Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Serum Free Radical Scavenging Capacity Profiles of Patients with Chronic Obstructive Pulmonary Disease
Authors Sakaguchi K, Yoshikawa M, Fujita Y, Yamamoto Y, Ibaraki T, Fujioka N, Osa T, Yamauchi M ![]() , Ichikawa H, Muro S
, Ichikawa H, Muro S ![]()
Received 9 September 2022
Accepted for publication 27 March 2023
Published 19 April 2023 Volume 2023:18 Pages 615—624
DOI https://doi.org/10.2147/COPD.S385780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Kazuhiro Sakaguchi,1 Masanori Yoshikawa,1 Yukio Fujita,1 Yoshifumi Yamamoto,1 Takahiro Ibaraki,1 Nobuhiro Fujioka,1 Takao Osa,1 Motoo Yamauchi,1 Hiroshi Ichikawa,2 Shigeo Muro1
1Department of Respiratory Medicine, Nara Medical University, Kashihara, Nara, Japan; 2Major of Medical Life Systems, Graduate School of Life and Medical Sciences, Doshisha University, Kyotanabe, Kyoto, Japan
Correspondence: Masanori Yoshikawa, Department of Respiratory Medicine, Nara Medical University, 840 Shijo-cho, Kashihara, Nara, 634-8522, Japan, Tel +81-744-22-3051, Fax +81-744-29-0907, Email [email protected]
Background: Oxidative stress is an important mechanism for the development and progression of chronic obstructive pulmonary disease (COPD). It may also contribute to systemic manifestation in patients with COPD. Reactive oxygen species (ROS) including free radicals play a crucial role in oxidative stress in COPD. The aims of this study were to determine serum scavenging capacity profile against multiple free radicals and to evaluate its correlation with pathophysiology, exacerbations, and prognosis in patients with COPD.
Methods: Serum scavenging capacity profile against multiple free radicals comprising hydroxyl radical (•OH), superoxide radical (O2−•), alkoxy radical (RO•), methyl radical (•CH3), alkylperoxyl radical (ROO•), and singlet oxygen (1O2) was assessed using the multiple free-radical scavenging method in 37 patients with COPD (mean age, 71 years; mean forced expiratory volume in 1 s, 55.2% predicted). The severity of emphysema was evaluated by Goddard classification on chest computed tomography. Exacerbations were recorded prospectively for 1 year and the overall mortality was assessed 5 years after the initial assessment.
Results: •OH scavenging capacity was significantly decreased (p < 0.05) and O2−• and •CH3 scavenging capacity tended to decrease in patients with COPD compared to that in healthy controls. On the other hand, ROO• scavenging capacity tended to increase. In addition, RO• scavenging capacity was associated with severity of emphysema (p < 0.05) and exacerbation frequency (p < 0.02). There was a difference in the profile of the scavenging capacity between survived and deceased patients with COPD for 5 years after initial assessment.
Conclusion: Characteristic profile of free radical scavenging capacity can provide insight into the pathophysiology and prognosis of patients with COPD.
Keywords: oxidative stress, free radicals, the multiple free-radical scavenging method, pathophysiology, exacerbations, prognosis
Introduction
Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease that is characterized by persistent airflow limitation and is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases.1 Although cigarette smoking is the most common risk factor of COPD, the mechanisms of the amplified inflammation in these patients are not fully elucidated.
Oxidative stress has been shown to play a crucial role to the development and progression of COPD.2,3 Oxidative stress may be an important amplifying mechanism in the inflammatory response in COPD of the lung.4,5 The enhanced inflammation through transcription factor such as nuclear factor κB (NF-κB) impair the function of antiproteases including α-1 antitrypsin and secretory leukoprotease inhibitor and induce the secretion of matrix metaloproteinases (MMPs), serine proteinases including neutrophil elastase, cathepsin G and proteinase-3 which contribute to alveolar destruction and development of emphysema.6,7
Systemic inflammation is also found in patients with COPD and it may contribute to systemic manifestation and could worsen comorbidities. Patients with persistent systemic inflammation had increased mortality and more frequent exacerbations.6
Oxidative stress including damage to lipids, proteins and nucleic acids originally occurs when oxidants overwhelm the capacity of antioxidants. Numerous biomarkers of oxidant and antioxidant have been investigated in different biological samples such as blood, urine, exhaled breath condensate (EBC) and induced sputum. The majority of these studies reported that higher levels of oxidants, especially lipid and protein oxidation products and diminished antioxidant defenses, particularly protein SH groups, glutathione (GSH), and antioxidant enzymes such as superoxide dismutase (SOD) and catalase in these samples of patients with COPD compared to the healthy controls. However, suitable biomarkers to accurately diagnose COPD and to monitor its progression have not yet been identified.8
Reactive oxygen species (ROS) and reactive nitrogen species (RNS) in cigarette smoke and air pollutants induce exogenous oxidative stress. Free radicals are very reactive, and free radical scavenging capacity is considered a defensive capacity against oxidative stress.9,10 Although free radicals are generally unstable because they retain unpaired electrons, the electron spin resonance (ESR) spin-trapping method, originally proposed by Janzen et al,11 is used to detect short-lived radicals such as ROS and RNS. Fundamentally, spin-trapping reagents react with short-lived radicals, which are subsequently changed to long-lived radicals called spin-adducts. The ESR method utilizing 5-(2,2-dimethyl-1,3-propoxycyclophosphoryl)-5-methyl-1-pyrroline N-oxide (CYPMPO)11 as a spin-trapping reagent is called the multiple free-radical scavenging (MULTIS) method12 that can be applied to assess the free radical scavenging capacity of serum. The characteristic changes in the scavenging capacity have been identified by MULTIS method in chronic kidney disease (CKD)13 and in autism spectrum disorder.14 These studies concluded that MULTIS profile may become a useful diagnostic tool in these patients. However, free radical scavenging capacity has not yet been evaluated by MULTIS method in patients with COPD.
