Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
sCD36 as a Biomarker for Progression and Recurrence in Type 2 Diabetes Mellitus Associated Hepatocellular Carcinoma
Authors Dai W, Yang F, Guo F, Ding Y, He D, Zhang J, Guo Y, Gao Y, Xiao A
Received 3 September 2025
Accepted for publication 31 October 2025
Published 14 November 2025 Volume 2025:12 Pages 2541—2552
DOI https://doi.org/10.2147/JHC.S565006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Weiwei Dai,1,* Fan Yang,2,* Furao Guo,1 Yuling Ding,1 Deying He,1 Jiajia Zhang,1 Ying Guo,1 Yingying Gao,1 Anhua Xiao1,3,4
1Department of Clinical Laboratory, Affiliated Banan Hospital of Chongqing Medical University, Chongqing, 401320, People’s Republic of China; 2College of Clinical Medicine, Jiamusi University, Heilongjiang, 154007, People’s Republic of China; 3Key Laboratory of Molecular Biology for Infectious Diseases (Ministry of Education), Institute for Viral Hepatitis, Department of Infectious Diseases, the second Affiliated Hospital, Chongqing Medical University, Chongqing, 400016, People’s Republic of China; 4School of Basic Medical Sciences, Chongqing Medical University, Chongqing, 40016, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Anhua Xiao, Email [email protected] Yingying Gao, Email [email protected]
Background: To evaluate the relationship between soluble CD36 (sCD36) and type 2 diabetes mellitus complicated by hepatocellular carcinoma (T2DM-HCC), and to explore its potential clinical prognostic value.
Methods: A prospective study was conducted enrolling newly diagnosed T2DM-HCC patients from two medical centers, along with control groups including healthy individuals (HC), T2DM patients, and HCC patients. Clinical, biochemical, and pathological data were collected. Serum sCD36 levels were measured by ELISA. Univariate and multivariate analyses were used to identify recurrence risk factors, and ROC analysis was performed to evaluate diagnostic performance.
Results: Among 258 participants, the T2DM-HCC group exhibited the highest sCD36 levels, impaired liver function, lower platelets, and mild chronic inflammation. In this group, sCD36 levels positively correlated with tumor stage, size, and proliferation. In univariable analysis, it was associated with postoperative recurrence (OR = 2.57, 95% CI: 0.68– 9.67). The predictive ability of sCD36 for recurrence (AUC = 0.86) was comparable to AFP (AUC = 0.89), while their combination showed the highest accuracy (AUC = 0.94).
Conclusion: sCD36 is associated with tumor progression in T2DM-HCC patients and serves as an independent risk factor for recurrence. To the best of our knowledge, this is the first study to identify sCD36 as a critical clinical biomarker for disease progression in T2DM-HCC, with strong potential for clinical application.
Trial Registration: This study was registered in September 2024 with the Chinese Clinical Trial Registry (ChiCTR), registration number: ChiCTR2400089651.
Keywords: sCD36, T2DM, hepatocellular carcinoma, predictive, prognosis
Introduction
Globally, liver cancer ranks as the sixth most common cancer and the third leading cause of cancer-related deaths.1 HCC is the most common type of liver cancer, which accounts for 90% of all the cases.2 Although the incidence and mortality of HCC have declined in some regions,3 the overall survival remains poor, with a median survival ranging from 6 to 10 months or less than 2 years in most cases.4,5 The well-known risk factors for HCC include hepatitis B virus (HBV) and hepatitis C virus infection (HCV), alcoholism, non-alcoholic fatty liver disease (NAFLD), aflatoxin exposure, and T2DM.
The prevalence of T2DM has been increasing worldwide, with one study estimating that the number of T2DM patients will rise to 642 million by 2040.6 Moreover, since T2DM is a risk factor for HCC, the rising prevalence of T2DM may be a contributing factor to the higher incidence of HCC. Studies have shown that individuals with T2DM face a 2.31-fold increased risk of developing HCC compared to those without diabetes, while the mortality rate of HCC in T2DM patients is 2.43 times higher.7 Therefore, addressing the management of HCC in patients with T2DM has become an essential strategy to reduce HCC-related mortality. In recent years, the remarkable success of atezolizumab combined with bevacizumab in clinical trials has revolutionized the therapeutic landscape of HCC. The treatment paradigm has shifted from single-agent targeted therapy to combination regimens centered on immunotherapy.8 Within this evolving landscape, the focus of HCC management has progressively moved from sequential drug use toward precision and individualized decision-making based on biomarkers, liver function, and patient status.9 On this basis, identifying robust prognostic biomarkers has become a key step toward improving survival outcomes in HCC.10–12 Particularly, since T2DM is closely linked to metabolic dysregulation, exploring metabolism-related prognostic biomarkers is crucial for patients with T2DM complicated by HCC.
Fatty acid translocase (FAT/CD36) is a multifunctional receptor expressed in various tissues, where it plays diverse biological roles, including regulation of lipid metabolism, modulation of chronic inflammation, and contribution to obesity-induced insulin resistance.13–15 CD36 expressed in adipose tissue and skeletal muscle is associated with long-chain fatty acid uptake and plays a critical role in obesity-induced insulin resistance.16 In hepatocytes, CD36 can induce sterile inflammation by promoting the production of endogenous damage-associated molecular patterns (DAMPs) and enhancing the phagocytosis of pathogenic components.17 Additionally, CD36 regulates lipid metabolism homeostasis through the MAPK signaling pathway, thereby influencing the progression of NAFLD-HCC.18 In macrophages, CD36 has been shown to mediate the development and progression of liver metastasis by regulating macrophage migration and polarization phenotypes,19,20 and it is also implicated in the pathophysiology of T2DM.21 Interestingly, previous studies have demonstrated that the sCD36 in circulation serves as a non-invasive biomarker for T2DM, NAFLD, atherosclerosis, poor prognosis of HBV infection, and liver failure.22–24
The above-mentioned studies have provided a rationale that the homeostasis of sCD36 is altered in the context of T2DM-HCC, suggesting that sCD36 could serve as a potential biomarker for predicting the progress of T2DM-HCC. Therefore, in this study, we aim to evaluate the relationship between serum sCD36 levels and T2DM-HCC.
Materials and Method
Patients Recruitment and Study Design
Participants of the study were recruited from the Chongqing Liver Cancer Cohort, which is an prospective, ongoing cohort study initiated at Affiliated Banan Hospital of Chongqing Medical University and The First Affiliated Hospital of Chongqing Medical University. The required sample size for this study was calculated using the formula: N = Z2 × σ2 / d2. Based on a standard deviation (σ) of 0.46 for sCD36 in the population,25 a margin of error (d) of 0.15, and a 95% confidence level (Z = 1.96), the estimated sample size was 36.12. Accounting for a 20% potential loss to follow-up, the adjusted sample size was approximately 43. To ensure sufficient statistical power, the final sample size was rounded up to 50 participants.
