Back to Journals » Journal of Pain Research » Volume 19
Spinal Cord Stimulators’ Displacement: Systematic Review and Single-Institution Case Series with Anchoring Technique
Authors Mariadas R ![]() , Pan E, Boesel TW, Di Ieva A
, Pan E, Boesel TW, Di Ieva A
Received 15 July 2025
Accepted for publication 17 February 2026
Published 9 April 2026 Volume 2026:19 547502
DOI https://doi.org/10.2147/JPR.S547502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Rachael Mariadas,1 Elizabeth Pan,2 Tillman W Boesel,1 Antonio Di Ieva1,2
1Macquarie Medical School, Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, NSW, 2109, Australia; 2Computational NeuroSurgery (CNS) Lab, Macquarie Medical School, Macquarie University, Sydney, NSW, 2109, Australia
Correspondence: Antonio Di Ieva, Email [email protected]
Objective: Spinal cord stimulation (SCS) is an established neuromodulation therapy for chronic pain, but lead displacement remains a frequent hardware complication with important implications for long-term efficacy. This systematic review quantifies electrode displacement rates worldwide and evaluates whether a spine-anchoring technique is associated with reduced displacement via a single-institution case series.
Materials and Methods: A systematic review was conducted in MEDLINE, Embase, and Cochrane Central (1967–February 2024) to identify SCS studies reporting lead displacement. The protocol was registered prospectively (PROSPERO CRD42024536758). Methodological quality was assessed using the Newcastle–Ottawa Scale (NOS), the Cochrane risk-of-bias tools, and the GRADE approach. In parallel, a single-institution retrospective case series (2017– 2024) included 128 chronic pain patients treated with SCS using an open surgical laminar anchoring technique with mini-plate and screw fixation.
Results: The review included 117 articles (20,427 participants). Trial lead displacement occurred in 7.33% of patients (113/1,542), and permanent lead displacement in 6.64% (1,309/19,677). Studies judged at low risk of bias reported a permanent displacement rate of 2.1% versus 7.1% in high-risk studies. In the institutional case series, all 128 patients underwent a 7– 10-day trial, and 125 proceeded to permanent implantation. Trial displacement was 0% (0/128), and permanent displacement was 2.4% (3/125). All three displaced leads showed cranio‑caudal migration and ultimately required surgical revision after unsuccessful reprogramming; all revisions were successful, with no recurrent displacement.
Conclusion: Heterogeneity in study design and reporting limits direct comparison of displacement rates across the literature, but methodological quality clearly influences reported outcomes. The open laminar anchoring technique used at our institution was associated with a 2.4% permanent displacement rate, lower than many historical estimates and comparable to rates in lower-risk studies, suggesting that robust anchoring strategies may reduce clinically important lead displacement in selected chronic pain populations.
Keywords: spinal cord stimulation, lead displacement, anchoring technique, chronic pain, systematic review, lead migration, surgical technique
Introduction
Spinal cord stimulation (SCS) is a neuromodulation procedure first clinically utilised in 1967 following Melzack and Wall’s gate control theory of pain.1 Following FDA approval in 1989, SCS has emerged as an important treatment option for patients with chronic pain refractory to conventional medical management (CMM).1,2 The therapy involves surgical implantation of a pulse generator with subcutaneous positioning that delivers electrical signals through electrode arrays positioned in the epidural space adjacent to the dorsal columns of the spinal cord.1 The electrical stimulation modulates neural activity, potentially reducing pain transmission via gate-control mechanisms and other neuromodulatory pathways.1,2
Recent systematic reviews and randomized controlled trials provide moderate-quality evidence for SCS efficacy in specific chronic pain populations.3,4 A 2025 systematic review of RCTs comparing SCS to conventional medical management in persistent spinal pain syndrome-type 2 (PSPS-T2) demonstrated responder rates of 14–80% for ≥50% pain relief in SCS groups compared with 3–20% for CMM, with moderate GRADE evidence for clinical effectiveness.5 PSPS-T2 is chronic pain persisting after surgery and was formerly known as failed back surgery syndrome (FBSS). In FBSS, 48% of SCS patients achieved ≥50% leg pain relief compared to 9% in CMM groups.6 However, efficacy varies substantially by indication. Patients with diabetic neuropathy achieved the highest success rates (83.3%), while complex regional pain syndrome patients had lower response rates (67.6%).7 Most patients sustaining treatment require long-term device therapy, with studies reporting 76.6% maintaining ≥50% pain improvement at follow-ups ranging from 3 to 34 months.7
Despite clinical benefits, efficacy is not universal. Long-term durability remains controversial, with some studies documenting loss of efficacy over time.7 Cochrane reviews have noted that evidence quality for low back pain specifically is modest, with recommendations for careful patient selection and comprehensive informed consent regarding the chronic nature of therapy and revision surgery risk.3,4
The most common indications for SCS are failed back surgery syndrome (FBSS) and complex regional pain syndrome (CRPS). FBSS, representing persistent pain (typically ≥6 months) following spinal surgery despite anatomic correction, accounts for 25–33% of SCS candidates.8,9 CRPS, characterized by disproportionate pain with autonomic dysfunction, represents 20–49% of cohorts.8,9 Other established indications include diabetic neuropathy, chronic neuropathic pain, postherpetic neuralgia, and chronic angina pectoris.7 Emerging indications under investigation include intractable headache disorders and chemotherapy-induced pain.7
A significant concern regarding long-term SCS therapy is the phenomenon of loss of efficacy (LOE), wherein patients experience waning pain relief despite previously successful pain control.7 LOE occurs in 10–20% of patients over multi-year follow-up periods.7 Mechanisms are incompletely understood but may include accommodation, neuroplasticity, development of opioid tolerance in those receiving concurrent opioids, and mechanical complications including lead migration and disconnection.7
Among the most frequent SCS complications are lead displacement and infection.1,8–10 Lead displacement (also termed lead migration) refers to unintended movement of implanted electrodes from their original therapeutic position.10 Displacement is clinically significant when it results in loss of paraesthesia coverage, reduced pain relief, development of dysesthesia, or generation of off-target stimulation effects.10 While mild displacement without clinical consequences may not require intervention, clinically significant displacement may necessitate reprogramming or surgical revision, representing substantial morbidity and healthcare costs.1,10
Lead displacement is poorly reported in the literature, with many studies neither specifically tracking nor reporting this complication.10 As such, the true incidence may exceed published estimates. Historically reported rates have varied from 2.1% to 27% in permanent implants.1,8–11 Variation reflects differences in: (1) study population and indication, (2) implantation technique (percutaneous vs. open), (3) electrode type (cylindrical vs. paddle), (4) anchoring methodology, (5) follow-up duration and surveillance intensity, (6) definition of displacement, and (7) methodological quality.1,8–11
Patient-related factors influence lead displacement risk. Tobacco use correlates with increased revision surgery requirements, though the specific association with lead displacement is unclear.12 Higher body mass index (BMI ≥ 30) combined with depression is associated with long-term SCS failure and increased explantation rates.13 In our case series, all three patients experiencing lead displacement demonstrated both depression and elevated BMI, suggesting a possible association between the combination of depression and elevated BMI and displacement risk, although the small number of events precludes firm conclusions.
