Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
COPD Risk Factor Profiles in General Population and Referred Patients: Potential Etiotypes
Authors Lee JH ![]() , Kim S
, Kim S ![]() , Kim YJ
, Kim YJ ![]() , Lee SW
, Lee SW ![]() , Lee JS
, Lee JS ![]() , Oh YM
, Oh YM ![]()
Received 26 June 2023
Accepted for publication 1 November 2023
Published 9 November 2023 Volume 2023:18 Pages 2509—2520
DOI https://doi.org/10.2147/COPD.S427774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Jang Ho Lee,1 Sehee Kim,2 Ye-Jee Kim,2 Sei Won Lee,1 Jae Seung Lee,1 Yeon-Mok Oh1
1Department of Pulmonary and Critical Care Medicine, Asan Medical Centre, University of Ulsan College of Medicine, Seoul, Republic of Korea; 2Department of Clinical Epidemiology and Biostatistics, Asan Medical Centre, University of Ulsan College of Medicine, Seoul, Republic of Korea
Correspondence: Yeon-Mok Oh, Department of Pulmonary and Critical Care Medicine, University of Ulsan College of Medicine, Asan Medical Centre, 88 Olympic-Ro 43-Gil, Songpa-Gu, Seoul, 05505, Republic of Korea, Tel +82-2-3010-3136, Fax +82-2-3010-6968, Email [email protected]
Purpose: To identify the risk factors for chronic obstructive pulmonary disease (COPD) in view of potential etiotypes in a general population and referred COPD patients.
Patients and Methods: We performed a cross-sectional observational study utilizing two distinct datasets: a dataset of a general population including 2430 subjects with COPD from the Korea National Health and Nutrition Examination Survey (KNHANES) and another dataset of referral clinics including 579 patients with COPD from the Korean Obstructive Lung Disease (KOLD).
Results: The mean age of both groups was 67 years, and 71.2% and 93.8% were male in the COPD subjects from the KNHANES and the KOLD, respectively. The mean forced expiratory volume in 1 second of predicted value was 79.1% (KNHANES) and 55.4% (KOLD). The frequency of risk factors of cigarette smoking (C), infection (I), pollution (P), and asthma (A) was 54.6%, 9.4%, 10.7%, and 7.9%, respectively, in the KNHANES COPD subjects, and 88.4%, 26.6%, 41.6%, and 35.2%, respectively, in the KOLD COPD subjects. Risk factors were unidentified in 32.6% (KNHANES) and 3.1% (KOLD) of COPD subjects. Additionally, 14.1% and 66.2% of subjects with COPD had two or more risk factors in the KNHANES and KOLD, respectively.
Conclusion: The profiles of risk factors C, I, P, and A were identified and appeared to be different among the two COPD groups from a general population or referral clinics. In some of the COPD subjects, risk factors were not identified, so we should endeavour to find out unidentified COPD risk factors, especially in the general population.
Keywords: chronic obstructive pulmonary disease, etiotype, smoking, tuberculosis, asthma, pollutants
Introduction
Exposure to noxious particles or cigarette smoke has been traditionally regarded as an important cause of chronic obstructive pulmonary disease (COPD), one of the global, high-burden diseases.1 Although cigarette smoking is the most important etiology of COPD, several studies have been conducted in never-smoker COPD populations.2–5 In particular, the relationship between COPD and various risk factors not associated with exposure to noxious particles or gases led to a change in the definition of COPD with the development of the etiotype concept in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 update.6,7 These factors included previous pulmonary infection, exposure to biomass combustion or air pollutants, and asthma. Previous studies reported risk factors for COPD, excluding smoking.8–11 However, previous studies did not collectively evaluate these COPD risk factors of cigarette smoking, previous pulmonary infection, pollution exposure, or asthma. Asthma, in particular, was not seriously investigated as a risk factor for COPD in the aforementioned studies.
In this study, we therefore comprehensively analyzed the risk factors of subjects with COPD collectively using a nationwide general population dataset (the Korea National Health and Nutrition Examination Survey, KNHANES) and a well-established dataset of subjects with COPD (the Korean Obstructive Lung Disease cohort, KOLD) of referral clinics in South Korea.12,13 Additionally, we compared the prevalence of exposure to risk factors between subjects with and without COPD in a general population–the KNHANES.
Materials and Methods
COPD and Non-COPD Subjects
We extracted eligible subjects from two datasets: the KNHANES of a general population between January 01, 2015 and December 31, 2019 and the KOLD of referral clinics between June 01, 2005 and June 30, 2015. The KNHANES provides nationwide data of a general population in South Korea based on the stratified, multistage, cluster probability sampling considering the geographical area.14 From the data of the KNHANES, we selected COPD and non-COPD subjects who performed spirometry. Those who performed spirometry in the KNHANES were 40 years or older given the original design of the KNHANES. For this study, we defined subjects with COPD with the criteria of the pre-bronchodilator ratio of forced expiratory volume in 1 sec (FEV1) to forced vital capacity (FVC): <0.7; non-COPD subjects: FEV1/FVC ≥0.7.
