Back to Journals » Journal of Pain Research » Volume 16
Interventional Pain Procedures: A Narrative Review Focusing On Safety and Complications. PART 2 Interventional Procedures For Back Pain
Authors Lo Bianco G ![]() , Tinnirello A, Papa A
, Tinnirello A, Papa A ![]() , Marchesini M, Day M, Palumbo GJ, Terranova G, Di Dato MT, Thomson SJ
, Marchesini M, Day M, Palumbo GJ, Terranova G, Di Dato MT, Thomson SJ ![]() , Schatman ME
, Schatman ME ![]()
Received 13 December 2022
Accepted for publication 4 March 2023
Published 9 March 2023 Volume 2023:16 Pages 761—772
DOI https://doi.org/10.2147/JPR.S396215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Giuliano Lo Bianco,1,2 Andrea Tinnirello,3 Alfonso Papa,4 Maurizio Marchesini,5 Miles Day,6 Gaetano Joseph Palumbo,7 Gaetano Terranova,8 Maria Teresa Di Dato,4 Simon J Thomson,9 Michael E Schatman10,11
1Department of Biomedical and Biotechnological Sciences, University of Catania, Catania, Italy; 2Anesthesiology and Pain Department, Fondazione Istituto G. Giglio, Cefalù, Italy; 3Anesthesiology and Pain Medicine Department, ASST Franciacorta, Ospedale di Iseo, Iseo, 25049, Italy; 4Pain Department, AO “Ospedali dei Colli”, Monaldi Hospital, Naples, Italy; 5Mininvasive Surgery Department, Unit of Pain Medicine IRCCS Maugeri Pavia, Pavia, 27100, Italy; 6Pain Research, The Pain Center at Grace Clinic, Texas Tech University HSC, Lubbock, TX, USA; 7Azienda Ospedale - Università Padova, Department of Anesthesia and Intensive Care, Padova, Italy; 8Anaesthesia and Intensive Care Department, Asst Gaetano Pini, Milano, Italy; 9Pain Management, Mid and South Essex University Hospitals NHSFT, Basildon, SS16 5NL, UK; 10Department of Anesthesiology, Perioperative Care, and Pain Medicine, NYU School of Medicine, New York, NY, USA; 11Department of Population Health – Division of Medical Ethics, NYU School of Medicine, New York, NY, USA
Correspondence: Giuliano Lo Bianco, Email [email protected]
Abstract: In patients where conservative approaches have failed to relieve from chronic pain, interventional procedures may be an option in well selected patients. In recent years there has been an increase in the use and development of invasive procedures. Concomitantly, there has also been an increase in the complications associated with these procedures. Taken this into consideration, it is important for healthcare providers to take a cautious and vigilant approach, with a focus on patient safety, in order to minimize the risk of adverse events and ensure the best possible outcome for the patient. This may include careful selection of patients for procedures, use of proper techniques and equipment, and close monitoring and follow-up after the procedure. The aim of this narrative review is to summarize the primary complications associated with commonly performed image-guided (fluoroscopy or ultrasound-guided) interventional procedures and provide strategies to reduce the risk of these complications. We conclude that although complications from interventional pain procedures can be mitigated to a certain degree, they cannot be eliminated altogether. In order to avoid adverse events, patient safety should be given considerable attention and physicians should be constantly aware of the possibility of developing complications.
Keywords: chronic pain, pain management procedures, complications, spinal cord stimulation, intrathecal drug delivery, low back pain
Introduction
Chronic pain is defined by the International Association for the Study of Pain (IASP) such as “pain that persists or recurs for longer than 3 months. Such pain often becomes the sole or predominant clinical problem in some patients”. The most frequent chronic pain condition is low back pain. When conservative treatment fails to relieve pain, interventional procedures may be an alternative option in selected patients. Recent years have witnessed a significant increase in image-guided interventional procedures performed for the management of acute and chronic pain. However, rising numbers of complications related to these procedures has also been observed,1,2 varying from minor to severe and debilitating.3 There is considerable concern regarding severe complications which may occur following interventional procedures for pain treatment. Exceedingly severe complications have been reported,4–11 including infection and spinal cord infarction. The occurrence of adverse events regarding various spine interventions varies greatly and, although detailed evidence-based guidelines are available to reduce the risks associated with these procedures,12 there are considerable variations in clinical practice. A certain procedure carries an inherently non-zero, adverse-effect risk. However, this risk will increase if the technique is employed poorly or incorrectly. Physicians are urged to be heedful of patient safety to ensure that adverse events are reduced to a minimum. The safety of interventional procedures depends not only on physician expertise but also patient selection and preparation. This narrative review aims to describe complications that may result from commonly performed image-guided interventional pain procedures. In this second installment of our three-part series, we analyze complications arising from common interventional pain procedures for chronic back pain. Clinicians frequently propose minimally invasive treatments, such as branch nerve blocks, epidural steroid injections or radiofrequency ablation, when managing non-cancer spinal pain chronic in nature. In 2020, the UK National Institute of Health and Care Excellence (NICE) issued an update to its guidelines confirming this recommendation.13 The American Society of Interventional Pain Physicians (ASIPP) also provided updates in the same year, reiterating their endorsement of interventional pain techniques (facet joint injections, nerve blocks and radiofrequency ablation).14
It is important to understand the potential risks and benefits of each procedure and to carefully consider the individual patient’s medical history and risk factors. In addition, interventional pain procedures should be performed by trained and experienced healthcare professionals, using proper technique and equipment, and with appropriate monitoring and documentation. Patients should be fully informed of the risks and benefits of the procedure, and should be encouraged to ask questions and express any concerns. In our opinion, besides focusing on efficacy and patients’ outcomes, it is essential to emphasize the limitations and potential risks associated with these procedures, thus enabling the clinician to preemptively plan an appropriate clinical strategy to manage any complications which may arise. Regular education and training for healthcare providers, as well as collaboration with interdisciplinary teams, can also help to minimize the risk of adverse events. We conducted a narrative review to summarize the most common complications of interventional pain procedures, their reported incidence and possible strategies to reduce associated risks. The bibliographic research for this review was carried out by three authors (GLB, AT, GJP) using Pubmed, Scopus, Embase and the Cochrane Library for articles published in English between 1/1/1980 and 31/08/2022. The search terms used were “Interventional pain techniques” OR “Epidural Lysis” OR “Spinal Cord Stimualtion” OR “Intrathecal Drug Delivery System” OR “Vertebroplasty” OR “Kyphoplasty” OR “Intradiscal Procedures” OR “IDET” OR “Biacuplasty” OR “Percutaneous Laser Disc Decompression” AND (“Complications” OR “Infection” OR “Neurological Damage” OR “Safety”).
