Back to Journals » Patient Related Outcome Measures » Volume 14
Sensitivity for Change Analyses of the Patient-Reported Outcomes in Obesity (PROS) Questionnaire: A Prospective Cohort Study
Authors Hegland PA ![]() , Kolotkin RL, Andersen JR
, Kolotkin RL, Andersen JR ![]()
Received 25 March 2023
Accepted for publication 30 June 2023
Published 1 August 2023 Volume 2023:14 Pages 235—241
DOI https://doi.org/10.2147/PROM.S414144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Pål André Hegland,1 Ronette L Kolotkin,2– 4 John Roger Andersen1,4
1Faculty of Health and Social Sciences, Western Norway University of Applied Sciences, Førde, Norway; 2Department of Family Medicine and Community Health, Duke University School of Medicine, Durham, NC, USA; 3Quality of Life Consulting, PLLC, Durham, NC, USA; 4Centre of Health Research, Førde Hospital Trust, Førde, Norway
Correspondence: Pål André Hegland, Faculty of Health and Social Sciences, Western Norway University of Applied Sciences, Svanehaugvegen 1, Førde, 6812, Norway, Tel +47 90697135, Email [email protected]
Purpose: Many patients seeking bariatric surgery experience reduced health-related quality of life (HRQOL). A simple clinical tool, the Patient-Reported Outcomes in Obesity (PROS), was developed to address patients’ HRQOL concerns during clinical consultations and facilitate meaningful dialogue. The present study aims to explore its sensitivity to change.
Patients and Methods: A prospective study of patients undergoing bariatric surgery was conducted. The patients responded to items on the PROS and the Obesity-related Problems Scale (OP) before surgery and three, 12 and 24 months after surgery. Longitudinal mixed-effects models were applied to estimate the change in PROS and OP scores over time.
Results: Thirty-eight patients were included. A significant change over time was detected for the PROS with the largest effect size at 24 months (effect size − 1.34, p ˂ 0.001), while the corresponding effect size for the OP was − 1.32 (p ˂ 0.001). In all items of the PROS, the majority of patients responded not bothered at 24 months. The items physical activity, pain, sleep and self-esteem showed the largest change in the percentage of patients reporting not bothered from baseline to 24 months after surgery.
Conclusion: The PROS is sensitive to change over time and may be used as a brief, easy to administer tool to facilitate a conversation about obesity-specific quality of life in clinical consultations.
Keywords: health-related quality of life, Patient-Reported Outcomes in Obesity, PROS, patient-centered follow-up, bariatric surgery
Introduction
Bariatric surgery can significantly improve obesity-specific health-related quality of life (HRQOL).1 However, the initial improvement in HRQOL is often shown to decline over time, especially the mental component.2 This highlights the importance of assessing HRQOL over time in clinical consultations.
Several multidimensional questionnaires have been used to assess obesity-specific HRQOL in patients with obesity, including bariatric surgery patients.3 Examples of well-known questionnaires are the Impact of Weight on Quality of Life-Lite questionnaire (IWQOL-Lite),4 the Bariatric Quality of Life Index (BQL)5 and the Bariatric and obesity-specific survey (BOSS).6 Many obesity-related HRQOL questionnaires are lengthy or focus on limited domains of HRQOL. Thus, questionnaires that permit a broad but simple and rapid assessment of HRQOL in patients who undergo bariatric surgery are warranted. In response, the Patient-Reported Outcomes in Obesity (PROS) was developed.7 It is worth mentioning that disease specific measures tend to be highly sensitive to the condition being measured.
The PROS is a brief questionnaire developed to facilitate the clinical conversation in patient-centered follow-up. The questionnaire has been implemented as the principal HRQOL measure in the quality registry for patients undergoing bariatric surgery in Norway, SOReg-N.8 The PROS showed good psychometric properties in cross-sectional studies in Norway, Brazil and Turkey.4,9,10
However, the PROS has not been assessed for sensitivity to change (also often referred to as responsiveness), a crucial feature of an HRQOL instrument. This study aimed to investigate its sensitivity to change over time in patients with severe obesity who underwent bariatric surgery.
