Back to Journals » Journal of Pain Research » Volume 19
Risk Factors and Nomogram for Postpartum Myofascial Pelvic Pain: A Prospective Cohort Study
Authors Cai Y, Cai Y, Chen Y, Hu Y, Zhang Y, Lin Y ![]()
Received 31 March 2026
Accepted for publication 17 June 2026
Published 24 June 2026 Volume 2026:19 613518
DOI https://doi.org/10.2147/JPR.S613518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D'Souza
Yueyun Cai,* Yuting Cai,* Yuefen Chen,* Yuanling Hu,* Yu Zhang, Yueqing Lin
Department of Gynaecology and Obstetrics, Zhangzhou Affiliated Hospital of Fujian Medical University, Zhangzhou, Fujian, 363000, People’s Republic of China
*Yueyun Cai, Yuting Cai, Yuefen Chen and Yuanling Hu contributed equally to this work
Correspondence: Yu Zhang, Department of Gynaecology and Obstetrics, Zhangzhou Affiliated Hospital of Fujian Medical University, 193 Shuixian Street, Longwen District, Zhangzhou, Fujian, 363000, People’s Republic of China, Tel +86-596-2089541, Email [email protected] Yueqing Lin, Department of Gynaecology and Obstetrics, Zhangzhou Affiliated Hospital of Fujian Medical University, 193 Shuixian Street, Longwen District, Zhangzhou, Fujian, 363000, People’s Republic of China, Tel +86-0596-2089556, Email [email protected]
Background: Myofascial pelvic pain (MFPP) is a common but underrecognized postpartum complication. Early identification of women at increased risk may facilitate targeted surveillance and timely postpartum rehabilitation. This study aimed to identify risk factors for postpartum MFPP and develop a predictive nomogram.
Methods: This prospective cohort study included 671 women who delivered at a tertiary hospital between December 2022 and December 2024. Postpartum MFPP was diagnosed using standardized trigger point assessments by two independent blinded specialists. Participants were randomly assigned to training (n = 505) and validation (n = 166) sets. Multivariable logistic regression was used to identify independent risk factors and construct a nomogram.
Results: The incidence of MFPP was 12.9% in the training set and 11.4% in the validation set. Four independent risk factors were identified: neonatal birth weight ≥ 4 kg (OR 3.632), vaginal laceration (OR 2.448), parity ≥ 3 (OR 2.975), and history of dyspareunia (OR 2.381). The nomogram achieved an AUC of 0.681 in the training set and 0.656 in the validation set, indicating moderate discriminative ability. Calibration analysis showed acceptable agreement between predicted and observed risks, and decision curve analysis suggested a positive net clinical benefit across clinically relevant threshold probabilities.
Conclusion: Macrosomia, vaginal laceration, grand multiparity, and history of dyspareunia are independently associated with postpartum MFPP. The proposed nomogram may serve as a preliminary and clinically accessible tool for early risk stratification, although further multicenter validation is needed before widespread clinical application.
Keywords: postpartum period, myofascial pelvic pain, risk factors, nomogram, predictive model, prospective cohort study
Introduction
Myofascial pelvic pain (MFPP) is a common yet frequently underrecognized musculoskeletal disorder characterized by the presence of myofascial trigger points (MTrPs) in the pelvic floor muscles, lower abdominal wall, and associated fascial structures, manifesting as acute or chronic pain that substantially impairs physical function, psychological well-being, and quality of life.1–3 During pregnancy and childbirth, the pelvic floor undergoes profound biomechanical stress, including sustained postural adaptation to accommodate the growing fetus, direct mechanical trauma during vaginal delivery, and subsequent tissue remodeling during the postpartum period.4–6 These pregnancy- and delivery-related mechanical stresses may induce pelvic floor muscle microtrauma, fascial irritation, local inflammatory responses, and the formation of myofascial trigger points, thereby contributing to postpartum pelvic pain and functional impairment. Clinically, early recognition of women at increased risk is important because timely surveillance and targeted postpartum rehabilitation may help reduce persistent pain, sexual dysfunction, urinary symptoms, and impaired quality of life. Epidemiological studies have demonstrated that MFPP affects a considerable proportion of postpartum women, with reported incidence ranging from 12.9% to 29.9% in the early postpartum period and up to 57.1% in certain high-risk cohorts.7–9 Moreover, MFPP is increasingly recognized as an important contributor to chronic pelvic pain and is frequently associated with sexual dysfunction, urinary symptoms, and diminished quality of life if left untreated.10–14
Despite increasing recognition of postpartum MFPP, several issues remain unresolved. First, diagnosis relies mainly on physical examination, but substantial heterogeneity exists across studies in examination techniques, trigger point definitions, palpation pressure, and documentation methods, limiting comparability and reproducibility.15 Recent terminology reports from the International Continence Society and related professional organizations have emphasized the importance of standardized assessment of pelvic floor muscle tenderness, tone, and trigger points.16,17 Second, although previous studies have identified several potential risk factors for MFPP or related pelvic floor disorders, including vaginal delivery, perineal trauma, episiotomy, higher parity, neonatal macrosomia, advanced maternal age, and excessive gestational weight gain, the findings remain inconsistent across populations and diagnostic criteria.8,18–22 Third, most existing studies have focused on individual risk factors rather than their combined predictive value, and clinically accessible prediction tools specifically designed for postpartum MFPP remain limited.
Clinical prediction models and nomograms can translate multiple risk factors into individualized risk estimates and have been increasingly used in obstetrics and gynecology.20,23–33 Compared with models requiring specialized imaging, electrophysiological testing, or biomarker measurements, a nomogram based on routinely available maternal and obstetric variables may be easier to apply in postpartum care. However, prediction models for postpartum MFPP remain scarce, and some previously reported models have been limited by complex predictor requirements, lack of validation, or insufficient diagnostic standardization. Therefore, there is a need for a rigorously designed prospective study that applies standardized diagnostic procedures, identifies independent risk factors from readily available clinical variables, and evaluates the performance and potential clinical utility of a practical risk prediction tool.