Epidural Lysis
Epidural lysis or epiduroplasty is used to treat chronic pain, mainly radicular, in a multitude of clinical conditions (disc protrusions, spinal stenosis, persistent pain after spinal surgery). It is known to be effective in chronic low-back and lower limb pain.15–17 The estimated incidence of adverse events after this procedure is up to 5%.18 Complications are related to the intervention itself (and, for the most part, immediately apparent) or related to drug administration (typically emerging subsequently).19 Immediate and delayed complications are summarized in Table 1.18–21 Dural puncture is the most reported complication, with Veihelmann et al reporting 2 dural punctures in a sample of 47 patients.21 Dural puncture occurring during epidurolysis is believed to be higher (approx. 4%) than traditional single-shot epidural steroid injections (1 −2%).22 Although dural puncture usually does not require specific intervention, the accidental penetration of hypertonic saline solution into the subdural or intrathecal space can lead to extremely serious complications.23,24 The osmotic properties of the solution can create direct lesion of nerve roots23 and, if injected into the subdural space, may act like a mass lesion.24 In addition to the common and well-known complications associated with epidural injections (dural puncture with associated headache, spinal or epidural haematoma formation), specific complications related to the chemical and osmotic properties of hypertonic saline can occur. Cauda equina syndrome or paraplegia have been reported after accidental penetration for hypertonic saline into the subdural space.23–26 Before injecting hypertonic saline it is mandatory to carefully evaluate the spread of contrast medium in anteroposterior and lateral view, to avoid accidental injection into the subdural spread.19 Local anesthetic (typically 10 mL for lumbar and 5 mL for cervical procedures) should be injected before hypertonic saline, the patient should be monitored for 20 minutes for the manifestation of paresthesias or muscle weakness indicating a possible subdural spread. If a subdural placement of the catheter is suspected the injection of hypertonic saline must be avoided.19 The common fluoroscopically guided caudal approach reduces the risk of hematoma formation compared to higher interlaminar access, as point of entry to the epidural space is nearer to the surface. With the caudal approach, the entry area (sacral hiatus) is more easily compressed than the cervical spinal and lumbar regions, and the nerve roots which supply the lower extremities and most of the bladder and bowel lie highly proximally.27,28 Intravascular injection is a relatively common finding (up to 11% of patients),28,29 although, generally, it is not particularly dangerous, particularly when treating lower lumbar regions. Shearing of the catheter was reported in 1.2% of patients in a retrospective evaluation of 250 procedures,29 and, in one case, a segment of the catheter sheath was torn off completely and remained in the epidural space following catheter withdrawal. The retained catheter fragment generally does not require removal unless the patient becomes symptomatic as a result.29,30 Delayed complications (ie, on the second or third day of a multi-injection lysis protocol) can also occur.31,32 Despite correct initial positioning, the catheter can become displaced and, eventually, subdural or subarachnoid penetration may occur.29 Erdine and Talu29 reported development of permanent paresthesias in 3 of 250 patients, with all 3 reporting symptoms following the third injection of hypertonic saline. Two of these patients experienced urinary incontinence and the third experienced bowel incontinence. The pathophysiology of these late complications is still questionable. Delayed breaching of the dura by the catheter tip or a cumulative effect of repeated hypertonic saline have been hypothesized as causal, although these remain speculative.29 Delayed infections can occur in the form of superficial infection at the skin entry point and, far more dangerous, epidural abscess. These complications have an incidence up to 2%.29
 |
Table 1 Epidural Lysis Immediate and Delayed Complications |
Intradiscal Interventional Procedures
An acute episode of low back pain (LPB) is characterized by frequent recurrences or exacerbations, fluctuating over time, rather than a clinical course that is acute and self-limiting.33 One of the leading causes of chronic LPB are intervertebral disc herniations (approximately 40% of cases).34,35 Surgical intervention had been the only option for those patients not responding well to conventional methods of treating discogenic pain. When conservative treatments fail, intradiscal interventions minimally invasive in nature can be proposed in place of surgery.36 Intradiscal electrothermal therapy (IDET), biacuplasty, percutaneous laser disc decompression (PLDD) are the most commonly performed intradiscal procedures, they have several advantages such as preserving the native disc structure and the incidence of reported complications is low.37 Regarding IDET, procedure complications have been reported in only approximately 0.8% of patients and were usually mild (transient radiculopathy being the most common)38–40 The existing literature for intradiscal biacuplasty shows a good safety profile and no significant perioperative and postoperative complications were reported in various studies41–44. PLDD delivers laser energy into the nucleus pulposus, and in an extended review of 3377 procedures a complication rate of 0.5% was identified.45 Quigley reported severe complications, such as discitis, abdominal perforation o cauda equina syndrome, in less than 1% of patients.46 When compared in a randomized clinical trial to surgery, PLDD showed fewer complications; the rate of unfavorable outcomes in the surgical group was found to be more than double (11% compared to 5%) than the PLDD group.47 Furthermore, a study by Tassi identified a complete absence of complications in the PLDD group.48
Spinal Cord Stimulation
Spinal Cord Stimulation (SCS) is a long-established method, with the first epidural lead implanted in 1967.49 Indications of SCS are type 2 persistent spinal pain syndrome (aka failed back surgery syndrome (FBSS), complex regional pain syndrome (CRPS), neuropathic pain, vascular and ischemic pain, and refractory angina.50,51 The mechanisms of action regarding SCS are not yet fully understood. Gate control theory postulated by Melzack and Wall in 1965 is still deemed to be the basic principle explaining SCS mechanism of action.52,53 Despite being minimally invasive, SCS implantation is connected with a series of complications which need to be considered when scheduling a patient for this procedure. Biological complications (infections, epidural bleeding, CSF leakage), and complications arising from hardware malfunction and human error in implantation should be taken into account. Indeed, the latter are are more common than biological complications, and are responsible for the vast majority of revisions and explants. The total complication rate ranges from 30% to 40% in various studies54 and, as is true of many medical procedures, the complication rate depends on the experience and skill of the implanter. A frequent obstacle arising from the hardware used in SCS is lead migration, with an incidence of up to 20%.55,56 Lead migration has been reported twice as high in patients with cervical placements55 compared to those with lumbar placements. In sacral nerve stimulation, the incidence of lead migration was determined to be as high as for cervical displacement.56 Lead migration is more commonly detected following permanent implantation rather than during the trial phase.57 Despite lead migration not representing a life-threatening condition, it eventually requires revision and reinsertion of the leads if reprograming is ineffective, thereby increasing the risks associated with surgery as well as additional costs. Although less common, lead fractures have also been reported, with the most frequent point of fracture located distal to insertion of the lead into the muscular fascia.57–59 With the advent of new waveforms requiring higher power consumption, rechargeable batteries have become the standard but non-rechargeable devices are still being implanted. A non-rechargeable battery that requires replacement prior to the expected date is defined as “battery failure” and it has an incidence of 1.7–10%.58–61 An additional aspect linked to the hardware which cannot be ignored is pain or discomfort experienced at the battery site or other SCS component sites. This complication which can alter the outcome of therapy and lead to revisions and explants.57 Several factors may contribute to this; however, the size of the implantable pulse generator (IPG) is possibly relevant. Thus, it is highly likely that the complication rate will decrease in the future with the development of more compact IPGs. Among biological complications of SCS the most common is infection,54 and it represents a frequent cause for explantation. In the vast majority of cases, infection occurs at location of the IPG pocket, followed by the lead track and incision site.62 Most infections are caused by staphylococci, although in more than 50% of cases, a specific agent is not identifiable.62 Diabetes, debilitation status, malnutrition, obesity, pre-existing infection, corticosteroid use, autoimmune disorder, poor hygiene, and urinary or fecal incontinence have been reported as risk factors for SCS infection and should be addressed and prevented whenever possible.62 Severe neurological accidents after SCS implantations have been rarely reported. In a case report of a surgically placed paddle lead complicated by epidural abscess the patient reported a permanent paralysis.63 Skin erosion due to hardware is also a rare occurrence, with Cameron et al reporting a rate of 0.2%.58 As with any intervention which requires the insertion of a needle into the epidural space, post dural puncture headaches (PDPH) can ensue.64 Risks factors include young age, female gender, and low body mass index;65 however, the size and shape of the needle have also been demonstrated to contribute greatly to the development of PDPH. Generally, this is a self-limiting condition, managed with bed rest and medications such as caffein, NSAIDs and paracetamol. However, should symptoms persist, a sphenopalatine ganglion block66 or autologous blood patch may be considered initially, as well as surgical revision as a final option.67 The most concerning complication arising from SCS is permanent neurological damage. Intraoperatively, nerve injury can be caused by needle puncture or surgical paddle lead lateral placement, and postoperatively, nerve damage may occur due to epidural hematoma or epidural abscess.54
One fatality has been described in an RCT.68 The authors stated that a dural puncture occurred during procedure and the patient was subsequently discharged after conservative treatment. Three days later, the patient developed a sudden increase in intensity of headache and became unresponsive. A CT scan identified a large subdural hematoma and the patient died 10 days later, despite surgical intervention.68 Complication rates are summarized in Table 2.
