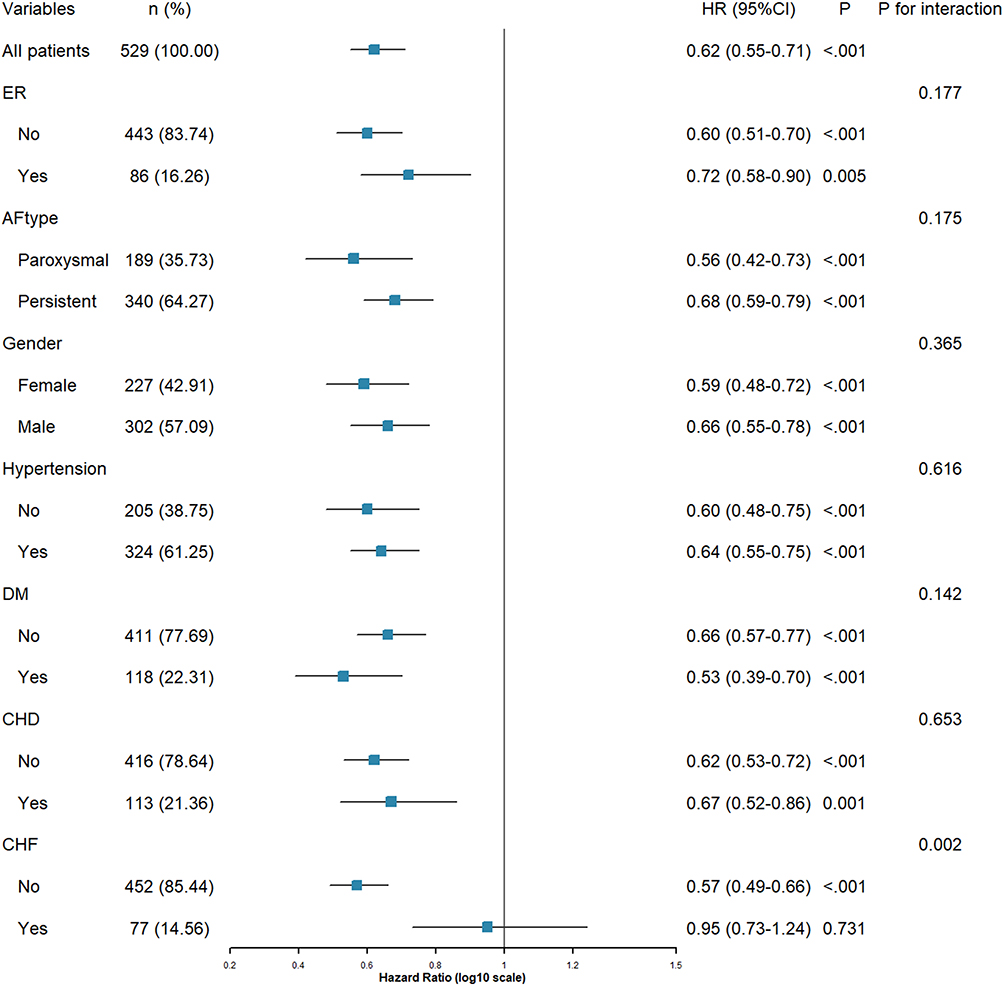 |
Figure 5 Subgroup analysis of SPISE index with AF recurrence. Abbreviations: AF, atrial fibrillation; PAF, paroxysmal atrial fibrillation; PerAF, persistent atrial fibrillation; DM, diabetes mellitus; CHD, coronary heart disease; CHF, chronic cardiac failure; ER, early recurrence; HR, hazard ratio; CI, confidence interval. |
Kaplan-Meier Survival Curve of the SPISE Index and Atrial Fibrillation Recurrence in Different Subgroups
The Kaplan-Meier survival analysis revealed significant differences in the recurrence rates of AF among populations with varying SPISE index levels. However, among patients with CHF, no significant difference in recurrence was observed across different SPISE index levels (log-rank P = 0.762) (Figure 6).