We hypothesized that routinely collected maternal and obstetric characteristics could be used to identify women at increased risk of postpartum MFPP. Accordingly, this prospective cohort study was conducted to: (1) identify independent risk factors for postpartum MFPP using prospectively collected data from women delivering at a tertiary hospital; (2) develop a nomogram-based prediction model incorporating readily available clinical variables; and (3) evaluate the model’s discrimination, calibration, and clinical utility in separate training and validation cohorts. By providing a preliminary and clinically accessible tool for early risk stratification, this study aims to support timely recognition and targeted postpartum surveillance for women at increased risk of MFPP.
Materials and Methods
Study Design, Registration, and Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Zhangzhou Affiliated Hospital of Fujian Medical University (No. 2025KYZ161). The study was registered with the Chinese Clinical Trial Registry (No. ChiCTR2600119151). All participants provided written informed consent prior to enrollment.
Study Population
A total of 671 women who delivered at our institution between December 1, 2022, and December 30, 2024, and completed the postpartum follow-up assessment were enrolled.
Inclusion criteria were: (1) antenatal care and delivery at our institution; (2) complete obstetric records; (3) singleton pregnancy; (4) completion of pelvic pain assessment at 1–3 months postpartum; and (5) provision of written informed consent.
Exclusion criteria were: (1) acute genitourinary infection or confirmed organic disease (eg., urolithiasis); (2) history of pelvic trauma, pelvic surgery, or pelvic malignancy; (3) central nervous system disorders or definite neurological conditions (eg., sciatica); (4) psychiatric disorders or cognitive impairment that would preclude study cooperation; and (5) prior receipt of pelvic floor rehabilitation or pain-related interventions.
Sample Size and Data Partition
Using R software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria), the total cohort of 671 participants was randomly allocated into a training set and a validation set in a 7:3 ratio. The training set (n = 505) was used for variable selection and model development, and the validation set (n = 166) was reserved for model validation. Randomization was performed using a computer-generated random number sequence to ensure reproducibility.
Diagnostic Criteria for Postpartum MFPP
All participants underwent a standardized pelvic myofascial pain assessment at 1–3 months postpartum. To minimize diagnostic bias, a prospective double-blind design was implemented: two independent specialists with expertise in pelvic floor disorders evaluated each participant separately, with both examiners blinded to each other’s findings and to the study grouping.15 In cases of disagreement, a third senior specialist (attending physician level) performed a blinded reassessment to establish the final diagnosis. All examiners were specialists in gynecology and obstetrics with clinical experience in postpartum pelvic floor disorders and myofascial pain assessment. Before the study began, the examiners received unified training and used the same diagnostic criteria and standardized assessment form, including predefined definitions of myofascial trigger points, palpation sites, pain referral patterns, and the VAS threshold for clinically significant pain, to reduce inter-examiner variability.
The assessment protocol began with a routine gynecologic examination and pelvic ultrasound to exclude organic causes of pelvic pain. Thereafter, a standardized physical examination was conducted to identify myofascial trigger points (MTrPs) in the pelvic floor musculature. MTrPs were defined as localized, hypersensitive nodules within taut, shortened, or thickened muscle bands, with palpation eliciting distinct local pain and often referred pain to the lower abdomen, buttocks, perineum, vagina, rectum, or urethra.1,2 Pain intensity was quantified using a visual analog scale (VAS) ranging from 0 (no pain) to 10 (worst imaginable pain). A diagnosis of postpartum MFPP was established when MTrPs were identified and palpation of the trigger point produced a VAS score of ≥3, indicating clinically significant pain.9
Data Collection and Variables
Demographic, obstetric, and clinical data were prospectively collected using a standardized case report form. Variables assessed included maternal age (<35 vs. ≥35 years), parity (<3 vs. ≥3), gravidity (<2 vs. ≥2), mode of delivery (vaginal vs. cesarean section), neonatal birth weight (≥4 kg [macrosomia] vs. <4 kg), episiotomy (yes vs. no), vaginal laceration (yes vs. no), premature rupture of membranes (yes vs. no), method of placental delivery (spontaneous vs. manual removal), postpartum urinary incontinence (yes vs. no), history of dyspareunia before pregnancy (yes vs. no), and laboratory parameters including white blood cell count and serum albumin level.
Statistical Analysis and Model Development
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and R software (version 4.2.2). Categorical variables were presented as frequencies and percentages [n (%)]. Comparisons between groups were performed using the chi-square test or Fisher’s exact test, as appropriate. All tests were two-sided, and a P value <0.05 was considered statistically significant. In the training set, candidate variables were first identified based on univariable analysis and clinical relevance. Variables with P < 0.10 in univariable analysis or those considered clinically relevant were entered into a multivariable logistic regression model to identify independent risk factors for MFPP, using the occurrence of MFPP as the dependent variable. Variables with P <0.10 in univariable analysis or those with established clinical relevance were entered into the multivariable model. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). A nomogram was constructed based on the independent predictors identified from the multivariable logistic regression model to provide an individualized risk prediction tool.29,30 Model performance was evaluated in both the training and validation sets using the following metrics:25
Discrimination: Assessed by the concordance index (C-index) and the area under the receiver operating characteristic curve (AUC). An AUC of 0.5 indicates no discrimination, 0.7–0.8 acceptable discrimination, and >0.8 excellent discrimination.
Calibration: Evaluated using the Hosmer–Lemeshow goodness-of-fit test and calibration plots, which compare predicted probabilities with observed outcomes.