The aim of the present study was to determine whether the characteristic changes in free radical scavenging capacities are observed in patients with stable COPD and to investigate the association between the scavenging capacities and pathophysiology and mortality in among these patients.
Materials and Methods
Study Design and Subjects
Patients were recruited from the Nara Medical University Hospital in this prospective study. Consecutive patients with stable COPD who visited our hospital were eligible for enrollment. COPD was diagnosed according to the definition of Global Initiative for Chronic Obstructive Lung Disease (GOLD).1 We excluded patients who had known heart disease, malignancy, cor pulmonale, or any other severe condition of inflammatory or metabolic disease. In addition, the patients with asthma-COPD overlap syndrome (ACO) were excluded. After the initial assessment, the patients were scheduled to visit our hospital every month or every other month for follow-up visits. Exacerbations were recorded prospectively for 1 year. The overall mortality was assessed 5 years after the initial assessment.
The local ethics committee of Nara Medical University approved the study and all subjects gave written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Monitoring and Definition of Exacerbation
After the initial assessment, the patients were scheduled to visit our hospital every month or every other month for follow-up visits. An exacerbation was defined as an increase in respiratory symptoms (dyspnea, cough, and sputum production) that was beyond normal day-to-day variation and required additional treatment with bronchodilator inhalation, antibiotics, and/or a systemic corticosteroid.1 The attending physician checked for occurrence of exacerbations based on these criteria at each visit, and patient was followed up for 1 year. Patients who experienced ≥2 exacerbations per year were classified as frequent exacerbators.
Pulmonary Function Tests
All patients underwent pulmonary function testing. Vital capacity (VC), forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), residual volume (RV), and total lung capacity were measured using a pulmonary function instrument with computer processing (FUDAC 70, Fukuda Denshi, Tokyo, Japan) and the FEV1/FVC ratio was calculated. Lung volumes were determined using the helium gas dilution method, and the diffusing capacity for carbon monoxide (DLCO) was measured using the single-breath method. The values obtained were expressed as a percentage of the predicted values.15
Measurement of Serum Free Radical Scavenging Capacity
Blood samples from patients with COPD were collected at initial assessment. Control blood samples were taken from 8 healthy controls (male: 6, female: 2, age: 69.8±4.7 years, body mass index [BMI]: 22.3 ± 2.4 kg/m2) who performed regular exercise at the gym in Doshisha University. Serum samples were immediately separated and stored at –80℃ until analysis. The serum scavenging capacities of different free radical species including hydroxyl radical (•OH), superoxide radical (O2−•), alkoxy radical (RO•), methyl radical (•CH3), alkylperoxyl radical (ROO•), and singlet oxygen (1O2) were measured according to the method reported by Kamibayashi et al.12 The scavenging capacity of each free radical was measured using an X-band Microwave Unit ESR instrument (RE SERIES, JEOL, Tokyo, Japan) under the conditions shown in Table 1. Hydrogen peroxide (H2O2), riboflavin, t-butyl hydroperoxide, rosebengal, 4-hydroxy-2,2,6,6-tetra-methylpiperidine (4-OH-TEMP), buffers and biochemical regents were obtained from Wako Pure Chem. Ind. Ltd. (Osaka, Japan). 2,2’-azobis (2-amidinopropane) hydrochloride (AAPH) were purchased from Funakoshi Co. (Tokyo, Japan). WIN-RAD (Radical Research Inc, Version 1.30, Tokyo, Japan) was used for data analysis. In the MULTIS method, ultraviolet or visible light irradiation of precursors can generate various radicals such as •OH, O2−•, RO•, •CH3, ROO•, and 1O2. Since free radicals are short-lived and disappear quickly, they are trapped by the spin-trapping agents listed in Table 1, converted to stable spin adducts, and the spectra of the spin adducts are analyzed using WIN-RAD. Briefly, we prepared a solution containing 20 µL of 1:5 diluted serum samples, 100 µL of 200mM phosphate buffer, 20 µL of 100 mM CYPMPO, 20 µL of 10 mM dimethylene triamine pentaacetic acid (WAKO, Osaka, Japan), 20 µL of distilled water, and 20 µL of 100 mM H2O2 for hydroxy radical generation. This solution was exposed to ultraviolet light (SUPERCURE-203, SAN-EI ELECTRIC, Osaka, Japan) for 5 s (total reflection mirror, hot-cut filter). CYPMPO was used as a spin-trapping reagent to capture any radicals produced in the solution. The height of the fifth signal of each sample was recorded. The fifth signal of control was set to 100% and compared with each sample to obtain a relative ratio. A standard calibration curve was determined using glutathione disulfide (WAKO, Osaka, Japan). The relative ratios of the control and each concentration were set as I0 and I, respectively, when glutathione disulfide was added to each sample. For other free radicals, such as O2−•, RO•, •CH3, ROO•, and 1O2 each suitable reaction mixture was used and measured for each condition. Typical spectrometer settings were as follows: field modulation width, 0.1 mT; microwave power, 6 mW; field scan width and rate, ±7.5 mT/2 min; and time constant, 0.1 s.
