")
Back to Journals » Journal of Pain Research » Volume 16
Real World Clinical Utility of Neurophysiological Measurement Utilizing Closed-Loop Spinal Cord Stimulation in a Chronic Pain Population: The ECAP Study Protocol
Authors Leitner A , Hanson E, Soliday N, Staats P, Levy R, Pope J, Kallewaard JW , Doleys D, Li S , Weisbein J , Amirdelfan K, Poree L
Received 10 March 2023
Accepted for publication 12 July 2023
Published 21 July 2023 Volume 2023:16 Pages 2497—2507
DOI https://doi.org/10.2147/JPR.S411927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Angela Leitner,1 Erin Hanson,1 Nicole Soliday,1 Peter Staats,2 Robert Levy,3 Jason Pope,4 Jan W Kallewaard,5,6 Daniel Doleys,7 Sean Li,2 Jacqueline Weisbein,8 Kasra Amirdelfan,9 Lawrence Poree10
1Saluda Medical Pty Ltd, Artarmon, New South Wales, Australia; 2National Spine and Pain Centers, Shrewsbury, NJ, USA; 3Departments of Neurosurgery and Clinical Research, Anesthesia Pain Care Consultants, Tamarac, FL, USA; 4Evolve Restorative Center, Santa Rosa, CA, USA; 5Department of Anaesthesiology and Pain Management, Rijnstate Hospital, Arnhem, the Netherlands; 6Department of Anesthesiology and Pain Medicine, Amsterdam University Medical Centre, Amsterdam, the Netherlands; 7Pain and Rehabilitation Institute, Birmingham, AL, USA; 8Napa Valley Orthopaedic Medical Group, Napa, CA, USA; 9Boomerang Healthcare, Walnut Creek, CA, USA; 10Department of Anesthesia and Perioperative Care, University of California at San Francisco, San Francisco, CA, USA
Correspondence: Angela Leitner, Saluda Medical, Ground Floor, 407 Pacific Hwy, Artarmon, NSW, 2064, Australia, Email [email protected]
Background: Spinal cord stimulation (SCS) is an established chronic pain treatment, but the effectiveness of traditional, open-loop paradigms has been plagued by variable sustainability in a real-world setting. A new approach, utilizing evoked compound action potential (ECAP) controlled closed-loop (CL) SCS, continuously monitors spinal cord activation and automatically adjusts the stimulation amplitude of every pulse, maintaining stimulation at the prescribed ECAP level through this continual feedback mechanism. Recent studies demonstrated the long-term safety and efficacy of ECAP-controlled CL-SCS. Here, we report the design of a prospective, multicenter, single-arm feasibility study to characterize clinical outcomes in a real-world chronic pain population utilizing ECAP-controlled CL-SCS. Objective neurophysiological measurements such as device performance and patient therapy compliance, will be analyzed against baseline biopsychosocial assessments, to explore the clinical utility of these objective physiologic biomarkers in patient phenotyping.
Methods: This study will enroll up to 300 subjects with chronic, intractable trunk and/or limb pain in up to 25 United States investigation sites. Subjects meeting eligibility criteria will undergo a trial procedure and a permanent implant following a successful trial. Neurophysiological measurements (measured in-clinic and continuously during home use) and clinical outcomes including pain, quality-of-life, psychological, emotional, and functional assessments will be collected at baseline, trial end, and up to 24-months post-implantation.
Discussion: Associations between objective neurophysiological data, clinical evaluation and patient-reported outcomes may have important clinical and scientific implications. They may provide novel insights about the chronic pain pathophysiology, its modulation during CL-SCS, and identification of pain phenotypes and/or mechanisms associated with treatment response during SCS trials and long-term therapy. Data from the ECAP study could lead to improvements in diagnosis, assessment, patient identification and management of chronic pain. It could also provide the foundation for development of a new SCS treatment approach customized by the patient’s pain phenotype, unique neurophysiology, and disease severity.
Keywords: chronic pain, closed-loop, evoked compound action potentials, spinal cord stimulation
Introduction
Chronic pain (CP) is a multi-symptomatic, heterogenous dynamic disease condition that is one of the top causes of disability worldwide,1 resulting in significant patient and healthcare system burden. The International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”.2 CP is described as “biopsychosocial” due to the dynamic interaction between biological, psychological, and social factors in this disease condition.2 A better understanding of mechanisms of pain and how to identify which are present in a particular patient is needed to select the best treatment options for each individual, especially for those experiencing multiple, overlapping mechanisms of pain. CP research continues to strive for more objective tools to phenotype these complex, interacting mechanisms.3
Spinal cord stimulation (SCS) is an established therapeutic approach for the management of CP. SCS involves the application of electrical stimuli to the spinal cord (SC) to activate fibers such as Aβ fibers that contribute to the inhibition of pain signaling in the dorsal horn of the SC.4 Unfortunately, there are many variables that complicate the optimal delivery of energy. For example, the delivered electrical impulse must travel through the cerebral spinal fluid (CSF) to reach the target SC fibers. This is complicated by the dynamic nature of the depth of the CSF layer, which varies constantly both across and within individuals, leading to variable therapeutic delivery of electricity. Standard approaches employed in conventional paresthesia or paresthesia-free SCS paradigms are open-loop (OL) in nature: a stimulus is delivered at a constant, fixed amplitude that does not adjust, even as the physiologic state of the patient changes. This results in fluctuations in the stimulus received by the target fibers and/or neurons and inconsistency in the therapeutic effect; the neural “dose” of therapeutic stimulation varies with each pulse.5,6 Moreover, in the OL approach, there is no identification or measurement of any objective physiologic biomarker for therapeutic activation of the SC; it relies solely on subjective feedback from the patient.