Clinical Utility: Assessed by decision curve analysis (DCA), which quantifies the net benefit of using the model across a range of threshold probabilities.30
Internal validation was performed in the training set using bootstrap resampling with 200 iterations to estimate the optimism-corrected AUC. Hold-out validation was conducted in the validation set randomly derived from the same single-center cohort. Differences in AUC between cohorts were compared using the DeLong test.
Results
Study Population and Baseline Characteristics
A total of 671 women who met the eligibility criteria were enrolled in this prospective cohort study. Using R software, the cohort was randomly allocated into a training set (n = 505, 75.3%) and a validation set (n = 166, 24.7%) in a 7:3 ratio. The baseline characteristics of both sets are summarized in Table 1. No statistically significant differences were observed between the training and validation sets with respect to demographic characteristics, obstetric variables, or clinical parameters (all P > 0.05), indicating that random allocation achieved satisfactory comparability between the two cohorts.
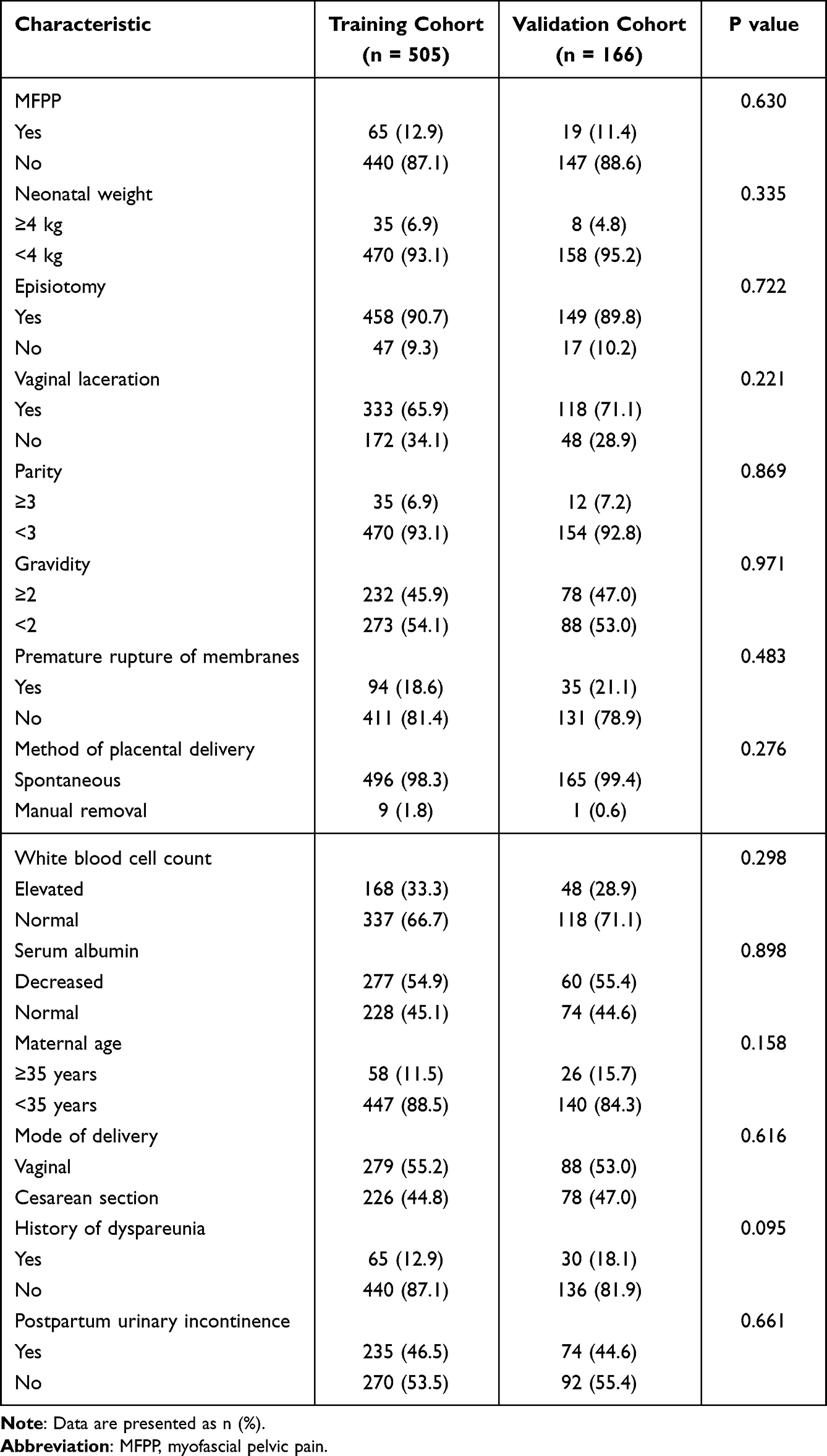 |
Table 1 Patient Characteristics in the Training and External Validation Cohorts (n=671) |
Incidence of Postpartum MFPP
In the training set, 65 of 505 participants (12.9%) were diagnosed with postpartum MFPP according to the standardized diagnostic criteria (VAS score ≥3 upon MTrP palpation). In the validation set, the incidence was 11.4% (19/166). The overall incidence in the total cohort was 12.5% (84/671).
Comparison of MFPP and Non-MFPP Groups in the Training Set
In the training set, participants with MFPP (MFPP group) and those without MFPP (non-MFPP group) were compared across all clinical variables. As shown in Table 2, the MFPP group had significantly higher proportions of the following factors compared with the non-MFPP group: neonatal birth weight ≥4 kg (16.9% vs. 5.5%, P = 0.001), vaginal laceration (52.3% vs. 31.4%, P = 0.001), parity ≥3 (16.9% vs. 6.9%, P = 0.001), and history of dyspareunia (21.5% vs. 11.6%, P = 0.025). No statistically significant differences were observed between the two groups for other variables, including episiotomy, gravidity, premature rupture of membranes, method of placental delivery, white blood cell count, serum albumin level, maternal age, mode of delivery, or postpartum urinary incontinence (all P > 0.05).
