Back to Journals » Infection and Drug Resistance » Volume 19
Risk Factors for Sepsis in Pediatric All During Induction Chemotherapy-Induced Neutropenia: A Single-Center Retrospective Study
Authors Zhao C, Yan M, Yue Y, Zhao L, Liu Y
Received 26 November 2025
Accepted for publication 5 February 2026
Published 7 February 2026 Volume 2026:19 584439
DOI https://doi.org/10.2147/IDR.S584439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Changda Zhao, Mei Yan, Yingbin Yue, Li Zhao, Yu Liu
Department of Pediatric Center, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Yu Liu, Department of Pediatric Center, The First Affiliated Hospital of Xinjiang Medical University, 137 Liyushan South Road, Xinshi District, Urumqi, Xinjiang, 830054, People’s Republic of China, Tel +86 991-4361253, Email [email protected]
Objective: To identify clinical factors associated with sepsis during induction chemotherapy–induced neutropenia (CIN) in children with acute lymphoblastic leukemia (ALL).
Methods: This single-center retrospective study included 292 children with ALL who received induction chemotherapy between January 2019 and July 2024. Candidate variables were extracted within 24 hours after the first onset of CIN. Sepsis was defined using the pediatric Sequential Organ Failure Assessment (pSOFA). Univariable Cox regression, collinearity assessment using variance inflation factor (VIF), and multivariable Cox regression analyses were performed to identify risk factors associated with time to sepsis. Kaplan-Meier analyses were used to illustrate sepsis-free survival according to key factors.
Results: Sepsis occurred in 48/292 (16.4%) patients. In multivariable analysis, oral mucosal status (HR=1.336, 95% CI: 1.061– 1.681, P=0.014), C-reactive protein to albumin ratio (CAR) (HR=1.407, 95% CI: 1.088– 1.806, P=0.050), red cell distribution width (RDW) (HR=1.126, 95% CI: 1.028– 1.233, P=0.011), and procalcitonin (PCT) (HR=1.017, 95% CI: 1.002– 1.036, P=0.043) were independently associated with sepsis risk. Kaplan-Meier analyses showed significantly different sepsis-free survival across strata of these factors (all P< 0.05).
Conclusion: Oral mucosal status, CAR, RDW, and PCT were independently associated with sepsis risk during CIN in children with ALL. These findings may inform early risk assessment and warrant confirmation in larger, multicenter cohorts.
Keywords: acute lymphoblastic leukemia, children, sepsis, chemotherapy-induced neutropenia, risk factors, cox regression analysis
Introduction
Acute lymphoblastic leukemia (ALL) is the most prevalent malignant tumor of the hematopoietic system in children, with an annual incidence of approximately 3–4 per 100,000, accounting for 75–80% of childhood hematologic malignancies.1 In recent years, continuous optimization of chemotherapy regimens and the widespread application of stratified treatment strategies have led to improved long-term therapeutic outcomes for childhood ALL, with the 5-year event-free survival (EFS) rate exceeding 80% in some developed countries.2,3 Nonetheless, severe adverse events during treatment remain a critical factor affecting patient prognosis, with infectious complications being the most common.
During the induction remission phase, all patients with ALL are treated with high-dose chemotherapy, which can frequently lead to chemotherapy-induced neutropenia (CIN). This condition compromises immune barriers and increases susceptibility to pathogens such as bacteria, viruses, and fungi, significantly elevating the risk of infection.4,5 Studies indicate that severe infections are a leading cause of mortality in ALL patients, with global infection-related mortality rates during chemotherapy estimated at 2–4%,6 while in developed regions this rate is approximately 1.7–2.4%.7,8 In children, sepsis is commonly operationalized as infection-associated organ dysfunction, and delayed recognition may lead to shock, multi-organ failure, treatment interruption, and worse outcomes.9,10 Therefore, clarifying clinical correlates and factors associated with sepsis during CIN remains a key issue in pediatric oncology supportive care.
However, evidence targeting sepsis risk specifically in the early window after the first onset of induction-phase CIN remains limited. Previous studies and routine practice have largely relied on ALL risk stratification, treatment intensity, and single inflammatory markers such as CRP and PCT to characterize infection risk.11 In contemporary care, antimicrobial prophylaxis or empiric therapy during CIN may alter pathogen spectra and increase the likelihood of resistant colonization, which can reduce the discriminatory value of traditional single markers in this time window.12 In addition, induction chemotherapy frequently causes mucosal barrier injury. Such injury may facilitate microbial translocation and bloodstream infection, plausibly contributing to sepsis during CIN. Together, these considerations support further evaluation of clinically accessible factors assessed early at CIN onset, including oral mucosal status and integrated inflammation–nutrition indices.
Sepsis is characterized by a dysregulated host response involving complex interactions between inflammation and immunity, often evolving from an initial hyperinflammatory phase to later immunosuppression.13,14 Emerging evidence also indicates a bidirectional negative feedback between inflammation and nutritional status.15 In recent years, the C-reactive protein–to–albumin ratio (CAR) has been proposed as an integrated inflammation–nutrition index and has been reported to be associated with disease severity and outcomes in pediatric critical illness and adult sepsis.16–18 Meanwhile, red cell distribution width (RDW), an indicator reflecting systemic inflammation and bacterial infection, has attracted significant attention in sepsis research.19,20
This study is based on a single-center retrospective cohort of children with ALL who developed CIN. We focused on this population because CIN onset marks a clinically vulnerable period with heightened susceptibility to infection, during which sepsis remains a major concern. Using Cox proportional hazards regression with time zero at the first episode of CIN, we aimed to identify factors associated with subsequent sepsis onset during induction chemotherapy. These findings are hypothesis-generating and warrant validation in larger, multicenter cohorts.
Materials and Methods
Study Population: Enrollment and Follow-Up
We conducted a single-center, retrospective, observational cohort study, with data from the cohort of 292 pediatric ALL patients extracted from the Jiahe electronic medical record system of the First Affiliated Hospital of Xinjiang Medical University. Eligible patients were screened based on discharge diagnoses and verified through medical record review, which was performed independently by qualified physicians. Inclusion criteria were: (i) ages 1–18 years; (ii) diagnosis of ALL according to the Recommendations for the Diagnosis and Treatment of Acute Lymphoblastic Leukemia in Children (Fourth Revision)21 issued by the Hematology Group of the Pediatrics Branch of the Chinese Medical Association; and (iii) receipt of induction therapy at initial diagnosis. Exclusion criteria were: (i) prior chemotherapy or other anticancer treatments, such as immunotherapy, radiotherapy, or hematopoietic stem cell transplantation, before admission; (ii) history of other malignancies; (iii) glucocorticoid exposure within one month before enrollment.
