Back to Journals » Journal of Inflammation Research » Volume 16
Effects of Inflammatory Cell Death Caused by Catheter Ablation on Atrial Fibrillation
Received 19 May 2023
Accepted for publication 8 August 2023
Published 17 August 2023 Volume 2023:16 Pages 3491—3508
DOI https://doi.org/10.2147/JIR.S422002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Dishiwen Liu,1– 3,* Yajia Li,1– 3,* Qingyan Zhao1– 3
1Department of Cardiology, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 2Cardiovascular Research Institute, Wuhan University, Wuhan, 430060, People’s Republic of China; 3Hubei Key Laboratory of Cardiology, Wuhan, 430060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingyan Zhao, Department of Cardiology & Cardiovascular Research Institute Renmin Hospital of Wuhan University, 238 Jiefang Road, Wuchang District, Wuhan, Hubei, 430060, People’s Republic of China, Tel +86- 027 88041911, Fax +86- 027 88042292, Email [email protected]
Abstract: Atrial fibrillation (AF) poses a serious healthcare burden on society due to its high morbidity and the resulting serious complications such as thrombosis and heart failure. The principle of catheter ablation is to achieve electrical isolation by linear destruction of cardiac tissue, which makes AF a curable disease. Currently, catheter ablation does not have a high long-term success rate. The current academic consensus is that inflammation and fibrosis are central mechanisms in the progression of AF. However, artificially caused inflammatory cell death by catheter ablation may have a significant impact on structural and electrical remodeling, which may affect the long-term prognosis. This review first focused on the inflammatory response induced by apoptosis, necrosis, necroptosis, pyroptosis, ferroptosis and their interaction with arrhythmia. Then, we compared the differences in cell death induced by radiofrequency ablation, cryoballoon ablation and pulsed-field ablation. Finally, we discussed the structural and electrical remodeling caused by inflammation and the association between inflammation and the recurrence of AF after catheter ablation. Collectively, pulsed-field ablation will be a revolutionary innovation with faster, safer, better tissue selectivity and less inflammatory response induced by apoptosis-dominated cell death.
Keywords: atrial fibrillation, inflammatory cell death, radiofrequency ablation, cryoballoon ablation, electroporation
Introduction
Atrial fibrillation (AF) is a common arrhythmia with high morbidity and mortality.1 Without proper intervention, this arrhythmia may develop into a permanent condition. Current therapeutic regimens include catheter ablation and drug therapy. Although antiarrhythmic drugs can help maintain sinus rhythm, most of them are ineffective and associated with intolerable side effects. AF and heart failure are closely related and mutually reinforcing. Evidence supported that catheter ablation reduces all-cause mortality in patients with AF combined with heart failure compared with drug therapy.2
Since Haissaguerre identified the pulmonary veins as the main trigger of AF,3 isolation of the electrical activity of the pulmonary veins by utilizing various form of energy (radiofrequency, cryoballoon, laser, ultrasound, pulsed-field) has become the cornerstone of catheter ablation. The primary goal of catheter ablation is to eliminate the symptoms associated with AF and improve quality of life. However, numerous clinical evidences have shown that the success rate of catheter ablation is not very high. After weighing complications such as atrioesophageal fistula, cardiac tamponade, phrenic nerve injury, esophageal injury, and pulmonary vein contracture, catheter ablation is not a routine choice as a first-line option.4 This awkward positioning of catheter ablation suggests that there is much room for improvement and optimization.
Catheter ablation leads to the membrane-breaking cell death of localized cardiomyocytes, releasing diverse bioactive substances. Undoubtedly, the local pro-inflammatory microenvironment may create a substrate for structural and electrical remodeling. This review will focus on the possible inflammatory response induced by cell death as well as arrhythmias, and attempt to clarify the differences in catheter ablation induced cell death at a microscopic level, with a view to translate the available evidence into clinical guides.
Cell Death and AF
Excessive cardiomyocytes death with limited regenerative capacity leads to a variety of cardiac diseases, including myocardial infarction, malignant arrhythmia, heart failure, and sudden cardiac death. Currently, known modes of cell death include, but are not limited to, apoptosis, necrosis, necroptosis, pyroptosis, and ferroptosis, which occur independently and interact with each other. Dead cells can exhibit features of autophagy, apoptosis, pyroptosis, and necrosis simultaneously.5 Except for apoptosis, all other membrane-breaking cell deaths (necrosis, necroptosis, pyroptosis, and ferroptosis) all occur in conjunction with an inflammatory response. More importantly, the loss of cardiomyocytes may not only imply diminished systolic function, but also activate the cascade of inflammatory responses, which may further contribute to the development of arrhythmia (Figure 1). Additionally, arrhythmia can exist as a single or cardiomyopathy-related disorder, and myocardial injury associated with arrhythmia is usually accompanied by a temporary or permanent inflammatory response.6
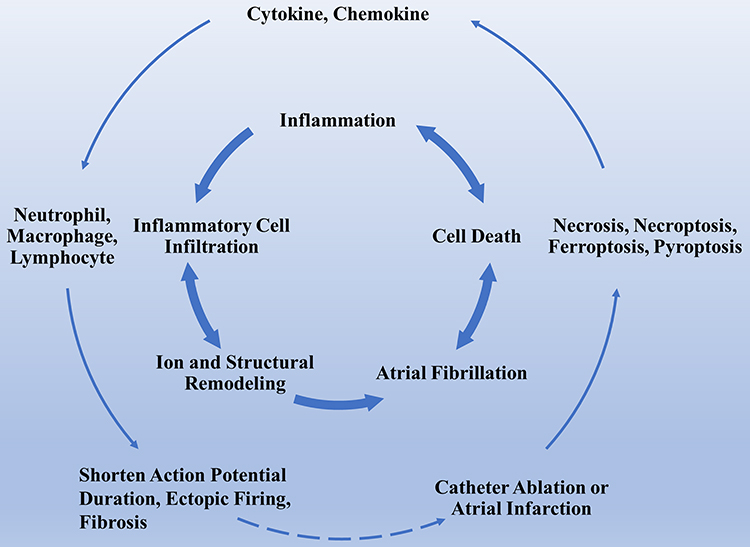 |
Figure 1 The association between inflammatory cell death and AF. This figure briefly recapitulates the association between inflammatory cell death and AF induce inflammatory cell death. Inflammatory cell death caused by artificial therapeutic regimens releases inflammatory factors that lead to structural and electrical remodeling, thereby contributing to the permanent progression of the arrhythmia. The cross-link between AF and inflammatory cell death creates a vicious loop. Abbreviation: AF, atrial fibrillation. |
Apoptosis and AF
Apoptosis is required for the clearance of damaged or senescent cells. Since 1972, the ultra-structural features of apoptosis have been characterized as the integrity of the cell membrane structure and the absence of a significant inflammatory response.7 Apoptosis has been shown to be associated with ischemia/reperfusion (I/R) injury, heart failure, and atherosclerosis. In 1994, evidence of apoptosis in the I/R myocardial tissue of rabbits was obtained by transmission electron microscopy and DNA gel electrophoresis.8 Apoptosis was present in the sinoatrial node, atrioventricular node, and conduction tissues during embryonic development and the postnatal weeks of development. Excessive, insufficient, or delayed apoptosis can cause arrhythmia.9 James et al observed typical apoptosis in surgically resected sinus nodes in patients who were recurrent ventricular arrhythmia combined with syncopal long Q-T syndrome, suggesting that arrhythmia is implicated in apoptosis, with limited, non-inflammatory degeneration in the sinus node.10 Thus, an imbalance of apoptosis may underlie the pathogenesis of some arrhythmia.
Sustained tachycardia and rapid pacing promote cardiomyocytes apoptosis, which have been corroborated by extensive clinical data.11–13 Knocking down caspase-3 in a porcine AF model could prevent intra-atrial conduction delay and inhibit the development of sustained AF.14 Additionally, ATG5 and M30, which are associated with autophagy and apoptosis, were elevated in the serum of patients with paroxysmal AF.15 Besides, epicardial isolation of pulmonary veins also reduced the apoptosis indicators in AF.16
Apoptosis may be the ultimate culmination of various unfavorable stimuli. However, how apoptosis without inflammatory response contributes to the progression of AF has not been investigated clearly. A possible explanation is that widespread apoptosis of cardiomyocytes or conduction system implies a weakening of atria contractile function which causes the atria to enlarge, ultimately leading to structural remodeling and electrical remodeling.
Necrosis and AF
Necrosis is usually considered a non-programmed, unregulated cell death process resulting from exposure to external violent stimuli or severe imbalance in the homeostasis of the internal environment. Necrosis is characterized by cell swelling, rupture, and spillage of cell contents, which triggers an inflammatory response.
Necrotic myocardium can trigger innate and adaptive immunity.17 Damage-associated molecular patterns (DAMP) bind to pattern recognition receptors to induce activation of downstream signaling pathways on cardiomyocytes or resident immune cells (Figure 2). Many DAMPs have been identified, including high-mobility group box 1 (HMGB1), uric acid, double-stranded DNA, amyloid-β-peptide, heat shock proteins (HSP), interleukin-1α (IL-1α), and IL-33. Ultimately, the cascade leads to the upregulation of chemokines and cytokines.18 The inflammatory response is also exacerbated because of elevated fibrinogen, fibronectin, bilirubin, metallopeptidase 2 (MMP-2), tissue inhibitors of metalloproteinase 2 (TIMP-2), and thrombospondin 2 in neutrophils or polarized macrophages.19–21
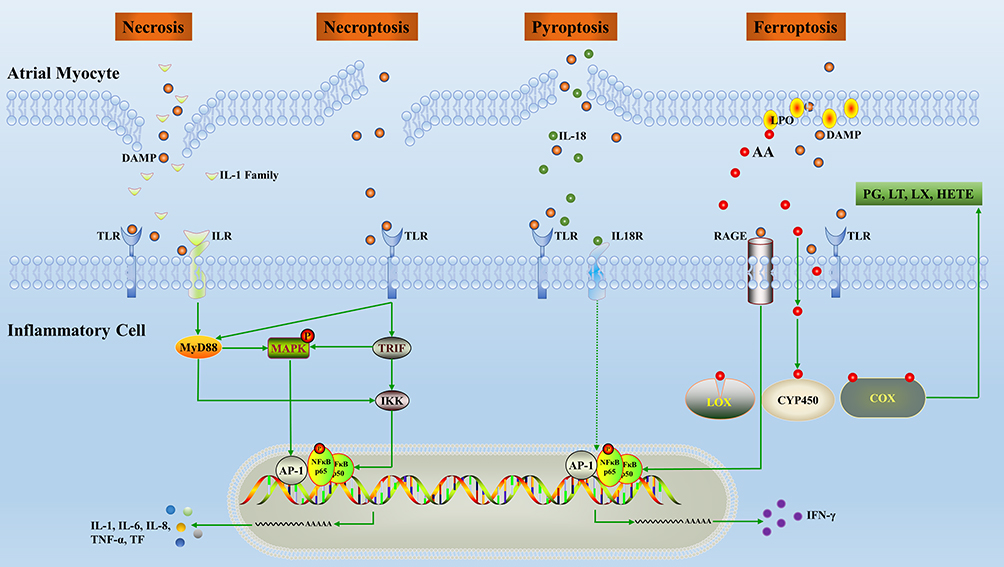 |
Figure 2 Overview of the inflammatory pathways induced by inflammatory cell death. Release of inflammatory factors, mainly DAMPs, following cardiomyocytes death promotes polarization and chemotaxis of inflammatory cells. In turn, inflammatory cells secrete inflammatory factors which alter the structure and electrical conduction activity of the local microenvironment. Abbreviations: AA, arachidonic acid; TF, tissue factor; AP, activating protein; NF, nuclear factor; IFN, interferon; IL, interleukin; PG, prostaglandin; LT, leukotriene; LX, lipoxin; CYP450, cytochrome P450; MyD, myeloid differentiation factor; LOX, lipoxygenase; COX, cyclooxygenase; TNF, tumor necrosis factor; IKK, inhibitor of kappa B kinase; TLR, toll-like receptors; LPO, lipid hydroperoxide; DAMP, damage-associated molecular patterns; RAGE, the receptor of advanced glycation end products; HETE, hydroxyeicosatetraenoic acid; MAPK, mitogen-activated protein kinase; TRIF, TIR-domain-containing adaptor inducing interferon β. |
There are few direct studies of necrosis on arrhythmia, but we can draw an analogy to myocardial infarction as a more severe form of myocardial necrosis. Studies have found that larger infarct sizes in the heart are more prone to arrhythmia.22–24 The cumulative morbidity of AF over 5 years after acute myocardial infarction is 6%-21%, compared to 3% in the general population.25 Recent studies have shown that the morbidity of supraventricular tachycardia in atrial infarction patients is 27%.26 A prospective cohort study has shown that artificial atrial coronary occlusion causes atrial arrhythmias and delayed intra-atrial conduction.27 Moreover, the more atrial branches are blocked, the higher morbidity of AF.28,29 It has been verified that atrial infarction is associated with slower atrial conduction velocity, increased conduction heterogeneity, increased susceptibility to AF, and a longer duration of AF.30 Coincidentally, in the canine model of chronic atrial infarction, researchers found an approximately 50-fold increase in spontaneous atrial ectopic activity and conduction abnormalities, and significant fibrosis at the border of the atrial infarct region. Patch-clamp implied that the initiating activity of atrial myocytes in infarct boundary areas was enhanced, with faster decay of caffeine-induced Ca2+ transients and enhanced Na+-Ca2+ exchange currents.31 A refined study by Uma et al reported that ligation of the atrial branch of the left anterior descending coronary artery resulted in spontaneous AF. Optical mapping observed focal spontaneous discharges and conduction delays at the border of the ischemic/normal zone, which provided substrates for reentry. The possible mechanism involved is that the physiological binding of calmodulin to ryanodine receptor type 2 (RyR) is altered by hypoxic and inflammatory responses.32 Taken together, these results suggest that local myocardial tissue necrosis has profound effects on electrophysiology. However, little is known about whether catheter ablation of the pulmonary veins and extensive linear ablation in the atria could cause atrial infarction by damaging the corresponding arteries and whether it has any effect on the recurrence of AF after the procedure.