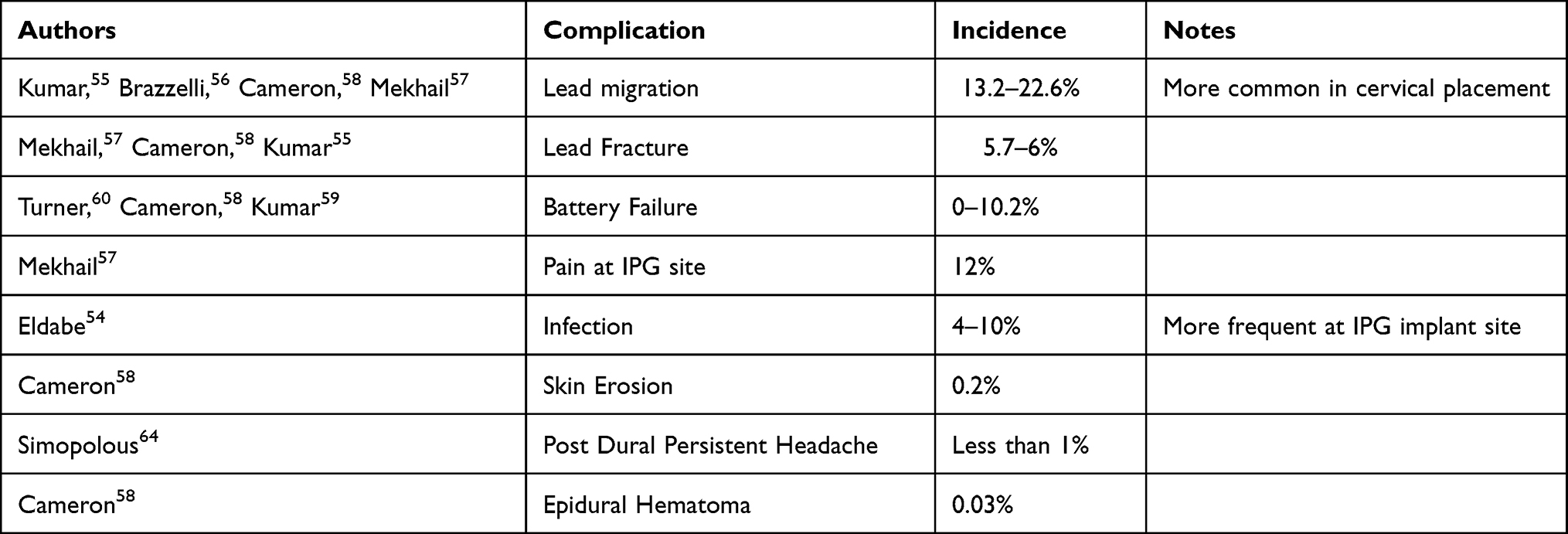 |
Table 2 Rate of Spinal Cord Stimulation (SCS) Complications |
Intrathecal Drug Delivery
Intrathecal drug delivery (ITDD) has been employed successfully in the treatment of cancer pain; however, its efficacy and cost-effectiveness for chronic, non-cancer pain treatment have not yet been established.69–71 One RCT of ITDD demonstrated reduced pain, improved clinical success in pain control, significantly relieved common drug toxicities, and greater survival in patients with refractory cancer pain.71 Several retrospective case series and health economic modelling provide weaker evidence of the clinical efficacy and cost-effectiveness of ITDD in non-cancer pain. The main benefits of implantable, programmable ITDD systems comprise the ability to provide targeted, local delivery of drugs at a constant or adjustable flow, to reduce systemic drug requirements, to reduce side effects, and to increase treatment efficacy.72–74 Complications and side effects which may arise as a result of intrathecal drug delivery systems, similar to any invasive procedure, are well-described in the literature.75 An implantable systems performance registry (ISPR) was generated in 2016 to track performance of ITDD systems, deep brain stimulation and sacral neuromodulation systems, and spinal cord stimulation systems which are commercially available in the United States.76 Between August 2003 and January 2014, data were collected from fifty locations which implanted and followed 6093 patients. Data collection allowed for the creation of an Event Classification, which is still used to estimate the range, incidence and variety of possible adverse effects due to intrathecal drug delivery and pump implantation.76 All the events collected can be grouped into two categories: 1) product performance events, and 2) non-product performance events. Fifty-five percent of patients experienced product-performance events, which can be defined as occurrences feasibly due to the system or its components.76 Non-product performance events can be described as any unexpected event, associated or not with clinical signs, symptoms, illness, or other medical events, appearing or worsening during or after implantation due to the implant procedure, therapy or the delivery of therapy. Hardware and biological complications are summarized in Table 3. Unlike product performance events, which are all related to devices themselves, non-product performance events are all related to clinical practice. For these events, particularly in cancer patients, medical judgment generally plays an important role in their prevention and treatment. Baclofen, for example, or ziconotide infusions to an even greater extent, can result in potentially severe side effects. Side effects include Baclofen withdrawal symptoms (including pruritus, sweating, neurogenic pulmonary edema, anxiety, hyperthermia, seizures, myoclonus, rhabdomyolysis, disseminated intravascular coagulations, multisystem organ failure, cardiac arrest, coma, and death), depression, suicidality, cognitive impairment, decreased levels of consciousness, and raised creatine kinase levels.77–79 Implantation of these devices relatively rarely leads to serious complications; however, particularly in cancer patients suffering from an immunocompromised state, a potentially devastating complication is infection due to their immunocompromised states. The most frequent post-operative infection related to these devices is a surgical site infection (SSI). SSIs are infections occurring within one year of implantation, although this applies only in cases in which the device is not handled, and the infection seems to be associated with surgical implantation.80 According to the classification system for SSIs of the United States Centers for Disease Control and Prevention (CDC), 3 specific infection subtypes can be recognized: superficial-incisional, deep-incisional, and organ space. Superficial-incisional SSIs frequently do not entail re-hospitalization and are commonly detected during outpatient, post-discharge surveillance. Deep incisional and organ space infections are classified as “invasive” SSIs and represent severe infections that typically necessitate hospitalization, treatment with intravenous antibiotic, and potentially surgical revision or device explantation.62 General risk factors for SSIs are leukopenia, diabetes, poor performance status, poor nutritional status, smoking, and use of corticosteroids.62,81,82 Furthermore, cancer patients often receive radio- and/or chemotherapy, which may interfere with wound healing and subsequently increase the risk of infection. The rate of infection following ITDD system implant varies from 0.9% to 6.3%.83–85 Another serious potential complication of ITDD for pain management is catheter-tip-associated granuloma.86 Catheter-tip-associated granulomas can result in potentially serious and sometimes permanent neurological consequences occurring in <3% of patients, if not promptly detected. Since the majority of granulomas are asymptomatic their exact incidence is unknown. Morphine sulfate infusion is most likely linked to the formation of catheter-tip inflammatory masses, particularly when high drug concentrations are associated with slow infusion rates.87 Reduced flow of cerebrospinal fluid (CSF) around the catheter tip, as in spinal stenosis or after spinal surgery, are risk factors for granuloma formation.88 Remarkably, granuloma development has also been found with the use of baclofen.88 In conclusion, ITDD is potentially highly successful for managing chronic pain in suitably selected patients. Complications associated with ITDD are primarily pharmacologic and momentary. However, it is imperative to minimize these risks through correct hardware selection and scrupulous care with the implant procedure. The involvement of staff specialized in these procedures can dramatically diminish adverse events and complications. ITDD can represent a safe and feasible solution for the management of pain and can be considered for chronic refractory pain due to multiple etiologies.