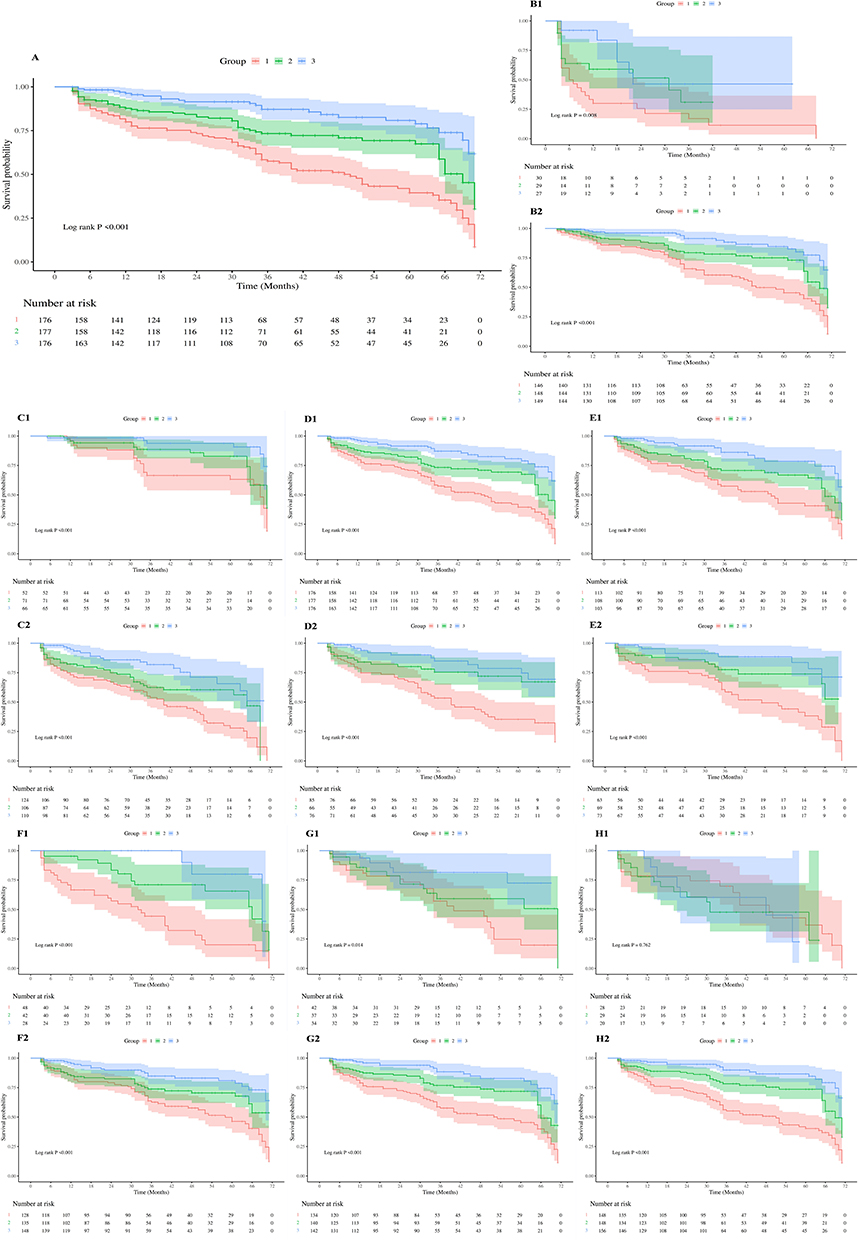 |
Figure 6 Kaplan-Meier survival curve of SPISE index and AF recurrence in different subgroups. (A) the general population; (B1) with ER and (B2) without ER; (C1) PAF and (C2) PerAF; (D1) Male and (D2) Female; (E1) with hypertension and (E2) without hypertension; (F1) with DM and (F2) without DM; (G1) with CHD and (G2) without CHD; (H1) with CHF and (H2) without CHF. Abbreviations: SPISE, single-point insulin sensitivity estimator; AF, atrial fibrillation; PAF, paroxysmal atrial fibrillation; PerAF, persistent atrial fibrillation; DM, diabetes mellitus; CHD, coronary heart disease; CHF, chronic cardiac failure; ER, early recurrence. |
Correlation Analysis of the SPISE Index
The Spearman correlation analysis revealed that SPISE was negatively correlated with LAD (r = −0.123, P = 0.005), platelets (r = −0.134, P = 0.002), lymphocytes (r = −0.128, P = 0.003), and glucose (r = −0.113, P = 0.009) (Figure 7).