Of course, researchers have also conducted a series of mechanistic explorations to find interventions. Previous research prompted that C1q/TNF-related protein 9 may reduce atrial inflammation and fibrosis effectively and reduce the incidence of concomitant AF after myocardial infarction through its inhibitory effects on TLR4/NF-κB and Smad2/3 signaling pathways.33 Relaxin exerts beneficial anti-fibrotic and anti-inflammatory effects and reduces the susceptibility of AF after myocardial infarction.34
Necroptosis and AF
Necroptosis is a newly discovered mechanism of cell death that combines the features of necrosis and apoptosis.35 A cascade of physicochemical factors stimulates the activation of autophosphorylation of receptor-interacting serine/threonine protein kinase. It leads to the release of DAMPs, which promote the inflammatory response (Figure 2).
Several studies have shown that necroptosis plays an accelerating role in myocardial infarction, I/R injury, and heart failure.36–38 Inhibition of necroptosis was found to reduce the susceptibility to CaCl2-acetylcholine or high lipid-induced AF and reverse structural remodeling of the atria.39 TGF-β activated kinase 1 acts as a key survival factor by antagonizing necroptosis directly, which is essential for maintaining myocardial homeostasis and preventing unfavorable myocardial remodeling.40 A recent study demonstrated that tumor necrosis factor receptor-associated factor 2-mediated NF-κB independent pro-survival pathway inhibited necrotic signaling, and it could be used as a therapeutic target for ventricular remodeling and heart failure.37 More studies are needed to gain a better understanding of the relationship between necroptosis and arrhythmia.
Ferroptosis and AF
Ferroptosis is a regulated cell death characterized by iron-dependent lipid peroxidation (LPO) accumulation.41 Ferroptosis has been shown to release mitochondrial and intranuclear material,42 but the study of inflammation in ferroptosis is still in the early stage.43
Ferroptotic cells were found to be extremely pro-inflammatory by recruiting macrophages through chemokine ligand 2.44 Ferroptotic cells release HMGB145 and anti-HMGB1-neutralizing antibodies mitigated the inflammatory response of macrophages.46 Inhibition of ferroptosis has been reported to inhibit leukocyte extravasation.47 The activation of the toll-like receptors (TLR) inflammatory response led to neutrophil accumulation and myocardial injury in cardiac transplantation, and Ferrostatin (selective ferroptosis inhibitor) reversed this alteration.48 4-hydroxynonenal, which is the LPO product, is a ligand for the TLR4 receptor and triggers an inflammatory response.49 In addition, LPO drives an increase in modified low-density lipoprotein, which promotes inflammation through macrophage polarization.50 Reducing glutathione peroxidase 4 (GPX4) expression up-regulates the expression of 12-lipoxygenase (ALOX12) and cyclooxygenase 1 (COX-1).51,52 (Figure 2) In contrast, GPX4 activation inhibits ferroptosis and inflammatory responses by attenuating arachidonic acid oxidation and NF-κB pathway activation.53 Arachidonic acid is an unsaturated fatty acid that is metabolized by COX, LOX, cytochrome P450, and monooxygenases to synthesize biologically active inflammatory mediators such as prostaglandins, leukotrienes, epoxyeicosatrienoic acid, and hydroxyeicosatetraenoic acid.54 Excessive reactive oxygen species (ROS) and iron overload are strongly associated with arrhythmia.55,56 A recent study reported that SARS-CoV-2 induced ferroptosis, leading to the dysfunction of human embryonic stem cell-derived sinoatrial node-like pacemaker cells.57 AF is a common cause of death in β-thalassemia patients, and it can be hypothesized that the presence of ferroptosis in β-thalassemia patients promotes the development of AF.58 Basic research hinted that rapid pacing cardiac fibroblast-derived exosomes exacerbated cardiomyocytes ferroptosis, and AF could be prevented by intervening in exosomal miRNAs.59 In addition, LPS-induced endotoxemia,60 excessive alcohol consumption,61 and obesity-related gut flora dysbiosis62 could increase AF susceptibility through ferroptosis.
Pyroptosis and AF
Pyroptosis is an inflammatory form of programmed cell death involving the activation of caspase-1 by the inflammasome. Pyroptosis exhibits a plasma membrane blistering morphology and therefore is usually considered a monocyte-specific form of apoptosis. However, the recent discovery of Gasdermin-D of pore-forming activity, which is a key executor of pyroptosis, has redefined pyroptosis as a necrotic form of cell death.
Pyroptosis is a type of pro-inflammatory cell death that is closely associated with the activation of NOD-like receptor thermal protein domain associated protein 3 (NLRP3) inflammasome and is intensively involved in AF.63 A previous report claimed the NLRP3 inhibitor glibenclamide reversed atrial remodeling partially and prevented AF in diabetic rabbits.64 Yao et al found that NLRP3 inflammasome activity was enhanced significantly in atrial myocytes from AF patients and dogs with atrial tachycardia pacing.63 Over activation of the NLRP3 signaling pathway promotes the expression of apoptotic mechanisms mediated by RyR2 and caspase-1, resulting in increased Ca2+ release from the sarcoplasmic reticulum and increased secretion of inflammatory cytokines.63,65 At the same time, enhanced transcription of Kcna5 leads to an increase of Kv1.5-current, shortening the effective refractory period and forming a reentry substrate.63 Cold exposure increased trimethylamine N-oxide by enhancing gut-derived trimethylamine production, which promoted M1 macrophage infiltration, induced the pyroptosis of cardiomyocytes in rats, exacerbates atrial structural remodeling, and ultimately led to AF.66 LncRNA x–inactive specific transcript (XIST) may promote Arl2 expression through the uptake of miR-214-3p to blunt the pyroptosis of cardiomyocytes, providing encouraging insights for XIST-based AF-targeted therapy.67
Pulsed-Field Ablation (PFA) versus Conventional Catheter Ablation
Catheter ablation has formed a scenario in which radiofrequency ablation (RFA) is the mainstay, supplemented by cryoballoon, laser, and ultrasound ablation during the past decades. The success rates of RFA, cryoballoon ablation (CBA), and PFA for paroxysmal AF within 1 year are 61.1%–92%, 51.7%–88% and 66.2%–90% respectively (Table 1). Although a shoulder-to-shoulder comparison of the effectiveness of RFA and PFA is not yet available, the published data from small samples of PFA is worth envisioning. Unlike RFA and CBA, which use extreme temperatures to destroy myocardial tissue, PFA utilizes strong electric fields to disrupt the phospholipid bilayer integrity of cell membranes or organelles to induce cell death.68 Cardiomyocytes have the lowest electroporation threshold of all tissues, which makes this technique particularly appropriate for cardiac ablation.69 This difference in sensitivity between cardiomyocytes and other non-target tissues may reduce the risk of collateral damage to the esophagus and phrenic nerve.
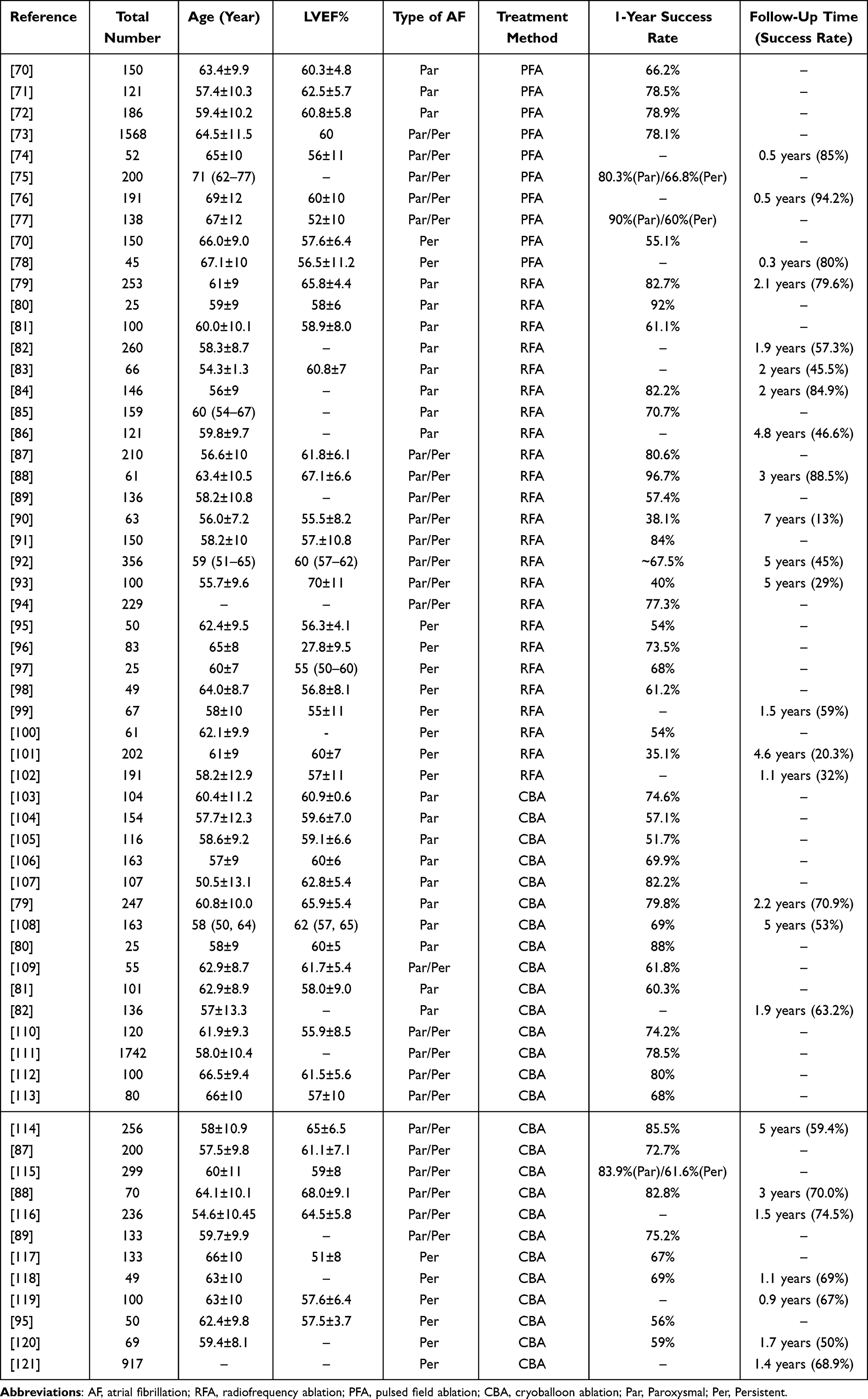 |
Table 1 Summary of Success Rate After Different Ablation Procedures of Atrial Fibrillation |
Cell Death in RFA and CBA
RFA uses radiofrequency currents to generate high temperature to cause damage to the target tissue, while CBA uses argon to absorb surrounding heat as it expands rapidly to cause a rapid drop in the temperature of the surrounding tissue. Both RFA and CBA are energy-based ablations that utilize extreme temperatures, resulting in irreversible cellular damage.