In addition, we defined the subjects with COPD from the KOLD with the same spirometry criteria of pre-bronchodilator FEV1/FVC <0.7 and the physician diagnosis of COPD based on clinical findings of history, physical exam, and chest radiography. Although the KOLD had enrolled patients with COPD or/and asthma, those with asthma were excluded from the original KOLD data for this study. No data on subjects without COPD were available as the KOLD only enrolled patients with COPD or/and asthma.
Subject Characteristics and Spirometry
Subject characteristics were investigated, including age, sex, and body mass index (BMI), and FEV1 (L and % of predicted value) and FVC (L and % predicted value), and FEV1/ FVC ratio. Pulmonary function tests were conducted utilizing dry rolling seal Spirometer Model 2130 (Sensor Medics Corporation, Yorba Linda, CA, USA) and Vyntus Spiro (Care Fusion, San Diego, CA, USA) in the KNHANES and Vmax 22 (Sensor Medics, Yorba Linda, CA, USA) and PFDX (Medgraphics, St Paul, MN, USA) in the KOLD, following the standard protocol established by the American Thoracic Society and European Respiratory Society.15
Definition and Identification of COPD Risk Factors as Potential Etiotypes
We investigated the following four risk factors of COPD in view of potential etiologies based on the patient-reported information. Cigarette smoking (C) was defined by either current or past smoking history of more than 10 pack-years;16 infection (I) by a history of pulmonary tuberculosis; and asthma (A) by a history of asthma with physician diagnosis. The arbitrary definition of biomass or/and pollution exposure (P) differed in the two datasets: the occupation history of simple labor jobs in the KNHANES and the occupation history of skilled workers or simple labor jobs related to agriculture, forestry, cooking, construction, metalwork, machinery, wood, and textile industry in the KOLD, respectively. We selected the aforementioned occupational categories based on the reported information, with potential exposure to organic or inorganic dust, as risk factor P. Specific classification of occupation was based on the Korean Standard Classification of Occupations.17 All information was collected by trained interviewers according to the pre-specified study protocol and newly developed survey questions for each dataset.12,14
We investigated the profile of risk factors by identifying 1) each risk factor in the groups of COPD and non-COPD subjects, 2) the number of risk factors in each subject, and 3) the combination of risk factors if two or more were identified. Additionally, we investigated the association between the risk factors for COPD only in the KNHANES because only this dataset had data on subjects with and without COPD.
Statistical Analysis
All data are presented as means and standard deviations for the continuous variables and numbers and percentages for categorical variables. We compared the data using Student’s t-test for the continuous variables and the χ2 or Fisher’s exact test for the categorical variables between COPD and non-COPD groups in the KNHANES.
To explore the effects of risk factors C, I, P, and A as potential etiologies of COPD, we first evaluated marginal associations between those risk factors and COPD while adjusting for age, sex and BMI. Then, interaction effects between sex and those risk factors were further evaluated. Key strengths in this interaction analysis are 1) to overcome sex disparities in those risk factors and 2) to assess whether the effects of risk factors are the same for males and females. We performed a logistic regression analysis to calculate the adjusted odds ratio (aOR) with 95% confidence intervals (CIs). All tests of significance were two-sided, and p-values of <0.05 were considered to indicate statistical significance. All analyses were performed using SPSS software (version 24.0; Chicago, IL, USA).
Study Approval and Informed Consent
The Institutional Review Board of Asan Medical Center (IRB no.: 2022–1717) approved this study. The board waived the requirement for informed consent because of the retrospective nature of the analysis. This study was conducted in accordance with the amended Declaration of Helsinki.
Results
Subject Selection and Characteristics
Between 2015 and 2019, 39,759 subjects were enrolled in the KNHANES. Among them, 22,151 were excluded due to an age of less than 40 years and having no appropriate spirometry result. Therefore, 17,608 subjects were included, comprising 2430 COPD and 15,178 non-COPD subjects from the KNHANES (Figure 1A). Among 677 subjects with airflow limitation in the KOLD, 81 who had been clinically diagnosed with asthma and 17 without airflow limitation (defined by an FEV1 to FVC ratio of less than 0.7) were excluded. Finally, 579 COPD subjects from the KOLD were included in this study (Figure 1B).
 |
Figure 1 Selection of study subjects from the KNHANES, a dataset of the general population (A), and from the KOLD, a dataset of referral clinics (B). *According to the original study design of the KNHANES, spirometry was performed in subjects 40 years or older only. Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 sec; FVC, forced vital capacity; KNHANES, Korea National Health and Nutrition Examination Survey; KOLD, Korean Obstructive Lung Disease cohort. |
Table 1 presents the characteristics of the study subjects. The mean age of subjects with COPD was 66.6 years in KNHANES and 67.3 years in KOLD, with a predominance of males in both, at 71.2% and 93.8%, respectively. The mean BMI was 23.7 kg/m2 in the subjects with COPD from the KNHANES and 23.1 kg/m2 in those from the KOLD. The mean ratio of FEV1/FVC was 63.4% in subjects with COPD in the KNHANES and 46.2% in those from the KOLD. The mean FEV1% predicted was 79.1% in subjects with COPD from the KNHANES and 55.4% in those from the KOLD.