SCS implantation employs either percutaneous or open surgical approaches.1,2,8 Percutaneous techniques using cylindrical leads are less invasive and associated with fewer lead fractures, whereas open approaches reduce lead displacement incidence but require greater tissue trauma.2,8 The epidural space may be accessed via percutaneous needle (most common) or via small laminotomy/flavectomy allowing direct visualization.1,8 Lead anchoring techniques vary widely between institutions with no established consensus on optimal methodology.1,8
Recent advances in technique, including improved anchoring strategies and intraoperative neuromonitoring, may have contributed to reduced contemporary displacement rates compared to historical data.11 One such technique involves “midline anchoring” of percutaneous leads, which reduced displacement from 23% to 6% in trial periods and from 24% to 7% in permanent implants in one institutional series.14 However, comparative evidence remains limited.
The true incidence of lead displacement remains uncertain due to heterogeneous reporting, variable methodological quality, and selective publication favoring larger, more rigorous studies.11 Previous literature reviews have emphasized randomized trials and higher-quality observational studies, potentially underestimating displacement rates from smaller studies and missing important patterns related to implantation technique.11
This systematic review intentionally includes observational studies of varying quality to capture the full spectrum of reported displacement rates across institutions worldwide. We stratify findings by methodological quality to distinguish true variation in clinical practice from bias-related variation. We present an institutional case series employing a specific spine-anchoring technique involving mini-plate and screw laminar fixation under direct visualization with intraoperative neuromonitoring, comparing outcomes to the published literature.
Aim
This systematic review had three primary objectives. First, to estimate the global incidence of spinal cord stimulator electrode displacement during both trial and permanent implantation. Second, to examine how methodological quality influences reported displacement rates. Third, to compare these rates with those observed in a single institution using a specific open laminar anchoring technique.
Methods
Systematic Review Protocol and Registration
This systematic review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines.15 The protocol was registered with PROSPERO; CRD42024536758 prior to data extraction.
Literature Search Strategy
A comprehensive systematic search was conducted across three major databases:
- MEDLINE (Ovid) through February 2024
- Embase (Ovid) through February 2024
- Cochrane Central Register of Controlled Trials (CENTRAL), Issue 2, 2024
The search strategy combined free text terms, keywords, and Medical Subject Heading (MeSH) terminology to capture relevant articles published from 1967 (year of first SCS implantation) through February 2024. Search terms included combinations of: “spinal cord stimulator”, “lead”, “electrode”, “migration”, “displacement”, “dislocation”, “dislodgement”, and specific indications including “failed back surgery syndrome”, “complex regional pain syndrome”, “neuropathic pain”, “brachialgia”, “phantom limb syndrome”, “postherpetic neuralgia”, and “chronic pain”. The search strategy was developed with a clinical medical librarian. Supplementary Table 1 provides the complete search string.
Study Selection and Screening
Initial literature search identified all potentially relevant articles. Two investigators independently screened titles and abstracts. The first author conducted full-text screening with the second author independently verifying at each stage. Discrepancies were resolved by consensus between two senior authors. Inclusion and exclusion criteria are detailed in Supplementary Table 2.
Data Extraction
Data extraction was performed with verification by the second author. Extracted variables included: author name, publication year, article title, article type (RCT, prospective study, retrospective cohort, case series, case report, registry data), chronic pain indication (as reported by study authors), total participant number, number of trial patients, trial electrode displacements, total permanent implant recipients, permanent electrode displacements, displacement episodes, displacement direction (lateral, cranio-caudal, rotational, or extraspinal), displacement management (reprogramming vs. surgical revision), implantation approach (percutaneous vs. open), electrode type (cylindrical vs. paddle), anchoring technique (if specified), mean/median follow-up duration, and complications. Displacement was recorded as present if authors utilised terminology including “lead migration”, “electrode migration”, “lead displacement”, “dislocation”, or “dislodgement”.
Quality Assessment Methods
Newcastle-Ottawa Scale for Observational Studies
Two investigators independently assessed cohort and case-control studies using the Newcastle-Ottawa Scale (NOS).16 The NOS evaluates: selection (representative cohort, adequate exposure/outcome ascertainment, no outcome at baseline), comparability (controlled confounding variables), and outcome (adequate follow-up, appropriate outcome assessment). Overall scores ≥7 = low risk of bias; ≤6 = high risk of bias. Results are presented in Supplementary Table 3.
Cochrane Collaboration Risk of Bias for RCTs
Randomised controlled trials were assessed using the Cochrane Collaboration Risk of Bias tool17 evaluating key domains including random sequence generation, allocation concealment, blinding of participants and outcome assessors, completeness of outcome data, selective outcome reporting, and other potential sources of bias. Each domain was scored as “low”, “unclear”, or “high” risk, with overall risk determined by the most unfavourable domain assessment. Results are in Supplementary Table 4.