 |
Table 1 Measurement Conditions of Each Free Radical Scavenging Capacity |
Emphysematous Change Evaluated by Chest Computed Tomography
High resolution computed tomography (HRCT) was performed for all the patients to detect low attenuation area characterized as pulmonary emphysema in COPD. Computed tomography scans were performed using a multidetector row scanner (Aquilion 64; Toshiba; Tokyo, Japan) with technical parameters of 120 kVp, 350-mm field of view, lung reconstruction algorithm, and no contrast media. During the scanning, the subjects held their breath after a deep inspiration in the supine position. The severity of emphysema was evaluated by Goddard classification,16 a visual scale by which areas of low attenuation area were scored for each lung field of HRCT. Lung regions were graded as follows: no emphysema (score 0), ≤25% emphysema (score 1), ≤50% emphysema (score 2), ≤75% emphysema (score 3), and >75% emphysema (score 4). Scores of the six regions were summed to obtain total scores, giving a minimum total score of 0 and a maximum of 24. The patients were classified as having mild (<8 points), moderate (8–15), or severe (≥16) COPD. To evaluate pulmonary emphysema quantitatively, two chest physicians, masked to subject identities and other characteristics were engaged. The average of two values of Goddard score was used as an assessment of severity of emphysema.
Statistical Analysis
The values obtained are expressed as means ± SD. The differences in free radical scavenging capacity between stable patients with COPD and healthy controls were determined through unpaired Student’s t-test. Parameters were compared between three or four groups by using one-way analysis of variance followed by the Bonferroni multiple comparison test. Correlation between pulmonary function variables and individual free radial scavenging capacity was determined by Pearson’s correlation coefficient. P values <0.05 were considered statistically significant. All statistical tests were carried out using SPSS for Windows version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient Characteristics
The patients’ characteristics are summarized in Table 2. Thirty-seven patients with stable COPD (35 men and 2 women) were enrolled. Mean age was 70.9±8.9 years. Of the 37, 22 (59%) had mild-to-moderate airflow limitation and 15 (41%) had severe or very severe airflow limitation. The mean value on the modified Medical Research Council scale was 2.2±1.0. At enrollment, 33 patients (89%) used long-acting muscarinic antagonists and 18 patients (49%) used long-acting beta-agonists. In addition, 13 patients (35%) were treated with combination of inhaled corticosteroids and long-acting beta-agonists. 14 patients (38%) used theophylline. No patients used oral corticosteroids.
 |
Table 2 Patients Characteristics |
Serum Free Radical Scavenging Capacity
