Back to Journals » Risk Management and Healthcare Policy » Volume 19
Spatial Epidemiology of the Ischemic Heart Disease–Asthma Comorbidity: A Global Analysis of Burden Patterns, Risk Drivers, and a Composite Risk Index
Authors Fan S, Wang L, Zhang S, Wu X ![]()
Received 25 April 2026
Accepted for publication 19 June 2026
Published 23 June 2026 Volume 2026:19 619944
DOI https://doi.org/10.2147/RMHP.S619944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Sha Fan,1 Lu Wang,1 Shufen Zhang,2 Xiaojing Wu1
1Department of Respiratory Medicine, Heji Hospital Affiliated to Changzhi Medical College, Changzhi, Shanxi, 046000, People’s Republic of China; 2Department of Laboratory Medicine, Heji Hospital Affiliated to Changzhi Medical College, Changzhi, Shanxi, 046000, People’s Republic of China
Correspondence: Xiaojing Wu, Department of Respiratory Medicine, Heji Hospital Affiliated to Changzhi Medical College, No. 271, Taihang East Street, Luzhou District, Changzhi, Shanxi, 046000, People’s Republic of China, Email [email protected]
Background: Although ischemic heart disease (IHD) and asthma are major contributors to the global disease burden, the geographical distribution patterns of their comorbidity and its macro-level drivers remain unclear. This study aims to analyze the global spatial distribution of IHD-asthma comorbidity and to identify the key risk factors driving this comorbid pattern.
Methods: Based on a secondary analysis of the Global Burden of Disease Study 2021, this study categorized 204 countries and territories worldwide into three spatial patterns—namely “concordant type”, “IHD-dominant type”, and “asthma-dominant type”—using the quartile method of disability-adjusted life years (DALYs). A three-stage screening approach was employed to identify significant risk factors: random forest modeling combined with Shapley additive explanations was first used to rank and select candidate variables, followed by negative binomial regression analysis to confirm significant associations. Furthermore, population attributable fraction and a composite risk index were constructed to quantify cumulative exposure levels.
Results: Approximately one-quarter of countries worldwide exhibit a “concordant pattern” of disease burden levels, primarily located in Asia, Africa, and Oceania. Thirteen significant risk factors were identified, with deficiency in omega-6 polyunsaturated fatty acids and iron deficiency being common risk factors for both diseases. Overall, 43.083% of IHD DALYs and 28.963% of asthma DALYs were attributable to the combined exposure to their respective risk factors.
Conclusion: The global joint burden of IHD and asthma exhibits substantial spatial heterogeneity, with particularly severe challenges in socioeconomically resource-limited regions of Africa and Asia. Comprehensive strategies integrating nutritional interventions, environmental improvements, and metabolic risk control are crucial for mitigating the global burden of cardiopulmonary comorbidities.
Plain Language Summary: Why was the study done?
Ischemic heart disease and asthma are among the world’s most common chronic diseases. When people live with both conditions, they face unique health challenges. Yet researchers have not fully explored where this combination appears most often or what drives it.
What did the researchers do and find?
Our team used data from the Global Burden of Disease 2021 study to map how ischemic heart disease and asthma co-occur across 204 countries and territories. We combined spatial analysis, machine learning, and statistical models to identify geographic patterns and key risk factors.
We found that nearly one in four countries carries a high burden of both diseases simultaneously — a pattern we call “concordant”. These countries cluster mainly in Africa, Asia, and Oceania. We identified 13 significant risk factors. Two — low intake of omega-6 fats (a type of healthy dietary fat) and iron deficiency — increased the risk of both diseases. Others affected only one condition: kidney dysfunction raised ischemic heart disease risk, while household air pollution from solid fuels raised asthma risk. We also created a composite risk index to measure each country’s overall risk exposure, revealing that nations in Africa and Asia face the greatest cumulative risk.
What do these results mean?
These results show that ischemic heart disease and asthma should be treated as interconnected health problems. Strategies targeting their shared risk factors — such as improving nutrition and reducing indoor air pollution — could ease the burden of both diseases, especially in the hardest-hit regions.
Keywords: ischemic heart disease, asthma, comorbidity, risk factors, population attributable fraction
Introduction
Ischemic heart disease (IHD) is the leading cause of death and disability-adjusted life years (DALYs) worldwide, particularly in low- and middle-income countries.1,2 Epidemiological data indicates that IHD contributes to approximately 7 million deaths and 129 million DALYs annually, imposing a substantial socioeconomic burden.2 Its epidemiological patterns show significant global heterogeneity—meaning that the distribution, magnitude, and temporal trends of disease burden vary markedly across geographic regions, driven by differences in environmental exposures, healthcare infrastructure, population demographics, and risk factor profiles—with distinct trends in incidence and mortality across different countries and regions.3,4 Asthma, as a common chronic respiratory disease, also exhibits epidemiological variations by age, gender, and geography. With population aging, the prevalence of multiple chronic comorbidities among asthma patients has increased markedly.5 Growing epidemiological evidence suggests that asthma may be intrinsically linked to cardiovascular diseases and represents an independent risk factor for coronary heart disease, with a more pronounced risk observed particularly among female patients.6,7
From a mechanistic perspective, the co-occurrence of IHD and asthma may be underpinned by several shared biological pathways. Chronic systemic inflammation, characterized by elevated levels of C-reactive protein, interleukin-6, and tumor necrosis factor-α, is a well-established contributor to both atherosclerotic plaque development and airway hyperresponsiveness.8,9 Additionally, immune dysregulation, including imbalances in T-helper cell subsets and aberrant cytokine signaling, may further link airway inflammation to vascular endothelial dysfunction.10 Beyond these shared inflammatory mediators, emerging evidence highlights a more direct mechanistic bridge between allergic airway disease and cardiovascular pathology through the immunoglobulin E (IgE)–mast cell axis. IgE concentrations are significantly elevated in patients with ischemic heart disease, and the interaction between IgE and mast cells triggers the release of mediators—including cysteinyl-leukotrienes, histamine, and platelet-activating factor—that promote vascular permeability, platelet activation, and thrombosis.11–13 Mast cells that accumulate within atherosclerotic lesions can stimulate foam cell formation, plaque degradation, and the initiation of coagulation through proteolytic enzymes and cytokine release from their granules.12 Furthermore, uncontrolled eosinophilic asthma has been shown to promote a procoagulant state, further amplifying the thrombotic risk in these patients.12,14 These overlapping pathophysiological pathways suggest that upstream risk factors may simultaneously promote both diseases through convergent inflammatory and metabolic cascades.
When IHD and asthma coexist, the resulting comorbid condition poses distinct challenges to patient prognosis and healthcare systems. A nationwide cohort study of acute myocardial infarction patients revealed that more than half of the patients had one or more long-term comorbidities, including asthma, at the time of admission.15 Among hypertensive patients, comorbid asthma is significantly associated with increased risks of all-cause mortality and myocardial infarction.16 Moreover, patients with coronary heart disease who also have chronic obstructive pulmonary disease or asthma are less likely to receive coronary revascularization therapy.17 Therefore, a deeper understanding of the epidemiological patterns and determinants of the IHD–asthma comorbidity is essential for improving the integrated management of this high-risk population.
Current understanding of the risk factors for the IHD–asthma comorbidity remains at an early stage. Traditionally, the two diseases share several common risk factors, such as smoking and physical inactivity.18,19 However, the occurrence of comorbidity may be driven by a more complex network of risk factors, including environmental exposures, socioeconomic conditions, specific metabolic indicators, and systemic inflammatory states.20 Most previous studies have either focused on a single disease or examined comorbidity only at the individual patient level, lacking a macro public health perspective that systematically delineates the geographic landscape of the co-burden of these two diseases and its underlying drivers on a global scale. Geographic mapping of comorbidity patterns is of particular importance for health policy planning, as it enables the identification of high-burden regions where dual-disease interventions may yield the greatest public health returns, facilitates more efficient allocation of limited healthcare resources, and supports the development of region-specific prevention strategies tailored to local risk factor profiles rather than relying on one-size-fits-all approaches. Thus, this study aims, within the framework of the Global Burden of Disease Study (GBD), to employ spatial analytical methods to uncover the global geographic distribution pattern of the co-burden of ischemic heart disease and asthma. By categorizing countries into regions based on disease burden indicators for both conditions, and using a combined strategy of machine learning and negative binomial regression models to screen and identify significant risk factors associated with the comorbidity pattern from a wide range of candidate factors, we further developed a comprehensive risk index to quantify cumulative exposure levels, which provided an evidence-based macro-level perspective and decision-making basis for the prevention and control of this important comorbidity issue worldwide.