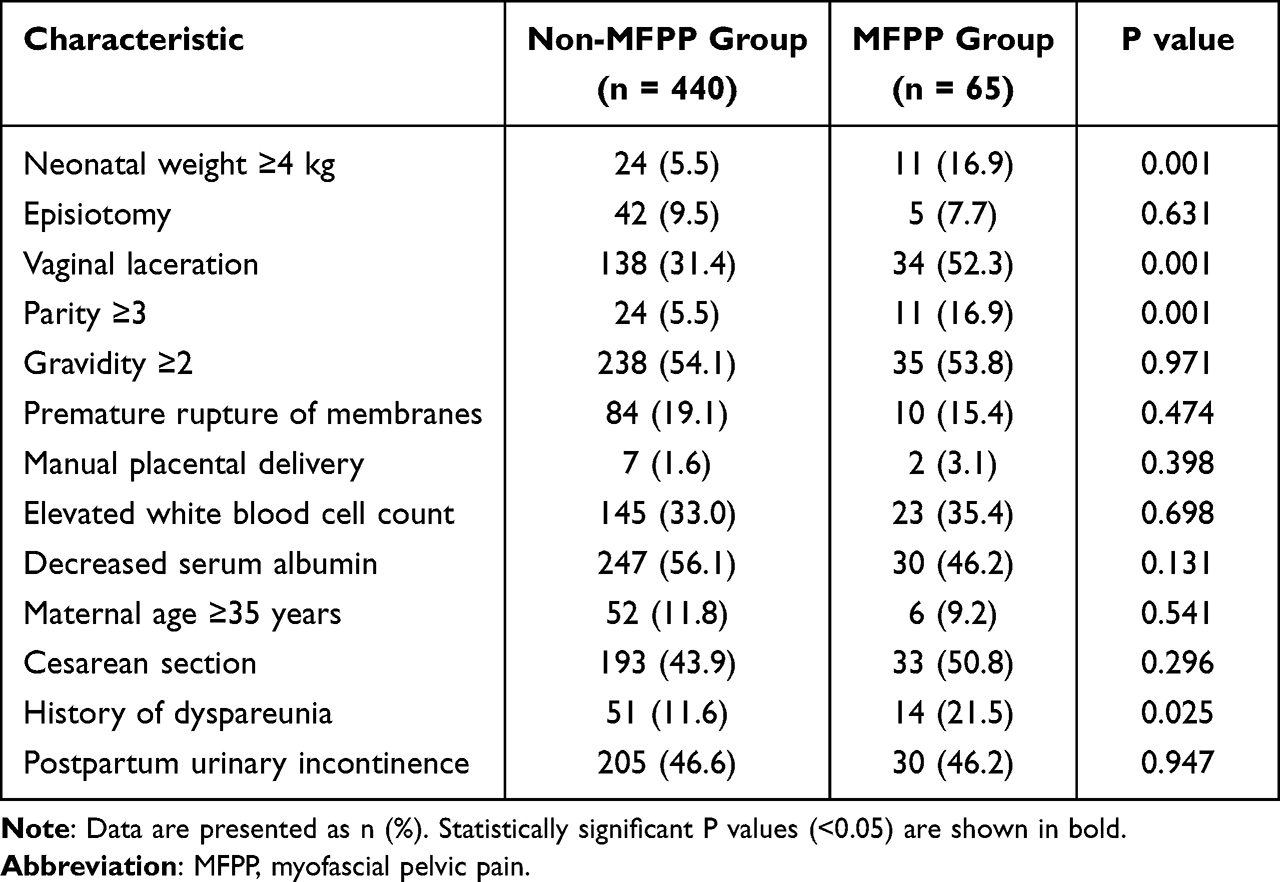 |
Table 2 Comparison of Characteristics Between MFPP and Non-MFPP Groups in the Training Set (n = 505) |
Multivariable Logistic Regression Analysis
Multivariable logistic regression analysis was performed in the training set to identify independent risk factors for postpartum MFPP. All variables with clinical relevance were entered into the model simultaneously. The results are presented in Table 3. Four variables emerged as independent predictors of MFPP: Neonatal birth weight ≥4 kg (OR 3.632; 95% CI 1.570–8.402; P = 0.003); Vaginal laceration (OR 2.448; 95% CI 1.419–4.222; P = 0.001); Parity ≥3 (OR 2.975; 95% CI 1.295–6.834; P = 0.010); History of dyspareunia (OR 2.381; 95% CI 1.194–4.747; P = 0.014); No other variables showed statistically significant associations with MFPP in the multivariable model.
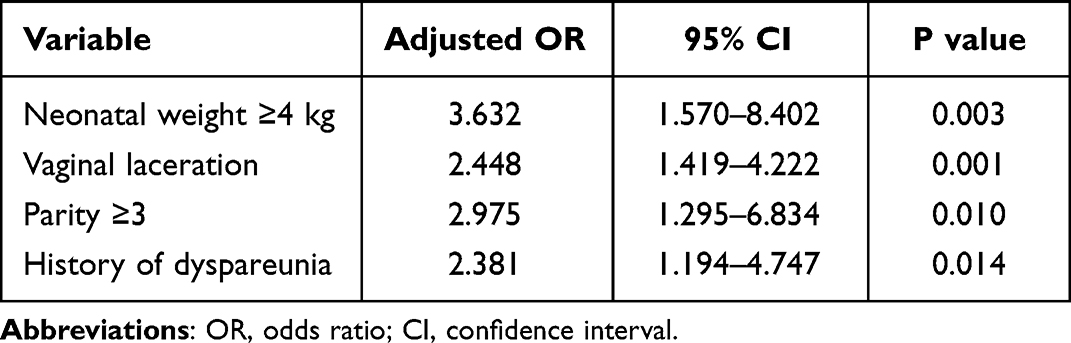 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with Postpartum MFPP in the Training Set (n = 505) |
Nomogram Development and Performance
A nomogram was constructed based on the four independent predictors identified in the multivariable logistic regression model to provide a visual tool for individualized risk prediction of postpartum MFPP (Figure 1). Each predictor was assigned a weighted point score, and the total points were used to estimate the probability of MFPP occurrence.