Serum free radical scavenging capacities in control subjects and patients with COPD according to the GOLD classification of airflow limitation severity are shown in Table 3. •OH scavenging capacity was significantly decreased in patients with COPD compared to control subjects (p < 0.05). However, there was no significant association between •OH scavenging capacity and severity of airflow limitation. O2−• and •CH3 scavenging capacity tended to decrease in patients with COPD compared to healthy controls. In contrast, ROO• scavenging capacity tended to increase. Percent changes in the scavenging capacity of patients with COPD compared to healthy controls in each free radical species are calculated. A radar chart illustration of the relative scavenging capacity data is shown in Figure 1. In patients with COPD, ROO• scavenging capacity was higher than in controls, whereas •OH scavenging capacity was lower.
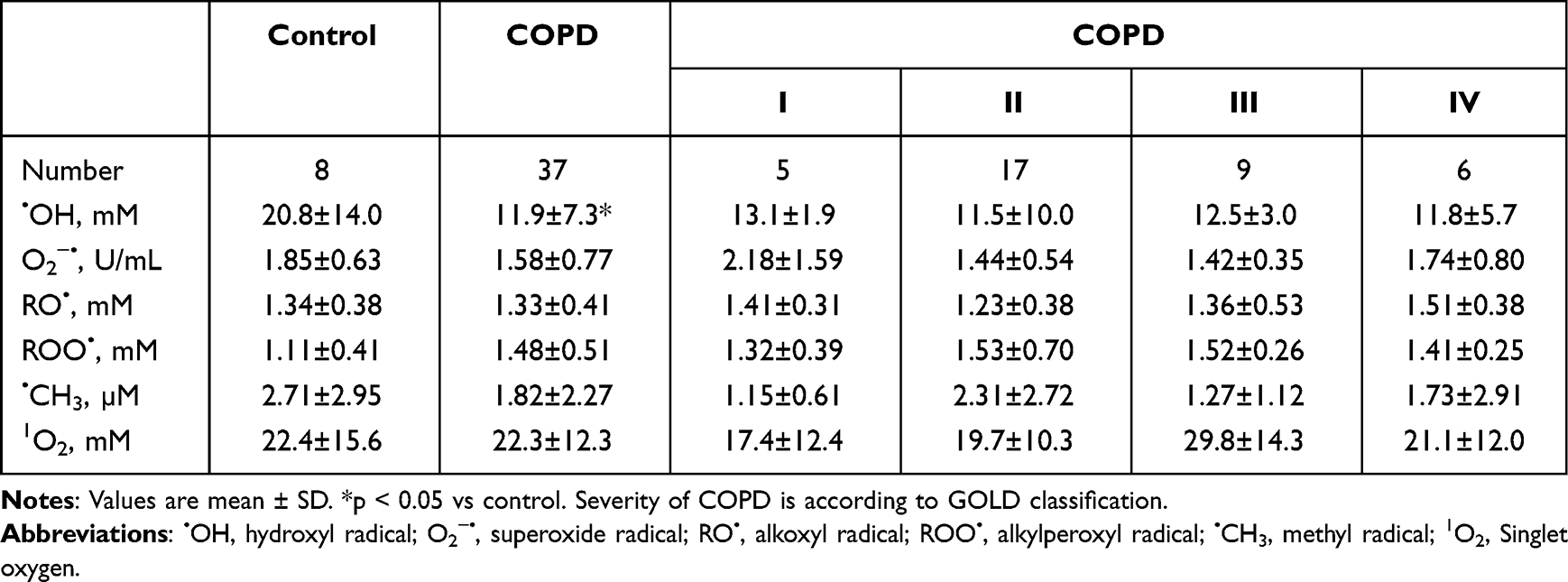 |
Table 3 Free Radical Scavenging Capacity and Severity of COPD |
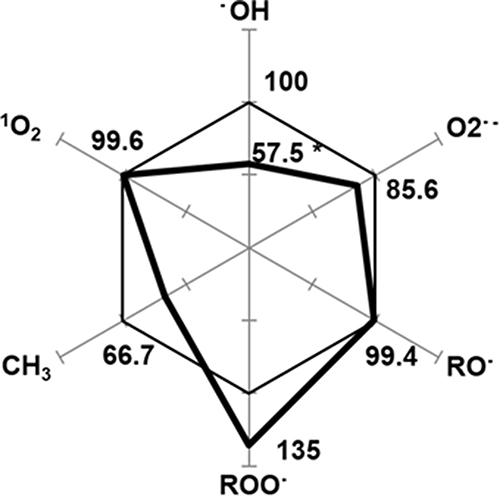 |
Figure 1 A radar chart illustration of the relative scavenging capacity data listed in Table 1. Percent changes in the capacity of COPD patients are shown in each free radical species. *p < 0.05 vs control subjects. Abbreviations: ・OH, hydroxyl radical; O2−・, superoxide radical; RO・, alkoxyl radical; ROO・, alkylperoxyl radical; ・CH3, methyl radical; 1O2, Singlet oxygen. |
Association Between Pulmonary Function Variables and Serum Free Radical Scavenging Capacity
•OH scavenging capacity was significantly correlated with %VC (r = 0.375, p = 0.026). In addition, RO• scavenging capacity was significantly correlated with %RV (r = 0.374, p = 0.029). There was no significant correlation between other free radical scavenging capacities, such as O2−•, ROO•, •CH3, and 1O2 and pulmonary function including %VC, %RV, and %DLCO.
Association Between Pulmonary Emphysema and Serum Free Radical Scavenging Capacity
Serum free radical scavenging capacities according to Goddard classification are shown in Table 4. RO• scavenging capacity was significantly associated with Goddard classification (p = 0.0401). RO• scavenging capacity in the severe group (1.46 ± 0.36 mM) was higher than that in the mild (1.21 ± 0.46 mM) and moderate (1.06 ± 0.41 mM) groups. Other free radical scavenging capacities for •OH, O2−•, ROO•, •CH3, and 1O2 were not associated with Goddard classification.
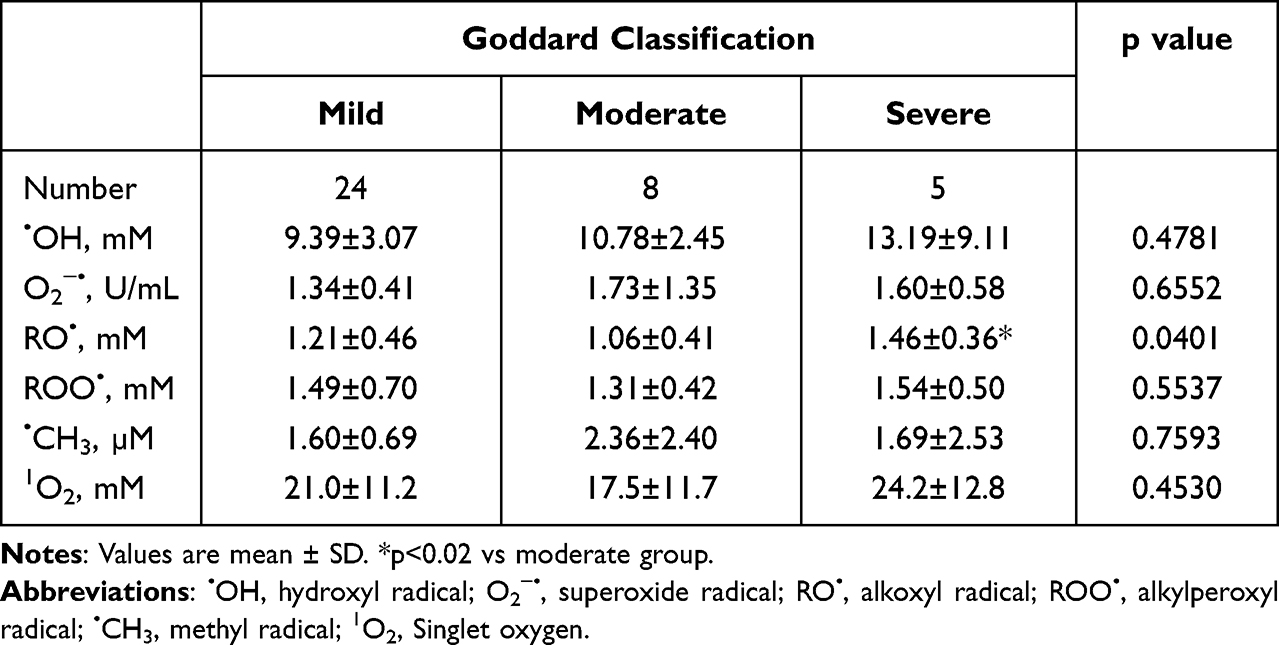 |
Table 4 Relationship Between Free Radical Scavenging Capacity and Goddard Classification |
Association Between Exacerbation Frequency and Serum Free Radical Scavenging Capacity
Exacerbation frequency and free radical scavenging capacity are presented in Table 5. Exacerbation frequency was significantly associated with RO• scavenging capacity (p = 0.0129). Namely, RO• scavenging capacity in the one exacerbation group (1.68 ± 0.34 mM) was significantly higher than that in the no exacerbation group (1.27 ± 0.32 mM). In contrast, RO• scavenging capacity in the frequent exacerbation group (1.09 ± 0.62 mM) was significantly lower than that in the one exacerbation group. Other free radical scavenging capacities for •OH, O2−•, ROO•, •CH3, and 1O2 were not associated with exacerbation frequency.