Methods
Data Sources
The GBD 2021 study framework integrates epidemiological data for 371 diseases and injuries and 88 risk factors, providing standardized estimates by age, sex, region, and year. Detailed modeling strategies and estimation procedures have been described in previous publications.21 Using the GBD 2021 database, this study obtained estimates of DALYs for IHD and asthma in 2021, as well as exposure estimates for the 68 most detailed risk factors, to analyze the global co-occurrence patterns of IHD and asthma and their associated risk factors.
Classification of IHD-Asthma Co-Occurrence Patterns
To characterize co-occurrence patterns and geographical heterogeneity, countries were classified based on the quartiles of DALYs for both IHD and asthma (low: <25th percentile; medium-low: 25th–50th percentile; medium-high: 50th–75th percentile; high: >75th percentile). Countries where both diseases fell within the same quartile interval were categorized as concordant regions; countries where the quartile of IHD was higher than that of asthma were designated as IHD-dominant; conversely, countries with a higher asthma quartile were classified as asthma-dominant. This approach divided the globe into three mutually exclusive regions, reflecting distinct patterns of co-burden of diseases.
Screening of Risk Factors and Feature Selection
This study employed a three-stage independent screening procedure to assess risk factors within a unified study framework.20 First, based on epidemiological plausibility and preliminary correlation analysis, risk factors unlikely to be associated with IHD and asthma were excluded. These included risks specific to minors and certain occupational exposures, reducing the candidate variables from 68 to 45. Second, a random forest model combined with Shapley additive explanations (SHAP) was used to rank variable importance. SHAP quantifies the contribution of each predictor to the model output and can handle complex non-linear and collinearity relationships.22 To balance model interpretability and explanatory breadth, the top 20 risk factors according to the SHAP ranking were retained for subsequent regression analysis. To assess the sensitivity of the feature selection procedure, the negative binomial regression analysis was repeated by retaining the top 15 and top 25 risk factors according to SHAP rankings, respectively.
Subsequently, these selected risk factors were incorporated into negative binomial regression models to estimate the association between exposure to the risk factors and disease DALYs, reporting relative risks (RRs) and their 95% confidence intervals (CIs). It should be noted that, given the ecological design of this study—where the unit of analysis is the country rather than the individual—the regression models were not adjusted for additional covariates. The primary purpose of these models is to quantify the population-level association between risk factor exposure and disease burden rather than to infer individual-level causal relationships. Finally, risk factors with statistically significant associations were retained and integrated to construct a composite risk index to summarize the overall exposure intensity. P-value < 0.05 was considered statistically significant.
Calculation of Population Attributable Fraction
For the identified risk factors, we calculated the population attributable fraction (PAF) using RR derived from negative binomial regression. PAF represents the proportion of outcome events that could theoretically be prevented if a given risk factor were eliminated, assuming a causal relationship exists. The detailed calculation method is described in previously published literature.23 Subsequently, we used PAF to estimate the burden of IHD and asthma attributable to each risk factor across different regions.
Ethics Statement
This study utilized data from the GBD 2021, a publicly and freely accessible database that contains no individually identifiable patient information. In accordance with the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, issued by the National Health Commission of the People’s Republic of China, specifically Article 32, Items 1 and 2, this study was reviewed and approved as exempt from ethical review and informed consent by the Ethics Review Committee of Heji Hospital Affiliated to Changzhi Medical College.
Results
Global Overview and Spatial Association of IHD and Asthma
Globally, the median age-standardized DALY rate (ASDR) for IHD (2105.26 per 100,000) is substantially higher than that for asthma (289.24 per 100,000) (Table S1). The comorbid patterns of the two diseases exhibit considerable spatial heterogeneity. Countries/territories showing a “concordant” pattern are primarily concentrated in Asia, Africa, and Oceania; “IHD-dominant” areas are mainly distributed across Eastern Europe, Asia (particularly Central Asia, East Asia, and the Middle East), and North Africa; whereas “asthma-dominant” areas are largely clustered in Africa, the Americas, and Europe (Figure 1A). In terms of the spatial distribution of the diseases, high ASDR for IHD is predominantly observed in Asia, Europe, Oceania, and Africa; in contrast, high ASDR for asthma is mainly distributed across Africa, Asia, and Oceania (Figure 1B and C). Spatial clustering analysis further indicates an association between the disease categories: countries with IHD ASDR in the lower quartile mostly have asthma ASDR in the lower quartile as well, while countries with IHD in the upper quartile tend to have asthma ASDR in the upper quartile (Figure 1D). Overall, among 204 countries, 24.51% (50) are classified as concordant, 33.33% (68) as IHD-dominant, and 42.16% (86) as asthma-dominant (Table S1).
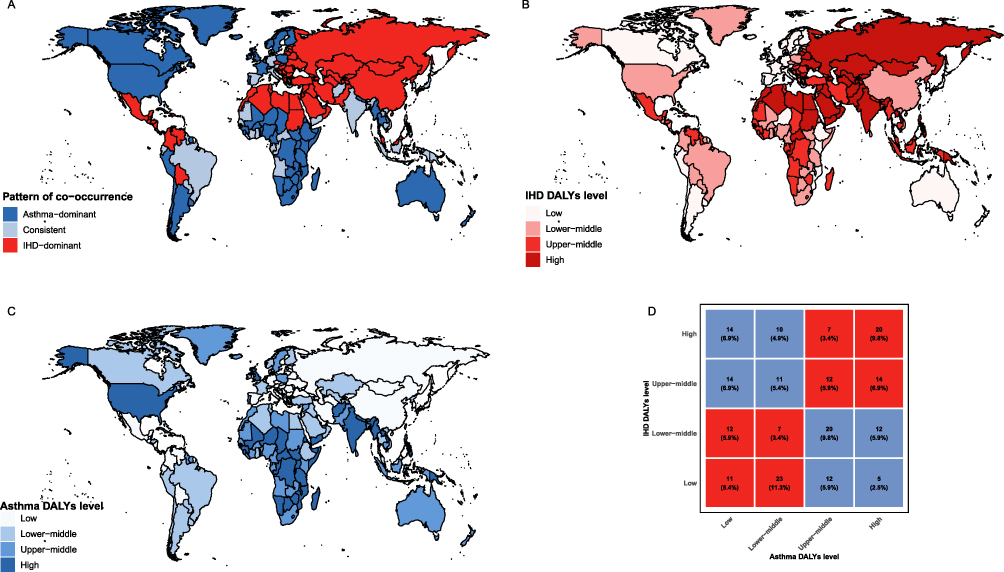 |
Figure 1 Global epidemiology and comorbidity of ischemic heart disease and asthma. (A and B) Characteristics of the co-occurrence of ischemic heart disease and asthma; (C) Global distribution of the disability-adjusted life years of ischemic heart disease and asthma; (D) Cross-tabulation of ischemic heart disease and asthma disability-adjusted life years levels in 2021. |
Screening of Risk Factors
We employed a random forest model combined with SHAP to analyze 45 candidate risk factors potentially influencing DALYs for IHD and asthma (Figure 2). Given that these risk factors are not specific to IHD or asthma, the present study focused on those demonstrating a positive effect. Overall, the variability of SHAP values for risk factors associated with asthma was significantly greater than that for IHD. Notably, for IHD, the SHAP values of risk factors ranked beyond the top 20 tended to stabilize. To ensure an adequate number of variables and a consistent screening criterion, we ultimately selected the top 20 variables exhibiting a positive effect on both IHD and asthma for in-depth analysis.