From January 2024 to October 2025, a total of 56 T2DM-HCC patients were recruited, these patients had any prior anticancer treatment and were scheduled to undergo either surgical resection or TACE therapy. Additionally, we established three control cohorts: Control cohort 1 comprising 89 patients with HCC who had not received any prior treatment (HCC group), Control cohort 2 consisting of 72 patients with T2DM (T2DM group), and Control cohort 3 including 86 healthy individuals (HC group). HCC diagnosis was based on imaging scan and histopathological examination following the American Association for the Study of Liver Diseases (AASLD) guidelines.26 The staging of HCC was evaluated based on the Chinese Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022 Edition).27 The inclusion and exclusion criteria for the whole cohort are detailed in the Supplementary Information. All participants provided written informed consent. This study was approved by the Ethics Committee of Banan Hospital Affiliated to Chongqing Medical University (BNLL-KY-2024-025) and was registered with the Chinese Clinical Trial Registry (ChiCTR2400089651).
Data Collection
The electronic medical record (EMR) system of our institution was utilized to document patients’ baseline characteristics. Data were collected at the following time points, including at the initial diagnosis of T2DM-HCC. The following baseline characteristics were collected: age, sex, body weight, height, duration of diabetes, comorbidities (including hypertension, dyslipidemia, and fatty liver disease), clinical laboratory test results, number and size of tumor nodules, and Child–Turcotte–Pugh (CTP) score.
Serum sCD36 Measurement
Baseline blood samples were obtained from patients. The serum separation tubes (SST, clot activator tubes) were centrifuged at 3000 rpm for 10 min at 4 °C, and the supernatant (serum) was then collected and stored at −80 °C. Serum sCD36 levels were quantified using a human sCD36 ELISA kit (Shanghai Enzyme-linked Biotechnology, China, ml038125) following the manufacturer’s protocol.
Immunohistochemical (IHC) Staining
Collected paraffin-embedded tissue samples of T2DM-HCC from Chongqing Medical University Affiliated Banan Hospital between January 2024 and March 2025. Immunohistochemical staining was performed to detect Ki67 expression levels. A professional pathologist evaluated the percentage of positively stained cells within the field of view to determine tumor proliferation status. The staining procedure utilized the Rabbit Two-Step Detection Kit (Zhongshan Golden Bridge, China, PV-9001) and Ki67 polyclonal antibody (Proteintech, China, 27309-1-AP). All operations were conducted in strict accordance with the reagent manufacturer’s instructions.
Follow-Up and Outcomes Evaluation
Patients in the study cohort with T2DM-HCC and HCC were followed up at 1, 3, 6, and 12 months after surgery, with the follow-up period lasting at least two years. Follow-up was conducted either through in-person hospital visits or by telephone reminders encouraging patients to return for examination. The follow-up primarily involves: (1) imaging examinations such as abdominal ultrasound, CT, or MRI to evaluate tumor recurrence; (2) laboratory tests to assess liver function, kidney function, serum AFP, fasting blood glucose (FBG), and glycated hemoglobin (HbA1c) levels; (3) collection of serum samples, stored at −80°C for subsequent measurement of serum sCD36 levels; (4) documentation of survival status. Main outcomes: the recurrences of patients.
This is an ongoing prospective cohort study with an originally planned period from January 2024 to January 2026. All eligible patients are required to be followed for at least two years; therefore, the actual study duration will extend beyond the initially planned timeline. At the time of manuscript preparation, the six-month follow-up data were the most complete; hence, the present analysis was based on patients who had completed six months of follow-up.
Statistic Analysis
SPSS statistical software26.0 (IBM, USA) was used to perform statistics analysis. Normally distributed continuous variables data are showed as mean ± standard deviation (SD), difference between groups are performed using a Student’s t-test or analysis of variance (ANOVA). Skewed continuous variables as median (interquartile range), and difference between groups are performed using Wilcoxon rank sum test. Categorical variables as count (percent), χ2 test is used to evaluate difference of categorical variables. Logistic regression analysis was used to examine the relationship between variable parameters and renal dysfunction, with effect sizes expressed as odds ratios (ORs) and their 95% confidence intervals (95% CIs). The “RMS” package in R software (version 3.5) was used to construct the nomogram, and “forestplot” package is used for drawing forest plots. To evaluate whether there were statistically significant differences in predictive performance among the models, the bootstrap method was applied.
Results
Population Characterized
This study design and the number of included patients were presented in detail in Figure 1. Baseline characteristics of all study cohorts are presented in Table 1. In the T2DM-HCC cohort, the median age was 60 years and the median BMI was 23.928, with males accounting for 54% of the population. In the T2DM cohort, the median age was 53 years and the median BMI was 22.262, with males accounting for 69.231%. In the HCC cohort, the median age was 67 years and the median BMI was 21.931, with males accounting for 79.167%. In the HC cohort, the median age was 54.5 years and the median BMI was 22.140, with males accounting for 45.238%.
