Back to Journals » Patient Preference and Adherence » Volume 20
Sleep Quality and Its Relationship with Temporomandibular Disorders and Oral Health-Related Quality of Life Among Dental Students and Interns: A Cross-Sectional Study
Authors Alsubaie N, Alshahrani W, Alabdulkarim SS, Alghannam RJ ![]() , Shahin S
, Shahin S ![]() , Alamri A, Nazir MA
, Alamri A, Nazir MA ![]()
Received 19 October 2025
Accepted for publication 13 March 2026
Published 27 March 2026 Volume 2026:20 575424
DOI https://doi.org/10.2147/PPA.S575424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Noof Alsubaie,1 Wejdan Alshahrani,1 Shaikha Salah Alabdulkarim,1 Razan Jaber Alghannam,1 Suliman Shahin,2 Abdulaziz Alamri,2 Muhammad Ashraf Nazir2
1College of Dentistry, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 2Department of Preventive Dental Science, College of Dentistry, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia
Correspondence: Muhammad Ashraf Nazir, Email [email protected]
Purpose: This cross-sectional study aimed to evaluate sleep quality and its relationship with temporomandibular disorders and oral health-related quality of life among dental students and interns.
Patients and Methods: This study was conducted on dental students and interns at Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. Undergraduate male and female dental students and interns voluntarily participated in the study. The participants completed the Pittsburgh Sleep Quality Index (PSQI) questionnaire for sleep quality, Fonseca’s questionnaire for temporomandibular disorders (TMD), and the Oral Health Impact Profile (OHIP) for oral health-related quality of life (OHRQoL) in addition to demographic data. Pearson’s correlation test and multiple linear regression analysis were performed in the study.
Results: The study included 159 participants, with 42.8% males and 57.2% females. Most participants (89.3%) demonstrated poor sleep quality. More than half of the study sample (57.2%) had TMD, with 29.6% having mild TMD, 23.3% having moderate TMD, and 4.4% having severe TMD. Bivariate analysis showed that sleep quality was significantly correlated with TMD (r=0.211, P=0.008) and OHRQoL (r=0.200, P=0.012). In addition, TMD were significantly correlated with OHRQoL (r=0.443, P< 0.001). According to multiple linear regression analysis models, sleep quality was significantly correlated with TMD (P= 0.029) and OHRQoL (P=0.016) after controlling for age, gender, class year, educational levels of parents, and monthly family income. Similarly, regression analysis showed that TMD was significantly correlated with OHRQoL (P< 0.001). Mediation analysis showed a significant indirect effect of sleep quality on OHRQoL through TMD (effect = 0.31, 95% CI=0.09, 0.56).
Conclusion: The study showed that poor sleep quality was very common among dental students and interns. Sleep quality was significantly correlated with TMD and OHRQoL, and TMD significantly impacted OHRQoL.
Keywords: sleep quality, temporomandibular disorders, quality of life
Introduction
Sleep quality is defined as “an individual’s satisfaction with all aspects of the sleep experience”.1 Sleep is crucial for human development and mental health, and inadequate sleep can lead to depression, fatigue, and reduced attention span.2 An individual with poor sleep quality is at an increased risk of cognitive, systemic, and oral health problems.3 It has been recommended that adults regularly get seven or more hours of sleep per night to promote optimal health.4 However, 1 in every 3 adults was found to sleep less than 7 hours per night in Riyadh, Saudi Arabia.5 On average, Saudi dental students sleep for 5.85 ± 1.85 hours per night.6 Academic stress and anxiety can cause students to experience insufficient sleep, potentially leading to sleep disorders, and decreased academic performance.2 In Saudi Arabia, 35% of dental students were reported to have poor sleep quality, which was negatively correlated with academic performance.6
Evidence shows that sleep disorders can affect the immune system and periodontal health of individuals, hence compromising their oral health.7 Sleep deficiency is significantly associated with tooth loss, which has adverse effects on systemic health and quality of life.8 Therefore, poor sleep quality can significantly compromise oral health-related quality of life (OHRQoL).9 Globally, temporomandibular disorders (TMD) affect approximately 31.1% of adults and the elderly.10 In Saudi Arabia, 54.2% of health professions students and 36.99% of dental students experience TMD.11,12 Previous studies reported that poor sleep quality was common among young adults, and it was associated with TMD with dysfunctional pain.13–15 On the other hand, a study of dental students showed no association between poor sleep quality and TMD.16 A recent overview of systemic reviews reported an association between sleep disorders and TMD among adults.17 Poor sleep quality is a significant factor associated with TMD due to increased production of inflammatory cytokines, which enhance pain associated with TMD.18,19 In addition, sleep disorders can cause hyperalgesia, which may contribute to heightened TMD symptoms.19
There is a high prevalence of poor sleep quality among dental students, affecting their health as well as academic performance. However, the influence of poor sleep quality on TMD and OHRQoL has not been adequately investigated among dental students and interns. Additionally, previous studies have explored the relationship between sleep quality and TMD and OHRQoL in isolation and have not modelled them together. It is hypothesized that poor sleep quality contributes to an increased severity of TMD symptoms and deteriorates OHRQoL. Poor sleep quality may not only directly affect OHRQoL but also indirectly affect it through its exacerbation of TMD symptoms. The study results may guide stakeholders to implement interventions aimed at improving sleep quality and oral health among student populations. Therefore, this cross-sectional study aimed to evaluate sleep quality and its relationship with temporomandibular disorders and oral health-related quality of life among dental students and interns in Dammam, Saudi Arabia.
Materials and Methods
Study Population
A cross-sectional questionnaire-based study was conducted on dental students and interns at the College of Dentistry, Imam Abdulrahman Bin Faisal University (IAU), Dammam, Saudi Arabia. Undergraduate male and female students from the 2nd to the 6th year and interns were eligible to participate in the study. At IAU, students complete a one-year preparatory program and then start dental courses from the second year to the sixth year. The participants who provided written informed consent were eligible to participate in the study. The exclusion criteria included participants under treatment for TMD, sleep disorder, and neurological conditions because these may have confounding effects on their assessment as well as relationships between TMD, sleep quality and OHRQoL.
Ethics and Consent
This study is part of the project, which was approved (IRB-2025-02-0054) by the Institutional Review Board at the Deanship of Scientific Research, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. The participants received information about the aims and details of the study. They were assured of the privacy and confidentiality of their responses. Participation in the survey was anonymous and voluntary. The voluntary and written consent forms were obtained from the participants who agreed to participate in the study. The research protocol followed the ethical guidelines of the Declaration of Helsinki.