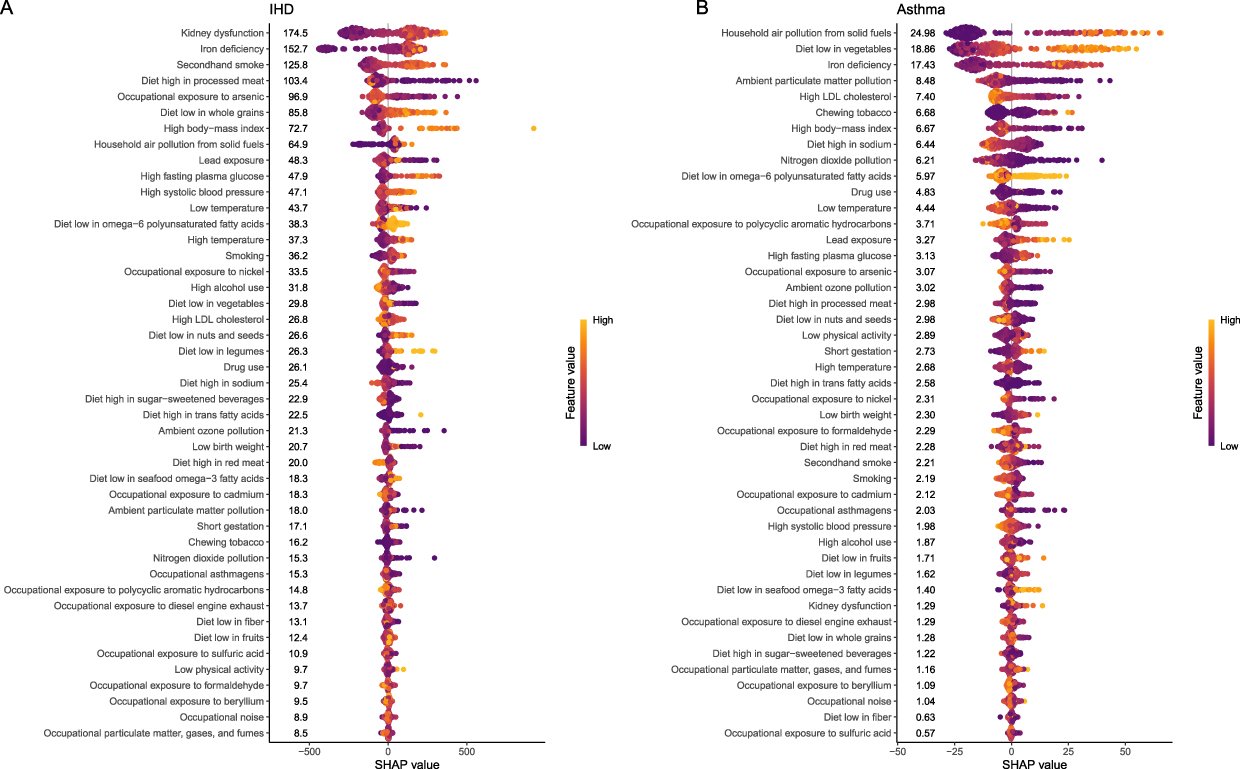 |
Figure 2 SHAP feature importance summary for ischemic heart disease (A) and asthma (B). The SHAP value on the horizontal axis reflects the impact of each factor on the outcome. Greater absolute SHAP values signify stronger influence on disease occurrence. |
Through this screening, 12 risk factors associated with IHD were identified: kidney dysfunction, iron deficiency, secondhand smoke, diet low in whole grains, high body-mass index, household air pollution from solid fuels, high fasting plasma glucose, high systolic blood pressure, diet low in omega-6 polyunsaturated fatty acids, high temperature, smoking, and diet low in nuts and seeds. Seven risk factors were associated with asthma: household air pollution from solid fuels, diet low in vegetables, iron deficiency, diet low in omega-6 polyunsaturated fatty acids, lead exposure, high fasting plasma glucose, and low physical activity.
Further analysis using a negative binomial regression model identified 13 risk factors with significant effects (Figure 3). These included 2 shared risk factors (diet low in omega-6 polyunsaturated fatty acids and iron deficiency) for IHD and asthma, 8 IHD-specific risk factors (diet low in nuts and seeds, diet low in whole grains, high body-mass index, high fasting plasma glucose, high systolic blood pressure, high temperature, kidney dysfunction and secondhand smoke), and 3 asthma-specific risk factors (diet low in vegetables, household air pollution from solid fuels and lead exposure). Among them, kidney dysfunction had the most significant effect on IHD (RR = 1.364, 95% CI: 1.257–1.482). The risk factor with a significant effect on asthma was diet low in vegetables (RR = 1.378, 95% CI: 1.309–1.450). To evaluate the sensitivity of feature selection to the threshold used, we repeated the negative binomial regression analysis by retaining the top 15 and top 25 SHAP-ranked risk factors, respectively. The results demonstrated that all 13 risk factors identified as significant in the primary analysis remained statistically significant across both alternative thresholds, confirming the robustness of the variable selection.
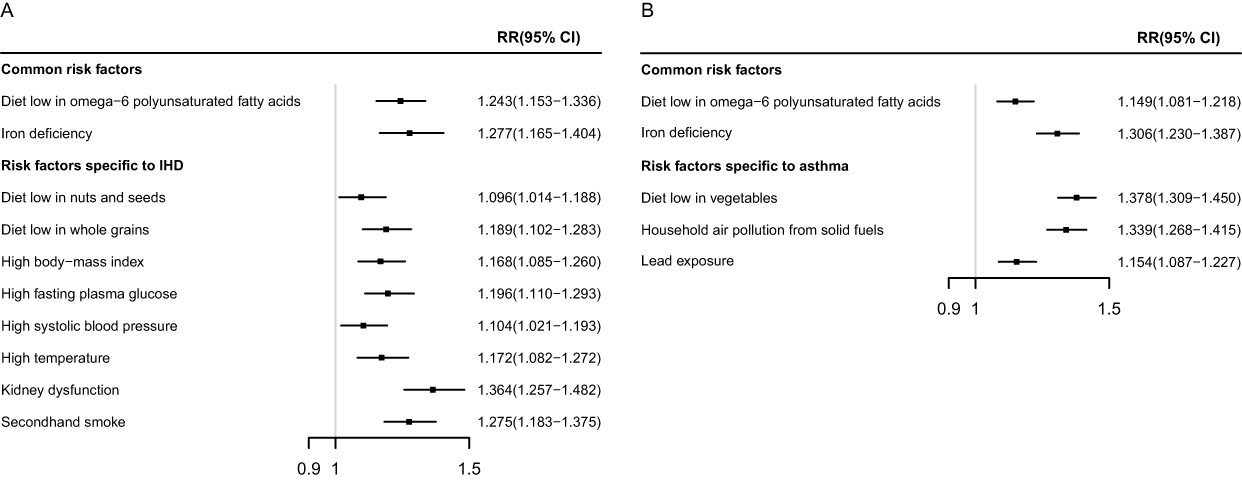 |
Figure 3 Risk factors for ischemic heart disease (A) and asthma (B) showing relative risks and 95% CIs. Relative risks (RR) of risk factors were derived from negative binomial regression models. |
Distribution Patterns of Risk Exposure
We adopted a percentile-based classification approach (<25th percentile, 25th–50th percentile, 50th–75th percentile, >75th percentile) to map the global distribution of the 13 significant risk factors identified (Figure 4). Overall, exposure levels of diet low in omega-6 polyunsaturated fatty acids and iron deficiency were relatively high in African and Asian countries; the IHD-specific risk factor—kidney dysfunction—was more prevalent in Latin America, Western Asia, and Southern Africa; while the asthma-specific risk factor—diet low in vegetables—also showed higher prevalence in Africa.