All eligible patients were enrolled at the first occurrence of CIN during induction therapy; the calendar date of first CIN onset was defined as the index time (T0). The primary outcome was sepsis. Follow-up started at T0 and ended at sepsis onset or censoring at neutrophil recovery (NEU ≥ 1.5 × 10^9/L), whichever occurred first. Patients who discontinued treatment for personal reasons or died before developing sepsis were censored at the date of discontinuation or death. Complete blood counts were obtained approximately every 3 days. To avoid underestimation of follow-up in the presence of events, the median follow-up time was estimated using the reverse Kaplan–Meier method. During follow-up, children who developed sepsis were classified as sepsis cases, whereas those who did not develop sepsis were treated as censored observations, most commonly at neutrophil recovery.
Definition
In this study, risk stratification of ALL was based on the CCLG-ALL-2018 protocol, which comprehensively evaluated patients clinical features, cellular immunology, biological characteristics, and treatment responses. Following a 7-day prednisone trial, prednisone response was categorized as good prednisone response (GPR) or poor prednisone response (PPR): a peripheral blood blast count < 1.0 × 10^9/L indicated GPR, whereas ≥ 1.0 × 10^9/L indicated PPR. In conjunction with minimal residual disease levels, patients were classified into three categories: low-risk, intermediate-risk, and high-risk. We defined pediatric sepsis using the Pediatric Sequential Organ Failure Assessment (pSOFA) score.22 An increase of ≥2 points in pSOFA indicates organ dysfunction and supports the diagnosis of sepsis. As a sensitivity analysis, we repeated the Cox regression analyses using a PELOD-2–based sepsis definition to assess the robustness of the identified associations. Nutritional status was assessed in accordance with World Health Organization’s standards for evaluating children’s nutritional status. Using age- and sex-specific standard deviation (Z-score) reference.23 Based on these assessment, children were categorized into two groups: well-nourished and malnourished. Oral mucosal status was evaluated according to WHO oral mucosal grading standards. Grades were as follows: Grade 0, normal mucosa without symptoms; Grade 1, mucosa erythema/edema without ulcers; Grade 2, ulcers present with ability to consume solid food; Grade 3, severe ulceration restricting intake to liquids; Grade 4, inability to take oral nutrition due to severe pain or lesions, requiring parenteral nutritional support.24
Treatment
All children with ALL received standard induction chemotherapy. Induction chemotherapy followed the CCLG-ALL-2018 protocol for the treatment of pediatric ALL in China. The regimen comprised the following: vincristine, 1.5 mg/m2 per dose (maximum single dose 2 mg), administered once weekly for four doses; daunorubicin, 30 mg/m2 per dose, administered once weekly for two to four doses; L-asparaginase, 5,000–10,000 U/m2 per dose, for a total of ten doses; and dexamethasone (DXM) 6–8 mg/m2/day from day 8 to day 28, followed by a taper from days 29 to day 35 in which the daily dose was reduced by half every two days until discontinuation.
During induction chemotherapy, if a patient developed neutropenia, granulocyte colony-stimulating factor (G-CSF) was routinely administered to promote granulocyte recovery. A short-acting G-CSF preparation was given at 3–5 µg/kg/day and continued until the neutrophil count returned to the normal range, after which it was discontinued. In the event of fever, stepwise anti-infective therapy was initiated according to the Chinese Guidelines for Clinical Diagnosis and Treatment of Antimicrobial Agents in Patients with Febrile Neutropenia (2016 Edition).25 The initial empirical antibiotic regimen was selected based on the site of infection, clinical presentation, and ancillary test findings. Broad-spectrum antibiotics were used as first-line therapy; for example, meropenem (10–20 mg/kg every 8 hours) to provide broad coverage. If clinical symptoms improved within 48–72 hours or the identified pathogen was susceptible to narrower-spectrum agents, de-escalation was implemented—for example, switching to targeted treatment such as ceftriaxone (20–80 mg/kg/d, once daily) for Enterobacterales-susceptible infections. For patients with fever persisting ≥ 72 hours without microbiological evidence of infection, empirical antifungal therapy was initiated-with voriconazole as the first choice-and subsequently adjusted according to mycological findings and imaging results. All medications were administered by trained nursing staff at 10:00 a.m. (Beijing time).
Data Collection
Data collected included: (i) general information(sex and age); (ii) Clinical characteristics(risk group, prednisone response, immunophenotype, and oral mucosal status); (iii) laboratory indices, including white blood cell count [WBC], platelet count [PLT], neutrophil count [NEU], C-reactive protein [CRP], procalcitonin [PCT], red cell distribution width [RDW], interleukin-6 [IL-6], albumin [ALB], and others routinely measured parameters. All laboratory variables were extracted from the first test results obtained within 24 hours after the first onset of chemotherapy-induced neutropenia (CIN; index time), rather than peak values during the CIN period. Oral mucosal status was assessed within the same 24-hour window by trained physicians using a standardized clinical assessment protocol and was documented in the medical record.
Statistical Methods
Statistical analysis was conducted using R version 4.3.0. Normality of continuous variables was assessed with the Shapiro–Wilk test, non-normally distributed data are reported as median (interquartile range, IQR). Categorical variables were summarized as frequency and percentage (n, %). Initially, univariable comparisons were performed to screen candidate variables, selecting those with P < 0.05. Univariable Cox proportional hazards regression was subsequently conducted for each variable, and variables with P < 0.05 were selected for collinearity assessment. Collinearity was evaluated using correlation heatmaps and variance inflation factor (VIF), and highly collinear variables were removed. The remaining variables were incorporated into a multivariable Cox regression to identify variables independently associated with sepsis among children undergoing chemotherapy for ALL who developed neutropenia. Survival differences were visualized with Kaplan-Meier (KM) curves and compared using the Log rank test. Missingness for all variables included in the analyses was 0%; therefore, no imputation was performed (Supplementary Figure 1).