 |
Table 1 Characteristics of Subjects Selected from the KNHANES, the Data of the General Population, and from the KOLD, the Data of Referral Clinics |
Risk Factors in Subjects with COPD in the KNHANES and KOLD
Figure 2 presents the profile of risk factors for the subjects with COPD from the KNHANES (Figure 2A) and the KOLD (Figure 2B). All four risk factors were more frequently observed in KOLD subjects with COPD (Table 2 and Figure 3A). The profile of risk factors C, I, P, A, and U (unidentified) was 54.6%, 9.4%, 10.7%, 7.9%, and 32.6%, respectively, in the KNHANES subjects with COPD, and 88.4%, 26.6%, 41.6%, 35.2%, and 3.1%, respectively, in the KOLD subjects with COPD.
 |
Table 2 Risk Factors of Subjects in the COPD Groups from the KNHANES and the KOLD |
 |
Figure 2 Profiles of risk factors in subjects with COPD from the KNHANES, a dataset of the general population (A) and from the KOLD, a dataset of referral clinics (B). Abbreviations: C, cigarette smoking; I, infection; P, exposure to biomass or pollution; A, asthma; COPD, chronic obstructive pulmonary disease; KNHANES, Korea National Health and Nutrition Examination Survey; KOLD, Korean Obstructive Lung Disease cohort. |
 |
Figure 3 Profile (A) and number (B) of risk factors in subjects with COPD from the KNHANES (general population) and from the KOLD (referral clinics). Abbreviations: C, cigarette smoking; I, infection; P, exposure to biomass or pollution; A, asthma; COPD, chronic obstructive pulmonary disease; KNHANES, Korea National Health and Nutrition Examination Survey; KOLD, Korean Obstructive Lung Disease cohort. |
Figure 3B presents the number of identified risk factors in each subject with COPD. The proportion of subjects with COPD with two or more risk factors was higher in those from the KOLD (66.1% vs 14.1% in the KNHANES). Over a quarter of KOLD subjects with COPD had three or more risk factors, whereas only 28 (1.2%) had three risk factors in the COPD subjects from the KNHANES. Supplementary Figure S1 presents the proportion of subjects with COPD from both datasets with each combination of risk factors.
Risk Factors in Non-COPD Subjects from the KNHANES
Table 3 shows the risk factors in subjects with and without COPD from the KNHANES. Risk factors C (25.0% vs 54.6% in subjects with COPD, p-value <0.001), I (3.7% vs 9.4% in subjects with COPD, p-value <0.001), and A (1.8% vs 7.9% in subjects with COPD, p-value <0.001) were significantly less frequently observed in subjects without COPD. However, there was no difference in the frequency of risk factor P between subjects without and with COPD (10.1% vs 10.7%, respectively, p-value = 0.415). Significantly fewer subjects having any risk factors were observed in those without COPD (36.5% vs 67.4% in subjects with COPD, p-value <0.001).
 |
Table 3 Risk Factors of Subjects in the COPD and the Non-COPD Groups from the KNHANES |
Contribution of Risk Factors for COPD in Male and Female Subjects
We identified a significant interaction between sex and risk factor I (p-value for interaction = 0.002). Therefore, we investigated the relation of risk factors to COPD separately according to sex. Supplementary Tables S1 and S2 present the profile of risk factors in male and female subjects. Although most risk factors were more common in subjects with COPD, there was no difference in the risk factor P, between non-COPD and COPD female subjects. In the multivariate analysis, risk factor A presented a significant association with COPD in male (aOR 5.92, 95% CI 3.97–8.85, Table 4) and female subjects (aOR 5.13, 95% CI 3.89–6.76, Table 5), followed by risk factor C (male aOR 2.14, 95% CI 1.88–2.45; female aOR 2.99, 95% CI 2.10–4.24, respectively) and I (male aOR 1.51, 95% CI 1.20–1.90; female aOR 2.76, 95% CI 2.04–3.74). There was no significant association between COPD and risk factor P in either sex (male aOR 0.98, 95% CI 0.80–1.20; female aOR 0.96, 95% CI 0.75–1.22).