RFA causes a high temperature and then transmits it to the surrounding tissues, forming the main characteristic lesion centered on coagulative necrosis. When the temperature exceeds 60 °C, the time to reach irreversible damage decreases exponentially. The inactivation of important enzymes is the initial feature of the damage, and proteins are denatured quickly and followed by cytotoxicity causing coagulative necrosis (Figure 3). At temperatures around 40–45 °C, irreversible cellular damage only occurs with prolonged exposure (30–60 minutes). Temperature gradients caused by catheter can induce apoptosis and lead to the progression of injury. Besides, stimulation of apoptosis can be triggered by various cytokines and can induce direct alterations in the tissue microenvironment.122 In particular, endothelial pyroptosis after RFA of liver tissue has been reported to be closely associated with systemic inflammatory response syndrome, confirming that pyroptosis occurs with thermal injury.123,124 There is little ferroptosis reported from RFA or thermal injury. However, ferroptosis mediated alkali burn-induced corneal injury has been reported in ophthalmology.125 In sum, cell death in the injury zone is a complex process and various types of cell death may need to be further explored.
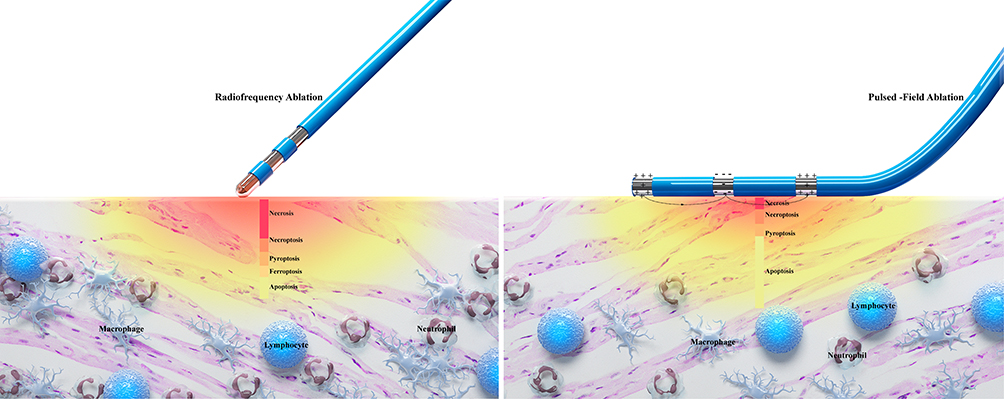 |
Figure 3 Comparison of cell death patterns due to RFA and PFA. RFA causes damage by localized cell necrosis, whereas PFA causes damage by apoptotic cell death. By comparing the schematic diagrams, RFA causes widespread necrosis, and the area of necrosis may contain patterns of death including necrosis, necroptosis, pyroptosis, and ferroptosis. A large accumulation of inflammatory cells such as neutrophils, monocytes and lymphocytes are chemotactic to the migrated area, which in turn induces a strong inflammatory response. Whereas the necrosis by PFA is limited to the area close to the catheter, the wider damage is predominantly apoptotic. There is also relatively little infiltration of inflammatory cells in the migratory zone. Abbreviations: RFA, radiofrequency ablation; PFA, pulsed field ablation. |
CBA creates an injury similar to RFA, a pattern of injury centered on necrosis.126 Ice crystals can form inside and outside the cells during CBA and are accelerated by nucleation. Spontaneous nucleation of cells can occur at −5°C to −15°C.127 The percentage of intracellular ice increases during rapid temperature reduction. Cell damage occurs due to shearing, and the damage caused during rapid temperature reduction is lethal.128 Animal studies verified that the sublethal temperature in the peripheral zone causes cells to activate apoptosis.129,130 Regrettably, the existence of other types of cell death in the migratory region has not yet been reported clearly.
Cell Death in PFA
Unlike RFA and CBA, which are energy-based ablations, PFA uses multiple strong pulses to generate an electric field that causes irreversible cell membrane damage.131 Electric fields are most commonly generated by a high-voltage direct current delivered between two or more electrodes. When a sufficiently strong electric field is applied to a cell and increases the permeability of its membrane, electroporation occurs, leading to increased ion transport and overall membrane instability.132 Its nonthermal mechanism of ablation allows PFA to ablate the atrial myocardium because it has a lower threshold for injury compared to the phrenic nerve and esophagus which are close to the heart. At a certain distance from the electrode, there will be an area of tissue at the PFA threshold that forms the edge of the lesion. With the use of higher voltages or increasing other exposure metrics (including pulse duration and the number of pulses), the lesion volume will increase. Cell death due to field exposure above the PFA threshold and permanent hyperpermeability is attributed to adenosine triphosphate depletion, ion channel failure, calcium overload, and a general loss of intracellular homeostasis.133–135
This non-thermal damage maintains the integrity of the extracellular matrix and thus reduces structural remodeling. Apoptosis has been reported widely as the most common form of cell death by PFA.136 (Figure 3) Animal models showed that the injury zone is delineated well and bounded by the surrounding tissue clearly.137 This ensures that tissues outside the lesion are less affected during ablation and reduces the occurrence of inflammation. The PFA delivery energy is determined by the voltage, the pulse duration, and the number of pulses. In the region close to the electrodes, where the electric field reaches high amplitude, cells may undergo thermal damage.138,139 Sometimes, PFA-ablated tissues experience necrosis, pyroptosis, or necroptosis rather than apoptosis.140–142 Therefore, appropriate electroporation parameters could mitigate the degree of necrosis and the inflammatory response.
Inflammation and AF
The inflammatory response in local myocardial tissue leads to structural remodeling, which slows down atrial myocardial conduction velocity and prolongs the effective induction period, ultimately leading to the AF toward permanent arrhythmia. In patients with an acute systemic inflammation such as sepsis, the morbidity of AF can be up to 23%.143 In patients with more severe septic shock, the morbidity of new-onset AF can be up to 46%.144 Other chronic systemic inflammatory diseases such as rheumatoid arthritis,145 psoriasis,146 and inflammatory bowel disease147 have all reported high incidences of AF. In addition, AF can lead to the release of inflammatory factors. Elevated IL-6 and tumor necrosis factor (TNF) were detected in both atrial tissue and peripheral blood in canines with atrial rapid pacing.148 Recent studies have shown that T-cell-mediated inflammation can be regulated by modulating gut flora, which reduces atrial structural remodeling in turn and the development of age-related AF.149
In addition to elevated serum inflammatory factors in AF, the local inflammatory status of myocardial tissue was also validly assessed. Epicardial adipose tissue from persistent AF patients expressed IL-1β in large abundances at the transcriptional level.150 High expression of tissue factors was produced by inflammatory stimuli in the left atrial appendage obtained from AF patients.151 Narducci et al showed high expression of CRP in atrial septum specimens from patients with paroxysmal AF.152 Local inflammation produces abundantly pentraxin 3. Markedly elevated pentraxin 3 expression by serology and immunohistochemistry confirmed an increased local inflammatory burden in AF.153
Inflammation and Electrical Remodeling
Inflammatory cytokines such as platelet derived growth factor (PDGF), IL-2, and TNF-α regulate cellular ion channels and calcium homeostasis. PDGF from myofibroblasts can reduce the action potential duration and Ca2+ transients.154 TNF-α can increase the potential for pulmonary veins to cause arrhythmogenesis and induce abnormalities in calcium homeostasis, leading to inflammation-associated AF.155 It has been shown that mice overexpressing TNF-α have prolonged action potentials and Ca2+ transients, higher diastolic Ca2+ currents, and lower systolic Ca2+ currents.156,157
Inflammation, in addition to regulating cellular ion channels and calcium homeostasis, has been associated with the heterogeneity of atrial conduction. Heterogeneous conduction may be the result of altered expression or distribution of connexin (Cx) 40, Cx43, or atrial fibrosis. In a canine model of aseptic pericarditis, reduced expression and transmural gradients of Cx40 and Cx43 (both absent in the epicardium, reduced in the pericardium, and normal in the endocardium) were associated with marked atrial conduction abnormalities and the induction and maintenance of AF.158 One study found that the serum IL-6 level is negatively correlated with the expression level of Cx43. The expression of Cx40 and Cx43 decreased rapidly after direct exposure of IL-6 to HL-1 cells, and their expression recovered rapidly after the cessation of IL-6 exposure.159 Ishii et al found that the degree of atrial inflammation was associated with the atrial conduction heterogeneity and the duration of AF.160 Topical application of arachidonic acid to the atria of canines produced heterogeneous conduction, whereas methyl-prednisolone reversed it.161 Additionally, endurance athletes have increased risk for AF, and a longitudinal study of athletes participating in marathons found that prolonged signal-averaged P-wave duration was accompanied by transient increases of high-sensitivity C-reactive proteins (hs-CRP), pro-inflammatory cytokines, leukocytes, neutrophils, pro-cardiac natriuretic peptide, and high-sensitivity troponin, suggesting that acute changes in inflammatory cytokines are associated with atrial electrical conduction and susceptibility to AF.162
Inflammation and Structural Remodeling
Inflammation is also closely related to structural remodeling of the heart, and clinical and experimental studies of AF have revealed that atrial fibrosis is the most important histopathological change in AF.163 PDGF-A promotes cell proliferation and collagen expression in cardiac fibroblasts and increases susceptibility to atrial fibrosis and AF, which can be reversed by mast cell stabilizers and PDGF-A blockers.164 PDGF and its receptors are expressed in atrial fibroblasts more strongly compared to ventricular fibroblasts. Whereas induction of HSPs, especially HSPA1A, attenuates the remodeling of atrial substrates.165 TNF-α/TGF-β signaling pathway could increase secretion of MMPs which is involved in the pathogenesis of mouse atrial fibrosis.166 In contrast, anti-TNF-α treatment reduced the activation of MMP-2 and MMP-9 and prevented collagen synthesis and deposition.167 Recruitment of macrophages is critical for tissue fibrosis. Macrophages can stimulate IL-6 in cardiac fibroblasts, which leads to TGF-β1 in cardiac fibroblasts and the phosphorylation of Smad3, stimulating cardiac fibrosis.168 In clinical studies, high levels of CRP, IL-6, and IL-18 and low levels of HSP27 were associated with increased atrial size and susceptibility to AF, which further supports the role of inflammation in atrial remodeling.169–171
Inflammatory Response After Ablation Procedures
There is no doubt that invasive catheter ablation procedures impart inflammatory response to the tissue, but this inflammatory response may be intimately correlated with the form of energy.
The ablated tissue or cells and extracellular matrix may release pro-inflammatory cytokines.172 Serum levels of IL-1β, IL-6, IL-8, and TNF-α are shown to be elevated after RFA.173–175 Infiltration of inflammatory cells such as neutrophils, macrophages, dendritic cells, and natural killer cells has been reported in migratory zone.176–178 There is controversy regarding the cellular damage and inflammatory response produced after CBA. Some studies have shown a weak systemic inflammatory response after CBA,179 while others have shown comparable cellular damage and inflammatory response between CBA and RFA.180 Antolič et al found that myocardial damage was more pronounced with CBA than RFA. However, there was no significant difference between the two ablation techniques in terms of inflammatory response and coagulation activation.181 Nonetheless, Shinsuke et al found that RFA and CBA groups had comparable peak blood hs-CRP and produced comparable inflammatory responses, and CBA caused greater myocardial damage.182
The inflammatory response after PFA has been less studied. Massimo et al reported a detailed histological analysis of atrial lesions after PFA and performed the first comparative study of the histological findings at 7 and 30 days, finding that the degree of tissue inflammation was evident at 7 days and reduced with almost no inflammatory cells observed at 30 days, indicating a shorter duration of the inflammatory response.183 Another study found that significant ablation-related necrosis, inflammation and fibrosis were seen in all tissue sections of RFA compared with PFA, and they speculated that RFA causes a greater inflammatory burden compared with PFA.184 Comparing the inflammatory response generated by the organism after PFA and RFA in patients with hepatocellular carcinoma, it was found that the serum of macrophage migration inhibitory factor was elevated immediately after PFA, while this phenomenon was not observed in the RFA group, which may promote the early repair process after PFA and lead to a significant reduction of the ablation zone and alleviate the inflammatory burden in the organism.185 Further studies are still needed regarding the strength of the inflammatory response after different ablation procedures for AF.
