Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Risk and Protective Factors of COPD Among Smokers: A Cross-Sectional Study Using NHANES Database
Authors Guo X ![]() , Luo Q, Chen D, Lin H
, Luo Q, Chen D, Lin H ![]()
Received 1 August 2024
Accepted for publication 22 March 2025
Published 11 April 2025 Volume 2025:20 Pages 1027—1038
DOI https://doi.org/10.2147/COPD.S489581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Xuequn Guo,1,* Qiu Luo,2,* Dongdong Chen,1 Hongsheng Lin1
1Department of Respiratory Medicine, Quanzhou First Hospital Affiliated to Fujian Medical University, Quanzhou, Fujian, 362000, People’s Republic of China; 2Department of Emergency Medicine, Quanzhou First Hospital Affiliated to Fujian Medical University, Quanzhou, Fujian, 362000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuequn Guo, Department of Respiratory Medicine, Quanzhou First Hospital Affiliated to Fujian Medical University, No. 250 East Street, Quanzhou, Fujian, 362000, People’s Republic of China, Email [email protected]
Purpose: Smoking plays a significant role in the pathogenesis of chronic obstructive pulmonary disease (COPD), underscoring the importance of smoking cessation. Nevertheless, not all smokers who do not quit will necessarily develop COPD. This study aimed to examine the risk and protective factors associated with COPD among individuals who smoke.
Patients and Methods: The study included a cohort of 2619 adult smokers with lung function data, whose demographic characteristics, health status, lifestyle behaviors, and dietary patterns were examined using T-tests, Chi-square tests, and logical analysis.
Results: Among the study participants, 441 individuals were identified as having COPD by analyzing pulmonary function data. Advanced age (p< 0.001), low body mass index (BMI, p< 0.001), ethnicity (p=0.019), and comorbid asthma (p< 0.001) were found to be statistically correlated with the presence of COPD. Additionally, a higher intake of fruits and vegetables (p=0.026) was shown to have a beneficial impact. After considering factors related to type 2 inflammation, nutrient intake from vegetables and fruits, and other variables, it was observed that vitamin C (p< 0.001) exhibited a protective effect against COPD in smokers. Additionally, advanced age (p< 0.001), low BMI (p< 0.001), comorbid asthma (p< 0.001), and higher consumption of fruits and vegetables (p=0.032) remained significant independent risk factors for COPD in smokers. Furthermore, subgroup analysis revealed that COPD patients who consumed fewer fruits and vegetables had lower levels of vitamin C intake (p=0.004).
Conclusion: The findings of our study suggest that smokers who are older, have a lower BMI, and comorbid asthma are at an increased risk of developing COPD. Conversely, higher consumption of fruits and vegetables, as well as increased intake of vitamin C, may help reduce this risk. Additionally, our results indicate that among smokers with lower fruit and vegetable intake, COPD patients tend to have lower levels of vitamin C consumption.
Keywords: smoking, chronic obstructive pulmonary disease, fruits and vegetables, vitamin C, nutrition, oxidation
Introduction
Chronic obstructive pulmonary disease (COPD) is a persistent pulmonary inflammatory condition that can result in progressive and irreversible airway obstruction.1 It ranks as the third leading cause of mortality globally, with 3.23 million COPD-related deaths reported in 2019.2 Furthermore, COPD is associated with significant healthcare costs and frequent hospitalizations, in addition to its high mortality rate.3 It is also the leading cause of disability-adjusted life years, accounting for 3% of healthcare expenditures in Europe.4 In the northern region of Sweden, the prevalence of COPD among individuals aged 45 and above is reported to be 14%.5,6 Furthermore, both the prevalence and incidence of COPD were found to escalate with advancing age. It is noteworthy that the economic burden of healthcare for individuals suffering from severe COPD is tenfold greater compared to those with mild COPD.5
While smoking is commonly acknowledged as a significant factor in the development of COPD, research indicates that only a minority of persistent smokers, approximately 20–25%, will ultimately develop COPD.7,8 This suggests that additional factors may play a role in the pathogenesis of COPD among smokers. Previous studies have demonstrated a correlation between COPD development and environmental factors, lifestyle choices, and genetic predisposition, although these analyses have typically included smoking as a confounding variable.8 Despite the widely recognized importance of smoking cessation for individuals with COPD in effectively managing the condition, there are still individuals who persist in smoking even after receiving a diagnosis of COPD.5 Research has indicated that cessation of smoking at various stages of life can attenuate the decline in forced expiratory volume in 1 second, as well as mitigate the associated risks of disability and mortality.9 Despite variations in tobacco control policies among nations, a significant portion of smokers continue to face challenges in achieving successful cessation, particularly in low- and middle-income countries.5,10 The aim of our study was to investigate the determinants influencing the progression of COPD in smokers, with the ultimate goal of averting COPD development in individuals facing challenges in quitting through the regulation or reduction of exposure to pertinent risk factors.
Materials and Methods
Study Sample
Data from the National Health and Nutrition Examination Survey (NHANES) database (2007–2012) was incorporated into the analysis. The NHANES database is a publicly available, nationally representative program of studies designed to assess the health and nutritional status of the population in the USA (https://www.cdc.gov/nchs/nhanes/index.htm), which combines personal interviews, physical examinations, and laboratory tests and approved by the National Center for Health Statistic’s Research Ethics Review Board.11 In this research, participants who were current smokers and had no prior diagnosis of COPD were included. Current smoking was determined by positive responses to smoking questionnaires (“Have you smoked at least 100 cigarettes in your lifetime?” and “Do you currently smoke cigarettes?”). Exclusion criteria encompassed individuals under the age of 18, a history of COPD diagnosis, lack of pulmonary function data, and pulmonary function indicative of obstructive ventilation dysfunction that improved with bronchodilation testing. More details are shown in Figure 1.
 |
Figure 1 Study flow. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Data Collection
Quantitative variables, such as age, gender, body mass index (BMI), lifestyle factors (including physical activity status, sleep status, and diet), comorbidities (such as asthma, congestive heart failure, hypertension, diabetes, etc.), and family history, were collected for analysis in the study. The main focus of our study was to determine the initial diagnosis of COPD. The initial diagnosis of COPD was determined by a FEV1/FVC ratio of less than 0.7 and a negative bronchodilation test result, in the absence of a previous COPD diagnosis.12 The previous COPD diagnosis was defined by affirmative responses to medical conditions questionnaires (“Has a doctor or other health professional ever told you that you have emphysema/chronic bronchitis?”). The asthma diagnosis was defined by affirmative responses to medical conditions questionnaires (“Has a doctor or other health professional ever told you that you have asthma?”).13 It is important to note that, in light of the absence of blood nutrient levels, particularly vitamin C, we opted to substitute the dietary nutrient intake data obtained from the day before and 3 to 10 days after the interview.