Advancements in the field have led to the ability to measure the evoked compound action potentials (ECAPs) that are generated by the target SC neurons in response to therapeutic stimulation. ECAPs represent a direct measurement of the SC fiber recruitment resulting from each SCS pulse.7,8 This has facilitated the development of ECAP-controlled, closed-loop (CL) SCS (CL-SCS), a method of stimulation that can be adjusted with each pulse to maintain a consistent degree of SC activation at the prescribed ECAP (Figure 1).5,6 In contrast to CL-SCS, traditional OL-SCS systems are blind to the physiologic dose of therapy actually being delivered to the SC.9 Without physiologic measurement, confirmation that therapy has been delivered to the intended target in the clinic during programming, or confirmation of successful, consistent delivery of treatment (ie, treatment adherence) outside the clinic is not possible. Thereby, objective evaluation and reproducibility of therapeutic efficacy is also not possible.6
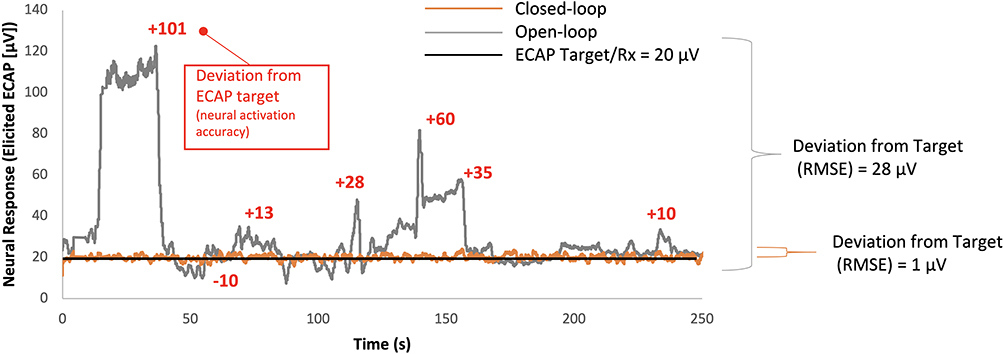 |
Figure 1 Neural activation and activation accuracy during open- and closed-loop SCS. Neural activation accuracy is the ability of the SCS device to adhere to the target neural response (ie, ECAP, prescription [Rx]) (black line at 20µV in this example). In open-loop (grey line), with a fixed amplitude of 1.8 µC/pulse, over the course of 250 seconds there was an average deviation from the target of 28µV, which included levels above and below the prescribed physiologic target, and produced an erratic neural activation (elicited ECAP). In closed-loop (Orange line), performing the same posture assessment, with the stimulation amplitude continuously modified with each pulse for a range of 1.1–2.1µC, there was an average deviation of 1µV, which produced a neural activation aligned with the target ECAP. |
While there have been many studies of SCS to manage patients with CP, other than two CL-SCS studies,6,10 all have employed OL-SCS approaches.11–17 That said, limitations exist to confound the true clinical efficacy results of OL-SCS because i) all OL-SCS parallel randomized controlled trials (RCTs) to date have been open-label, ii) results of blinded cross-over RCTs are inconsistent and iii) OL-SCS is not able to ensure that the physiologic therapeutic dose of stimulation is being delivered in a consistent and reliable manner. Consequently, results have been inconsistent, difficult to reproduce, and are unable to clearly differentiate the relative benefits of differing SCS therapies.18–21
The long-term safety, efficacy, and cost-effectiveness of CL-SCS have recently been demonstrated in studies which have produced Level 1 and 2 evidence.5,6,10,22,23 The EVOKE Study, a double-blind, randomized, multicenter, comparative study, demonstrated greater improvements in both the primary pain outcome measure and the secondary outcome measures, including physical and emotional functioning and health-related quality of life (HRQoL) in the CL-SCS group at the two-year follow-up period when compared to OL-SCS.6
The nature of the double-blinded design of the EVOKE study24 supports that the difference between the CL- and OL-SCS systems in achieving these endpoints was due to the consistent and reliable activation of the spinal cord.25 Therefore, it is now possible, with CL-SCS, to properly investigate the therapeutic benefits of SCS for CP and further elucidate the mechanisms of CP and its management. The ECAP study described in this protocol manuscript has been developed to gather information that will further advance our understanding of the clinical utility of ECAP-derived neurophysiological measurements in combination with clinical outcomes. Additionally, neurophysiologic recordings will be collected to understand the chronic pain pathophysiology and to characterize phenotypes potentially predictive of CL-SCS treatment response, while also aiming to characterize optimal patient selection in the real-world population of patients who are using ECAP-controlled SCS.
Evoke CL-SCS bases its device performance on measuring in vivo ECAPs evoked by epidural SCS as a biomarker for physiologic response, uses an individual’s objective SC response to personalize therapy, and provides high neural activation accuracy using an individualized CL-SCS ECAP amplitude target. The use of an objective biomarker for the therapy target (ECAPs) and evaluating its relationship with pain relief, as established in the previous studies,6,10 is a first in SCS history.
Materials and Methods
Objectives
The primary objective of this study is to evaluate neurophysiological measures and clinical outcomes of the Evoke ECAP-controlled CL-SCS System to treat trunk and/or limb pain in a real-world population. This study has been developed to further understand the clinical utility of these neurophysiological measurements.
Trial Design
The ECAP Study is a prospective, multicenter, single-arm feasibility study designed to evaluate neurophysiological measures and clinical outcomes with CL-SCS to treat patients with chronic pain of the trunk and/or limbs.