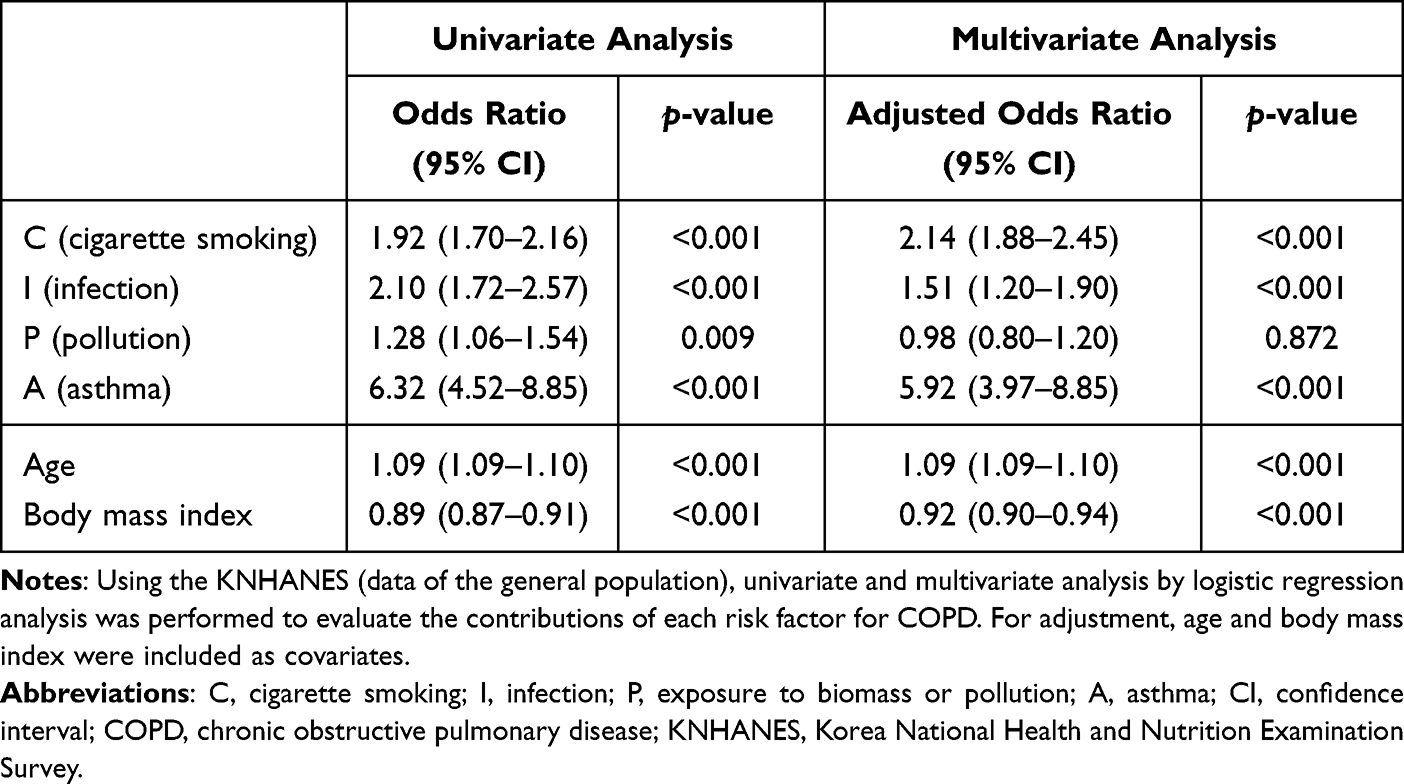 |
Table 4 Contribution of Each Risk Factor for COPD in the Male Subjects of the KNHANES |
 |
Table 5 Contribution of Each Risk Factor for COPD in the Female Subjects of the KNHANES |
Discussion
In this study, we demonstrated the profile of risk factors as potential etiotypes of subjects with COPD from a general population dataset, the KNHANES, and referral clinics, the KOLD. The risk factors appeared to be less frequently identified in subjects with COPD from the general population than from referral clinics. As expected, the risk factors were less frequently identified in subjects without compared to those with COPD in the KNHANES. After collectively evaluating the contribution of each risk factor, risk factor C, I, and A showed a significant association with COPD. To our knowledge, this is the first study to show the comprehensive profile of risk factors in subjects with COPD from a general population vs referral clinics given potential COPD etiotypes, which had been proposed by the GOLD 2023 update.6
The KNHANES data represent a general population of apparently healthy individuals in South Korea. The framework of the KNHANES study design and methods were adopted from those of the National Health and Nutrition Examination Survey (NHANES) of the United States.14,18 For the KNHANES, participants underwent a comprehensive interview with trained interviewers, spirometry by trained technicians, and other exams based on the standardized protocol.14 Therefore, the data of the KNHANES represent the general population of South Korea, in which females are much less frequently reported as smokers compared with males. Therefore, careful consideration is warranted when applying the results of this study to a population with a higher smoking rate in females, although KNHANES has been utilized in many studies related to COPD.19,20
The KOLD cohort had enrolled patients with airway diseases, including COPD, asthma, or both in outpatient clinics of secondary or tertiary referral hospitals in South Korea.12 There was a predominance of males in the KOLD, probably because the higher smoking rate in males than in females in South Korea. The value of the KOLD data may be indirectly validated by many publications using the data.21–23
Subjects with COPD in the KNHANES and the KOLD had different frequencies of risk factors. Distinct characteristics of each dataset could lead to these differences. Subjects in the KNHANES were recruited from a general population, whereas those in the KOLD had visited referral clinics before recruitment. Therefore, subjects in the KOLD may have COPD-related symptoms and more severe lung impairment. The mean value of FEV1 of subjects with COPD was 63.4% of the predicted value in the KNHANES and 46.2% predicted in the KOLD. Compared with the KNHANES, the incidence of each risk factor was higher in the KOLD, with 66.2% of subjects having two or more risk factors. Based on these results, the severity of COPD could be associated with the number of accompanying risk factors. Several studies have previously highlighted a combination of risk factors related to the development of COPD.8–11,24–26 Another potential cause of the difference in the profile of risk factors was that decreased prevalence of smoking led to increased contribution of other risk factors for COPD. The two datasets recruited eligible subjects at different time points (2005 to 2015 in the KOLD and 2015 to 2019 in the KNHANES). Chang et al reported that smoking prevalence decreased annually, and that high socioeconomic status was related to a lower smoking rate in South Korea.27