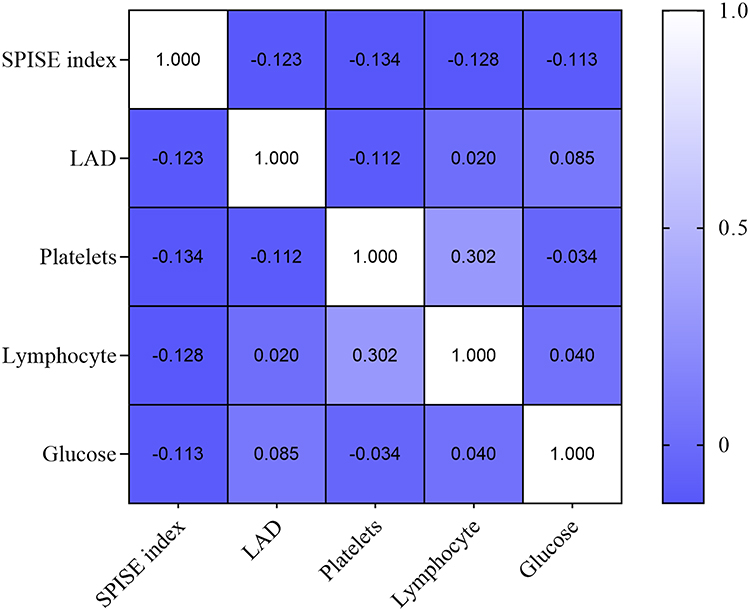 |
Figure 7 Correlation analysis of the SPISE index. |
Threshold Analysis of SPISE Index and AF Recurrence
The standard linear regression model was first applied to explore the association between the independent variable and the outcome. The overall effect size was 0.66 (95% CI: 0.58–0.76, P < 0.001). A two-piecewise linear regression model was then used to fit the nonlinear relationship, identifying an inflection point at 4.55. Stratified analysis based on this inflection point showed that for values less than 4.55, the effect size was 0.33 (95% CI: 0.12–0.92, P = 0.034); for values greater than or equal to 4.55, the effect size increased to 0.71 (95% CI: 0.60–0.83, P < 0.001). The likelihood ratio test yielded P = 0.317, suggesting that the two-piecewise model did not provide a significantly better fit than the standard linear model (Table 5).
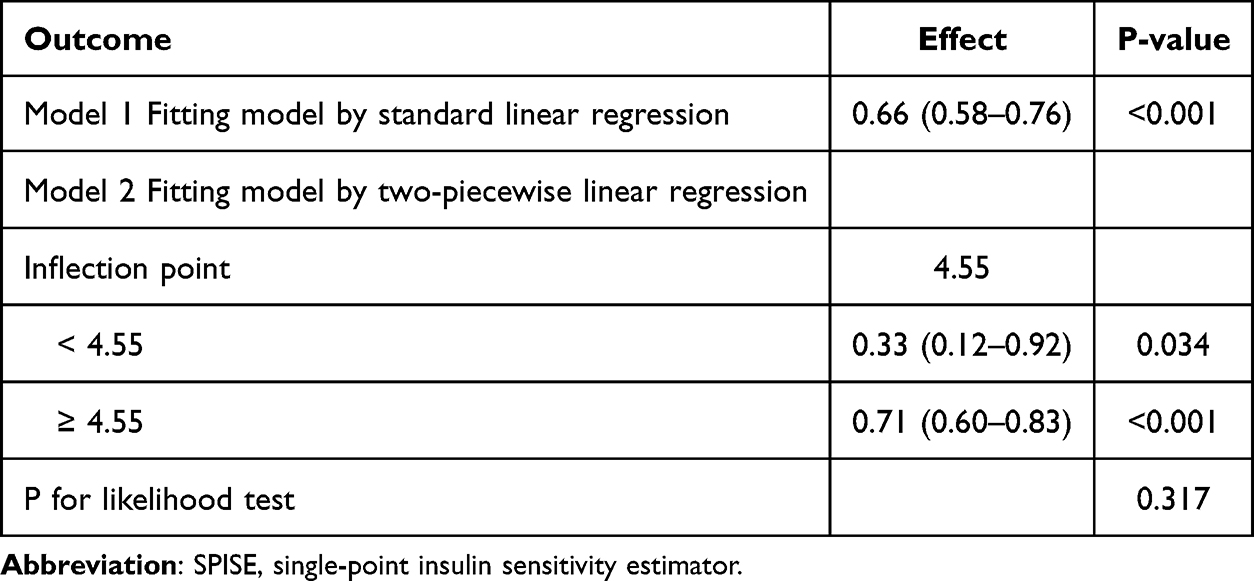 |
Table 5 Threshold Analysis of SPISE Index and AF Recurrence |
Discussion
This study found that the SPISE index was negatively correlated with the recurrence of AF after RFA in elderly patients. Furthermore, subgroup analysis revealed that, except for patients with CHF, this negative correlation remained consistent across most demographic groups. The results of the survival analysis also confirmed that, in various groups, patients with a low SPISE index were more likely to experience AF recurrence.