GRADE Approach for Evidence Certainty
Evidence certainty was rated using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach.18 RCT evidence began at “high” certainty; observational studies began at “low” certainty. Certainty was downgraded for: study design limitations, indirectness of evidence, inconsistency/heterogeneity, imprecision, and publication bias. Certainty was upgraded for large effect sizes, dose-response gradients, and consideration of confounders. Final ratings: “very low”, “low”, “moderate”, or “high” certainty. Quality assessment was performed with sample verification by the second author (85% agreement rate). Results are in Supplementary Table 5.
Statistical Analysis of Systematic Review
Meta-analysis was not performed due to substantial heterogeneity in study designs, patient populations, outcome definitions, and follow-up periods. Instead, summary displacement rates were calculated as: total displacements ÷ total participants, expressed as percentages. Median and interquartile ranges were calculated for comparable groups. Subgroup analysis was performed stratifying studies by methodological quality (low vs. high risk of bias per NOS/Cochrane assessment) to examine the relationship between quality and reported displacement rates.
Case Series: Patient Selection and Ethics
Records of 128 consecutive chronic pain patients who underwent SCS treatment at Macquarie University Hospital, Sydney, Australia, between 2017 and 2024 were reviewed retrospectively. Ethics approval was obtained from the Macquarie University Human Research Ethics Committee (Reference No: 520221180639703). The study complies with the Declaration of Helsinki. All participants provided informed consent allowing the use of de-identified data for approved research.
Inclusion Criteria
- Adult patients (≥18 years) with chronic pain syndrome of ≥6 months duration
- Pain refractory to medical management and/or prior surgical interventions
- Deemed suitable candidates for SCS therapy
- Underwent both trial and/or permanent SCS implantation at the study institution
Exclusion Criteria
- SCS implantation at other institutions
- Incomplete follow-up records (<12 months data)
- Paediatric patients (<18 years)
Case Series: Patient Characteristics and Data Collection
Patient demographics recorded included: age, sex, BMI (calculated from recorded height and weight; BMI ≥ 30 defined as overweight per standard criteria or physician documentation of overweight status), depression diagnosis (defined as formal psychiatric diagnosis or current antidepressant use), active tobacco use, history of tobacco use, and surgical history. Table 1 outlines the patient characteristics by sex and age. SCS indications were categorised according to diagnostic classification and outlined in Table 2. Operative details recorded included: implantation date, lead type (cylindrical vs. paddle), approach (percutaneous vs. open), implant brand (Abbott, Medtronic, Nevro, Saluda), implantation level (cervical, thoracic, or combined), and anchoring methodology.
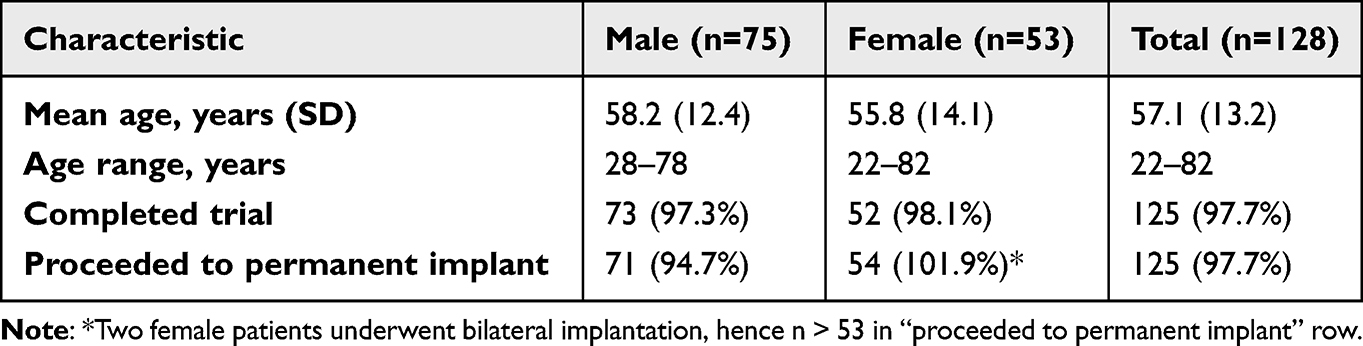 |
Table 1 Patient Characteristics by Sex and Age (Case Series, n=128) |
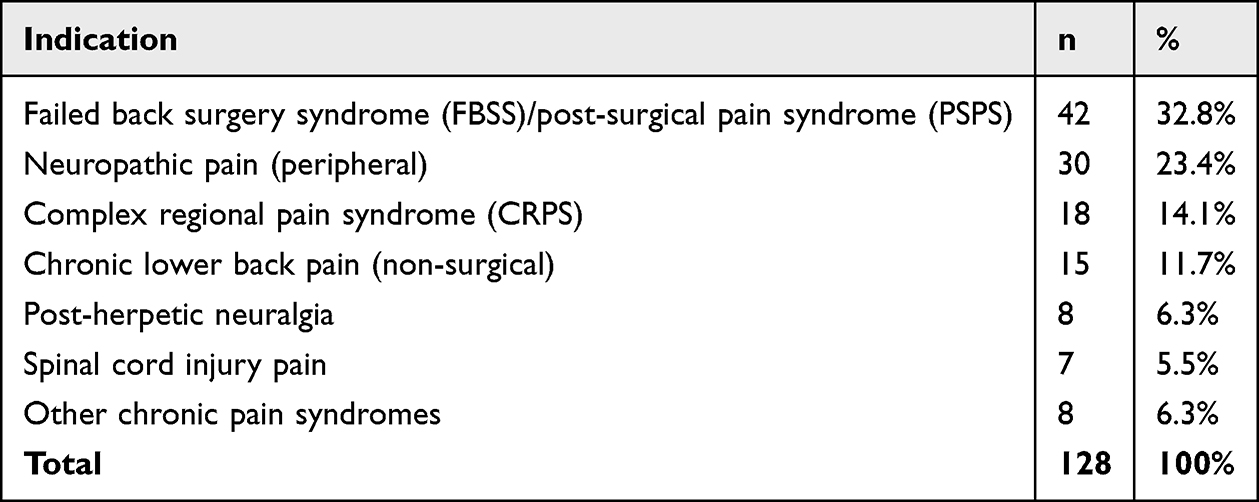 |
Table 2 Indications for SCS Insertion in Case Series |
Permanent implantation was performed in patients who achieved a successful trial, under general anaesthesia with continuous intraoperative neurophysiological monitoring using motor and sensory evoked potentials. The institutional technique uses an open approach with a limited laminotomy and/or a small flavectomy to expose the epidural space under direct vision. Through the distal portion of the incision, an 18‑gauge Tuohy needle is advanced toward the laminotomy/flavectomy site to obtain epidural access under direct visual guidance, and cylindrical electrode arrays are then introduced and positioned to provide coverage of the target dermatomes. The key anchoring innovation consists of fixing the leads to the lamina using a 3–4 mm mini‑plate and screws oriented perpendicular to the leads, providing rigid cranio‑caudal and lateral fixation that resists both axial and rotational displacement. Additional stabilisation is achieved by creating a strain‑relief loop and securing the leads to the dorsal fascia, after which the pulse generator is placed in a subcutaneous pocket. Mollica et al reports no lead displacement in their cohort of 39 patients when using this technique19 Throughout the procedure, neuromonitoring is maintained to minimise the risk of spinal cord compression or neurological injury. The rationale for this approach is that direct visualisation of epidural access reduces dural puncture risk, cylindrical leads offer a lower volumetric profile than paddle leads and may lessen the chance of cord compression, and laminar mini‑plate fixation provides robust multidirectional mechanical anchoring, with technique consistency ensured by a single‑centre team comprising a senior pain surgeon and neurosurgeon. Systems from Abbott, Medtronic, Nevro, and Saluda were used in this series, and the same anchoring technique was used to secure all systems.