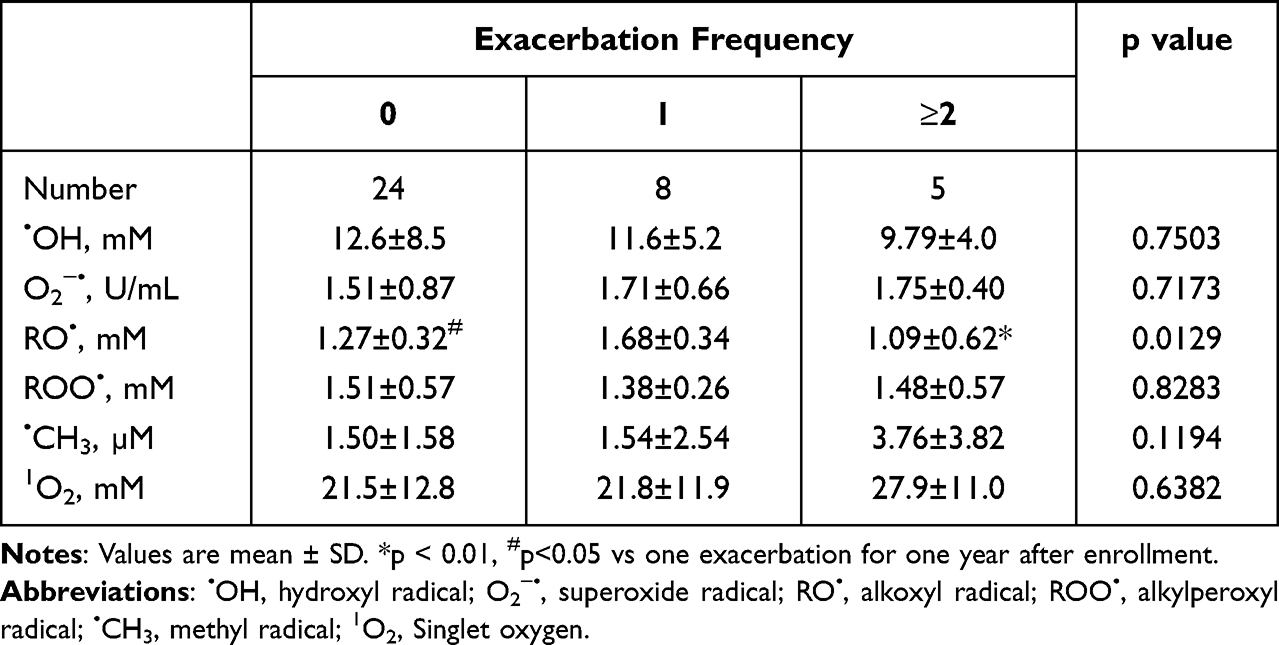 |
Table 5 Relationship Between Free Radical Scavenging Capacity and Exacerbation Frequency |
Association Between Serum Free Radical Scavenging Capacity and Mortality
During the 5 follow-up years, 12 of the 37 (32.4%) patients died. 1O2 scavenging capacity in the deceased patients (28.1 ± 16.0 mM) after initial assessment for 5 years was significantly higher than that in survived patients (19.2 ± 8.7 mM). There was an apparent difference in pattern of free radical scavenging capacity between survived and deceased patients with COPD (Figure 2).