Results
Baseline Characteristics
During induction therapy, 292 children with ALL were enrolled at the index time. Sepsis occurred in 48 patients(16.4%) during the CIN window, whereas 244 patients(83.6%) achieved neutrophil recovery (NEU ≥ 1.5 × 109/L). The participant flow and outcome classification during the CIN window are shown (Figure 1). The median follow-up time from T0 was 4 days (IQR 3–8; range 2–12). Notably, approximately half of the sepsis events occurred after CIN lasted more than 7 days (Supplementary Table 1). In sensitivity analyses, 45 of 48 (93.8%) pSOFA-defined sepsis cases also met the PELOD-2 criteria assessed in the same window, indicating high concordance. The cohort included 131 boys (45%) and 161 girls (55%). No statistically significant differences in baseline characteristics-sex, age, prednisone response and nutritional status-were observed between the two groups (P > 0.05) (Table 1). Regarding risk stratification, the proportion of sepsis in the high-risk group was higher than that in the low and intermediate-risk groups (P = 0.001). Sepsis occurred more frequently among children with oral mucosal suppuration (P < 0.001). Overall, 11 laboratory/clinical indicators differences between groups (P < 0.05). Including risk level, NEU, RDW, WBC, PLT, CRP, PCT, IL-6, CAR,ALB, and oral mucosal status. Among sepsis cases, a total of 31 isolates were identified from positive blood cultures obtained during the CIN window. Gram-negative bacteria predominated (58.1%, 18/31), followed by Gram-positive bacteria (32.3%, 10/31) and fungi (9.6%, 3/31). The most frequently isolated pathogens were Escherichia coli (n = 11) and Pseudomonas aeruginosa (n = 7). Details of pathogen distribution are provided (Supplementary Table 2).
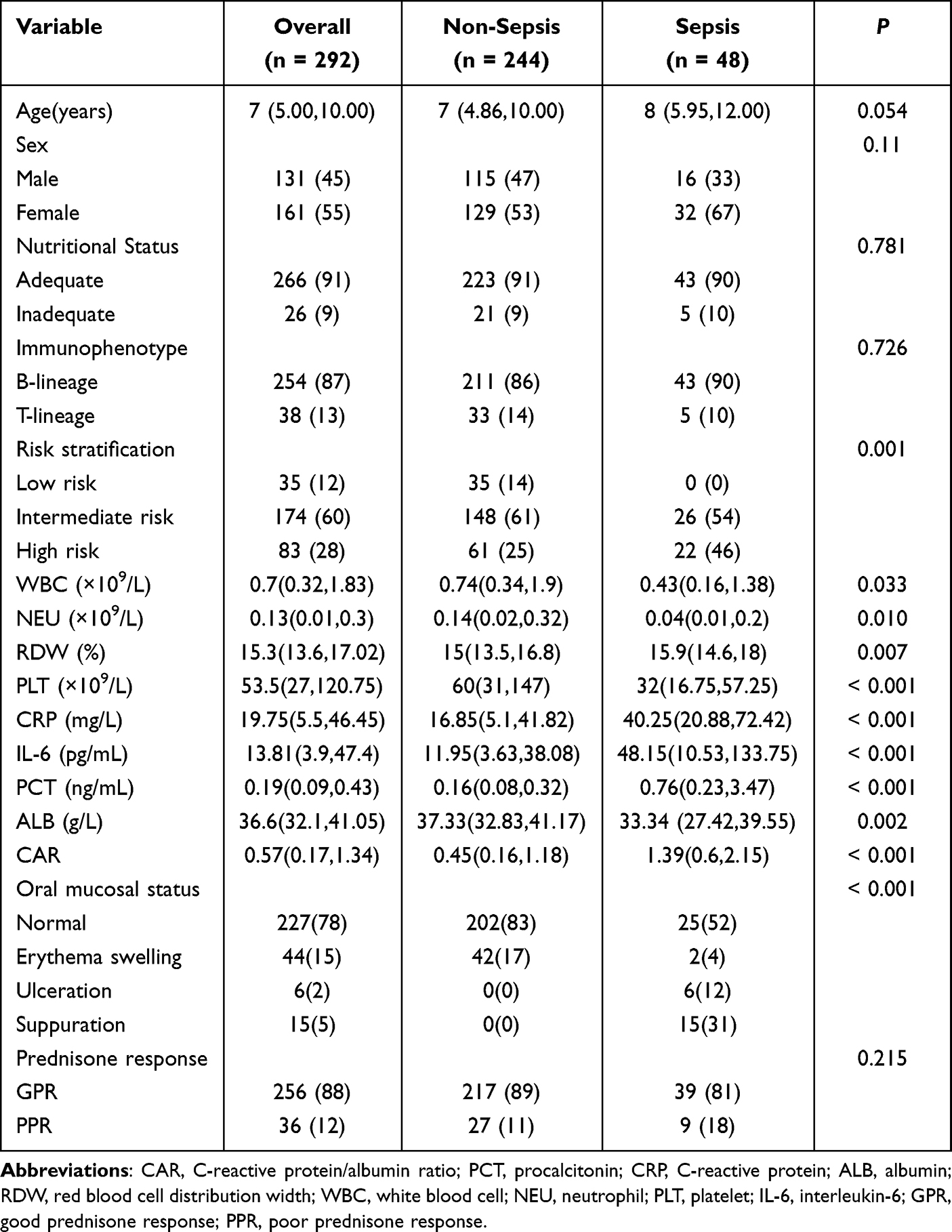 |
Table 1 Comparison of Baseline Characteristics Between CIN Recovery and Sepsis Groups |
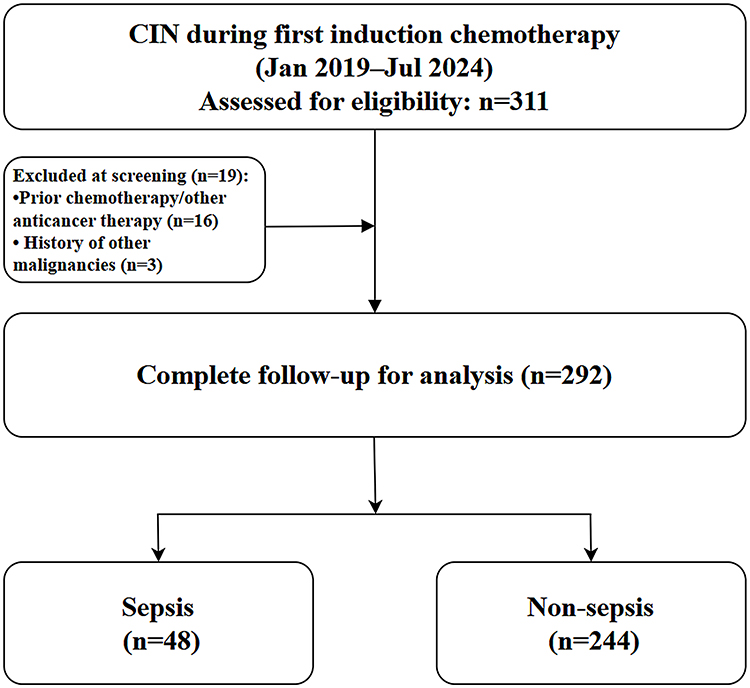 |
Figure 1 Modeling Workflow for Sepsis Development in Pediatric ALL Patients with CIN. |
Univariate Cox Regression Analysis
Based on preliminary between-group comparisons (P < 0.05), 11 candidate variables were entered into univariable Cox proportional hazards models for time to sepsis: WBC, NEU, RDW, PLT, CRP, PCT, IL-6, ALB, CAR, risk stratification, and oral mucosal status. In the univariable analyses, RDW, PLT, CRP, PCT, IL-6, CAR, risk stratification, and oral mucosal status met the screening threshold of P< 0.05 screening threshold and were retained for multivariable modeling (Table 2).