Subjects who provide informed consent and meet the study eligibility criteria will undergo a trial procedure and be enrolled. Following the trial phase, subjects may receive a permanent implant and be followed up at 1-, 3-, 6-, 12-, 18-, and 24-months after the permanent implant (Figure 2).
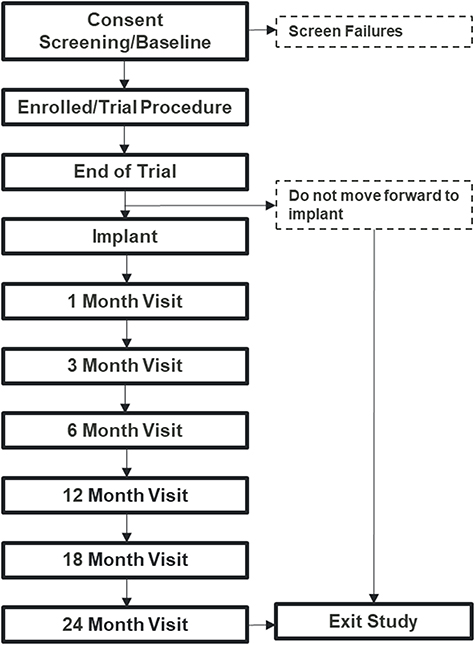 |
Figure 2 ECAP Study Design. |
Ethics
The study will be conducted in accordance with the United States Food and Drug Administration (FDA) regulatory requirements, good clinical practice (GCP, per ISO 14155), Institutional Review Board (IRB) approval, and the Declaration of Helsinki guided ethical principles. The study is registered with ClinicalTrials.gov (NCT04319887).
Patient Selection
The study will recruit patients with chronic intractable pain in the trunk and/or limbs. A subject must meet all the inclusion criteria and none of the exclusion criteria to be eligible for the study (Table 1). The study will enroll up to 300 subjects from a maximum of 25 US clinical sites. Patients who are identified will undergo authorization for SCS through their personal insurance, for both the trial, and if successful, the permanent therapy.
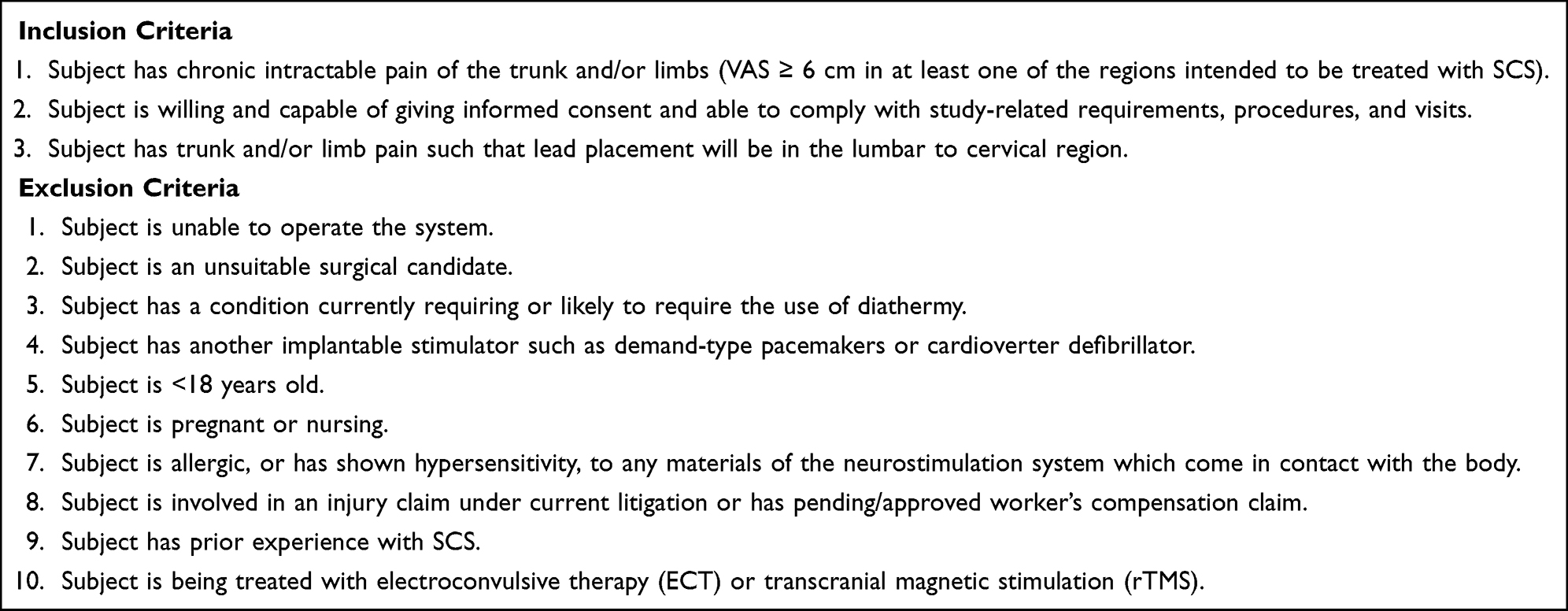 |
Table 1 ECAP Study Inclusion and Exclusion Criteria |
Interventions
After insurance authorization, subjects will first undergo a temporary trial stimulation phase during which an external stimulator (Evoke Trial System, Saluda Medical, Sydney, Australia) will be connected to one or two percutaneous Evoke leads (12-contact leads, all capable of stimulation and ECAP measurement) placed in the dorsal epidural space of the spinal canal. As a real-world, pragmatic study, the duration of the temporary trial phase may vary by physician, clinic, region and insurance policy, and can range from hours up to 30 days. Subjects who have a successful temporary trial, as determined by the patient and corroborated by the investigator, will be implanted with a permanent implantable pulse generator (IPG; Evoke® System, Saluda Medical, Sydney, Australia) at a later date. Standard clinical practice guidelines, in accordance with the manufacturer’s instructions for use (IFU) will be followed for the trial and permanent implant procedures, at the investigator’s discretion.