In this study, more than half of subjects with COPD in the KNHANES and 88.4% of subjects with COPD in the KOLD had a smoking history of more than 10 pack-year. In both datasets, risk factor C accounted for the highest proportion as a sole risk factor compared with other factors. Although there are some reports that female subjects may be more susceptible to cigarette smoking than male,6,28,29 we did not find a significant difference between males and females in the development of COPD when exposed to smoking, defined risk factor C in this study. Because smoking prevalence was related to COPD prevalence and relatively high in South Korea, further study might be needed to apply this result to other population, especially in lower smoking prevalence countries.30,31
In previous studies, a history of tuberculosis was reported as a cause of COPD.32,33 Similarly, risk factor I was shown to be related to COPD in this study. Kamenar et al demonstrated that the prevalence of COPD in subjects with a previous history of tuberculosis was 25.9%,32 which was in line with our findings in the KNHANES population (29.1%, 229 among 786 subjects with risk factor I, Supplementary Figure S2). In that study, notably, females with a previous history of tuberculosis had a higher aOR compared with males. In our study, significant interaction effects between sex and risk factor I were present, and higher aOR in female subjects compared with male subjects (aOR 2.763, 95% CI 2.039–3.743 vs aOR 1.510, 95% CI 1.200–1.899 in male subjects) was also observed. Considering some reports on female susceptibility to cigarette smoking,28,29 it is possible that females could be more susceptible to pulmonary infection, which could result in persistent limitation in airflow. Because prevalence of tuberculosis in South Korea was higher, contribution of tuberculosis for COPD development might be higher than other countries.34
In our study, risk factor A was also a significant risk factor for COPD and had the highest aOR among the four risk factors in both males and females. These results were in line with previous studies.35–38 Uncontrolled asthma in early life could hinder normal lung development and decrease the level of maximal FEV1.7,39,40 Additionally, a decline in lung function was reported regardless of time of asthma onset.38,39,41 Given a history of asthma is an important risk factor for COPD development and controlled asthma has a lower risk for COPD diagnosis than uncontrolled asthma,36 clinicians may be required to investigate and treat asthma to reduce the risk of COPD development.
Exposure to biomass and air pollutants was also known as a risk factor for developing COPD.6,42–44 In this study, risk factor P was the second most commonly identified risk factor after risk factor C in COPD subjects in the KNHEANES and KOLD. However, we found no association between occupational exposure and COPD development, which could be attributed to several reasons. First, we could only investigate occupation history and not possible exposure to biomass and air pollutants. The relationship between occupational exposure to biomass and air pollutants and COPD development has been reported in the literature.45,46 Second, simple labor workers, which we operatively defined as risk factor P, did not directly relate to exposure to occupational pollutants. In addition to type of work, respiratory protection equipment use may substantially affect the development of COPD.47,48 Thirdly, we could not estimate the quantitative amount of exposure to occupational hazard. Therefore, the contribution of risk factor P for COPD development may require reevaluation with sufficient information.