Measurement Instruments
The participants completed the Pittsburgh Sleep Quality Index (PSQI) questionnaire, Fonseca’s questionnaire, and Oral Health Impact Profile (OHIP) in addition to demographic data. The study administered English versions of PSQI, Fonseca, and OHIP-14 instruments because all participants were proficient in English, as it is the medium of instruction at the dental college.
The PSQI was used to evaluate sleep quality among participants. Developed by Buysse et al, the instrument is used to assess sleep quality and disturbances over one month. Nineteen items in PSQI yield seven component scores, such as subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The addition of individual scores of each component produces a final score ranging from 0 to 21.20 A higher score on the scale indicates lower sleep quality (a score of ≥ 5 shows poor sleep quality).21 A previous study showed that PSQI had validity, internal reliability, and internal homogeneity.22
Fonseca’s questionnaire is a valid and reliable instrument for screening participants with TMD.23,24 It is commonly used in research and clinical practice because of its simplicity. The instrument is composed of 10 questions, each with a three-option scale (yes, sometimes, and no).25 A score of 10 is assigned to “yes”, 5 to “sometimes” and 0 to “no”. The total score is calculated by adding the score of individual items, and it ranges from 0 to 100. Fonseca index classification is used to assess the severity of TMD, and a score of the instrument from 0 to15 is classified as the absence of TMD, 20–40 as mild TMD, 45–65 as moderate TMD, and 70–100 as severe TMD.11
The Oral Health Impact Profile (OHIP-14) questionnaire is widely used to evaluate Oral Health-Related Quality of Life (OHRQoL).26 It is a reliable and valid tool and consists of 14 questions that describe various health aspects affecting quality of life from an oral health perspective.27,28 Each item is rated on a 5-point Likert scale (never=0, rarely=1, occasionally=2, often=3, and very often=4). These items describe seven dimensions of the instrument such as functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap.26 The final score of the questionnaire is obtained by adding the score of each item, and it ranges from 0 to 56. The greater score of the scale indicates lower OHRQoL and vice versa.27
Procedure
The researchers made an announcement in classrooms, student lounges, and clinical settings, and they physically distributed hard copies of questionnaires in classrooms after their lectures and in student lounges and clinical settings during break time. The participants were provided with further information if they experienced any difficulty in understanding certain questions. The researchers ensured that participants completely understood the questions and responded to all items in the survey. They returned questionnaires to the participants if any item was not answered completely. This approach resulted in the collection of complete questionnaires without any missing data. There were approximately 271 dental students and interns, and all of them were approached. However, 180 participants agreed to participate in the study, and they were provided with questionnaires, 159 returned completed questionnaires, resulting in a response rate of 88.3%.
Statistical Analysis
Data analysis was performed by using SPSS software (IBM SPSS Statistics for Windows, version 22.0. Armonk, NY: IBM Corp) and a statistical significance level of 0.05 was used. Descriptive statistics were presented in tables and graphs and included means, standard deviation, and proportions. Parametric tests were performed after checking the normality of data for PSQI, TMD, and OHIP-14 (Shapiro–Wilk test, p > 0.05). One-way ANOVA test was used to compare mean scores of TMD and OHIP-14 in categories of participants with different sleep quality to determine the relationship between sleep quality and TMD and OHRQoL. Pearson’s correlation test and multiple linear regression analysis were performed to evaluate the relationship between sleep quality and TMD and OHRQoL. Age, gender, GPA in the last year, monthly family income, and parental education levels were used as covariate for regression models. The multicollinearity in these regression models was assessed using variance inflation factors, which was less than 3. PROCESS macro (Model 4) was used to conduct mediation analysis to examine the relationship between sleep quality, TMD, and OHRQoL. A p-value of less than 0.05 was considered statistically significant.
Results
The study included data from 159 dental students and interns with 42.8% males and 57.2% females. The mean age of the study sample was 22.07± 1.81 years and their mean GPA in the last year was 4.32±0.33. Most participants had college/university education fathers (70.4%) and mothers (66.0) and 49.1% belonged to the high-income group (Table 1). More than half of the study sample (57.2%) demonstrated TMD. Mild TMD were found in 29.6%, moderate TMD in 23.3%, and severe TMD in 4.4% of participants (Figure 1).
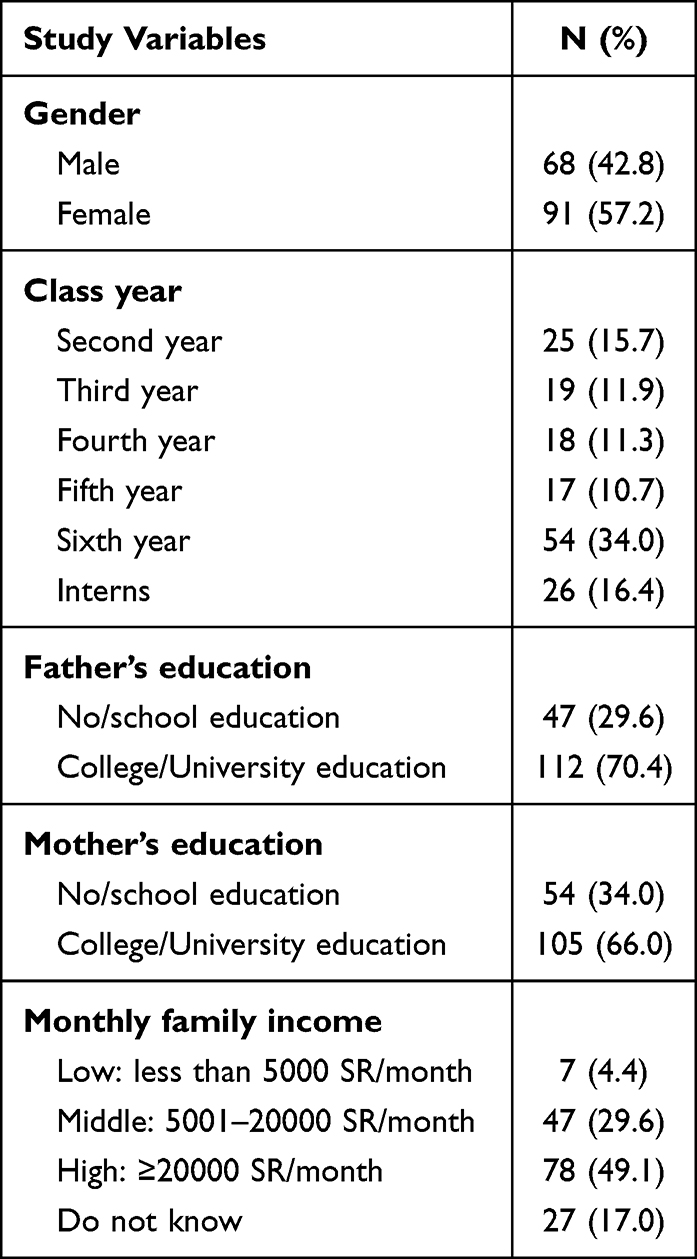 |
Table 1 Demographic Data of the Study Participants (N=159) |
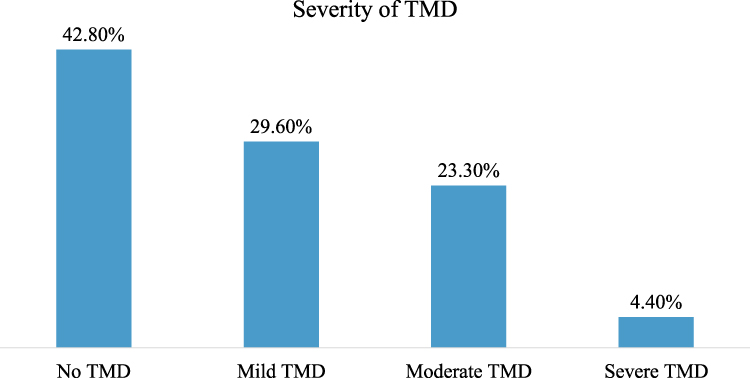 |
Figure 1 Distribution of participants’ responses about the severity of TMD. |
The results show a high prevalence of poor sleep quality (89.3%) among participants. The mean score for the PSQI scale of the study sample was 9.02±3.51. The sleep efficiency component had the highest mean score (2.34±1.15), and this was followed by sleep latency (1.36±1.0), and subjective sleep quality (1.30±0.85), whereas the lowest mean score was related to the use of sleep medicine (0.50±0.82) (Table 2).