RFA is a well-established treatment for AF that can improve quality of life and alleviate symptoms associated with AF.4 One year after ablation, the success rate for paroxysmal AF is approximately 70% to 90%, while for persistent AF, it ranges from 65% to 75%.13–15 Advancing age is the strongest independent risk factor for AF. However, identifying the mechanisms by which aging promotes AF is challenging because many comorbidities-such as CHD, diabetes, valvular disease, and heart failure-become more common and severe with age.16 Studies have shown that the effectiveness of RFA treatment for elderly patients with AF is no different from that for younger patients.17,18 However, because elderly patients have more comorbidities, the incidence of complications related to RFA is higher in this population.19 The recurrence of AF after RFA in elderly patients is associated with frailty, LAD, and the type of AF (persistent AF).20,21
IR is a central mechanism underlying chronic metabolic diseases such as type 2 diabetes, obesity, metabolic syndrome, and non-alcoholic fatty liver disease. It is characterized by a diminished or impaired cellular response to insulin. IR has been confirmed to be associated with the development and pathogenesis of AF and also influences the recurrence rate of AF following RFA.22 Relevant studies have shown that IR and related diseases significantly increase the risk of AF.23 IR-related derivatives, such as the triglyceride-glucose index, metabolic score for IR, triglyceride glucose-BMI, and HOMA-IR, have been shown to be associated with the recurrence of AF after RFA.6,7 Inflammatory response and oxidative stress are the primary mechanisms through which IR promotes the onset of AF and its recurrence after ablation. In the state of IR, inflammation in adipocytes intensifies, free fatty acid levels continue to rise, and multiple inflammatory factors are activated. This cascade induces atrial structural remodeling and fibrosis, exacerbating cardiac tissue damage and remodeling.24,25 Enhanced inflammation of adipocytes and activation of cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) can promote atrial fibrosis and tissue remodeling, increase susceptibility to arrhythmias, and further facilitate the development and recurrence of AF.23,26 The enlargement of the LAD is an indicator of atrial remodeling, and its size is significantly correlated with the recurrence of AF.27 Qin et al confirmed that IR-related indicators, specifically the triglyceride glucose-BMI, are associated with left atrial remodeling and show a positive correlation with LAD.28 Both SGLT-2 inhibitors and GLP-1 RAs can improve IR and significantly reduce the risk of AF through multiple mechanisms, including metabolic regulation, anti-inflammatory effects, and electrophysiological remodeling. SGLT-2 inhibitors exert indirect yet significant effects in improving IR through weight loss, reduced lipotoxicity, and decreased inflammation. Simultaneously, they directly prevent AF by reversing electrical and structural remodeling, inhibiting the CaMKII and NLRP3 pathways, and reducing cardiac workload. GLP-1 RAs enhance insulin sensitivity by directly activating insulin signaling pathways and exerting significant anti-inflammatory effects. Their atrial protective benefits are primarily mediated by substantial weight loss and metabolic improvements, along with additional direct electrophysiological stabilization of the atrial myocardium.29,30
The SPISE index is a novel IR alternative indicator, incorporating BMI, TG, and HDL-C, which shows a significant correlation with various cardiovascular diseases.10,31–33 The BMI is an important indicator for predicting the incidence of AF in the general population. It is also associated with an increased risk of AF recurrence after RFA.34 Patients with a higher BMI exhibited elevated levels of various inflammatory and oxidative stress markers, which are closely associated with the onset and progression of AF.35 Multiple clinical studies have demonstrated that serum lipids contribute to inflammation and elevate the risk of AF.36,37 However, the relationship between the occurrence of AF is related to the lipid levels in the population remains controversial.38 There are few studies on the SPISE index and the recurrence of AF after RFA. Our study found that, in elderly patients with AF, the SPISE index was higher in the non-recurrence group. After adjusting for various risk factors, the SPISE index was found to be negatively correlated with AF recurrence. This association persisted whether the SPISE index was treated as a continuous or categorical variable. The postoperative recurrence rate in AF patients with a low SPISE index was 3.4 times higher than in those with a high SPISE index. Our analysis using the RCS model revealed a statistically significant, non-linear