Statistical Analysis
Subjects were stratified based on their initial diagnosis of COPD, and statistical analyses were conducted using the Student’s t-test, Wilcoxon rank-sum test, or Kruskal–Wallis test for comparisons of continuous baseline characteristics. The Chi-square test was utilized for categorical data. Quantitative variables were presented as mean ± standard deviation (Mean ± SD) or median and quartile (M [Q1, Q3]), while qualitative variables were expressed as number and percentage (n [%]). Multivariate logistic analysis was initially utilized to identify the risk factors associated with the initial diagnosis of COPD, followed by a backward stepwise logistic analysis to confirm independent risk factors. It is noteworthy that, in comparison to multivariable logistic analysis, stepwise logistic analysis can eliminate irrelevant variables, identify significant variables, streamline the model, and mitigate the risk of overfitting. Then, markers of type 2 inflammation and correlative nutrient intake from fruits and vegetables were compared between subgroups with and without newly diagnosed COPD using a Kruskal–Wallis test. Subsequently, multivariate and backward stepwise logistic analyses were employed to identify significant variables related to risk factors for initial COPD diagnosis, type 2 inflammatory markers, and nutrient intake factors about fruits and vegetables. Ultimately, meaningful variables were discerned by categorizing fruit and vegetable intake into subgroups, which were analyzed using the Kruskal–Wallis test. Variance inflation factor (VIF) was taken to test collinearity between continuous variables, and VIF ≤ 5 was seen as non-collinearity.14 Stata 15.1 software (StataCorp, Texas, USA) was employed for the statistical analysis, and p < 0.05 was considered statistically significant.
Results
Following the application of the inclusion and screening criteria, a total of 2619 subjects were enrolled in the study, with 2178 failing to meet the criteria for initial diagnosis of COPD and 441 meeting.