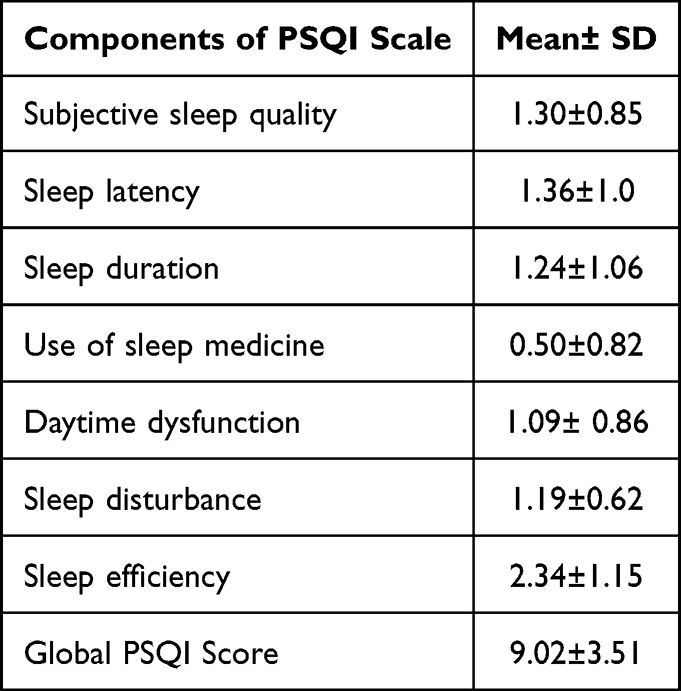 |
Table 2 Descriptive Statistics for the Seven Components and Global Score of the PSQI |
There was a statistically significant relationship between sleep quality and TMD (P=0.012) with a medium effect size (η2= 0.069), and participants with no TMD showed significantly lower scores of the PSQI compared to those with TMD. The participants with no TMD demonstrated significantly lower scores on the OHIP-14 scale than those with severe TMD (P<0.001), indicating better oral health-related quality of life, with a large effect size (η2= 0.162) (Table 3).
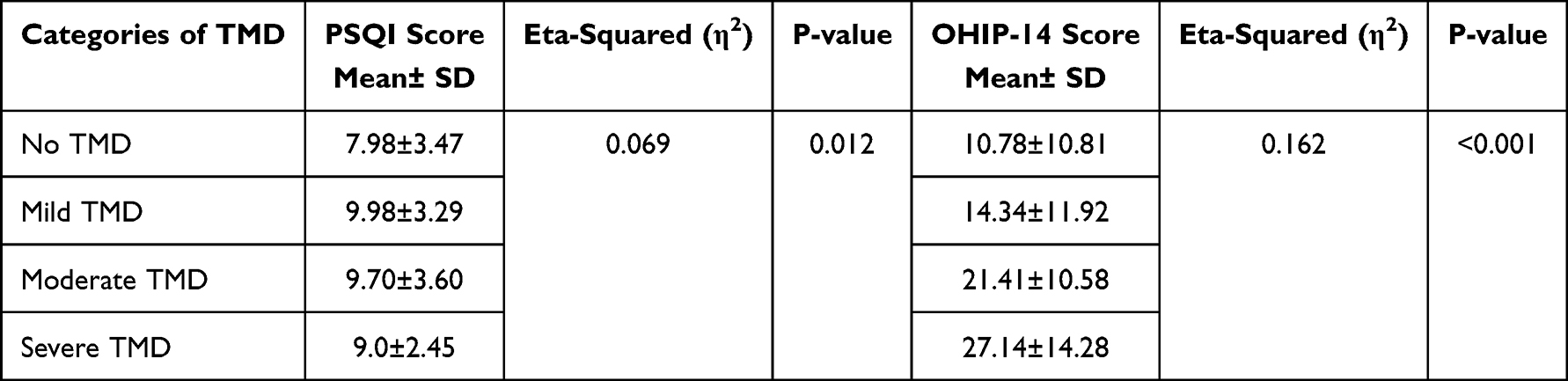 |
Table 3 Comparison of Sleep Quality (PSQI) and OHRQoL (OHIP-14) Scores Across TMD Severity Groups |
The Table 4 shows that the participants with mild TMD demonstrated significantly poorer sleep quality compared to the participants with no TMD (P= 0.013). However, no statistically significant differences in sleep quality were observed between no TMD group versus moderate TMD group (P = 0.071) and between no TMD group versus the severe TMD group (P= 0.878). The pairwise comparisons in Table 5 revealed no statistically significant difference in OHRQoL between the participants with no TMD versus the participants with mild TMD (P= 0.344). Statistically significant differences in OHRQoL were found between no TMD group versus moderate TMD group (P= 0.001) and between no TMD group versus severe TMD group (P= 0.002).