relationship between the SPISE index and AF recurrence. Subgroup analyses based on gender, ER, AF type, hypertension, CHD and diabetes showed a consistent association, thereby enhancing the reliability of the SPISE index as an indicator of AF recurrence across different subgroups. However, in elderly AF patients with CHF, no correlation was found between the SPISE index and AF recurrence. Notably, the predictive value of the SPISE index is significantly diminished in patients with CHF. Beyond the acknowledged limitation of sample size, this phenomenon can be largely attributed to the overwhelming pathophysiological alterations associated with atrial remodeling in advanced heart failure. These changes may overshadow the metabolic effects of IR reflected by SPISE. Advanced heart failure results in persistent atrial pressure and volume overload, driving progressive structural remodeling characterized by atrial dilation and interstitial fibrosis. This remodeling is accompanied by electrophysiological disturbances, excessive activation of the renin–angiotensin–aldosterone system and sympathetic nervous system, as well as myocardial metabolic reprogramming. These comprehensive cardiac pathological changes become the primary determinants of atrial dysfunction and adverse clinical events.39,40 IR activates the mitogen-activated protein kinase (MAPK) signaling pathway, promoting oxidative stress, cardiac hypertrophy, fibrosis, and cell apoptosis. Specifically, in the IR state, adipocyte inflammation intensifies, free fatty acid levels continue to rise, and various inflammatory factors-such as TNF-α and IL-6-are activated. This promotes the activation of atrial progenitor cells, induces atrial structural remodeling and fibrosis, and exacerbates cardiac tissue damage and remodeling. This suggests that the metabolic abnormalities associated with IR collectively increase the risk of adverse atrial remodeling and arrhythmia, thereby contributing to the recurrence of AF.41 In this context, the systemic metabolic signal of IR captured by SPISE is largely masked by the profound mechanical, neurohormonal, and structural abnormalities of atrial remodeling. Consequently, SPISE fails to maintain reliable predictive performance in populations with heart failure, as local cardiac remodeling, rather than peripheral metabolic disturbances, predominates disease progression. Excluding patients with CHF, significant differences in postoperative recurrence were observed among elderly AF patients with different SPISE index levels; those with a low SPISE index had significantly higher recurrence rates than those with a high SPISE index. Compared with other risk factors, the SPISE index demonstrated superior predictive value for AF recurrence.
To date, previous studies have not systematically investigated the association between the SPISE index and the recurrence of AF. Our findings suggest that the SPISE index may serve as a significant predictor of AF recurrence in elderly patients following RFA. These findings have potential clinical implications, offering guidance for the early identification and intervention of high-risk elderly patients with AF. Elderly patients with AF often have multiple coexisting conditions, such as metabolic syndrome, which complicates the identification of individuals at high risk. Incorporating IR into the management of AF can help address the limitations of current prevention and control strategies, thereby improving the identification of “high-risk” patients. The presence of IR and metabolic abnormalities may act as “invisible driving factors” in the remodeling of atrial structure and electrophysiology, potentially impacting the overall effectiveness of comprehensive AF management. Our research has demonstrated a significant correlation between the SPISE index and AF recurrence. Therefore, proactive early interventions- such as optimizing dietary patterns, prescribing exercise, promoting scientific weight loss, pharmacological treatment, and managing comorbidities- may improve the success rate of RFA. However, our study has several limitations. First, as a single-center retrospective study, there may have been insufficient monitoring of AF recurrence, potentially leading to an overestimation of the success rate of AF ablation. More intensive follow-up methods, such as the use of smartwatches or long-term ambulatory electrocardiograms, may be necessary. Second, relying on a single SPISE index measurement may be insufficient; dynamic changes in the index should be observed over time. Third, the use of hypoglycemic and lipid-lowering medications may influence SPISE index measurements. The underlying mechanism linking the SPISE index to AF recurrence remains unclear. Therefore, future prospective studies with larger sample sizes are needed to further evaluate its impact on AF recurrence.