Device programming will initially occur following the trial and implant procedures, performed by sponsor representatives in accordance with the IFU, and subsequent adjustments can be made throughout the course of the study as needed to optimize therapy. The system is designed to operate in either ECAP-controlled, CL-stimulation mode, or OL-stimulation (fixed-output) mode equivalent to other commercially available SCS systems.5 ECAPs may be measured and recorded in either stimulation mode to monitor the SC neural response to stimulation. In OL-SCS, ECAPs can assist in determining ideal stimulation settings but are not used to produce a real-time physiological CL system. In CL-SCS mode, the feedback mechanism minimizes the difference between the measured ECAP amplitude and the ECAP amplitude target (set by the clinician and adjusted by the patient using the patient handheld programmer) by automatically adjusting the stimulation current for every stimulus. In doing so, it maintains SC activation at or near the target level.
Assessments and Objective Measurements
Assessments will be performed per the visit schedule outlined in Table 2. In alignment with IMMPACT recommendations,18 data collected in this study will be used to interrogate and analyze the underlying neurophysiological mechanisms of chronic pain with the goal of furthering a mechanism-based treatment approach to improve the efficacy of neuromodulation therapies. Objective data on programming parameters, neural activation, and neurophysiological properties will be collected along with clinician and patient-reported pathophysiology and outcome measures including pain, quality of life, psychological, emotional and functional assessments.
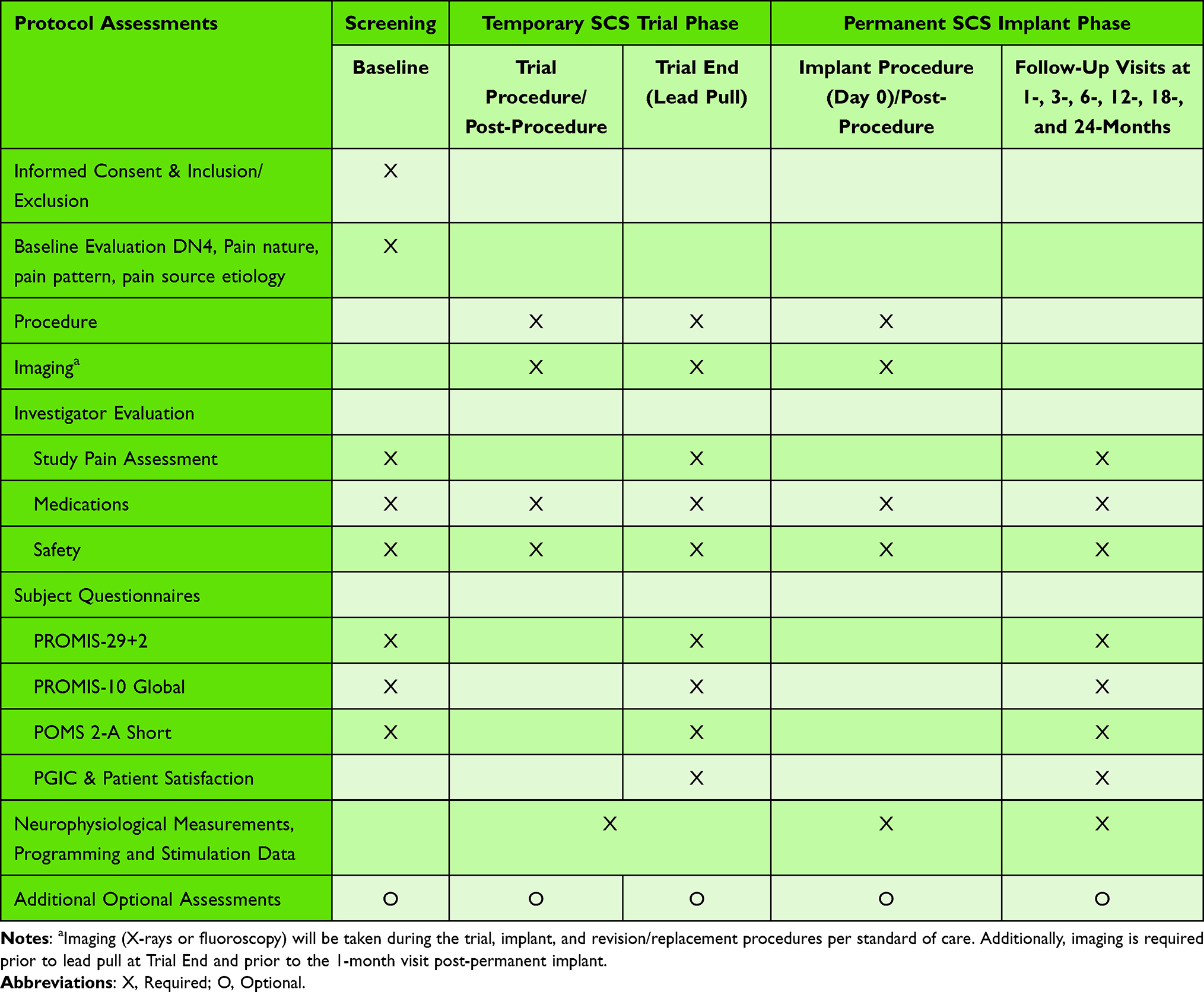 |
Table 2 Visit Schedule |
Baseline Assessment
Subjects who provide informed consent for study participation will complete the study-specific baseline assessments. This includes determination of subject study eligibility using the inclusion and exclusion criteria, demographics, medical history, and physical examination. The study pain assessment includes a body map to assess a subject’s pain locations targeted for SCS treatment, visual analog scale(s) [VAS] to record pain intensity for each region shaded on the body map, sleep, and pain quality and nature. In addition, pain etiology and pathophysiology and the DN4 are included at baseline. These will be completed by an investigator with the subject and validated patient report outcome assessments will be completed by the subject (PROMIS-29+2, PROMIS-10 Global, POMS 2-A Short; see below) as part of the baseline evaluation.