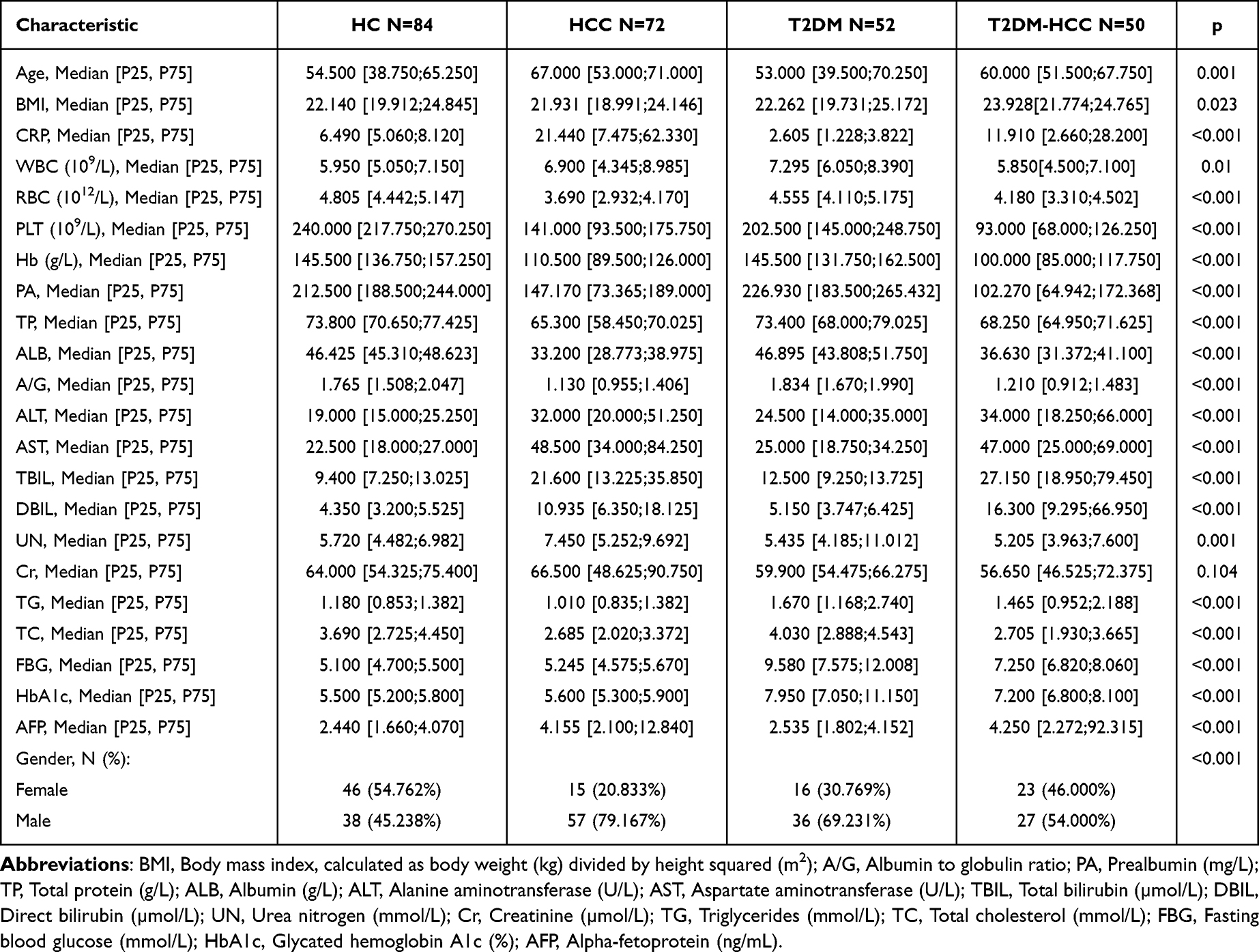 |
Table 1 The Characteristics of the Four Study Cohorts |
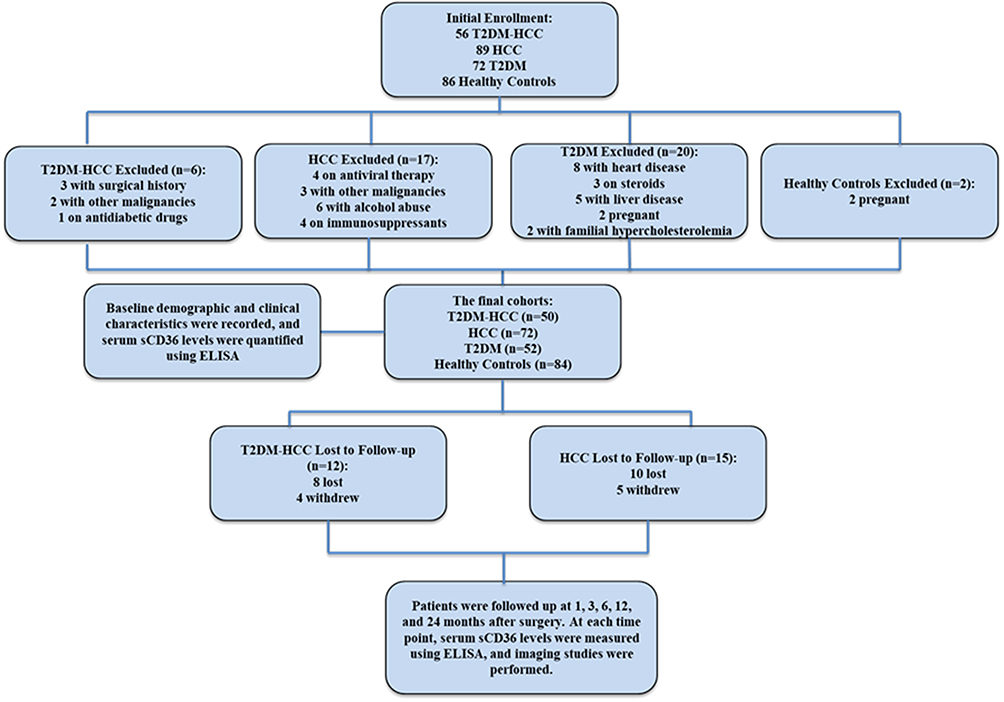 |
Figure 1 Flowchart of the study design. A total of 56 patients with T2DM-HCC, 89 with HCC, 72 with T2DM, and 86 healthy individuals were initially enrolled. Participants were excluded for reasons including prior surgical treatment, history of other malignancies, use of antidiabetic or immunosuppressive medications, antiviral therapy, pregnancy, cardiovascular disease, liver disease, steroid use, or familial hypercholesterolemia. The final study population consisted of 50 T2DM-HCC patients, 72 HCC patients, 52 T2DM patients, and 84 healthy controls. T2DM-HCC and HCC patients underwent follow-up at 1, 3, 6, 12, and 24 months postoperatively to monitor sCD36 levels and tumor recurrence. During follow-up, 12 T2DM-HCC patients (8 lost to follow-up, 4 withdrew) and 15 HCC patients (10 lost to follow-up, 5 withdrew) were excluded from final analysis. |
Compared with the HC cohort, individuals in the T2DM-HCC cohort were older and had higher levels of CRP, ALT, AST, TBIL, DBIL, TG, FBG, HbA1c, and AFP, while showing lower levels of RBC, Hb, Plt, PA, TP, ALB, A/G, and TC (sTable 1). These findings suggest that individuals in the T2DM-HCC group exhibit mild chronic inflammation, impaired liver function, and dysregulated glucose and lipid metabolism. Compared with the T2DM cohort, the T2DM-HCC group still showed evident liver function impairment, although differences in glucose and lipid metabolism were observed (sTable 2). When compared to the HCC cohort, the T2DM-HCC group exhibited higher BMI, FBG, and HbA1c levels, along with gender differences, indicating that T2DM-HCC may have distinct disease characteristics (sTable 3).
These results indicated that the observed differences in baseline characteristics were likely attributable to the diverse physiological and pathological states of the study populations.
sCD36 is Associated with the Progression of T2DM-HCC and HCC
sCD36 has been reported to play an important role in various diseases.28 In this study, we analyzed sCD36 concentrations in all cohorts and found that they were significantly higher in both the T2DM-HCC and HCC cohorts compared to the HC cohort. Moreover, sCD36 concentrations in the T2DM-HCC cohort were significantly higher than those in the HCC cohort. However, there was no significant difference in sCD36 levels between the T2DM and HC cohorts (Figure 2A).