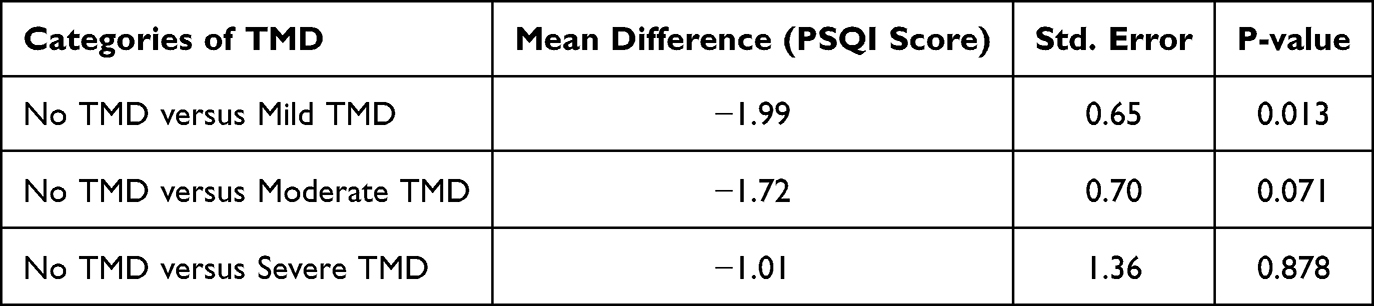 |
Table 4 Tukey’s HSD Post-Hoc Pairwise Comparisons of TMD Severity Groups on Sleep Quality (PSQI Score) |
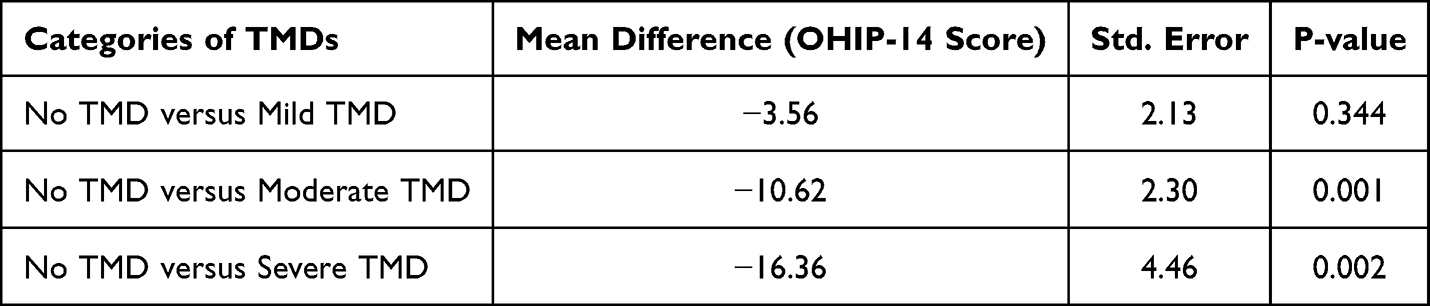 |
Table 5 Tukey’s HSD Post-Hoc Pairwise Comparisons of TMD Severity Groups on Oral Health-Related Quality of Life (OHIP-14 Score) |
In the study, the mean score for TMD was 26.98±23.27 and for OHIP-14 was 15.03±12.17. Bivariate analysis showed that sleep quality was significantly correlated with TMD (r=0.211, P=0.008) and OHRQoL (r=0.200, P=0.012), indicating modest effect sizes. In addition, TMD was significantly correlated with OHRQoL (r=0.443, P<0.001) (Table 6). Figure 2 shows a weak positive correlation between sleep quality and OHIP-14 scores among participants. Similarly, a weak correlation was found between sleep quality and TMD scores (Figure 3). There was a moderate correlation between TMD and OHIP-14 scores (Figure 4).
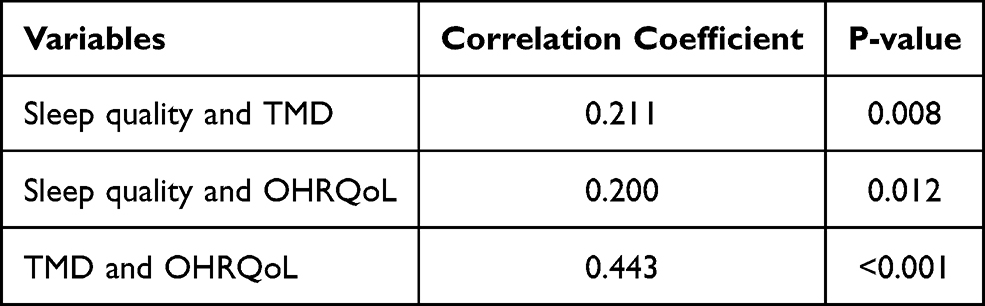 |
Table 6 Bivariate Analysis: Relationship Between Sleep Quality and TMD and OHRQoL Among Study Participants |
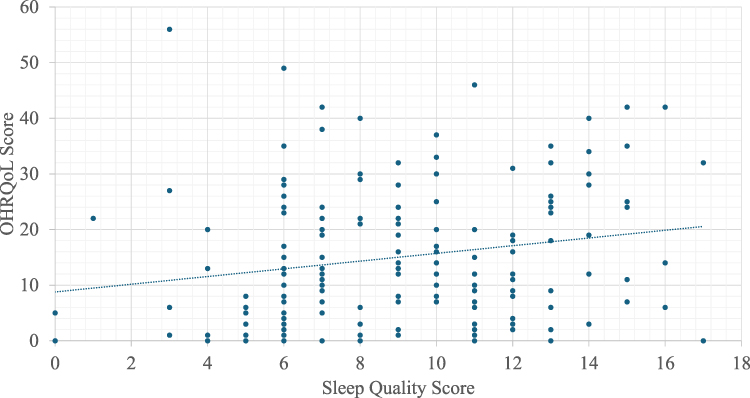 |
Figure 2 Scatterplot of the correlation between sleep quality and OHRQoL among study participants. |
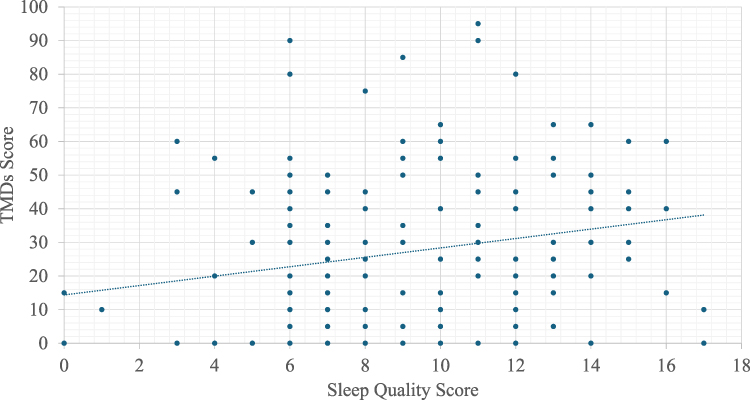 |
Figure 3 Scatterplot of the correlation between sleep quality and TMD among study participants. |
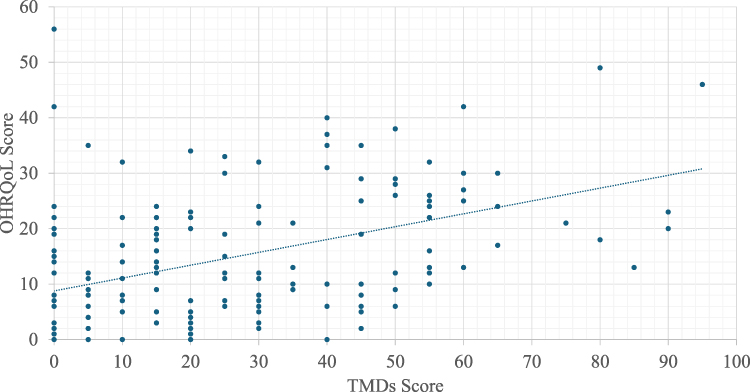 |
Figure 4 Scatterplot of the correlation between TMD and OHRQoL among study participants. |
After adjusting for covariates in multiple linear regression analysis models, poor sleep quality remained significantly associated with higher odds of TMD (B = 1.89, 95% CI: 0.19, 3.59, p 0.029), indicating that each one-point increase in PSQI score was associated with a 1.89-point increase in TMD severity. Poor sleep quality was also associated with worse OHRQoL (B = 0.06, 95% CI: 0.011, 0.103, p 0.016). Similarly, TMD severity remained significantly associated with poor OHRQoL (B = 0.21, 95% CI: 0.10, 0.33, p <0.001), demonstrating that each one-point increase in TMD severity was associated with a 0.21-point increase in OHIP-14 scores (Table 7).
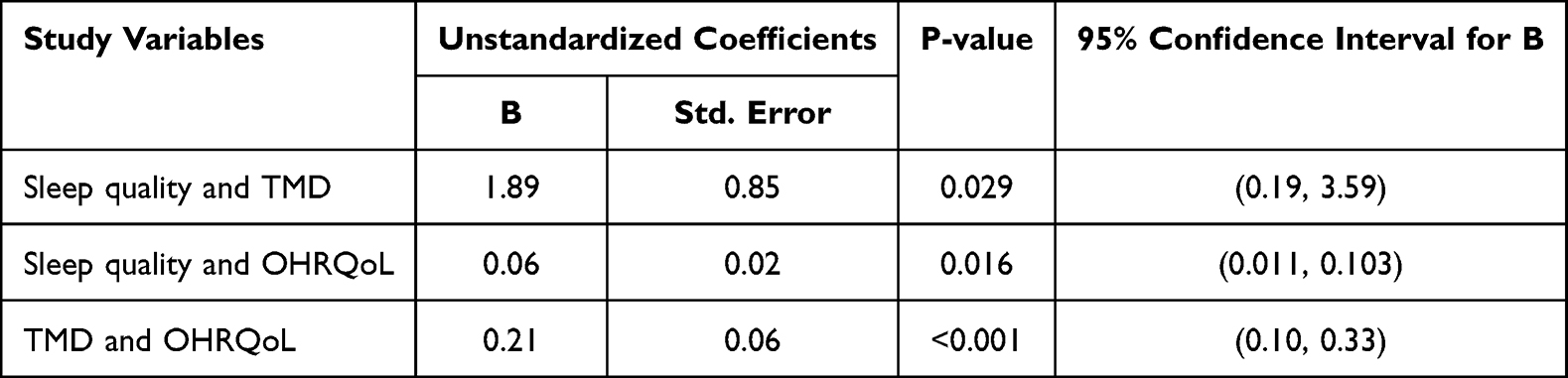 |
Table 7 Multivariable Regression Analysis: Relationship Between Sleep Quality and TMD and OHRQoL Among Study Participants |
Mediation analysis showed that poor sleep quality significantly influenced the severity of TMD (B = 1.39, P = 0.008). Similarly, there was a statistically significant effect of TMD on OHRQoL (B = 0.22, P <0.001). Poor sleep quality was not significantly associated with OHRQoL (B = 0.39, P = 0.129). However, there was a significant indirect effect of sleep quality on OHRQoL through TMD (effect = 0.31, 95% CI=0.09, 0.56) (Table 8).
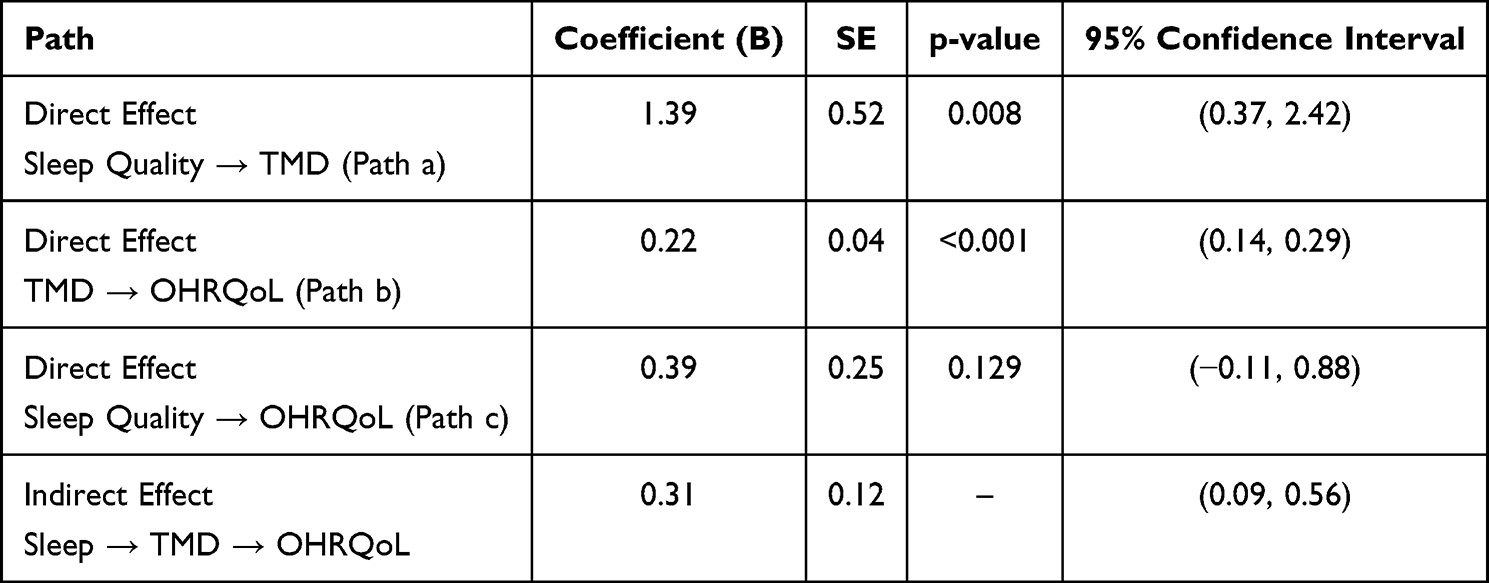 |
Table 8 Mediation Analysis: Indirect Effect of Sleep Quality (PSQI) on OHRQoL (OHIP-14) Through TMD Severity |
Discussion
The present study evaluated the prevalence of poor sleep quality among dental students in the eastern province of Saudi Arabia. The study also investigated the relationship between poor sleep quality and TMD and OHRQoL. In the present study, poor sleep quality was found in most participants (89.3%), which was similar to the results reported by Gaikwad et al, who showed that 89.8% of dental students experienced poor sleep quality in India.29 Compared to the present study, a lower proportion of dental students (68.13%) reported poor sleep quality in Brazil.16 On the other hand, the prevalence of poor sleep quality was 36.7% and 38% among dental students in Malaysia30 and India,31 respectively. Studies of university students conducted in different countries showed poor sleep quality in 58.7% of participants in