Materials and Methods
This prospective cohort study included patients who had undergone bariatric surgery at Førde Hospital Trust, Norway. All patients underwent laparoscopic sleeve gastrectomy (LSG) from February 2018 to January 2022. Our power analyses showed that a minimum of 22 patients would be required to detect a statistical difference equaling one standard deviation for the PROS over time (based on paired t-test, power = 0.9, P = 0.05, and a correlation between scores of 0.4).
The Norwegian Centre for Research Data, Department of Data Protection Services (reference number 282738) approved the study. All patients signed informed consent to participate in research. The study complies with the Declaration of Helsinki.
The patients responded to a clinical feedback system (CFS) before the consultations with a nurse in the bariatric outpatient clinic.11 PROS was one of the questionnaires included in the CFS. Inclusion criteria was patients which had responded to the CFS before surgery, 12 and 24 months after bariatric surgery.
Variables
We collected data on age, biological sex, BMI (kg/m²), and body weight (kg) at baseline, 12 months, and 24 months post-surgery.
The PROS is a obesity-specific multidimensional questionnaire containing eight items assessing physical activity, pain, discrimination, sleep, sex life, social life, work/school, and self-esteem. The patients are asked whether their body weight or shape bothers them in any of these domains. There are four response categories: not bothered (0), mildly bothered (1), moderately bothered (2), and considerably bothered (3). The questionnaire is intended to be used in clinical consultations to facilitate a patient-centered consultation. However, the PROS may also be used for research and can be analyzed through sub-scores and a sum score. The sum score is calculated by summing all items and multiplying by eight; scores < 0.5 indicate no discomfort, 0.5–1.49 mild discomfort, 1.5–2.49 moderate discomfort, and ≥ 2.5 extreme discomfort.7 Figure 1 displays the questionnaire.
 |
Figure 1 The Patient-Reported Outcomes in Obesity (PROS). |
We also used the Obesity-related problems scale (OP), a well-known questionnaire measuring the impact of obesity on psychosocial functioning, which has demonstrated excellent sensitivity to change after bariatric surgery.12,13 The OP questionnaire contains eight items, which asks the patients how bothered they are by obesity in specific social situations. The responses are on a four-point scale. The responses are aggregated on a scale of 0–100, where lower scores indicate less psychosocial bother. OP has been demonstrated to be highly sensitive to change.
Analyses
We performed descriptive analyses on the patients’ characteristics with percentages (%) and number (n) for categorical measures; and mean and standard deviations (SD) for continuous measures. Longitudinal mixed-effects models were used to estimate the change in PROS and OP scores over time. To estimate the effect size for PROS and OP sum score changes over time, we extracted the mean difference at each time point and divided each by the baseline standard deviation. We used the standard criteria proposed by Cohen to judge effect sizes: trivial (< 0.2), small (0.2 to < 0.5), moderate (0.5 to < 0.8), and large (≥ 0.8). To analyze the single items of the PROS, we performed descriptive analyses on the number (%) of patients responding to each of the four response categories at each assessment point. A 1000-repetition bootstrap analysis was added to the mixed effect models for estimating 95% confidence intervals and p-values for change in the PRO-items, as these are on an ordinal scale. P-values are two-sided and are judged as continuous indicators of probability. A p-value < 0.05 were considered statistically significant. The analyses were conducted with IBM SPSS Statistics version 27.14
Results
For demographic information on the included patients, see Table 1. All 38 patients underwent LSG, and almost all patients were female. The mean preoperative BMI was 42.6 (range 35.7–52.2); at 12 months mean BMI was 29.5 (range 23.6–37.9) and at 24 months it was 30.1 (range 23.6–40.0). Six patients were not included due to missing data.
 |
Table 1 Characteristics of the Included Patients (n=38) |
The mean sum score of the PROS at baseline indicated that the patients had mild discomfort, and the mean sum score at 12 and 24 months indicated no discomfort. The effect size showed significant changes at three months, 12 months, and 24 months, with the largest effect size at 24 months. As a reference, the OP showed scores compatible with mild discomfort at baseline and no discomfort at 12 and 24 months after surgery. The effect sizes of the OP also showed significant change over time, however the maximum effect size was at 12 months (Table 2).
 |
Table 2 Mean Score, and Effect Size for Changes Over Time for the PROS and the OP Total Scores |
In Table 3 we present the percentage of patients responding to each of the four categories of each item for each time point. All items show an improvement in that more patients report being not bothered at 12 and 24 months compared to baseline. The items physical activity, pain, sleep and self esteem show the largest difference in patients reporting not bothered from baseline to 24 months after surgery. The item discrimination appears to be experienced less bothersome in this specific population.
 |
Table 3 Percentage of Patients Reporting the Sub-Items of PROS at the Four Measuring Times Presented by Response Category |
In Table 4 we present the sub-item scores over time, and the change scores with 95% CI for final versus first observation.