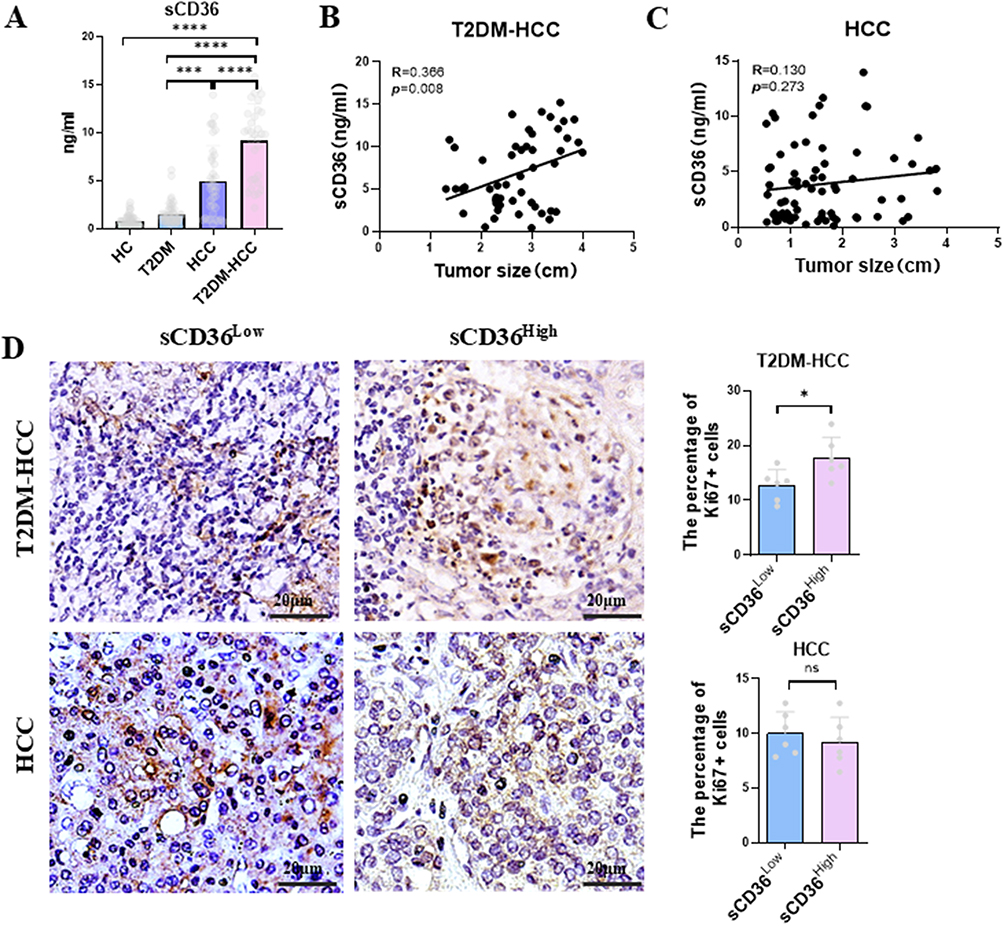 |
Figure 2 sCD36 is associated with tumor progression in T2DM-HCC. (A) Serum sCD36 levels were measured in all four study cohorts using an ELISA kit. B-C:The correlation between sCD36 and tumor size was evaluated using Pearson analysis in the T2DM-HCC (B) and HCC (C) groups. (D) Representative images of Ki-67 staining with quantitative analysis in T2DM-HCC (n=12) and HCC groups (n=12). *, p<0.05, ***p<0.001, ****p<0.0001. |
To further explore the relationship between sCD36 and the progression of T2DM-HCC and HCC, we analyzed the baseline characteristics and sCD36 concentrations in patients at different disease stages within the T2DM-HCC and HCC cohorts. In the T2DM-HCC cohort, sCD36 concentrations increased progressively with advancing stages. Advanced stages were also associated with greater liver function impairment, as indicated by elevated ALT and AST levels, as well as increased AFP concentrations (Table 2). Similarly, in the HCC cohort, sCD36 concentrations, along with ALT and AST levels, increased with disease progression (sTable 4). These findings suggest that sCD36 may play an important role in the progression of both T2DM-HCC and HCC.
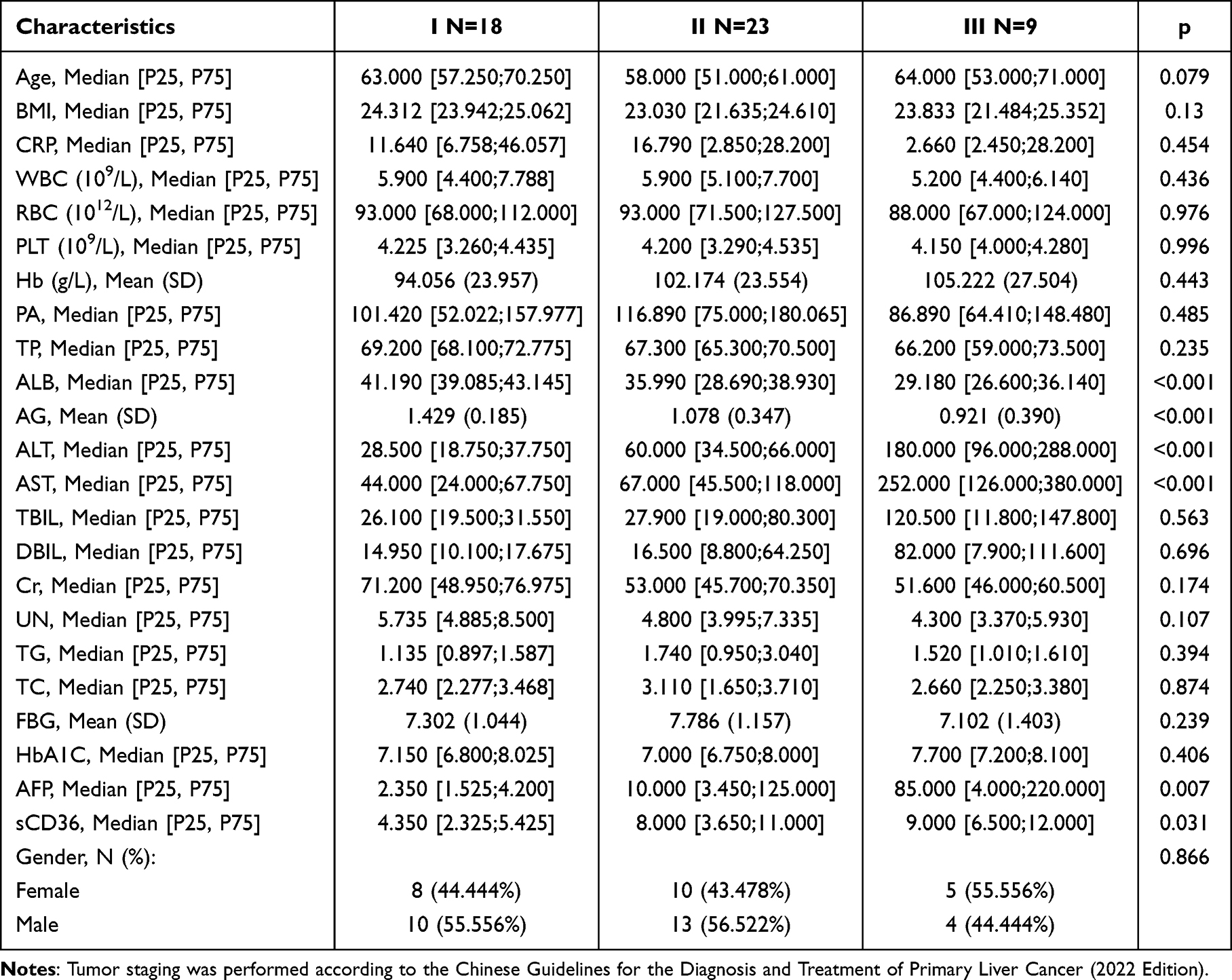 |
Table 2 Baseline Characteristics of T2DM-HCC Patients According to Tumor Stage |
sCD36 Correlates with Tumor Cell Proliferation and Tumor Burden
Given that sCD36 may contribute to the progression of both T2DM-HCC and HCC, and considering that T2DM-HCC represents a distinct subtype of liver cancer characterized by coexisting diabetes, with previous studies reporting that sCD36 promotes the development of HCC in diabetic patients, we aimed to further investigate the relationship between sCD36 and tumor characteristics. Firstly, we compared tumor burden between the T2DM-HCC and HCC cohorts (Table 3). The results showed that