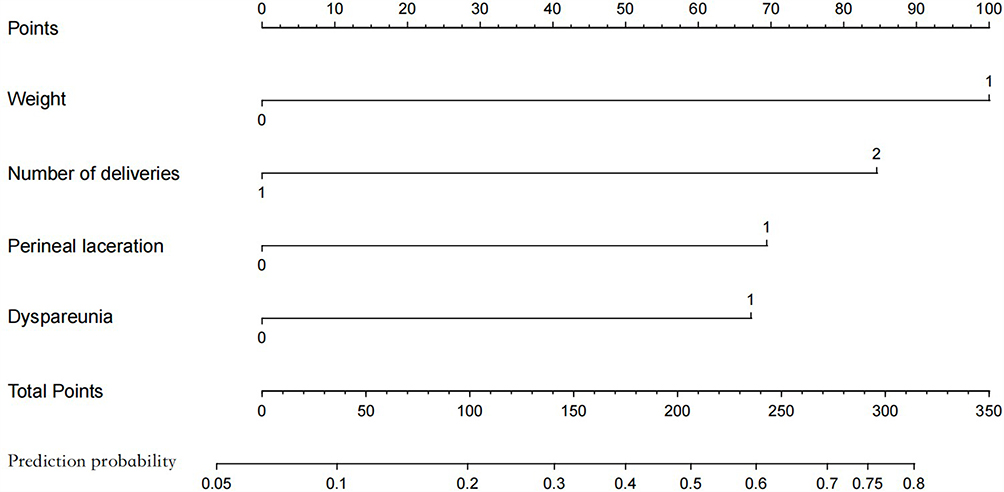 |
Figure 1 Nomogram for predicting postpartum myofascial pelvic pain (MFPP).The nomogram was developed based on four independent predictors identified in the multivariable logistic regression analysis: neonatal birth weight ≥4 kg, vaginal laceration, parity ≥3, and history of dyspareunia. Each predictor is assigned a point value according to its contribution to the model. The total points are calculated by summing the points for all predictors and are then projected onto the prediction probability scale to estimate the individual probability of postpartum MFPP. For binary variables, 0 indicates absence of the factor and 1 indicates presence of the factor, unless otherwise specified in the figure. |
Model Discrimination
The discriminative ability of the nomogram was assessed using the area under the receiver operating characteristic curve (AUC). In the training set, the model achieved an AUC of 0.681 (95% CI 0.612–0.750), indicating moderate discriminative capacity (Figure 2A). Internal validation using bootstrap resampling with 200 iterations yielded a mean AUC of 0.682, closely approximating the original training set AUC and confirming satisfactory internal stability. In the validation set, the nomogram demonstrated an AUC of 0.656 (95% CI 0.507–0.804), indicating that the model maintained moderate discriminative ability in an independent cohort (Figure 2B). DeLong test revealed no statistically significant difference between the AUC values of the training and validation sets (P = 0.734). Overall, these findings indicate that the nomogram had moderate, but not strong, discriminative ability; therefore, the statistical significance of the identified risk factors should not be interpreted as evidence of strong predictive performance.
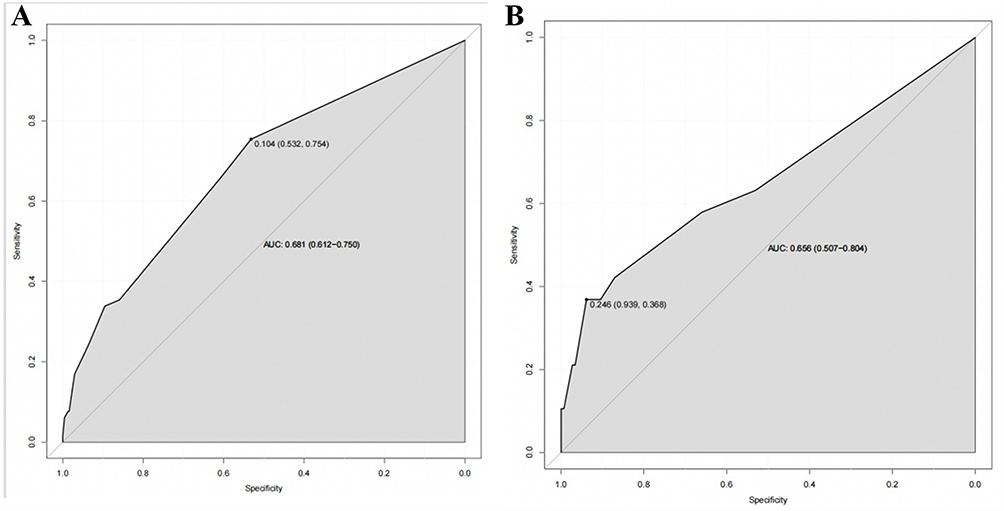 |
Figure 2 Receiver operating characteristic (ROC) curves for the nomogram in the training and validation cohorts.(A) ROC curve of the nomogram in the training cohort. The area under the ROC curve (AUC) was 0.681, with a 95% confidence interval (CI) of 0.612–0.750. (B) ROC curve of the nomogram in the validation cohort. The AUC was 0.656, with a 95% CI of 0.507–0.804. The black curve represents the discriminative performance of the nomogram. The grey diagonal reference line represents a model with no discriminative ability. The marked point on each curve indicates the selected cut-off value, with the corresponding specificity and sensitivity shown in parentheses. Abbreviations: AUC, area under the receiver operating characteristic curve; CI, confidence interval; ROC, receiver operating characteristic. |
Model Calibration
Calibration of the prediction model was evaluated using the Hosmer–Lemeshow goodness-of-fit test and calibration plots. The Hosmer–Lemeshow test yielded non-significant P values in both the training set (P = 0.521) and the validation set (P = 0.634), indicating no evidence of poor fit. Calibration plots demonstrated good agreement between predicted probabilities and observed outcomes in both cohorts (Figure 3A and B). The calibration curves showed slight deviations from the ideal 45-degree diagonal line at the extremes of predicted risk but remained within acceptable ranges, suggesting that the model’s predictions are well-calibrated overall.
