Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Smoking-Attributable Burden of Chronic Obstructive Pulmonary Disease from 1990 to 2021: Temporal Trends and Evidence from the Global Burden of Disease Study
Authors Ma T, Yue X, Rong S, Sun R, Wang J, Zheng X, Chen X, Sun R
Received 27 January 2026
Accepted for publication 9 May 2026
Published 22 May 2026 Volume 2026:21 599370
DOI https://doi.org/10.2147/COPD.S599370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Tianqi Ma,1,2,* Xianfeng Yue,3,4,* Shuyu Rong,5,* Rongqian Sun,3 Junyao Wang,3 Xin Zheng,3 Xueyu Chen,3 Rongqin Sun1
1Department of Emergency, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, Shandong, People’s Republic of China; 2Sydney School of Public Health, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia; 3School of Public Health, Shandong First Medical University & Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 4School of Public Health, Jining Medical University, Jining, Shandong, People’s Republic of China; 5School of Radiology, Shandong First Medical University & Shandong Academy of Medical Sciences, Taian, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xueyu Chen, Email [email protected] Rongqin Sun, Email [email protected]
Introduction: Chronic obstructive pulmonary disease (COPD) is a leading cause of death and disability worldwide, with smoking being the primary contributor. This study aims to assess the temporal and spatial trends in the burden of smoking-attributable COPD from 1990 to 2021 and project future trajectories, providing insights for COPD prevention strategies.
Methods: The data were sourced from the Global Burden of Disease (GBD) 2021 database, incorporating estimates and uncertainty intervals (UI) for deaths, disability-adjusted life years (DALYs), and age-standardized rates (ASRs) of smoking-attributable COPD across 204 countries and regions worldwide. Estimated annual percentage change (EAPC), frontier analysis, decomposition analysis, and Bayesian age-period-cohort (BAPC) modeling were used to evaluate temporal trends, development-related gaps, drivers of change, and future burden.
Results: From 1990 to 2021, global smoking-attributable COPD showed a divergence between rising absolute burden and declining ASRs. Deaths increased from 10,538 (95% UI: 8,724– 12,339) hundred to 13,350 (95% UI: 10,533– 15,966) hundred, and DALYs rose from 23,601 (95% UI: 19,648– 27,495) thousand to 27,795 (95% UI: 22,234– 32,884) thousand, whereas ASRs declined across most regions. The steepest declines in ASRs were observed in High-middle SDI regions, whereas Middle and Low-middle SDI regions carried the greatest absolute burden in 2021. Males consistently bore a higher burden than females. DALYs increased with age, peaking at 70– 74 years. Ageing and population growth were the main contributors to the rise in DALYs, while epidemiological changes had a negative effect. By 2040, global ASMR and ASDR are projected to decline to 11.62 and 240.32 per 100,000 population, respectively.
Conclusion: Despite global progress in reducing the ASRs of smoking-related COPD, the absolute burden continues to rise. Further progress may require sustained tobacco control, earlier detection, and improved long-term COPD care, especially in settings where demographic pressures offset epidemiological gains.
Keywords: chronic obstructive pulmonary disease, smoking, global burden of disease, socio-demographic index, age-standardized rates
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable lung disorder characterized by persistent respiratory symptoms and spirometry-verified progressive airflow limitation.1,2 Development of COPD has been associated with an aberrant pulmonary inflammatory response to inhaled noxious particles and gases.3 Recent global estimates attribute more than three million deaths per year to COPD, underscoring its substantial contribution to global mortality.4 As prevalence continues to climb, COPD has moved from the fourth to the third leading cause of death worldwide and, by 2020, has already surpassed 400 million cases—ten years earlier than the World Health Organization’s original projection for 2030.1,5,6 Numerous factors contribute to COPD development, including air pollution, occupational exposures, genetic predisposition, recurrent respiratory infections, and socioeconomic factors, all of which play critical roles in disease onset and progression.7
Major risk factors for COPD remain widespread worldwide. An estimated 2 billion people are exposed to emissions from biomass-fuel combustion, 1 billion to ambient (outdoor) air pollution, and about 1 billion are current smokers—thereby exposing a comparable number of nonsmokers to secondhand smoke.8 Environmental and occupational hazards together with tobacco use are the predominant risk factors for chronic respiratory diseases (CRDs). Tobacco smoke is a complex aerosol of particulate tar and reactive gases that deposits throughout the respiratory tract depending on particle size, with smaller particles reaching peripheral bronchioles and alveoli and initiating chronic injury of the airway and parenchyma.9 The chemical constituents drive oxidative stress, persistent airway inflammation, mucociliary dysfunction, and defective epithelial repair, fostering infection, small airway remodeling, and the progressive airflow limitation that typifies COPD.10 Global Burden of Disease (GBD) 2021 identified smoking as the leading contributor to COPD DALYs worldwide, exceeding ambient particulate matter pollution, household air pollution from solid fuels, and occupational particulate matter, gases, and fumes;11 this provides a clear rationale for examining smoking-attributable COPD burden separately from total COPD burden. Smoking patterns vary substantially by geography, culture, age, and sex,12 with prevalence remaining markedly higher among men than among women worldwide.13 They also differ across birth cohorts, as later-born cohorts in some settings tend to experience lower smoking initiation, higher cessation, and reduced cumulative lifetime exposure compared with earlier-born cohorts, which may influence future COPD burden.14
Although the effects of tobacco smoking on COPD have been widely studied, notable gaps persist—particularly the scarcity of long-term spatiotemporal analyses across diverse geographies and Socio-demographic Index (SDI) strata, as well as forward-looking burden projections.15,16 Prior GBD evidence has provided important insight into the burden of COPD attributable to major risk factors across SDI levels, age groups, and sex,17 but has largely relied on GBD 2019 estimates through 2019 and has not incorporated the GBD 2021 update or the broader analytical framework. Leveraging data from the GBD 2021 study, the present study updates and extends prior evidence by quantifying temporal and spatial trends in smoking-attributable COPD burden from 1990 to 2021, delineating heterogeneity by sex, age, region, and SDI level, conducting frontier and decomposition analyses, and projecting future burden using a Bayesian age-period-cohort (BAPC) framework. The results of this study would provide policy-relevant evidence to inform the design and targeting of tobacco-control and respiratory-health interventions worldwide.
Methods
Overview
Data were obtained from the GBD 2021 database, a comprehensive, systematic resource covering 371 diseases and injuries and 88 risk factors.18 Estimates with 95% uncertainty intervals (UIs) for smoking-attributable deaths, disability-adjusted life years (DALYs), and age-standardized rates (ASRs) for COPD were extracted. ASRs include the age-standardized mortality rates (ASMR) and age-standardized disability-adjusted life years (ASDR). Analyses were performed for 5-year age groups from 30 to 95 years old, with an additional category for ≥95 years. Because GBD estimates are generated through statistical modeling and data synthesis rather than direct observation alone, uncertainty may be greater in settings with sparse or lower-quality primary data. Accordingly, all estimates are reported with 95% UI, and these intervals should be interpreted with particular caution in data-sparse locations.