patients in the T2DM-HCC cohort had larger tumors than those in the HCC cohort. In addition, sCD36 levels were associated with tumor size in the T2DM-HCC cohort, but no such correlation was observed in the HCC cohort (Figure 2B and C). Therefore, patients in both cohorts were divided into sCD36High and sCD36Low groups based on the median sCD36 concentration to evaluate the correlation between sCD36 and tumor burden in the two cohorts. The Ki67 staining results showed that the sCD36High group exhibited greater proliferative ability in the T2DM-HCC cohort, whereas this phenomenon was not observed in the HCC cohort (Figure 2D). These findings suggest that sCD36 may play a unique role in tumor growth in T2DM-HCC, but not in HCC.
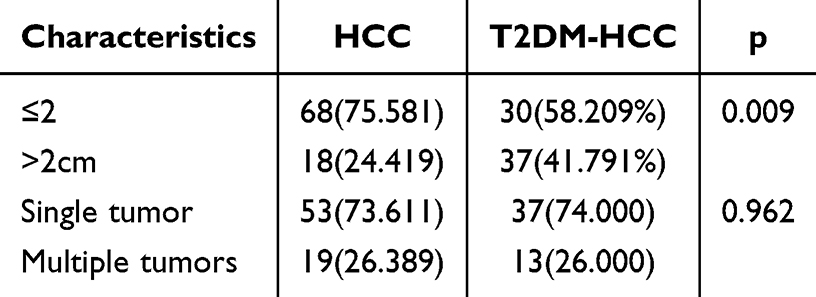 |
Table 3 Tumor Burden Comparison Between T2DM-HCC and HCC Groups |
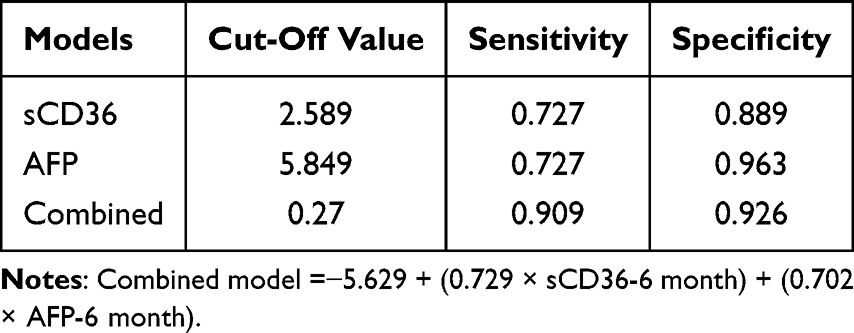 |
Table 4 Diagnostic Performance of sCD36, AFP, and the Combined Model for Predicting Postoperative Recurrence in T2DM-HCC Patients |
sCD36 Serves as a Potential Predictor of T2DM-HCC Recurrence
To further investigate the association between sCD36 and postoperative recurrence in T2DM-HCC, we first analyzed sCD36 levels in recurrence and non-recurrence patients within the T2DM-HCC cohort. The results demonstrated that sCD36 levels were significantly elevated in recurrent patients compared to non-recurrence individuals at 6 months after surgery (Figure 3A), indicating that sCD36 may serve as a potential biomarker for predicting recurrence. In contrast, no such difference in sCD36 levels was observed between recurrent and non-recurrent patients in the HCC cohort (Figure 3B). Moreover, the postoperative sCD36 concentration at 6 months was significantly higher in the T2DM-HCC cohort than in the HCC cohort (sTable 5), further suggesting a possible T2DM-specific role of sCD36 in recurrence.