The descriptive statistics were presented individually in Tables 1 and 2. Among smokers, individuals with COPD were found to be significantly older (p<0.001), more likely to be male (p=0.003), have a lower BMI (p<0.001), fewer family members (p<0.001), a higher ratio of family income to poverty guidelines (p=0.013), longer duration of smoking (p<0.001), smoke more cigarettes per month (p<0.001), more frequent exposed to second-hand smoke (p<0.001), and have close relatives diagnosed with asthma (p=0.027). Additionally, participants with coronary heart disease, hypertension, diabetes, hyperlipidemia, cerebrovascular disease, arthritis, cancer, and depression (p<0.050) were more prone to developing COPD. Additionally, a notable disparity in engagement with vigorous recreational activity (p<0.001) was noted between the non-initial COPD diagnosis and initial COPD diagnosis groups. Similar discrepancies were observed in engagement with moderate recreational activity (p=0.002), reduction in food intake (p<0.001), adherence to a low-calorie diet (p=0.022), adherence to a low-carbohydrate diet (p=0.010), generous water consumption (p<0.001), and increased intake of fruits and vegetables (p=0.010).
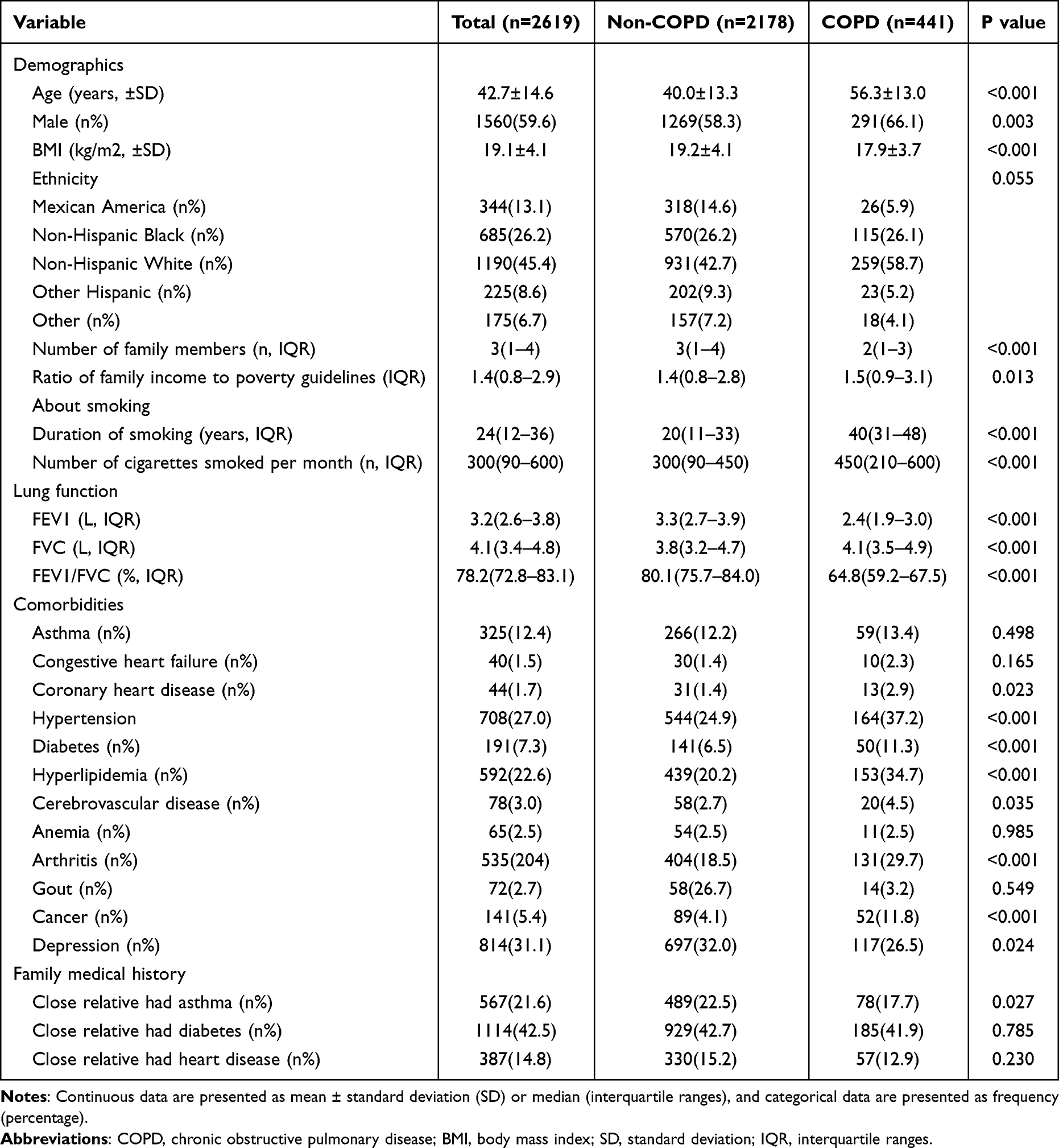 |
Table 1 Baseline Characteristics of Study Subjects |
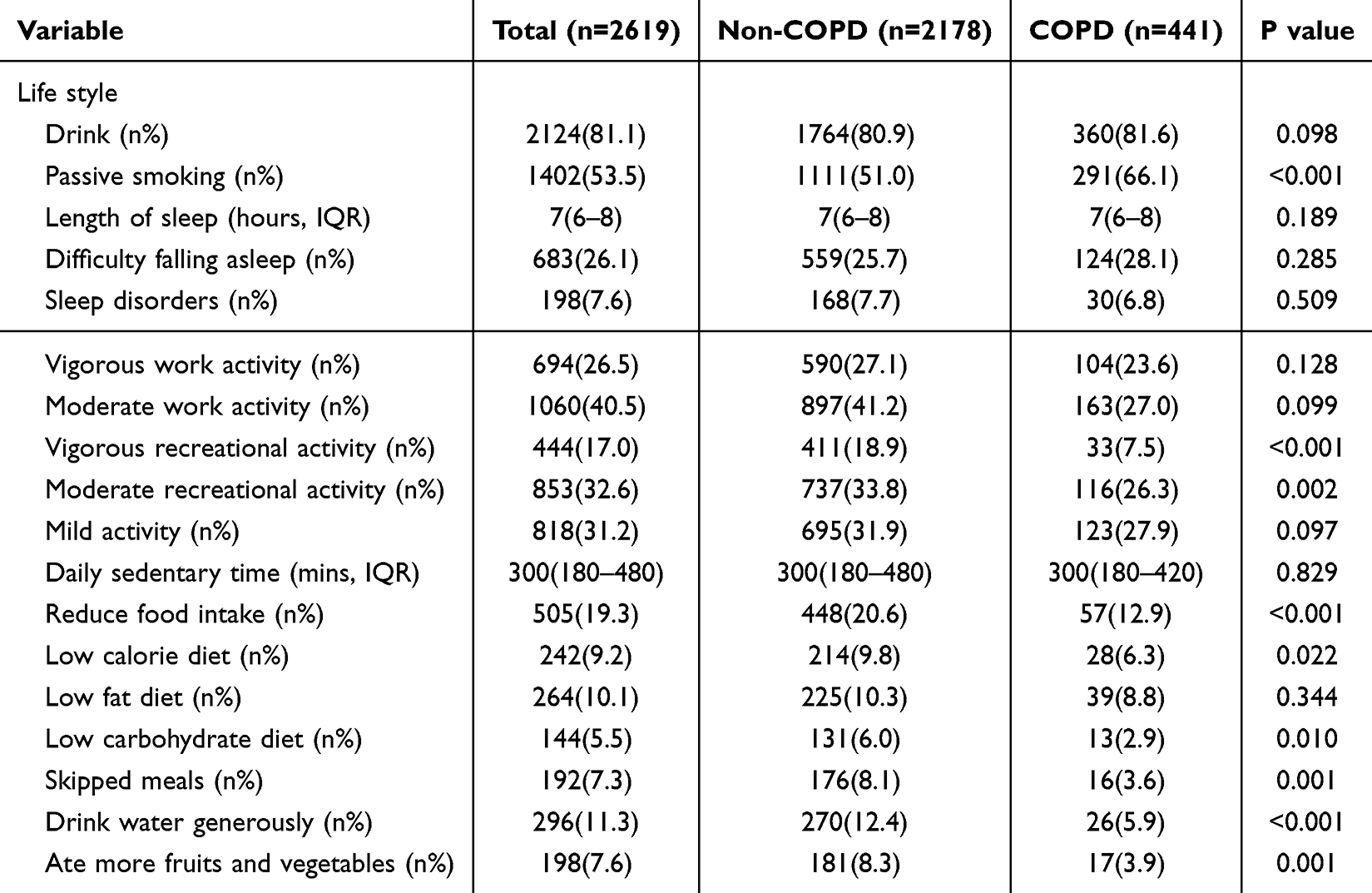 |
Table 2 Life Style of Study Subjects |
As presented in Table 3, the multivariate logistic model was conducted with age, gender, BMI, etc. identified as significant variables. The subsequent backward stepwise logistic analysis further confirmed age (p<0.001), BMI (p<0.001), ethnicity (p=0.019), asthma (p<0.001), and propensity for fruit and vegetable intake (p=0.026) as independent risk factors. Given the association of asthma and increased fruit and vegetable intake with the development of COPD in smokers, we conducted a comparison of eosinophilic counts and ratios, as well as nutrient intake indicators related to fruit and vegetable consumption, among subgroups to evaluate disparities in COPD development, as shown in Table 3. It was evident that individuals with COPD who smoke exhibited elevated eosinophilic counts (p=0.037) and higher dietary intake of vitamin B2 (p=0.002) and vitamin D (p=0.006), with decreased intake of vitamin C (p=0.002) and lycopene (p=0.007).