Conclusions
A higher SPISE index is associated with a reduced risk of recurrence after RFA in elderly patients with AF. The SPISE index exhibits a nonlinear relationship with AF recurrence. Compared to traditional risk factors, the SPISE index has superior predictive value for the recurrence of AF following RFA in elderly patients.
Data Sharing Statement
This article includes all data related to the research. Due to participants’ privacy concerns, the data have not been made publicly available. However, the research data can be obtained from the corresponding author upon request.
Ethics Approval and Informed Consent
This research was approved by the Ethics Committee of Yantai Yuhuangding Hospital, affiliated with Qingdao University (No. K2026-155). All patients provided informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82200503).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–18. doi:10.1016/j.jacc.2020.11.010
2. Dewland TA, Olgin JE, Vittinghoff E, Marcus GM. Incident atrial fibrillation among Asians, Hispanics, blacks, and whites. Circulation. 2013;128(23):2470–2477. doi:10.1161/circulationaha.113.002449
3. Rahman F, Kwan GF, Benjamin EJ. Global epidemiology of atrial fibrillation. Nat Rev Cardiol. 2014;11(11):639–654. doi:10.1038/nrcardio.2014.118
4. Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45(36):3314–3414. doi:10.1093/eurheartj/ehae176
5. Kuck KH, Fürnkranz A, Chun KR, et al. Cryoballoon or radiofrequency ablation for symptomatic paroxysmal atrial fibrillation: reintervention, rehospitalization, and quality-of-life outcomes in the FIRE AND ICE trial. Eur Heart J. 2016;37(38):2858–2865. doi:10.1093/eurheartj/ehw285
6. Ghoshouni H, Sepehri Shamloo A, Mirjalili SR, et al. Association between surrogate insulin resistance markers and postablation atrial fibrillation recurrence: a systematic review and meta-analysis. Heart Rhythm. 2025;22(9):e605–e617. doi:10.1016/j.hrthm.2025.04.050
7. Wang Z, He H, Xie Y, et al. Non-insulin-based insulin resistance indexes in predicting atrial fibrillation recurrence following ablation: a retrospective study. Cardiovasc Diabetol. 2024;23(1):87. doi:10.1186/s12933-024-02158-6
8. Song K, Lee E, Lee HS, et al. Comparison of SPISE and METS-IR and other markers to predict insulin resistance and elevated liver transaminases in children and adolescents. Diabet Metabol J. 2025;49(2):264–274. doi:10.4093/dmj.2024.0302
9. Paulmichl K, Hatunic M, Højlund K, et al. Modification and validation of the Triglyceride-to-HDL cholesterol ratio as a surrogate of insulin sensitivity in white juveniles and adults without diabetes mellitus: the Single Point Insulin Sensitivity Estimator (SPISE). Clin Chem. 2016;62(9):1211–1219. doi:10.1373/clinchem.2016.257436
10. Yao X, Liu L, Zhao L, Zhang N. Association between the single-point insulin sensitivity estimator and cardiovascular disease incidence: a prospective nationwide cohort study involving two cohorts. Atherosclerosis. 2026;412:120591. doi:10.1016/j.atherosclerosis.2025.120591
11. Wang Z, Qu Y, Wang H, Wang C. The HALP index is associated with the recurrence of persistent atrial fibrillation following radiofrequency catheter ablation. J Inflamm Res. 2025;18:5821–5833. doi:10.2147/jir.S518233
12. Stein RA. Tables of the number of patients required in clinical trials using the logrank test. Stat Med. 1986;5(1):97–98. doi:10.1002/sim.4780050112
13. Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. 2005;293(21):2634–2640. doi:10.1001/jama.293.21.2634
14. Clarnette JA, Brooks AG, Mahajan R, et al. Outcomes of persistent and long-standing persistent atrial fibrillation ablation: a systematic review and meta-analysis. Europace. 2018;20(Fi_3):f366–f376. doi:10.1093/europace/eux297