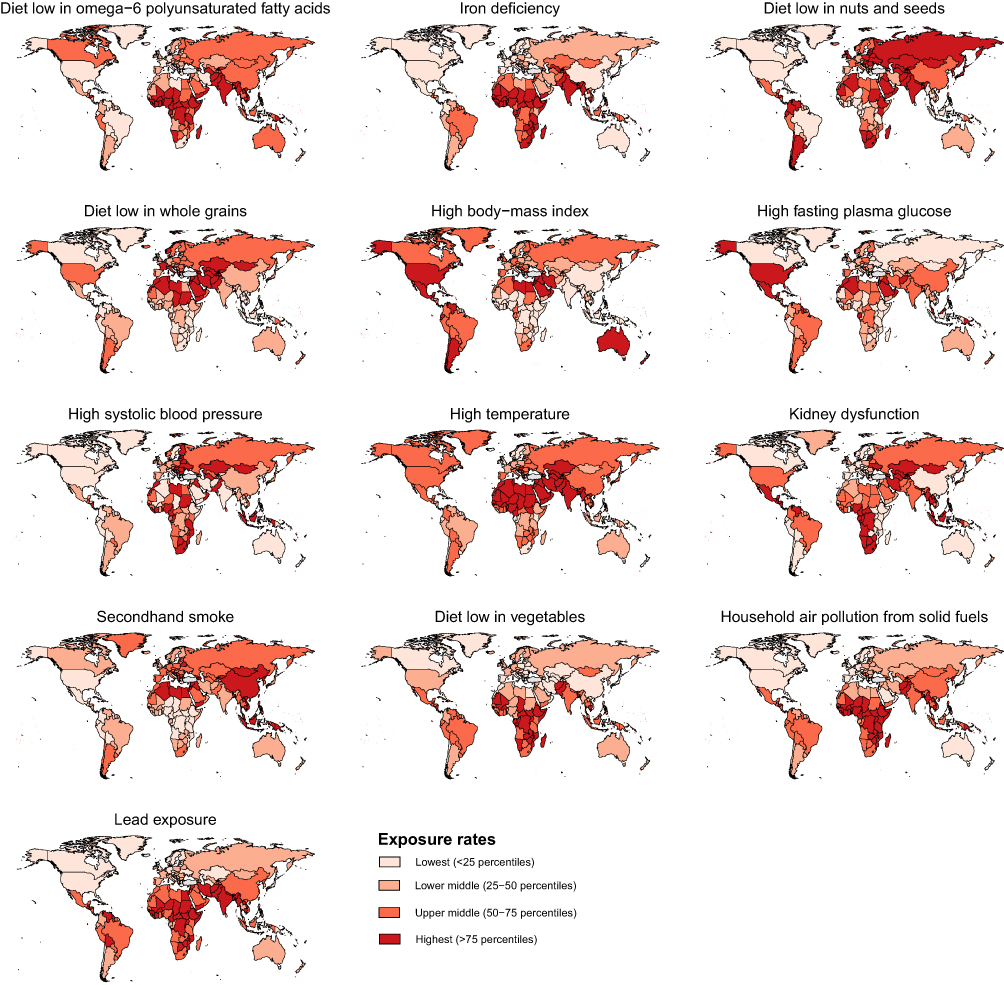 |
Figure 4 Global distribution of thirteen risk factor categories and their risk indices. |
Construction of a Composite Risk Index
We constructed a composite risk index based on the aforementioned 13 significant risk factors to quantify cumulative exposure; a higher index value indicates a greater risk of IHD and asthma. Countries with the highest composite risk are primarily located in Africa and Asia, which aligns with the distribution of concordant pattern regions and supports the cumulative risk framework (Figure 5A). The composite index exhibited wide variation across 204 countries, ranging from 7 to 33 (Figure 5B and Table S2). The most common index value was 20, observed in 25 countries. The lowest index value of 7 was recorded in Canada, Greenland, and the Netherlands, whereas Pakistan recorded the highest index value of 33. These findings collectively indicate significant global heterogeneity in the shared burden of IHD and asthma, and highlight the common and region-specific risk architecture underlying disease distribution.
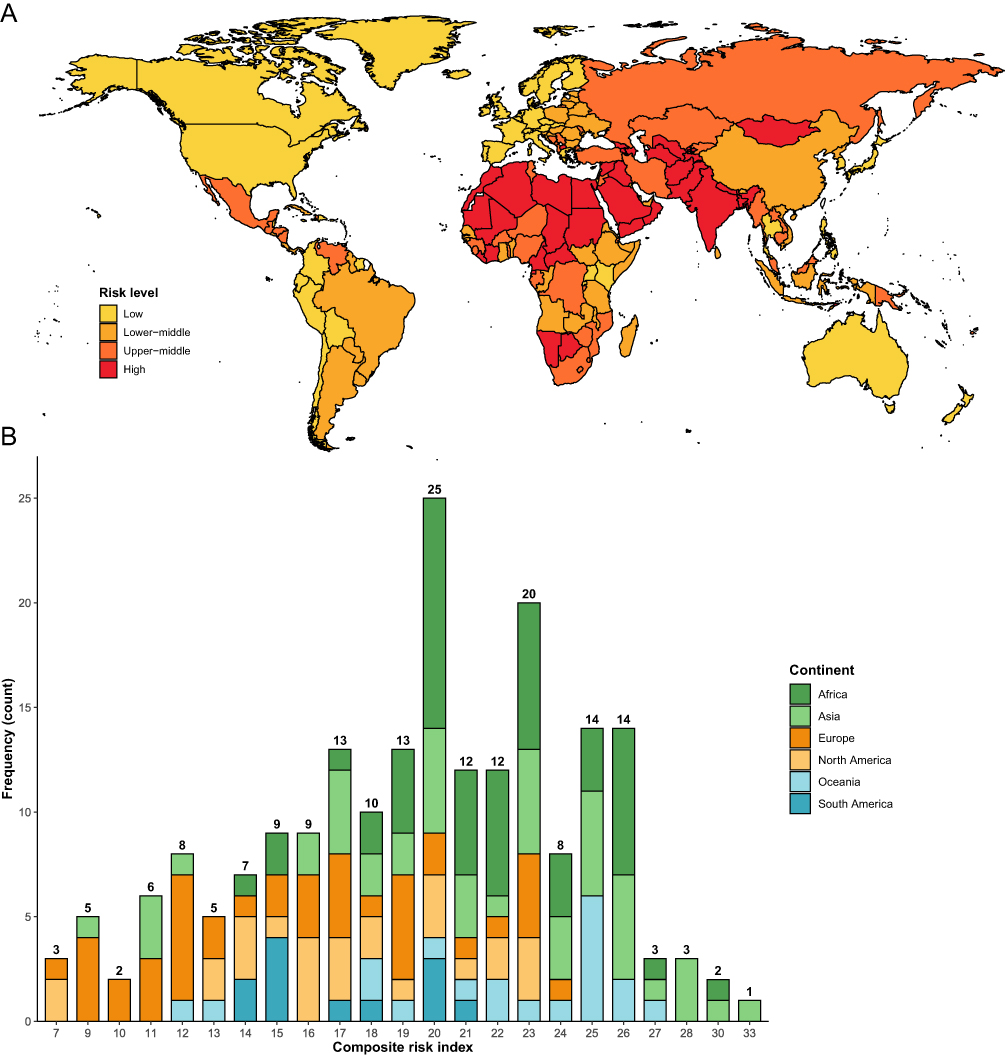 |
Figure 5 Global distribution and frequency characteristics of the composite risk index for thirteen risk factors. (A) Composite risk index; (B) Frequency distribution bar chart. |
PAF Analysis of Risk Factors
There are significant regional variations in the attributable proportions of risk factors for IHD and asthma worldwide (Figure 6). Overall, 43.083% of IHD DALYs were attributable to the combined exposure to its 10 risk factors, while 28.963% of asthma DALYs were attributable to the combined exposure to its 5 risk factors. Among these, a diet low in omega-6 polyunsaturated fatty acids contributed the most to the DALYs for both diseases, accounting for 15.526% of IHD DALYs and 10.128% of asthma DALYs (Table S3).