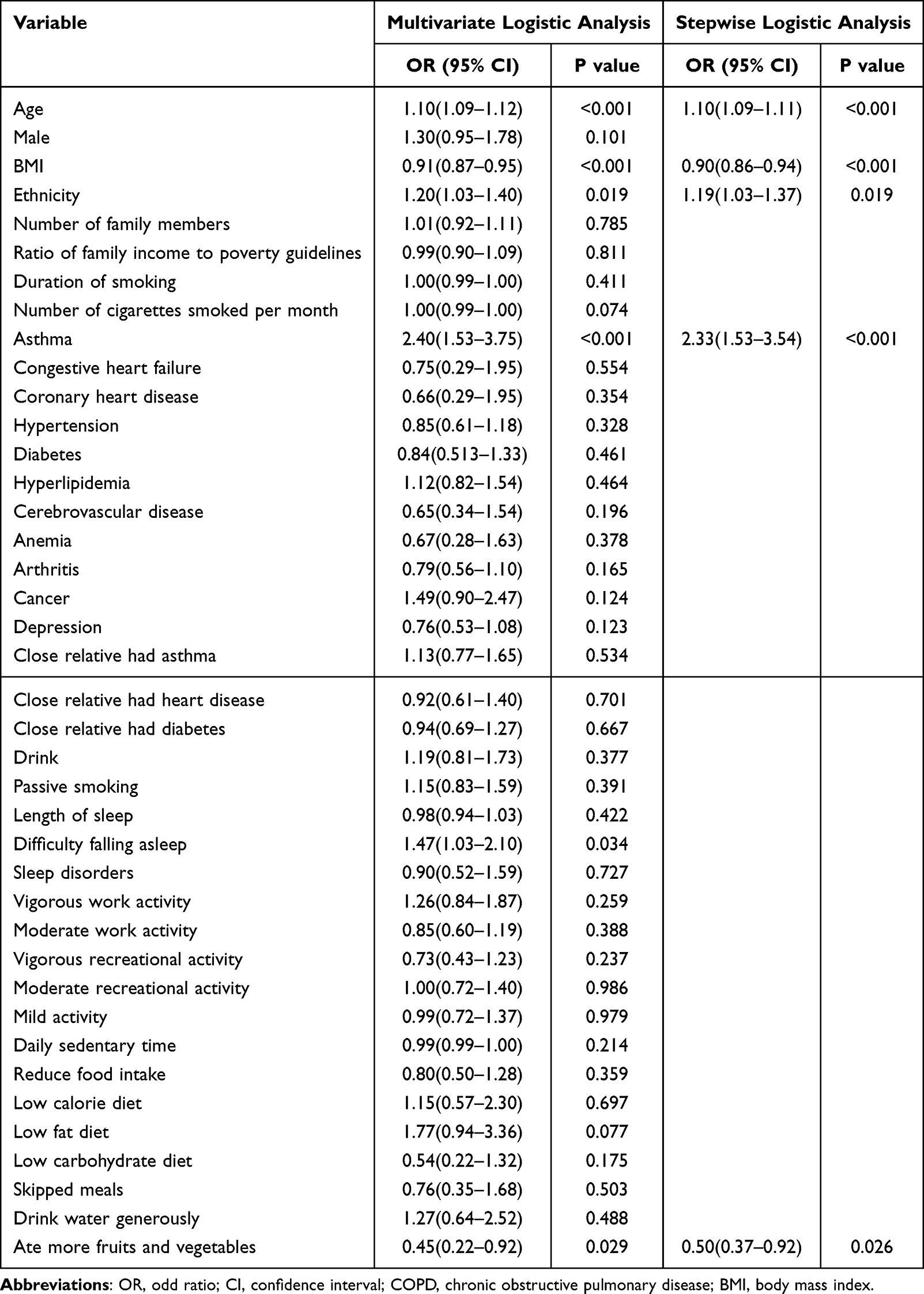 |
Table 3 Multivariate and Stepwise Logistic Analysis of Variables and COPD |
Subsequently, employing multivariate and backward stepwise logical analysis models, we proceeded to identify risk factors in Table 2 and markers of type 2 inflammatory factors and nutritional indicators in Table 4. The findings of our analysis indicate that vitamin C (p<0.001) has been identified as a significant independent risk factor for the progression of COPD in smokers, along with age (p<0.001), BMI (p<0.001), asthma (p<0.001), and propensity for fruit and vegetable intake (p=0.032), as illustrated in Table 5.
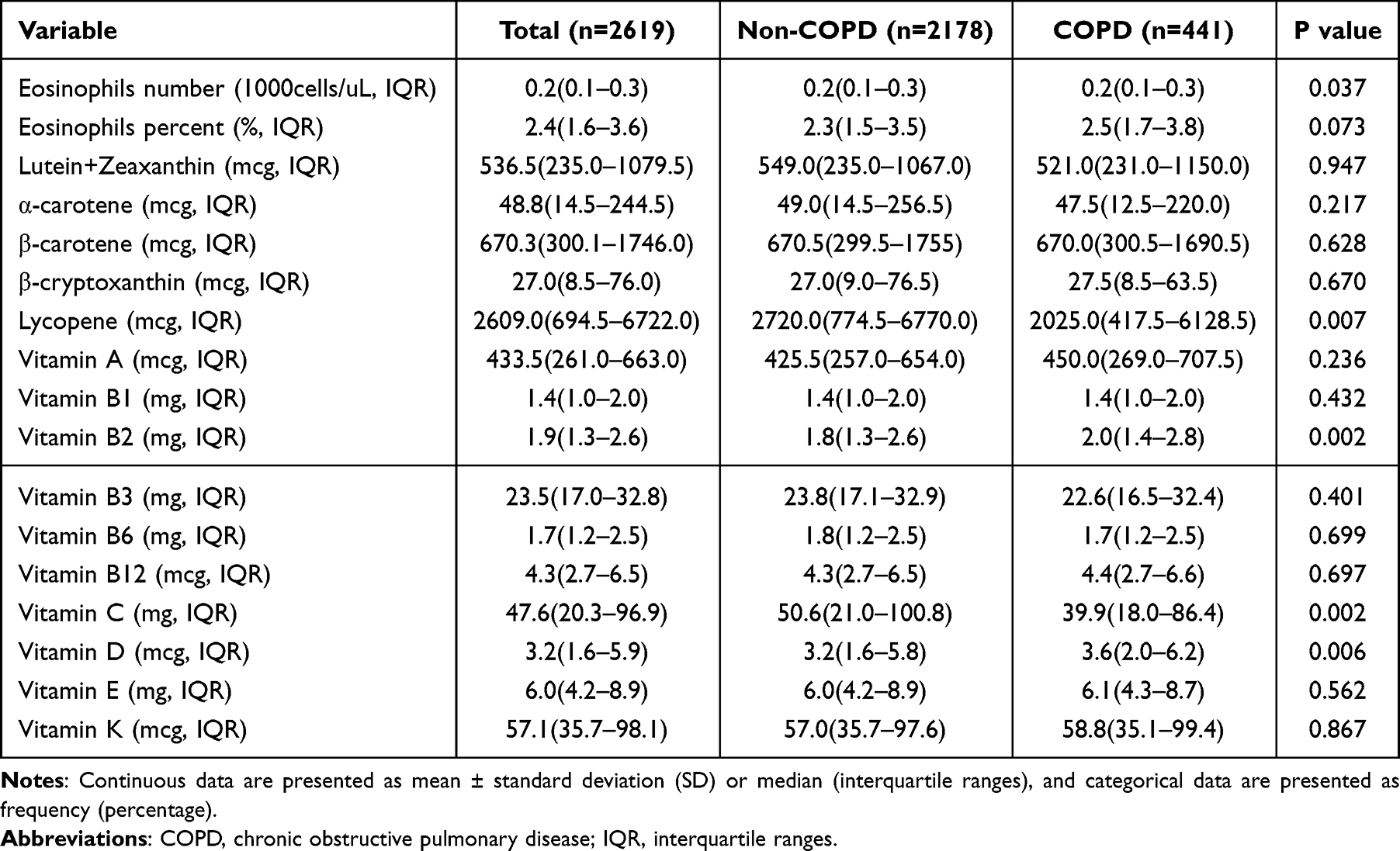 |
Table 4 Markers of Type 2 Inflammation and Micronutrient Status According to Fruits and Vegetables of Study Subjects |
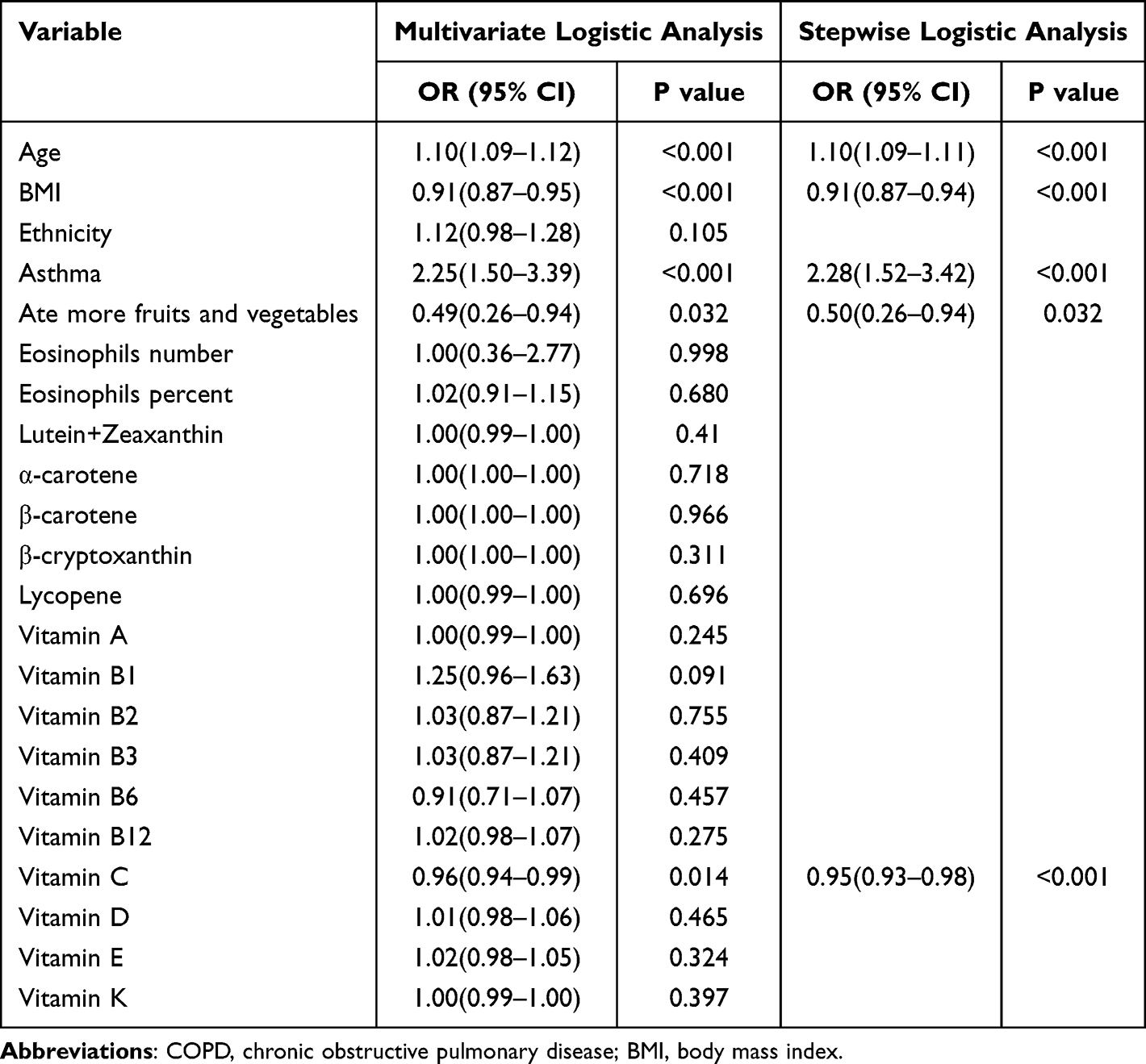 |
Table 5 Correlation Analysis of Markers of Type 2 Inflammation and Micronutrient Status and COPD by Independent Risk Factors |
Finally, in order to more intuitively determine the impact of intake of fruits and vegetables and vitamin C on whether smokers develop COPD, as in Table 6, we divided the samples into subgroups according to intake habits of fruits and vegetables. After comparison, it was found that regardless of whether smokers tended to eat more fruits and vegetables, elderly smokers were more likely to develop COPD (p<0.001), while asthma was the opposite (p>0.050). Among people who ate more fruits and vegetables, there was no difference in BMI and vitamin C intake between COPD individuals and non-COPD individuals (p>0.050). However, individuals with lower fruit and vegetable intake who developed COPD exhibited significantly lower BMI (p<0.001) and lower vitamin C intake levels (p=0.004).
 |
Table 6 Comparison of Risk Factors Between Subgroups Categorized Based on Their Consumption of Fruits and Vegetables |
Discussion