Lebanon,32 54.7% in Taiwan,33 and 60% in the U.S.34 The variations in the prevalence of poor sleep quality in dental and other student populations can be attributed to different didactic and clinical workloads, study hours, levels of psychological stress, and cultural differences related to sleep habits.29,30 There is a trend of sleeping late at night and having a short duration of nighttime sleep among populations in Saudi Arabia, which may account for a high prevalence of poor sleep quality in the present study.35 The findings of present study should not be generalized to other populations from different geographic locations due to its limited external validity.
Globally, the prevalence of TMD among dental students, as assessed by the Fonseca Anamnestic Index, is as follows: Pakistan (66.9%),36 Brazil (58.9%),37 and India (42%).38 The present study showed that 57.2% of dental students exhibited signs of TMD. These findings corroborate the results of a previous study conducted in Dammam, Saudi Arabia, where 55% of health professions students reported having TMD.11 Previous studies on dental students in Saudi Arabia showed that the prevalence of TMD ranged from 45% to 62.8%.39,40 Gender and demographic differences, lifestyle variations, academic stress, and methodological differences in the conduct of studies may account for differences in the prevalence of TMD among dental students in the present and previous studies.11,36 TMD is a multifactorial disorder which may explain the high prevalence of TMD in our sample, which included considerable population of high-income students. A high prevalence of poor sleep quality and TMD in the present study underscores the importance of preventive measures to minimize their adverse consequences on the oral health of dental students.
According to a systematic review and meta-analysis, individuals with poor sleep quality were 4.45 times more likely to have TMD than those without poor sleep quality.41 It is known that poor sleep can affect the immune system, causing the production of inflammatory cytokines, which promote pain and inflammation in the temporomandibular joint.42 Sleep quality was significantly correlated with TMD in our sample of dental students. In addition, the regression analysis in the present study showed that sleep quality was significantly correlated with TMD. Moreover, mediation analysis revealed that sleep quality significantly influenced TMD. These results are in accordance with findings of an Iranian study that showed lower sleep quality was significantly correlated with higher severity of TMD after controlling for demographic factors.43 A recent study from Pakistan also confirmed significant correlation between sleep quality and TMD symptoms.44 On the contrary, a study of dental students found no significant correlation between sleep quality and TMD in India.29 Similarly, another study of dental students showed no significant association between poor sleep quality and TMD symptoms in Brazil.16
The findings of the present study demonstrate a clear relationship between sleep quality and OHRQoL, showing a statistically significant correlation between these variables. However, mediation analysis found no significant influence of sleep quality on OHRQoL but sleep quality indirectly affected OHRQoL through TMD. The study also showed that an increase in TMD significantly and independently deteriorated OHRQoL in our sample. This was also confirmed in the mediation analysis, which showed a significant effect of TMD on OHRQoL. There were statistically significant associations between sleep quality and TMD, sleep quality and OHRQoL, and TMD and OHRQoL; however, the effect sizes were modest, indicating that other factors