15. Steinberg JS, Palekar R, Sichrovsky T, et al. Very long-term outcome after initially successful catheter ablation of atrial fibrillation. Heart Rhythm. 2014;11(5):771–776. doi:10.1016/j.hrthm.2014.02.003
16. Heijman J, Linz D, Schotten U. Dynamics of atrial fibrillation mechanisms and comorbidities. Annu Rev Physiol. 2021;83:83–106. doi:10.1146/annurev-physiol-031720-085307
17. Fink T, Metzner A, Willems S, et al. Procedural success, safety and patients satisfaction after second ablation of atrial fibrillation in the elderly: results from the German Ablation Registry. Clin Res Cardiol. 2019;108(12):1354–1363. doi:10.1007/s00392-019-01471-5
18. Jilek C, Lewalter T. Ablation von Vorhofflimmern beim älteren Menschen. Herzschr Elektrophys. 2017;28(1):39–47. doi:10.1007/s00399-017-0484-4
19. Kawamura I, Aikawa T, Yokoyama Y, Takagi H, Kuno T. Catheter ablation for atrial fibrillation in elderly patients: systematic review and a meta-analysis. Pacing Clin Electrophysiol. 2022;45(1):59–71. doi:10.1111/pace.14413
20. Boehmer AA, Rothe M, Keim C, et al. Pulmonary vein isolation in elderly patients ≥ 75 years: a propensity score-matched analysis with focus on differences among atrial fibrillation types. Can J Cardiol. 2024;40(9):1541–1550. doi:10.1016/j.cjca.2024.01.027
21. Lin H, Lin M, Li H, Sun D. Frailty may be a new predictive factor of recurrence after radiofrequency catheter ablation in elderly atrial fibrillation patients. Geriatr Nurs. 2025;61:429–433. doi:10.1016/j.gerinurse.2024.12.008
22. Chan YH, Chang GJ, Lai YJ, et al. Atrial fibrillation and its arrhythmogenesis associated with insulin resistance. Cardiovasc Diabetol. 2019;18(1):125. doi:10.1186/s12933-019-0928-8
23. Huang T, Fang Z, Zhang Q, Li Y, Shi L. Insulin resistance and atrial fibrillation: from disease onset to post-ablation outcomes: a systematic review and meta-analysis. Systematic Review. Front Cardiovasc Med. 2026;12:1700730. doi:10.3389/fcvm.2025.1700730
24. Yao C, Qin Y, Yan X, et al. Correlation between triglyceride-glucose index and atrial fibrillation in acute coronary syndrome patients: a retrospective cohort study and the establishment of a LASSO-Logistic regression model. BMC Cardiovasc Disord. 2024;24(1):702. doi:10.1186/s12872-024-04385-x
25. Kan F, Yang Z, Bao D, Tang M, Ji N. Association between triglyceride-glucose index and all-cause mortality in patients with congestive heart failure and atrial fibrillation. Front Cardiovasc Med. 2025;12:1476815. doi:10.3389/fcvm.2025.1476815
26. Li X, Zhou Z, Xia Z, et al. Association between estimated glucose disposal rate and atrial fibrillation recurrence in patients undergoing radiofrequency catheter ablation: a retrospective study. Eur J Med Res. 2024;29(1):325. doi:10.1186/s40001-024-01911-7
27. Wang Q, Zhuo C, Shang Y, et al. U-Shaped relationship between left atrium size on echocardiography and 1-year recurrence of atrial fibrillation after radiofrequency catheter ablation-prognostic value study. Circ J. 2019;83(7):1463–1471. doi:10.1253/circj.CJ-19-0167
28. Qin S, Luo Y, Hou J, et al. Insulin resistance, left atrial anatomical remodeling, and recurrence in patients with atrial fibrillation undergoing radiofrequency ablation. Eur J Med Res. 2025;30(1):819. doi:10.1186/s40001-025-03093-2
29. Fakhrolmobasheri M, Abhari AP, Manshaee B, et al. Effect of sodium-glucose cotransporter 2 inhibitors on insulin resistance; a systematic review and meta-analysis. Acta Diabetol. 2023;60(2):191–202. doi:10.1007/s00592-022-01981-1
30. Karakasis P, Fragakis N, Vlachos K, et al. GLP-1 receptor agonists and atrial fibrillation: chronotropy, atrial substrate, and cardiometabolic mechanisms. Metabolism. 2026;179:156605. doi:10.1016/j.metabol.2026.156605
31. Zhu XF, Mo YT, Hu YQ, Feng YX, Liu EH. Association between single-point insulin sensitivity estimator and heart failure in older adults: a cross-sectional study. Exp Gerontology. 2024;196:112578. doi:10.1016/j.exger.2024.112578