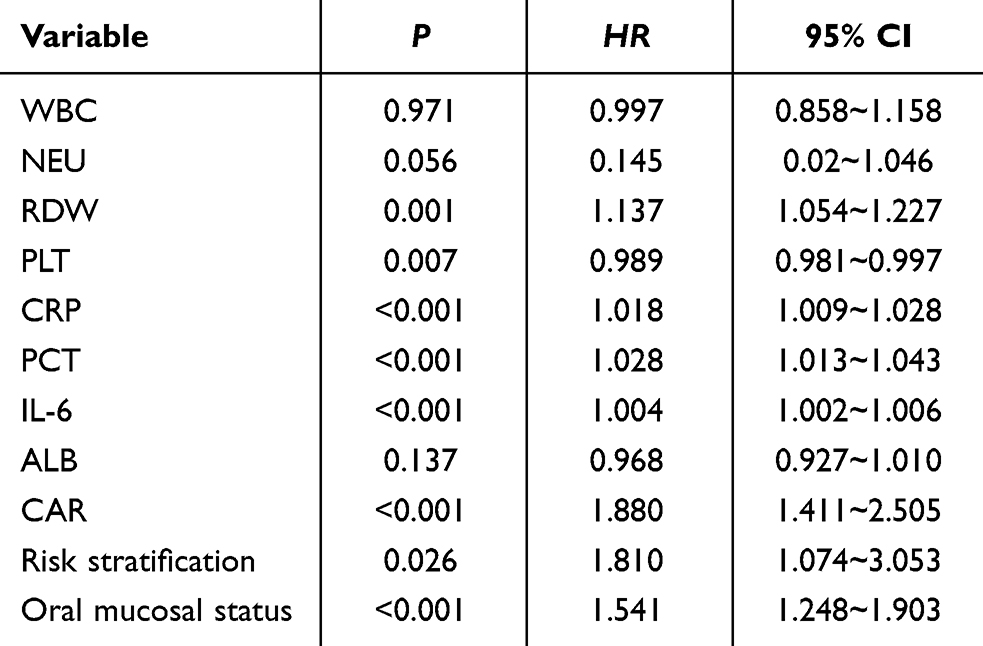 |
Table 2 Univariable Cox Regression for Time to Sepsis During the CIN Episode (Analytic N = 292; Events = 48) |
Collinearity Analysis
To evaluate pairwise correlations among variables that were significant in the univariable Cox analyses (P < 0.05) and to assess potential collinearity, we computed Pearson correlation coefficients. The analysis included eight key variables: RDW, PLT, CRP, PCT, IL-6, CAR, risk stratification, and oral mucosal status. We generated and visualized the Pearson correlation matrix (Figure 2). Most absolute correlation coefficients were < 0.4, suggesting a low overall risk of collinearity. Notably, CRP and CAR were highly correlated(r = 0.98, P < 0.001), indicating a strong association between these variables.
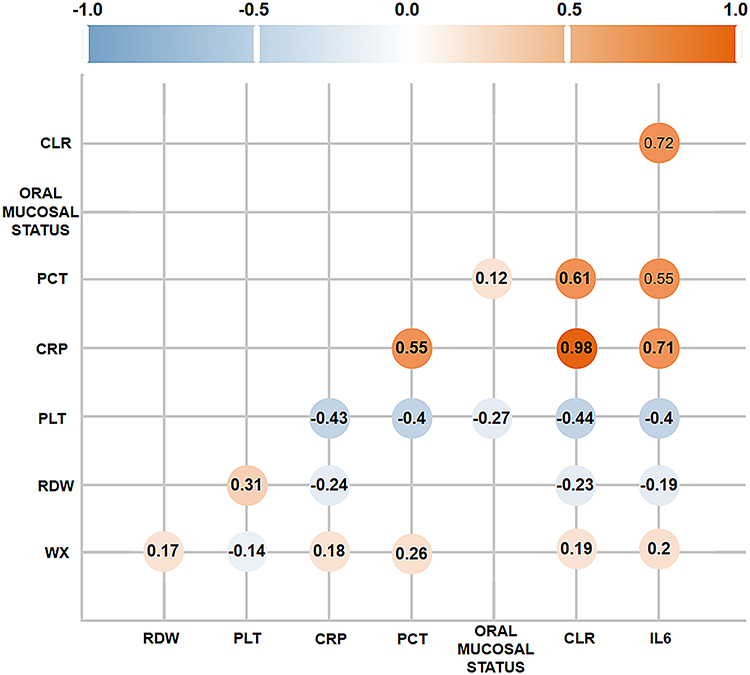 |
Figure 2 Pearson correlation matrix of variables included in the collinearity assessment. Circle color indicates the direction of correlation (blue, negative; Orange, positive), and circle size reflects the magnitude of the correlation coefficient (r). |
To further quantify multicollinearity among the above variables, we calculated variance inflation factors (VIF) for the eight variables (RDW, PLT, CRP, PCT, IL-6, CAR, risk stratification, and oral mucosal status). Consistent with the Pearson correlation matrix, CRP and CAR exhibited marked collinearity, with VIF exceeding the commonly used threshold of 10 (CRP: 11.23; CAR: 11.42; corresponding tolerances 1/VIF: 0.09 and 0.08, respectively) (Table 3). Given that CAR is derived from C-reactive protein and albumin (CRP-to-albumin ratio), we excluded CRP to avoid redundancy and re-assessed multicollinearity. After removing CRP, all remaining variables showed VIF < 10, indicating no problematic multicollinearity (Supplementary Table 3).