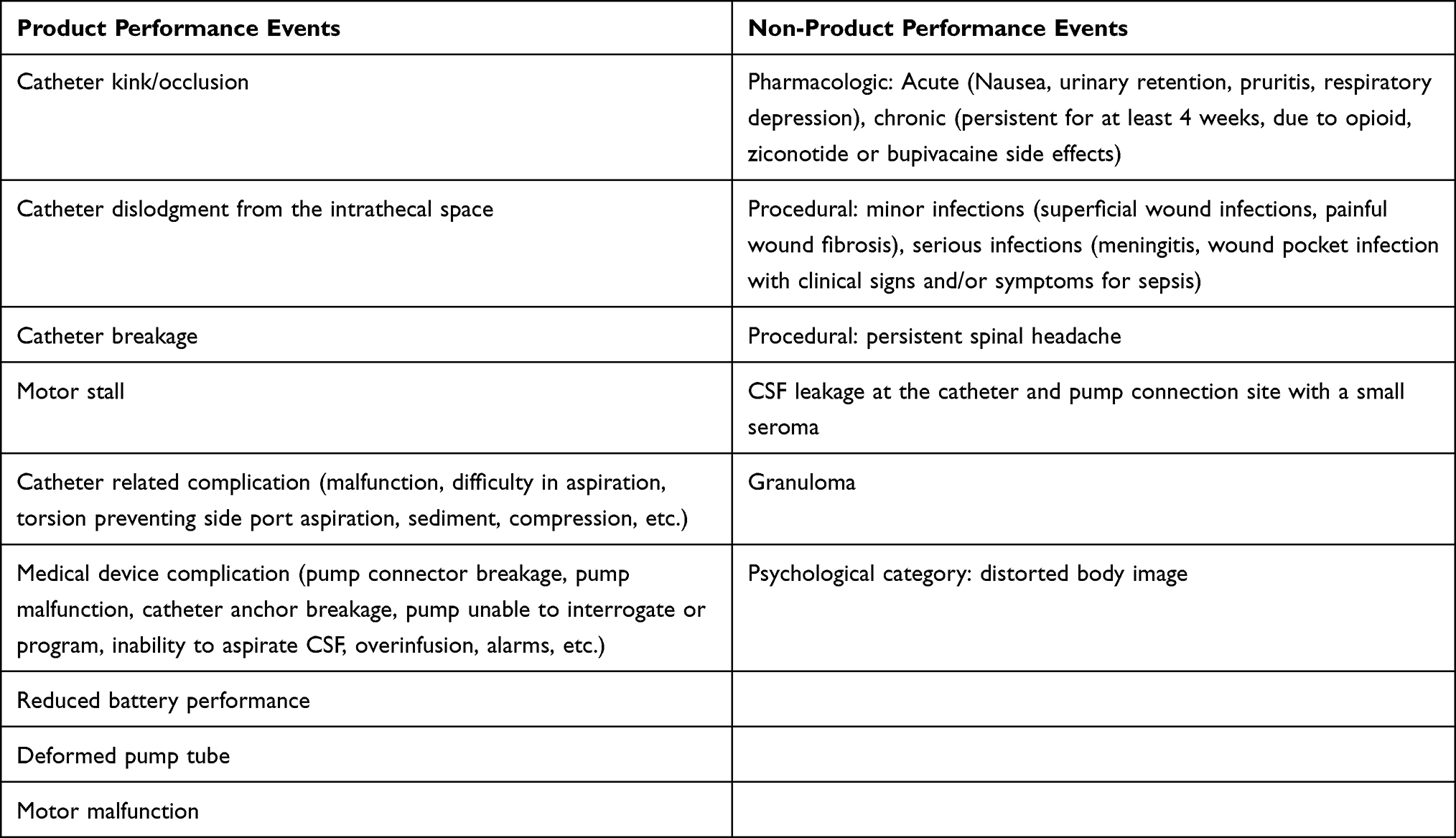 |
Table 3 Product Performance Events Vs Non-Product Performance Events |
Vertebroplasty and Kyphoplasty
Percutaneous vertebroplasty (VP) and balloon kyphoplasty (BKP) are minimally invasive procedures performed to stabilize painful vertebral fractures. Despite advancements in vertebral augmentation techniques, various complications have been reported.89 Serious complications have been described, such as pedicular fractures, segmental nerve and spinal cord injury, bone cement extrusion to the spinal canal and intradiscal, infection, pulmonary embolism, cerebral embolism, cardiac perforation, and death.90–92 Risks linked to cement extrusion from the vertebra into the spinal canal have been found to be markedly increased for VP.93 No significant difference was reported for subsequent fractures between the procedures.94 A meta-analysis comparing complications of percutaneous VP and BKP to treat osteoporotic vertebral compression showed no significative differences regarding subsequent fractures.95 Additionally, regarding disc spaces extravasations, no substantial differences were found between one intervention and the other. In contrast, total extravasations and paravertebral extravasations rates were found to be significantly higher in the VP group compared to the BKP group.95 A study reviewing 100 radiographs of consecutive balloon kyphoplasties found the overall cement leakage rate to be 31%, with most leakages anterior and superior.96 Only 2% were posterior and most leakages were less than 3 mm. Regarding the location of leakages reported in kyphoplasties, 48% were paraspinal, 38% intradiscal, 11% epidural, 1.5% pulmonary, and 1.5% foraminal.97 Epidural cement leakage appeared to cause the most serious neurological outcomes.98
After performing kyphoplasty, one should exclude any new symptoms that may appear in a postoperative setting. Patients may experience improvement in back pain with an epidural cement spread; however, new symptoms may appear in the lower extremities, such as radicular pain, weakness and numbness. These patients may not ambulate or perform a positive straight leg raise. Cement spread into the paravertebral veins can result in pulmonary embolism or cardiorespiratory distress.97 After assessing post-procedure radiographs of 64 patients, researchers found no significant correlation between cement embolism to the lungs and the type of procedure performed, even though kyphoplasty had a lower incidence of cement leak than vertebroplasty.99 For cases in which a vertebral wall is not intact, a method known as the “eggshell” method was proposed by Greene et al in 2007.100 Antero-posterior and lateral images are obtained if cortical bone is violated during initial balloon inflation.100 The balloon is then deflated and removed, and a small quantity of doughy cement is injected to repair the defect. The balloon can then be inserted once again and inflated slowly, thus expanding against the cement. Once hardened, a barrier of cement stops extravasation of subsequent cement injection.100 Success in this technique requires the consistency of the cement to be paste-like rather than more fluid. Polymethyl methacrylate (PMMA) can spread from the perivertebral and azygos veins to the inferior vena cava, and eventually to the pulmonary veins.99,101,102 When injecting, large volumes of cement, high PMMA pressure and relatively liquescent cement may contribute to vascular PMMA uptake. Host factors such as higher vertebral body vascularity, due to invasive vascular tumors, and the occurrence of osteoporosis may also contribute to greater PMMA vascular uptake. Subsequent cement embolic phenomenon comprises inferior vena cava thrombosis,102 cardiac tamponade from cement penetration in the right ventricle, renal artery pulmonary cement embolism (PCE) and other peripheral arterial emboli. Most reported cases of PCE are without symptoms. In order to reduce the occurrence of vascular PMMA uptake during VP and KP, recommendations include providing abdominal support to the patient to maintain elevated venous pressure, the use of blush venography before injection, injection of the appropriate amount of cement, injection without excessive pressure, avoidance of excessive cement liquescency, and vigilance for cement extravasation - aborting the procedure if this occurs.103,104 The patient should be closely monitored for an extended period following intervention for cardiorespiratory symptoms, such as chest pain and shortness of breath. The responsible physician must be notified immediately should any such symptoms occur days and even weeks post-procedure. Overall, BKP appears to be safer than VP. Symptomatic complications are rare with both procedures; however, further research is needed to be able to offer more detailed and complete conclusions.