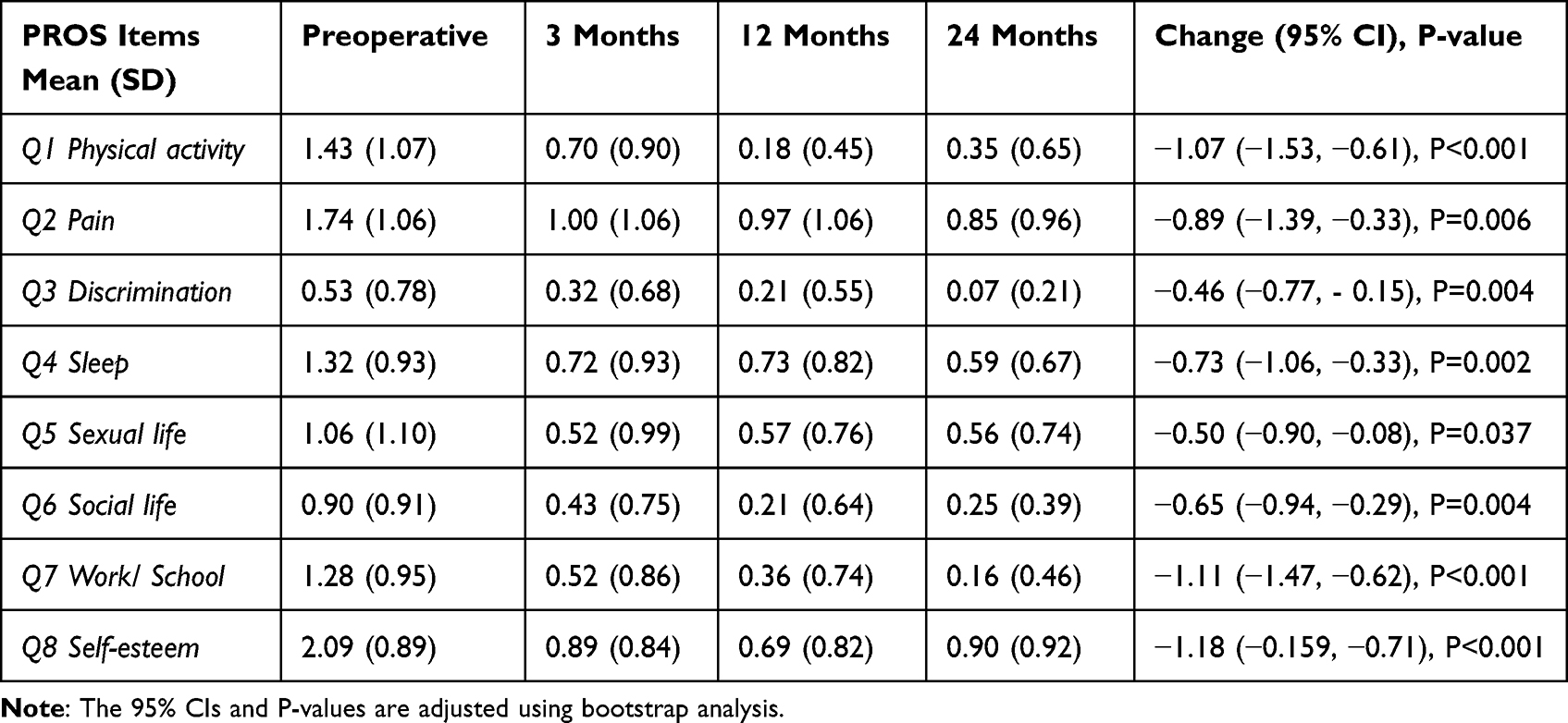 |
Table 4 Mean (SD) PROS Sub-Item Scores Over Time and Change Scores (95% CI) for Final versus First Observation |
Discussion
Previous research showed the PROS to be a reliable and valid of measure obesity-specific quality of life, and the results of the current study indicate that it is also sensitive to change over time. The PROS showed maximum effect at the last measurement point (24 months), suggesting that improvements in obesity-specific HRQOL after bariatric surgery endured. The effect sizes for PROS are comparable with the effect sizes for OP in this study. Unlike the PROS, the effect size for change in the OP was highest at 12 months. Karlsson, Taft15 conducted a controlled study where HRQOL was explored using the OP. During the 10-year follow-up, the peak improvements in the OP occurred after one year. Based on the results from the present study it seems that the PROS measures domains of obesity-specific quality of life that are more sustainable. One possible explanation may be that the OP scale measures only psychosocial functioning, whereas the PROS measures several aspects of HRQOL. However, data beyond two years are needed to establish when the maximum change in effect size is, as many patients experience maximum weight loss around this time.