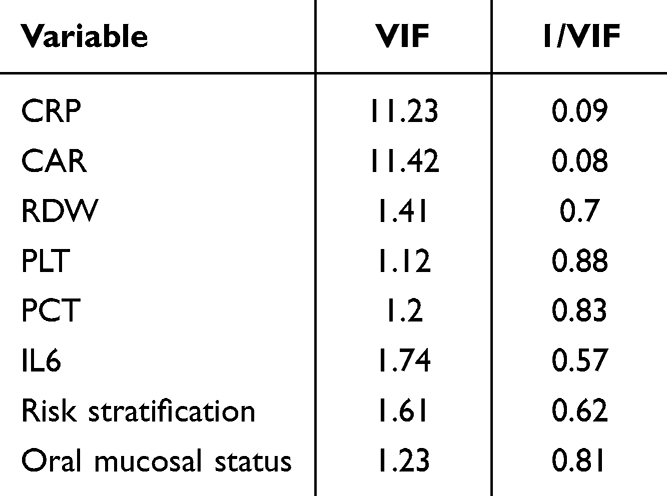 |
Table 3 Variance Inflation Factor (VIF) Analysis for Univariate Cox Model Covariates |
Multivariate Cox Regression Analysis
Based on the VIF results indicating marked collinearity between CRP and CAR, CRP was excluded. The remaining seven variables (RDW, PLT, PCT, CAR, IL-6, risk stratification, and oral mucosal status) were entered into a multivariable Cox proportional hazards model. In the adjusted analysis, RDW (HR = 1.126, 95% CI: 1.028–1.233; P = 0.011), PCT (HR = 1.017, 95% CI: 1.002–1.036; P = 0.043), CAR (HR = 1.407, 95% CI: 1.088–1.806; P = 0.050), and oral mucosal status (HR = 1.336, 95% CI: 1.061–1.681; P = 0.014) remained independently associated with the risk of sepsis. PLT, IL-6, and risk stratification were not significantly associated with sepsis risk (Table 4). In sensitivity analyses using PELOD-2–defined sepsis, the direction and significance of the identified associations were not meaningfully changed compared with the primary pSOFA-based analysis.
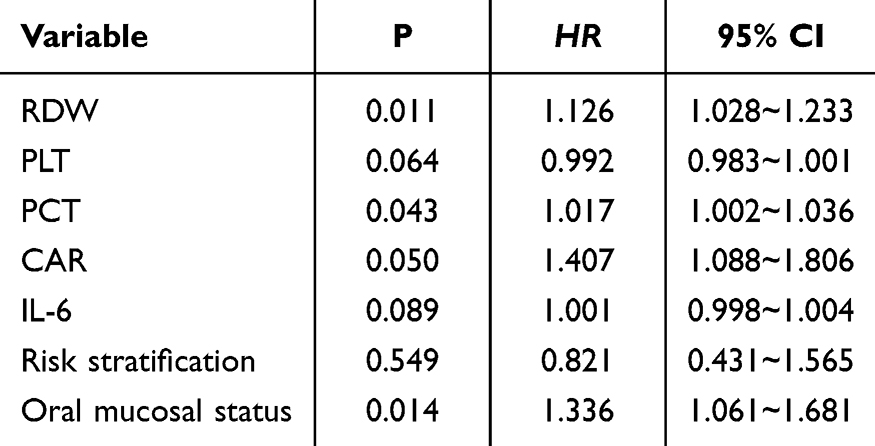 |
Table 4 Multivariable Cox Regression for Time to Sepsis During the CIN Episode (Analytic N = 292; Events = 48) |
Kaplan-Meier Curve
To further characterize the time-to-sepsis patterns associated with variables retained in the multivariable analysis, we generated Kaplan–Meier curves for sepsis-free survival stratified by oral mucosal status and by quartiles of CAR, RDW, and PCT. Sepsis-free survival differed significantly across strata for all variables (log-rank P < 0.05). Overall, higher levels of CAR, RDW, and PCT, as well as more severe oral mucosal impairment, were associated with lower sepsis-free survival, consistent with an increased risk of sepsis (Figure 3).
 |
Figure 3 Kaplan–Meier curves of sepsis-free survival during CIN episode. (A) Oral mucosal status (Normal, Erythema swelling, Ulceration, Suppuration). (B-D) CAR, RDW and PCT were categorized into quartiles using rank-based grouping (approximately equal numbers per group; Q1 = lowest, Q4 = highest) based on the distribution in the overall cohort. Shaded areas indicate 95% confidence intervals and tick marks denote censoring. P values were obtained from Log rank tests. Numbers at risk are shown below each panel. |
Discussion
ALL remains the most common hematologic malignancy in children. With continuous refinements in treatment protocols and the implementation of risk-adapted therapy, long-term survival has improved markedly in recent decades.26,27 However, treatment-related complications remain major determinants of prognosis, particularly severe infections during CIN.28 Previous reports indicate that 40–70% of children with ALL experience infections during CIN, and sepsis in this context is associated with chemotherapy delays and an increased risk of relapse.29,30 Prior studies have suggested that the degree of immunosuppression, the duration of neutropenia, and inflammatory markers such as CRP are associated with sepsis risk in children with ALL during CIN.31 With ongoing changes in supportive care, antibiotic strategies, and antimicrobial resistance, traditional single markers may be less informative for early assessment at CIN onset.32 In this context, integrated inflammation–nutrition indices and indicators of barrier injury may provide complementary information. Accordingly, we examined the associations of oral mucosal status, CAR, PCT, and RDW with sepsis risk during CIN.12 Notably, traditional ALL risk stratification was not retained as an independent factor after multivariable adjustment in this CIN-defined cohort, which may relate to the restricted early CIN window, the distribution of risk categories in our sample, and the limited number of sepsis events.