Postoperative Follow-Up and Complication Detection
All patients followed a standardised postoperative protocol. Within 7 days of the trial, pain intensity was reassessed using the visual analogue scale (VAS), and at 4–6 weeks after permanent implantation patients underwent clinical review and imaging. Subsequent care consisted of regular clinic visits for ongoing VAS monitoring, optimisation of stimulator programming, and surveillance for complications. Postoperative plain radiographs (anteroposterior and lateral views) were obtained at 4–6 weeks and at final follow‑up, and compared with intraoperative fluoroscopic images to detect lead displacement, defined as any change from the original electrode position. Displacement was identified by a combination of loss of therapeutic paraesthesia requiring reprogramming, radiological evidence of lead migration relative to spinal landmarks, and the emergence of new, off‑target dysaesthesia suggestive of electrode shift; all three patients with displacement had imaging confirmation and received appropriate management.
Results
Systematic Review: Study Identification and Selection
The initial literature search identified 2,847 potentially relevant articles. After duplicate removal, 1,956 unique articles underwent title/abstract screening. In total, 117 articles met full inclusion criteria (see PRISMA flow diagram, Figure 1). Inter-reviewer agreement exceeded 85% at each screening stage.
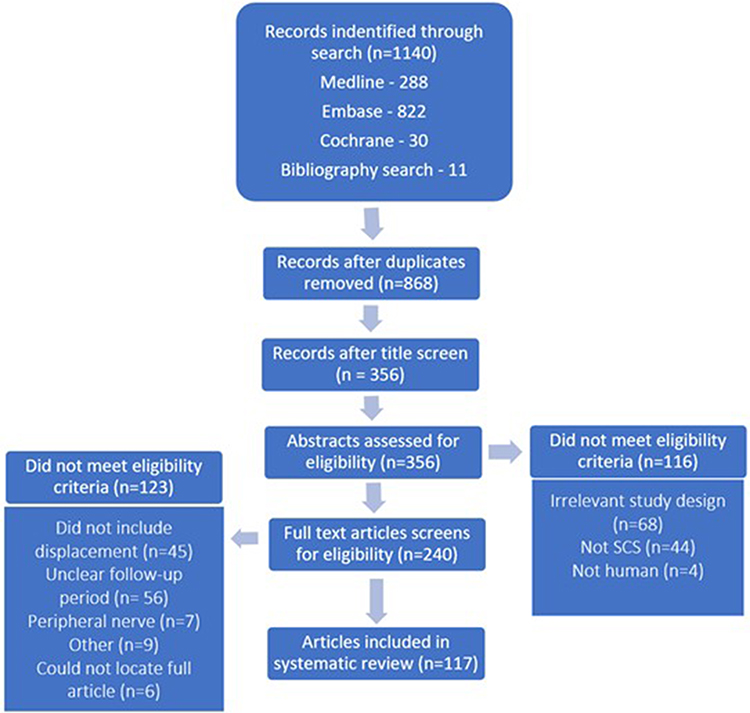 |
Figure 1 PRISMA Diagram. PRISMA flow diagram illustrating the process and rationale of article inclusion and exclusion. |
Systematic Review: Characteristics of Included Studies
The systematic review comprised 117 articles published between 1977 and 2024, with a median publication year of 2015. The dataset included 8 randomised controlled trials (7.0%) and 109 observational studies (93%), spanning prospective and retrospective cohorts, cross‑sectional designs, case series, case reports, and conference abstracts. Across all studies, there were 20,427 participants (range 1–3,947 per study), of whom 1,542 underwent trial SCS electrode placement and 19,677 received permanent SCS implants; some individuals contributed data to both trial and permanent cohorts, whereas others were represented in only one category. The most common indications were failed back surgery syndrome (FBSS; 42.5% of studies), complex regional pain syndrome (CRPS; 28.0%), neuropathic pain (15.5%), chronic pain syndrome (8.5%), and a heterogeneous group of other conditions such as refractory angina, abdominal pain, and headache (5.5%). The median follow‑up duration was 12 months (interquartile range ±21 months), with individual study follow‑up ranging from 0.5 to 120 months.
Systematic Review: Displacement Rates
Across all studies, trial lead displacement occurred in 7.33% of patients (113 out of 1,542 individuals who underwent trial stimulation). Permanent electrode displacement occurred in 6.64% of patients (1,309 among 19,677 individuals with permanent implants).