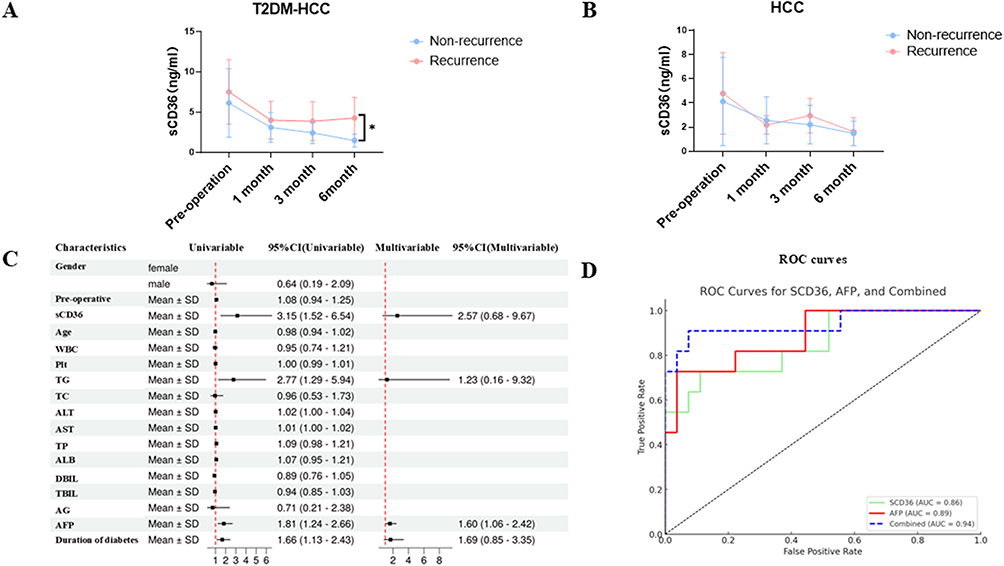 |
Figure 3 Serum sCD36 levels were significantly associated with postoperative recurrence in patients with T2DM-HCC. (A and B), Serum sCD36 concentrations were measured using an ELISA kit at 1, 3, 6months postoperatively. (C) Forest plot integrating the results of both univariate and multivariate analysis. (D) ROC curves for sCD36, AFP, and their combined model in predicting postoperative recurrence. Preoperative, the serum sCD36 of preoperative. sCD36, the serum sCD36 of 6 months postoperative. |
To further elucidate the role of sCD36 in T2DM-HCC, we performed univariate and multivariate analyses to identify risk factors associated with postoperative recurrence in T2DM-HCC patients (Figure 3C). In the univariate analysis, both AFP and sCD36 were identified as statistically significant risk factors (sTable 6), with odds ratios of 1.81 (95% CI: 1.44–2.66) and 3.15. (95% CI: 1.52–6.54), respectively. However, when these two variables were included in a multivariate logistic regression model (sTable 7), sCD36 did not show statistically significant, which may be attributed to the limited sample size of our cohort.
Interestingly, when we evaluated the predictive value of sCD36 and AFP using their optimal cut-off values (sCD36: 2.589; AFP: 5.849), as well as that of a combined diagnostic model constructed using logistic regression (cut-off: 0.27) we found that the AUCs of sCD36 and AFP alone were not significantly different (sTable 8). However, the AUC of the combined model was significantly higher than that of either marker used alone, indicating improved predictive performance (Table 4), the results were visualized in Figure 3D.
Discussion
In this prospective study, we systematically investigated the potential role of sCD36 in T2DM-HCC. Our findings suggest that sCD36 may be involved in tumor staging, tumor size, tumor cell proliferation, and postoperative recurrence in T2DM-HCC, indicating its potential predictive value. In addition, elevated sCD36 expression was also observed in HCC patients and was found to be associated with disease stage, suggesting a broader relevance of sCD36 in liver cancer progression.
sCD36 is a soluble form of CD36 detectable in peripheral blood, primarily derived from the cleavage or secretion of membrane-bound CD36. Hepatocytes are among the major cell types expressing CD36, and earlier research has demonstrated that hepatic CD36 plays a critical role in various liver and metabolism-related diseases by regulating fatty acid uptake, lipid metabolic reprogramming,17,29 and inflammatory responses.30 Therefore, circulating sCD36 levels may, to some extent, reflect the expression activity and metabolic status of hepatic CD36.The development of T2DM is closely associated with hepatic metabolic homeostasis. One study has shown that the loss of CD36 in hepatocytes may disrupt insulin signaling by inducing endoplasmic reticulum stress, thereby contributing to insulin resistance and promoting the onset of T2DM.31 Notably, in our study cohort, we did not observe a significant elevation of sCD36 levels in patients with T2DM, which is consistent with findings from a previous report.32 sCD36 has been widely recognized as playing an important role in the pathogenesis of T2DM.22,33 One studies have reported that elevated sCD36 levels are associated with insulin resistance; however, its predictive value often depends on additional metabolic parameters such as FBG and insulin levels.23 Moreover, a large-scale prospective cohort study confirmed that sCD36 levels are generally higher in individuals with T2DM.34 Collectively, these findings suggest a potential biological role of sCD36 in T2DM and its related conditions, although its utility as a predictive biomarker warrants further investigation.
T2DM not only promotes pathological changes in the liver through mechanisms such as hyperglycemia, insulin resistance, and chronic inflammation, but also accelerates the development and progression of HCC.35 Therefore, T2DM-HCC, as a comorbid condition in which T2DM and HCC coexist, may simultaneously exhibit pathological and physiological processes associated with both diseases. In the context of T2DM-HCC comorbidity, abnormal glucose metabolism and alterations in the tumor microenvironment interact and form a vicious cycle, further exacerbating disease progression. This dual pathological basis leads to more complex pathogenesis, more severe clinical manifestations, and poorer prognosis.36,37 However, current prognostic biomarkers for T2DM-HCC remain limited and are primarily based on conventional tumor-related indicators such as AFP,38 tumor size,39 and liver function scores.40 These markers fail to reflect the metabolic characteristics unique to T2DM-HCC. In recent years, CD36 has emerged as a key metabolic regulator with dual roles in both T2DM and HCC. It has been shown that CD36 promotes aerobic glycolysis and tumor cell proliferation by activating the Src/PI3K/AKT signaling axis, thereby reshaping cellular metabolism in favor of tumor progression.41 In this study, we observed that higher serum levels of sCD36 in T2DM-HCC patients were associated with greater proliferative capacity in tumor cells. Additionally, sCD36 levels were positively correlated with tumor size, suggesting that it may reflect tumor burden. Notably, such associations were not observed in HCC patients without T2DM, indicating a potential specificity of sCD36 for the T2DM-HCC subtype. Furthermore, we found that sCD36 levels were significantly associated with tumor stage in both T2DM-HCC and HCC cohorts, implying its potential as an indicator of disease progression. Our previous studies24 also reported a close relationship between sCD36 and hepatic dysfunction in HBV-infected patients. Based on these findings, we hypothesize that the stage-dependent changes in sCD36 observed in HCC may be more reflective of liver dysfunction rather than tumor progression. In contrast, sCD36 appears to have higher predictive value in T2DM-HCC, where it may serve as a biomarker linking metabolic disturbance with tumor development.