There are several limitations to this study. First, we only evaluated the risk factors based on the available information in each dataset. Therefore, the contribution of each risk factor could be under- or overestimated due to other risk factors not included in this study. For example, human immunodeficiency virus infection, data on which were not included in the KNHANES, is generally regarded as an important cause of COPD, although the rate of infection is low in South Korea.49,50 Data related to childhood hospital admission for severe respiratory illness, regarded as another crucial COPD risk factor, were lacking in the dataset.6,31 Additionally, the contribution of genetic factors (COPD-G) and abnormal lung development (COPD-D) for COPD could not be evaluated owing to lack of information. Because only four of the six etiotypes were investigated except COPD-D and COPD-G, the lack of information could lead to information bias. Additionally, because information for the differential diagnosis of COPD and asthma was not available in the KNHANES, patients with asthma could have been misclassified as having COPD. In particular, the absence of post-bronchodilator spirometry results in the KNHANES dataset suggests that the diagnosis of some patients with COPD may be incorrect. Secondly, there was a difference in the definition of risk factor P between the KNHANES and the KOLD; therefore, we could not directly compare the difference between them. In this study, we obtained only information on occupational exposure for evaluating biomass and pollution exposure and arbitrarily selected occupational categories, with potential for exposure to organic or inorganic dust, as risk factor P. It is therefore possible that risk factor P was insufficient to reflect biomass and pollution exposure. Further study is therefore warranted to obtain more information about household pollution, ambient air pollution, and wildfire smoke to evaluate biomass and pollution. Whereas those of risk factors I, P, and A were defined by exposure history to each risk factor without information related to duration, definition of risk factor C reflected exposure amount to smoking. Therefore, this point could result in underestimating the contribution of risk factor C and overestimating those of risk factors I, P, and A. Thirdly, the history of asthma, tuberculosis, and occupation was based on patient reports, which might have led to recall bias. However, trained interviewers obtained the KNHANES and the KOLD data with the pre-specified study protocol and survey questions. Finally, we utilized only nationwide population dataset in South Korea. Compared with subjects in western countries, prevalence of smoking, tuberculosis and asthma in South Korea was distinctly reported.34,51,52 Further studies might be required to investigate the profile of COPD risk factors in various study populations.
Conclusions
Although there were some limitations to this study, this is the first to collectively present the risk factor profiles for subjects with COPD. Risk factors appeared to be less frequently identified in subjects with COPD from the general population than in those from referral clinics. Compared with non-COPD subjects, risk factors C, I, and A were significantly related to COPD in the general population in this study. However, the association between risk factor P and COPD should be further analyzed with complete information about indoor and outdoor pollution. Additionally, the effects of genetics and developmental abnormalities on COPD require investigation. Based on the results of this study, more effort should be made to elucidate the risk factors, especially for subjects with COPD in the general population.
Abbreviations
C, cigarette smoking; I, infection; A, asthma; P, biomass or/and pollution exposure; aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 sec; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; KNHANES, the Korea National Health and Nutrition Examination Survey; KOLD, the Korean Obstructive Lung Disease cohort.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The study protocol was approved by the Institutional Review Board of the Asan Medical Centre (IRB no.: 2022-1717). The board waived the requirement for obtaining patient informed consent because of the nature of the analysis. The KNHANES and KOLD datasets are, respectively, managed and supervised by the Korea Centers for Disease Control and Prevention and Obstructive Lung Disease Research Foundation for data protection and privacy regulation. All provided information is anonymized in the KNHANES and KOLD datasets. The data accessed complied with relevant data protection and privacy regulations.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2022 Report. Available from: www.goldcopd.org.
2. Tan WC, Sin DD, Bourbeau J, et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: results from the CanCOLD study. Thorax. 2015;70(9):822–829. doi:10.1136/thoraxjnl-2015-206938
3. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respirat Med. 2022;10(5):497–511. doi:10.1016/S2213-2600(21)00506-3
4. Terzikhan N, Verhamme KM, Hofman A, Stricker BH, Brusselle GG, Lahousse L. Prevalence and incidence of COPD in smokers and non-smokers: the Rotterdam study. Eur J Epidemiol. 2016;31(8):785–792. doi:10.1007/s10654-016-0132-z
5. Lee SJ, Kim SW, Kong KA, Ryu YJ, Lee JH, Chang JH. Risk factors for chronic obstructive pulmonary disease among never-smokers in Korea. Int J Chron Obstruct Pulmon Dis. 2015;10:497–506. doi:10.2147/COPD.S77662
6. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2023 report. Available from: www.goldcopd.org.
7. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission. Lancet. 2022;400(10356):921–972. doi:10.1016/S0140-6736(22)01273-9
8. Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. doi:10.1016/S0140-6736(07)61377-4
9. Menezes AM, Perez-Padilla R, Jardim JR, et al. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. doi:10.1016/S0140-6736(05)67632-5
10. Caballero A, Torres-Duque CA, Jaramillo C, et al. Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest. 2008;133(2):343–349. doi:10.1378/chest.07-1361
11. Miravitlles M, Soriano JB, Garcia-Rio F, et al. Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities. Thorax. 2009;64(10):863–868. doi:10.1136/thx.2009.115725
12. Park TS, Lee JS, Seo JB, et al. Study design and outcomes of Korean obstructive lung disease (KOLD) cohort study. Tuberc Respir Dis. 2014;76(4):169–174. doi:10.4046/trd.2014.76.4.169
13. Oh K, Kim Y, Kweon S, et al. Korea national health and nutrition examination survey, 20th anniversary: accomplishments and future directions. Epidemiol Health. 2021;43:e2021025. doi:10.4178/epih.e2021025
14. Kweon S, Kim Y, Jang MJ, et al. Data resource profile: the Korea national health and nutrition examination survey (KNHANES). Int J Epidemiol. 2014;43(1):69–77. doi:10.1093/ije/dyt228
15. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
16. Mathew AR, Bhatt SP, Colangelo LA, et al. Life-course smoking trajectories and risk for emphysema in middle age: the CARDIA lung study. Am J Respir Crit Care Med. 2019;199(2):237–240. doi:10.1164/rccm.201808-1568LE
17. Korea National Statistical Office. Korean standard classification of occupations. Daejeon: Korea National Statistical Office; 2007. Available from: https://kssc.kostat.go.kr:8443/ksscNew_web/index.jsp.