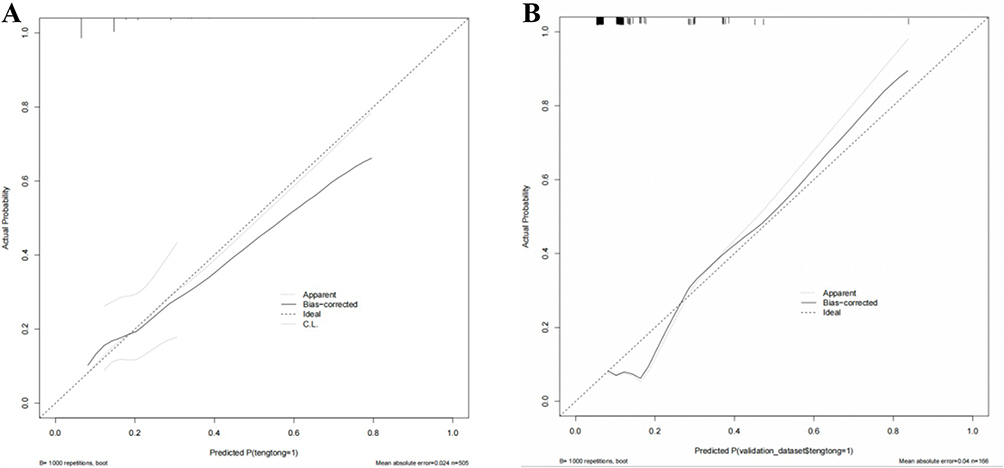 |
Figure 3 Calibration curves for the nomogram in the training and validation cohorts.(A) Calibration curve of the nomogram in the training cohort. (B) Calibration curve of the nomogram in the validation cohort. The dotted line represents the ideal calibration line, indicating perfect agreement between predicted and observed probabilities. The apparent curve represents the original model performance, and the bias-corrected curve represents the bootstrap-corrected calibration performance. The rug marks along the upper margin indicate the distribution of predicted probabilities among participants. A curve closer to the ideal line indicates better agreement between predicted and observed risks. Bootstrap resampling was performed with 1000 repetitions. Abbreviations: MFPP, myofascial pelvic pain. |
Clinical Utility
Decision curve analysis (DCA) was performed to evaluate the clinical net benefit of the nomogram across a range of threshold probabilities.30 As shown in Figure 4A (training set) and Figure 4B (validation set), the nomogram provided a positive net benefit across clinically relevant threshold probability ranges compared with the “treat-all” or “treat-none” strategies. This finding indicates that implementation of the prediction model would support clinical decision-making by identifying high-risk women who may benefit from early intervention, without incurring unnecessary harm.
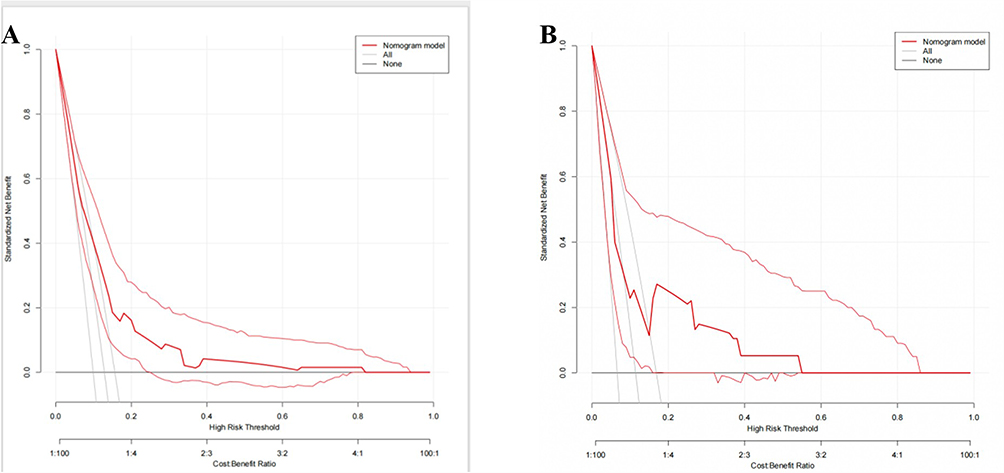 |
Figure 4 Decision curve analysis (DCA) for the nomogram in the training and validation cohorts. (A) DCA of the nomogram in the training cohort. (B) DCA of the nomogram in the validation cohort. The red line represents the nomogram model. The grey line represents the treat-all strategy, assuming that all postpartum women would receive intervention. The black horizontal line represents the treat-none strategy, assuming that no postpartum women would receive intervention. The x-axis indicates the threshold probability, and the y-axis indicates the standardized net benefit. A higher net benefit across a clinically relevant range of threshold probabilities indicates greater potential clinical utility of the nomogram. Abbreviations: DCA, decision curve analysis; MFPP, myofascial pelvic pain. |
Discussion
Overview of the Present Study
In this prospective cohort study of 671 postpartum women, we systematically investigated the risk factors associated with postpartum myofascial pelvic pain (MFPP) using a standardized diagnostic protocol incorporating independent blinded assessments by two specialists and adjudication by a third senior specialist. The overall incidence of MFPP in our cohort was 12.5%, consistent with previously reported estimates in early postpartum populations.7,9 Our multivariable analysis identified four independent risk factors: neonatal birth weight ≥4 kg, vaginal laceration, parity ≥3, and a history of dyspareunia. Based on these predictors, we developed a nomogram that provides individualized risk estimates with moderate discriminative ability (AUC 0.681 in the training set, 0.656 in the validation set), satisfactory calibration, and positive net clinical benefit across clinically relevant threshold probabilities. To our knowledge, this is among the first studies to develop and validate a clinically accessible prediction tool specifically for postpartum MFPP, with rigorous diagnostic standardization and independent validation.