There is little direct histological evidence of inflammation in local myocardial tissue post catheter ablation, mainly due to concerns about the safety of invasive myocardial biopsy procedures. However, advances in imaging technology have made it possible to assess atrial inflammation in a non-invasive manner. Xie et al proposed that 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET-CT) would reflect favorably the degree of inflammatory burden after catheter ablation.186 Late-gadolinium enhancement magnetic resonance imaging (LGE-MRI) is superior for assessing fibrosis as the final terminus of local inflammation. Clinical studies have reported that the higher the grade of fibrosis appraised by LGE-MRI after catheter ablation, the increased the rate of recurrence. In addition, enhanced CT assessment epicardial adipose tissue associated with local inflammation has been extensively utilized in clinical practice.187–189 Artificial intelligence algorithms can effectively predict the recurrence of AF after catheter ablation. By evaluating patient data, artificial intelligence algorithms can select the most effective AF treatment based on the patient’s unique characteristics.190 These tools considerably enrich the means of objectively appraise the local inflammatory response after catheter ablation. Early identification of excessive inflammatory responses and interventions facilitate a better prognosis.
Relationship Between Inflammation and Recurrence After Ablation Procedures
The primary goal of catheter ablation is to eliminate triggers that cause fibrillation, such as reentry, or to eliminate areas that lead to multiple depolarization, but it does not address the underlying process of myocardial remodeling.
The report published by Andrade et al suggested that early recurrence is thought to be due to inadequate early structural remodeling after pulmonary vein isolation (PVI), leading to leakage of the electrical impulses. Late recurrence may be the ectopic foci shifting from the pulmonary veins to other sites.191 In addition to other comorbidities, there is a fact that the levels of markers associated with myocardial injury like creatine kinase, creatine kinase-MB and troponin are high after catheter ablation.192 Troponin has been shown to be the most sensitive marker for detecting myocardial injury.193 A systemic review found that the level of troponin was closely associated with AF recurrence after RFA.194 During PVI, both radiofrequency ablation and cryoballoon ablation indiscriminately damage myocardial tissue, including blood vessels, nerves and myocardium. Complete PVI inevitably damages the left coronary artery branch, and stenosis with thrombosis causes myocardial tissue damage to extend from the ablation line to other areas. As mentioned above, ectopic foci activity is enhanced by subsequent atrial infarction and inflammation. The increase of local inflammation after catheter ablation may contribute to recurrence.
Several studies identified lymphocytes/neutrophils as a reliable predictor of recurrence after catheter ablation.195,196 Galectin-3 is a biomarker of AF that mediates atrial inflammation and may reflect progressive atrial fibrosis in AF. More studies have shown that galectin-3 is an independent predictor of recurrence after catheter ablation of AF,197–199 and Takemoto et al demonstrated that inhibition of galectin-3 could improve outcomes in persistent AF treated with catheter ablation.200 Besides, it has been reported that uric acid/albumin,201 myeloperoxidase,202,203 monocyte/HDL,204 TLR4,205 MMP-2 and TNF-α,206 and CRP207 were associated with higher recurrence after catheter ablation. The inhibitory effects of anti-inflammatory drugs such as steroids, colchicine, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, and statins on AF are summarized in a review by Kensuke et al in detail.208 In addition, the AntaEP study indicated that antazoline may be suitable for pharmacological cardioversion of AF occurring during PVI, hinting the potential participation of histamine in the progression of AF.209
Conclusion
Inflammatory cell death is strongly associated with the development and recurrence of AF. Therefore, avoiding inflammatory and unnecessary cell death in myocardial tissue is essential to prevent the recurrence of AF. In the current review, PFA, a new energy source of non-thermal irreversible electroporation, has great advantages over traditional catheter ablation. From the cellular perspective, catheter ablation uses extreme temperatures to cause necrosis of diseased tissues and cells, and the inflammatory response generated places a certain burden on the organism. In contrast, PFA benefits patients by protecting adjacent tissues and inducing apoptosis with a less inflammatory response on the organism while ensuring significant efficacy of durable PVI. However, different parameters cause different types of cell death in the tissues. There is still a lack of clinical trials on PFA, and further research is needed to investigate its safety and effects.
Funding
This work was supported by National Natural Science Foundation of China (81970277, 82170312).
Disclosure
Dishiwen Liu and Yajia Li are co-first authors for this study. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Santhanakrishnan R, Wang N, Larson MG, et al. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation. 2016;133(5):484–492. doi:10.1161/CIRCULATIONAHA.115.018614
2. Şaylık F, Çınar T, Akbulut T, Hayıroğlu M. Comparison of catheter ablation and medical therapy for atrial fibrillation in heart failure patients: a meta-analysis of randomized controlled trials. Heart Lung. 2023;57:69–74.
3. Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659–666. doi:10.1056/NEJM199809033391003
4. Nogami A, Kurita T, Abe H, et al. JCS/JHRS 2019 guideline on non-pharmacotherapy of cardiac arrhythmias. Circ J. 2021;85(7):1104–1244. doi:10.1253/circj.CJ-20-0637
5. Li P, Dong XR, Zhang B, et al. Molecular mechanism and therapeutic targeting of necrosis, apoptosis, pyroptosis, and autophagy in cardiovascular disease. Chin Med J. 2021;134(22):2647–2655. doi:10.1097/cm9.0000000000001772
6. Ji N, Qi Z, Wang Y, et al. Pyroptosis: a new regulating mechanism in cardiovascular disease. J Inflamm Res. 2021;14:2647–2666. doi:10.2147/jir.S308177
7. Kerr JF, Wyllie AH, Currie AR. Apoptosis: a basic biological phenomenon with wide-ranging implications in tissue kinetics. Br J Cancer. 1972;26(4):239–257. doi:10.1038/bjc.1972.33
8. Gottlieb RA, Burleson KO, Kloner RA, Babior BM, Engler RL. Reperfusion injury induces apoptosis in rabbit cardiomyocytes. J Clin Invest. 1994;94(4):1621–1628. doi:10.1172/jci117504
9. James TN. Normal and abnormal consequences of apoptosis in the human heart. From postnatal morphogenesis to paroxysmal arrhythmias. Circulation. 1994;90(1):556–573.
10. James TN, Terasaki F, Pavlovich ER, Vikhert AM. Apoptosis and pleomorphic micromitochondriosis in the sinus nodes surgically excised from five patients with the long QT syndrome. J Lab Clin Med. 1993;122(3):309–323.
11. Kuramochi Y, Guo X, Sawyer DB, Lim CC. Rapid electrical stimulation induces early activation of kinase signal transduction pathways and apoptosis in adult rat ventricular myocytes. Exp Physiol. 2006;91(4):773–780. doi:10.1113/expphysiol.2006.033894
12. Aimé-Sempé C, Folliguet T, Rücker-Martin C, et al. Myocardial cell death in fibrillating and dilated human right atria. J Am Coll Cardiol. 1999;34(5):1577–1586. doi:10.1016/s0735-1097(99)00382-4
13. Zhao J, Li J, Li W, et al. Effects of spironolactone on atrial structural remodelling in a canine model of atrial fibrillation produced by prolonged atrial pacing. Br J Pharmacol. 2010;159(8):1584–1594. doi:10.1111/j.1476-5381.2009.00551.x
14. Trappe K, Thomas D, Bikou O, et al. Suppression of persistent atrial fibrillation by genetic knockdown of caspase 3: a pre-clinical pilot study. Eur Heart J. 2013;34(2):147–157. doi:10.1093/eurheartj/ehr269
15. Fedai H, Altiparmak IH, Tascanov MB, et al. The relationship between oxidative stress and autophagy and apoptosis in patients with paroxysmal atrial fibrillation. Scand J Clin Lab Invest. 2022;82(5):391–397. doi:10.1080/00365513.2022.2100274
16. Osmancik P, Peroutka Z, Budera P, et al. Decreased apoptosis following successful ablation of atrial fibrillation. Cardiology. 2010;116(4):302–307. doi:10.1159/000319619
17. Adamo L, Rocha-Resende C, Prabhu SD, Mann DL. Reappraising the role of inflammation in heart failure. Nat Rev Cardiol. 2020;17(5):269–285. doi:10.1038/s41569-019-0315-x
18. Mann DL, Topkara VK, Evans S, Barger PM. Innate immunity in the adult mammalian heart: for whom the cell tolls. Trans Am Clin Climatol Assoc. 2010;121:34–50.