Our research investigated the determinants of COPD development in current smokers. Following an examination of lung function in 2619 persistent smokers without a prior COPD diagnosis, 441 individuals were identified as having COPD-compatible lung function. Subsequent statistical analysis revealed that advanced age, low BMI, and a history of asthma were associated with an increased likelihood of COPD development among smokers. Additionally, smokers who frequently consumed fruits and vegetables exhibited a lower prevalence of COPD. Additionally, the incidence of COPD was found to be influenced by ethnicity. Further analysis revealed that a higher intake of vitamin C serves as a protective factor against the development of COPD in smokers.
After extensive research findings, the notion that smoking is a significant factor in the onset and progression of COPD has become widely acknowledged.7,8,15 The reasons for certain individuals displaying resistance to the deleterious effects of smoking and not developing COPD remain unclear. Several studies have indicated that the frequency of daily smoking and the age of initiation of smoking are associated with lung function impairment and the onset of COPD.16–18 However, our study has found that neither the duration of smoke nor the monthly consumption of cigarettes among smokers are significant risk factors for the development of COPD. This phenomenon may be attributed to our focus on analyzing persistent smokers, a group that may have shared similar smoking histories, thereby potentially diminishing the impact of smoking-related variables in contrast to prior research. Additionally, the population under study may have predominantly originated from developed nations, where elevated per capita incomes could attenuate the influence of smoking-related factors.19 This conclusion demonstrates that, alongside smoking-related factors, other variables significantly influence the progression of COPD in individuals who continue to smoke.