Validated Patient Reported Outcomes
PROMIS-29+2
The PROMIS-29+2 consists of the PROMIS-29 profile (v2.1) and two PROMIS Cognitive Function Abilities items. The PROMIS-29 is a 29-item profile instrument that assesses eight universal non-disease-specific domains (not disease-specific): Physical Function, Anxiety, Depression, Fatigue, Sleep Disturbance, Ability to Participate in Social Roles and Activities, Pain Interference, and Pain Intensity.26 It evaluates physical, mental, and social health and can be used both with the general population and with individuals living with chronic pain. Crosswalks between PROMIS and other legacy measures have also been developed so that the PROMIS scores can be cross-walked and compared to other common outcome variables.27,28 The addition of the two items from the PROMIS Cognitive Function Abilities, for a total of 31 questions, allows for incorporation of the PROMIS Preference Scoring System (PROPr), which is a generic societal, preference-based summary score (also called a health utility score). The PROPr is measured on scale where 0 is the utility of being dead and 1 the utility of “full health”. The lowest possible score is –0.022 (for a state viewed as worse than dead), and the highest possible score is 1.
PROMIS-10 Global
The PROMIS Global Health measure will be collected to evaluate overall physical and mental health.29 It includes 10 items: four items that reflect different aspects of physical health (eg, fatigue, physical function, pain), and four items that reflect different aspects of mental health (eg, mood, cognition, social activities/role). Links have also been developed between this instrument and other legacy measures, including EQ-5D.
Profile of Mood States 2nd Edition – Adult Short (POMS 2-A Short)
The POMS 2-A Short is a 35 item, 5-point Likert scale that measures mood states overall (Total Mood Disturbance) as well as for six mood clusters: Tension-Anxiety, Depression-Dejection, Anger-Hostility, Vigor-Activity, Fatigue-Inertia, and Confusion-Bewilderment.30
Patient Global Impression of Change (PGIC) and Patient Satisfaction
Patient Global Impression of Change (PGIC) is a single-item measure of global improvement with treatment.31 The subject will be presented with a 7-point rating scale ranging from “very much improved” to “very much worse”. Subject recommendation of and satisfaction with the stimulation therapy and study pain relief will also be collected. The 5 recommendation options utilized for this study range from “strongly recommend” to “definitely not recommend”, and the 5 satisfaction options range from “very satisfied” to “very unsatisfied”.
Douleur Neuropathique 4 (DN4)
DN4 is a validated clinical screening tool to indicate the presence of neuropathic pain in the index painful area.32
Neurophysiological Measurements, Programming and Stimulation Data
Individual variability in neurophysiological properties is expected due to patient differences in pathophysiological characteristics, neuronal sensitivity to stimulation, and lead location. Neural health can be monitored based on fiber properties to potentially provide insight into disease, injury, effects of medication and neural excitability over time.33
Objective neurophysiological measurements, as well as program parameter data (eg, frequency, pulse width, stimulation amplitude) and stimulation characteristics will be collected. Measurements will be automatically recorded and collected on the device. Data collected both in clinic and outside the clinic will be analyzed to evaluate a subject’s neural signature as it relates to programming prescription and how patients utilize stimulation in the real-world setting.
Objective neurophysiological measurements include but are not limited to:
- ECAP waveform features (eg, ECAP amplitude, width, slope, and shape)
- Conduction velocity (ie, the speed at which an ECAP propagates along the spinal cord)
- Rheobase (ie, the minimum stimulus current needed for neural activation at an infinitely long pulse width)
- Chronaxie (ie, the minimum pulse width needed for neural activation at twice the rheobase)
- Sensitivity (slope of the dose–response; μV/μC per pulse)
- Dose–Response Curve (the neural responses (ECAP amplitude [μV]) measured from the dose–response curves from threshold to maximum, including at each stimulus intensity increase)
- Neural activation accuracy (the ability of the device to adhere to the prescribed neural response as compared to the elicited neural response, that is, device performance)
- Patient adherence (patient compliance to the prescription [eg, device utilization and the level of spinal cord activation during home use]).
Medications
All medications being taken by the subject at baseline will be recorded for the study, as will any changes to these medications or any new medications.
Safety Measurements
Adverse events (AEs), protocol noncompliance and device deficiencies will be assessed from the point of consent and at all follow-up visits.
Additional Optional Assessments
To further evaluate neurophysiological measurements and their association with clinical outcomes, optional assessments to collect additional data have been added to the protocol and may be requested if subjects elect to participate. These assessments may occur anytime during the study. These optional assessments are in addition to the required protocol data collection and there are no foreseeable additional risks to the subject. If additional testing is deemed to have additional risks, the investigator will obtain a separate patient consent. Examples of the additional optional assessments include, but are not limited to, collecting data during medication changes, collecting additional data on pain signs and symptoms with stimulation on and/or off, evaluating various programming parameters or levels of therapy, and usability data if new or modified products become available.