19. Mouton AJ, DeLeon-Pennell KY, Rivera Gonzalez OJ, et al. Mapping macrophage polarization over the myocardial infarction time continuum. Basic Res Cardiol. 2018;113(4):26. doi:10.1007/s00395-018-0686-x
20. Daseke MJ, Valerio FM, Kalusche WJ, Ma Y, DeLeon-Pennell KY, Lindsey ML. Neutrophil proteome shifts over the myocardial infarction time continuum. Basic Res Cardiol. 2019;114(5):37. doi:10.1007/s00395-019-0746-x
21. Rurik JG, Aghajanian H, Epstein JA. Immune Cells and immunotherapy for cardiac injury and repair. Circ Res. 2021;128(11):1766–1779. doi:10.1161/circresaha.121.318005
22. Majidi M, Kosinski AS, Al-Khatib SM, et al. Reperfusion ventricular arrhythmia ‘bursts’ in TIMI 3 flow restoration with primary angioplasty for anterior ST-elevation myocardial infarction: a more precise definition of reperfusion arrhythmias. Europace. 2008;10(8):988–997. doi:10.1093/europace/eun123
23. Majidi M, Kosinski AS, Al-Khatib SM, et al. Reperfusion ventricular arrhythmia ‘bursts’ predict larger infarct size despite TIMI 3 flow restoration with primary angioplasty for anterior ST-elevation myocardial infarction. Eur Heart J. 2009;30(7):757–764. doi:10.1093/eurheartj/ehp005
24. van der Weg K, Majidi M, Haeck JD, et al. Ventricular arrhythmia burst is an independent indicator of larger infarct size even in optimal reperfusion in STEMI. J Electrocardiol. 2016;49(3):345–352. doi:10.1016/j.jelectrocard.2016.03.013
25. Belkouche A, Yao H, Putot A, et al. The multifaceted interplay between atrial fibrillation and myocardial infarction: a review. J Clin Med. 2021;10(2). doi:10.3390/jcm10020198
26. Bocharov AV, Popov LV, Lagkuev MD. The frequency of atrial infarction in patients with supraventricular arrhythmias. Kardiologiia. 2022;62(3):28–31. doi:10.18087/cardio.2022.3.n1648
27. Álvarez-García J, Vives-Borrás M, Gomis P, et al. Electrophysiological effects of selective atrial coronary artery occlusion in humans. Circulation. 2016;133(23):2235–2242. doi:10.1161/circulationaha.116.021700
28. Biccirè FG, Pastori D, Torromeo C, et al. Acute atrial ischemia associates with early but not late new-onset atrial fibrillation in STEMI patients treated with primary PCI: relationship with in-hospital outcomes. J Cardiol. 2021;78(5):368–374. doi:10.1016/j.jjcc.2021.05.013
29. Shiba T, Kondo Y, Senoo K, et al. Proximal occlusion in the right coronary artery involving the atrial branch as a strong predictor of new-onset atrial fibrillation in acute myocardial infarction. Int Heart J. 2019;60(6):1308–1314. doi:10.1536/ihj.18-713
30. Alasady M, Shipp NJ, Brooks AG, et al. Myocardial infarction and atrial fibrillation: importance of atrial ischemia. Circ Arrhythm Electrophysiol. 2013;6(4):738–745. doi:10.1161/circep.113.000163
31. Nishida K, Qi XY, Wakili R, et al. Mechanisms of atrial tachyarrhythmias associated with coronary artery occlusion in a chronic canine model. Circulation. 2011;123(2):137–146. doi:10.1161/circulationaha.110.972778
32. Avula UMR, Hernandez JJ, Yamazaki M, et al. Atrial infarction-induced spontaneous focal discharges and atrial fibrillation in sheep: role of dantrolene-sensitive aberrant ryanodine receptor calcium release. Circ Arrhythm Electrophysiol. 2018;11(3):e005659. doi:10.1161/circep.117.005659
33. Liu M, Li W, Wang H, et al. CTRP9 ameliorates atrial inflammation, fibrosis, and vulnerability to atrial fibrillation in post-myocardial infarction rats. J Am Heart Assoc. 2019;8(21):e013133. doi:10.1161/jaha.119.013133
34. Beiert T, Tiyerili V, Knappe V, et al. Relaxin reduces susceptibility to post-infarct atrial fibrillation in mice due to anti-fibrotic and anti-inflammatory properties. Biochem Biophys Res Commun. 2017;490(3):643–649. doi:10.1016/j.bbrc.2017.06.091
35. Zhou W, Yuan J. Necroptosis in health and diseases. Semin Cell Dev Biol. 2014;35:14–23. doi:10.1016/j.semcdb.2014.07.013
36. Koudstaal S, Oerlemans MI, Van der Spoel TI, et al. Necrostatin-1 alleviates reperfusion injury following acute myocardial infarction in pigs. Eur J Clin Invest. 2015;45(2):150–159. doi:10.1111/eci.12391
37. Guo X, Yin H, Li L, et al. Cardioprotective role of tumor necrosis factor receptor-associated factor 2 by suppressing apoptosis and necroptosis. Circulation. 2017;136(8):729–742. doi:10.1161/circulationaha.116.026240
38. Szobi A, Gonçalvesová E, Varga ZV, et al. Analysis of necroptotic proteins in failing human hearts. J Transl Med. 2017;15(1):86. doi:10.1186/s12967-017-1189-5
39. Fu Y, Jiang T, Sun H, et al. Necroptosis is required for atrial fibrillation and involved in aerobic exercise-conferred cardioprotection. J Cell Mol Med. 2021;25(17):8363–8375. doi:10.1111/jcmm.16796
40. Li L, Chen Y, Doan J, Murray J, Molkentin JD, Liu Q. Transforming growth factor β-activated kinase 1 signaling pathway critically regulates myocardial survival and remodeling. Circulation. 2014;130(24):2162–2172. doi:10.1161/circulationaha.114.011195
41. Dixon SJ, Lemberg KM, Lamprecht MR, et al. Ferroptosis: an iron-dependent form of nonapoptotic cell death. Cell. 2012;149(5):1060–1072. doi:10.1016/j.cell.2012.03.042
42. Friedmann Angeli JP, Schneider M, Proneth B, et al. Inactivation of the ferroptosis regulator Gpx4 triggers acute renal failure in mice. Nat Cell Biol. 2014;16(12):1180–1191. doi:10.1038/ncb3064
43. Proneth B, Conrad M. Ferroptosis and necroinflammation, a yet poorly explored link. Cell Death Differ. 2019;26(1):14–24. doi:10.1038/s41418-018-0173-9
44. Wang Y, Quan F, Cao Q, et al. Quercetin alleviates acute kidney injury by inhibiting ferroptosis. J Adv Res. 2021;28:231–243. doi:10.1016/j.jare.2020.07.007
45. Wen Q, Liu J, Kang R, Zhou B, Tang D. The release and activity of HMGB1 in ferroptosis. Biochem Biophys Res Commun. 2019;510(2):278–283. doi:10.1016/j.bbrc.2019.01.090
46. Luo X, Gong HB, Gao HY, et al. Oxygenated phosphatidylethanolamine navigates phagocytosis of ferroptotic cells by interacting with TLR2. Cell Death Differ. 2021;28(6):1971–1989. doi:10.1038/s41418-020-00719-2
47. Linkermann A, Skouta R, Himmerkus N, et al. Synchronized renal tubular cell death involves ferroptosis. Proc Natl Acad Sci U S A. 2014;111(47):16836–16841. doi:10.1073/pnas.1415518111
48. Li W, Feng G, Gauthier JM, et al. Ferroptotic cell death and TLR4/Trif signaling initiate neutrophil recruitment after heart transplantation. J Clin Invest. 2019;129(6):2293–2304. doi:10.1172/jci126428
49. Wang Y, Wang W, Yang H, Shao D, Zhao X, Zhang G. Intraperitoneal injection of 4-hydroxynonenal (4-HNE), a lipid peroxidation product, exacerbates colonic inflammation through activation of Toll-like receptor 4 signaling. Free Radic Biol Med. 2019;131:237–242. doi:10.1016/j.freeradbiomed.2018.11.037
50. Yu Y, Yan Y, Niu F, et al. Ferroptosis: a cell death connecting oxidative stress, inflammation and cardiovascular diseases. Cell Death Discov. 2021;7(1):193. doi:10.1038/s41420-021-00579-w
51. Chen CJ, Huang HS, Chang WC. Depletion of phospholipid hydroperoxide glutathione peroxidase up-regulates arachidonate metabolism by 12S-lipoxygenase and cyclooxygenase 1 in human epidermoid carcinoma A431 cells. FASEB J. 2003;17(12):1694–1696. doi:10.1096/fj.02-0847fje
52. Sakamoto H, Imai H, Nakagawa Y. Involvement of phospholipid hydroperoxide glutathione peroxidase in the modulation of prostaglandin D2 synthesis. J Biol Chem. 2000;275(51):40028–40035. doi:10.1074/jbc.M003191200
53. Li C, Deng X, Xie X, Liu Y, Friedmann Angeli JP, Lai L. Activation of glutathione peroxidase 4 as a novel anti-inflammatory strategy. Front Pharmacol. 2018;9:1120. doi:10.3389/fphar.2018.01120
54. Calder PC. Polyunsaturated fatty acids, inflammation, and immunity. Lipids. 2001;36(9):1007–1024. doi:10.1007/s11745-001-0812-7
55. Xie LH, Gwathmey JK, Zhao Z. Cardiac adaptation and cardioprotection against arrhythmias and ischemia-reperfusion injury in mammalian hibernators. Pflugers Arch. 2021;473(3):407–416. doi:10.1007/s00424-020-02511-0
56. Gordan R, Wongjaikam S, Gwathmey JK, Chattipakorn N, Chattipakorn SC, Xie LH. Involvement of cytosolic and mitochondrial iron in iron overload cardiomyopathy: an update. Heart Fail Rev. 2018;23(5):801–816. doi:10.1007/s10741-018-9700-5
57. Jacobs W, Lammens M, Kerckhofs A, et al. Fatal lymphocytic cardiac damage in coronavirus disease 2019 (COVID-19): autopsy reveals a ferroptosis signature. ESC Heart Fail. 2020;7(6):3772–3781. doi:10.1002/ehf2.12958
58. Nomani H, Bayat G, Sahebkar A, et al. Atrial fibrillation in β-thalassemia patients with a focus on the role of iron-overload and oxidative stress: a review. J Cell Physiol. 2019;234(8):12249–12266. doi:10.1002/jcp.27968
59. Liu D, Yang M, Yao Y, et al. Cardiac fibroblasts promote ferroptosis in atrial fibrillation by secreting exo-miR-23a-3p targeting SLC7A11. Oxid Med Cell Longev. 2022;2022:3961495. doi:10.1155/2022/3961495
60. Fang J, Kong B, Shuai W, et al. Ferroportin-mediated ferroptosis involved in new-onset atrial fibrillation with LPS-induced endotoxemia. Eur J Pharmacol. 2021;913:174622. doi:10.1016/j.ejphar.2021.174622
61. Dai C, Kong B, Qin T, et al. Inhibition of ferroptosis reduces susceptibility to frequent excessive alcohol consumption-induced atrial fibrillation. Toxicology. 2022;465:153055. doi:10.1016/j.tox.2021.153055
62. Kong B, Fu H, Xiao Z, Zhou Y, Shuai W, Huang H. Gut microbiota dysbiosis induced by a high-fat diet increases susceptibility to atrial fibrillation. Can J Cardiol. 2022. doi:10.1016/j.cjca.2022.08.231
63. Yao C, Veleva T, Scott L, et al. Enhanced cardiomyocyte NLRP3 inflammasome signaling promotes atrial fibrillation. Circulation. 2018;138(20):2227–2242. doi:10.1161/circulationaha.118.035202
64. Wu X, Liu Y, Tu D, et al. Role of NLRP3-inflammasome/caspase-1/galectin-3 pathway on atrial remodeling in diabetic rabbits. J Cardiovasc Transl Res. 2020;13(5):731–740. doi:10.1007/s12265-020-09965-8
65. Chen G, Chelu MG, Dobrev D, Li N. Cardiomyocyte inflammasome signaling in cardiomyopathies and atrial fibrillation: mechanisms and potential therapeutic implications. Front Physiol. 2018;9:1115. doi:10.3389/fphys.2018.01115
66. Luo Y, Zhang Y, Han X, et al. Akkermansia muciniphila prevents cold-related atrial fibrillation in rats by modulation of TMAO induced cardiac pyroptosis. EBioMedicine. 2022;82:104087. doi:10.1016/j.ebiom.2022.104087
67. Yan B, Liu T, Yao C, Liu X, Du Q, Pan L. LncRNA XIST shuttled by adipose tissue-derived mesenchymal stem cell-derived extracellular vesicles suppresses myocardial pyroptosis in atrial fibrillation by disrupting miR-214-3p-mediated Arl2 inhibition. Lab Invest. 2021;101(11):1427–1438. doi:10.1038/s41374-021-00635-0
68. Lavee J, Onik G, Mikus P, Rubinsky B. A novel nonthermal energy source for surgical epicardial atrial ablation: irreversible electroporation. Heart Surg Forum. 2007;10(2):E162–E167. doi:10.1532/hsf98.20061202
69. Ramirez FD, Reddy VY, Viswanathan R, Hocini M, Jaïs P. Emerging Technologies for Pulmonary Vein Isolation. Circ Res. 2020;127(1):170–183. doi:10.1161/circresaha.120.316402
70. Verma A, Haines DE, Boersma LV, et al. Pulsed field ablation for the treatment of atrial fibrillation: PULSED AF pivotal trial. Circulation. 2023. doi:10.1161/CIRCULATIONAHA.123.063988
71. Reddy VY, Dukkipati SR, Neuzil P, et al. Pulsed field ablation of paroxysmal atrial fibrillation: 1-year outcomes of IMPULSE, PEFCAT, and PEFCAT II. JACC Clin Electrophysiol. 2021;7(5):614–627. doi:10.1016/j.jacep.2021.02.014
72. Duytschaever MA-O, De Potter TA-OX, Grimaldi MA-O, et al. Paroxysmal atrial fibrillation ablation using a novel variable-loop biphasic pulsed field ablation catheter integrated with a 3-dimensional mapping system: 1-year outcomes of the multicenter inspIRE study. Circulation. 2023;16(3):e011780.
73. Turagam MA-O, Neuzil PA-O, Schmidt BA-O, et al. Safety and effectiveness of pulsed field ablation to treat atrial fibrillation: one-year outcomes from the MANIFEST-PF Registry. Circulation. 2023;2023:1.
74. Badertscher P, Weidlich S, Serban T, et al. Pulsed-field ablation versus single-catheter high-power short-duration radiofrequency ablation for atrial fibrillation: procedural characteristics, myocardial injury, and mid-term outcomes. Heart Rhythm. 2023. doi:10.1016/j.hrthm.2023.05.007
75. Urbanek LA-OX, Bordignon SA-O, Schaack DA-O, et al. Pulsed field versus cryoballoon pulmonary vein isolation for atrial fibrillation: efficacy, safety, and long-term follow-up in a 400-patient cohort. Circulation. 2023;16(7):389–398.