Our study revealed a positive association between age and the development of COPD among smokers, even when accounting for smoking duration. Prior research has indicated that nearly half of older smokers are affected by COPD.20 This phenomenon may be attributed to cellular senescence and apoptosis, although the exact mechanism remains unclear. Some studies suggest that macrophage migration inhibition factor (MIF) may play a role in this process.21 MIF, a pleiotropic cytokine known for its anti-apoptotic and anti-senescence properties, was proved to be decreased in older smokers with COPD compared to older smokers without the disease.21
Prior research has demonstrated that the rate of decline in lung function is 0.98% per pack-year for men and 1.21% per pack-year for women, suggesting that female smokers are at a higher risk of experiencing a decline in lung function compared to male smokers. This disparity may contribute to the increased prevalence of COPD among women. The exact mechanism underlying this phenomenon remains unclear, but it is hypothesized that the smaller lung size of women in comparison to men may play a role.22 Our research did not identify a statistically significant gender disparity in the progression of COPD among smokers. This lack of difference may be attributed to the BMI as a mitigating factor, which helps to equalize variations in lung volume between males and females. Additionally, the findings may be influenced by the demographic composition of the study sample, which was drawn from the United States. The higher living standards and income levels in this population may contribute to women having a more favorable nutritional status compared to the global average.
Our research revealed that higher BMI was associated with a protective effect against COPD among smokers. Spelta et al documented a noteworthy protective effect of obesity against overall mortality in individuals with COPD, labeling it as the “obesity paradox”.23 Consistent with this finding, Tang et al illustrated that individuals with higher BMI had a reduced risk of COPD advancement and mortality compared to those within the normal BMI range.24 One potential hypothesis is that the decreased FEV1 observed in individuals with obesity may be attributed to restrictive ventilation dysfunction rather than obstructive, while another theory posits that elevated BMI could lead to an accumulation of abdominal fat mass, subsequently diminishing lung compliance.24
The 2022 GOLD report emphasizes the potential role of asthma as a risk factor for the progression to chronic airflow limitation and COPD, indicating that adults with asthma may face a significantly elevated risk of developing COPD compared to individuals without asthma, even after controlling for the impact of smoking.4 A study, involving 5176 adults aged 40 years and above, further corroborated these findings by identifying a history of asthma as the most consistently independent risk factor associated with COPD, irrespective of smoking habits.25 In the United States, Europe, and China, the prevalence of non-smoking-related COPD with asthma is estimated to be between 25–30%.26 In low- and middle-income countries with significant rural populations, such as India and South Africa, asthma may also play a role in increasing the risk of COPD, even in the absence of a clinical diagnosis.26 This association is likely due to the presence of airway inflammation in individuals with asthma, which is characterized by increased neutrophils and alterations in the extracellular matrix. This process, known as airway remodeling, shares common pathogenic mechanisms with COPD.27 Asthma-induced airway remodeling can result in chronic, irreversible airway obstruction and ultimately lead to irreversible obstructive airway changes, culminating in the development of COPD.27 Our research additionally indicates that individuals who smoke and have asthma are at an increased risk of developing COPD, regardless of eosinophil count and ratio, implying that type 2 inflammation, commonly linked to the advancement of irreversible airway damage in asthma, may not be a crucial factor.28
Our research also identified race as a factor in the development of COPD among smokers, however, statistical significance was not observed once type 2 inflammation-related factors and nutritional intake were considered. The impact of race on the initiation of COPD has been a subject of long-standing investigation. Park et al conducted a comparative analysis of COPD patients from Korea and the United States, revealing notable disparities in sociodemographic characteristics, clinical presentations, and comorbidities.29 The impact of race on the development of COPD may be attributed to genetic variances, as evidenced by Busch et al’s identification of genes implicated in disparate methylation patterns and Weighted Gene Co-expression Network Analysis (WGCNA) that could serve as potential mechanistic targets for susceptibility, exacerbation, and prognosis of COPD in individuals of African American descent.30
Our research findings support the notion that individuals who smoke and consume a higher quantity of fruits and vegetables have a decreased likelihood of developing COPD. This aligns with previous research, such as the study conducted by Kaluza et al, which demonstrated that a high daily intake of fruits and vegetables (≥5.3 servings) was linked to a 40% decrease in COPD risk among current smokers when compared to those with a lower intake of fruits and vegetables (<2 servings).31 Additionally, a meta-analysis conducted by Hai et al corroborated that higher consumption of fruits and vegetables was associated with a reduced risk of COPD in both smokers and non-smokers.32 The involvement of oxidative stress and inflammation in the pathogenesis of COPD may explain why smokers experience a more pronounced effect, while a higher intake of fruits and vegetables is significantly associated with lower levels of oxidative stress and inflammatory parameters, as well as increased antioxidant defense.31 Fruits and vegetables rich in vitamin A, vitamin C, vitamin D, vitamin E, and beta-carotene exhibit strong antioxidant effects that not only reduce oxidation levels but also mitigate inflammatory factors linked to the onset and exacerbation of COPD such as C-reactive protein and interleukin-6.33,34 Moreover, consumption of nitrate-rich vegetables has been linked to enhanced vascular function and lowered blood pressure, potentially benefiting pulmonary health by improving blood circulation and oxygen delivery to lung tissues.35 Furthermore, the dietary fiber present in fruits and vegetables may promote lung health by positively influencing gut microbiota composition, thereby affecting systemic inflammation and immune responses. The gut-lung axis represents a burgeoning field of study, with dietary fiber recognized for its advantageous effects on gut health, which may indirectly support pulmonary function and decrease the risk of COPD.36
After conducting a comprehensive analysis encompassing nutrients associated with type 2 inflammation and consuming fruits and vegetables, we discovered that vitamin C intake is a protective factor against COPD in smokers. Furthermore, it was observed that individuals with COPD who consumed fewer fruits and vegetables exhibited significantly lower levels of vitamin C intake. These analyses collectively suggest that an increased intake of vitamin C can potentially reduce the incidence of COPD among smokers, particularly those who consume limited amounts of fruits and vegetables. Park et al, through their study involving over 3000 samples, also found that vitamin C intake exerts a protective effect on COPD independent of smoking status.37 This conclusion has been corroborated by numerous studies.38,39 The underlying mechanism may be attributed to its potent ability to mitigate oxidative stress, thereby promoting collagen synthesis while restoring vascular endothelial growth factor levels and facilitating lung alveolar cell proliferation.37
A primary strength of our research lies in its utilization of a substantial sample size to investigate the risk and protective factors associated with the development of COPD among smokers. This study facilitates the identification of individuals at heightened risk for COPD, thereby enabling healthcare professionals to implement early detection and intervention strategies for those facing challenges in smoking cessation. Simultaneously, it is recommended to increase the consumption of fruits and vegetables and incorporate vitamin C supplementation, as these measures may mitigate the risk of developing COPD in individuals with a smoking history. Of course, the significance of smoking cessation as a strategy to prevent and enhance lung function in patients with COPD should be consistently underscored.1,40,41
However, our research is subject to limitations. Firstly, the data utilized in our study was sourced solely from the NHANES database, which comprises information gathered through a home interview and a mobile screening center (MEC) health examination. This reliance on a single data source may introduce inaccuracies and potentially compromise the objectivity of our findings. Secondly, the NHANES database only captures changes in each participant’s health status over a one-year period, thereby restricting the temporal scope of our study population. Furthermore, the nutritional intake data utilized in this study was derived from the participants’ dietary habits over a randomly selected two-day timeframe, as opposed to being obtained through direct blood collection. This methodological approach may introduce bias into the study’s findings. Additionally, the database limitations restricted the inclusion of key data related to type 2 inflammation, such as fractional exhaled nitric oxide (FeNO) and serum Immunoglobulin E (IgE) levels, thereby potentially diminishing the strength of our conclusions. Lastly, due to the constraints of the database, we lack data on e-cigarette usage, rendering the assessment of smoking status insufficiently comprehensive.