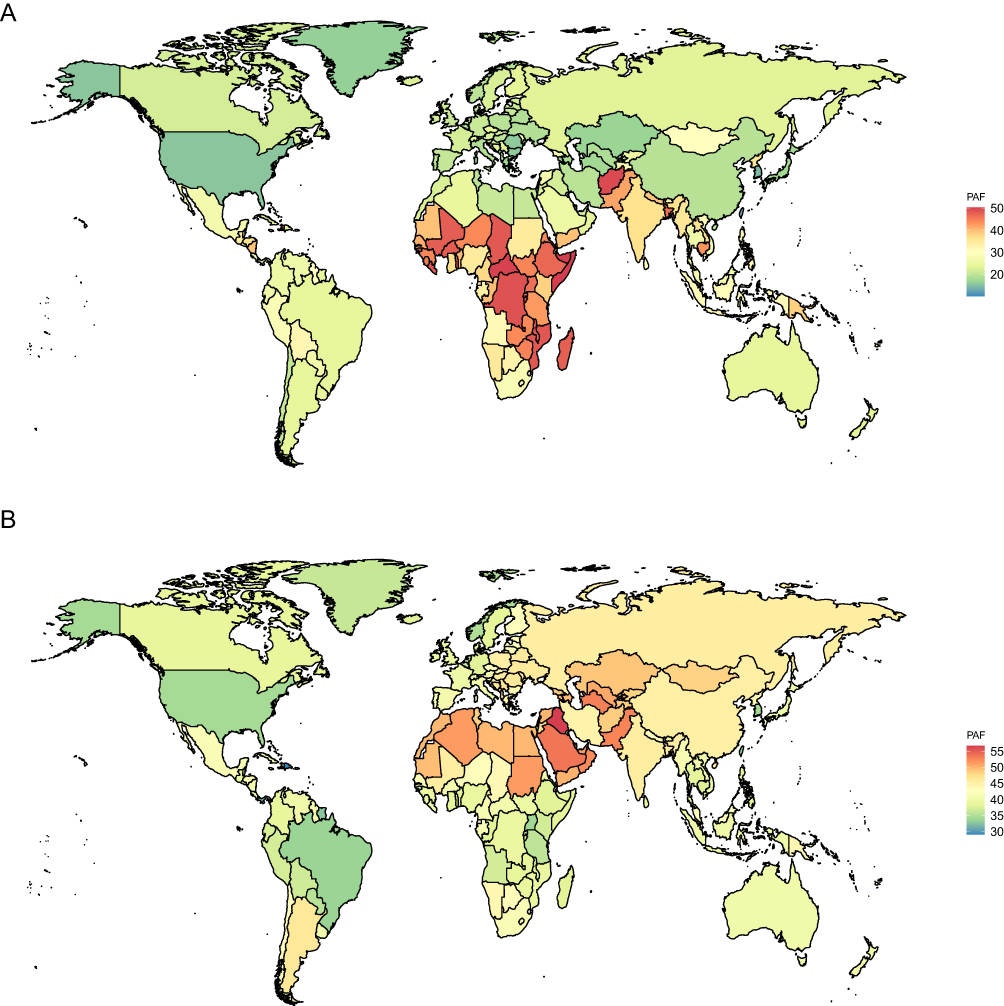 |
Figure 6 Population attributable fractions for asthma (A) and ischemic heart disease (B) of risk factors by locations. |
Discussion
This study presents, for the first time at a global scale, a systematic depiction of the shared patterns of disease burden between IHD and asthma, revealing significant spatial heterogeneity and identifying key exposure profiles—including both shared and specific risk factors—that drive this distribution pattern. The constructed comprehensive risk index further quantifies cumulative risk, highlighting the pronounced challenges faced by regions in Africa and Asia. These findings position the two traditionally distinct specialty diseases within a unified public health framework, providing important macro-epidemiological evidence for understanding their comorbid foundations and for developing regional prevention and control strategies.
Globally, the disease burden of IHD far exceeds that of asthma, a pattern consistent with long-term observations from the Global Burden of Disease studies.24,25 What is more revealing, however, are the three spatial patterns presented by the relative relationship of the burden levels of the two diseases. The findings indicate that nearly a quarter of countries worldwide exhibit a “concordant” pattern characterized by the coexistence of high burdens of IHD and asthma. These countries are not evenly distributed but are predominantly concentrated in regions with relatively limited socioeconomic and health system resources, such as Asia, Africa, and Oceania, which may reflect the dual burden of infectious and non-communicable diseases faced by these regions, as well as the compounding effects of environmental pollution and lifestyle changes amid rapid urbanization.26,27 In contrast, the IHD-dominant pattern observed in Eastern Europe and Central Asia may be closely associated with high smoking rates, high-salt diets, and population aging in these areas.28–31 Meanwhile, the asthma-dominant pattern seen in parts of Africa and the Americas may be more influenced by environmental allergens, indoor air pollution, and uneven distribution of healthcare resources.32–35
This study reveals that deficiencies in ω-6 polyunsaturated fatty acids and iron serve as common risk factors for IHD and asthma, suggesting that these two diseases may share certain pathophysiological mechanisms driven by nutritional and metabolic abnormalities. Notably, fatty acid–associated disease processes are increasingly recognized to involve epigenetic regulation. ω-6 polyunsaturated fatty acids, particularly arachidonic acid, have been shown to induce DNA hypermethylation at key metabolic regulators such as PPAR-α and sirtuin 1, thereby promoting pro-inflammatory and pro-atherogenic gene expression profiles.36 Conversely, ω-3 polyunsaturated fatty acids including EPA and DHA can attenuate inflammation partly through reducing IL-6 promoter methylation, inhibiting histone deacetylase activity, and suppressing histone acetyltransferase-mediated lipid metabolic gene expression.36,37 Furthermore, n-3 polyunsaturated fatty acids supplementation has been shown to induce differential DNA methylation at hundreds of CpG sites involved in inflammatory and immune responses, lipid metabolism, and cardiovascular signaling pathways.37,38 These epigenetic mechanisms may represent a shared upstream pathway through which polyunsaturated fatty acids imbalance simultaneously promotes atherosclerosis and airway inflammation, contributing to the observed comorbidity of IHD and asthma.39,40 Simultaneously, iron deficiency may exacerbate myocardial ischemia and airway hypersensitivity by inducing tissue hypoxia and immune dysfunction.41,42 These findings, taken together, deepen our mechanistic understanding of the critical role of nutritional and epigenetic disturbances in the comorbidity of these two conditions. However, this study further quantifies the association between specific nutritional indicators and disease risk through negative binomial regression, thereby deepening the understanding of the critical role of nutritional and metabolic disturbances in the comorbidity of these two conditions. Additionally, the observed regional differences in risk factors, particularly in Africa and Asia, suggest that environmental and genetic factors may modulate the epidemiological profiles of these nutritional deficiencies, echoing the complexity of gene-environment interactions in multimorbidity.43
Notably, the specific risk factor cluster for IHD is dominated by metabolic and dietary factors, which aligns closely with the pathophysiological understanding of ischemic heart disease as a core cardiometabolic disorder.44 The prominent risk ratio associated with kidney dysfunction further underscores the central role of the cardiorenal-metabolic axis within the chronic disease network.45 In contrast, the specific risk factors for asthma are significantly oriented toward environmental exposures. Household solid fuel pollution is identified as a key factor, consistent with findings from numerous studies conducted in developing regions such as Asia and Africa.46–49 The fine particulate matter and harmful gases released from solid fuel combustion can directly damage the airways, inducing and exacerbating asthma symptoms. Insufficient vegetable intake, as the factor with the highest risk, is supported by multiple observational studies.50–52 Vegetables are rich in antioxidant vitamins and phytochemicals, which may exert protective effects by reducing oxidative stress and modulating immune function.53 The association between lead exposure and asthma may be partially mediated through its immunotoxic effects; for example, some studies suggest that lead exposure can elevate serum immunoglobulin E levels, thereby increasing the risk of allergy and asthma.54,55
Furthermore, it is important to recognize that the relevance and magnitude of individual risk factors vary substantially across regions, reflecting the interplay between local dietary traditions, environmental conditions, and stages of epidemiological transition. For instance, iron deficiency may be compounded in South Asia and Sub-Saharan Africa by endemic parasitic infections such as hookworm and malaria, which exacerbate iron losses through chronic blood loss and impair intestinal absorption.56 Household air pollution from solid fuels—an asthma-specific risk factor—remains disproportionately prevalent in Sub-Saharan Africa and South Asia, where biomass fuels continue to dominate household energy use, particularly in rural settings with limited access to clean energy infrastructure.57 In contrast, metabolic risk factors such as high body-mass index and high fasting plasma glucose are gaining increasing relevance in regions undergoing rapid nutrition transitions, including parts of the Middle East, Latin America, Africa and East Asia, where the convergence of traditional dietary patterns with the widespread availability of energy-dense processed foods creates a dual burden of undernutrition and metabolic disease.58–60 Similarly, kidney dysfunction, which exhibited the strongest association with IHD in this study, is particularly relevant in regions with high prevalence of uncontrolled hypertension and diabetes, such as Latin America and Western Asia, where the cardiorenal-metabolic continuum imposes a substantial and growing disease burden.61–63 These regional nuances underscore the inadequacy of a one-size-fits-all approach to comorbidity prevention and highlight the necessity of tailoring intervention strategies to the specific risk factor profiles dominant in each geographic context.