Comparison with Existing Literature
Our findings extend and corroborate previous research on risk factors for MFPP and other pelvic floor disorders. The association between neonatal macrosomia (birth weight ≥4 kg) and MFPP (OR 3.632) aligns with the established understanding that excessive mechanical load during delivery predisposes to pelvic floor injury.18,22 Prolonged stretching and compression of the pelvic floor muscles and fascia during the passage of a large fetus may lead to microtrauma, ischemia, and subsequent myofascial trigger point formation.4,6 This mechanical insult is compounded by the sustained postural adaptations required during pregnancy to accommodate a larger fetus, which may further strain the lumbopelvic musculature.5 Our findings are consistent with those of Cardaillac et al,12 who reported that higher neonatal birth weight was associated with persistent postpartum pain, and with Ross et al,7 who identified macrosomia as a contributing factor in the development of chronic pelvic pain syndromes.
Vaginal laceration emerged as another strong independent predictor (OR 2.448). This finding supports the hypothesis that direct tissue trauma during delivery disrupts fascial integrity, triggers an inflammatory cascade, and promotes aberrant scar formation, all of which are recognized contributors to myofascial pain.15 Recent evidence suggests that fascia is not merely a passive structural element but a biologically active tissue containing nociceptive nerve endings that can become sensitized following injury.6 The healing process following vaginal laceration may involve fibrosis and nerve entrapment, creating a nidus for persistent pain. Our results are consistent with those of Tenfelde et al,9 who found that perineal trauma during delivery was associated with musculoskeletal pelvic pain at one year postpartum, and with Meister et al,15 who emphasized the importance of assessing perineal scar tenderness as a component of pelvic floor myofascial examination.
The association between parity ≥3 and MFPP (OR 2.975) reflects the cumulative impact of multiple pregnancies and deliveries on pelvic floor structures. Each pregnancy imposes repeated biomechanical stress, and the cumulative effect may exceed the reparative capacity of the pelvic floor, leading to progressive fascial densification, fibrosis, and reduced tissue elasticity.4,5 This “material fatigue” concept has been invoked to explain the dose-response relationship between parity and pelvic floor dysfunction.23 Our finding is consistent with previous studies reporting higher parity as a risk factor for chronic pelvic pain and pelvic floor disorders.8,19,34 Importantly, the effect of parity remained significant even after adjustment for other delivery-related factors, suggesting that both cumulative and individual birth events contribute independently to MFPP risk.
Unexpected or Novel Findings
One noteworthy finding of our study was the association between a history of dyspareunia before pregnancy and postpartum MFPP. This finding is clinically interesting because previous dyspareunia may indicate pre-existing pelvic floor hypertonicity, myofascial dysfunction, or heightened pain sensitivity before pregnancy. However, this association should be interpreted with caution. A history of dyspareunia may also reflect an unmeasured pre-pregnancy pain phenotype, selection or reporting bias, or residual confounding by psychosocial factors such as anxiety, depressive symptoms, pain catastrophizing, sleep disturbance, or social support, which were not assessed in the present study. Therefore, this finding should be regarded as hypothesis-generating rather than evidence of a direct causal relationship. Future studies incorporating pre-pregnancy pelvic floor assessment and psychosocial measures are needed to clarify whether dyspareunia is an independent predictor, a marker of pre-existing pain vulnerability, or part of a broader biopsychosocial pain phenotype.
This finding aligns with recent literature emphasizing the importance of preconception and antenatal assessment in predicting postpartum outcomes. Einig et al21 reported that pelvic floor myofascial pain is frequently associated with lower urinary tract symptoms and pelvic floor hypertonicity, suggesting that these conditions may share a common underlying pathophysiology. Similarly, Golanska et al20 highlighted the role of biopsychosocial modulation in myofascial pain syndromes, emphasizing that psychological distress and anxiety can lower pain thresholds and increase vulnerability to pain conditions. Our finding extends this concept to the perinatal period, suggesting that preconception pain history should be considered a key component of risk assessment for postpartum pelvic floor disorders.
Relationship to Broader Theoretical Frameworks
Our findings can be interpreted within the framework of the biopsychosocial model of pain,20,21 which posits that pain experiences are shaped by the dynamic interplay of biological, psychological, and social factors. From a biological perspective, the mechanical insults of macrosomia and vaginal laceration represent physical triggers that initiate tissue damage and inflammation. The repeated biomechanical stress of multiple pregnancies (parity ≥3) contributes to cumulative structural changes in the pelvic floor, including fascial densification, fibrosis, and altered tissue biomechanics.4,6 These biological processes converge to create a vulnerable musculoskeletal substrate. From a psychological perspective, a history of dyspareunia may serve as a marker of pre-existing central sensitization, heightened pain vigilance, or anxiety related to pelvic pain.11,20 Women with such a history may be more likely to interpret postpartum pelvic sensations as painful, engage in pain catastrophizing, and develop chronic pain behaviors. The physiological stress of childbirth may further amplify these psychological processes, contributing to the transition from acute to chronic pain. From a social perspective, postpartum recovery occurs within a context of sleep deprivation, caregiving demands, and often limited social support, all of which can modulate pain perception and coping.9,21
Our results also align with the “mechanical load–myofascial injury–dysfunction” continuum proposed by Gromakovskis6 and others.4,5 According to this model, sustained or excessive mechanical loading (eg., from macrosomia, vaginal laceration, or multiple pregnancies) disrupts fascial integrity, leading to inflammation, fibrosis, and the formation of myofascial trigger points. These structural changes, in turn, alter muscle activation patterns, create aberrant nociceptive input, and contribute to functional impairment. This continuum provides a coherent explanatory framework for our findings, linking the identified risk factors to the pathophysiology of MFPP. Furthermore, our study underscores the value of risk stratification and early intervention as key strategies in the prevention of chronic pain syndromes. The moderate predictive performance of our nomogram (AUC 0.68) is comparable to that of other well-established prediction tools in obstetrics and gynecology,23–25 and the positive net benefit observed in decision curve analysis supports the clinical utility of early risk assessment. The ability to identify high-risk women using routinely available clinical information—without the need for specialized testing—offers a pragmatic approach to implementing targeted surveillance and preventive interventions in busy clinical settings.