Data and Quality Management
The quality of the data and its management will be ensured through study and device training and data management training as well as data monitoring. Investigators and their staff will be trained on device use, study protocol and procedures, as applicable. Study data will be collected in an FDA 21 CFR Part 11 compliant electronic data capture (EDC) system. Neurophysiological measurements and programming parameters are automatically collected on the device. The study will be monitored to ensure protection of human subjects, accuracy of the data, compliance with the study protocol and ethical and regulatory requirements.
Statistical Methods and Data Analysis
Sample Size
This study will enroll up to 300 subjects at up to 25 study sites. A sample size of 300 will provide a precision, as defined as the half-width of the two-sided 95% exact binomial confidence interval, of approximately ±6% or less for any event based on an incidence of 50%; an observed lower or higher incidence will produce a more precise (ie, narrower) interval.34
Analysis Populations
Analysis populations for the study include intention-to-treat (ITT) and permanent implant subset (PIS). The ITT group includes all enrolled study subjects. The PIS group includes all enrolled subjects who receive permanent implant. Subgroup analysis of various etiologies and/or pain locations may be performed such as predominant trunk or leg pain. Missing data will be classified appropriately, and sensitivity analyses may be performed to qualify the potential impact on the observed results. These include best- and worst-case scenario procedures, the imputation of missing data as failures, using the last value carried forward technique, and multiple imputation technique.
Statistical Analysis
There are no pre-planned formal statistical hypothesis tests for this study. As there are no formal pre-planned hypothesis tests, statistical analyses may be completed at any time.
Standard summary descriptive statistics will be used to summarize baseline and outcome data collected during the study. Categorical variables will be summarized via incidence and percent. Continuous variables will be summarized via mean, median, standard deviation, and range. Summary statistics will include 95% confidence intervals where appropriate. In the event planned parametric methods are found to be inappropriate based upon observed distributions of individual variables, appropriate non-parametric methods will be employed. Standard tests for significance will be employed, including one sample t-tests. Additional exploratory analyses may be performed, and this includes association analysis, linear and logistic regression analyses, repeated measures analyses, and generalized estimating equation (GEE) analyses as appropriate.
Questionnaire instruments will be analyzed consistent with their validated methodology and summary statistics will be presented. Findings of significance may be presented and include p-values and/or confidence intervals as appropriate. Improvement will be demonstrated if the mean change from baseline is found to be significantly different from zero (at an alpha of 0.05), in the direction that indicates improvement for each scale or questionnaire.
An independent adjudication committee will be responsible for the review, evaluation, categorization, and adjudication of all AEs that occur during the clinical study. AEs will be reported based on this adjudication. AEs will be summarized by seriousness, severity, and relatedness to the procedure, device, and/or stimulation.
ECAP Steering Committee
Given the open inclusion/exclusion criteria and real-world population study design, an independent steering committee, including pain specialists and a clinical psychologist, was formed with the following purposes:
- Review and categorization of the clinical and psychological aspects of patient selection.
- Application of consistent definitions for categorization of patient phenotypes such as neuropathic, nociceptive or nociplastic pain mechanisms.
- Review of patient neurophysiological data including ECAPs and their derivatives, patient compliance and SCS outcomes at both the temporary trial and long-term permanent implant phase to further our understanding of how to merge objective and subjective data to improve patient selection for SCS.
Discussion
The long-term safety, pain relief superiority, and cost-effectiveness of ECAP-controlled CL-SCS have previously been demonstrated in studies providing both Level 1 and 2 evidence.5,6,10,22,23 The CL-SCS device to be used in this study is the only SCS device that can provide i) physiologic real-time measurement, ii) automatic adjustment of stimulation current for every stimulus, and iii) measurement capability to evaluate in-vivo if the electrical stimulation has been delivered to the intended target. Rigorous scientific exploration of these neurophysiologic measurements is currently underway.
SCS has been used to manage CP for many years, but to date, the traditional paresthesia or paresthesia-free OL-SCS approaches do not have a mechanism for measuring neural response feedback or determining whether a therapeutic dose of stimulation has reached the target neurons or nerve fibers. As a result, studies of OL-SCS are not able to determine the physiologic dose that produces the clinical effect. Furthermore, as OL-SCS systems do not identify and measure the response from their intended neural target, the reliability and reproducibility of results are undermined by lack of data on the actual therapy delivered. Therefore, despite the promise of SCS to manage chronic pain, there remain fundamental unknowns about the treatment compared to the foundational, pharmacological and pharmacokinetic research that is performed for drug-based therapeutics.35 Phase 1 drug studies typically evaluate the biodistribution of the compound and the dose–response relationship, but equivalent investigations of electrical stimulation (sometimes referred to as electroceuticals) have not been technologically feasible.24 In contrast to conventional medication, for which the dose is determined by therapeutic plasma concentration and patient characteristics such as age or weight, the amount of charge delivered in OL-SCS has not been guided by any objective measurement. This is particularly relevant due to the dynamic nature of the CSF and epidural space.36 For SCS, optimal-dose selection criteria would include consideration of neuroanatomic features, such as the thickness of the dorsal CSF layer36 or the responsiveness of the target fibers to stimulation. CL-SCS enables delivery of a prescribed physiologic therapeutic dose of stimulation in a consistent and reliable manner based on the individual’s neural response. While the clinical studies of ECAP-controlled CL-SCS have demonstrated the safety and efficacy of its use in the treatment of chronic back and leg pain, the unique ability to measure neurophysiological data presents an opportunity to overcome the limitations of traditional OL-SCS and advance the scientific field of pain management.