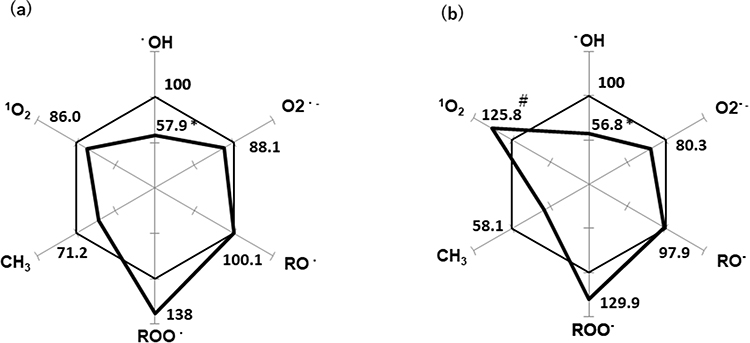 |
Figure 2 A radar chart illustration of the relative scavenging capacity. Percent changes in the capacity of COPD patients are shown in each free radical species. (a) Survived patients with COPD, (b) Deceased patients with COPD. *p < 0.05 vs control, #p<0.05 vs survived patients with COPD. Abbreviations:・OH, hydroxyl radical; O2−・, superoxide radical; RO・, alkoxyl radical; ROO・, alkylperoxyl radical; ・CH3, methyl radical; 1O2, Singlet oxygen. |
Discussion
In the present study, the characteristic changes in free radical scavenging capacity of serum in patients with COPD were noted. In particular, a significant decrease in scavenging capacity of •OH was noted, whereas O2−• and •CH3 showed a trend of decreasing scavenging capacity in patients with COPD. Contrastingly, ROO• scavenging capacity tended to increase, and RO• scavenging capacity was correlated with the severity of pulmonary emphysema and exacerbation frequency. There was a difference in profile of the scavenging capacity between survived and deceased patients with COPD for 5 years after initial assessment. To our knowledge, this is the first report of free-radical scavenging capacity in patients with stable COPD.
ROS can react with biological molecules such as lipid, protein, DNA, RNA, and mitochondrial DNA and lead to epithelial cell injury and death, which contribute to COPD development. The •OH radical is one of the most reactive chemical agents, and there are no effective detoxification strategies. It may act as a physiological intracellular agent that, in excess, is considered a risk factor for several respiratory diseases.17 In the present study, •OH scavenging capacity was decreased even in patients with mild COPD, suggesting that the decreased •OH scavenging capacity was associated with the development of COPD.
In patients with CKD, a characteristic scavenging-profile including decreased scavenging capacity in •OH, •CH3, and 1O2, and increased in O2−•, RO•, and ROO• have been previously reported.13 However, a different pattern in scavenging capacity of O2−•, RO•, and 1O2 was observed in patients with COPD in this study. In particular, we noted a decrease in scavenging capacity in O2−•. This may be because O2−• has been associated with nitrogen oxide (NOx) metabolism, which can contribute to the development of COPD. Although the activity of xanthine oxidase, which produces O2−•, was significantly elevated in the airway in COPD,18,19 increased O2−• may react with NO, suggesting that the scavenging capacity of O2−• was decreased because O2−• was extremely consumed to react with increased NO in the airway of patients with COPD.
Recently, a characteristic scavenging profile by MULTIS method was reported in autism spectrum disorder.14 These previous studies concluded that it may become a useful diagnostic tool in patients with CKD13 and autism spectrum disorder.14 We assume that the profile of multiple radical scavenging capacity may not only be associated with the development of COPD but also become one of the diagnostic tool of COPD. Large scale study is needed to test this hypothesis.
In the present study, biomarkers of oxidative stress including ROS and antioxidant were not evaluated. Numerous biomarkers of oxidative stress and antioxidant have been evaluated in a variety of biological samples such as blood, urine, EBC and sputum. However, they are unable to be sensitive indicators of oxidative stress because most of the biomarkers are end products of oxidative stress. In addition, direct measurement of ROS levels is difficult due to their short lifespan and rapid reactivity. Suitable biomarkers to accurately diagnose COPD and monitor its progression have not yet been identified. Multiple free radical scavenging capacity measured in this study may reflect a response to various oxidative stress including ROS and a variety of antioxidant capacity. Therefore, we can estimate the magnitude of oxidative stress by free radical scavenging capacity without measurements of biomarkers of oxidant and antioxidant.
The RO• scavenging capacity was increased in the severe emphysema group. RO• is as highly reactive as •OH, and is closely related in lipid peroxidation. Malondialdehyde (MDA), end product of lipid peroxidation, has been shown to increase in the blood of patients with COPD depending on the severity of the disease.20 MDA inactivates many cellular proteins by generating cross-linkages.21 This may stimulate pulmonary inflammation,22 promoting alveolar wall destruction and emphysema development leading to the pathogenesis of COPD. It is assumed that RO• scavenging capacity was increased as an antioxidative mechanism against lipid peroxidation in the patients with severe emphysema, but an oxidative burden overwhelmed the antioxidative potential in these patients. The severity of emphysema was not assessed % low attenuation area (%LAA) but Goddard classification. However, we consider Goddard classification as easily used and reliable method to evaluate emphysematous change in COPD.
The exacerbation frequency and RO• scavenging capacity were correlated among patients with COPD. In patients with COPD, RO• production may be elevated due to an increase in lipid peroxidation cause by increased •OH. High plasma MDA levels have been reported in patients with exacerbated disease.23,24 In addition, Trolox equivalent antioxidant capacity in plasma was lower in patients with exacerbated disease than in those with stable disease.23,25 Since Trolox is also utilized to measure RO• scavenging capacity, lower Trolox equivalent antioxidant capacity may be attributed to decreased RO• scavenging capacity. Therefore, it is assumed that patients with a decreased RO• scavenging capacity may be susceptible to exacerbations. A recent systematic review has described the presence of an imbalance between oxidant and antioxidant molecules in favor of the former in exacerbation of COPD.26
In the present study, RO• scavenging capacity in the one exacerbation group was significantly higher than that in the no exacerbation group. In contrast, RO• scavenging capacity in the frequent exacerbation group was significantly lower than that in the one exacerbation group. These results seem to be inconsistent. Basically, the scavenging capacity is determined against oxidative stress. We assume that in no exacerbation group, oxidative stress itself was lower than that in one exacerbation group. In contrast, frequent exacerbation group could not enhance the scavenging capacity against their oxidative stress compare to one exacerbation group. However, further study is required to elucidate precise mechanisms.