During CIN, reductions in neutrophil count and function are associated with increased susceptibility to infection rather than directly causing sepsis. Prolonged neutropenia further compromises host defense, predisposing patients to secondary bloodstream and opportunistic infections.33 In our cohort, impaired oral mucosal status was independently associated with a higher hazard of sepsis. Chemotherapy-induced mucosal injury disrupts the epithelial barrier, facilitating microbial translocation and systemic infection. Recent studies have shown that ulcerative mucositis compromises local immune defense, and that reduced oral microbiota diversity is associated with an increased risk of bacteremia.34,35 These findings suggest that the severity of oral mucosal injury may reflect systemic infection risk beyond local manifestations. In the present study, oral mucosal status was classified using predefined criteria. More severe findings—such as ulcers or erythema—were associated with a higher hazard of sepsis, suggesting that oral mucosal assessment may serve as clinically accessible indicator for early risk assessment during the CIN window. Further prospective studies are needed to determine whether targeted oral care could modify sepsis risk in this population.
Inflammation and nutritional status are interdependent factors that jointly influence susceptibility to infection.36 IL-6, a key cytokine in the inflammatory cascade, activates the Janus kinase/signal transducer and activator of transcription 3 (JAK/STAT3) pathway, which regulates acute-phase protein synthesis. Through this mechanism, elevated IL-6 levels promote increased production of CRP, a positive acute-phase reactant, and decreased ALB, a negative acute-phase reactant. Consequently, the CAR provides an integrated measure reflecting both systemic inflammation and nutritional reserve.37,38 Several studies have confirmed the clinical relevance of CAR. In a study of 178 children with sepsis admitted to intensive care, Mohamed et al found that higher CAR values at admission were linked to greater mortality, with each 1-unit rise in CAR increasing the risk by about 1.075-fold.16 In newborns, other studies17,18 showed that high CAR levels were independently associated with Gram-negative bacteremia and more severe infections. In adults, Zhou and Oh et al39,40 reported similar findings, showing that higher CAR were associated with worse outcomes in both severe infections and cancers, with effect sizes between 1.62 and 1.80 for each 1-unit increase. In our study, every 1-unit increase in CAR was also associated with a higher risk of sepsis (adjusted HR ≈ 1.41; see Results). Altogether, these findings suggest that CAR, influenced by IL-6–mediated inflammation, could represent a readily obtainable inflammatory-nutritional index independently associated with a higher hazard of sepsis during chemotherapy-induced neutropenia.
Given the multifactorial nature of sepsis development, markers reflecting both systemic inflammation and hematologic changes—such as PCT and RDW—were also evaluated. This study found that both PCT and RDW were independently associate with sepsis. PCT has been widely used as an inflammation-related biomarker in bacterial infections and has been reported to rise early even in the setting of CIN. Dagher and Nazer reported that initial PCT levels in children with bacteremia (mean 2.35 ng/mL) were markedly higher than in those without bacteremia (0.37 ng/mL), indicating a strong association between elevated PCT and infection severity.41,42
In this context, PCT may provide additional information for characterizing sepsis risk during CIN. RDW, which reflects variability in red blood cell size, has recently been recognized as a broader marker of inflammation, oxidative stress, and microcirculatory dysfunction. In a meta-analysis including more than 40,000 sepsis patients, Wu et al found that each 1-unit increase in RDW was associated with a 14% higher mortality.43 Consistent with prior evidence, RDW in our cohort was independently associated with sepsis among children with ALL during CIN. Because RDW is routinely available from complete blood counts, it offers a practical and low-cost indicator that may support heightened clinical vigilance during high-risk periods.
In summary, this single-center retrospective study identified that oral mucosal status, CAR, PCT, and RDW were independently associated with sepsis during induction-phase CIN in children with ALL. These findings are hypothesis-generating and require prospective validation in larger, multicenter cohorts. Together, these factors may facilitate risk awareness and closer surveillance in vulnerable patients; however, their clinical utility requires prospective validation. Although these findings are based on associations rather than causality, they provide a basis for future strategies to improve sepsis prevention and outcomes in this population.
This study has several limitations. As a single-center retrospective analysis with a relatively small sample size, the potential for selection bias cannot be excluded. In addition, although G-CSF administration followed a standardized institutional protocol, residual variability in timing or dose may still exist and could influence neutrophil recovery and infection risk. Some confounding factors—such as variability in anti-infective therapy, supportive care, and nursing compliance—were not fully captured. Additionally, cytokine profiling in this study was limited to IL-6, which precluded a more comprehensive assessment of the inflammatory network. Future multicenter, large-scale prospective studies are needed to validate these findings, incorporate additional dynamic biomarkers, and more systematically evaluate factors associated with sepsis during CIN as well as their generalizability. Such efforts will help strengthen the evidence base for risk-adapted infection prevention and supportive-care strategies in children with ALL.
Ethics Statements
This study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (approval number: K202412-96). Given the retrospective design and anonymized nature of patient data, the requirement for written informed consent was waived in accordance with institutional and national regulations. The study complied with the ethical standards of the Declaration of Helsinki.
Acknowledgments
We are also grateful to our peers for their suggestions and review of the manuscript. All the authors have agreed to the manuscript.