In alignment with IMMPACT recommendations,18 data collected in this study will be used to elucidate the neurophysiological mechanisms that underly chronic pain, with the goal of advancing mechanism- and evidence-based, precision medicine using SCS. The ECAP Study is designed to learn more about the important physiological relationships between objective neurophysiological data obtained via the Evoke System and patient-reported measures. These relationships could have important clinical and scientific utility and may lead to improvements in diagnosis, assessment, and treatment of chronic pain including more effective neuromodulation therapies. Additionally, it will also provide novel clinical and scientific insights on phenotyping patient characteristics and predicting SCS trial and treatment response.
Funding
This study was supported by Saluda Medical Pty Ltd., Artarmon, New South Wales, Australia.
Disclosure
AL, EH and NS are employees of Saluda Medical. PS has received consultancy fees from Medtronic, Saluda Medical, Nalu, and Biotronic and has stock options from Saluda Medical and Nalu. He also reports grants from National Spine. RL is an uncompensated consultant for Biotronik, Nalu, Saluda Medical, and Mainstay Medical and has stock options from Nalu and Saluda Medical obtained before 2019, not exercisable through the duration of his term as International Neuromodulation Society President and Editor-in-Chief of the journal, Neuromodulation: Technology at the Neural Interface. JP serves as a consultant for Abbott, Medtronic, Saluda Medical, Flowonix, SpineThera, Vertos, Vertiflex, SPR Therapeutics, Tersera, Aurora, Spark, Ethos, Biotronik, Mainstay, WISE, Boston Scientific, and Thermaquil; has received grant and research support from: Abbott, Flowonix, Saluda Medical, Aurora, Painteq, Ethos, Muse, Boston Scientific, SPR Therapeutics, Mainstay, Vertos, AIS, and Thermaquil; and is a shareholder of Vertos, SPR Therapeutics, Painteq, Aurora, Spark, Celeri Health, Neural Integrative Solutions, Pacific Research Institute, Thermaquil, and Anesthetic Gas Reclamation. He also reports DRG neuromonitoring patent issued to Neural Integrative Solutions. JK is on the advisory board for Saluda Medical, Boston Scientific, Nevro, Abbott and Medtronic. DD reports consultant fees from Saluda. SL is a consultant for Abbott, Avanos, Averitas Pharm, Biotronik, Boston Scientific, Nalu Medical, Nevro, PainTeq, PRIA Health, Saluda Medical, SPR Therapeutics, Vertos Medical, has equity in Nalu Medical and National Spine and Pain Centers. He has received department research funding from Avanos, Biotronik, Boston Scientific, Ethos Lab, Neuralace, SGX Medical, Nalu Medical, PainTeq, Saluda Medical and SPR Therapeutics. He also reports speaker bureau with Scilex Parma. JW is a consultant for SI Bone, Saluda Medical, Abbott, Medtronic and Biotronik. KA is an investigator and a consultant for Boston Scientific, Nevro, Medtronic, Nalu, Presidio and Biotronik. LP is a consultant for Medtronic, Saluda Medical and Nalu. The authors report no other conflicts of interest in this work.
References
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
3. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
4. Linderoth B, Foreman RD. Conventional and novel spinal stimulation algorithms: hypothetical mechanisms of action and comments on outcomes. Neuromodulation. 2017;20(6):525–533. doi:10.1111/ner.12624
5. Mekhail N, Levy RM, Deer TR, et al. Long-term safety and efficacy of closed-loop spinal cord stimulation to treat chronic back and leg pain (Evoke): a double-blind, randomised, controlled trial. Lancet Neurol. 2020;19(2):123–134. doi:10.1016/S1474-4422(19)30414-4
6. Mekhail N, Levy RM, Deer TR, et al. Durability of clinical and quality-of-life outcomes of closed-loop spinal cord stimulation for chronic back and leg pain: a secondary analysis of the evoke randomized clinical trial. JAMA Neurol. 2022;3(79):251–260. doi:10.1001/jamaneurol.2021.4998
7. Parker J, Karantonis D, Single P. Hypothesis for the mechanism of action of ECAP-controlled closed-loop systems for spinal cord stimulation. Healthc Technol Lett. 2020;7(3):76–80. doi:10.1049/htl.2019.0110
8. Parker JL, Karantonis DM, Single PS, Obradovic M, Cousins MJ. Compound action potentials recorded in the human spinal cord during neurostimulation for pain relief. Pain. 2012;153(3):593–601. doi:10.1016/j.pain.2011.11.023
9. Chakravarthy K, Reddy R, Al-Kaisy A, Yearwood T, Grider J. A call to action toward optimizing the electrical dose received by neural targets in spinal cord stimulation therapy for neuropathic pain. J Pain Res. 2021;14:2767–2776. doi:10.2147/JPR.S323372
10. Brooker C, Russo M, Cousins MJ, et al. ECAP-controlled closed-loop spinal cord stimulation efficacy and opioid reduction over 24-months: final results of the prospective, multicenter, open-label Avalon study. Pain Pract. 2021;21(6):680–691. doi:10.1111/papr.13008
11. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1–2):179–188. doi:10.1016/j.pain.2007.07.028
12. de Vos CC, Meier K, Zaalberg PB, et al. Spinal cord stimulation in patients with painful diabetic neuropathy: a multicentre randomized clinical trial. Pain. 2014;155(11):