Our study revealed that among smokers, advanced age, low BMI, and the presence of asthma were identified as significant risk factors for developing COPD. Additionally, a higher consumption of fruits and vegetables along with increased intake of vitamin C demonstrated a potential reduction in the likelihood of COPD occurrence. Notably, individuals who consumed fewer fruits and vegetables exhibited a correlation between COPD diagnosis and lower levels of vitamin C intake. Our research contributes to the early detection of individuals with a higher prevalence of COPD among smokers and offers suggestions for smokers to mitigate their risk of developing COPD, potentially leading to a decrease in the incidence of COPD and a reduction in associated healthcare expenditures.
Data Sharing Statement
The data utilized in this study was obtained from the National Health and Nutrition Examination Survey (NHANES) database (Weblink: NHANES Questionnaires, Datasets, and Related Documentation (cdc.gov)). The datasets employed in the analysis are accessible from the corresponding author upon request.
Ethics Approval and Consent to Participate
The NHANES is a nationally representative program of studies that evaluates the health and nutritional status of non-institutionalized individuals in the United States through a combination of questionnaires and laboratory tests (https://www.cdc.gov/nchs/nhanes/index.htm). Approval for the NHANES was obtained from the Research Ethics Review Board of the National Center for Health Statistics, and all participants provided written consent for their involvement in the study. More details at https://www.cdc.gov/nchs/nhanes/participant.htm. The ethics committee of Quanzhou First Hospital Affiliated to Fujian Medical University has concluded that this analysis does not involve research on human subjects and therefore does not require approval from a human subjects review board.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. The Lancet. 2012;380(9859):2095–2128. doi:10.1016/s0140-6736(12)61728-0
2. Rana JS, Khan SS, Lloyd-Jones DM, Sidney S. Changes in mortality in top 10 causes of death from 2011 to 2018. J General Internal Med. 2020;36(8):2517–2518. doi:10.1007/s11606-020-06070-z
3. Kunutsor SK, Jae SY, Mäkikallio TH, Laukkanen JA. Cardiorespiratory fitness does not offset the increased risk of chronic obstructive pulmonary disease attributed to smoking: a cohort study. European J Epidemiol. 2022;37(4):423–428. doi:10.1007/s10654-021-00835-4
4. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. European Respiratory J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
5. Eklund B-M, Nilsson S, Hedman L, Lindberg I. Why do smokers diagnosed with COPD not quit smoking? - a qualitative study. Tobacco Induced Dis. 2012;10(1):17. doi:10.1186/1617-9625-10-17
6. Lindberg A, Bjerg-Bäcklund A, Rönmark E, Larsson L-G, Lundbäck B. Prevalence and underdiagnosis of COPD by disease severity and the attributable fraction of smoking. Respiratory Med. 2006;100(2):264–272. doi:10.1016/j.rmed.2005.04.029
7. King PT. Inflammation in chronic obstructive pulmonary disease and its role in cardiovascular disease and lung cancer. Clin Transl Med. 2015;4(1). doi:10.1186/s40169-015-0068-z
8. He Y, Qian DC, Diao JA, et al. Prediction and stratification of longitudinal risk for chronic obstructive pulmonary disease across smoking behaviors. Nature Communications. 2023;14(1). doi:10.1038/s41467-023-44047-8
9. Lua YHA, How CH, Ng CW. Smoking cessation in primary care. Singapore Med J. 2024;65(1):38–44. doi:10.4103/singaporemedj.SMJ-2022-034
10. Yang J, Hammond D, Driezen P, et al. The use of cessation assistance among smokers from China: findings from the ITC China survey. BMC Public Health. 2011;11(1). doi:10.1186/1471-2458-11-75
11. Romero-Martínez M, Shamah-Levy T, Cuevas-Nasu L, et al. Diseño metodológico de la Encuesta Nacional de Salud y Nutrición de Medio Camino 2016. Salud Pública de México. 2017;59(3, may–jun). doi:10.21149/8593
12. Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on covid-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
13. Reddel HK, Bacharier LB, Bateman ED, et al. Global Initiative for Asthma Strategy 2021: executive summary and rationale for key changes. Eur Respir J. 2022;59(1). doi:10.1183/13993003.02730-2021
14. Marcoulides KM, Raykov T. Evaluation of variance inflation factors in regression models using latent variable modeling methods. Educational and Psychological Measurement. 2018;79(5):874–882. doi:10.1177/0013164418817803
15. Willinger CM, Rong J, Tanriverdi K, et al. MicroRNA signature of cigarette smoking and evidence for a putative causal role of microRNAs in smoking-related inflammation and target organ damage. Circulation: Cardiovascular Genetics. 2017;10(5). doi:10.1161/circgenetics.116.001678
16. Rennard SI, Drummond MB. Early chronic obstructive pulmonary disease: definition, assessment, and prevention. The Lancet. 2015;385(9979):1778–1788. doi:10.1016/S0140-6736(15)60647-X
17. Chung C, Lee KN, Han K, Shin DW, Lee SW. Effect of smoking on the development of chronic obstructive pulmonary disease in young individuals: a nationwide cohort study. Frontiers in Medicine. 2023;10. doi:10.3389/fmed.2023.1190885
18. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. The Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
19. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. The Lancet Respiratory Medicine. 2022;10(5):497–511. doi:10.1016/s2213-2600(21)00506-3
20. He Y, Jiang B, Li LS, et al. Secondhand smoke exposure predicted COPD and other tobacco-related mortality in a 17-year cohort study in China. Chest. 2012;142(4):909–918. doi:10.1378/chest.11-2884
21. Sauler M, Leng L, Trentalange M, et al. Macrophage migration inhibitory factor deficiency in chronic obstructive pulmonary disease. Am J Physiol-Lung Cellular Mol Physiol. 2014;306(6):L487–L496. doi:10.1152/ajplung.00284.2013