Definition of Smoking and COPD
In GBD 2021, smoking-attributable burden is estimated within the comparative risk assessment (CRA) framework, which combines population exposure distributions, relative risks, and a counterfactual theoretical minimum risk exposure level (TMREL).19 Therefore, the attributable burden reflects exposure–risk relationships over the life course rather than current smoking status alone. For descriptive purposes, smoking exposure includes the current use of any combustible tobacco product, whether daily or occasional.13
COPD is defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, with a forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) ratio of less than 0.7 following a spirometry test. The International Classification of Diseases (ICD) codes employed by the GBD study include J41, J42, J43, J44, and J47 (ICD-10 codes), as well as 491, 492, and 496 (ICD-9 codes), for the identification of cases related to COPD. In addition to the GOLD criteria, the GBD also takes into account a variety of alternative diagnostic standards. These include pre-bronchodilator GOLD criteria, lower limit of normal (LLN), and European Respiratory Society (ERS) guidelines. Because GBD integrates multiple diagnostic definitions across data sources, including GOLD, LLN, ERS, and related criteria, heterogeneity in diagnostic standards may introduce uncertainty into burden estimates. In particular, the fixed-ratio GOLD criterion may overdiagnose airflow limitation in older adults.20
Socio-Demographic Index (SDI)
SDI is a composite measure of overall socioeconomic development, scaled from 0 to 1, with higher values indicating greater development.21 The present study employed SDI to examine the relationship between the burden of smoking- attributable COPD and the degree of socioeconomic development. The dataset includes 204 countries and regions, stratified into five distinct regions based on SDI levels: Low (SDI ≤ 0.47), Low-middle (0.47 < SDI ≤ 0.62), Middle (0.62 < SDI ≤ 0.71), High-middle (0.71 < SDI ≤ 0.81), and High (SDI > 0.81).22 In addition, the classification system is segmented into 21 GBD regions, which are distinguished for geographic comparisons.
Time-Trend Analysis
Temporal trends in ASMR and ASDR were quantified using the estimated annual percentage change (EAPC).23,24 For each location, a linear model was fitted to the natural logarithm of the ASR over calendar year. The following equation was employed to estimate the EAPC:


The 95% confidence interval (CI) for the EAPC was derived from the standard error of β. Specifically, if the lower limit entirely above or below 0 indicated a significant increase or decrease; otherwise, the trend was considered stable.
Frontier Analysis
Frontier analysis was conducted in order to examine the non-linear association between the smoking-attributable COPD burden, measured by ASDR, and the SDI. A deterministic, non-parametric frontier approach was used. After observations were ordered by SDI, the frontier was defined as the empirical lower envelope of the relationship between SDI and ASDR, without assuming any prespecified functional form. To improve robustness, 500 bootstrap resamples were performed, and the frontier estimates were averaged across resamples. For each country or territory, the distance to the frontier quantifies the gap between the observed burden and the potential minimum, indicating the scope for further reduction.
Decomposition Analysis
Das Gupta decomposition method was employed to disaggregate the net changes in smoking-related COPD burden between 1990 and 2021 into the effects of ageing, population growth, and epidemiologic changes.25,26 Using 1990 as the reference year and 2021 as the comparison year, the decomposition analysis was performed on absolute DALY counts. This methodological approach enabled the disentangling of the overall variation in disease burden and the quantification of the independent effect of each factor. A thorough examination of these trends has enabled us to develop a more profound understanding of the potential factors that may lead to changes in the global burden of smoking-induced COPD.
Bayesian Age-Period-Cohort (BAPC)
To estimate and forecast the future burden of smoking-attributable COPD, the BAPC model was applied. Parameters were estimated via the Integrated Nested Laplace Approximations (INLA) method in R, incorporating the effects of age, period, and birth cohort. Age-specific deaths and DALYs, together with the corresponding population data, were organized into age-by-period matrices for model fitting. Separate projections were generated for males and females, and the projected age-specific estimates were subsequently used to calculate ASMR and ASDR. The ASMR and ASDR projections extend through the year 2040, with the results reported as estimates accompanied by their respective 95% CI. To evaluate the predictive performance of the BAPC model, a back-testing analysis was performed. Data from 1990 to 2011 were used for model fitting, and values for 2012–2021 were predicted and compared with the observed estimates. The mean absolute percentage error (MAPE) was calculated to quantify prediction accuracy.
Statistical Analysis
Analyses were stratified by sex, age group, SDI, country, and GBD region. The objective was to elucidate variation in the burden of smoking-induced COPD among different regions and demographics. Unless otherwise specified, point estimates were presented with 95% UIs (GBD outputs) or 95% CIs (model-based statistics such as EAPC). All analyses and graphical presentations were performed using the R software program (Version 4.4.2).
Results
Global Burden and Trends of Smoking-Related COPD
From 1990 to 2021, the global deaths and DALYs attributable to smoking-related COPD exhibited a gradual upward trajectory, increased by 27% and 18%, respectively (Figure 1A and B). Deaths rose from 10,538 (95% UI: 8,724–12,339) hundred in 1990 to 13,350 (95% UI: 10,533–15,966) hundred in 2021, while DALYs increased from 23,601 (95% UI: 19,648–27,495) thousand to 27,795 (95% UI: 22,234–32,884) thousand (Table 1). Despite the rising counts, both ASMR and ASDR declined over time (Figure 1C and D). In 2021, the global ASMR and ASDR were 16.12 (95% UI: 12.68–19.29) and 325.52 (95% UI: 260.32–385.52) per 100,000 people, respectively. EAPC was −2.26 (95% CI: −2.37 to −2.16) for ASMR and −2.31 (95% CI: −2.39 to −2.23) for ASDR, indicating sustained downward trajectory (Table 1).
