Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Effects of Continuous Nursing on the Disease Uncertainty, Coping Strategies and Quality of Sleep and Life of Patients with Inflammatory Bowel Disease
Authors Xu C, Xi W, Wu C, Liu L, Wang L
Received 24 March 2023
Accepted for publication 15 June 2023
Published 21 July 2023 Volume 2023:16 Pages 2071—2080
DOI https://doi.org/10.2147/JMDH.S414104
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Chongwu Xu,1 Weizhen Xi,2 Chen Wu,2 Ling Liu,2 Lingling Wang2
1Department of Endoscopy Center, Yijishan Hospital, Wannan Medical College, Wuhu, 241000, People’s Republic of China; 2Department of Gastroenterology, Yijishan Hospital, Wannan Medical College, Wuhu, 241000, People’s Republic of China
Correspondence: Weizhen Xi, Department of Gastroenterology, Yijishan Hospital, Wannan Medical College, No. 2 Zheshan West Road, Jinghu District, Wuhu, 241000, People’s Republic of China, Tel +86 13955363461, Email [email protected]
Purpose: To explore the clinical effects of continuous nursing on patients with inflammatory bowel disease (IBD).
Methods: Patients with IBD in the digestive department of the hospital from January 2020 to August 2021 were selected as the research participants and divided into an observation and control group by the random number table method. The patients were treated with a routine nursing intervention (control group) or routine plus continuous nursing interventions (observation group). The disease uncertainty, coping strategies, sleep and quality of life before and after the interventions were compared between the two groups.
Results: After 6 months of the intervention, the disease uncertainty score of the observation group was significantly lower than that of the control group (p < 0.05). Medical coping style score: There was no significant difference in the three dimensions of medical coping style between the two groups before the intervention (p > 0.05). After 6 months of the intervention, the facial score of the observation group was significantly higher, and the avoidance and yield scores were significantly lower compared with the control group (p < 0.05). Sleep quality and quality of life score: There was no significant difference in the sleep quality score between the two groups before the intervention (p > 0.05). After 6 months of the intervention, the observation group’s sleep quality and quality of life scores were significantly higher compared with the control group (p < 0.05).
Conclusion: Compared with routine nursing, continuous nursing can reduce the disease uncertainty of patients with IBD, help them to adopt an active coping style, as well as improve their sleep quality and quality of life to relieve physical and mental pain and better restore health.
Keywords: continuing care, inflammatory bowel disease, quality of life, sleep quality, coping style
Introduction
Inflammatory bowel disease (IBD) is a chronic non-specific intestinal inflammatory disease with an unclear aetiology that cannot be cured. The disease is generally divided into ulcerative colitis and Crohn’s disease;1 the former mainly damages the colon and rectum, while the latter can damage any part of the gastrointestinal tract from the mouth to the anus, particularly the end of the small intestine and colon. The main clinical symptoms of IBD include abdominal pain, diarrhoea, tenesmus, mucous purulent bloody stool and chronic inflammation. In addition, some patients present with a high fever, anaemia, weight loss, anxiety, depression and other manifestations.2 Moreover, IBD is characterised by an insidious onset and easy recurrence, as well as a potential cancer risk. The pathogenesis and aetiology of IBD have been reported to be related to environmental and genetic factors or dysbacteriosis of the intestinal flora.3
In recent years, the prevalence of IBD has become high globally, and the mortality rate is increasing.4 However, because the aetiology and pathogenesis of the disease are unclear, and there are differences between individuals, some treatment methods may not completely cure the disease. Therefore, the condition may affect patients with IBD’s physical and psychological status, thereby reducing their quality of life.5
In recent years, the incidence of IBD in China has also increased annually. According to incomplete statistics, the annual incidence of IBD in China is 3.44/100,000,6 and it is becoming younger. Due to the long course of the disease and the delay, patients with IBD’s everyday life and work can be seriously affected; they can also come to bear economic pressure and mental burdens. These factors all impair the quality of life of patients with IBD. Due to the long course of the disease, it is easy to relapse, and patients’ quality of life is significantly impaired.
Continuous nursing ensures that patients receive ongoing care, usually beginning at the patient’s discharge from the hospital. It is a widely used nursing model in China, mainly for patients with high nursing needs following hospital admission in the acute phase. Generally, care is divided into two stages, ie pre- and post-discharge.7 Continuous nursing care is comprehensive, coordinated, continuous and cooperative; accordingly, it can ensure the consistency and management of nursing services to improve the quality of nursing care. Furthermore, it can effectively improve patients’ health status after discharge, avoid adverse events and reduce unnecessary waste of resources.7
Previous studies on continuous nursing in treating patients with IBD explored its role in improving patients’ quality of life and self-efficacy and reported improvements.8,9 Therefore, this study selected patients with IBD from the Department of Gastroenterology of the hospital to investigate the effect of continuous nursing care from different perspectives, including the patients’ disease uncertainty, coping strategies and sleep and life quality.