22. Chen M, Li Y, Zhang D, Wu Y. Gender difference in the association between smoking and lung function: exploring the role of C-reactive protein as a mediating factor. Public Health. 2020;183:88–93. doi:10.1016/j.puhe.2020.03.030
23. Spelta F, Fratta Pasini AM, Cazzoletti L, Ferrari M. Body weight and mortality in COPD: focus on the obesity paradox. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity. 2017;23(1):15–22. doi:10.1007/s40519-017-0456-z
24. Tang Y, Zhang L, Zhu S, Shen M, Cheng M, Peng F. Associations between different body mass index and lung function impairment in Chinese people aged over 40 years: a multicenter cross-sectional study. BMC Pulmonary Med. 2024;24(1). doi:10.1186/s12890-024-02844-x
25. Tan WC, Sin DD, Bourbeau J, et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: results from the CanCOLD study. Thorax. 2015;70(9):822–829. doi:10.1136/thoraxjnl-2015-206938
26. Martinez CH, Mannino DM, Jaimes FA, et al. Undiagnosed obstructive lung disease in the United States. associated factors and long-term mortality. Annals of the American Thoracic Society. 2015;12(12):1788–1795. doi:10.1513/AnnalsATS.201506-388OC
27. Ulrik CS, Lange P. Decline of lung function in adults with bronchial asthma. Am J Respiratory and Critical Care Med. 1994;150(3):629–634. doi:10.1164/ajrccm.150.3.8087330
28. Maspero J, Adir Y, Al-Ahmad M, et al. Type 2 inflammation in asthma and other airway diseases. ERJ Open Research. 2022;8(3):00576–2021. doi:10.1183/23120541.00576-2021
29. Park HY, Lee H, Kang D, et al. Understanding racial differences of COPD patients with an ecological model: two large cohort studies in the US and Korea. Therapeutic Adv Chronic Dis. 2021;12. doi:10.1177/2040622320982455
30. Busch R, Qiu W, Lasky-Su J, Morrow J, Criner G, DeMeo D. Differential DNA methylation marks and gene comethylation of COPD in African-Americans with COPD exacerbations. Respiratory Research. 2016;17(1). doi:10.1186/s12931-016-0459-8
31. Kaluza J, Larsson SC, Orsini N, Linden A, Wolk A. Fruit and vegetable consumption and risk of COPD: a prospective cohort study of men. Thorax. 2017;72(6):500–509. doi:10.1136/thoraxjnl-2015-207851
32. Zhai H, Wang Y, Jiang W. Fruit and vegetable intake and the risk of chronic obstructive pulmonary disease: a dose-response meta-analysis of observational studies. BioMed Research International. 2020;2020(1):1–12. doi:10.1155/2020/3783481
33. Holt EM, Steffen LM, Moran A, et al. Fruit and vegetable consumption and its relation to markers of inflammation and oxidative stress in adolescents. Journal of the American Dietetic Association. 2009;109(3):414–421. doi:10.1016/j.jada.2008.11.036
34. Chen C, Yang T, Wang C. The dietary inflammatory index and early COPD: results from the national health and nutrition examination survey. Nutrients. 2022;14(14). doi:10.3390/nu14142841
35. van der Avoort CMT, Ten Haaf DSM, Bongers C, et al. Increasing nitrate-rich vegetable intake lowers ambulatory blood pressure in (pre)Hypertensive middle-aged and older adults: a 12-Wk randomized controlled trial. J Nutr. 2021;151(9):2667–2679. doi:10.1093/jn/nxab157
36. Frankenfeld CL, Hullar MAJ, Maskarinec G, et al. The gut microbiome is associated with circulating dietary biomarkers of fruit and vegetable intake in a multiethnic cohort. J Acad Nutr Diet. 2022;122(1):78–98. doi:10.1016/j.jand.2021.05.023
37. Park HJ, Byun MK, Kim HJ, et al. Dietary vitamin C intake protects against COPD: the Korea national health and nutrition examination survey in 2012. Int J Chronic Obstructive Pulmonary Dis. 2016;11:2721–2728. doi:10.2147/copd.S119448
38. Pirabbasi E, Shahar S, Manaf ZA, Rajab NF, Manap RA. Efficacy of ascorbic acid (Vitamin C) and/N-Acetylcysteine (NAC) Supplementation on nutritional and antioxidant status of male chronic obstructive pulmonary disease (COPD) patients. J Nutritional Sci Vitaminol. 2016;62(1):54–61. doi:10.3177/jnsv.62.54
39. Kodama Y, Kishimoto Y, Muramatsu Y, et al. Antioxidant nutrients in plasma of Japanese patients with chronic obstructive pulmonary disease, asthma‐COPD overlap syndrome and bronchial asthma. The Clinical Respiratory Journal. 2016;11(6):915–924. doi:10.1111/crj.12436
40. Pezzuto A, Ricci A, D’Ascanio M, et al. Short-Term Benefits of Smoking Cessation Improve Respiratory Function and Metabolism in Smokers. Int J Chron Obstruct Pulmon Dis. 2023;18:2861–2865. doi:10.2147/COPD.S423148
41. Pezzuto A, Tonini G, Ciccozzi M, et al. Functional benefit of smoking cessation and triple inhaler in combustible cigarette smokers with severe COPD: a retrospective study. J Clin Med. 2022;12(1):234. doi:10.3390/jcm12010234
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COPD Risk Factor Profiles in General Population and Referred Patients: Potential Etiotypes
Lee JH, Kim S, Kim YJ, Lee SW, Lee JS, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2509-2520
Published Date: 9 November 2023
Quantitative Assessment Characteristics of Small Pulmonary Vessel Remodelling in Populations at High Risk for COPD and Smokers Using Low-Dose CT
Pu Y, Zhou X, Zhang D, Guan Y, Xia Y, Liu S, Fan L
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:51-62
Published Date: 6 January 2024
Chronic Marijuana Use and Chronic Obstructive Pulmonary Disease: A Case Report
Ostertag BS, Hendrickson KW
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2305-2309
Published Date: 7 July 2025
Level of Awareness About Chronic Obstructive Pulmonary Disease Among Active Smokers
Al-Otaibi HM, Homoud MM, Alqarni MM, Alsobhi GJ, Al-Otaibi GZ, Alnahdi NA
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:580239
Published Date: 29 March 2026
Smoking-Attributable Burden of Chronic Obstructive Pulmonary Disease from 1990 to 2021: Temporal Trends and Evidence from the Global Burden of Disease Study
Ma T, Yue X, Rong S, Sun R, Wang J, Zheng X, Chen X, Sun R
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:599370
Published Date: 22 May 2026