13. Slangen R, Schaper NC, Faber CG, et al. Spinal cord stimulation and pain relief in painful diabetic peripheral neuropathy: a prospective two-center randomized controlled trial. Diabetes Care. 2014;37(11):3016–3024. doi:10.2337/dc14-0684
14. Kemler MA, Barendse GA, van Kleef M, et al. Spinal cord stimulation in patients with chronic reflex sympathetic dystrophy. N Engl J Med. 2000;343(9):618–624. doi:10.1056/NEJM200008313430904
15. Kapural L, Yu C, Doust MW, et al. Novel 10-kHz High-frequency therapy (HF10 Therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA-RCT randomized controlled trial. Anesthesiology. 2015;123(4):851–860. doi:10.1097/ALN.0000000000000774
16. Petersen EA, Stauss TG, Scowcroft JA, et al. Effect of high-frequency (10-kHz) spinal cord stimulation in patients with painful diabetic neuropathy: a randomized clinical trial. JAMA Neurol. 2021;78(6):687–698. doi:10.1001/jamaneurol.2021.0538
17. Eldabe S, Duarte RV, Gulve A, et al. Does a screening trial for spinal cord stimulation in patients with chronic pain of neuropathic origin have clinical utility and cost-effectiveness (TRIAL-STIM)? A randomised controlled trial. Pain. 2020;161(12):2820–2829. doi:10.1097/j.pain.0000000000001977
18. Katz N, Dworkin RH, North R, et al. Research design considerations for randomized controlled trials of spinal cord stimulation for pain: initiative on Methods, Measurement, and Pain Assessment in Clinical Trials/Institute of Neuromodulation/International Neuromodulation Society recommendations. Pain. 2021;162(7):1935–1956. doi:10.1097/j.pain.0000000000002204
19. Caylor J, Reddy R, Yin S, et al. Spinal cord stimulation in chronic pain: evidence and theory for mechanisms of action. Bioelectron Med. 2019;5:12. doi:10.1186/s42234-019-0023-1
20. Duarte RV, Nevitt S, McNicol E, et al. Systematic review and meta-analysis of placebo/sham controlled randomised trials of spinal cord stimulation for neuropathic pain. Pain. 2020;161(1):24–35. doi:10.1097/j.pain.0000000000001689
21. O’Connell NE, Ferraro MC, Gibson W, et al. Implanted spinal neuromodulation interventions for chronic pain in adults. Cochrane Database Syst Rev. 2021;12(12):Cd013756. doi:10.1002/14651858.CD013756.pub2
22. Russo M, Brooker C, Cousins MJ, et al. Sustained long-term outcomes with closed-loop spinal cord stimulation: 12-month results of the prospective, multicenter, open-label Avalon study. Neurosurgery. 2020;87(4):E485–e495. doi:10.1093/neuros/nyaa003
23. Duarte RV, Bentley A, Soliday N, et al. Cost-utility analysis of Evoke closed-loop spinal cord stimulation for chronic back and leg pain. Clin J Pain. 2023 doi:10.1097/AJP.0000000000001146. In press 2023.
24. Levy R, Deer TR, Poree L, et al. Multicenter, randomized, double-blind study protocol using human spinal cord recording comparing safety, efficacy, and neurophysiological responses between patients being treated with evoked compound action potential-controlled closed-loop spinal cord stimulation or open-loop spinal cord stimulation (the Evoke study). Neuromodulation. 2019;22(3):317–326. doi:10.1111/ner.12932
25. Food and Drug Administration. Summary of Safety and Effectiveness Data (SSED): Saluda Medical Evoke Spinal Cord Stimulation (SCS) System; 2022. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf19/P190002B.pdf.
26. Hays RD, Spritzer KL, Schalet BD, Cella D. PROMIS(®)-29 v2.0 profile physical and mental health summary scores. Qual Life Res. 2018;27(7):1885–1891. doi:10.1007/s11136-018-1842-3
27. Pope JE, Fishman M, Chakravarthy K, et al. A retrospective, multicenter, quantitative analysis of patients’ baseline pain quality (PROMIS-29) entering into pain and spine practices in the United States (ALIGN). Pain Ther. 2021;10(1):539–550. doi:10.1007/s40122-021-00238-z
28. Pope JE, Fishman MA, Gunn JA, Cotten BM, Hill MM, Deer TR. Cross-validation of the foundation pain index with PROMIS-29 in chronic pain patients. J Pain Res. 2021;14:2677–2685. doi:10.2147/JPR.S314021
29. Hays RD, Bjorner JB, Revicki DA, Spritzer KL, Cella D. Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Qual Life Res. 2009;18(7):873–880. doi:10.1007/s11136-009-9496-9
30. Heuchert J, McNair D. Profile of mood states. In: POMS 2.
31. Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
32. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1–2):29–36. doi:10.1016/j.pain.2004.12.010
33. Parker JL, Obradovic M, Hesam Shariati N, et al. Evoked compound action potentials reveal spinal cord dorsal column neuroanatomy. Neuromodulation. 2020;23(1):82–95. doi:10.1111/ner.12968
34. Fleiss JL, Levin B, Paik MC. Statistical Methods for Rates and Proportions. Hoboken, New Jersey: John Wiley & Sons, Inc.; 2003.
35. Knotkova H, Hamani C, Sivanesan E, et al. Neuromodulation for chronic pain. Lancet. 2021;397(10289):2111–2124. doi:10.1016/S0140-6736(21)00794-7
36. Holsheimer J, Wesselink WA. Effect of anode-cathode configuration on paresthesia coverage in spinal cord stimulation. Neurosurgery. 1997;41(3):654–659; discussion 659–660. doi:10.1097/00006123-199709000-00030
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.