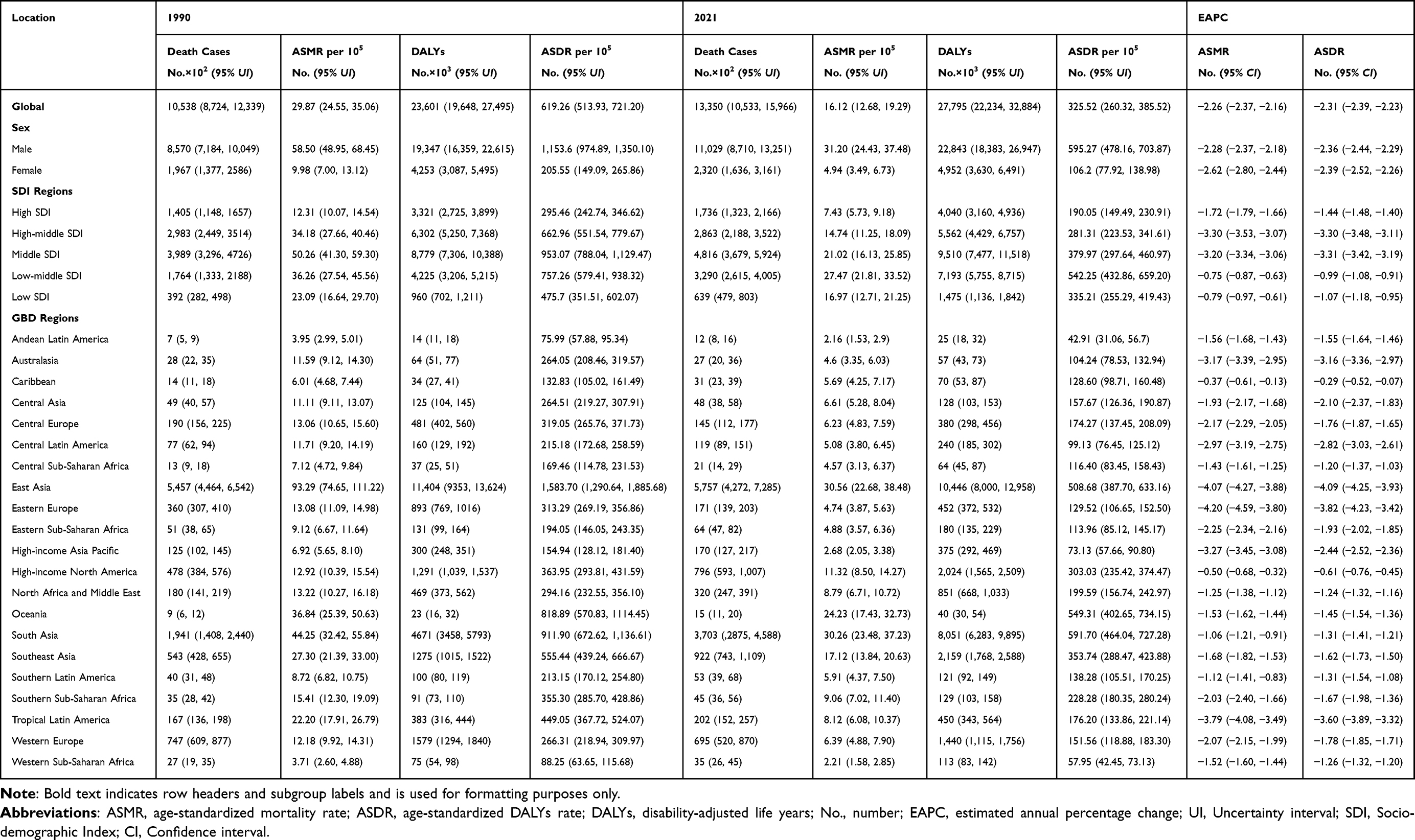 |
Table 1 The Global Burden of COPD Attributable to Smoking in 1990 and 2021 and the Temporal Trends During 1990–2021 |
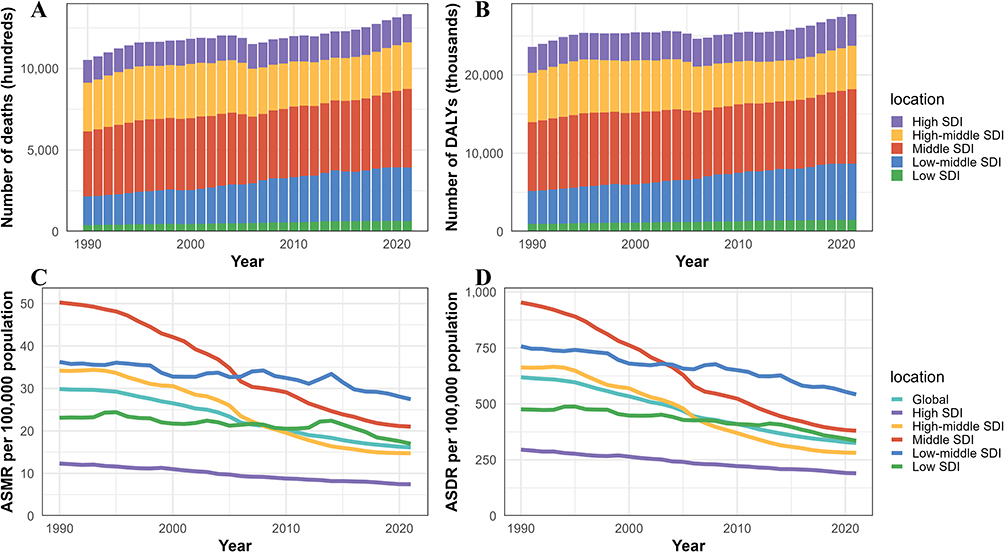 |
Figure 1 The COPD burden attributable to smoking by SDI regions from 1990 to 2021. (A) deaths; (B) DALYs; (C) ASMR; (D) ASDR. Abbreviations: COPD, chronic obstructive pulmonary disease; SDI, Socio-demographic Index; ASMR, age-standardized mortality rate; EAPC, estimated annual percentage change; DALYs, disability-adjusted life years; ASDR, age-standardized DALYs rate. |
Regional Burden and Trends of Smoking-Related COPD
In 1990, the burden of smoking-related COPD was primarily concentrated in Middle and High-middle SDI region (Table 1 and Figure 1). By 2021, deaths and DALYs increased in all SDI regions except for the High-middle SDI region. The most substantial increase was observed in Low-middle SDI region, which rose to rank second, following Middle SDI region (Table 1 and Figure 1A and B). The highest ASMR and ASDR in 2021 were observed in Low-middle SDI region, with values of 27.47 (95% UI: 21.81–33.52) and 542.25 (95% UI: 432.86–659.20) per 100,000 population, respectively (Table 1 and Figure 1C and D). From 1990 to 2021, the EAPCs of ASMR were negative in all SDI regions. The most pronounced decline was observed in High-middle SDI region, with EAPC of −3.30 (95% CI: −3.53 to −3.07) (Table 1).
Among the 21 GBD regions, both in 1990 and 2021, East Asia and South Asia exhibited a substantially higher burden of COPD attributable to smoking compared to other regions (Table 1 and Figure 2A and B). In 2021, East Asia reported the highest deaths (5,757 hundred; 95% UI: 4,272–7,285) and DALYs (10,446 thousand; 95% UI: 8,000–12,958), followed by South Asia with 3,703 (95% UI: 2,875–4,588) hundred deaths and 8,051 (95% UI: 6,283–9,895) thousand DALYs. With respect to ASR, East Asia exhibited the highest ASMR and ASDR in 1990 (Table 1). By 2021, East Asia maintained its position as the region with the highest ASMR, while South Asia surpassed East Asia in terms of ASDR. Conversely, Andean Latin America consistently exhibited the lowest burden in both 1990 and 2021, across all indicators (Table 1). The EAPCs for both ASMR and ASDR were negative in all GBD regions. East Asia demonstrated the most significant decrease in ASDR, exhibiting an EAPC of −4.09 (95% CI: −4.25 to −3.93). This was followed by Eastern Europe (Table 1).