Materials and Methods
General Information
Patients with IBD admitted to the above-noted department from January 2020 to August 2021 were selected, totalling 97 cases. The inclusion criteria were as follows: 1. definite diagnosis of IBD; 2. aged at least 18 years; 3. the condition was relatively stable, without any malignant tumours or significant disability, and no major surgical history in the preceding three months. The exclusion criteria included severe psychological, mental and communication disorders. The withdrawal criteria included the following: 1. unqualified – patients did not meet the inclusion criteria during the study period; 2. non-compliance – patients who lacked interest in the study or whose situation changed, eg their condition worsened; 3. sample loss – patients lost during follow-up or who died during the study period.
Patients were numbered according to their hospitalisation number. For random number generation, 97 random numbers were selected from randomly specified rows or columns of the random number table (if repeated numbers were excluded) and listed successively under each patient number. Random numbers were ranked from small to large to achieve random allocation; numbers 1–49 were assigned to the observation group and 50–97 to the control group.
Methods
A routine treatment and nursing model was adopted for the control group. After admission, the responsible nurses evaluated the patients, filed them, provided health education, guided them on diet and medication after discharge and made regular return visits. The observation group adopted a continuous nursing model as follows.
Establishment of the Continuous Nursing Team
The continuous nursing team comprised a gastroenterologist (department director and IBD specialist), head nurse, specialist nurse, psychologist, dietitian, clinical pharmacist and family liaison officer. The specialist nurse dynamically developed the patients’ personalised treatment and care plans. The nursing organisation structure was as follows: 1) The head nurse was responsible for building the nursing team, supervising and controlling the effective implementation of the care plan, as well as taking the role of leader in multidisciplinary communication. In addition, the head nurse was responsible for continuous nursing concepts, models, applications and related specialised treatment training and nursing knowledge for all members. 2) A specialist nurse with good communication skills, quality control ability and N2 and N3 nursing-level qualifications was responsible for formulating, implementing and evaluating case plans for patients with IBD. In addition, the specialist nurse managed the follow-up visits of patients discharged from the hospital, WeChat health education and interactive consultation. 3) The continuous nursing team participated in patient assessments, treatment and nursing during admission, hospitalisation and post-discharge. The gastroenterologists were responsible for screening the patients and participated in formulating the continuous nursing plan and safety monitoring. The dietitian was responsible for guiding the patient’s nutrition and dietary knowledge. The clinical pharmacist was responsible for providing clinical medication guidance. Psychological counselling was necessary. Each patient selected a family liaison officer, usually a family member or caregiver, with a degree of education, the ability to use the Internet and the time and enthusiasm to participate in the patient’s health management or the patient.
Intervention Programmes During Hospitalisation and After Discharge
Interventions During Hospitalisation
Assessment and continuous nursing of patient care issues on admission and before discharge included: 1) Establishing and completing the patient’s health records, including age, address, telephone contact number, other essential information, family and social relationships and primary caregivers. In addition, the patient’s medical history was recorded, including present and previous medication, main nursing problems and nursing measures and other aspects. 2) The patients’ symptoms were evaluated after admission. The laboratory examination and auxiliary examination reports were recorded dynamically during the hospitalisation. The patients’ primary nursing problems were determined and classified by comprehensive analysis. Then, the priority order of nursing problems was determined using Maslow’s hierarchy of basic human needs and the patient’s unique situation. 3) Interventions were developed according to patients’ nursing problems and existing nursing intervention plans and communicated to their doctors. Interventions included a dynamic focus on patient care problems, constantly adjusting the intervention plans and determining nutrition programmes with patients, including home enteral nutrition and avoiding poor nutrition habits. Patients’ health and personal care were addressed by improving their knowledge of the disease and providing them with the skills and developing behaviours to promote a healthy lifestyle. In addition, the patients were provided with psychological support to establish confidence in their treatment and rehabilitation.