76. Schmidt B, Bordignon S, Tohoku S, et al. 5S study: safe and simple single shot pulmonary vein isolation with pulsed field ablation using sedation. Circ Arrhythm Electrophysiol. 2022;15(6):e010817. doi:10.1161/circep.121.010817
77. Lemoine MD, Fink T, Mencke C, et al. Pulsed-field ablation-based pulmonary vein isolation: acute safety, efficacy and short-term follow-up in a multi-center real world scenario. Clin Res Cardiol. 2022. doi:10.1007/s00392-022-02091-2
78. Davong B, Adeliño R, Delasnerie H, et al. Pulsed-field ablation on mitral isthmus in persistent atrial fibrillation: preliminary data on efficacy and safety. JACC. 2023. doi:10.1016/j.jacep.2023.03.021
79. Wei Y, Chen L, Cao J, et al. Long-term outcomes of a time to isolation - based strategy for cryoballoon ablation compared to radiofrequency ablation in patients with symptomatic paroxysmal atrial fibrillation. Pacing Clin Electrophysiol. 2022;45(9):1015–1023. doi:10.1111/pace.14556
80. Kühne M, Suter Y, Altmann D, et al. Cryoballoon versus radiofrequency catheter ablation of paroxysmal atrial fibrillation: biomarkers of myocardial injury, recurrence rates, and pulmonary vein reconnection patterns. Heart Rhythm. 2010;7(12):1770–1776. doi:10.1016/j.hrthm.2010.08.028
81. Wasserlauf J, Pelchovitz DJ, Rhyner J, et al. Cryoballoon versus radiofrequency catheter ablation for paroxysmal atrial fibrillation. Pacing Clin Electrophysiol. 2015;38(4):483–489. doi:10.1111/pace.12582
82. Mugnai G, Chierchia GB, de Asmundis C, et al. Comparison of pulmonary vein isolation using cryoballoon versus conventional radiofrequency for paroxysmal atrial fibrillation. Am J Cardiol. 2014;113(9):1509–1513. doi:10.1016/j.amjcard.2014.01.425
83. Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of paroxysmal atrial fibrillation (RAAFT-2): a randomized trial. JAMA. 2014;311(7):692–700. doi:10.1001/jama.2014.467
84. Cosedis Nielsen J, Johannessen A, Raatikainen P, et al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med. 2012;367(17):1587–1595. doi:10.1056/NEJMoa1113566
85. Luik A, Radzewitz A, Kieser M, et al. Cryoballoon versus open irrigated radiofrequency ablation in patients with paroxysmal atrial fibrillation: the prospective, randomized, controlled, noninferiority FreezeAF study. Circulation. 2015;132(14):1311–1319. doi:10.1161/circulationaha.115.016871
86. Ouyang F, Tilz R, Chun J, et al. Long-term results of catheter ablation in paroxysmal atrial fibrillation: lessons from a 5-year follow-up. Circulation. 2010;122(23):2368–2377. doi:10.1161/circulationaha.110.946806
87. Choi JH, Park SJ, Park KM, Kim JS, On YK. Efficacy and safety of cryoballoon pulmonary vein isolation for paroxysmal and persistent atrial fibrillation: a comparison with radiofrequency ablation. PLoS One. 2022;17(7):e0265482. doi:10.1371/journal.pone.0265482
88. Tanaka N, Tanaka K, Ninomiya Y, et al. Comparison of the safety and efficacy of automated annotation-guided radiofrequency ablation and 2nd-generation cryoballoon ablation in paroxysmal atrial fibrillation. Circ J. 2019;83(3):548–555. doi:10.1253/circj.CJ-18-1035
89. Buist TJ, Adiyaman A, Smit JJJ, Ramdat Misier AR, Elvan A. Arrhythmia-free survival and pulmonary vein reconnection patterns after second-generation cryoballoon and contact-force radiofrequency pulmonary vein isolation. Clin Res Cardiol. 2018;107(6):498–506. doi:10.1007/s00392-018-1211-9
90. Castellá M, Kotecha D, van Laar C, et al. Thoracoscopic vs catheter ablation for atrial fibrillation: long-term follow-up of the FAST randomized trial. Europace. 2019;21(5):746–753. doi:10.1093/europace/euy325
91. Shin DG, Ahn J, Han SJ, Lim HE. Efficacy of high-power and short-duration ablation in patients with atrial fibrillation: a prospective randomized controlled trial. Europace. 2020;22(10):1495–1501. doi:10.1093/europace/euaa144
92. Wójcik M, Erkapic D, Berkowitsch A, et al. Ipsilateral circumferential radiofrequency ablation of atrial fibrillation with irrigated tip catheter: long-term outcome and pre-procedural predictors. Circ J. 2013;77(9):2280–2287. doi:10.1253/circj.cj-13-0275
93. Weerasooriya R, Khairy P, Litalien J, et al. Catheter ablation for atrial fibrillation: are results maintained at 5 years of follow-up? J Am Coll Cardiol. 2011;57(2):160–166. doi:10.1016/j.jacc.2010.05.061
94. Bertaglia E, Tondo C, De Simone A, et al. Does catheter ablation cure atrial fibrillation? Single-procedure outcome of drug-refractory atrial fibrillation ablation: a 6-year multicentre experience. Europace. 2010;12(2):181–187. doi:10.1093/europace/eup349
95. Ciconte G, Baltogiannis G, de Asmundis C, et al. Circumferential pulmonary vein isolation as index procedure for persistent atrial fibrillation: a comparison between radiofrequency catheter ablation and second-generation cryoballoon ablation. Europace. 2015;17(4):559–565. doi:10.1093/europace/euu350
96. Kuck KH, Merkely B, Zahn R, et al. Catheter ablation versus best medical therapy in patients with persistent atrial fibrillation and congestive heart failure: the randomized AMICA trial. Circ Arrhythm Electrophysiol. 2019;12(12):e007731. doi:10.1161/circep.119.007731
97. Pavlović N, Sticherling C, Knecht S, et al. One-year follow-up after irrigated multi-electrode radiofrequency ablation of persistent atrial fibrillation. Europace. 2016;18(1):85–91. doi:10.1093/europace/euv020
98. Shi LB, Rossvoll O, Tande P, Schuster P, Solheim E, Chen J. Cryoballoon vs radiofrequency catheter ablation: insights from Norwegian randomized study of PERSistent Atrial Fibrillation (NO-PERSAF study). Europace. 2022;24(2):226–233. doi:10.1093/europace/euab281
99. Verma A, Jiang C-Y, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812–1822. doi:10.1056/NEJMoa1408288
100. Fink T, Schlüter M, Heeger CH, et al. Stand-alone pulmonary vein isolation versus pulmonary vein isolation with additional substrate modification as index ablation procedures in patients with persistent and long-standing persistent atrial fibrillation: the randomized Alster-Lost-AF Trial (Ablation at St. Georg Hospital for Long-Standing Persistent Atrial Fibrillation). Circ Arrhythm Electrophysiol. 2017;10(7). doi:10.1161/circep.117.005114
101. Tilz RR, Rillig A, Thum A-M, et al. Catheter ablation of long-standing persistent atrial fibrillation: 5-year outcomes of the Hamburg Sequential Ablation Strategy. J Am Coll Cardiol. 2012;60(19):1921–1929. doi:10.1016/j.jacc.2012.04.060
102. McCready JW, Smedley T, Lambiase PD, et al. Predictors of recurrence following radiofrequency ablation for persistent atrial fibrillation. Europace. 2011;13(3):355–361. doi:10.1093/europace/euq434
103. Wazni OM, Dandamudi G, Sood N, et al. Cryoballoon ablation as initial therapy for atrial fibrillation. N Engl J Med. 2021;384(4):316–324. doi:10.1056/NEJMoa2029554
104. Andrade JG, Wells GA, Deyell MW, et al. Cryoablation or drug therapy for initial treatment of atrial fibrillation. N Engl J Med. 2021;384(4):305–315. doi:10.1056/NEJMoa2029980
105. Andrade JG, Champagne J, Dubuc M, et al. Cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation. 2019;140(22):1779–1788. doi:10.1161/circulationaha.119.042622
106. Packer DL, Kowal RC, Wheelan KR, et al. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. J Am Coll Cardiol. 2013;61(16):1713–1723. doi:10.1016/j.jacc.2012.11.064
107. Kuniss M, Pavlovic N, Velagic V, et al. Cryoballoon ablation vs antiarrhythmic drugs: first-line therapy for patients with paroxysmal atrial fibrillation. Europace. 2021;23(7):1033–1041. doi:10.1093/europace/euab029
108. Neumann T, Wójcik M, Berkowitsch A, et al. Cryoballoon ablation of paroxysmal atrial fibrillation: 5-year outcome after single procedure and predictors of success. Europace. 2013;15(8):1143–1149. doi:10.1093/europace/eut021
109. Schiavone M, Gasperetti A, Montemerlo E, et al. Long-term comparisons of atrial fibrillation ablation outcomes with a cryoballoon or laser-balloon: a propensity-matched analysis based on continuous rhythm monitoring. Hell J Cardiol. 2022;65:1–7. doi:10.1016/j.hjc.2022.03.006
110. Wu S-J, Li C-H, Weng C-J, et al. Efficacy of cryoballoon ablation for atrial fibrillation and recurrence predictors in an Asian cohort. J Pers Med. 2022;12(5):732. doi:10.3390/jpm12050732
111. Ferrero-De-Loma-Osorio Á, Cózar R, García-Alberola A, et al. Primary results of the Spanish Cryoballoon Ablation Registry: acute and long-term outcomes of the RECABA study. Sci Rep. 2021;11(1):17268. doi:10.1038/s41598-021-96655-3
112. Chun JKR, Bordignon S, Last J, et al. Cryoballoon versus laserballoon: insights from the first prospective randomized balloon trial in catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2021;14(2):e009294. doi:10.1161/circep.120.009294
113. Knecht S, Sticherling C, Roten L, et al. Efficacy and safety of a novel cryoballoon ablation system: multicentre comparison of 1-year outcome. Europace. 2022. doi:10.1093/europace/euac094
114. Chen X, Xia Y, Lin Y, et al. Cryoballoon ablation for treatment of atrial fibrillation in a Chinese population: five-year outcomes and predictors of recurrence after a single procedure. Front Cardiovasc Med. 2022;9:836392. doi:10.3389/fcvm.2022.836392
115. Lim HE, Oh IY, Kueffer FJ, van Bragt KA, On YK. Cryoballoon catheter ablation in Korean patients with paroxysmal and persistent atrial fibrillation: one year outcome from the Cryo Global Registry. Korean Circ J. 2022;52(10):755–767. doi:10.4070/kcj.2022.0127
116. Aytemir K, Oto A, Canpolat U, et al. Immediate and medium-term outcomes of cryoballoon-based pulmonary vein isolation in patients with paroxysmal and persistent atrial fibrillation: single-centre experience. J Interv Card Electrophysiol. 2013;38(3):187–195. doi:10.1007/s10840-013-9834-2
117. Yalin K, Abdin A, Lyan E, et al. Safety and efficacy of persistent atrial fibrillation ablation using the second-generation cryoballoon. Clin Res Cardiol. 2018;107(7):570–577. doi:10.1007/s00392-018-1219-1
118. Lemes C, Wissner E, Lin T, et al. One-year clinical outcome after pulmonary vein isolation in persistent atrial fibrillation using the second-generation 28 mm cryoballoon: a retrospective analysis. Europace. 2016;18(2):201–205. doi:10.1093/europace/euv092
119. Koektuerk B, Yorgun H, Hengeoez O, et al. Cryoballoon ablation for pulmonary vein isolation in patients with persistent atrial fibrillation: one-year outcome using second generation cryoballoon. Circ Arrhythm Electrophysiol. 2015;8(5):1073–1079. doi:10.1161/circep.115.002776
120. Guhl EN, Siddoway D, Adelstein E, Voigt A, Saba S, Jain SK. Efficacy of cryoballoon pulmonary vein isolation in patients with persistent atrial fibrillation. J Cardiovasc Electrophysiol. 2016;27(4):423–427. doi:10.1111/jce.12924
121. Omran H, Gutleben KJ, Molatta S, et al. Second generation cryoballoon ablation for persistent atrial fibrillation: an updated meta-analysis. Clin Res Cardiol. 2018;107(2):182–192. doi:10.1007/s00392-017-1171-5
122. Nikfarjam M, Muralidharan V, Christophi C. Mechanisms of focal heat destruction of liver tumors. J Surg Res. 2005;127(2):208–223. doi:10.1016/j.jss.2005.02.009
123. Yang M, Yang X, Wang S, et al. HMGB1-induced endothelial cell pyroptosis is involved in systemic inflammatory response syndrome following radiofrequency ablation of hepatic hemangiomas. Am J Transl Res. 2019;11(12):7555–7567.