Systematic Review: Impact of Methodological Quality on Displacement Rates
When studies were stratified by risk of bias, a marked difference in event rates emerged. In low risk-of-bias studies (8,491 patients), the permanent lead displacement rate was 2.1% (180/8,491), whereas in high or serious risk-of-bias studies (5,879 patients) the rate was 7.1% (417/5,879), representing approximately a 3.4‑fold increase. This pattern implies that methodological quality substantially influences reported displacement rates: lower‑risk studies more often used prospective designs, structured follow‑up, standardised outcome definitions, more complete data capture, and longer observation, while higher‑risk studies were typically retrospective, smaller, and characterised by incomplete follow‑up and greater potential for selection bias.
Systematic Review: Quality of Evidence
The overall quality of evidence in the systematic review was variable. Applying the GRADE framework, 47 studies (40.2%) were judged to provide very low‑certainty evidence, 36 (30.8%) low‑certainty evidence, 24 (20.5%) moderate‑certainty evidence, and only 10 (8.5%) high‑certainty evidence. On Newcastle–Ottawa Scale assessment, 67 studies (57.3%) were classified as high risk of bias, 42 (36.2%) as low risk, and 8 (6.8%) as having unclear risk. Among the eight randomised controlled trials, Cochrane risk‑of‑bias evaluation identified three as high risk, two as unclear, and one as low risk, with one additional trial showing a mixture of high, low, and unclear ratings across different domains.
Case Series: Participant Demographics and Indications
All 128 patients in the institutional cohort underwent a 7–10‑day SCS trial, after which 125 (97.7%) achieved a successful trial (defined as ≥50% reduction in VAS pain scores) and proceeded to permanent implantation, while 3 (2.3%) did not and were not implanted. Among the 125 permanent implant recipients, the mean age was 58 years (range 28–82), and 75 (60.0%) were male and 50 (40.0%) female. The mean BMI was 29.4 (range 18.2–47.8), with 48 patients (38.4%) classified as obese (BMI ≥ 30). A depression diagnosis or antidepressant use was documented in 82 patients (65.6%), whereas 43 (34.4%) had no recorded depression; however, psychiatric data were incomplete, with 82 missing entries in the source database. Smoking status was likewise incompletely documented: 32 patients (25.6%) were current smokers, 19 (15.2%) ex‑smokers, and 74 (59.2%) reported never smoking, with 93 missing data points overall. The mean clinical follow‑up after permanent implantation was 32 months (SD 16.8; range 16–48 months).
Case Series: Trial Electrode Outcomes
During the 7–10-day trial period, no lead displacements were observed (0/128; 0%). This appears lower than the 7.33% trial displacement rate identified in the systematic review, although direct comparison is constrained by differences in trial duration, monitoring intensity, and reporting practices across studies.
Case Series: Permanent Electrode Outcomes