beyond sleep quality and TMD also contribute substantially to OHRQoL. Weak to modest correlations observed in the study could be because of multifactorial nature of sleep quality, TMD, and OHRQoL, and small sample size. A recent study of dental and dental hygiene students in Spain showed that poor sleep quality significantly affected OHRQoL because of physical pain, physical disability, psychological disability, and functional limitation.45 Similarly, another recent study from Australia also reported a strong positive association between sleep quality and OHRQoL.9 Given the challenging and demanding nature of dental programs, students experience a decline in sleep quality and elevated stress levels, contributing to the perception of poor OHRQoL. The results of the present study suggest the need for oral health promotion strategies aimed at enhancing the sleep health of dental students to support their quality of life as well as academic performance.2
The impact of TMD on OHRQoL is multifaceted, often presenting as difficulties in mastication and speech, which can compromise nutritional intake. Additionally, pain and discomfort associated with TMD may contribute to impaired sleep quality, reduced ability to perform routine activities, and overall poor quality of life.46 Our data suggested that as TMD severity increased, OHRQoL worsened significantly. These findings are consistent with the results of a study by Bal et al, where dental students with TMD reported significantly poorer OHRQoL compared to those students without TMD.47 In a recent study from Saudi Arabia, AlSahman et al also showed that TMD was significantly associated with poor OHRQoL, affecting physical pain and psychological discomfort domains.48
This study used valid and reliable instruments to provide valuable evidence about the interrelationships between sleep quality, TMD, and OHRQoL among dental students. A comprehensive understanding of these factors can help improve the oral health of dental students, who in turn may play a role in the prevention of sleep disturbance, TMD, and OHRQoL in the community. The sample calculation was not performed because all dental students and interns were invited to participate in the study. A high response rate was achieved in the study and the sample of 159 participants demonstrated adequate power to detect the significant indirect effect in the mediation model. However, small and unbalanced TMD groups limited statistical power for some pairwise comparisons. The study was conducted in a dental college, which limits the generalizability of results to dental students from other institutions. Fonseca Anamnestic Index is a screening tool and not a clinical diagnostic instrument, which limits the accurate assessment of TMD in our sample. The administration of questionnaires is prone to bias due to students’ subjective replies as well as social desirability bias. In addition, stress, anxiety, depression, academic workload, caffeine intake, and screen time can influence relationships between sleep quality and TMD; however, these variables were not included in the study due to its scope and resource constraints. It is known that cross-sectional studies provide valuable evidence, which can be further investigated in cohort studies or intervention trials, but they are limited in drawing conclusions about cause and effect. In the future, longitudinal studies should be conducted among students from multiple dental institutions to determine the temporal and causal relationships between sleep quality, TMD, and OHRQoL after adjusting for demographic variables as well as stress, anxiety, and academic workload. Future studies should use clinical diagnostic tool for the assessment of TMD.