Intervention Measures After Discharge
Telephone, WeChat group and outpatient follow-ups were carried out in the first, third and sixth months after discharge. The primary aspects of follow-up were as follows. 1) The first aim was to solve the nursing problems of patients after discharge and evaluate their degree of improvement during hospitalisation, such as intestinal function, nutrition, self-care and perianal skin care after diarrhoea. Furthermore, the follow-up interventions aimed to guide the patients’ methods and skills for self-monitoring and home care, evaluate new nursing problems after discharge (eg the patient’s environment), symptoms such as diarrhoea or abdominal pain and provide timely health guidance. After release from the hospital, the discharge plan was formulated according to the patient’s condition, economic ability, access to family care and other conditions, and the patient was dynamically evaluated for the three aspects of cognition, behaviour and health status. 2) Exercise guidance was provided after assessing the patient’s self-care ability to determine a family exercise programme. In addition, the patient’s family management compliance was monitored, and exercise process problems were solved; encouragement and support were provided to patients with poor adherence. 3) Medication guidance and supervision were provided to patients and caregivers, including guiding patients in regular outpatient reviews of their liver and kidney functioning. Furthermore, guidance was provided to prevent the occurrence of drug side effects, how to save drugs and to solve medication-related problems promptly. 4) Psychosocial support was provided to assess the patient’s psychological condition after discharge. This was achieved by patiently listening to the patient’s main narrative, dredging up negative emotions timeously and guiding them to communicate with family, other patients with IBD and friends.
Observed Indexes
General Patient Information
Self-designed questionnaires were disseminated to collect the patients’ general information, including name, gender, age, education level, medical payment method, residence mode, disease course, family monthly income, average annual medical expenses, disease years, dependents and primary caregivers.
Disease Uncertainty Scale
The Xu disease uncertainty scale,10 developed in Taiwan, was used in this study after the translation and revision of 25 items and demonstrated good reliability and validity. This scale has been widely used in the domestic medical field and is suitable for the population in China. The ambiguity dimension had 15 items (1, 2, 3, 4, 8, 11, 12, 13, 14, 15, 16, 18, 21, 22 and 24), and the complexity dimension had 10 items (5, 6, 7, 9, 10, 17, 19, 20, 23 and 25). For this scale, Likert 5-level scoring method was used, with “strongly agree” counted as 5 points, “agree” counted as 4 points, “neither agree nor disagree” counted as 3 points, “disagree” counted as 2 points, and “strongly disagree” counted as 1 point, of which items 6, 7, 9, 23, and 25 were counterdirectional scoring questions. The scale score ranged from 25–125 points; 92–125 was high, 59–91 was medium and 25–58 was low. The higher the score, the higher the level of disease uncertainty.
Medical Coping Style Scale
Feifel developed the medical coping style scale with 19 items in 1987 to evaluate patients’ coping styles and strategies when faced with illness. In 2000, Shen et al11 scholars localized and revised the Chinese version of the MCMQ scale, which consists of 20 items, including three dimensions: face, avoidance, and yield, in line with the basic response pattern of people when facing dangerous events and is also easily explained. The Chinese version of the MCMQ had good reliability and validity, with test-retest reliability of 0.64, 0.85, and 0.67, respectively, and Cronbach’αcoefficients of 0.69, 0.60, and 0.76, respectively, indicating that this questionnaire is suitable for clinical psychological stress studies in Chinese patients. According to the intensity of the event, 0–4 points are counted from low to high, of which 8 items are reverse scored, with a total score of 20–80 points. The face score was accumulated by items 1, 2, 5, 10, 12, 15, 16 and 19. For avoidance, the scale points were collected by items 3, 7, 8, 9, 11, 14 and 17. The score of the yield scale was collected by items 4, 6, 13, 18 and 20. The higher the score of a coping style, the more likely the individual was to adopt this coping behaviour in the face of stress.
Pittsburgh Sleep Quality Scale
The total score of each factor component of the Pittsburgh sleep quality scale12 is between 0–21; the higher the score, the worse the sleep quality.
Quality of Life Scale
The quality of life scale13 for patients with IBD was a Likert 7-level scoring method with a total possible score of 32–224 points. The higher the score, the better the patient’s quality of life.
Statistical Analysis
Data analysis was conducted using the SPSS Statistics software (v.20.0 for Windows, IBM Statistical Software™, IBM Corp. Armonk, NY, USA). Measurement data were described by mean ± standard deviation ( ), and the t-test was used to compare the groups. Percentage description was used for count data, and a chi-square (χ2) test was used to compare groups. Statistical significance was considered at p < 0.05.
), and the t-test was used to compare the groups. Percentage description was used for count data, and a chi-square (χ2) test was used to compare groups. Statistical significance was considered at p < 0.05.