Conclusion
Pain has several dimensions and is best approached through a multimodal paradigm, of which interventional approaches are an important aspect. This narrative review has sought to provide a preliminary evaluation of evidence regarding safety and complications of interventional pain procedures for managing spinal pain. We conclude that interventional spine procedures are generally safely performed when adhering to evidence-based practice guidelines. However, it is essential to emphasize the limits and possible risks associated with these procedures, thereby enabling the clinician to plan a clinical strategy that can manage any complications which may arise.
Overall, the goal of interventional pain procedures is to improve the patient’s quality of life and to provide effective pain management. While complications can occur, they can often be prevented or minimized through careful consideration of patient selection, adherence to guidelines and best practices, and close monitoring and follow-up. In Table 4 we summarized the most dangerous and preventable complications of interventional procedures, including risk factors and strategies to decrease the occurrence of these complications. Irrespective of claims that interventional procedures are perfectly safe, we posit that no treatment of pain is absolutely safe. In conclusion, it is important for healthcare providers to be aware of the potential complications associated with image-guided interventional procedures and to take steps to minimize the risk of adverse events. This includes following established guidelines for infection prevention, discontinuing anticoagulants or antiaggregants as recommended, and being knowledgeable about the specific strategies and techniques used for each procedure. Additionally, close communication with the patient, including informed consent and discussion of potential risks and benefits, is critical for ensuring patient safety and satisfaction.
 |
Table 4 Summarize of Procedures, Indications, Complications, and Possible Safety Measures |
Disclosure
Dr Giuliano Lo Bianco reports personal fees from Stryker Italia, outside the submitted work. Dr Andrea Tinnirello reports personal fees from Avanos Medical, outside the submitted work. Dr Simon J Thomson reports personal fees from Boston Scientific Neuromodulation, Saluda Medical, Mainstay Medical, Galvani Bioelectronics, outside the submitted work. Dr Michael E Schatman is a research consultant for Modoscript, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Manchikanti L, Hirsch JA, Pampati V, Boswell MV. Utilization of facet joint and sacroiliac joint interventions in medicare population from 2000 to 2014: explosive growth continues. Curr Pain Headache Rep. 2016;20(10). doi:10.1007/S11916-016-0588-2
2. Hospital Episode Statistics (HES): Admitted patient care - procedures and interventions - NHS dataset. Available from: https://www.data.gov.uk/dataset/dc63429a-c689-4531-a8cb-12e342960428/hospital-episode-statistics-hes-admitted-patient-care-procedures-and-interventions.
3. Hynes JP, Fhlatharta MN, Ryan JW, MacMahon PJ, Eustace SJ, Kavanagh EC. Complications in image-guided musculoskeletal injections. Skeletal Radiol. 2021;50(2):343–349. doi:10.1007/S00256-020-03565-Y
4. Cooper AB, Sharpe MD. Bacterial meningitis and cauda equina syndrome after epidural steroid injections. Can J Anaesth. 1996;43(5 Pt 1):471–474. doi:10.1007/BF03018109
5. Epstein N. The risks of epidural and transforaminal steroid injections in the Spine: commentary and a comprehensive review of the literature. Surg Neurol Int. 2013;4(Suppl):2. doi:10.4103/2152-7806.109446
6. Glaser SE, Falco F. Paraplegia following a thoracolumbar transforaminal epidural steroid injection. Pain Physician. 2005;8(3):309–314. doi:10.36076/ppj.2005/8/309
7. Goodman BS, Posecion LWF, Mallempati S, Bayazitoglu M. Complications and pitfalls of lumbar interlaminar and transforaminal epidural injections. Curr Rev Musculoskelet Med. 2008;1:3–4. doi:10.1007/S12178-008-9035-2
8. Hooten WM, Mizerak A, Carns PE, Huntoon MA. Discitis after lumbar epidural corticosteroid injection: a case report and analysis of the case report literature. Pain Med. 2006;7(1):46–51. doi:10.1111/J.1526-4637.2006.00088.X
9. Huntoon MA, Martin DP. Paralysis after transforaminal epidural injection and previous spinal surgery. Reg Anesth Pain Med. 2004;29(5):494–495. doi:10.1016/j.rapm.2004.05.002
10. Muffoletto AJ, Ketonen LM, Mader JT, Crow WN, Hadjipavlou AG. Hematogenous pyogenic facet joint infection. Spine. 2001;26(14):1570–1576. doi:10.1097/00007632-200107150-00014
11. Wybier M, Gaudart S, Petrover D, Houdart E, Laredo JD. Paraplegia complicating selective steroid injections of the lumbar spine. Report of five cases and review of the literature. Eur Radiol. 2010;20(1):181–189. doi:10.1007/S00330-009-1539-7
12. Bogduk N. Practice Guidelines for Spinal Diagnostic Procedures.
13. NICE guideline [NG59]. Low back pain and sciatica in over 16S: assessment and management. Available from: https://www.nice.org.uk/guidance/ng59/chapter/Update-information.
14. Manchikanti L, Kaye AD, Soin A, et al. Comprehensive evidence-based guidelines for facet joint interventions in the management of chronic spinal pain: American society of interventional pain physicians (ASIPP) guidelines facet joint interventions 2020 guidelines. Pain Physician. 2020;23(3S):S1–S127. doi:10.36076/ppj.2020/23/S1
15. Helm S, Gerdesmeyer L, Justiz R, et al. Percutaneous and endoscopic adhesiolysis in managing low back and lower extremity pain: a systematic review and meta-analysis. PubMed. 2022;19(2):E245.