Conclusion
The study showed that the majority of dental students and interns demonstrated poor sleep quality. There were significant correlations between sleep quality and TMD and OHRQoL, and sleep quality was significantly associated with TMD and OHRQoL. The study also showed that TMD significantly impacted OHRQoL. Regular health check-ups of dental students should include screening for TMD and poor sleep quality. Dental institutions should support the well-being of students by integrating sleep hygiene and stress management into dental curricula, offer mental health and TMD screening services, and promote a culture that prioritizes work-life balance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nelson KL, Davis JE, Corbett CF. Sleep quality: an evolutionary concept analysis. Nurs Forum. 2022;57(1):144–11. doi:10.1111/nuf.12659
2. Muñoz MDS, Dantas PPA, Pola NM, Casarin M, de Almeida RZ, Muniz F. Poor quality of sleep is associated with lower academic performance in undergraduate dental students: a cross-sectional study. Sleep Vigil. 2023;1–10. doi:10.1007/s41782-022-00223-2
3. Schroeder K, Gurenlian JR. Recognizing poor sleep quality factors during oral health evaluations. Clin Med Res. 2019;17(1–2):20–28. doi:10.3121/cmr.2019.1465
4. Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American academy of sleep medicine and sleep research society. Sleep. 2015;38(6):843–844. doi:10.5665/sleep.4716
5. Ahmed AE, Al-Jahdali F, AlALwan A, et al. Prevalence of sleep duration among Saudi adults. Saudi Med J. 2017;38(3):276–283. doi:10.15537/smj.2017.3.17101
6. Elagra MI, Rayyan MR, Alnemer OA, et al. Sleep quality among dental students and its association with academic performance. J Int Soc Prev Community Dent. 2016;6(4):296–301. doi:10.4103/2231-0762.186788
7. Carra MC, Schmitt A, Thomas F, Danchin N, Pannier B, Bouchard P. Sleep disorders and oral health: a cross-sectional study. Clin Oral Investig. 2017;21:975–983. doi:10.1007/s00784-016-1851-y
8. Al-Zahrani MS, Alhassani AA, Zawawi KH. Tooth loss as a potential risk factor for deficient sleep: an analysis of a nationally representative sample of adults in the USA. Sleep Breath. 2021;25:1101–1107. doi:10.1007/s11325-020-02131-z
9. Ju X, Hedges J, Sethi S, Jamieson LM. Poor self-rated sleep quality and quantity associated with poor oral health-related quality of life among Indigenous Australian Adults. Int J Environ Res Public Health. 2024;21(4):453. doi:10.3390/ijerph21040453
10. Valesan LF, Da-Cas CD, Réus JC, et al. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig. 2021;25(2):441–453. doi:10.1007/s00784-020-03710-w
11. Alamri A, Shahin S, Bakhurji EA, Alsulaiman AA, Salloot Z, Nazir M. Association of test anxiety with temporomandibular disorder in health professions students: a cross-sectional study. Int J Dent. 2020;2020:8833804. doi:10.1155/2020/8833804
12. Srivastava KC, Shrivastava D, Khan ZA, et al. Evaluation of temporomandibular disorders among dental students of Saudi Arabia using Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): a cross-sectional study. BMC Oral Health. 2021;21(1):211. doi:10.1186/s12903-021-01578-0
13. Rener-Sitar K, John MT, Pusalavidyasagar SS, Bandyopadhyay D, Schiffman EL. Sleep quality in temporomandibular disorder cases. Sleep Med. 2016;25:105–112. doi:10.1016/j.sleep.2016.06.031
14. Sanders AE, Akinkugbe AA, Bair E, et al. Subjective sleep quality deteriorates before development of painful temporomandibular disorder. J Pain. 2016;17(6):669–677. doi:10.1016/j.jpain.2016.02.004
15. Natu VP, Yap AU, Su MH, Irfan Ali NM, Ansari A. Temporomandibular disorder symptoms and their association with quality of life, emotional states and sleep quality in South-East Asian youths. J Oral Rehabil. 2018;45(10):756–763. doi:10.1111/joor.12692
16. Santos ES, de Souza Prates AM, Barros FPCS, et al. Analysis of the relationship between temporomandibular dysfunction and sleep quality: a cross-sectional study. Res Soc Dev. 2021;10(7):e10210716088–e. doi:10.33448/rsd-v10i7.16088
17. Rigon M, Obara K, Paixão L, Cardoso JR, Machado Junior AJ. Relationship between temporomandibular and sleep disorders in adults: an overview of systematic reviews. Sleep Med. 2024;124:404–415. doi:10.1016/j.sleep.2024.10.002
18. Park JW, Chung JW. Inflammatory cytokines and sleep disturbance in patients with temporomandibular disorders. J Oral Facial Pain Headache. 2016;30(1):27–33. doi:10.11607/ofph.1367
19. Wan J, Lin J, Zha T, et al. Temporomandibular disorders and mental health: shared etiologies and treatment approaches. J Headache Pain. 2025;26(1):52. doi:10.1186/s10194-025-01985-6
20. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
21. Angelillo S, Sansone V, Paduano G, Lateano L, Di Giuseppe G, Nobile CGA. The quality of sleep: evaluation among university students. Front Public Health. 2023;11:1270426. doi:10.3389/fpubh.2023.1270426
22. Manzar MD, Moiz JA, Zannat W, Spence DW, Pandi-Perumal SR, Hussain ME. Validity of the Pittsburgh sleep quality index in Indian University Students. Oman Med J. 2015;30(3):193–202. doi:10.5001/omj.2015.41
23. Dos Santos Berni KC, Dibai-Filho AV, Rodrigues-Bigaton D. Accuracy of the Fonseca anamnestic index in the identification of myogenous temporomandibular disorder in female community cases. J Bodyw Mov Ther. 2015;19(3):404–409. doi:10.1016/j.jbmt.2014.08.001
24. Campos JA, Carrascosa AC, Bonafé FS, Maroco J. Severity of temporomandibular disorders in women: validity and reliability of the Fonseca Anamnestic Index. Braz Oral Res. 2014;28:16–21. doi:10.1590/S1806-83242013005000026
25. Fonseca DMD, Bonfante G, Valle ALD, Freitas SFTD. Diagnóstico pela anamnese da disfunção craniomandibular. RGO. 1994:23–28.