Results
General Patient Information
There were 55 male and 42 female patients, of which 39 were ulcerative colitis and 58 were Crohn’s disease cases. There was no significant difference in gender, age and education level between the two groups (p > 0.05), indicating comparability (Table 1).
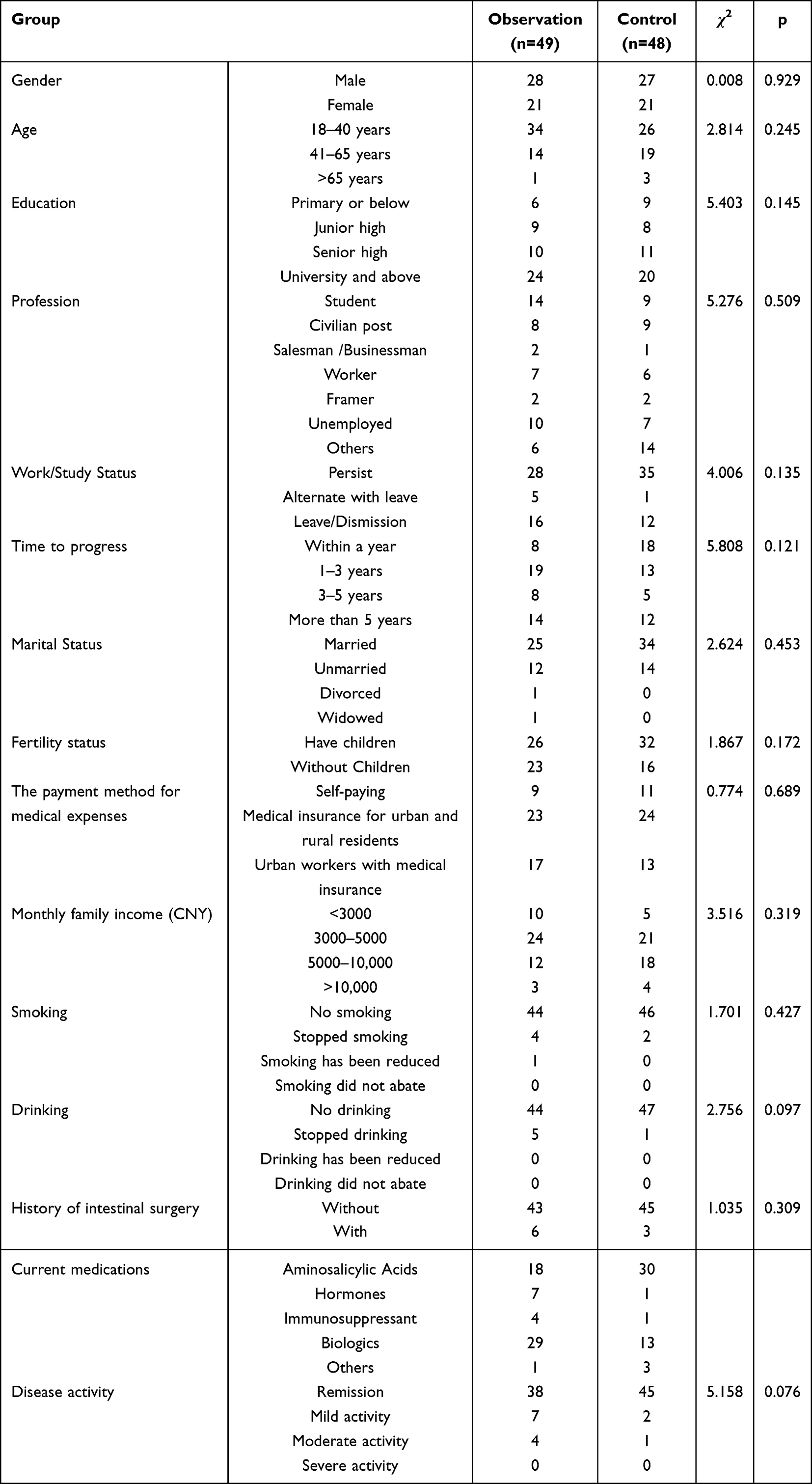 |
Table 1 Comparison of General Data of IBD Patients Between the Two Groups |
Comparison of Disease Uncertainty Scores
There was no significant difference in disease uncertainty scores between the two groups before the care intervention (p > 0.05). After 6 months of the intervention, the scores of the two groups were lower than before the intervention, and the difference before and after the intervention in the observation group was statistically significant (p < 0.05). The disease uncertainty score of the intervention group was significantly lower than that of the control group, and the difference between the two groups was statistically significant (p < 0.05) (Table 2).