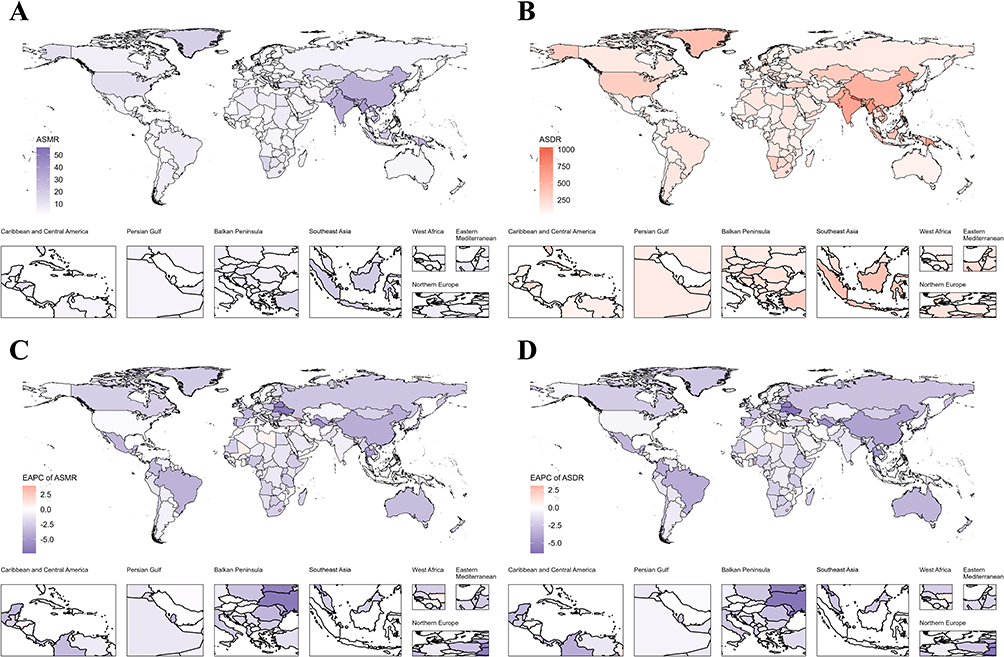 |
Figure 2 The burden of COPD attributable to smoking for both sexes in 204 countries and territories. (A) ASMR in 2021; (B) ASDR in 2021; (C) The EAPC of ASMR between 1990 and 2021; (D) The EAPC of ASDR between 1990 and 2021. Abbreviations: COPD, chronic obstructive pulmonary disease; ASMR, age-standardized mortality rate; EAPC, estimated annual percentage change; ASDR, age-standardized disability-adjusted life years rate. |
National Burden and Trends of Smoking-Related COPD
With respect to national burden, China and India had the highest smoking-related COPD deaths and DALYs in 1990 and remained consistent in 2021 (Tables S2 and S3). In 2021, DALYs reached 10,187 (95% UI: 7,747–12,691) thousand in China and 6,682 (95% UI: 5,199–8,310) thousand in India (Table S3). Relative to 1990, China experienced a 9.4% decrease in DALYs, whereas India showed an 82.7% increase. For ASMR, China had the highest ASMR in 1990 (96.37 per 100,000; 95% UI: 77.06–115.04), followed by Nepal (88.39 per 100,000; 95% UI: 61.21–118.16) and Myanmar (73.92 per 100,000; 95% UI: 53.54–97.36). By 2021, Nepal ranked first in ASMR, followed by Myanmar and Kiribati (Table S4 and Figure 2A). ASDR showed a largely similar ranking pattern (Table S5). Most countries exhibited declines in ASMR and ASDR over time (Table S1 and Figure 2C and D). The largest reductions were observed in Singapore, Ukraine, and Belarus, whereas Georgia experienced the largest increase, indicating substantial heterogeneity in global progress (Tables S6 and S7).
Patterns of Smoking-Related COPD by Sex and Age
Burden differed by sex throughout 1990 to 2021, with males consistently exceeding females in deaths and DALYs (Table 1 and Figure 3A and B). Male deaths increased from 8,570 (95% UI: 7,184–10,049) hundred to 11,029 (95% UI: 8,710–13,251) hundred. Female deaths rose modestly from 1,967 (95% UI: 1,377–2,586) hundred to 2,320 (95% UI: 1,636–3,161) hundred. ASMR and ASDR decreased in both sexes, with steeper declines in females, as reflected by larger absolute EAPCs (Table 1). Age-specific patterns showed deaths peaked in the 75–79 age group and DALYs in the 70–74 age group, with both declining thereafter. In contrast, both the age-specific death rate and DALY rate continued to rise with age, reaching their highest levels in the 90–94 age group (Figure 3C and D). This discrepancy may reflect the composite nature of DALYs, which include both years of life lost and years lived with disability. Absolute DALYs may peak earlier because more individuals survive with substantial COPD-related health loss, whereas age-specific death and DALY rates continue to increase in the oldest age groups as frailty, disease severity, and mortality risk accumulate.
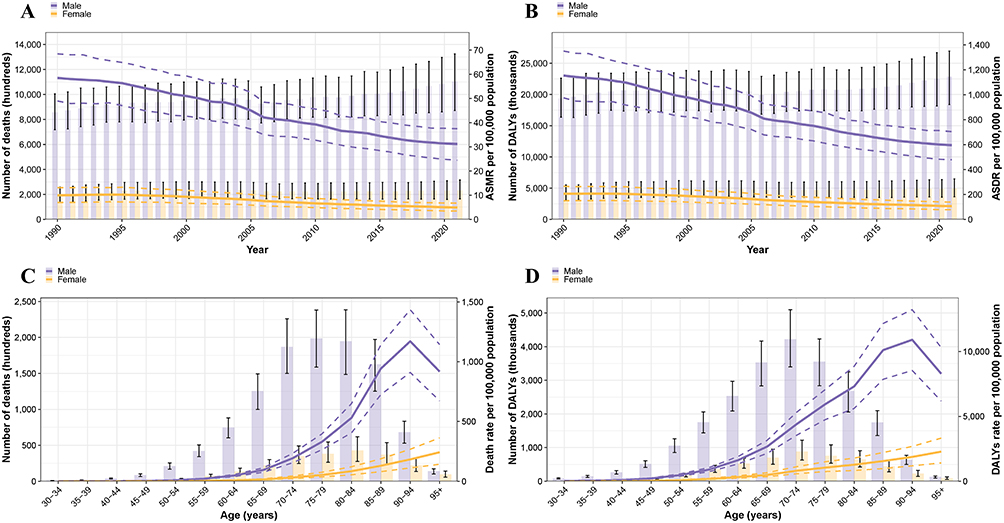 |
Figure 3 Temporal trends and age structure of the burden of smoking-attributable COPD by sex. (A) The number of deaths and ASMR from 1990 to 2021; (B) The number of DALYs and ASDR from 1990 to 2021; (C) The number of deaths and death rate in 2021; (D) The number of DALYs and DALYs rate in 2021. Bars correspond to the left y-axis and lines correspond to the right y-axis in all panels. Black error bars and dashed lines indicate 95% uncertainty intervals. Abbreviations: COPD, chronic obstructive pulmonary disease; ASMR, age-standardized mortality rate; DALYs, disability-adjusted life years; ASDR, age-standardized DALYs rate. |
Frontier Analysis and Decomposition Analysis
Frontier analysis illustrated each location’s distance to the efficiency frontier for ASDR given its SDI from 1990 to 2021. The distance generally decreased with higher SDI, implying that low SDI countries still have more potential for improvement (Figure 4A). In 2021, among lower-SDI countries, Somalia, Burkina Faso, Niger, Ethiopia, and Benin were closest to the frontier, indicating relatively strong performance at their development level. In contrast, among the countries with higher SDI, Denmark, the United States, the United Kingdom, the Netherlands, and Belgium are the furthest from the frontier, suggesting more room for reduction than expected for their SDI. The 15 most distant locations included Nepal, Kiribati, Myanmar, Papua New Guinea, North Korea, and others (Figure 4B).