The effects and consequences of bariatric surgery are more complex than weight loss and nutritional challenges. Both patients and clinicians acknowledge the importance of discussing HRQOL.16 There is therefore a need for brief, easily administered patient-reported measures that facilitate such a discussion. The PROS is a measure that can be used for such purposes because it measures different aspects of HRQOL that are important to patients, and at the same time the measure is brief. A lengthy measure may cause responder fatigue and as a consequence the patient may start responding carelessly to items.17 A recent study conducted in Australia and Aotearoa New Zealand explored the use of patient-reported outcome measures (PROMS) and patient-reported experience measures (PREMS) in bariatric clinics.18 While the majority of the clinics reported having not collected PROMS or PREMS, the respondents thought that PROMS would be useful to enhance patient-clinician communication, to monitor important changes and to get a deeper understanding of the patient’s life in relation to HRQOL.
Since the PROS was included as a measure in the national registry for bariatric surgery in Norway (SOReg-N) in March 2022,8 it was important to determine if it was sensitive to change over time – the aim of this study. A result of incorporating the PROS in the registry is that it may be used both for research purposes (such as examining long-term outcomes across and between bariatric surgery centers throughout Norway) and for clinical purposes (as a tool for facilitating meaningful dialogue in the clinical consultation). When completing the PROS, patients have the option to share the data with their healthcare professional.
Limitations
Some limitations of this study must be noted. Although the power analyses showed that an appropriate number of patients were included to detect a meaningful change over time, the sample size is small. If these analyses were performed in larger populations and in several locations, the effect-sizes would possibly have differed. However, a meaningful effect size was detected even with this limited population.
Another important limitation is that almost 90% of the population was female. This means that our findings for change over time may not be generalizable to the male gender. This is an empirical question for further study.
The patients reported only mild discomfort at baseline. In a population of patients experiencing higher distress with obesity-related HRQOL at baseline, one would expect an even larger change over time.
In this study, only patients who had undergone LSG were included as this is the only procedure currently performed at this hospital trust. We therefore have no data on whether these findings are transferable to patient who have undergone other surgical procedures.
Implications
Through this study, a brief, easy to administer questionnaire assessing obesity-related HRQOL has been shown to be sensitive to change over 24 months. The advantage of the questionnaire is that it may be used as both a clinical and a research tool. The fact that the measure is multidimensional and at the same time has few items is an advantage for clinical use. The questionnaire is available for use at no cost.
There is still a need to explore how best to help patients after bariatric surgery, not only to lose weight but also to experience improvement in other aspects such as pain, mental health and HRQOL. Also, research on how to tailor the follow up to the patient’s need are welcomed.
Conclusion
The PROS demonstrated satisfactory sensitivity to change over 24 months following bariatric surgery. This suggests that the PROS can be used for longitudinal studies in patients with obesity.
Disclosure
Professor Ronette L Kolotkin reports her company, Quality of Life Consulting, PLLC, receives royalties for weight-related quality of life questionnaires for IWQOL-Lite, IWQOL-Lite-CT, IWQOL-Kids. The authors report no other conflicts of interest in this work.
References
1. Kolotkin RL, Andersen JR. A systematic review of reviews: exploring the relationship between obesity, weight loss and health-related quality of life. Clin Obes. 2017;7(5):273–289. doi:10.1111/cob.12203
2. Szmulewicz A, Wanis KN, Gripper A, et al. Mental health quality of life after bariatric surgery: a systematic review and meta-analysis of randomized clinical trials. Clin Obes. 2019;9(1):e12290. doi:10.1111/cob.12290
3. Yazdani N, Sharif F, Elahi N, Ebadi A, Hosseini SV. Psychometric properties of quality of life assessment tools in morbid obesity: a review of literature. Evid Based Care. 2018;7(4):7–21.