16. Gerdesmeyer L, Noe C, Prehn-Kristensen A, et al. Long-term efficacy of percutaneous epidural neurolysis of adhesions in chronic lumbar radicular pain: 10 year follow-up of a randomized controlled trial. Pain Physician. 2021;24(5):359–367. doi:10.36076/ppj.2021.24.359
17. Vigneri S, Sindaco G, la Grua M, et al. Electrocatheter-mediated high-voltage pulsed radiofrequency of the dorsal root ganglion in the treatment of chronic lumbosacral neuropathic pain: a randomized controlled study. Clin J Pain. 2020;36(1):25–33. doi:10.1097/AJP.0000000000000766
18. Lee F, Jamison DE, Hurley RW, Cohen SP. Epidural lysis of adhesions. Korean J Pain. 2014;27(1):3–15. doi:10.3344/KJP.2014.27.1.3
19. Erdine S, Talu G. Precautions during epidural neuroplasty. Pain Pract. 2002;2(4):308–314. doi:10.1046/J.1533-2500.2002.02038.X
20. Lee HY, Wang HS, Kim SW, Ju C. Cerebellar infarction following epidural abscess after epidural neuroplasty. Korean J Spine. 2015;12(1):26. doi:10.14245/KJS.2015.12.1.26
21. Veihelmann A, Devens C, Trouillier H, Birkenmaier C, Gerdesmeyer L, Refior HJ. Epidural neuroplasty versus physiotherapy to relieve pain in patients with sciatica: a prospective randomized blinded clinical trial. J Orthop Sci. 2006;11(4):365–369. doi:10.1007/S00776-006-1032-Y
22. Bhatia A, Nelson A, Cohen SP. Breaking Bad (Tissue): epidural Adhesiolysis and Its Outcomes. Anesth Analg. 2017;124(6):1755–1757. doi:10.1213/ANE.0000000000001931
23. Birkenmaier C, Redeker J, Sievers B, Melcher C, Jansson V, Mayer-Wagner S. An evaluation of medications commonly used for epidural neurolysis procedures in a human fibroblast cell culture model. Reg Anesth Pain Med. 2011;36(2):140–144. doi:10.1097/AAP.0B013E31820D41C4
24. Lucas JT, Ducker TB, Perot PL. Adverse reactions to intrathecal saline injection for control of pain. J Neurosurg. 1975;42(5):557–561. doi:10.3171/JNS.1975.42.5.0557
25. Ho KY, Manghnani P. Acute monoplegia after lysis of epidural adhesions: a case report. Pain Pract. 2008;8(5):404–407. doi:10.1111/J.1533-2500.2008.00229.X
26. Justiz R, Taylor V, Day M. Neurogenic bladder: a complication after endoscopic adhesiolysis with return of bladder function while using nitrofurantoin. Anesth Analg. 2010;110(5):1496–1498. doi:10.1213/ANE.0B013E3181D77340
27. Wong GK, Arab AA, Chew SC, Naser B, Crawford MW. Major complications related to epidural analgesia in children: a 15-year audit of 3152 epidurals. Can J Anaesth. 2013;60(4):355–363. doi:10.1007/S12630-012-9877-3
28. Manchikanti L, Malla Y, Wargo BW, Cash KA, Pampati V, Fellows B. Complications of fluoroscopically directed facet joint nerve blocks: a prospective evaluation of 7500 episodes with 43,000 nerve blocks. Pain Physician. 2012;2;15:E143–E150. doi:10.36076/ppj.2012/15/E143
29. Talu GK, Erdine S. Complications of epidural neuroplasty: a retrospective evaluation. Neuromodulation. 2003;6(4):237–247. doi:10.1046/J.1525-1403.2003.03031.X
30. Kim TH, Shin JJ, Lee WY. Surgical treatment of a broken neuroplasty catheter in the epidural space: a case report. J Med Case Rep. 2016;10(1):1–6. doi:10.1186/S13256-016-1064-7
31. Wagner KJ, Sprenger T, Pecho C, et al. Schwerwiegende Risiken und Komplikationen der epiduralen Neurolyse nach Racz [Risks and complications of epidural neurolysis -- a review with case report]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2006;41(4):213–222. German. doi:10.1055/S-2006-925232
32. Kim SB, Kim MK, Kim KD, Lim YJ. Unintended complication of intracranial subdural hematoma after percutaneous epidural neuroplasty. J Korean Neurosurg Soc. 2014;55(3):170–172. doi:10.3340/JKNS.2014.55.3.170
33. Korff M. Studying the natural history of back pain. Spine (Phila Pa. 1994;19(18Suppl):2041S–2046S. doi:10.1097/00007632-199409151-00005
34. Kallewaard JW, Terheggen MAMB, Groen GJ, et al. Discogenic low back pain. Pain Pract. 2010;10(6):560–579. doi:10.1111/J.1533-2500.2010.00408.X
35. Lambeek LC, van Mechelen W, Knol DL, Loisel P, Anema JR. Randomised controlled trial of integrated care to reduce disability from chronic low back pain in working and private life. BMJ. 2010;340(7749):750. doi:10.1136/BMJ.C1035
36. Kapural L, Mekhail N. Novel intradiscal biacuplasty (IDB) for the treatment of lumbar discogenic pain. Pain Pract. 2007;7(2):130–134. doi:10.1111/J.1533-2500.2007.00120.X
37. Singh V, Manchikanti L, Benyamin RM, Helm S, Hirsch JA. Percutaneous lumbar laser disc decompression: a systematic review of current evidence. Pain Physician. 2009;12(3):573–588. doi:10.36076/ppj.2009/12/573
38. Freeman BJC. IDET: a critical appraisal of the evidence. Eur Spine J. 2006;15(Suppl3):448–457. doi:10.1007/S00586-006-0156-2
39. Andersson GBJ, Mekhail NA, Block JE. Treatment of intractable discogenic low back pain. A systematic review of spinal fusion and intradiscal electrothermal therapy (IDET) - PubMed. Pain Physician. 2006;2006:237–248.
40. Freeman BJC, Fraser RD, Cain CMJ, Hall DJ, Chapple DCL. A randomized, double-blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine. 2005;30(21):2369–2377. doi:10.1097/01.BRS.0000186587.43373.F2
41. Kapural L, Vrooman B, Sarwar S, et al. Radiofrequency intradiscal biacuplasty for treatment of discogenic lower back pain: a 12-month follow-up. Pain Med. 2015;16(3):425–431. doi:10.1111/PME.12595
42. Kapural L, Ng A, Dalton J, et al. Intervertebral disc biacuplasty for the treatment of lumbar discogenic pain: results of a six-month follow-up. Pain Med. 2008;9(1):60–67. doi:10.1111/J.1526-4637.2007.00407.X
43. Karaman H, Tüfek A, Gö K, et al. 6-month results of TransDiscal Biacuplasty on patients with discogenic low back pain: preliminary findings. Int J Med Sci. 2010;8(1):1–8. doi:10.7150/IJMS.8.1
44. Desai MJ, Kapural L, Petersohn JD, et al. Twelve-month follow-up of a randomized clinical trial comparing intradiscal biacuplasty to conventional medical management for discogenic lumbar back pain. Pain Med. 2017;18(4):751–763. doi:10.1093/PM/PNW184
45. Hellinger J. Complications of non-endoscopic percutaneous laser disc decompression and nucleotomy with the neodymium: YAG laser 1064 nm. Photomed Laser Surg. 2004;22(5):418–422. doi:10.1089/PHO.2004.22.418
46. Quigley MR. Percutaneous laser discectomy. Neurosurg Clin N Am. 1996;7(1):37–42. doi:10.1016/s1042-3680(18
47. Brouwer PA, Brand R, van den Akker-Van Marle ME, et al. Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. Spine J. 2015;15(5):857–865. doi:10.1016/J.SPINEE.2015.01.020
48. Tassi GP. Comparison of results of 500 microdiscectomies and 500 percutaneous laser disc decompression procedures for lumbar disc herniation. Photomed Laser Surg. 2006;24(6):694–697. doi:10.1089/PHO.2006.24.694