Permanent lead displacement occurred in 3 of 125 patients (2.4%), with all events arising within 12 months of implantation (mean 8 months, SD 2.6). The affected patients were all women with depression and elevated BMI and were non‑smokers; two had cervical implants (neuropathic pain and CRPS) and one a thoracic implant for FBSS. Each case presented with caudal migration (one with additional extraspinal displacement and one due to Twiddler’s syndrome), which is shown in Figure 2. All three patients ultimately required surgical revision after unsuccessful reprogramming, with no recurrent displacement during a mean follow‑up of 32 months. Table 3 summarises patient characteristics according to displacement status, and Table 4 shows detailed characteristics of the three cases with permanent electrode displacement.
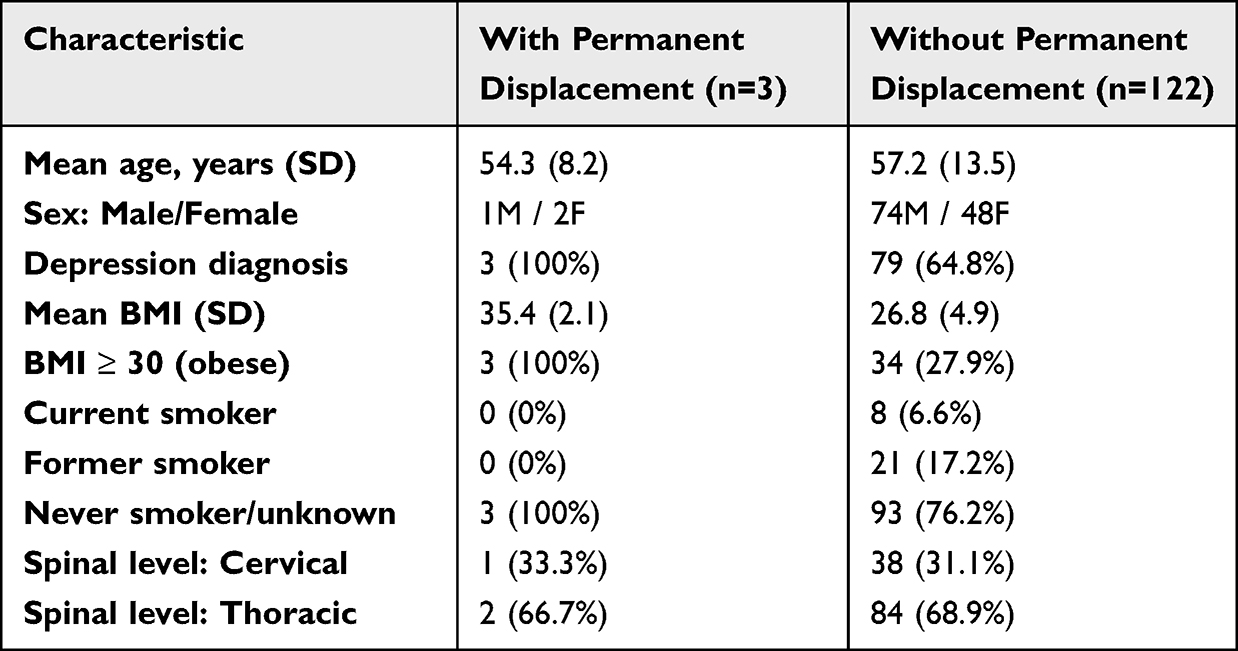 |
Table 3 Patient Characteristics Stratified by Electrode Displacement Status |
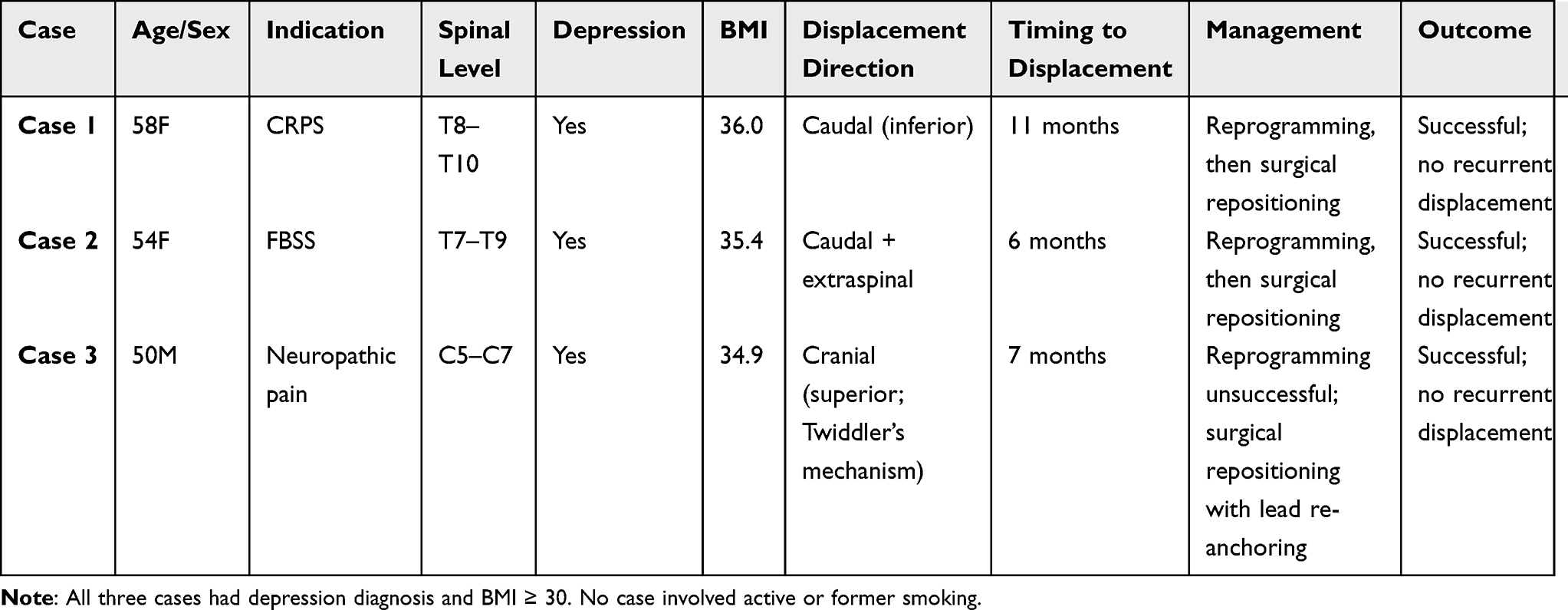 |
Table 4 Detailed Characteristics of Three Cases with Permanent Electrode Displacement |
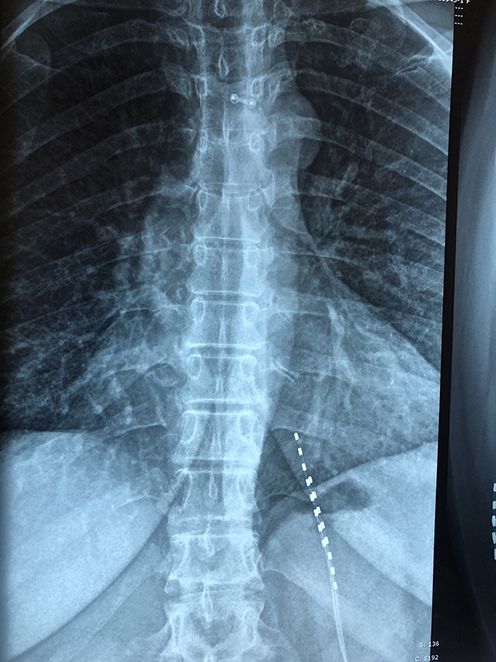 |
Figure 2 Lead Displacement Example on Imaging. |
Case Series: Direction of Displacement
All three displacements showed cranio-caudal (superior-to-inferior) migration. None demonstrated lateral displacement, rotational displacement, or superior (rostral) migration. The anchoring technique employing laminar fixation with perpendicular mini-plate and screws was designed to prevent both lateral and rotational displacement.
Discussion
The systematic review identified 117 studies reporting outcomes in 20,427 patients, with overall displacement rates of 7.33% for trial leads and 6.64% for permanent leads, which are broadly in line with contemporary estimates but lower than older reports of 13–27%.1,8,9,11 This likely reflects advances in implantation techniques and hardware, wider adoption of dedicated anchoring methods, improved imaging and follow‑up, and a growing proportion of prospective studies with clearer complication reporting.
A notable finding was the approximately 3.4‑fold difference in permanent displacement between low risk‑of‑bias studies (2.1%) and high or serious risk‑of‑bias studies (7.1%), indicating that methodological quality strongly influences reported event rates. Higher‑quality studies tended to use prospective designs, standardised definitions, structured follow‑up, and more complete data capture, whereas higher‑risk studies were often retrospective, smaller, and affected by missing data, variable displacement thresholds, and potential selection bias. Overall, only a small minority of studies achieved high‑certainty ratings on GRADE, with most judged to provide low or very low‑certainty evidence, underscoring the limited strength of the current evidence base to inform counselling and consent for SCS.
Compared with historical syntheses reporting displacement rates from 13.2% up to 27%,1,8,9,11 the lower permanent displacement estimate in this review may reflect genuine improvements in technology and technique, changes in the mix of study designs, and possible publication bias favouring more recent, better‑conducted series. Trial displacement (7.33%) was similar in magnitude to permanent displacement (6.64%), but direct comparison is constrained by shorter trial durations, looser fixation of trial leads, and sparse, inconsistent reporting of trial complications in the literature.