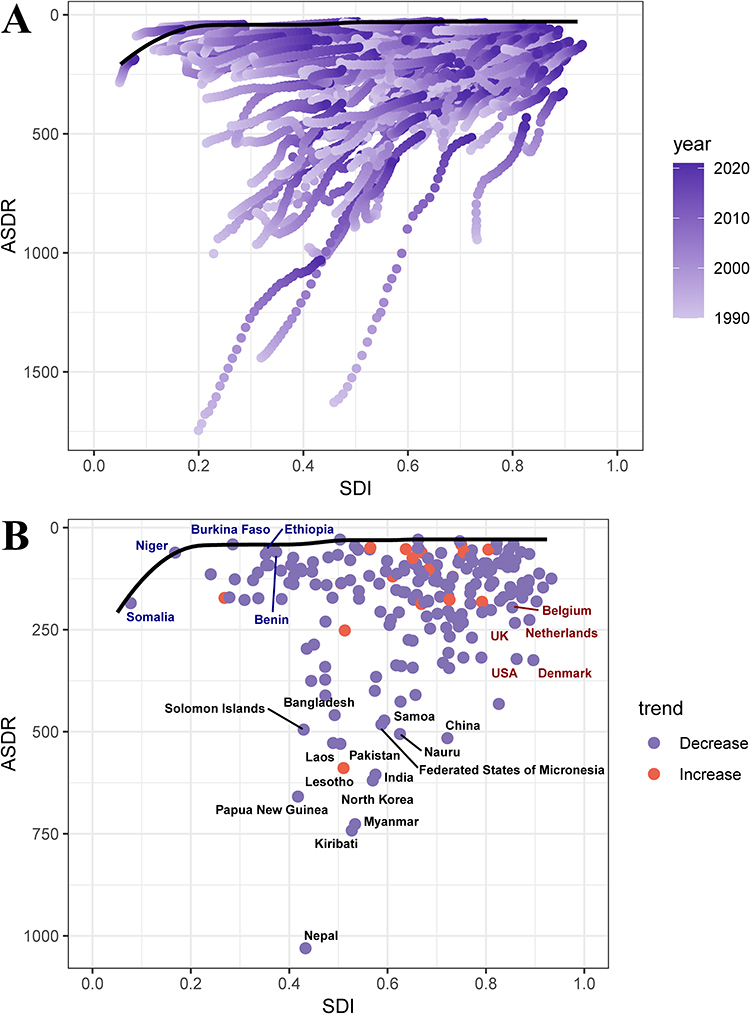 |
Figure 4 Frontier analysis of the relationship between the SDI and ASDR for smoking-attributable COPD. (A) Temporal shift from 1990 to 2021, with color gradients (light to dark purple) indicating changes over time; (B) Cross-sectional analysis in 2021, where each point represents a country or region. The black line denotes the efficiency frontier, representing the lowest theoretically attainable ASDR at a given SDI level. Country names in black highlight the 15 countries with the largest deviations from the frontier. Names in blue denote low-SDI countries with minimal deviation, while names in red represent high-SDI countries with substantial deviation. The color of each point reflects the direction of ASDR change from 1990 to 2021: purple indicates a decrease, and red indicates an increase. Abbreviations: SDI, Socio-demographic Index; ASDR, age-standardized disability-adjusted life years rate; COPD, chronic obstructive pulmonary disease. |
Decomposition analysis revealed that global DALYs increased by 4194 thousand between 1990 and 2021. Population growth and population ageing contributed increases of 17,521 thousand and 4,978 thousand DALYs, respectively, whereas epidemiological changes reduced DALYs by 18,305 thousand. Relative to the overall net increase, these corresponded to contributions of 417.74%, 118.70%, and −436.43%, respectively (Table S8). These large relative percentages reflect the fact that the absolute contributions of the individual components were much larger than the final net change, because positive and negative effects offset one another. Ageing had a positive impact in all SDI regions, except Low SDI region. Population growth was positive in all five SDI regions. Conversely, epidemiological changes offset increases in global DALYs, a pattern that was generally consistent across SDI strata. All three components had the largest impacts in Middle SDI, underscoring this stratum as a priority for targeted interventions (Table S8 and Figure 5).
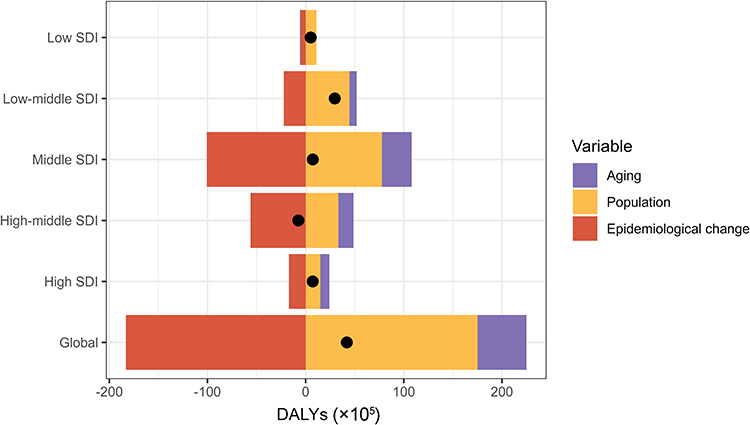 |
Figure 5 Decomposition analysis of changes in smoking-attributable COPD DALYs from 1990 to 2021. The decomposition, based on absolute DALY (×105) counts, includes contributions from population ageing, population growth, and epidemiological changes. Positive values indicate an increase in DALYs due to the respective component, while negative values represent a reduction. Black dots represent the net overall change contributed by all three components combined. Abbreviations: COPD, chronic obstructive pulmonary disease; DALYs, disability-adjusted life years; SDI, Socio-demographic Index. |
Future Projections of Smoking-Related COPD Burden
The BAPC model projected continued decline in smoking-related COPD burden over the next 19 years (Figure 6). By 2040, ASMR is predicted to decline to 11.62 per 100,000 population and ASDR to 240.32 per 100,000 population (Tables S9 and S10). By sex, ASDR in males is estimated to decrease by 23.56%, while females are projected to experience a 34.50% decline, indicating a greater relative improvement in women.