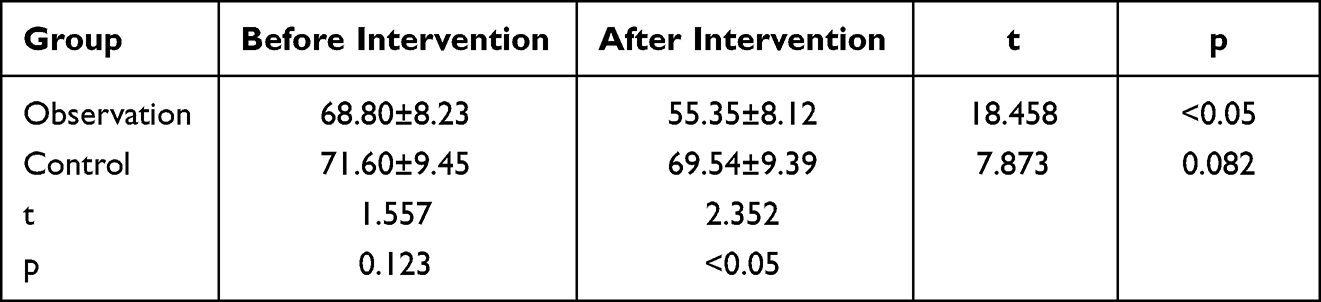 |
Table 2 Comparison of Disease Uncertainty Score Between the Two Groups (Score, |

Comparison of Medical Coping Style Score
There was no significant difference in the scores of the three dimensions of medical coping style between the two groups before the intervention (p > 0.05). After 6 months of the intervention, the face score of the two groups had increased, and the avoidance and yield scores had decreased. There were differences in the three dimensions of the observation group before and after the intervention (p < 0.05); however, there was no difference in the control group (p > 0.05). The facial score of the observation group was higher than that of the control group; however, the avoidance and yield scores were lower than the control group. The difference between the two groups was statistically significant (p < 0.05; see Table 3).
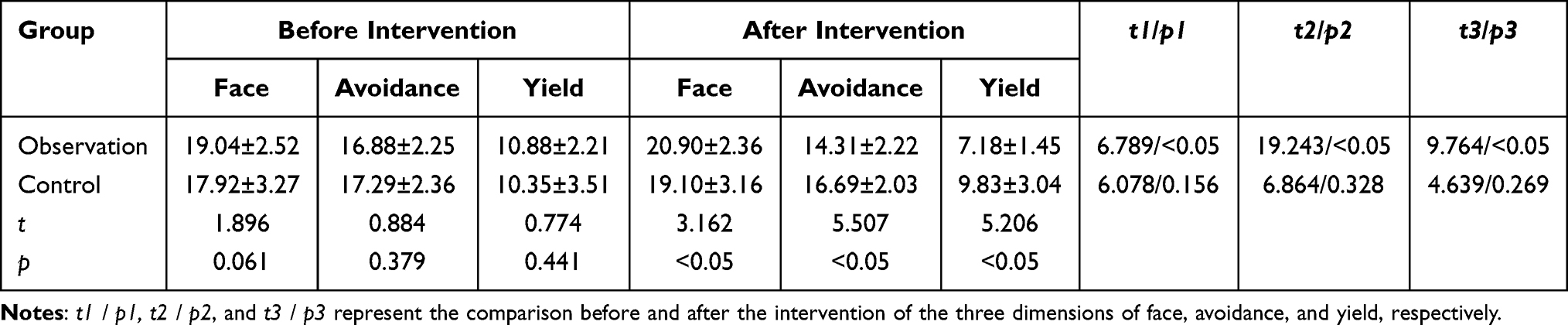 |
Table 3 Comparison of Scores of Medical Coping Styles Between the Two Groups (Points, |

Comparison of Sleep Quality Scores
There was no significant difference in sleep quality scores between the two groups before the intervention (p > 0.05). After 6 months of the intervention, the scores of the two groups were lower than before the intervention, and the difference between the scores before and after the intervention in the observation group was statistically significant (p < 0.05). The sleep quality score of the observation group was significantly higher compared with the control group (p < 0.05) (Table 4).