This study constructed a composite risk index to quantify the cumulative effect of IHD and asthma risk, reflecting a higher disease burden in African and Asian countries and revealing systemic manifestations of global health inequalities. The index comprehensively considers nutritional status, environmental exposures, and socioeconomic indicators, embodying the systems biology concept of multilevel factors intertwining to influence disease risk.64 Compared with traditional single-factor risk assessments, the composite index better reflects the multidimensional drivers of disease occurrence, helping to uncover pathogenic pathways underlying regional disparities and identify potential intervention targets. Moreover, the substantial overlap between the geographical distribution of the composite risk index and the “concordant-type” shared burden pattern holds significant public health implications, indicating that populations in regions with the highest risk indices are simultaneously exposed to multiple adverse environments that promote both ischemic heart disease and asthma, leading to a superimposed comorbidity burden. Therefore, interventions targeting these shared and specific risk factors—such as promoting clean household energy to reduce solid fuel pollution,65 encouraging a balanced diet rich in vegetables, and controlling traditional cardiometabolic risk factors—are expected to yield synergistic effects, simultaneously alleviating the dual disease burden on the cardiopulmonary system.
Our findings can also be meaningfully situated within the broader literature on large-scale multimorbidity studies. Previous research utilizing data from UK Biobank cohorts has consistently demonstrated that cardiovascular and respiratory diseases tend to cluster within individuals, suggesting shared pathophysiological substrates that transcend traditional organ-system boundaries.66 A recent multi-country analysis of multimorbidity patterns identified cardiometabolic–respiratory clusters as one of the most prevalent disease combinations globally, with particularly high co-occurrence rates in low- and middle-income countries.67 Our ecological-level findings extend these individual-level observations, revealing that the spatial clustering of IHD and asthma burden across nations mirrors the co-occurrence patterns described in patient-level studies. Moreover, the identification of nutritional deficiencies and environmental exposures as shared drivers aligns with an emerging body of evidence from the multimorbidity literature emphasizing systemic inflammation, oxidative stress, and adverse environmental exposures as upstream determinants of multi-organ disease.68,69 However, unlike most previous comorbidity studies, which have predominantly focused on high-income settings with well-established health surveillance infrastructure, the present study provides a truly global perspective that captures the disproportionate burden borne by resource-limited regions in Africa and Asia. In this regard, our work complements and extends existing large-scale comorbidity analyses by demonstrating that macro-level risk factor landscapes—encompassing dietary quality, environmental pollution, and metabolic health—collectively shape the global geography of cardiopulmonary multimorbidity.
An important limitation of this study pertains to its secondary analytical nature. All data used in this study were derived from the GBD 2021, a large-scale collaborative database constructed through systematic reviews, statistical modeling, and estimation procedures by the GBD consortium. Our research team did not directly participate in the original data collection, disease modeling, or estimation processes of the GBD study. Consequently, the contextual details underlying the original data—including local diagnostic criteria, case definitions, data collection instruments, surveillance system characteristics, and field-level operational factors—may not be fully transparent to us. This inherent reliance on secondary data limits our ability to fully assess the validity and generalizability of the source estimates at the subnational level and may introduce uncertainties that are difficult to quantify. Readers should therefore interpret our findings with the understanding that they are constrained by the quality, completeness, and methodological assumptions of the underlying GBD estimates, as detailed in the original GBD publications.70 Furthermore, it should be noted that the associations revealed in this study are at the national population level and cannot be directly extrapolated to individual-level causal relationships. In addition, the exposure data for risk factors used in the study are mostly estimates at the national level, which may not fully capture exposure differences among subpopulations or regions within a country, nor reflect the precise dosage and time window of individual exposure. For example, the assessment of household air pollution exposure may not have fully accounted for modifying factors such as ventilation conditions and cookstove types.71 Furthermore, despite efforts to screen via multi-stage models, there may still be unmeasured confounding factors—such as genetic background, healthcare access, and other environmental pollutants—that could affect the accuracy of the results. Moreover, this study is limited by its reliance on single-year (2021) cross-sectional data, which precludes the inference of temporal trends or causal relationships between risk factor exposure and disease burden. The observed associations represent a snapshot of the global burden landscape at a single time point and may be influenced by year-specific events, most notably the COVID-19 pandemic, which may have concurrently altered both disease burden estimates and risk factor exposure levels in 2021. Future research incorporating longitudinal data spanning multiple GBD cycles is warranted to elucidate the temporal dynamics and potential lagged effects of risk factor exposure on the comorbidity burden of IHD and asthma. An additional limitation concerns the practical implementation of the integrated prevention strategies suggested by this study. While the co-localization of shared risk factors with concordant disease burden patterns provides a compelling epidemiological basis for combined interventions, the synergistic advantages of such integrated approaches over separate, disease-specific programs remain theoretical and await empirical confirmation. Future research should therefore incorporate prospective cohort data to explore the interaction mechanisms of shared risk factors at the individual level, and should employ intervention study designs—including pragmatic cluster-randomized trials and quasi-experimental approaches—to directly evaluate whether integrated strategies targeting shared nutritional, metabolic, and environmental determinants yield greater cardiopulmonary health benefits than conventional single-disease prevention programs.
Conclusions
In summary, this study is the first to systematically delineate the comorbidity landscape of IHD and asthma on a global scale. It confirms that approximately one-quarter of countries face a “consistent-type” burden, characterized by the simultaneous high prevalence of both diseases. Through multi-stage machine learning and statistical modeling, this study reveals the complex interplay of nutritional, metabolic, and environmental factors in the formation of comorbidity. Based on these findings, a comprehensive risk index was constructed to quantify differences in cumulative risk levels across countries, providing macro-level evidence for identifying high-risk regions and supporting the development of targeted public health interventions.
From an implementation perspective, the findings of this study carry implications across multiple levels of the health system. At the primary care level, the identification of shared risk factors suggests that integrating cardiopulmonary risk co-screening into routine clinical assessments—particularly among patients presenting with either IHD or asthma—could facilitate early detection of the comorbid condition and enable more holistic management. At the public health level, community-based programs that simultaneously address nutritional supplementation, promotion of clean household energy, and reduction of environmental pollutant exposure have the potential to target multiple shared and disease-specific risk factors identified in this study, thereby achieving broader health gains within a single programmatic framework. At the policy level, the composite risk index developed in this study could serve as a practical tool for cross-sectoral resource allocation, enabling governments and international organizations to prioritize regions where populations face the greatest cumulative burden and to coordinate cardiovascular, respiratory, and nutrition-related policy agendas.
Data Sharing Statement
Data from this article are available in the Global Burden of Disease Study 2021 at https://vizhub.healthdata.org/gbd-results/.
Ethics Approval and Consent to Participate
This study used publicly available, anonymized data and did not involve individual-level human subjects. Therefore, this study was reviewed and approved as exempt from ethical review and informed consent by the Ethics Review Committee of Heji Hospital Affiliated to Changzhi Medical College.