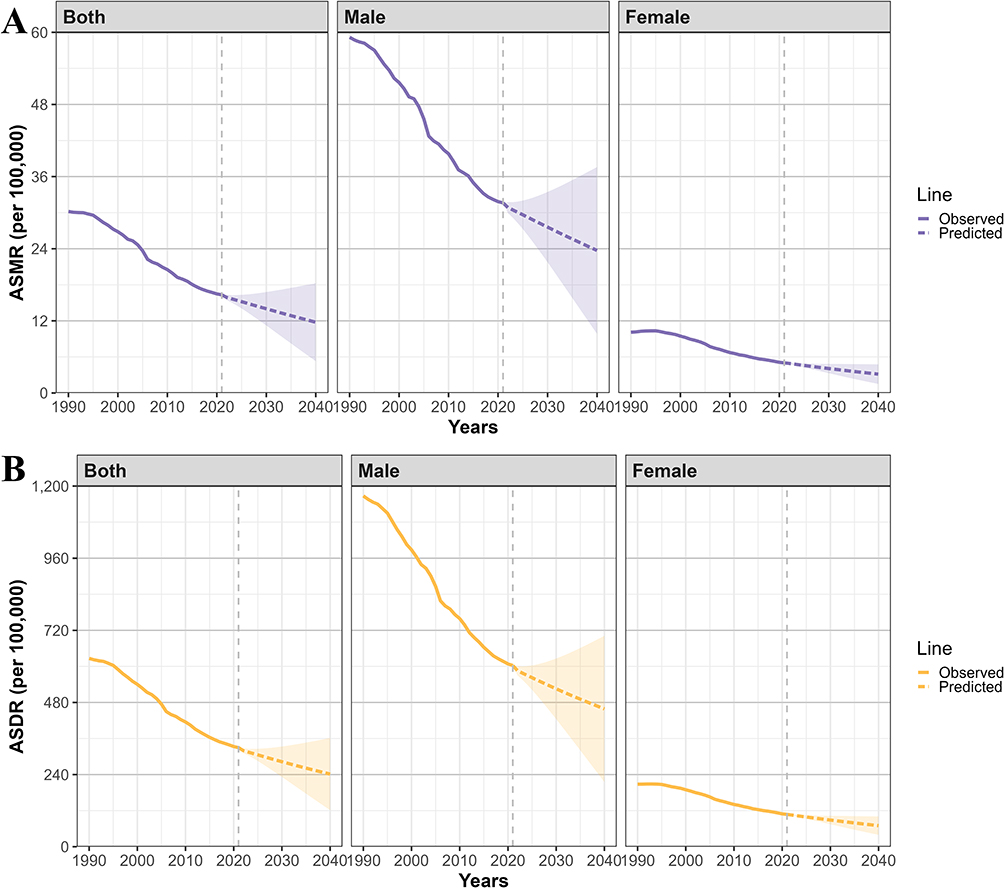 |
Figure 6 Future forecasts of global burden of COPD attributable to smoking from 2022 to 2040 based on the BAPC model. (A) ASMR; (B) ASDR. Abbreviations: COPD, chronic obstructive pulmonary disease; BAPC, Bayesian age-period-cohort; ASMR, age-standardized mortality rate; ASDR, age-standardized DALYs rate; DALYs, disability-adjusted life years. |
In the back-casting validation, the MAPE values for ASMR and ASDR across both sexes, males, and females were all below 10% (Table S11), indicating reasonable agreement between predicted and GBD-observed values.
Discussion
COPD is one of the leading causes of morbidity and mortality worldwide. Smoking is the primary modifiable risk factor for COPD. Despite sustained declines in ASMR and ASDR for smoking-attributable COPD since 1990, absolute deaths and DALYs increased. Decomposition analysis attributed this divergence primarily to demographic change, population growth and population ageing. Marked heterogeneity by development level, geography, sex, and age underscores the need for context-specific prevention and control strategies.
A previous GBD study assessed the burden of smoking-related COPD and reported declining ASDR in nearly all SDI regions. Although the authors did not explicitly state the global trend, the figures in their report indicate a downward trajectory.17 Our findings are consistent with this pattern, showing a continued decline in the global ASDR of smoking-related COPD between 1990 and 2021. This study also noted that the burden of smoking-related COPD was greater in males and increased with age, peaking at 85–89 years. Similarly, our study found that males experienced a substantially higher burden. However, we observed that the global DALY rate peaked later, at 90–94 years. This variation may be due to differences in the study period, data updates, and methodological approaches. Compared with earlier studies, our analysis incorporates the most recent data and provides a more nuanced assessment by incorporating advanced analytical approaches, including BAPC modeling and decomposition analysis, providing a more up-to-date and comprehensive view of global and regional trends.
At the global level, declining ASMR and ASDR are consistent with strengthened tobacco-control policies, earlier detection, and improvements in COPD management in many settings.27–32 Despite these global trends, Nepal’s ASMR and ASDR remained high in both 1990 and 2021, likely due to the persistent prevalence of smoking and the ongoing socioeconomic challenges experienced by the nation.33,34
Nevertheless, absolute burden increased, particularly in Low-middle and Middle SDI strata, where rapid demographic expansion and ageing offset epidemiologic gains. These patterns align with the decomposition findings, in which population growth and ageing contributed positively to DALY changes, whereas epidemiologic change contributed negatively, suggesting real—but insufficient—progress against risk and disease severity. The results of the decomposition analysis further support this conclusion. Inadequate tobacco control measures, limited access to healthcare, and delays in COPD diagnosis and treatment may also contribute to the growing absolute burden in settings with limited resources.35
Although East Asia and South Asia have made notable strides toward lowering the burden of COPD, they still account for the highest numbers of deaths and DALYs globally. This persistent burden likely reflects the combined effects of sustained tobacco exposure, large and ageing populations, and continuing challenges in healthcare infrastructure, early diagnosis, and long-term disease management across countries in these regions.36 Non-smoking inhalational exposures, including biomass smoke in some settings, may also contribute to this regional heterogeneity.37 China and India illustrate these contrasting patterns. Although China has experienced a decrease in the number of DALYs related to smoking-attributable COPD in recent years, it continues to report the highest number of deaths and DALYs, which may partly reflect the impact of its large and ageing population. By contrast, India has experienced substantial increases in both deaths and DALYs, which may also be influenced by differences in smoking patterns and tobacco products, including bidi use in some settings, as well as persistent barriers to healthcare access and timely diagnosis.38–40 These findings suggest that further reductions in burden in these regions will require not only strengthened tobacco-control policies but also improved access to accurate diagnosis, spirometry-based assessment, and long-term chronic respiratory care.41,42
Sex- and age-specific patterns were stable and biologically plausible. Males bore higher burdens than females across outcomes, consistent with greater cumulative smoking exposure in many settings.43 Burden increased with age, with DALYs peaking in the 70–74 age group and rates (death/DALY rate) peaking at older ages, reflecting the combined effects of cumulative exposure, age-related lung function decline, and comorbidity.44,45 These findings reinforce the need to intensify cessation among men, while expanding early detection and comprehensive, life-course COPD care for ageing populations. The projected greater relative decline in ASDR among females than among males by 2040 should, however, be interpreted cautiously. This projected pattern may not be uniform across all settings, as smoking trajectories among women have not improved consistently across populations and periods. Given the long latency between smoking initiation and COPD onset, this pattern may reflect sex-specific differences in historical smoking uptake, cessation, and cumulative exposure rather than immediate changes in current smoking behavior.46,47 In addition, because the BAPC model incorporates cohort effects, the projected declines may be consistent with more favorable smoking histories in later-born cohorts in some settings, whereas older cohorts with heavier cumulative exposure may continue to sustain a substantial burden.48,49
The frontier analysis indicates that the burden of COPD attributable to smoking generally decreases with rising levels of socioeconomic development. However, certain countries exhibit a discernible discrepancy between their observed burden and the expected levels based on the SDI. Such discrepancies suggest that socioeconomic development alone does not fully explain variation in smoking-attributable COPD burden. Countries located close to the frontier may not necessarily represent optimal performance, because lower observed burden could also reflect underdiagnosis, incomplete ascertainment, or limited diagnostic capacity in some settings.50,51 Conversely, high-SDI countries that remain well above the theoretical minimum may reflect not only the legacy effects of historical smoking exposure and population ageing,15,44,52,53 but also differences in healthcare-system performance, early detection, and long-term disease management. In addition, co-exposures such as biomass fuel smoke may contribute to COPD burden in ways not fully captured by an SDI-based frontier framework.37 These findings suggest that sustained tobacco control should be complemented by stronger case finding, spirometry access, and chronic respiratory care, even in higher-SDI settings.