Funding
This work was supported by the Science and Technology Department of Xinjiang Uygur Autonomous Region. The funded projects include Impact Analysis of Pre-chemotherapy Serum Metabolomics and Nutritional Index on the Prognosis of Children with Acute Lymphoblastic LeukemiA (2024D01C169) and Research on Basic Science of Major Childhood Diseases, Special Disease Cohort Studies, and Early Warning Model Construction (2024B03038).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen X, Lei X-Y, Guan X-M. Risk factors for recurrence of childhood acute lymphoblastic leukemia after treatment with the Chinese children’s cancer group all-2015 protocol. Chin J Contemp Pediatr. 2024;26(7):701–11. doi:10.7499/j.issn.1008-8830.2401010
2. Brown PA, Shah B, Advani A, et al. Acute lymphoblastic leukemia, version 2.2021, nccn clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(9):1079–1109. doi:10.6004/jnccn.2021.0042
3. Rheingold SR, Bhojwani D, Ji L, et al. Determinants of survival after first relapse of acute lymphoblastic leukemia: a children’s oncology group study. Leukemia. 2024;38(11):2382–2394. doi:10.1038/s41375-024-02395-4
4. Boccia R, Glaspy J, Crawford J, Aapro M. Chemotherapy-induced neutropenia and febrile neutropenia in the us: a beast of burden that needs to be tamed? Oncologist. 2022;27(8):625–636. doi:10.1093/oncolo/oyac074
5. Podpeskar A, Crazzolara R, Kropshofer G, et al. Supportive methods for childhood acute lymphoblastic leukemia then and now: a compilation for clinical practice. Front Pediatr. 2022;10:980234. doi:10.3389/fped.2022.980234
6. Ozturk AP, Koc B, Zulfikar B. Acute complications and survival analysis of childhood acute lymphoblastic leukemia: a 15-year experience. clin lymphoma myeloma leuk. Clin Lymphoma Myeloma Leuk. 2021;21(1):e39–e47. doi:10.1016/j.clml.2020.08.025
7. Yin T, Han J, Hao J, et al. Clinical characteristics and risk factors of acute lymphoblastic leukemia in children with severe infection during maintenance treatment. Cancer Med. 2023;12(19):19372–19382. doi:10.1002/cam4.6495
8. Inaba H, Pei D, Wolf J, et al. Infection-related complications during treatment for childhood acute lymphoblastic leukemia. Ann Oncol. 2017;28(2):386–392. doi:10.1093/annonc/mdw557
9. Miranda M, Nadel S. Pediatric sepsis: a summary of current definitions and management recommendations. Curr Pediatr Rep. 2023;11(2):29–39. doi:10.1007/s40124-023-00286-3
10. Goggin KP, Lu L, Lee DE, et al. Severe sepsis during treatment for childhood leukemia and sequelae among adult survivors. JAMA Netw Open. 2024;7(3):e242727. doi:10.1001/jamanetworkopen.2024.2727
11. Chuang CL, Yeh HT, Niu KY, Chen CB, Seak CJ, Yen CC. Diagnostic performances of procalcitonin and c-reactive protein for sepsis: a systematic review and meta-analysis. Eur J Emerg Med. 2025;32(4):248–258. doi:10.1097/MEJ.0000000000001235
12. Kairiene I, Tarutyte G, Vaisnore R, et al. Evaluation of biomarkers for intestinal damage in pediatric acute lymphoblastic leukemia. Sci Rep. 2025;15(1):16899. doi:10.1038/s41598-025-98947-4
13. Chousterman BG, Swirski FK, Weber GF. Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol. 2017;39(5):517–528. doi:10.1007/s00281-017-0639-8
14. Liu L, Sun B. Neutrophil pyroptosis: new perspectives on sepsis. Cell Mol Life Sci. 2019;76(11):2031–2042. doi:10.1007/s00018-019-03060-1
15. Wischmeyer PE. Nutrition Therapy in Sepsis. Crit Care Clin. 2018;34(1):107–125. doi:10.1016/j.ccc.2017.08.008
16. Mohamed SA, ElHawary R. C-reactive protein/albumin ratio as an independent predictor of mortality in critically ill pediatric patients. J Child Sci. 2020;10(01):e1–e11. doi:10.1055/s-0040-1701623
17. Gunes H, Yurttutan S, Cobanusagi M, Doganer A. Crp/albumin ratio: a promising marker of gram-negative bacteremia in late-onset neonatal sepsis. Turk Arch Pediatr. 2021;56(1):32–36. doi:10.14744/TurkPediatriArs.2020.99076
18. Li T, Li X, Wei Y, et al. Predictive value of c-reactive protein-to-albumin ratio for neonatal sepsis. J Inflamm Res. 2021;14:3207–3215. doi:10.2147/JIR.S321074
19. Gregoriano C, Heilmann E, Molitor A, Schuetz P. Role of PROCALCITONIN USE IN THE MANAGEMENT OF SEPSIS. J Thorac Dis. 2020;12(Suppl 1):S5–S15. doi:10.21037/jtd.2019.11.63
20. Katsaros M, Paschos P, Giouleme O. Red cell distribution width as a marker of activity in inflammatory bowel disease: a narrative review. Ann Gastroenterol. 2020;33(4):348–354. doi:10.20524/aog.2020.0486
21. Hematology Group SoP. Chinese medical association, pediatrics ebotcjo. recommendations for diagnosis and treatment of acute lymphocyte leukemia in children (4th revision). Chin J Pediatr. 2014;52(9):641–644.doi:10.3760/cma.j.issn.0578-1310.2014.09.001.
22. Matics TJ, Sanchez-Pinto LN. Adaptation and Validation of a pediatric sequential organ failure assessment score and evaluation of the sepsis-3 definitions in critically ill children. JAMA Pediatr. 2017;171(10):e172352. doi:10.1001/jamapediatrics.2017.2352
23. Pedretti L, Massa S, Leardini D, et al. Role of nutrition in pediatric patients with cancer. Nutrients. 2023;15(3):710. doi:10.3390/nu15030710
24. Abdalla-Aslan R, Bonomo P, Keefe D, et al. Guidance on mucositis assessment from the mascc mucositis study group and ISOO: an international delphi study. EClinicalMedicine. 2024;73:102675. doi:10.1016/j.eclinm.2024.102675
25. Chinese Society of Hematology CMA, Chinese Medical Doctor Association HB. Chinese guidelines for the clinical application of antibacterial drugs for agranulocytosis with fever. Zhonghua Xue Ye Xue Za Zhi. 2016;37(5):353–359.doi:10.3760/cma.j.issn.0253-2727.2016.05.001.