49. Shealy CN, Mortimer JT, Reswick JB. Electrical inhibition of pain by stimulation of the dorsal columns: preliminary clinical report. Anesth Analg. 1967;46:489???491. doi:10.1213/00000539-196707000-00025
50. Lo Bianco G, Papa A, Gazzerro G, et al. Dorsal root ganglion stimulation for chronic postoperative pain following thoracic surgery: a pilot study. Neuromodulation. 2021;24(4):774–778. doi:10.1111/NER.13265
51. Deer TR, Krames E, Mekhail N, et al. The appropriate use of neurostimulation: new and evolving neurostimulation therapies and applicable treatment for chronic pain and selected disease states. neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):599–615. doi:10.1111/NER.12204
52. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/SCIENCE.150.3699.971
53. Malinowski MN, Chopra PR, Francio VT, Budwany R, Deer TR. A narrative review and future considerations of spinal cord stimulation, dorsal root ganglion stimulation and peripheral nerve stimulation. Curr Opin Anaesthesiol. 2021;34(6):774–780. doi:10.1097/ACO.0000000000001072
54. Eldabe S, Buchser E, Duarte R. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17(2):325–336. doi:10.1093/PM/PNV025
55. Kumar K, Hunter G, Demeria D. Spinal cord stimulation in treatment of chronic benign pain: challenges in treatment planning and present status, a 22-year experience. Neurosurgery. 2006;58(3):481–494. doi:10.1227/01.NEU.0000192162.99567.96
56. Brazzelli M, Murray A, Fraser C. Efficacy and safety of sacral nerve stimulation for urinary urge incontinence: a systematic review. J Urol. 2006;175(3 Pt 1):835–841. doi:10.1016/S0022-5347(05)00326-5
57. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective review of 707 cases of spinal cord stimulation: indications and complications. Pain Pract. 2011;11(2):148–153. doi:10.1111/J.1533-2500.2010.00407.X
58. Cameron T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: a 20-year literature review. J Neurosurg. 2004;100(3):254–267. doi:10.3171/SPI.2004.100.3.0254
59. Kumar K, Taylor RS, Jacques L, et al. The effects of spinal cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective randomized controlled multicenter trial of the effectiveness of spinal cord stimulation. Neurosurgery. 2008;63(4):762–768. doi:10.1227/01.NEU.0000325731.46702.D9
60. Turner JA, Loeser JD, Deyo RA, Sanders SB. Spinal cord stimulation for patients with failed back surgery syndrome or complex regional pain syndrome: a systematic review of effectiveness and complications. Pain. 2004;108(1–2):137–147. doi:10.1016/j.pain.2003.12.016
61. North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98–106. doi:10.1227/01.NEU.0000144839.65524.E0
62. Follett KA, Boortz-Marx RL, Drake JM, et al. Prevention and management of intrathecal drug delivery and spinal cord stimulation system infections. Anesthesiology. 2004;100(6):1582–1594. doi:10.1097/00000542-200406000-00034
63. Levy R, Henderson J, Slavin K, et al. Incidence and avoidance of neurologic complications with paddle type spinal cord stimulation leads. Neuromodulation. 2011;14(5):412–422. doi:10.1111/J.1525-1403.2011.00395.X
64. Simopoulos TT, Sharma S, Aner M, Gill JS. The incidence and management of postdural puncture headache in patients undergoing percutaneous lead placement for spinal cord stimulation. Neuromodulation. 2016;19(7):738–743. doi:10.1111/NER.12445
65. Jabbari A, Alijanpour E, Mir M, Hashem NB, Rabiea SM, Rupani MA. Post spinal puncture headache, an old problem and new concepts: review of articles about predisposing factors. Caspian J Intern Med. 2013;4(1):595.
66. Jespersen MS, Jaeger P, Ægidius KL, et al. Sphenopalatine ganglion block for the treatment of postdural puncture headache: a randomised, blinded, clinical trial. Br J Anaesth. 2020;124(6):739–747. doi:10.1016/J.BJA.2020.02.025
67. Cohen S, Levin D, Mellender S, et al. Topical sphenopalatine ganglion block compared with epidural blood patch for postdural puncture headache management in postpartum patients: a retrospective review. Reg Anesth Pain Med. 2018;43(8):880–884. doi:10.1097/AAP.0000000000000840
68. Slangen R, Schaper NC, Faber CG, et al. Spinal cord stimulation and pain relief in painful diabetic peripheral neuropathy: a prospective two-center randomized controlled trial. Diabetes Care. 2014;37(11):3016–3024. doi:10.2337/DC14-0684
69. Kumar K, Rizvi S, Bishop S. Cost effectiveness of intrathecal drug therapy in management of chronic nonmalignant pain. Clin J Pain. 2013;29(2):138–145. doi:10.1097/AJP.0B013E31824B5FC9
70. Kumar K, Hunter G, Demeria DD. Treatment of chronic pain by using intrathecal drug therapy compared with conventional pain therapies: a cost-effectiveness analysis. J Neurosurg. 2002;97(4):803–810. doi:10.3171/JNS.2002.97.4.0803
71. Smith TJ, Staats PS, Deer T, et al. Randomized clinical trial of an implantable drug delivery system compared with comprehensive medical management for refractory cancer pain: impact on pain, drug-related toxicity, and survival. J Clin Oncol. 2002;20(19):4040–4049. doi:10.1200/JCO.2002.02.118
72. Krames ES. Intrathecal infusional therapies for intractable pain: patient management guidelines. J Pain Symptom Manage. 1993;8(1):36–46. doi:10.1016/0885-3924(93)90118-F
73. Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anaesth. 1995;42(10):891–903. doi:10.1007/BF03011037
74. Naumann C, Erdine S, Koulousakis A, van Buyten JP, Schuchard M. Drug adverse events and system complications of intrathecal opioid delivery for pain: origins, detection, manifestations, and management. Neuromodulation. 1999;2(2):92–107. doi:10.1046/J.1525-1403.1999.00092.X
75. Kamran S, Wright BD. Complications of intrathecal drug delivery systems. Neuromodulation. 2001;4(3):111–115. doi:10.1046/J.1525-1403.2001.00111.X
76. Konrad PE, Huffman JM, Stearns LM, et al. Intrathecal drug delivery systems (IDDS): the implantable systems performance registry (ISPR). Neuromodulation. 2016;19(8):848–856. doi:10.1111/NER.12524
77. Deer TR, Pope JE, Hanes MC, McDowell GC. Intrathecal therapy for chronic pain: a review of morphine and ziconotide as firstline options. Pain Med. 2019;20(4):784–798. doi:10.1093/PM/PNY132
78. Winter G, Beni-Adani L, Ben-Pazi H. Intrathecal baclofen therapy-practical approach: clinical benefits and complication management. J Child Neurol. 2018;33(11):734–741. doi:10.1177/0883073818785074
79. Matis G, de Negri P, Dupoiron D, Likar R, Zuidema X, Rasche D. Intrathecal pain management with ziconotide: time for consensus? Brain Behav. 2021;11(Suppl1). doi:10.1002/BRB3.2055
80. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. centers for disease control and prevention (CDC) hospital infection control practices advisory committee. Am J Infect Control. 1999;20(4):247–80.