124. Wang S, Yang M, Yang X, et al. Endothelial pyroptosis underlies systemic inflammatory response following radiofrequency ablation of hepatic hemangiomas. Scand J Clin Lab Invest. 2019;79(8):619–628. doi:10.1080/00365513.2019.1689428
125. Wang K, Jiang L, Zhong Y, et al. Ferrostatin-1-loaded liposome for treatment of corneal alkali burn via targeting ferroptosis. Bioeng Transl Med. 2022;7(2):e10276. doi:10.1002/btm2.10276
126. Chu KF, Dupuy DE. Thermal ablation of tumours: biological mechanisms and advances in therapy. Nat Rev Cancer. 2014;14(3):199–208. doi:10.1038/nrc3672
127. Gao D, Critser JK. Mechanisms of cryoinjury in living cells. ILAR J. 2000;41(4):187–196. doi:10.1093/ilar.41.4.187
128. Hoffmann NE, Bischof JC. The cryobiology of cryosurgical injury. Urology. 2002;60(2 Suppl 1):40–49. doi:10.1016/s0090-4295(02)01683-7
129. Hanai A, Yang WL, Ravikumar TS. Induction of apoptosis in human colon carcinoma cells HT29 by sublethal cryo-injury: mediation by cytochrome c release. Int J Cancer. 2001;93(4):526–533. doi:10.1002/ijc.1359
130. Yang WL, Addona T, Nair DG, Qi L, Ravikumar TS. Apoptosis induced by cryo-injury in human colorectal cancer cells is associated with mitochondrial dysfunction. Int J Cancer. 2003;103(3):360–369. doi:10.1002/ijc.10822
131. Davalos RV, Mir IL, Rubinsky B. Tissue ablation with irreversible electroporation. Ann Biomed Eng. 2005;33(2):223–231. doi:10.1007/s10439-005-8981-8
132. Yarmush ML, Golberg A, Serša G, Kotnik T, Miklavčič D. Electroporation-based technologies for medicine: principles, applications, and challenges. Annu Rev Biomed Eng. 2014;16:295–320. doi:10.1146/annurev-bioeng-071813-104622
133. Freeman SA, Wang MA, Weaver JC. Theory of electroporation of planar bilayer membranes: predictions of the aqueous area, change in capacitance, and pore-pore separation. Biophys J. 1994;67(1):42–56. doi:10.1016/s0006-3495(94)80453-9
134. Chen W, Zhongsheng Z, Lee RC. Supramembrane potential-induced electroconformational changes in sodium channel proteins: a potential mechanism involved in electric injury. Burns. 2006;32(1):52–59. doi:10.1016/j.burns.2005.08.008
135. Frandsen SK, Gissel H, Hojman P, Tramm T, Eriksen J, Gehl J. Direct therapeutic applications of calcium electroporation to effectively induce tumor necrosis. Cancer Res. 2012;72(6):1336–1341. doi:10.1158/0008-5472.Can-11-3782
136. Batista Napotnik T, Polajžer T, Miklavčič D. Cell death due to electroporation - A review. Bioelectrochemistry. 2021;141:107871. doi:10.1016/j.bioelechem.2021.107871
137. Lee EW, Loh CT, Kee ST. Imaging guided percutaneous irreversible electroporation: ultrasound and immunohistological correlation. Technol Cancer Res Treat. 2007;6(4):287–294. doi:10.1177/153303460700600404
138. Kim HB, Sung CK, Baik KY, et al. Changes of apoptosis in tumor tissues with time after irreversible electroporation. Biochem Biophys Res Commun. 2013;435(4):651–656. doi:10.1016/j.bbrc.2013.05.039
139. Long G, Bakos G, Shires PK, et al. Histological and finite element analysis of cell death due to irreversible electroporation. Technol Cancer Res Treat. 2014;13(6):561–569. doi:10.7785/tcrtexpress.2013.600253
140. van den Bos W, Jurhill RR, de Bruin DM, et al. Histopathological outcomes after irreversible electroporation for prostate cancer: results of an ablate and resect study. J Urol. 2016;196(2):552–559. doi:10.1016/j.juro.2016.02.2977
141. Jose A, Sobrevals L, Ivorra A, Fillat C. Irreversible electroporation shows efficacy against pancreatic carcinoma without systemic toxicity in mouse models. Cancer Lett. 2012;317(1):16–23. doi:10.1016/j.canlet.2011.11.004
142. Zhang Y, Lyu C, Liu Y, Lv Y, Chang TT, Rubinsky B. Molecular and histological study on the effects of non-thermal irreversible electroporation on the liver. Biochem Biophys Res Commun. 2018;500(3):665–670. doi:10.1016/j.bbrc.2018.04.132
143. Klein Klouwenberg PM, Frencken JF, Kuipers S, et al. Incidence, predictors, and outcomes of new-onset atrial fibrillation in critically ill patients with sepsis. A cohort study. Am J Respir Crit Care Med. 2017;195(2):205–211. doi:10.1164/rccm.201603-0618OC
144. Meierhenrich R, Steinhilber E, Eggermann C, et al. Incidence and prognostic impact of new-onset atrial fibrillation in patients with septic shock: a prospective observational study. Crit Care. 2010;14(3):R108. doi:10.1186/cc9057
145. Bacani AK, Crowson CS, Roger VL, Gabriel SE, Matteson EL. Increased incidence of atrial fibrillation in patients with rheumatoid arthritis. Biomed Res Int. 2015;2015:809514. doi:10.1155/2015/809514
146. Ahlehoff O, Gislason GH, Jørgensen CH, et al. Psoriasis and risk of atrial fibrillation and ischaemic stroke: a Danish Nationwide Cohort Study. Eur Heart J. 2012;33(16):2054–2064. doi:10.1093/eurheartj/ehr285
147. Choi YJ, Choi EK, Han KD, et al. Increased risk of atrial fibrillation in patients with inflammatory bowel disease: a nationwide population-based study. World J Gastroenterol. 2019;25(22):2788–2798. doi:10.3748/wjg.v25.i22.2788
148. Zhao Q, Zhang S, Zhao H, et al. Median nerve stimulation prevents atrial electrical remodelling and inflammation in a canine model with rapid atrial pacing. Europace. 2018;20(4):712–718. doi:10.1093/europace/eux003
149. Zhang Y, Sun D, Zhao X, et al. Bacteroides fragilis prevents aging-related atrial fibrillation in rats via regulatory T cells-mediated regulation of inflammation. Pharmacol Res. 2022;177:106141. doi:10.1016/j.phrs.2022.106141
150. Liu Q, Zhang F, Yang M, Zhong J. Increasing level of Interleukin-1β in epicardial adipose tissue is associated with persistent atrial fibrillation. J Interferon Cytokine Res. 2020;40(1):64–69. doi:10.1089/jir.2019.0098
151. Nakamura Y, Nakamura K, Fukushima-Kusano K, et al. Tissue factor expression in atrial endothelia associated with nonvalvular atrial fibrillation: possible involvement in intracardiac thrombogenesis. Thromb Res. 2003;111(3):137–142. doi:10.1016/s0049-3848(03)00405-5
152. Narducci ML, Pelargonio G, Dello Russo A, et al. Role of tissue C-reactive protein in atrial cardiomyocytes of patients undergoing catheter ablation of atrial fibrillation: pathogenetic implications. Europace. 2011;13(8):1133–1140. doi:10.1093/europace/eur068
153. Soeki T, Bando S, Uematsu E, et al. Pentraxin 3 is a local inflammatory marker in atrial fibrillation. Heart Vessels. 2014;29(5):653–658. doi:10.1007/s00380-013-0400-8
154. Musa H, Kaur K, O’Connell R, et al. Inhibition of platelet-derived growth factor-AB signaling prevents electromechanical remodeling of adult atrial myocytes that contact myofibroblasts. Heart Rhythm. 2013;10(7):1044–1051. doi:10.1016/j.hrthm.2013.03.014
155. Lee SH, Chen YC, Chen YJ, et al. Tumor necrosis factor-alpha alters calcium handling and increases arrhythmogenesis of pulmonary vein cardiomyocytes. Life Sci. 2007;80(19):1806–1815. doi:10.1016/j.lfs.2007.02.029
156. Saba S, Janczewski AM, Baker LC, et al. Atrial contractile dysfunction, fibrosis, and arrhythmias in a mouse model of cardiomyopathy secondary to cardiac-specific overexpression of tumor necrosis factor-{alpha}. Am J Physiol Heart Circ Physiol. 2005;289(4):H1456–H1467. doi:10.1152/ajpheart.00733.2004
157. Sawaya SE, Rajawat YS, Rami TG, et al. Downregulation of connexin40 and increased prevalence of atrial arrhythmias in transgenic mice with cardiac-restricted overexpression of tumor necrosis factor. Am J Physiol Heart Circ Physiol. 2007;292(3):H1561–H1567. doi:10.1152/ajpheart.00285.2006
158. Ryu K, Li L, Khrestian CM, et al. Effects of sterile pericarditis on connexins 40 and 43 in the atria: correlation with abnormal conduction and atrial arrhythmias. Am J Physiol Heart Circ Physiol. 2007;293(2):H1231–H1241. doi:10.1152/ajpheart.00607.2006
159. Lazzerini PE, Laghi-Pasini F, Acampa M, et al. Systemic inflammation rapidly induces reversible atrial electrical remodeling: the role of interleukin-6-mediated changes in connexin expression. J Am Heart Assoc. 2019;8(16):e011006. doi:10.1161/jaha.118.011006
160. Ishii Y, Schuessler RB, Gaynor SL, et al. Inflammation of atrium after cardiac surgery is associated with inhomogeneity of atrial conduction and atrial fibrillation. Circulation. 2005;111(22):2881–2888. doi:10.1161/circulationaha.104.475194
161. Tselentakis EV, Woodford E, Chandy J, Gaudette GR, Saltman AE. Inflammation effects on the electrical properties of atrial tissue and inducibility of postoperative atrial fibrillation. J Surg Res. 2006;135(1):68–75. doi:10.1016/j.jss.2006.03.024
162. Wilhelm M, Zueger T, De Marchi S, et al. Inflammation and atrial remodeling after a mountain marathon. Scand J Med Sci Sports. 2014;24(3):519–525. doi:10.1111/sms.12030
163. Burstein B, Nattel S. Atrial fibrosis: mechanisms and clinical relevance in atrial fibrillation. J Am Coll Cardiol. 2008;51(8):802–809. doi:10.1016/j.jacc.2007.09.064
164. Liao CH, Akazawa H, Tamagawa M, et al. Cardiac mast cells cause atrial fibrillation through PDGF-A-mediated fibrosis in pressure-overloaded mouse hearts. J Clin Invest. 2010;120(1):242–253. doi:10.1172/jci39942
165. Hoogstra-Berends F, Meijering RA, Zhang D, et al. Heat shock protein-inducing compounds as therapeutics to restore proteostasis in atrial fibrillation. Trends Cardiovasc Med. 2012;22(3):62–68. doi:10.1016/j.tcm.2012.06.013
166. Liew R, Khairunnisa K, Gu Y, et al. Role of tumor necrosis factor-α in the pathogenesis of atrial fibrosis and development of an arrhythmogenic substrate. Circ J. 2013;77(5):1171–1179. doi:10.1253/circj.cj-12-1155
167. Li YY, Feng YQ, Kadokami T, et al. Myocardial extracellular matrix remodeling in transgenic mice overexpressing tumor necrosis factor alpha can be modulated by anti-tumor necrosis factor alpha therapy. Proc Natl Acad Sci U S A. 2000;97(23):12746–12751. doi:10.1073/pnas.97.23.12746
168. Ma F, Li Y, Jia L, et al. Macrophage-stimulated cardiac fibroblast production of IL-6 is essential for TGF β/Smad activation and cardiac fibrosis induced by angiotensin II. PLoS One. 2012;7(5):e35144. doi:10.1371/journal.pone.0035144
169. Hu YF, Yeh HI, Tsao HM, et al. Electrophysiological correlation and prognostic impact of heat shock protein 27 in atrial fibrillation. Circ Arrhythm Electrophysiol. 2012;5(2):334–340. doi:10.1161/circep.111.965996
170. Psychari SN, Apostolou TS, Sinos L, Hamodraka E, Liakos G, Kremastinos DT. Relation of elevated C-reactive protein and interleukin-6 levels to left atrial size and duration of episodes in patients with atrial fibrillation. Am J Cardiol. 2005;95(6):764–767. doi:10.1016/j.amjcard.2004.11.032
171. Luan Y, Guo Y, Li S, et al. Interleukin-18 among atrial fibrillation patients in the absence of structural heart disease. Europace. 2010;12(12):1713–1718. doi:10.1093/europace/euq321
172. Sabel MS. Cryo-immunology: a review of the literature and proposed mechanisms for stimulatory versus suppressive immune responses. Cryobiology. 2009;58(1):1–11. doi:10.1016/j.cryobiol.2008.10.126
173. Ahmad F, Gravante G, Bhardwaj N, et al. Changes in interleukin-1β and 6 after hepatic microwave tissue ablation compared with radiofrequency, cryotherapy and surgical resections. Am J Surg. 2010;200(4):500–506. doi:10.1016/j.amjsurg.2009.12.025
174. Erinjeri JP, Thomas CT, Samoilia A, et al. Image-guided thermal ablation of tumors increases the plasma level of interleukin-6 and interleukin-10. J Vasc Interv Radiol. 2013;24(8):1105–1112. doi:10.1016/j.jvir.2013.02.015
175. Fietta AM, Morosini M, Passadore I, et al. Systemic inflammatory response and downmodulation of peripheral CD25+Foxp3+ T-regulatory cells in patients undergoing radiofrequency thermal ablation for lung cancer. Hum Immunol. 2009;70(7):477–486. doi:10.1016/j.humimm.2009.03.012
176. Zerbini A, Pilli M, Laccabue D, et al. Radiofrequency thermal ablation for hepatocellular carcinoma stimulates autologous NK-cell response. Gastroenterology. 2010;138(5):1931–1942. doi:10.1053/j.gastro.2009.12.051
177. Wissniowski TT, Hänsler J, Neureiter D, et al. Activation of tumor-specific T lymphocytes by radio-frequency ablation of the VX2 hepatoma in rabbits. Cancer Res. 2003;63(19):6496–6500.