Acknowledgments
We gratefully acknowledge the collaborators of the Global Burden of Disease Study 2021 for their invaluable contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/ and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
References
1. Duggan JP, Peters AS, Trachiotis GD, Antevil JL. Epidemiology of coronary artery disease. Surg Clin North Am. 2022;102(3):499–16. doi:10.1016/j.suc.2022.01.007
2. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob health. 2021;11(2):169–177. doi:10.2991/jegh.k.201217.001
3. Gouvinhas C, Severo M, Azevedo A, Lunet N. Worldwide patterns of ischemic heart disease mortality from 1980 to 2010. Int J Cardiol. 2014;170(3):309–314. doi:10.1016/j.ijcard.2013.11.004
4. Vancheri F, Tate AR, Henein M, et al. Time trends in ischaemic heart disease incidence and mortality over three decades (1990-2019) in 20 Western European countries: systematic analysis of the global burden of disease study 2019. Eur J Prevent Cardiol. 2022;29(2):396–403. doi:10.1093/eurjpc/zwab134
5. Jo EJ, Lee YU, Kim A, Park HK, Kim C. The prevalence of multiple chronic conditions and medical burden in asthma patients. PLoS One. 2023;18(5):e0286004. doi:10.1371/journal.pone.0286004
6. Liu H, Fu Y, Wang K. Asthma and risk of coronary heart disease: a meta-analysis of cohort studies. Ann Allergy Asthma Immunol. 2017;118(6):689–695. doi:10.1016/j.anai.2017.03.012
7. Iribarren C, Tolstykh IV, Miller MK, Sobel E, Eisner MD. Adult asthma and risk of coronary heart disease, cerebrovascular disease, and heart failure: a prospective study of 2 matched cohorts. Am J Epidemiol. 2012;176(11):1014–1024. doi:10.1093/aje/kws181
8. Panichi V, Scatena A, Migliori M, Marchetti V, Paoletti S, Beati S. Biomarkers of chronic inflammatory state in uremia and cardiovascular disease. Int J Inf. 2012;2012:360147. doi:10.1155/2012/360147
9. Lee HS, Kim BK, Lee SY, Kwon H, Park HW. Essential role of Card11 in airway hyperresponsiveness in high-fat diet-induced obese mice. Exp Mol Med. 2024;56(12):2747–2754. doi:10.1038/s12276-024-01367-z
10. Palmer-Crocker RL, Hughes CC, Pober JS. IL-4 and IL-13 activate the JAK2 tyrosine kinase and Stat6 in cultured human vascular endothelial cells through a common pathway that does not involve the gamma c chain. J Clin Invest. 1996;98(3):604–609. doi:10.1172/JCI118829
11. Potaczek DP. Links between allergy and cardiovascular or hemostatic system. Int J Cardiol. 2014;170(3):278–285. doi:10.1016/j.ijcard.2013.11.029
12. Cazzola M, Hanania NA, Rogliani P, Matera MG. Cardiovascular disease in asthma patients: from mechanisms to therapeutic implications. Kardiol Pol. 2023;81(3):232–241. doi:10.33963/KP.a2023.0038
13. Lippi G, Cervellin G, Sanchis-Gomar F. Immunoglobulin E (IgE) and ischemic heart disease. Which came first, the chicken or the egg? Ann Med. 2014;46(7):456–463. doi:10.3109/07853890.2014.927714
14. Garg VS, Sojitra MH, Ubhadiya TJ, et al. Understanding the link between adult asthma and coronary artery disease: a narrative review. Cureus. 2023;15(8):e43621. doi:10.7759/cureus.43621
15. Hall M, Dondo TB, Yan AT, et al. Multimorbidity and survival for patients with acute myocardial infarction in England and Wales: latent class analysis of a nationwide population-based cohort. PLoS Med. 2018;15(3):e1002501. doi:10.1371/journal.pmed.1002501
16. Lee CJ, Hwang J, Kang CY, et al. Asthma and increased risk of myocardial infarction and mortality among hypertensive Korean patients. Hypertens Res. 2023;46(7):1694–1704. doi:10.1038/s41440-023-01257-3
17. Carter P, Lagan J, Fortune C, et al. Association of cardiovascular disease with respiratory disease. J Am Coll Cardiol. 2019;73(17):2166–2177. doi:10.1016/j.jacc.2018.11.063
18. Xu YY, Xie J, Yin H, et al. The global burden of disease attributable to low physical activity and its trends from 1990 to 2019: an analysis of the global burden of disease study. Front Public Health. 2022;10:1018866. doi:10.3389/fpubh.2022.1018866
19. Ma J, Wang X, Gao M, Ding Y, Guan Y. Effect of smoking status on coronary artery disease among Chinese post-menopausal women. Intern Emerg Med. 2016;11(4):529–535. doi:10.1007/s11739-015-1334-1
20. An X, Liu Z, Zhang L, et al. Co-occurrence patterns and related risk factors of ischaemic heart disease and ischaemic stroke across 203 countries and territories: a spatial correspondence and systematic analysis. Lancet Glob Health. 2025;13(5):e808–e819. doi:10.1016/S2214-109X(25)00013-0
21. GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2162–2203. doi:10.1016/S0140-6736(24)00933-4
22. Roth AE. The Shapley Value: Essays in Honor of Lloyd S. Shapley. Cambridge University Press; 1988.
23. Ezzati M, Hoorn SV, Rodgers A, Lopez AD, Mathers CD, Murray CJ. Estimates of global and regional potential health gains from reducing multiple major risk factors. Lancet. 2003;362(9380):271–280. doi:10.1016/S0140-6736(03)13968-2
24. Soriano JB, Kendrick PJ, Paulson KR; GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
25. Chong B, Jayabaskaran J, Jauhari SM, et al. Global burden of cardiovascular diseases: projections from 2025 to 2050. Eur J Prevent Cardiol. 2025;32(11):1001–1015. doi:10.1093/eurjpc/zwae281
26. He KJ, Wang H, Liu X, Yang R, Gong G. Global, regional, and national burden of IHD attributable to PM pollution aged 70 and above: an age-period-cohort modeling and frontiers analysis study. Front Public Health. 2025;13:1573599. doi:10.3389/fpubh.2025.1573599
27. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
28. Zhao D. Epidemiological features of cardiovascular disease in Asia. JACC Asia. 2021;1(1):1–13. doi:10.1016/j.jacasi.2021.04.007
29. Hâncean MG, Lerner J, Perc M, et al. Processed food intake assortativity in the personal networks of older adults. Sci Rep. 2025;15(1):10459. doi:10.1038/s41598-025-94969-0
30. Lui M, Safiri S, Mereke A, et al. Burden of ischemic heart disease in central Asian countries, 1990-2017. Int J Cardiol Heart Vasculature. 2021;33:100726. doi:10.1016/j.ijcha.2021.100726
31. Smolić Š. Golden aging: prospects for healthy, active, and prosperous aging in Europe and Central Asia. Public Sector Economics. 2018;42(3):347–351. doi:10.3326/pse.42.3.6
32. Perera E, Codispoti C, Mahdavinia M. The concept of environmental injustice in allergy and asthma. Curr Opin Allergy Clin Immunol. 2026;26(1):21–28. doi:10.1097/ACI.0000000000001127
33. Kuyinu YA, Adeyeye OO, Addo-Yobo E, et al. ‘It makes us sick’: experiences of air pollution among children with asthma and their caregivers in African countries. IJTLD Open. 2025;2(9):505–511. doi:10.5588/ijtldopen.24.0659
34. Zhang ZQ, Li JY, Guo Q, et al. Association between air pollution and allergic upper respiratory diseases: a meta-analysis. Eur Respir Rev. 2025;34(176):240266. doi:10.1183/16000617.0266-2024
35. Desalu O, Ozoh O. Achieving asthma control in low-middle-income countries: why it is important? J Pan Afr Thorac Soc. 2021;2(2):59–60. doi:10.25259/JPATS_18_2021
36. Chung MY, Kim BH. Fatty acids and epigenetics in health and diseases. Food Sci Biotechnol. 2024;33(14):3153–3166. doi:10.1007/s10068-024-01664-3
37. González-Becerra K, Ramos-Lopez O, Barrón-Cabrera E, et al. Fatty acids, epigenetic mechanisms and chronic diseases: a systematic review. Lipids Health Dis. 2019;18(1):178. doi:10.1186/s12944-019-1120-6
38. van Esch B, Porbahaie M, Abbring S, et al. The impact of milk and its components on epigenetic programming of immune function in early life and beyond: implications for allergy and asthma. Front Immunol. 2020;11:2141. doi:10.3389/fimmu.2020.02141
39. DiNicolantonio JJ, O’Keefe JH. Importance of maintaining a low omega-6/omega-3 ratio for reducing inflammation. Open Heart. 2018;5(2):e000946. doi:10.1136/openhrt-2018-000946
40. Hodge L, Salome CM, Hughes JM, et al. Effect of dietary intake of omega-3 and omega-6 fatty acids on severity of asthma in children. Eur Respir J. 1998;11(2):361–365. doi:10.1183/09031936.98.11020361