Although there was no difference in RO• scavenging capacity between patients with COPD and controls, it was associated with the severity of emphysema and exacerbation frequency. RO• is considered to be produced through •OH. Therefore, we speculated that •OH acts as the first step in the development of COPD, and RO• plays a role in determining the phenotype of COPD. Further studies are needed to clarify the relationship between RO• and the pathophysiology of COPD.
We found the distinctly different profile in free radical scavenging capacity at enrollment between survived and deceased patients with COPD after 5 year follow up. In particular, 1O2 scavenging capacity was significantly increased in deceased patients with COPD, while it was not associated with pathophysiology of COPD. 1O2 is a highly reactive free radical. Recently, 1O2 generated from hydrogen peroxide was shown to provoke oxidative distress resulting in cell death and diseases.27 1O2 scavenging capacity may be associated with a compensatory increase in deceased patients. Oxidative stress play an important role in developing of systemic inflammation of COPD. Persistent systemic inflammation in COPD might contribute to the development and progression of comorbidities such as cardiovascular disease, diabetes, osteoporosis, and lung cancer6 and cause increased mortality and more frequent exacerbations.6 Even though the mechanism of the difference in free radical scavenging capacity between survived and deceased patients with COPD was unclear, the characteristic profile of free radical scavenging capacity may be helpful of predicting the prognosis in patients with COPD.
Our study had some limitations. First, the sample size of COPD or each severity of COPD was small. A validation study is needed to apply the measuring technique of scavenging capacity for patients with COPD. In addition, large scale cohort study is required to confirm our data.
Second, we did not evaluate free radical scavenging capacity of healthy smokers, and the effect of smoking on free radical scavenging capacity was not examined. The effect of smoking on free radical scavenging capacity has not yet been reported. In the present study, there was no significant difference in serum free radical scavenging capacity between current smokers (n=12) and ex-smokers (n=25) (data not shown). Instead, we speculate that characteristic change in free radical scavenging capacity is associated with susceptibility to COPD in smokers.
Third, free radical scavenging capacity in sputum and exhaled breath condensate was not assessed. It is unclear whether our data in serum is consistent with that in the airways.
Conclusion
We revealed the characteristic profile of free radical scavenging capacity of patients with stable COPD by MULTIS method. The profile of the free radical scavenging capacity may be associated with the development of COPD. The characteristic profile related to clinical phenotype of COPD develop severe emphysema and frequent exacerbation was determined. In addition, we found the characteristic profile which may be helpful of predicting the prognosis in patients with COPD.
Acknowledgments
The authors thank Ran Takahashi, Yuki Tatsumi and Yuta Noguchi for their contributions to the data collection using the multiple free-radical scavenging method.
Author Contributions
All authors made a significant contribution to the work reported. KS and MY contributed to the study conception or design, data acquisition, data analysis, and data interpretation. YF, YY, TI, and NF contributed to data acquisition, data analysis, and data interpretation. TO and MY contributed to data analysis and data interpretation. HI and SM contributed to the study conception or design, data analysis and data interpretation. All authors took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
There was no funding obtained to conduct this study.
Disclosure
Dr Shigeo Muro reports grants from ROHTO Pharmaceutical Co., Ltd., personal fees from Novartis Pharma, personal fees from AstraZeneka Japan, personal fees from Nippon Boehringer Ingelheim, personal fees from TEIJIN PHARMA, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. The Global Initiative for Chronic Obstructive Lung disease (GOLD). Executive summary: global strategy for the diagnosis, management, and prevention of COPD; 2020. Available from: http://www.goldcopd.com.
2. MacNee W. Pulmonary and systemic oxidant/antioxidant imbalance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2(1):50–60. doi:10.1513/pats.200411-056SF
3. Barnes PJ. Mediators of chronic obstructive pulmonary disease. Pharmacol Rev. 2004;56(4):515–548. doi:10.1124/pr.56.4.2
4. Lakhdar R, Denden S, Kassab A, et al. Update in chronic obstructive pulmonary disease: role of antioxidant and metabolizing gene polymorphisms. Exp Lung Res. 2011;37(6):364–375. doi:10.3109/01902148.2011.580416
5. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
6. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138:16–27. doi:10.1016/j.jaci.2016.05.011
7. Taniguchi A, Tsuge M, Miyahara N, et al. Reactive oxygen species and antioxidative defense in chronic obstructive pulmonary disease. Antioxidants. 2021;10(10):1537. doi:10.3390/antiox10101537
8. Zinellu E, Zinellu A, Fois AG, et al. Reliability and usefulness of different biomarkers of oxidative stress in chronic obstructive pulmonary disease. Oxid Med Cell Longev. 2020;2020:4982324. doi:10.1155/2020/4982324