4. Kolotkin R, Crosby R. Psychometric evaluation of the impact of weight on quality of life-lite questionnaire (IWQOL-Lite) in a community sample. Qual Life Res. 2002;11(2):157–171. doi:10.1023/A:1015081805439
5. Weiner S, Sauerland S, Weiner R, Cyzewski M, Brandt J, Neugebauer E. Validation of the adapted Bariatric Quality of Life Index (BQL) in a prospective study in 446 bariatric patients as one-factor model. Obes Facts. 2009;2(Suppl 1):63–66. doi:10.1159/000198263
6. Tayyem R, Atkinson J, Martin C. Development and validation of a new bariatric-specific health-related quality of life instrument”bariatric and obesity-specific survey (BOSS)”. J Postgrad Med. 2014;60(4):357. doi:10.4103/0022-3859.143952
7. Aasprang A, Våge V, Flølo TN, et al. Patient-reported quality of life with obesity – development of a new measurement scale. Tidsskr nor Laegeforen. 2019;139. doi:10.4045/tidsskr.18.0493
8. SOReg-Norge. Norsk kvalitetsregister for fedmekirurgi (SOReg-Norge) 2021 [04.08]; 2020. Available from: https://helse-bergen.no/avdelinger/laboratorieklinikken/medisinsk-biokjemi-og-farmakologi/norsk-kvalitetsregister-for-fedmekirurgi-soreg-norge#les-meir-om-norsk-kvalitetsregister-for-fedmekirurgi-soreg-norge.
9. Traebert J, Rodrigues MD, Chaves MS, et al. Transcultural adaptation of Patient-Reported Outcomes in Obesity (PROS) questionnaire for Brazil. Rev Bras Epidemiol. 2022;25:E220015. doi:10.1590/1980-549720220015.2
10. Demircioğlu A, Özkal Ö, Dağ O. Validity, reliability, and factorial structure of the Turkish version of the patient-reported outcomes in obesity questionnaire. Bariatr Surg Pract Patient Care. 2022;18:254.
11. Hegland PA, Aasprang A, Kolotkin RL, Moltu C, Tell GS, Andersen JR. A novel patient-reported outcome monitoring with clinical feedback system in bariatric surgery care: study protocol, design and plan for evaluation. BMJ Open. 2020;10(6):e037685. doi:10.1136/bmjopen-2020-037685
12. Karlsson J, Taft C, Sjostrom L, Torgerson JS, Sullivan M. Psychosocial functioning in the obese before and after weight reduction: construct validity and responsiveness of the Obesity-related Problems scale. Int J Obes. 2003;27(5):617–630. doi:10.1038/sj.ijo.0802272
13. Aasprang A, Andersen JR, Våge V, Kolotkin RL, Natvig GK. Psychosocial functioning before and after surgical treatment for morbid obesity: reliability and validation of the Norwegian version of obesity-related problem scale. PeerJ. 2015;3:e1275. doi:10.7717/peerj.1275
14. IBM Corp. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp; 2020.
15. Karlsson J, Taft C, Ryden A, Sjostrom L, Sullivan M. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes. 2007;31(8):1248–1261. doi:10.1038/sj.ijo.0803573
16. Coulman KD, MacKichan F, Blazeby JM, Donovan JL, Owen-Smith A. Patients’ experiences of life after bariatric surgery and follow-up care: a qualitative study. BMJ open. 2020;10(2):e035013. doi:10.1136/bmjopen-2019-035013
17. Bowling NA, Gibson AM, Houpt JW, Brower CK. Will the questions ever end? Person-level increases in careless responding during questionnaire completion. Organ Res Methods. 2020;24(4):718–738. doi:10.1177/1094428120947794
18. Budin AJ, Sumithran P, MacCormick AD, Caterson I, Brown WA. Surgeon engagement with patient-reported measures in Australian and Aotearoa New Zealand bariatric practices. Obes Surg. 2022;32(10):3410–3418. doi:10.1007/s11695-022-06237-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.