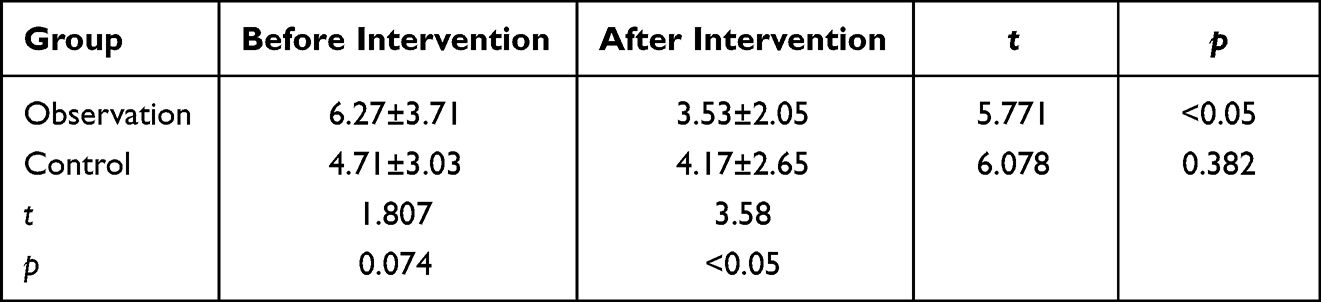 |
Table 4 Comparison of Sleep Quality Scores Between the Two Groups (Score, |

Comparison of Quality of Life Scores
There was no significant difference between the two groups before the interventions (p > 0.05). After 6 months of the intervention, the scores of the two groups were higher than before; there was also a significant difference in the observation group’s scores before and after the intervention (p > 0.05). The quality of life score of the observation group was significantly higher compared with the control group (p < 0.05) (Table 5).
 |
Table 5 Comparison of Quality of Life Scores Between the Two Groups (Points, |

Discussion
Inflammatory bowel disease is a group of chronic non-specific intestinal diseases with an unclear aetiology, and the onset age tends to be younger.14 Patients are prone to disease uncertainty in the face of repeated conditions, complex treatment, adverse drug reactions, impaired cognition and confusion about the development and outcome of the disease. Disease uncertainty interferes with patients’ ability to obtain information about the condition and impacts their psychological well-being, treatment confidence and compliance.15 Good coping strategies are conducive to maintaining mental health and improving the quality of life of patients with IBD.15 Continuous care involves doctors and nurses from multiple disciplines and requires their cooperation to provide patients with multifaceted care and health guidance. The onset of IBD is extremely complex, and diagnosis involves multiple disciplines; therefore, diagnosis and treatment by multidisciplinary teams are essential for the treatment and prognosis of patients with IBD, an approach that is supported by the European Crohn’s and Colitis Organisation.16 After understanding and evaluating the development and changes of the disease, gastroenterologists communicate with radiology, ultrasound, pathology and other disciplines. Furthermore, they must cooperate closely with the surgical procedures of the patient’s treatment to discuss diagnostic strategies. Follow-up of patients and nutritional control are equally important and can help to prevent disease recurrence.
The Continuous Nursing Model Significantly Reduced Patients’ Disease Uncertainty
This study used the patient’s existing nursing problems to develop an individualised care intervention plan. This approach involved a dynamic new focus on patient care problems and constantly adjusting the intervention plans. The nutrition programmes were designed in consultation with the patient and included home enteral nutrition, nutrition, health and personal care, prevention and poor nutrition. Further, patients were provided with the methods and skills to manage their IBD, psychological support and continuous care services. The study’s results showed that after the intervention, the control group disease uncertainty score was 69.54 ± 9.39 in the control group. In contrast, the observation group’s score was 65.35 ± 8.12; this suggests that the continuous nursing model effectively increased the patients’ disease-related knowledge and understanding, improved self-care and nursing levels and enhanced confidence to conquer the disease. Keefer et al’s17 research findings support the importance of recommending treatment to the concept of a goal; here, the goal is to control inflammation and improve emotional health.