81. Neumayer L, Hosokawa P, Itani K, El-Tamer M, Henderson WG, Khuri SF. Multivariable predictors of postoperative surgical site infection after general and vascular surgery: results from the patient safety in surgery study. J Am Coll Surg. 2007;204(6):1178–1187. doi:10.1016/J.JAMCOLLSURG.2007.03.022
82. Sørensen LT. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: a systematic review and meta-analysis. Arch Surg. 2012;147(4):373–383. doi:10.1001/ARCHSURG.2012.5
83. Engle MP, Vinh BP, Harun N, Koyyalagunta D. Infectious complications related to intrathecal drug delivery system and spinal cord stimulator system implantations at a comprehensive cancer pain center. Pain Physician. 2013;3;16:251–257. doi:10.36076/ppj.2013/16/251
84. Sindt JE, Larsen SD, Dalley AP, Collier WH, Brogan SE. The rate of infectious complications after intrathecal drug delivery system implant for cancer-related pain is low despite frequent concurrent anticancer treatment or leukopenia. Anesth Analg. 2020;131(1):280–287. doi:10.1213/ANE.0000000000004639
85. Scanlon MM, Gazelka HM, Moeschler SM, et al. Surgical site infections in cancer patients with intrathecal drug delivery devices. Pain Med. 2017;18(3):520–525. doi:10.1093/PM/PNW203
86. Haering M, Saleh C, Jaszczuk P, Koehler M, Hund-Georgiadis M. Intrathecal pump catheter-tip granuloma recurrence with associated myelomalacia - How safe is intrathecal analgesic infusion therapy? A case report. Surg Neurol Int. 2019;10(62):1–4. doi:10.25259/SNI-33-2019
87. Deer TR, Prager J, Levy R, et al. Polyanalgesic Consensus Conference--2012: consensus on diagnosis, detection, and treatment of catheter-tip granulomas (inflammatory masses). Neuromodulation. 2012;15(5):483–496. doi:10.1111/J.1525-1403.2012.00449.X
88. Deer TR, Raso LJ, Coffey RJ, Allen JW. Intrathecal baclofen and catheter tip inflammatory mass lesions (granulomas): a reevaluation of case reports and imaging findings in light of experimental, clinicopathological, and radiological evidence. Pain Med. 2008;9(4):391–395. doi:10.1111/J.1526-4637.2008.00468.X
89. Zhang J, Poffyn B, Sys G, Uyttendaele D. Comparison of vertebroplasty and kyphoplasty for complications. Orthop Surg. 2011;3(3):158–160. doi:10.1111/J.1757-7861.2011.00141.X
90. Al-Nakshabandi NA. Percutaneous vertebroplasty complications. Ann Saudi Med. 2011;31(3):294–297. doi:10.4103/0256-4947.81542
91. Chotivichit A, Korwutthikulrangsri E, Churojana A, Songsaeng D. Complications in vertebroplasty. J Med Assoc Thai. 2022;95(Suppl 9):S75–81.
92. Saracen A, Kotwica Z. Complications of percutaneous vertebroplasty: an analysis of 1100 procedures performed in 616 patients. Medicine. 2016;95:24. doi:10.1097/MD.0000000000003850
93. Zou D, Dong S, Du W, Sun B, Wu X. Risk factor analysis of pulmonary cement embolism during percutaneous vertebroplasty or kyphoplasty for osteoporotic vertebral compression fractures. J Orthop Surg Res. 2021;16(1):312. doi:10.1186/S13018-021-02472-9
94. Zhang H, Xu C, Zhang T, Gao Z, Zhang T. Does percutaneous vertebroplasty or balloon kyphoplasty for osteoporotic vertebral compression fractures increase the incidence of new vertebral fractures? a meta-analysis. Pain Physician. 2017;20(1):E13–E28. doi:10.36076/ppj.2017.1.e13
95. Xiao H, Yang J, Feng X, et al. Comparing complications of vertebroplasty and kyphoplasty for treating osteoporotic vertebral compression fractures: a meta-analysis of the randomized and non-randomized controlled studies. Eur J Orthop Surg Traumatol. 2015;25(Suppl 1):77–85. doi:10.1007/S00590-014-1502-4
96. Becker S, Meissner J, Tuschel A, Chavanne A, Ogon M. Cement leakage into the posterior spinal canal during balloon kyphoplasty: a case report. J Orthop Surg (Hong Kong). 2007;15(2):222–225. doi:10.1177/230949900701500220
97. Hulme PA, Krebs J, Ferguson SJ, Berlemann U. Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine. 2006;31(17):1983–2001. doi:10.1097/01.BRS.0000229254.89952.6B
98. Patel AA, Vaccaro AR, Martyak GG, et al. Neurologic deficit following percutaneous vertebral stabilization. Spine. 2007;32(16):1728–1734. doi:10.1097/BRS.0B013E3180DC9C36
99. Choe DH, Marom EM, Ahrar K, Truong MT, Madewell JE. Pulmonary embolism of polymethyl methacrylate during percutaneous vertebroplasty and kyphoplasty. AJR Am J Roentgenol. 2004;183(4):1097–1102. doi:10.2214/AJR.183.4.1831097
100. Greene DL, Isaac R, Neuwirth M, Bitan FD. The eggshell technique for prevention of cement leakage during kyphoplasty. J Spinal Disord Tech. 2007;20(3):229–232. doi:10.1097/01.BSD.0000211276.76024.30
101. Krueger A, Bliemel C, Zettl R, Ruchholtz S. Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: a systematic review of the literature. Eur Spine J. 2009;18(9):1257–1265. doi:10.1007/S00586-009-1073-Y
102. Kao FC, Tu YK, Lai PL, Yu SW, Yen CY, Chou MC. Inferior vena cava syndrome following percutaneous vertebroplasty with polymethylmethacrylate. Spine (Phila Pa 1976). 2008;33:10. doi:10.1097/BRS.0B013E31816F6A10
103. Guarnieri G, Masala S, Muto M. Update of vertebral cementoplasty in porotic patients. Interv Neuroradiol. 2015;21(3):372–380. doi:10.1177/1591019915582364
104. Peh WCG, Gilula LA. Additional value of a modified method of intraosseous venography during percutaneous vertebroplasty. AJR Am J Roentgenol. 2003;180(1):87–91. doi:10.2214/AJR.180.1.1800087
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real World Clinical Utility of Neurophysiological Measurement Utilizing Closed-Loop Spinal Cord Stimulation in a Chronic Pain Population: The ECAP Study Protocol
Leitner A, Hanson E, Soliday N, Staats P, Levy R, Pope J, Kallewaard JW, Doleys D, Li S, Weisbein J, Amirdelfan K, Poree L
Journal of Pain Research 2023, 16:2497-2507
Published Date: 21 July 2023
Spinal Cord Stimulation for Intractable Visceral Pain Originating from the Pelvic and Abdominal Region: A Narrative Review on a Possible New Indication for Patients with Therapy-Resistant Pain
Bieze M, van Haaps AP, Kapural L, Li S, Ferguson K, de Vries R, Schatman ME, Mijatovic V, Kallewaard JW
Journal of Pain Research 2024, 17:691-736
Published Date: 19 February 2024
A Systematic Guideline by the ASPN Workgroup on the Evidence, Education, and Treatment Algorithm for Painful Diabetic Neuropathy: SWEET
Sayed D, Deer TR, Hagedorn JM, Sayed A, D'Souza RS, Lam CM, Khatri N, Hussaini Z, Pritzlaff SG, Abdullah NM, Tieppo Francio V, Falowski SM, Ibrahim YM, Malinowski MN, Budwany RR, Strand NH, Sochacki KM, Shah A, Dunn TM, Nasseri M, Lee DW, Kapural L, Bedder MD, Petersen EA, Amirdelfan K, Schatman ME, Grider JS
Journal of Pain Research 2024, 17:1461-1501
Published Date: 13 April 2024
Long-Term Reductions in Opioid Medication Use After Spinal Stimulation: A Claims Analysis Among Commercially-Insured Population
Yong RJ, Tran OV, McGovern AM, Patil PG, Gilligan CJ
Journal of Pain Research 2024, 17:1773-1784
Published Date: 17 May 2024
Spinal Cord Stimulation Explantation and Chronic Pain: A Systematic Review and Technology Recommendations
Wahezi SE, Yener U, Naeimi T, Lewis JB, Yerra S, Sgobba P, Ciftci HB, Vydyanathan A, Chiu E, Cherkalin D, Darji JY, Masterson R, Lee D, Jarusriwanna A, Palee S, Ortiz NR, Caparo M, Dayon E, Fontaine C, Bikson M, Schatman ME, Pritzlaff SG, Deer TR, Hunter CW
Journal of Pain Research 2025, 18:1327-1340
Published Date: 18 March 2025