Decomposition analysis identified demographic transitions as the dominant drivers of smoking-attributable COPD burden: population ageing and growth continue to push deaths and DALYs upward, only partially offset by advances in prevention, diagnosis and treatment. The disproportionate impact in Middle SDI settings signals a critical inflection point, with demand from demographic change outpacing health-system capacity.54 Priority responses include sustained tobacco control, expanded early detection (risk-based case finding and spirometry) and accessible long-term management integrated into primary care. If effectively implemented at scale, these measures may help mitigate the future burden of tobacco-related COPD in these regions.
Several limitations of this study should be considered. First, reliance on GBD data introduces potential biases due to the limitations of model-based estimates, especially in regions with insufficient primary data.55 Second, the cross-sectional nature of some data limits our ability to establish causal relationships between smoking-related COPD burden and various demographic or regional factors. Third, although decomposition clarifies the direction and relative magnitude of demographic versus epidemiologic forces, unmeasured factors (eg, air pollution trends, occupational exposures, or care quality) may also influence trajectories. Fourth, smoking-attributable estimates in GBD are derived from a comparative risk assessment framework using fixed exposure–response functions,56 which may not fully capture heterogeneity in tobacco product types across settings, particularly in lower-income regions where products such as bidis, kreteks, or waterpipe are more common.
Conclusions
In conclusion, although the age-standardized burden of smoking-attributable COPD declined globally from 1990 to 2021, absolute deaths and DALYs continued to rise, particularly in Middle and Low-middle SDI settings where demographic expansion and ageing offset epidemiological gains. The burden remained disproportionately high in males and older adults, and some high-SDI settings still showed considerable room for further reduction relative to their level of development. Looking ahead, the burden is projected to continue declining through 2040. However, sustaining this progress will likely require stronger tobacco control, earlier detection, improved long-term COPD management, and better implementation of prevention strategies in settings facing the greatest demographic pressure.
Data Sharing Statement
The data utilized in this analysis are accessible to the public through the Global Health Data Exchange (GHDx) at http://ghdx.healthdata.org/gbd-results-tool.
Ethics
This study was based on publicly available, de-identified data from the Global Burden of Disease Study. According to institutional policy of Shandong First Medical University & Shandong Academy of Medical Sciences, ethical approval was not required.
Acknowledgments
We would like to express our profound gratitude to the collaborators of the Global Burden of Disease, Injuries, and Risk Factors Study 2021 for their invaluable contributions, as well as to the Institute for Health Metrics and Evaluation (IHME) for providing access to the GBD data. We gratefully acknowledge the funding assistance provided by the Student Research Training Program of Shandong First Medical University & Shandong Academy of Medical Sciences (No. 2024104390508; No. 2024104391194), and the College Student Research Training Program of Shandong Youth & Children of Academy Educational Sciences (No. 24SSR225; 24SSR310).
This paper has been uploaded to Research Square https://www.researchsquare.com/article/rs-7797060/v1 as a preprint.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received financial support from the Student Research Training Program of Shandong First Medical University & Shandong Academy of Medical Sciences (No. 2024104390508; No. 2024104391194), and College Student Research Training Program of Shandong Youth & Children of Academy Educational Sciences (No. 24SSR225; 24SSR310). The funding source had no involvement in the research’s conceptualization, data gathering, analysis, interpretation, or manuscript preparation.
Disclosure
All authors have declared no conflicts of interest in this work.
References
1. Labaki WW, Rosenberg SR. Chronic obstructive pulmonary disease. Ann Internal Med. 2020;173(3):Itc17–15. doi:10.7326/AITC202008040
2. Lareau SC, Fahy B, Meek P, Wang A. Chronic obstructive pulmonary disease (COPD). Am J Respir Crit Care Med. 2019;199(1):P1–p2. doi:10.1164/rccm.1991P1
3. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American college of physicians, American college of chest physicians, American thoracic society, and European respiratory society. Ann Internal Med. 2011;155(3):179–191. doi:10.7326/0003-4819-155-3-201108020-00008
4. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
5. Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Global Health. 2015;5(2):020415. doi:10.7189/jogh.05.020415
6. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
7. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
8. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
9. Pappas RS. Toxic elements in tobacco and in cigarette smoke: inflammation and sensitization. Metallomics. 2011;3(11):1181–1198. doi:10.1039/c1mt00066g
10. Lu W, Aarsand R, Schotte K, et al. Tobacco and COPD: presenting the world health organization (WHO) Tobacco Knowledge Summary. Respir Res. 2024;25(1):338. doi:10.1186/s12931-024-02961-5
11. Wang Z, Lin J, Liang L, et al. Global, regional, and national burden of chronic obstructive pulmonary disease and its attributable risk factors from 1990 to 2021: an analysis for the global burden of disease study 2021. Respir Res. 2025;26(1):2. doi:10.1186/s12931-024-03051-2
12. Momtazmanesh S, Moghaddam SS, Ghamari S-H. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
13. Reitsma MB, Kendrick PJ, Ababneh E. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the global burden of disease study 2019. Lancet. 2021;397(10292):2337–2360. doi:10.1016/S0140-6736(21)01169-7
14. Jeon J, Cao P, Fleischer NL, et al. Birth cohort‒specific smoking patterns by family income in the US. Am J Preventive Med. 2023;64(4 Suppl 1):S32–s41. doi:10.1016/j.amepre.2022.07.019
15. Wheaton AG, Liu Y, Croft JB, et al. Chronic obstructive pulmonary disease and smoking status - United States, 2017. MMWR Morb Mortal Wkly Rep. 2019;68(24):533–538. doi:10.15585/mmwr.mm6824a1
16. Chen L, Xiong H, Wen Q, et al. The role of active and passive smoking in chronic obstructive pulmonary disease and systemic inflammation: a 12-year prospective study in China. J Epidemiol Global Health. 2024;14(3):1332–1340. doi:10.1007/s44197-024-00290-w
17. Zou J, Sun T, Song X, et al. Distributions and trends of the global burden of COPD attributable to risk factors by SDI, age, and sex from 1990 to 2019: a systematic analysis of GBD 2019 data. Respir Res. 2022;23(1):90. doi:10.1186/s12931-022-02011-y
18. GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
19. GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2162–2203. doi:10.1016/S0140-6736(24)00933-4
20. Güder G, Brenner S, Angermann CE, et al. “GOLD or lower limit of normal definition? A comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study”. Respir Res. 2012;13(1):13. doi:10.1186/1465-9921-13-13
21. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