26. Slade GD. Derivation and validation of a short-form oral health impact profile. Community Dent Oral Epidemiol. 1997;25(4):284–290. doi:10.1111/j.1600-0528.1997.tb00941.x
27. Feng Y, Lu -J-J, Ouyang Z-Y, et al. The Chinese version of the Oral Health Impact Profile-14 (OHIP-14) questionnaire among college students: factor structure and measurement invariance across genders. BMC Oral Health. 2022;22(1):405. doi:10.1186/s12903-022-02441-6
28. Uzarevic Z, Bulj A. Oral health-related quality of life among Croatian University Students. Int J Environ Res Public Health. 2021;18(12):6483. doi:10.3390/ijerph18126483
29. Gaikwad S, Waingade M, Medikeri RS, Jangam DK. Correlation between temporomandibular joint disorders, sleep quality and stress among dental students: a cross-sectional study. J Clin Diagn Res. 2023;17(7):ZC25–ZC8.
30. Hashim H, Ng JS, Ngo JX, Ng YZ, Aravindkumar B. Lifestyle factors associated with poor sleep quality among undergraduate dental students at a Malaysian private university. Sleep Sci. 2022;15(4):399–406. doi:10.5935/1984-0063.20220070
31. Nagarajappa R, Mohapatra U, Satyarup D, Panda S. Association of sleep quality and stress with academic performance among undergraduate dental students of Bhubaneswar, India. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2024;24:e230013. doi:10.1590/pboci.2024.064
32. Kabrita CS, Hajjar-Muça TA, Duffy JF. Predictors of poor sleep quality among Lebanese university students: association between evening typology, lifestyle behaviors, and sleep habits. Nat Sci Sleep. 2014;6:11–18. doi:10.2147/NSS.S55538
33. Cheng SH, Shih CC, Lee IH, et al. A study on the sleep quality of incoming university students. Psychiatry Res. 2012;197(3):270–274. doi:10.1016/j.psychres.2011.08.011
34. Lund HG, Reider BD, Whiting AB, Prichard JR. Sleep patterns and predictors of disturbed sleep in a large population of college students. J Adolesc Health. 2010;46(2):124–132. doi:10.1016/j.jadohealth.2009.06.016
35. Bamagoos AA, Altayeb AA, Rawas HF, et al. Patterns of sleep and napping in Saudi Arabia: a cross-sectional evaluation. Saudi J Med Med Sci. 2025;13(2):124–132. doi:10.4103/sjmms.sjmms_679_24
36. Nazir MA, Izhar F, Hassan S, et al. Temporomandibular disorders among dental students in Pakistan: assessment of prevalence, severity, and associated factors based on questionnaire. Scientifica. 2023;2023:8895544. doi:10.1155/2023/8895544
37. Rocha CO, Peixoto RF, Resende CM, Alves AC, Oliveira ÂG, Barbosa GA. Psychosocial aspects and temporomandibular disorders in dental students. Quintessence Int. 2017;48(3):241–249. doi:10.3290/j.qi.a37128
38. Kumar M, Harshitha C. Prevalence of temporomandibular disorders among dental undergraduate students. Drug Invent Today. 2018;10(7).
39. Alfawzan AA. An assessment of the prevalence and severity of temporomandibular disorders among undergraduate dental students at Qassim University. World J Dent. 2020;11(2):134–138. doi:10.5005/jp-journals-10015-1715
40. AlHussaini AA, AlHudithy LH, AlHadlaq MA, et al. The prevalence and severity of temporomandibular disorder (TMD) among female dental students in Riyadh, Saudi Arabia. Saudi Dent J. 2019;31:S55–S6. doi:10.1016/j.sdentj.2019.02.015
41. Roithmann CC, Silva C, Pattussi MP, Grossi ML. Subjective sleep quality and temporomandibular disorders: systematic literature review and meta-analysis. J Oral Rehabil. 2021;48(12):1380–1394. doi:10.1111/joor.13265
42. Wu G, Chen L, Wei G, et al. Effects of sleep deprivation on pain-related factors in the temporomandibular joint. J Surg Res. 2014;192(1):103–111. doi:10.1016/j.jss.2014.05.035
43. Zamani A, Haghnegahdar A, Vossoughi M. Evaluation of association between the severity of temporomandibular disorders and quality of sleep in a selected Iranian population. Front Dent. 2019;16(3):206–213. doi:10.18502/fid.v16i3.1592
44. Wandala A, Ikram N, Safiullah MB, et al. Association between sleep quality and Temporomandibular Disorders (TMD) symptoms among adults: a cross-sectional study. Cureus. 2025;17(7):e87818. doi:10.7759/cureus.87818
45. Vaca CS, Rosales Leal JI, Barrios-Rodríguez R. Oral health-related quality of life and daytime sleepiness in students. Oral Health Prev Dent. 2025;23:211–216.
46. Qamar Z, Alghamdi AMS, Haydarah NKB, et al. Impact of temporomandibular disorders on oral health-related quality of life: a systematic review and meta-analysis. J Oral Rehabil. 2023;50(8):706–714. doi:10.1111/joor.13472
47. Bal B, Sarak G, Oral K. Oral health-related quality of life and psychological states of dental students with temporomandibular disorders. J Dent Educ. 2022;86(11):1459–1467. doi:10.1002/jdd.12951
48. AlSahman L, AlBagieh H, AlSahman R, Correa LP, Mehta NR. Functional, physical and psychosocial impacts of oral health-related quality of life in temporomandibular disorders-a comparative study. Diagnostics. 2025;15(5):602. doi:10.3390/diagnostics15050602
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
Effects of Continuous Nursing on the Disease Uncertainty, Coping Strategies and Quality of Sleep and Life of Patients with Inflammatory Bowel Disease
Xu C, Xi W, Wu C, Liu L, Wang L
Journal of Multidisciplinary Healthcare 2023, 16:2071-2080
Published Date: 21 July 2023
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024
The Sequelae and Moderators of Influence of Dandruff on Mental Health Among Mainland Chinese Adults
Chan CS, Smith T, He Z, Garter C
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1333-1346
Published Date: 11 June 2024
Unravelling the Association of Physical Exercise, Quality of Life and Sleep Quality Among Chinese Perimenopausal Women
Li Y, Liu X, Zhou J, Zhang X
International Journal of Women's Health 2026, 18:603641
Published Date: 14 July 2026