The Continuous Nursing Model Significantly Improved Patients’ Coping Styles
The main characteristics of IBD are recurrent diarrhoea, abdominal pain, haematochezia and other clinical manifestations. The course of IBD is prolonged and cannot be cured entirely. Due to the long treatment period and high cost, patients have poor adherence to treatment and low trust in medical staff, resulting in negative emotions, such as patients becoming evasive and submissive. Another important phenomenon in the incidence of IBD is its genetic tendency; it is not only a polygenic disease but also a genetically heterogeneous disease (caused by different genes in different people).18 Therefore, patients with IBD often feel sorry for themselves and lack confidence. The results of this study showed that, in the control group, the face, avoidance and yield scores were 19.10 ± 3.16, 16.69 ± 2.03 and 9.83 ± 3.04, respectively. In contrast, the observation group’s face, avoidance and yield scores were 20.90 ± 2.36, 14.31 ± 2.22 and 7.18 ± 1.45, respectively. These results demonstrate that the continuous nursing model could guide patients in actively confronting the disease and choosing to overcome it rather than give up, thereby improving their medical coping style. Additionally, continuous care could enhance the patient’s beliefs and transform physical behaviour, helping them to take action and a positive approach to living healthily and actively. Through positive psychological intervention, the patient’s coping style with the disease and medication compliance was improved; furthermore, their confidence in their treatment was enhanced. These results are consistent with those of Bian et al.19 It has also been shown that continuous care can enhance patients’ self-efficacy and improve their subjective initiative, thereby enhancing compliance and optimising their treatment and care.8
The Continuous Nursing Model Improved Patients’ Sleep Quality
Patients with IBD are prone to insomnia due to the high number of stools, haematochezia, concerns about the outcome of the disease and the related heavy economic burden. Therefore, most patients have poor sleep quality. The results of this study show that the sleep quality score after the intervention was 4.17 ± 2.65 in the control group and 3.53 ± 2.05 in the observation group. Therefore, continuous and precise nursing and standardised treatment protocols improved the effects of patients’ treatment, including physical conditions and sleep quality, reducing their psychological burden. According to Marinelli et al,20 sleep quality is mainly related to patients’ emotional state, disability and quality of life. Gastroenterologists and psychologists should work together to assess emotional states during clinical visits to better manage patients with IBD.
The Continuous Nursing Model Improved Patients’ Quality of Life
Activity level is a critical factor affecting the quality of life of patients with IBD. This study showed that the control group’s quality of life score after the intervention was 194.17 ± 15.05; in contrast, the observation group’s score was higher at 202.63 ± 15.76. These results are consistent with those reported by Qi and Wang.21 The results suggest that the continuous nursing model’s standardised treatment and ongoing nursing effectively reduced patients’ disease activity levels, making them feel relaxed and physically and mentally happy, thus improving their quality of life.
Limitations
The sample size of this study was small, and the duration of the continuous care measures was short. These factors may have negatively impacted the results. Future studies should expand the sample size and extend the duration of the continuous nursing care interventions to improve the quality of the results.
Conclusion
In conclusion, this study’s results showed that continuous nursing effectively promoted the self-management of patients with IBD, reduced their uncertainty about the disease and improved their coping style. Furthermore, patients’ sleep quality, self-care ability and quality of life improved, and their physical pain and mental anguish were reduced. In addition, continuous nursing promoted the reintegration of patients with IBD into society and reduced medical costs.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Yijishan Hospital, Wannan Medical College. We obtained signed informed consent from the participants in this study.
Funding
Key Scientific Research Project of Anhui Universities SK2020A0369.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fabián O, Kamaradová K. Morphology of inflammatory bowel diseases (IBD). Cesk Patol. 2022;58(1):27–37. English. PMID: 35387455.
2. Glassner KL, Abraham BP, Quigley EMM. The microbiome and inflammatory bowel disease. J Allergy Clin Immunol. 2020;145(1):16–27. PMID: 31910984. doi:10.1016/j.jaci.2019.11.003
3. Wang Z, Yang L, Sun S. Effect of intestinal microbiota transplantation on intestinal flora and inflammatory factor levels in patients with ulcerative colitis. Infect Drug Resist. 2023;16:1183–1191. PMID: 36879853; PMCID: PMC9985455. doi:10.2147/IDR.S394614