In the institutional case series, all three permanent displacements involved caudal migration, consistent with the design of the laminar anchoring construct, which is intended to minimise lateral and rotational movement but cannot completely abolish axial drift. Two of the three events occurred in cervical implants, echoing literature that suggests higher displacement rates in the cervical region because of greater segmental mobility,1,9 and all events occurred within 12 months, in keeping with reports that most clinically relevant migrations arise early before complete fibrous stabilisation and osseointegration.1,20 The observed association between concurrent depression and elevated BMI in all displacement cases, compared with a minority of non‑displacement cases, is consistent with guidelines highlighting higher SCS failure and explantation risk in overweight, depressed patients13 and supports more intensive perioperative counselling and monitoring in this subgroup.
Smoking was not identified as a displacement risk factor in this cohort, in contrast to some reports linking smoking to higher revision or failure rates,12 although the relatively modest smoking prevalence may limit power to detect such an effect. In all three displacement cases, reprogramming failed and surgical revision was required, differing from some series in which reprogramming can restore coverage, particularly with paddle leads that offer broader mediolateral coverage.8 Finally, because the institutional experience relied exclusively on an open laminar anchoring technique while most published studies used percutaneous approaches, the similar or lower displacement rates seen here and in other anchored open series suggest a potential advantage for open anchoring that warrants confirmation in controlled comparative studies, balanced against the greater invasiveness and resource demands of open surgery.
Study Limitations
The systematic review is limited by substantial heterogeneity in study design, patient populations, definitions of displacement, follow‑up protocols, and outcome reporting, which precluded formal meta‑analysis and complicates pooled interpretation of displacement rates. The overall certainty of evidence is constrained by the generally poor methodological quality of many included studies, the inclusion of registry and commercial data that may be prone to favorable reporting, and inconsistent definitions of what constitutes clinically meaningful displacement. Under‑ascertainment is also likely in studies that lacked systematic imaging or structured surveillance for migration, and publication bias cannot be excluded, with a tendency for studies showing particularly high or low complication rates to be preferentially reported.
The institutional case series has additional limitations, including its retrospective design from two proceduralists at a single tertiary center, which restricts external generalisability. The cohort encompassed heterogeneous chronic pain indications (for example, FBSS, CRPS, and neuropathic pain), so the observed outcomes may not reflect disorder‑specific performance, and the small number of displacement events (n = 3) limits the strength of any risk‑factor inferences. The findings relate to one institution’s open laminar anchoring technique and may not apply to percutaneous systems or alternative anchoring strategies, and potential selection bias is present in a regional referral population with complex pain. Finally, missing data for key variables such as depression and smoking status in a substantial proportion of patients and the absence of a contemporaneous control group using a different implantation technique constrain causal interpretation of any apparent protective effect.
Clinical Implications
From a clinical perspective, these findings support more nuanced preoperative counselling and technique planning. Patients with depression and elevated BMI may warrant explicit discussion about their higher risk of adverse SCS outcomes, including displacement and loss of efficacy, and this should inform shared decision‑making around implantation. Where feasible, open approaches with secure, bone‑anchored fixation may offer a mechanistic advantage in reducing displacement compared with standard percutaneous anchoring, although this hypothesis requires confirmation in prospective comparative studies. Cervical SCS implants, in particular, appear to justify heightened clinical and radiographic surveillance for migration, and a structured imaging strategy—such as routine radiographs at 4–6 weeks postoperatively and at long‑term follow‑up—may improve detection of clinically important lead movement. Given the heterogeneity and overall low certainty of the current evidence base, clinicians should communicate that estimates of SCS benefit and complication rates, including displacement, are based on moderate‑to‑low certainty data and may evolve as higher‑quality prospective studies become available.
Future Directions
Future research should prioritise prospective comparative studies that directly evaluate different anchoring techniques and implantation approaches, using standardized definitions and reporting of lead displacement severity in clinical trials. Long-term (at least five‑year) prospective cohorts with systematic radiographic monitoring are needed, alongside mechanistic work exploring scar formation, osseointegration, and the biomechanics of various anchoring strategies. In parallel, studies should investigate which patient factors—such as depression, body mass index, activity level, and behavioural patterns—predict displacement risk, while also developing closed‑loop systems capable of automated lead position monitoring and bioengineered anchoring materials designed to improve mechanical integration.
Conclusion
This systematic review of 117 articles involving 20,427 participants demonstrates overall SCS electrode displacement rates of 7.33% for trial implants and 6.64% for permanent implants. Substantial heterogeneity and variable methodological quality characterize the literature, with low-risk bias studies reporting 3.4-fold lower displacement rates than high-risk bias studies, suggesting methodological quality strongly influences outcomes.
The single-institution case series employing open surgical technique with laminar mini-plate anchoring achieved a 2.4% permanent electrode displacement rate, comparable to low-risk bias studies and lower than historical rates. All displacements were cranio-caudal and successfully managed with surgical revision. Patients with both depression and elevated BMI showed increased displacement risk.
Spine-anchoring techniques involving direct laminar fixation represent a plausible strategy for reducing SCS electrode displacement that merits further evaluation. However, robust comparative prospective studies are needed to definitively establish superiority over alternative techniques. The open surgical approach involves greater operative trauma than percutaneous methods, warranting individualized risk-benefit discussion with patients.
Clinical teams should consider anchoring technique selection, implantation approach, patient risk stratification, and surveillance intensity when counselling patients and selecting therapeutic strategies. Future research should standardize displacement definitions, employ prospective designs, maintain long-term follow-up, and conduct direct technique comparisons.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project did not receive any financial support.
Disclosure
The authors declare no competing interests in this work.
References
1. Cameron T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: a 20-year literature review. J Neurosurg. 2004;100(3):254–12. doi:10.3171/spi.2004.100.3.0254
2. Blackburn AZ, Chang HH, DiSilvestro K, et al. Spinal Cord Stimulation via Percutaneous and Open Implantation: systematic Review and Meta-Analysis Examining Complication Rates. World Neurosurg. 2021;154:132–143. doi:10.1016/j.wneu.2021.07.077
3. O’Connell NE, Ferraro MC, Gibson W, et al. Implanted spinal neuromodulation interventions for chronic pain in adults. Cochrane Database Syst Rev. 2021;2021(12).