41. Packer M, Anker SD, Butler J, et al. Identification of three mechanistic pathways for iron-deficient heart failure. Eur Heart J. 2024;45(26):2281–2293. doi:10.1093/eurheartj/ehae284
42. Roth-Walter F, Pacios LF, Bianchini R, Jensen-Jarolim E. Linking iron-deficiency with allergy: role of molecular allergens and the microbiome. Metallomics. 2017;9(12):1676–1692. doi:10.1039/C7MT00241F
43. Aschard H, Chen J, Cornelis MC, Chibnik LB, Karlson EW, Kraft P. Inclusion of gene-gene and gene-environment interactions unlikely to dramatically improve risk prediction for complex diseases. Am J Hum Genet. 2012;90(6):962–972. doi:10.1016/j.ajhg.2012.04.017
44. Bisciglia A, Pasceri V, Irini D, Varveri A, Speciale G. Risk factors for ischemic heart disease. Rev Recent Clin Trials. 2019;14(2):86–94. doi:10.2174/1574887114666190328125153
45. Lu X, Peng X, Zhang Y, et al. Global trends and the case of China in cardio-kidney-metabolic multimorbidity: development and validation of a composite risk index using GBD 1990-2021 data. J Health Popul Nutr. 2026;45(1):44. doi:10.1186/s41043-025-01194-6
46. Shi W, Zhang T, Li Y, Huang Y, Luo L. Association between household air pollution from solid fuel use and risk of chronic diseases and their multimorbidity among Chinese adults. Environ Int. 2022;170:107635. doi:10.1016/j.envint.2022.107635
47. Lee KK, Bing R, Kiang J, et al. Adverse health effects associated with household air pollution: a systematic review, meta-analysis, and burden estimation study. Lancet Glob Health. 2020;8(11):e1427–e1434. doi:10.1016/S2214-109X(20)30343-0
48. Jo H, Kim TH, Park J; GBD 2023 Asia Chronic Respiratory Disease Collaborators. Burden of chronic respiratory disease in Asia, 1990-2023: a systematic analysis for the global burden of disease study 2023. Lancet Respir Med. 2026;14(3):233–255. doi:10.1016/S2213-2600(25)00404-7
49. Abebe Y, Ali A, Kumie A, Haile T, Tamire M, Addissie A. Determinants of asthma in Ethiopia: age and sex matched case control study with special reference to household fuel exposure and housing characteristics. Asthma Res Pract. 2021;7(1):14. doi:10.1186/s40733-021-00080-2
50. Hosseini B, Berthon BS, Wark P, Wood LG. Effects of fruit and vegetable consumption on risk of asthma, wheezing and immune responses: a systematic review and meta-analysis. Nutrients. 2017;9(4):341. doi:10.3390/nu9040341
51. Mendes FC, Paciência I, Cavaleiro Rufo J, et al. Higher diversity of vegetable consumption is associated with less airway inflammation and prevalence of asthma in school-aged children. Pediatr Allergy Immunol. 2021;32(5):925–936. doi:10.1111/pai.13446
52. Yang Z, Zheng W, Yung E, Zhong N, Wong GW, Li J. Frequency of food group consumption and risk of allergic disease and sensitization in schoolchildren in urban and rural China. Clin Exp Allergy. 2015;45(12):1823–1832. doi:10.1111/cea.12532
53. Nurmatov U, Devereux G, Sheikh A. Nutrients and foods for the primary prevention of asthma and allergy: systematic review and meta-analysis. J Allergy Clin Immunol. 2011;127(3):
54. Wells EM, Bonfield TL, Dearborn DG, Jackson LW. The relationship of blood lead with immunoglobulin E, eosinophils, and asthma among children: NHANES 2005-2006. Int J Hyg Environ Health. 2014;217(2–3):196–204. doi:10.1016/j.ijheh.2013.04.010
55. Wang IJ, Karmaus WJJ, Yang CC. Lead exposure, IgE, and the risk of asthma in children. J Expo Sci Environ Epidemiol. 2017;27(5):478–483. doi:10.1038/jes.2017.5
56. Mahittikorn A, Masangkay FR, De Jesus Milanez G, Kuraeiad S, Kotepui M. Prevalence and effect of Plasmodium spp. and hookworm co-infection on malaria parasite density and haemoglobin level: a meta-analysis. Sci Rep. 2022;12(1):6864. doi:10.1038/s41598-022-10569-2
57. van Gemert F, van der Molen T, Jones R, Chavannes N. The impact of asthma and COPD in sub-Saharan Africa. Prim Care Respir J. 2011;20(3):240–248. doi:10.4104/pcrj.2011.00027
58. Xia J, Fan S, Ding X, et al. Development of sustainable healthy diets in China. Strat Study Chin Acad Eng. 2023;25(4):120–127.
59. Vorster HH, Kruger A, Margetts BM. The nutrition transition in Africa: can it be steered into a more positive direction? Nutrients. 2011;3(4):429–441. doi:10.3390/nu3040429
60. Peña M, Bacallao J. Obesity and Poverty: A New Public Health challenge. Pan American Health Org; 2000.
61. Gonzalez-Bedat M, Rosa-Diez G, Pecoits-Filho R, et al. Burden of disease: prevalence and incidence of ESRD in Latin America. Clin Nephrol. 2015;83(7 Suppl 1):3–6. doi:10.5414/CNP83S003
62. Suriyong P, Ruengorn C, Shayakul C, Anantachoti P, Kanjanarat P. Prevalence of chronic kidney disease stages 3-5 in low- and middle-income countries in Asia: a systematic review and meta-analysis. PLoS One. 2022;17(2):e0264393. doi:10.1371/journal.pone.0264393
63. Hasan MJ, Haque A, Ray NC, Rahman AMMT. Coexistence of cardiovascular and renal disease: a study on burden of cardiorenal syndrome in a tertiary care hospital in Bangladesh. Commun Based Med J. 2026;15(1):155–161. doi:10.3329/cbmj.v15i1.87626
64. Mutch DM, Zulyniak MA, Rudkowska I, Tejero ME. Lifestyle genomics: addressing the multifactorial nature of personalized health. Lifestyle Genomics. 2018;11(1):1–8. doi:10.1159/000492297
65. Puzzolo E, Fleeman N, Lorenzetti F, et al. Estimated health effects from domestic use of gaseous fuels for cooking and heating in high-income, middle-income, and low-income countries: a systematic review and meta-analyses. Lancet Respir Med. 2024;12(4):281–293. doi:10.1016/S2213-2600(23)00427-7
66. Dong G, Feng J, Sun F, Chen J, Zhao XM. A global overview of genetically interpretable multimorbidities among common diseases in the UK Biobank. Genome Med. 2021;13(1):110. doi:10.1186/s13073-021-00927-6
67. Garin N, Koyanagi A, Chatterji S, et al. Global multimorbidity patterns: a cross-sectional, population-based, multi-country study. J Gerontol a Biol Sci Med Sci. 2016;71(2):205–214. doi:10.1093/gerona/glv128
68. Burke H, Wilkinson TMA. Unravelling the mechanisms driving multimorbidity in COPD to develop holistic approaches to patient-centred care. Eur Respir Rev. 2021;30(160):210041. doi:10.1183/16000617.0041-2021
69. Zeliger HI. Predicting disease onset in clinically healthy people. Interdiscip Toxicol. 2016;9(2):39–54. doi:10.1515/intox-2016-0006
70. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
71. Dai X, Bui DS, Perret JL, et al. Exposure to household air pollution over 10 years is related to asthma and lung function decline. Eur Respir J. 2021;57(1):2000602. doi:10.1183/13993003.00602-2020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence, Management, and Risk Factors of Asthma Among School-Age Children in Yogyakarta, Indonesia
Triasih R, Setyowireni D, Nurani N, Setyati A
Journal of Asthma and Allergy 2023, 16:23-32
Published Date: 5 January 2023
Comorbid Heart Disease in Patients with COPD is Associated with Increased Hospitalization and Mortality – A 15-Year Follow-Up
Giezeman M, Sundh J, Athlin Å, Lisspers K, Ställberg B, Janson C, Montgomery S, Kisiel MA, Nager A, Sandelowsky H, Hasselgren M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:11-21
Published Date: 9 January 2023
Predictors of Tuberculosis and Non-Communicable Disease Comorbidities Among Newly Enrolled Tuberculosis Patients, Southern Ethiopia
Nunemo MH, Gidebo KD, Woticha EW, Lemu YK
Integrated Blood Pressure Control 2023, 16:95-109
Published Date: 22 November 2023
Extrapulmonary Comorbidities Associated with Chronic Obstructive Pulmonary Disease: A Review
Xiang Y, Luo X
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:567-578
Published Date: 29 February 2024
Global, Regional, and National Burden of Ischemic Heart Disease Attributable to 25 Risk Factors and Their Summary Exposure Value Across 204 Countries With Different Socio-Demographic Index Levels, 1990–2021: A Systematic Fixed-Effects Analysis and Comparative Study
Tan J, Xue M, Li H, Liu Y, He Y, Liu J, Liu J, Tang L, Lin J
Clinical Epidemiology 2025, 17:105-129
Published Date: 20 February 2025