18. Johnson CL, Dohrmann SM, Burt VL, Mohadjer LK. National health and nutrition examination survey: sample design, 2011–2014. Vital Health Stat 2. 2014; 162:1–33.
19. Lee H, Shin SH, Gu S, et al. Racial differences in comorbidity profile among patients with chronic obstructive pulmonary disease. BMC Med. 2018;16(1):178. doi:10.1186/s12916-018-1159-7
20. Jo YS, Kim KJ, Rhee CK, Yoo KH, Jung KS, Park YB. Prevalence, characteristics, and risk of exacerbation in young patients with chronic obstructive pulmonary disease. Respir Res. 2022;23(1):212. doi:10.1186/s12931-022-02144-0
21. Cho YH, Seo JB, Lee SM, et al. Radiomics approach for survival prediction in chronic obstructive pulmonary disease. Eur Radiol. 2021;31(10):7316–7324. doi:10.1007/s00330-021-07747-7
22. Kim YW, Lee CH, Hwang HG, et al. Resting hyperinflation and emphysema on the clinical course of COPD. Sci Rep. 2019;9(1):3764. doi:10.1038/s41598-019-40411-1
23. Jung JY, Kim YS, Kim SK, et al. Relationship of vitamin D status with lung function and exercise capacity in COPD. Respirology. 2015;20(5):782–789. doi:10.1111/resp.12538
24. Pallasaho P, Kainu A, Sovijärvi A, Lindqvist A, Piirilä PL. Combined effect of smoking and occupational exposure to dusts, gases or fumes on the incidence of COPD. COPD. 2014;11(1):88–95. doi:10.3109/15412555.2013.830095
25. Thomson NC. Asthma with a smoking history and pre-chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;204(1):109–110. doi:10.1164/rccm.202102-0440LE
26. Govender N, Lalloo UG, Naidoo RN. Occupational exposures and chronic obstructive pulmonary disease: a hospital based case–control study. Thorax. 2011;66(7):597–601. doi:10.1136/thx.2010.149468
27. Chang Y, Kang HY, Lim D, Cho HJ, Khang YH. Long-term trends in smoking prevalence and its socioeconomic inequalities in Korea, 1992–2016. Int J Equity Health. 2019;18(1):148. doi:10.1186/s12939-019-1051-x
28. Sorheim IC, Johannessen A, Gulsvik A, Bakke PS, Silverman EK, DeMeo DL. Gender differences in COPD: are women more susceptible to smoking effects than men? Thorax. 2010;65(6):480–485. doi:10.1136/thx.2009.122002
29. Aryal S, Diaz-Guzman E, Mannino DM. Influence of sex on chronic obstructive pulmonary disease risk and treatment outcomes. Int J Chron Obstruct Pulmon Dis. 2014;9:1145–1154. doi:10.2147/COPD.S54476
30. Dai X, Gakidou E, Lopez AD. Evolution of the global smoking epidemic over the past half century: strengthening the evidence base for policy action. Tob Control. 2022;31(2):129–137. doi:10.1136/tobaccocontrol-2021-056535
31. Adeloye D, Song P, Zhu Y, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respirat Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
32. Kamenar K, Hossen S, Gupte AN, et al. Previous tuberculosis disease as a risk factor for chronic obstructive pulmonary disease: a cross-sectional analysis of multicountry, population-based studies. Thorax. 2022;77(11):1088–1097. doi:10.1136/thoraxjnl-2020-216500
33. Fan H, Wu F, Liu J, et al. Pulmonary tuberculosis as a risk factor for chronic obstructive pulmonary disease: a systematic review and meta-analysis. Ann Transl Med. 2021;9(5):390. doi:10.21037/atm-20-4576