4. Traeger AC, Gilbert SE, Harris IA, Maher CG. Spinal cord stimulation for low back pain. Cochrane Database Syst Rev. 2023;3(3). doi:10.1002/14651858.CD014789.pub2
5. Przybysz AG, Vu TN, Pisansky AJ, et al. A systematic review of evidence comparing spinal cord stimulation to sham or conservative medical management in the treatment of persistent spinal pain syndrome - Type 2. Intervent Pain Med. 2025;4(3).
6. North RB, Kidd DH, Farrokhi F, Piantadosi S. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98–107. doi:10.1227/01.NEU.0000144839.65524.E0
7. Gheith R, Wortmann M, Najjar M, et al. Real-World Outcomes of Spinal Cord Stimulation: a Consecutive Institutional Experience with 505 Trials, Trial-to-Implant Ratio, Long-Term Efficacy, and Explantation Risk Factors. J Pain Res. 2025;18:6381–6395. doi:10.2147/JPR.S552361
8. Eldabe S, Buchser E, Duarte RV. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17(2):325–336. doi:10.1093/pm/pnv025
9. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective Review of 707 Cases of Spinal Cord Stimulation: indications and Complications. Pain Pract. 2011;11(2):148–153. doi:10.1111/j.1533-2500.2010.00407.x
10. West T, ElSaban M, Hussain N, et al. Incidence of Lead Migration With Loss of Efficacy or Paresthesia Coverage After Spinal Cord Stimulator Implantation: systematic Review and Proportional Meta-Analysis of Prospective Studies and Randomized Clinical Trials. Neuromodulation. 2023;26(5):917–927. doi:10.1016/j.neurom.2023.03.016
11. Kumar K, Wilson JR, Taylor RS, Gupta S. Complications of spinal cord stimulation, suggestions to improve outcome, and financial impact. J Neurosurg Spine. 2006;5(3):191–203. doi:10.3171/spi.2006.5.3.191
12. Sethi Z, Aijaz T, Ortega-Camacho A, Nasr NF, Knezevic NN. Uncomfortable Paresthesia and Dysesthesia Following Tonic Spinal Cord Stimulator Implantation. Brain Sciences. 2025;15(6):616. doi:10.3390/brainsci15060616
13. Shanthanna H, Eldabe S, Provenzano DA, et al. Evidence-based consensus guidelines on patient selection and trial stimulation for spinal cord stimulation therapy for chronic non-cancer pain. Reg Anesth Pain Med. 2023;48(6):273–287. doi:10.1136/rapm-2022-104097
14. Mironer E, Brown C, Satterthwaite JR, et al. A New Technique of “Midline Anchoring” in Spinal Cord Stimulation Dramatically Reduces Lead Migration. Neuromodulation. 2004;7(1):32–37. doi:10.1111/j.1525-1403.2004.04004.x
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;327:n71. doi:10.1136/bmj.n71
16. Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses; 2000. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
17. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
18. Schünemann HJ, Higgins JP, Vist GE, et al. Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In: Cochrane Handbook for Systematic Reviews of Interventions [Internet]. 2022. www.training.cochrane.org/handbook.
19. Mollica S, Awad M, Teddy PJ. Lead Migration in Neuromodulation. J Clin Neurosci. 2021;90:32–35. doi:10.1016/j.jocn.2021.05.014
20. Al-Kaisy A, Royds J, Al-Kaisy O, et al. Explant rates of electrical neuromodulation devices in 1177 patients in a single center over an 11-year period. Reg Anesth Pain Med. 2020;45(11):883–890. doi:10.1136/rapm-2020-101681
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Interventional Pain Procedures: A Narrative Review Focusing On Safety and Complications. PART 2 Interventional Procedures For Back Pain
Lo Bianco G, Tinnirello A, Papa A, Marchesini M, Day M, Palumbo GJ, Terranova G, Di Dato MT, Thomson SJ, Schatman ME
Journal of Pain Research 2023, 16:761-772
Published Date: 9 March 2023
Real World Clinical Utility of Neurophysiological Measurement Utilizing Closed-Loop Spinal Cord Stimulation in a Chronic Pain Population: The ECAP Study Protocol
Leitner A, Hanson E, Soliday N, Staats P, Levy R, Pope J, Kallewaard JW, Doleys D, Li S, Weisbein J, Amirdelfan K, Poree L
Journal of Pain Research 2023, 16:2497-2507
Published Date: 21 July 2023
Spinal Cord Stimulation for Intractable Visceral Pain Originating from the Pelvic and Abdominal Region: A Narrative Review on a Possible New Indication for Patients with Therapy-Resistant Pain
Bieze M, van Haaps AP, Kapural L, Li S, Ferguson K, de Vries R, Schatman ME, Mijatovic V, Kallewaard JW
Journal of Pain Research 2024, 17:691-736
Published Date: 19 February 2024
A Systematic Guideline by the ASPN Workgroup on the Evidence, Education, and Treatment Algorithm for Painful Diabetic Neuropathy: SWEET
Sayed D, Deer TR, Hagedorn JM, Sayed A, D'Souza RS, Lam CM, Khatri N, Hussaini Z, Pritzlaff SG, Abdullah NM, Tieppo Francio V, Falowski SM, Ibrahim YM, Malinowski MN, Budwany RR, Strand NH, Sochacki KM, Shah A, Dunn TM, Nasseri M, Lee DW, Kapural L, Bedder MD, Petersen EA, Amirdelfan K, Schatman ME, Grider JS
Journal of Pain Research 2024, 17:1461-1501
Published Date: 13 April 2024
Spinal Cord Stimulation Explantation and Chronic Pain: A Systematic Review and Technology Recommendations
Wahezi SE, Yener U, Naeimi T, Lewis JB, Yerra S, Sgobba P, Ciftci HB, Vydyanathan A, Chiu E, Cherkalin D, Darji JY, Masterson R, Lee D, Jarusriwanna A, Palee S, Ortiz NR, Caparo M, Dayon E, Fontaine C, Bikson M, Schatman ME, Pritzlaff SG, Deer TR, Hunter CW
Journal of Pain Research 2025, 18:1327-1340
Published Date: 18 March 2025