4. Ananthakrishnan AN, Kaplan GG, Ng SC. Changing global epidemiology of inflammatory bowel diseases: sustaining health care delivery into the 21st century. Clin Gastroenterol Hepatol. 2020;18(6):1252–1260. PMID: 32007542. doi:10.1016/j.cgh.2020.01.028
5. Halper-Stromberg A, Dalal SR. The role of the microbiome in the etiology of inflammatory bowel diseases. Clin Colon Rectal Surg. 2023;36(2):120–126. PMID: 36844713; PMCID: PMC9946717. doi:10.1055/s-0042-1760680
6. Zhao Y, Zhu X. Continuous care education for patients with inflammatory bowel disease. World Chin J Dig. 2019;27(3):197–202. doi:10.11569/wcjd.v27.i3.197
7. Lou F. Observation of the effect of continuation care on self-efficacy and quality of life score in patients with inflammatory bowel disease. World Latest Med Inf. 2019;19(A0):244–245. doi:10.19613/j.cnki.1671-3141.2019.100.128
8. Wang L, Wang X, Fu Z. Effects of continuing care on self-efficacy and life quality in patients with inflammatory bowel disease. J Hubei Univ Nationalities. 2018;35(01):32–35. doi:10.13501/j.cnki.42-1590/r.2018.01.010
9. Yu J, Ren Q, Yao W. Effect of continuous nursing on self-efficacy and quality of life of patients with inflammatory bowel disease. J Qilu Nurs. 2022;28(13):53–56. doi:10.3969/j.issn.1006-7256.2022.13.016
10. Ye Z, She Y, Liang M, et al. Revised Chinese version of mishel uncertainty in illness scale: development, reliability and validity. China Gen Med. 2018;21(9):1091–1097. doi:10.3969/j.issn.1007-9572.2018.00.068
11. Shen X, Jiang Q. Report on application Chinese version of MCMQ in 701 patients. Chin J Behav Med Sci. 2000;9(1):18. doi:10.3760/cma.j.issn.1674-6554.2000.01.008
12. Lu T, Li Y, Xia P, Zhang G, Wu D. Analysis on reliability and validity of the Pittsburgh Sleep Quality Index. Chongqing Med J. 2014;43(03):260–263. doi:10.3969/j.issn.1671-8348.2014.03.002
13. Zhou W, You L, Li Y, Chen B. The reliability and validity of inflammatory bowel disease questionnaire in Chinese version. Int J Nurs. 2006;25(08):620–622. doi:10.3760/cma.j.issn.1673-4351.2006.08.020
14. Sreevastava DK, Verma RN, Verma R. A randomized controlled trial comparing gastro-laryngeal tube with endotracheal intubation for airway management in patients undergoing ERCP under general anaesthesia. Med J Armed Forces India. 2019;75(2):146–151. PMID: 31065182; PMCID: PMC6495098. doi:10.1016/j.mjafi.2018.01.006
15. Wang Y, Chen Y. Correlations among the uncertainty in illness, anxiety and depression in patients with Crohn’s Disease. Nurs J Chin PLA. 2019;36(3):20–23. doi:10.3969/j.issn.1008-9993.2019.03.005
16. Kucharzik T, Ellul P, Greuter T, et al. ECCO guidelines on the prevention, diagnosis, and management of infections in inflammatory bowel disease. J Crohns Colitis. 2021;15(6):879–913. Erratum in: J Crohns Colitis. 2022 Aug 16; PMID: 33730753. doi:10.1093/ecco-jcc/jjab052
17. Keefer L, Bedell A, Norton C, Hart AL. How should pain, fatigue, and emotional wellness be incorporated into treatment goals for optimal management of inflammatory bowel disease? Gastroenterology. 2022;162(5):1439–1451. PMID: 34995528. doi:10.1053/j.gastro.2021.08.060
18. Chen J, Geng J, Wang J, et al. Associations between inflammatory bowel disease, social isolation, and mortality: evidence from a longitudinal cohort study. Therap Adv Gastroenterol. 2022;15:17562848221127474. PMID: 36199290; PMCID: PMC9528002. doi:10.1177/17562848221127474
19. Bian J. Continuous knowledge support to improve the quality of life of patients with inflammatory bowel disease (IBD). J Clin Med Lit. 2018;5(65):190–191. doi:10.3877/j.issn.2095-8242.2018.65.141
20. Marinelli C, Savarino EV, Marsilio I, et al. Sleep disturbance in inflammatory bowel disease: prevalence and risk factors - A cross-sectional study. Sci Rep. 2020;10(1):507. PMID: 31949257; PMCID: PMC6965196. doi:10.1038/s41598-020-57460-6
21. Qi Y, Wang A. Analysis of the current status and influencing factors of the quality of life in patients with inflammatory bowel disease. J Nurs Train. 2020;35(24):2297–2300. doi:10.16821/j.cnki.hsjx.2020.24.020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
Fatigue, Physical Activity, and Quality of Life in Patients with Inflammatory Bowel Disease: A Cross-Sectional Study
Qiao R, Zhou Y, Ding T, Jiang X
International Journal of General Medicine 2024, 17:49-58
Published Date: 8 January 2024
Correlation Between Illness Uncertainty in Caregivers of Patients with Liver Cancer, Their Coping Styles, and Quality of Life
Wang X, Hu JX, Wang Y, Wang F, Wu X, Wang F, Zhao YC, Wang XL, Zhang LL
Journal of Multidisciplinary Healthcare 2024, 17:1541-1548
Published Date: 9 April 2024
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024
The Sequelae and Moderators of Influence of Dandruff on Mental Health Among Mainland Chinese Adults
Chan CS, Smith T, He Z, Garter C
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1333-1346
Published Date: 11 June 2024