34. World Health Organization. Global Tuberculosis Report 2022. Geneva, Switzerland: World Health Organization; 2022.
35. Sears MR. Smoking, asthma, chronic airflow obstruction and COPD. Eur Respir J. 2015;45(3):586–588. doi:10.1183/09031936.00231414
36. Silva GE, Sherrill DL, Guerra S, Barbee RA. Asthma as a risk factor for COPD in a longitudinal study. Chest. 2004;126(1):59–65. doi:10.1378/chest.126.1.59
37. Hayden LP, Cho MH, Raby BA, et al. Childhood asthma is associated with COPD and known asthma variants in COPDGene: a genome-wide association study. Respir Res. 2018;19(1):209. doi:10.1186/s12931-018-0890-0
38. Mattes J, Gibson PG. The early origins of COPD in severe asthma: the one thing that leads to another or the two things that come together? Thorax. 2014;69(9):789–790. doi:10.1136/thoraxjnl-2014-205401
39. McGeachie MJ, Yates KP, Zhou X, et al. Patterns of growth and decline in lung function in persistent childhood asthma. N Engl J Med. 2016;374(19):1842–1852. doi:10.1056/NEJMoa1513737
40. McGeachie MJ. Childhood asthma is a risk factor for the development of chronic obstructive pulmonary disease. Curr Opin Allergy Clin Immunol. 2017;17(2):104–109. doi:10.1097/ACI.0000000000000348
41. Porsbjerg C, Lange P, Ulrik CS. Lung function impairment increases with age of diagnosis in adult onset asthma. Respir Med. 2015;109(7):821–827. doi:10.1016/j.rmed.2015.04.012
42. Pérez-Padilla R, Ramirez-Venegas A, Sansores-Martinez R. Clinical characteristics of patients with biomass smoke-associated COPD and chronic bronchitis, 2004–2014. Chronic Obstruct Pulmon Dis. 2014;1(1):23–32. doi:10.15326/jcopdf.1.1.2013.0004
43. Camp PG, Ramirez-Venegas A, Sansores RH, et al. COPD phenotypes in biomass smoke- versus tobacco smoke-exposed Mexican women. Eur Respir J. 2014;43(3):725–734. doi:10.1183/09031936.00206112
44. Ackermann-Liebrich U, Leuenberger P, Schwartz J, et al. Lung function and long term exposure to air pollutants in Switzerland. Study on air pollution and lung diseases in adults (SAPALDIA) Team. Am J Respir Crit Care Med. 1997;155(1):122–129. doi:10.1164/ajrccm.155.1.9001300
45. Zhao J, Li M, Wang Z, et al. Role of PM2.5 in the development and progression of COPD and its mechanisms. Respir Res. 2019;20(1):120. doi:10.1186/s12931-019-1081-3
46. Liu S, Zhou Y, Liu S, et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: results from a cross-sectional study in China. Thorax. 2017;72(9):788–795. doi:10.1136/thoraxjnl-2016-208910
47. Majee AM, Dutta S. Pulmonary functions and work-related musculoskeletal disorders of road construction workers of West Bengal, India. Int J Occup Saf Health. 2022;12(3):185–195. doi:10.3126/ijosh.v12i3.40316
48. Boadu EF, Okeke SR, Boadi C, Bonsu EO, Addo IY. Work-related respiratory health conditions among construction workers: a systematic narrative review. BMJ Open Respirat Res. 2023;10(1):e001736. doi:10.1136/bmjresp-2023-001736
49. Choi Y, Choi BY, Kim SM, et al. Epidemiological characteristics of HIV infected Korean: Korea HIV/AIDS Cohort Study. Epidemiol Health. 2019;41:e2019037. doi:10.4178/epih.e2019037
50. Lee YH, Bang JH, Park SM, et al. Cost-effectiveness of Voluntary HIV testing strategies in a very low-prevalence country, the Republic of Korea. J Korean Med Sci. 2018;33(46):e304. doi:10.3346/jkms.2018.33.e304
51. Gunter R, Szeto E, Jeong SH, Suh S, Waters AJ. Cigarette smoking in South Korea: a narrative review. Korean J Fam Med. 2020;41(1):3–13. doi:10.4082/kjfm.18.0015
52. Song W-J, Kang M-G, Chang Y-S, Cho S-H. Epidemiology of adult asthma in Asia: toward a better understanding. APA. 2014;4(2):75–85.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Affecting Patient Adherence to Inhalation Therapy: An Application of SEIPS Model 2.0
Ma J, Sun X, Wang X, Liu B, Shi K
Patient Preference and Adherence 2023, 17:531-545
Published Date: 3 March 2023
β2-Adrenoceptor Agonists in Asthma or Chronic Obstructive Pulmonary Disease and Risk of Parkinson’s Disease: Nested Case-Control Study
Paakinaho A, Tiihonen M, Koskela H, Koponen M, Tiihonen J, Hartikainen S, Tolppanen AM
Clinical Epidemiology 2023, 15:695-705
Published Date: 12 June 2023
Exercise Rehabilitation and Chronic Respiratory Diseases: Effects, Mechanisms, and Therapeutic Benefits
Xiong T, Bai X, Wei X, Wang L, Li F, Shi H, Shi Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1251-1266
Published Date: 19 June 2023
COPD in People with HIV: Epidemiology, Pathogenesis, Management, and Prevention Strategies
Byanova KL, Abelman R, North CM, Christenson SA, Huang L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2795-2817
Published Date: 29 November 2023
Real-World Disease Burden and Healthcare Resource Utilization Among Patients with COPD and Asthma Using Triple Therapy (FF/UMEC/VI) in the United States
Igboekwe E, Verma S, Paczkowski R
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:281-296
Published Date: 25 January 2024