A recent meta-analysis that reviewed multiple studies on T2DM-HCC identified T2DM as a significant risk factor for postoperative recurrence and poor long-term prognosis in patients with HCC.42 Given this context, we further investigated the association between serum sCD36 levels and postoperative recurrence in patients with T2DM-HCC. Our results demonstrated that patients with T2DM-HCC, who represent a metabolically distinct subgroup, exhibited a higher recurrence rate compared to those with HCC alone, indicating a worse overall prognosis. Notably, elevated serum levels of sCD36 were consistently observed in T2DM-HCC patients with recurrence. To identify potential predictors of recurrence, both univariate and multivariate analyses were conducted. In the univariate model, significant correlations with recurrence risk were observed for both sCD36 and AFP. However, the association between sCD36 and recurrence risk did not remain statistically significant in the multivariate model, suggesting that the predictive ability of sCD36 for recurrence in T2DM-HCC may be weaken in this cohort. Several factors may account for this result. First, the sample size of the present study was relatively small. The sample size estimation was based on the population distribution of serum sCD36 levels, whereas recurrence is a time-dependent event. After the corresponding power estimation (data not shown), the sample size appeared insufficient to fully evaluate the prognostic potential of sCD36 for recurrence in T2DM-HCC. Second, the relatively short follow-up period may have constrained the detection of long-term recurrence events. Since recurrence is a dynamic and cumulative process, the current follow-up duration might only reflect the predictive value of sCD36 for early recurrence rather than long-term outcomes. Interestingly, ROC curve analysis revealed that the diagnostic performance of sCD36, which was comparable to that of AFP in predicting postoperative recurrence, supports its potential clinical utility in T2DM-HCC. Furthermore, the combination of sCD36 and AFP in a logistic regression model yielded a significantly higher diagnostic accuracy than either marker alone. These findings indicate that sCD36, by capturing both metabolic and tumor-related alterations, may act as a promising biomarker complementary to AFP for assessing postoperative recurrence and long-term prognosis in T2DM-HCC patients.
Limitation
In this study, several limitations of this study should be acknowledged. First, during the follow-up period, no definitive cases of HCC development were identified in the diabetic cohort, limiting our ability to assess the predictive value of sCD36 in early tumorigenesis. Second, although this was a multicenter study, the relatively short follow-up duration and limited sample size may have contributed to the lack of a significant difference in sCD36 levels between the T2DM and HC cohorts. Third, the limited sample size and relatively short follow-up duration in this study may have reduced the statistical power to detect the prognostic effect of sCD36 on recurrence. Therefore, the present findings only provide preliminary evidence that the combination of sCD36 and AFP may have potential value in assessing the risk of early recurrence in T2DM-HCC. Further validation in larger cohorts with longer follow-up is warranted to confirm the independent predictive role of sCD36. Finally, adjuvant pharmacological treatments administered to T2DM-HCC patients during the postoperative period may have introduced confounding effects.
Therefore, future studies with larger cohorts, longer follow-up periods, and more rigorous control of confounding variables are needed to further clarify the causal relationship between sCD36 and the development and progression of T2DM-HCC.
Conclusion
Overall, this study is the first to reveal a potential association between sCD36 levels and both tumor stage and tumor size in patients with T2DM-HCC. These findings may be attributed to the elevated levels of sCD36 observed in T2DM-HCC, which could be linked to enhanced tumor cell proliferation. In addition, we demonstrated that the combination of sCD36 and AFP provides a robust model for predicting postoperative recurrence in T2DM-HCC patients. However, the predictive ability of sCD36 alone appeared to be limited in this cohort, suggesting that its prognostic value may be enhanced when used in conjunction with AFP.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Banan Hospital Affiliated to Chongqing Medical University (BNLL-KY-2024-025). The entire experimental procedure strictly adhered to the principles of the Declaration of Helsinki.
Consent for Publication
All participants provided written informed consent for the publication of their data.
Funding
This work was supported by Joint youth project of Chongqing Health Commission and Science and Technology Bureau (2024QNXM031).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Bruno Sangro, Josepmaria Argemi, Maxime Ronot et al. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
3. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77(6):1598–1606. doi:10.1016/j.jhep.2022.08.021
4. Toh MR, Wong EYT, Wong SH, et al. Global epidemiology and genetics of hepatocellular carcinoma. Gastroenterology. 2023;164(5):766–782. doi:10.1053/j.gastro.2023.01.033
5. Chen VL, Xu D, Wicha MS, Lok AS, Parikh ND. Utility of liquid biopsy analysis in detection of hepatocellular carcinoma, determination of prognosis, and disease monitoring: a systematic review. Clin Gastroenterol Hepatol. 2020;18(13):13. doi:10.1016/j.cgh.2020.04.019
6. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
7. Wang P, Kang D, Cao W, Wang Y, Liu Z. Diabetes mellitus and risk of hepatocellular carcinoma: a systematic review and meta-analysis. Diabetes Metab Res Rev. 2012;28(2):109–122. doi:10.1002/dmrr.1291
8. Rizzo A, Ricci AD. Challenges and future trends of hepatocellular carcinoma immunotherapy. Int J Mol Sci. 2022;23(19):19. doi:10.3390/ijms231911363
9. Bas O, Sahin TK, Karahan L, Rizzo A, Guven DC. Prognostic significance of the cachexia index (CXI) in patients with cancer: a systematic review and meta-analysis. Clin Nutr ESPEN. 2025;68:240–247. doi:10.1016/j.clnesp.2025.03.023
10. Liu Z-Y, Luo Y, Fang A-P, et al. High serum fibroblast growth factor 21 is associated with inferior hepatocellular carcinoma survival: a prospective cohort study. Liver Int. 2022;42(3):663–673. doi:10.1111/liv.15100
11. Nault J-C, Villanueva A. Biomarkers for Hepatobiliary Cancers. Hepatology. 2021;73(Suppl 1):115–127. doi:10.1002/hep.31175
12. Vitale E, Rizzo A, Santa K, Jirillo E. Associations between “cancer risk”, “inflammation” and “metabolic syndrome”: a scoping review. Biology. 2024;13:5.
13. Wang J, Li Y. CD36 tango in cancer: signaling pathways and functions. Theranostics. 2019;9(17):4893–4908. doi:10.7150/thno.36037
14. Glatz JFC, Luiken JJFP. Dynamic role of the transmembrane glycoprotein CD36 (SR-B2) in cellular fatty acid uptake and utilization. J Lipid Res. 2018;59(7):1084–1093. doi:10.1194/jlr.R082933
15. Zeng H, Qin H, Liao M, et al. CD36 promotes de novo lipogenesis in hepatocytes through INSIG2-dependent SREBP1 processing. Mol Metab. 2022;57:101428. doi:10.1016/j.molmet.2021.101428
16. Baranova IN, Kurlander R, Bocharov AV, et al. Role of human CD36 in bacterial recognition, phagocytosis, and pathogen-induced JNK-mediated signaling. J Immunol. 2008;181(10):7147–7156. doi:10.4049/jimmunol.181.10.7147
17. Zhao L, Zhang C, Luo X, et al. CD36 palmitoylation disrupts free fatty acid metabolism and promotes tissue inflammation in non-alcoholic steatohepatitis. J Hepatol. 2018;69(3):705–717. doi:10.1016/j.jhep.2018.04.006
18. Zheng E, Chen Q, Xiao A, et al. Systemic loss of CD36 aggravates NAFLD-related HCC through MEK1/2-ERK1/2 signaling pathway. Biochem Biophys Res Commun. 2024;707:149781. doi:10.1016/j.bbrc.2024.149781
19. Qin H, Xiao A, Lu Q, et al. The fatty acid receptor CD36 promotes macrophage infiltration via p110γ signaling to stimulate metastasis. J Adv Res. 2025;74:237–253.