26. Kim H, Yoon SH, Kang S, et al. Improved survival in pediatric acute lymphoblastic leukemia through therapy intensification based on minimal residual disease and protocol-driven early response risk classification. Blood Res. 2025;60(1):40. doi:10.1007/s44313-025-00085-3
27. Correa BT, Silva GSS, Mendes WJS, et al. Association of the clinical profile and overall survival of pediatric patients with acute lymphoblastic leukemia. Front Pediatr. 2023;11:1223889. doi:10.3389/fped.2023.1223889
28. Malczewska M, Kosmider K, Bednarz K, Ostapinska K, Lejman M, Zawitkowska J. Recent advances in treatment options for childhood acute lymphoblastic leukemia. Cancers. 2022;14(8):2021. doi:10.3390/cancers14082021
29. Moriyama K, Nishida O. Targeting cytokines, pathogen-associated molecular patterns, and damage-associated molecular patterns in sepsis via blood purification. Int J Mol Sci. 2021;22(16):8882. doi:10.3390/ijms22168882
30. Segulja S, Vranesevic K, Dordevic A, Roganovic J. Infections in Children with Acute Lymphoblastic Leukemia. Medicina. 2024;60(9):1395. doi:10.3390/medicina60091395
31. Lu YA, Liu HC, Hou JY, Chiu NC, Huang TH, Yeh TC. The clinical impact of primary granulocyte-colony stimulating factor prophylaxis in children with acute lymphoblastic leukemia who underwent induction chemotherapy. J Microbiol Immunol Infect. 2024;57(6):879–886. doi:10.1016/j.jmii.2024.08.004
32. Zama D, Leardini D, Baccelli F, et al. Recommendations for antibacterial prophylaxis in children receiving chemotherapy: a joint initiative of sitip and infectious disease group of aieop. Ital J Pediatr. 2025;51(1):309. doi:10.1186/s13052-025-02141-1
33. Benzoni NS, Carey KA, Bewley AF, et al. Temperature trajectory subphenotypes in oncology patients with neutropenia and suspected infection. Am J Respir Crit Care Med. 2023;207(10):1300–1309. doi:10.1164/rccm.202205-0920OC
34. Zecha J, Raber-Durlacher JE, Brandt BW, et al. Oral MICROBIAL CHANGES, ORAL MUCOSITIS AND FEBRILE NEUTROPENIA DURING MYELOSUPPRESSIVE CHEMOTHERAPY IN PATIENTS DIAGNOSED WITH A SOLID TUMOR OR LYMPHoma. Front Oral Health. 2024;5:1461463. doi:10.3389/froh.2024.1461463
35. AlHarbi SG, Almushayt AS, Bamashmous S, Abujamel TS, Bamashmous NO. The Oral microbiome of children in health and disease-a literature review. Front Oral Health. 2024;5:1477004. doi:10.3389/froh.2024.1477004
36. Park JE, Chung KS, Song JH, et al. The C-reactive protein/albumin ratio as a predictor of mortality in critically ill patients. J Clin Med. 2018;7(10):333. doi:10.3390/jcm7100333
37. Atas H, Atak T, Kartal SP, Tas Aygar G. The association of c-reactive protein to albumin ratio with lichen planus. Rev Assoc Med Bras. 2025;71(2):e20241166. doi:10.1590/1806-9282.20241166
38. Mantovani A, Garlanda C. Humoral innate immunity and acute-phase proteins. N Engl J Med. 2023;388(5):439–452. doi:10.1056/NEJMra2206346
39. Zhou X, Fu S, Wu Y, et al. C-reactive protein-to-albumin ratio as a biomarker in patients with sepsis: a novel lasso-cox based prognostic nomogram. Sci Rep. 2023;13(1). doi:10.1038/s41598-023-42601-4
40. Oh TK, Song IA, Lee JH. Clinical usefulness of c-reactive protein to albumin ratio in predicting 30-day mortality in critically ill patients: a retrospective analysis. Sci Rep. 2018;8(1):14977. doi:10.1038/s41598-018-33361-7
41. Nazer LH, Awad W, Thawabieh H, et al. Procalcitonin-guided management and duration of antibiotic therapy in critically ill cancer patients with sepsis (pro-can study): a randomized controlled trial. Crit Care Explor. 2024;6(10):e1173. doi:10.1097/CCE.0000000000001173
42. Dagher H, Chaftari AM, Hachem R, et al. Procalcitonin level monitoring in antibiotic de-escalation and stewardship program for patients with cancer and febrile neutropenia. Cancers. 2024;16(20):3450. doi:10.3390/cancers16203450
43. Wu H, Liao B, Cao T, Ji T, Huang J, Ma K. Diagnostic value of rdw for the prediction of mortality in adult sepsis patients: a systematic review and meta-analysis. Front Immunol. 2022;13:997853. doi:10.3389/fimmu.2022.997853
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multidrug-Resistant Bacteria on Critically Ill Patients with Sepsis at Hospital Admission: Risk Factors and Effects on Hospital Mortality
Maia MDO, da Silveira CDG, Gomes M, Fernandes SES, Bezerra de Santana R, de Oliveira DQ, Amorim FFP, Neves FDAR, Amorim FF
Infection and Drug Resistance 2023, 16:1693-1704
Published Date: 23 March 2023
Characteristics, Outcomes, and Clinical Indicators of Bloodstream Infections in Neutropenic Patients with Hematological Malignancies: A 7-Year Retrospective Study
Wang S, Song Y, Shi N, Yin D, Kang J, Cai W, Duan J
Infection and Drug Resistance 2023, 16:4471-4487
Published Date: 8 July 2023
Pathogenic Profile Characteristics and Clinical Risk Factor Analysis of Patients Who Died from Sepsis Combined with Pulmonary Infection by Metagenomic Next-Generation Sequencing
Chen SX, Lin R, Shi JL, Lin W, Yu XF, Chen JY
Infection and Drug Resistance 2023, 16:7695-7705
Published Date: 19 December 2023
Prevalence and Risk Factors of Childhood Asthma in Jazan Region, Saudi Arabia
Gohal G, Yassin A, Darraj H, Darraj A, Maghrabi R, Abutalib YB, Talebi S, Mutaen AA, Hamdi S
Journal of Asthma and Allergy 2024, 17:33-43
Published Date: 20 January 2024
Survival and Treatment Outcomes of Childhood Acute Lymphoblastic Leukemia in a Low-Middle Income Country: A Single-Center Experience in West Java, Indonesia
Ramadhan MH, Sari NM, Peryoga SU, Susanah S
Journal of Blood Medicine 2024, 15:77-85
Published Date: 19 February 2024