9. McCord JM, Wong K. Oxygen free radicals and tissue damage. Excerpta Med. 1979;65:343–351.
10. Halliwell B, Gutteridge JMC. Free Radicals in Biology and Medicine. Tokyo: Japan Scientific Societies Press; 1988.
11. Janzen EG. Spin trapping. Acc Chem Res. 1971;4:31–40. doi:10.1021/ar50037a005
12. Kamibayashi M, Oowada S, Kameda H, et al. Synthesis and characterization of a practically better DEPMPO-type spin trap, 5- (2,2- dimethyl-1,3-propoxy cyclophosphoryl) −5 -methyl-1-pyrroline N-oxide (CYPMPO). Free Radic Res. 2006;40:1166–1172. doi:10.1080/10715760600883254
13. Oowada S, Endo N, Kamayama H, et al. Multiple free-radical scavenging capacity in serum. J Clin Biochem Nutr. 2012;51:117–121. doi:10.3164/jcbn.11-113
14. Hirayama A, Wakusawa K, Fujioka T, et al. Simultaneous evaluation of antioxidative serum profiles facilitates the diagnostic screening of autism spectrum disorder in under-6-year-old children. Sci Rep. 2020;10(1):20602. doi:10.1038/s41598-020-77328-z
15. Kubota M, Kobayashi H, Quanjer PH, et al. Clinical pulmonary functions committee for the Japanese respiratory society, reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig. 2014;52(4):242–250. doi:10.1016/j.resinv.2014.03.003
16. Goddard PR, Nicholson EM, Laszlo G, et al. Computed tomography in pulmonary emphysema. Clin Radiol. 1982;33(4):379–387. doi:10.1016/S0009-9260(82)80301-2
17. Domej W, Oettl K, Renner W. Oxidative stress and free radicals in COPD-implications and relevance for treatment. Int J Chron Obstruct Pulmon Dis. 2014;9:1207–1224. doi:10.2147/COPD.S51226
18. Ichinose M, Sugiura H, Yamagata S, et al. Xanthine oxidase inhibition reduces reactive nitrogen species production in COPD airways. Eur Respir J. 2003;22(3):457–461. doi:10.1183/09031936.03.00052002
19. Komaki Y, Sugiura H, Koarai A, et al. Cytokine-mediated xanthine oxidase upregulation in chronic obstructive pulmonary disease’s airways. Pulm Pharmacol Ther. 2005;18:297–302. doi:10.1016/j.pupt.2005.01.002
20. Kluchova Z, Petrasova D, Joppa P, et al. The association between oxidative stress and obstructive lung impairment in patients with COPD. Physiol Res. 2007;56:51–56. doi:10.33549/physiolres.930884
21. Siu GM, Draper HH. Metabolism of malonaldehyde in vivo and in vitro. Lipids. 1982;17(5):349–355. doi:10.1007/BF02535193
22. Rahman I, Adcock IM. Oxidative stress and redox regulation of lung inflammation in COPD. Eur Respir J. 2006;28:219–242. doi:10.1183/09031936.06.00053805
23. Rahman I, Morrison D, Donaldson K, et al. Systemic oxidative stress in asthma, COPD, and smokers. Am J Respir Crit Care Med. 1996;154(4):1055–1060. doi:10.1164/ajrccm.154.4.8887607
24. Zeng M, Li Y, Jiang Y, et al. Local and systemic oxidative stress status in chronic obstructive pulmonary disease patients. Can Respir J. 2013;20(1):35–41. doi:10.1155/2013/985382
25. Sadowska AM, Luyten C, Vints AM, et al. Systemic antioxidant defences during acute exacerbation of chronic obstructive pulmonary disease. Respirology. 2006;11(6):741–747. doi:10.1111/j.1440-1843.2006.00943.x
26. Zinellu E, Zinellu A, Fois AG, et al. Oxidative stress biomarkers in chronic obstructive pulmonary disease exacerbations: a systematic review. Antioxidants. 2021;10(5):710. doi:10.3390/antiox10050710
27. Sies H. Hydrogen peroxide as a central redox signaling molecule in physiological oxidative stress: oxidative eustress. Redox Biol. 2017;11:613–619. doi:10.1016/j.redox.2016.12.035
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Superoxide Dismutase and Glutathione Reductase as Indicators of Oxidative Stress Levels May Relate to Geriatric Hip Fractures’ Survival and Walking Ability: A Propensity Score Matching Study
Liu M, Yang C, Chu Q, Fu X, Zhang Y, Sun G
Clinical Interventions in Aging 2022, 17:1081-1090
Published Date: 12 July 2022
A Risk Score Based on Immune- and Oxidative Stress-Related LncRNAs Predicts Prognosis in Lung Adenocarcinoma: Insights from in vitro Experiments and Large-Scale Transcriptome Analysis
Liu X, Zhao F, Wang X, Ma Z, Yan H, Lu X, Li S, Zhu H, Gao S
Journal of Inflammation Research 2024, 17:1453-1465
Published Date: 5 March 2024
Bilirubin Elevation During Hospitalization Post Radiofrequency Catheter Ablation of Persistent Atrial Fibrillation: Variation Trend, Related Factors, and Relevance to 1-Year Recurrence
Shao JM, Shen B, Zhou ZX, D'Angelo L, James SM, Lin JF, Zheng C
Clinical Interventions in Aging 2024, 19:817-825
Published Date: 13 May 2024
An Oxidative Stress-Related Prognostic Signature Predicts Treatment Response and Outcomes for Hepatocellular Carcinoma After Transarterial Chemoembolization
Ma H, Yu T, Li ZC, Zhang L, Chen RX, Ren ZG
Journal of Hepatocellular Carcinoma 2024, 11:1569-1580
Published Date: 13 August 2024
Guillain-Barré Syndrome: Progress in Diagnosis, Biomarkers, Neuroimaging and Management
Freiha J, Min YG, Osman C, Rajabally YA
ImmunoTargets and Therapy 2026, 15:390161
Published Date: 2 April 2026