32. Deng S, Hu X, Zhang X. Association of single-point insulin sensitivity estimator index (SPISE) with future cardiovascular outcomes in patients with type 2 diabetes. Diabetes Obes Metab. 2024;26(7):2820–2829. doi:10.1111/dom.15600
33. Cederholm J, Zethelius B. SPISE and other fasting indexes of insulin resistance: risks of coronary heart disease or type 2 diabetes. Comparative cross-sectional and longitudinal aspects. Ups J Med Sci. 2019;124(4):265–272. doi:10.1080/03009734.2019.1680583
34. Liu F, Song T, Hu Q, et al. Body mass index and atrial fibrillation recurrence post ablation: a systematic review and dose-response meta-analysis. Front Cardiovasc Med. 2022;9:999845. doi:10.3389/fcvm.2022.999845
35. Karam BS, Chavez-Moreno A, Koh W, Akar JG, Akar FG. Oxidative stress and inflammation as central mediators of atrial fibrillation in obesity and diabetes. Cardiovasc Diabetol. 2017;16(1):120. doi:10.1186/s12933-017-0604-9
36. Stiekema LCA, Willemsen L, Kaiser Y, et al. Impact of cholesterol on proinflammatory monocyte production by the bone marrow. Eur Heart J. 2021;42(42):4309–4320. doi:10.1093/eurheartj/ehab465
37. Westerterp M, Fotakis P, Ouimet M, et al. Cholesterol efflux pathways suppress inflammasome activation, NETosis, and atherogenesis. Circulation. 2018;138(9):898–912. doi:10.1161/circulationaha.117.032636
38. Hayıroğlu M, Şaylık F, Çınar T, Tokgözoğlu L. Meta-analysis of the current research on the relationship between blood lipid levels and the occurrence of atrial fibrillation. Heart Lung Circ. 2023;32(10):1158–1166. doi:10.1016/j.hlc.2023.08.006
39. Melenovsky V, Hwang SJ, Redfield MM, Zakeri R, Lin G, Borlaug BA. Left atrial remodeling and function in advanced heart failure with preserved or reduced ejection fraction. Circulation. 2015;8(2):295–303. doi:10.1161/circheartfailure.114.001667
40. Fang Z, Raza U, Song J, et al. Systemic aging fuels heart failure: molecular mechanisms and therapeutic avenues. ESC Heart Fail. 2025;12(2):1059–1080. doi:10.1002/ehf2.14947
41. Fan Z, Shi T, Yang C, et al. Associations of the triglyceride-glucose index and its obesity-related derivatives with cardiac structure, function, and incident atrial fibrillation: a prospective cohort study using cardiac magnetic resonance. Cardiovasc Diabetol. 2026;25:151. doi:10.1186/s12933-026-03143-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Risk Nomogram Model for Predicting Recurrence in Patients with Atrial Fibrillation After Radiofrequency Catheter Ablation
Zhao Z, Zhang F, Ma R, Bo L, Zhang Z, Zhang C, Wang Z, Li C, Yang Y
Clinical Interventions in Aging 2022, 17:1405-1421
Published Date: 25 September 2022
Effects of Inflammatory Cell Death Caused by Catheter Ablation on Atrial Fibrillation
Liu D, Li Y, Zhao Q
Journal of Inflammation Research 2023, 16:3491-3508
Published Date: 17 August 2023
Platelet-to-Lymphocyte Ratio Improves the Predictive Ability of the Risk Score for Atrial Fibrillation Recurrence After Radiofrequency Ablation
Huang W, Sun H, Tang Y, Luo Y, Liu H
Journal of Inflammation Research 2023, 16:6023-6038
Published Date: 11 December 2023
Predictive Value of Serum microRNA-29b-3p in Recurrence of Atrial Fibrillation After Radiofrequency Catheter Ablation
Zhan J, Peng C, Liu Y, Bi Z, Lu G, Hao S, Tong Y, Zhang G
Clinical Interventions in Aging 2024, 19:715-725
Published Date: 3 May 2024
Comparison of Long-Term Outcomes Between Repeated Hepatic Resection and Radiofrequency Ablation in Patients with Small Recurrent Hepatocellular Carcinoma After Initial Curative Resection: A Propensity Score Matched Study

Hsiao CY, Hu RH, Liang PC, Wu CH
Journal of Hepatocellular Carcinoma 2025, 12:1587-1598
Published Date: 23 July 2025