22. Xu C, Jiang C, Liu X, et al. Epidemiological and sociodemographic transitions in the global burden and risk factors for Alzheimer’s disease and other dementias: a secondary analysis of GBD 2021. Int J Equity Health. 2025;24(1):149. doi:10.1186/s12939-025-02530-2
23. Ferreira ML, De luca K, Haile LM. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(6):e316–e329. doi:10.1016/S2665-9913(23)00098-X
24. Hankey BF, Ries LA, Kosary CL, et al. Partitioning linear trends in age-adjusted rates. Cancer Causes Control. 2000;11(1):31–35. doi:10.1023/A:1008953201688
25. Chevan A, Sutherland M. Revisiting Das Gupta: refinement and extension of standardization and decomposition. Demography. 2009;46(3):429–449. doi:10.1353/dem.0.0060
26. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
27. Polednak AP. Trends in mortality from COPD in selected US States differing in tobacco control efforts. Copd. 2010;7(1):63–69. doi:10.3109/15412550903499514
28. Wu Y, Wang Z, Zheng Y, et al. Trends in hospital admissions for chronic obstructive pulmonary diseases after comprehensive tobacco control policies in Beijing, China. Nicotine Tobacco Res. 2022;24(12):1978–1984. doi:10.1093/ntr/ntac137
29. Chan KH, Xiao D, Zhou M, Peto R, Chen Z. Tobacco control in China. Lancet Public Health. 2023;8(12):e1006–e1015. doi:10.1016/S2468-2667(23)00242-6
30. Matera MG, Page CP, Calzetta L, Rogliani P, Cazzola M. Pharmacology and therapeutics of bronchodilators revisited. Pharmacol Rev. 2020;72(1):218–252. doi:10.1124/pr.119.018150
31. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/European respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
32. Taichman DB, Drazen JM. Making long-term oxygen therapy less burdensome. New Engl J Med. 2024;391(11):1050–1051. doi:10.1056/NEJMe2410129
33. Sreeramareddy CT, Ramakrishnareddy N. Association of adult tobacco use with household food access insecurity: results from Nepal demographic and health survey, 2011. BMC Public Health. 2017;18(1):48. doi:10.1186/s12889-017-4579-y
34. Sapkota T, Houkes I, Bosma H. Vicious cycle of chronic disease and poverty: a qualitative study in present day Nepal. Int Health. 2021;13(1):30–38. doi:10.1093/inthealth/ihaa016
35. Ghorpade D, Salvi S. Awareness of COPD in low-and middle-income countries and implications for treatment. Expert Rev Respiratory Med. 2024;18(9):721–733. doi:10.1080/17476348.2024.2400983
36. Tan WC. Trends in chronic obstructive pulmonary disease in the Asia-Pacific regions. Curr Opin Pulm Med. 2011;17(2):56–61. doi:10.1097/MCP.0b013e32834316cd
37. Hu G, Zhou Y, Tian J, et al. Risk of COPD from exposure to biomass smoke: a metaanalysis. Chest. 2010;138(1):20–31. doi:10.1378/chest.08-2114
38. Rana K, Goel S, Prinja S. An analysis of affordability of cigarettes and bidis in India. Indian J Tuberculosis. 2021;68s:S55–s59. doi:10.1016/j.ijtb.2021.08.020
39. Jindal SK, Aggarwal AN, Chaudhry K, et al. A multicentric study on epidemiology of chronic obstructive pulmonary disease and its relationship with tobacco smoking and environmental tobacco smoke exposure. Indian J Chest Dis Allied Sci. 2006;48(1):23–29.
40. Chawla NS. Unveiling the ABCs: identifying India’s healthcare service gaps. Cureus. 2023;15(7):e42398. doi:10.7759/cureus.42398
41. Rhee CK, Chau NQ, Yunus F, Matsunaga K, Perng DW. Management of COPD in Asia: a position statement of the Asian Pacific society of respirology. Respirology. 2019;24(10):1018–1025. doi:10.1111/resp.13633
42. Yu WC, Fu SN, Tai EL, et al. Spirometry is underused in the diagnosis and monitoring of patients with chronic obstructive pulmonary disease (COPD). Int J Chronic Obstr. 2013;8:389–395. doi:10.2147/COPD.S48659
43. Kodriati N, Pursell L, Hayati EN. A scoping review of men, masculinities, and smoking behavior: the importance of settings. Global Health Action. 2018;11(sup3):1589763. doi:10.1080/16549716.2019.1589763
44. Schneider JL, Rowe JH, Garcia-de-Alba C, Kim CF, Sharpe AH, Haigis MC. The aging lung: physiology, disease, and immunity. Cell. 2021;184(8):1990–2019. doi:10.1016/j.cell.2021.03.005
45. Ulldemolins A, Narciso M, Sanz-Fraile H, et al. Effects of aging on the biomechanical properties of the lung extracellular matrix: dependence on tissular stretch. Front Cell Develop Biol. 2024;12:1381470. doi:10.3389/fcell.2024.1381470
46. Menson KE, Coleman SRM. Smoking and pulmonary health in women: a narrative review and behavioral health perspective. Preventive Med. 2024;185:108029. doi:10.1016/j.ypmed.2024.108029
47. Dai X, Gakidou E, Lopez AD. Evolution of the global smoking epidemic over the past half century: strengthening the evidence base for policy action. Tobacco Control. 2022;31(2):129–137. doi:10.1136/tobaccocontrol-2021-056535
48. Okui T. An age-period-cohort analysis of the difference in smoking prevalence between urban and non-urban areas in Japan (2004-2019). Epidemiol Health. 2020;42:e2020072. doi:10.4178/epih.e2020072
49. Holford TR, Levy DT, McKay LA, et al. Patterns of birth cohort-specific smoking histories, 1965-2009. Am J Preventive Med. 2014;46(2):e31–37. doi:10.1016/j.amepre.2013.10.022
50. Diab N, Gershon AS, Sin DD, et al. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(9):1130–1139. doi:10.1164/rccm.201804-0621CI
51. Ho T, Cusack RP, Chaudhary N, Satia I, Kurmi OP. Under- and over-diagnosis of COPD: a global perspective. Breathe. 2019;15(1):24–35. doi:10.1183/20734735.0346-2018
52. Pallin DJ, Espinola JA, Camargo CA. US population aging and demand for inpatient services. J Hospital Med. 2014;9(3):193–196. doi:10.1002/jhm.2145
53. Hinchliff S. Ageing and sexual health in the UK: how should health psychology respond to the challenges? J Health Psychol. 2009;14(3):355–360. doi:10.1177/1359105308101673
54. GBD 2016 Healthcare Access and Quality Collaborators. Measuring performance on the healthcare access and quality index for 195 countries and territories and selected subnational locations: a systematic analysis from the global burden of disease study 2016. Lancet. 2018;391(10136):2236–2271. doi:10.1016/S0140-6736(18)30994-2
55. Wu A-M, Cross M, Elliott JM. Global, regional, and national burden of neck pain, 1990-2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2024;6(3):e142–e155. doi:10.1016/S2665-9913(23)00321-1
56. GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1923–1994. doi:10.1016/S0140-6736(18)32225-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COPD Risk Factor Profiles in General Population and Referred Patients: Potential Etiotypes
Lee JH, Kim S, Kim YJ, Lee SW, Lee JS, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2509-2520
Published Date: 9 November 2023
Global, Regional, and National Burden of COPD Attributable to Occupational Particulate Matter, Gases, and Fumes, 1990–2019: Findings from the Global Burden of Disease Study 2019
Su X, Gu H, Li F, Shi D, Wang Z
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2971-2983
Published Date: 12 December 2023
Quantitative Assessment Characteristics of Small Pulmonary Vessel Remodelling in Populations at High Risk for COPD and Smokers Using Low-Dose CT
Pu Y, Zhou X, Zhang D, Guan Y, Xia Y, Liu S, Fan L
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:51-62
Published Date: 6 January 2024
Risk and Protective Factors of COPD Among Smokers: A Cross-Sectional Study Using NHANES Database
Guo X, Luo Q, Chen D, Lin H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1027-1038
Published Date: 11 April 2025
Chronic Marijuana Use and Chronic Obstructive Pulmonary Disease: A Case Report
Ostertag BS, Hendrickson KW
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2305-2309
Published Date: 7 July 2025