178. Dromi SA, Walsh MP, Herby S, et al. Radiofrequency ablation induces antigen-presenting cell infiltration and amplification of weak tumor-induced immunity. Radiology. 2009;251(1):58–66. doi:10.1148/radiol.2511072175
179. Oswald H, Gardiwal A, Lissel C, Yu H, Klein G. Difference in humoral biomarkers for myocardial injury and inflammation in radiofrequency ablation versus cryoablation. Pacing Clin Electrophysiol. 2007;30(7):885–890. doi:10.1111/j.1540-8159.2007.00776.x
180. Herrera Siklódy C, Arentz T, Minners J, et al. Cellular damage, platelet activation, and inflammatory response after pulmonary vein isolation: a randomized study comparing radiofrequency ablation with cryoablation. Heart Rhythm. 2012;9(2):189–196. doi:10.1016/j.hrthm.2011.09.017
181. Antolič B, Pernat A, Cvijić M, Žižek D, Jan M, Šinkovec M. Radiofrequency catheter ablation versus balloon cryoablation of atrial fibrillation: markers of myocardial damage, inflammation, and thrombogenesis. Wien Klin Wochenschr. 2016;128(13–14):480–487. doi:10.1007/s00508-016-1002-0
182. Miyazaki S, Kuroi A, Hachiya H, et al. Early recurrence after pulmonary vein isolation of paroxysmal atrial fibrillation with different ablation technologies - prospective comparison of radiofrequency vs second-generation cryoballoon ablation. Circ J. 2016;80(2):346–353. doi:10.1253/circj.CJ-15-1051
183. Grimaldi M, Di monaco A, Gomez T, et al. Time course of irreversible electroporation lesion development through short- and long-term follow-up in pulsed-field ablation-treated hearts. Circ Arrhythm Electrophysiol. 2022;15(7):e010661. doi:10.1161/circep.121.010661
184. Koruth JS, Kuroki K, Kawamura I, et al. Focal pulsed field ablation for pulmonary vein isolation and linear atrial lesions: a preclinical assessment of safety and durability. Circ Arrhythm Electrophysiol. 2020;13(6):e008716. doi:10.1161/circep.120.008716
185. Sugimoto K, Kakimi K, Takeuchi H, et al. Irreversible electroporation versus radiofrequency ablation: comparison of systemic immune responses in patients with hepatocellular carcinoma. JVIR. 2019;30(6):845–853.e846. doi:10.1016/j.jvir.2019.03.002
186. Xie B, Chen BX, Nanna M, et al. 18F-fluorodeoxyglucose positron emission tomography/computed tomography imaging in atrial fibrillation: a pilot prospective study. Eur Heart J Cardiovasc Imaging. 2021;23(1):102–112. doi:10.1093/ehjci/jeab088
187. Chang TY, Hsiao YW, Guo SM, et al. Resistin as a biomarker for the prediction of left atrial substrate and recurrence in patients with drug-refractory atrial fibrillation undergoing catheter ablation. Int Heart J. 2020;61(3):517–523. doi:10.1536/ihj.19-680
188. Kusayama T, Furusho H, Kashiwagi H, et al. Inflammation of left atrial epicardial adipose tissue is associated with paroxysmal atrial fibrillation. J Cardiol. 2016;68(5):406–411. doi:10.1016/j.jjcc.2015.11.005
189. Yorgun H, Canpolat U, Aytemir K, et al. Association of epicardial and peri-atrial adiposity with the presence and severity of non-valvular atrial fibrillation. Int J Cardiovasc Imaging. 2015;31(3):649–657. doi:10.1007/s10554-014-0579-5
190. Hayıroğlu Mİ, Altay SAO. The role of artificial intelligence in coronary artery disease and atrial fibrillation. Balkan Med J. 2023;40(3):151.
191. Andrade JG, Khairy P, Macle L, et al. Incidence and significance of early recurrences of atrial fibrillation after cryoballoon ablation. Circulation. 2014;7(1):69–75. doi:10.1161/circep.113.000586
192. Hernández-Romero D, Marín F, Roldán V, et al. Comparative determination and monitoring of biomarkers of necrosis and myocardial remodeling between radiofrequency ablation and cryoablation. Pacing Clin Electrophysiol. 2013;36(1):31–36. doi:10.1111/pace.12017
193. Del Rey JM, Madrid AH, Novo L, et al. Evaluación de marcadores de lesión miocárdica tras la ablación con radiofrecuencia. Utilidad de la troponina I [Evaluation of biochemical markers of myocardial lesion after radiofrequency ablation. Value of troponin I]. Rev Esp Cardiol. 1997;50(8):552–560. Spanish. doi:10.1016/s0300-8932(97)73263-9
194. Bai Y, Guo SD, Liu Y, Ma CS, Lip GYH. Relationship of troponin to incident atrial fibrillation occurrence, recurrence after radiofrequency ablation and prognosis: a systematic review, meta-analysis and meta-regression. Biomarkers. 2018;23(6):512–517. doi:10.1080/1354750x.2018.1463562
195. Canpolat U, Aytemir K, Yorgun H, et al. Role of preablation neutrophil/lymphocyte ratio on outcomes of cryoballoon-based atrial fibrillation ablation. Am J Cardiol. 2013;112(4):513–519. doi:10.1016/j.amjcard.2013.04.015
196. Guo X, Zhang S, Yan X, et al. Postablation neutrophil/lymphocyte ratio correlates with arrhythmia recurrence after catheter ablation of lone atrial fibrillation. Chin Med J. 2014;127(6):1033–1038.
197. Ruan ZB, Gao RF, Wang F, et al. Circulating galectin-3 and aldosterone for predicting atrial fibrillation recurrence after radiofrequency catheter ablation. Cardiovasc Ther. 2022;2022:6993904. doi:10.1155/2022/6993904
198. Clementy N, Benhenda N, Piver E, et al. Serum galectin-3 levels predict recurrences after ablation of atrial fibrillation. Sci Rep. 2016;6:34357. doi:10.1038/srep34357
199. Berger WR, Jagu B, van den Berg NWE, et al. The change in circulating galectin-3 predicts absence of atrial fibrillation after thoracoscopic surgical ablation. Europace. 2018;20(5):764–771. doi:10.1093/europace/eux090
200. Takemoto Y, Ramirez RJ, Yokokawa M, et al. Galectin-3 regulates atrial fibrillation remodeling and predicts catheter ablation outcomes. Basic Transl Sci. 2016;1(3):143–154. doi:10.1016/j.jacbts.2016.03.003
201. Karataş MAO, Durmuş G, Zengin A, et al. Association of uric acid albumin ratio with recurrence of atrial fibrillation after cryoballoon catheter ablation. Medicina. 2022;58(12):1872.
202. Li SB, Yang F, Jing L, et al. Myeloperoxidase and risk of recurrence of atrial fibrillation after catheter ablation. J Investig Med. 2013;61(4):722–727. doi:10.2310/JIM.0b013e3182857fa0
203. Richter B, Gwechenberger M, Socas A, et al. Markers of oxidative stress after ablation of atrial fibrillation are associated with inflammation, delivered radiofrequency energy and early recurrence of atrial fibrillation. Clin Res Cardiol. 2012;101(3):217–225. doi:10.1007/s00392-011-0383-3
204. Canpolat U, Aytemir K, Yorgun H, et al. The role of preprocedural monocyte-to-high-density lipoprotein ratio in prediction of atrial fibrillation recurrence after cryoballoon-based catheter ablation. Europace. 2015;17(12):1807–1815. doi:10.1093/europace/euu291
205. Gurses KM, Kocyigit D, Yalcin MU, et al. Monocyte toll-like receptor expression in patients with atrial fibrillation. Am J Cardiol. 2016;117(9):1463–1467. doi:10.1016/j.amjcard.2016.02.014
206. Kimura T, Takatsuki S, Inagawa K, et al. Serum inflammation markers predicting successful initial catheter ablation for atrial fibrillation. Heart Lung Circ. 2014;23(7):636–643. doi:10.1016/j.hlc.2014.02.003
207. Meyre PB, Sticherling C, Spies F, et al. C-reactive protein for prediction of atrial fibrillation recurrence after catheter ablation. BMC Cardiovasc Disord. 2020;20(1):427. doi:10.1186/s12872-020-01711-x
208. Ihara K, Sasano T. Role of inflammation in the pathogenesis of atrial fibrillation. Front Physiol. 2022;13:862164. doi:10.3389/fphys.2022.862164
209. Farkowski MM, Maciag A, Kowalik I, Konka M, Szwed H, Pytkowski M. Intravenous antazoline, a first-generation antihistaminic drug with antiarrhythmic properties, is a suitable agent for pharmacological cardioversion of atrial fibrillation induced during pulmonary vein isolation due to the lack of influence on atrio-venous conduction and high clinical effectiveness (AntaEP Study). Br J Clin Pharmacol. 2019;85(7):1552–1558. doi:10.1111/bcp.13940
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Atrial Fibrillation Types and Chronic Kidney Disease are Independent Predictors of Atrial Fibrillation Recurrence After Radiofrequency Ablation
Mo P, Fan C, Chen J, Wang Y, Xiao W, Peng Z, Lin XZ, Luo CF, Zhang C
Therapeutics and Clinical Risk Management 2024, 20:817-828
Published Date: 3 December 2024
SPISE Index (Single-Point Insulin Sensitivity Estimator): A Long-Term Predictor of Recurrence in Elderly Patients with Atrial Fibrillation After Radiofrequency Ablation
Wang Z, Qu Y, Wang H, Liu X
Clinical Interventions in Aging 2026, 21:608687
Published Date: 12 June 2026