20. Yang P, Qin H, Li Y, et al. CD36-mediated metabolic crosstalk between tumor cells and macrophages affects liver metastasis. Nat Commun. 2022;13(1):5782. doi:10.1038/s41467-022-33349-y
21. Sampson MJ, Davies IR, Braschi S, Ivory K, Hughes DA. Increased expression of a scavenger receptor (CD36) in monocytes from subjects with Type 2 diabetes. Atherosclerosis. 2003;167(1):129–134. doi:10.1016/S0021-9150(02)00421-5
22. Handberg A, Højlund K, Gastaldelli A, et al. Plasma sCD36 is associated with markers of atherosclerosis, insulin resistance and fatty liver in a nondiabetic healthy population. J Intern Med. 2012;271(3):294–304. doi:10.1111/j.1365-2796.2011.02442.x
23. Handberg A, Norberg M, Stenlund H, Hallmans G, Attermann J, Eriksson JW. Soluble CD36 (sCD36) clusters with markers of insulin resistance, and high sCD36 is associated with increased type 2 diabetes risk. J Clin Endocrinol Metab. 2010;95(4):1939–1946. doi:10.1210/jc.2009-2002
24. Cai C, Xiao A, Luo X, et al. Circulating soluble CD36 as a novel biomarker for progression and prognosis of HBV-related liver diseases. Front Microbiol. 2022;13:1039614. doi:10.3389/fmicb.2022.1039614
25. Heebøll S, Poulsen MK, Ornstrup MJ, et al. Circulating sCD36 levels in patients with non-alcoholic fatty liver disease and controls. Int J Obes (Lond). 2017;41(2):262–267. doi:10.1038/ijo.2016.223
26. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
27. China GO; National Health Commission of the People’s Republic of. Clinical practice guidelines for the diagnosis and treatment of primary liver cancer (2022. %J Journal of Clinical Hepatobiliary Diseases. 2022;38(2):288–303.
28. Rada P, González-Rodríguez Á, García-Monzón C, Valverde ÁM. Understanding lipotoxicity in NAFLD pathogenesis: is CD36 a key driver? Cell Death Dis. 2020;11(9):802. doi:10.1038/s41419-020-03003-w
29. Li Y, Yang P, Zhao L, et al. CD36 plays a negative role in the regulation of lipophagy in hepatocytes through an AMPK-dependent pathway. J Lipid Res. 2019;60(4):844–855. doi:10.1194/jlr.M090969
30. Luo X, Li Y, Yang P, et al. Obesity induces preadipocyte CD36 expression promoting inflammation via the disruption of lysosomal calcium homeostasis and lysosome function. EBioMedicine. 2020;56:102797. doi:10.1016/j.ebiom.2020.102797
31. Yang P, Zeng H, Tan W, et al. Loss of CD36 impairs hepatic insulin signaling by enhancing the interaction of PTP1B with IR. FASEB J. 2020;34(4):5658–5672. doi:10.1096/fj.201902777RR
32. Castelblanco E, Sanjurjo L, Falguera M, et al. Circulating soluble CD36 is similar in type 1 and type 2 diabetes mellitus versus non-diabetic subjects. J Clin Med. 2019;8:5. doi:10.3390/jcm8050710
33. Touré M, Samb A, Sène M, et al. Impact of the interaction between the polymorphisms and hypermethylation of the CD36 gene on a new biomarker of type 2 diabetes mellitus: circulating soluble CD36 (sCD36) in Senegalese females. BMC Med Genomics. 2022;15(1):186. doi:10.1186/s12920-022-01337-2
34. Liani R, Halvorsen B, Sestili S, et al. Plasma levels of soluble CD36, platelet activation, inflammation, and oxidative stress are increased in type 2 diabetic patients. Free Radic Biol Med. 2012;52(8):1318–1324. doi:10.1016/j.freeradbiomed.2012.02.012
35. Wainwright P, Scorletti E, Byrne CD. Type 2 Diabetes And Hepatocellular Carcinoma: Risk Factors And Pathogenesis. Curr Diab Rep. 2017;17(4):20. doi:10.1007/s11892-017-0851-x
36. Zhang X-P, Chai Z-T, Feng J-K, et al. Association of type 2 diabetes mellitus with incidences of microvascular invasion and survival outcomes in hepatitis B virus-related hepatocellular carcinoma after liver resection: a multicenter study. Eur J Surg Oncol. 2022;48(1):142–149. doi:10.1016/j.ejso.2021.08.010
37. Yang S-Y, Yan M-L, Feng J-K, et al. Impact of type 2 diabetes mellitus on the prognosis of patients with hepatocellular carcinoma after laparoscopic liver resection: a multicenter retrospective study. Front Oncol. 2022;12:979434. doi:10.3389/fonc.2022.979434
38. Yang S, Liu L, Luo Y, et al. Lower alpha fetoprotein and higher risk of hepatocellular carcinoma, study from the type 2 diabetes mellitus patients. Diabetes Res Clin Pract. 2018;143:239–244. doi:10.1016/j.diabres.2018.07.018
39. Zhang W, Wang X, Jiang R, et al. Effect of tumor size on cancer-specific survival in small hepatocellular carcinoma. Mayo Clin Proc. 2015;90(9):1187–1195. doi:10.1016/j.mayocp.2015.06.018
40. Mulla N, Katib Y, Almughamsi AM, et al. The impact of alpha-fetoprotein (AFP), child-turcotte-pugh (CTP) score and disease staging on the survival of hepatocellular carcinoma (HCC) patients: a retrospective cohort from single oncology center. Oncol Res. 2025;33(1):149–160. doi:10.32604/or.2024.050903
41. Luo X, Zheng E, Wei L, et al. The fatty acid receptor CD36 promotes HCC progression through activating Src/PI3K/AKT axis-dependent aerobic glycolysis. Cell Death Dis. 2021;12(4):328. doi:10.1038/s41419-021-03596-w
42. Mrzljak A, Cigrovski Berković M, Giovanardi F, Lai Q. The prognostic role of diabetes mellitus type 2 in the setting of hepatocellular carcinoma: a systematic review and meta-analysis. Croat Med J. 2022;63(2):176–186. doi:10.3325/cmj.2022.63.176
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Decaprenyl Diphosphate Synthase Subunit 1 (PDSS1): A Potential Prognostic Biomarker and Immunotherapy-Target for Hepatocellular Carcinoma
Yang Y, Li J, Tang M, Nie B, Huang W
Cancer Management and Research 2022, 14:1627-1639
Published Date: 3 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Low MARCO Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma Following Liver Transplantation
Zhang Q, Wei Y, Li Y, Jiao X
Cancer Management and Research 2022, 14:1935-1944
Published Date: 11 June 2022
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022