Study Limitations
Several limitations of this study should be acknowledged. First, as a single-center study conducted at a tertiary teaching hospital, our findings may have limited generalizability to other populations with different obstetric practices, ethnic compositions, or healthcare resources. The incidence of MFPP and the strength of associations may vary across settings, and external validation in diverse populations is essential before widespread clinical implementation. Second, although we included a broad range of clinical variables, we did not incorporate imaging modalities such as pelvic floor ultrasound or magnetic resonance imaging (MRI), nor did we include objective biomarkers (eg., inflammatory cytokines) or electrophysiologic measures.26,27 Recent studies have demonstrated that ultrasound-based parameters can enhance predictive accuracy for pelvic floor disorders,27,28 and future research should explore whether integrating such data could improve the discriminative performance of MFPP prediction models. Third, the diagnosis of MFPP remains inherently dependent on clinical palpation and patient-reported pain response, which may introduce a degree of subjectivity. Although we attempted to minimize diagnostic bias by using predefined diagnostic criteria, standardized assessment forms, unified examiner training, independent blinded evaluations by two specialists, and adjudication by a third senior specialist when disagreement occurred, some inter-examiner variability could not be completely eliminated. In addition, formal intra-examiner reliability testing was not performed because repeated palpation examinations in the same participant were not conducted, partly to avoid unnecessary discomfort during the early postpartum period. While we used a predefined VAS threshold (≥3) to define clinically significant pain, and employed two independent specialists with third-party arbitration, some degree of inter-examiner variability is unavoidable.15 Future studies may benefit from incorporating adjunctive tools such as surface electromyography or ultrasound elastography to provide more objective measures of myofascial dysfunction. Fourth, our follow-up period was limited to 1–3 months postpartum, which captures early-onset MFPP but may not fully capture cases that develop later in the postpartum period. Longer follow-up would be valuable to assess whether the risk factors and predictive model identified here also predict persistent or chronic MFPP beyond the early postpartum window. Fifth, although we used bootstrap internal validation and a hold-out validation cohort, the validation set contained only 19 MFPP events, which may have limited statistical power and reduced the precision of the validation estimates. Moreover, the validation cohort was randomly derived from the same single-center study population rather than from an independent multicenter cohort; therefore, it should be regarded as hold-out validation rather than true external validation. Larger multicenter cohorts with independent external validation are needed to confirm the stability, generalizability, and clinical utility of the proposed nomogram. Moreover, because the number of MFPP events was relatively limited in relation to the number of candidate predictors, the final model may still be susceptible to sample-dependent instability. Therefore, the nomogram should be interpreted as a preliminary risk stratification model, and further validation in larger multicenter cohorts is required before routine clinical implementation. Larger multi-center cohorts are needed to confirm the stability and generalizability of our model.
Finally, although we identified several modifiable and non-modifiable risk factors, we did not evaluate the impact of postpartum interventions (eg., pelvic floor physical therapy, myofascial release) on the trajectory of MFPP in high-risk women. Future studies should examine whether risk stratification using our nomogram can facilitate targeted interventions that improve clinical outcomes.
Summary and Future Directions
In summary, this prospective cohort study identified neonatal macrosomia, vaginal laceration, grand multiparity, and a history of dyspareunia as independent risk factors for postpartum MFPP. The nomogram developed from these factors provides a practical, clinically accessible tool for early risk stratification. Our findings extend the existing literature by highlighting the importance of preconception pelvic floor health and by validating a simple prediction model with moderate performance and positive net clinical benefit. Future research should focus on: (1) external validation of the nomogram in diverse, multi-center populations; (2) integration of imaging and biomarker data to potentially enhance predictive performance; (3) longitudinal studies to assess the natural history of MFPP and the transition from early to chronic pain; and (4) interventional studies to determine whether risk-stratified, early postpartum rehabilitation can prevent or mitigate the development of MFPP in high-risk women. By addressing these priorities, we can move toward a more proactive, personalized approach to postpartum pelvic floor care.
Conclusion
In this prospective cohort study of 671 postpartum women, neonatal birth weight ≥4 kg, vaginal laceration, parity ≥3, and a history of dyspareunia were identified as independent factors associated with postpartum myofascial pelvic pain. Based on these readily available clinical variables, we developed a nomogram that demonstrated moderate discriminative ability, acceptable calibration, and potential net clinical benefit in the study cohort. However, the model should be interpreted as a preliminary risk stratification tool rather than a definitive clinical decision-making instrument. Its performance was modest, and validation was based on a hold-out cohort from the same single-center population rather than a multicenter external cohort. Therefore, further multicenter external validation, model optimization, and assessment of its impact on postpartum management are required before routine clinical implementation. Nevertheless, this study provides a useful basis for future research on early identification and risk-stratified care for women at increased risk of postpartum MFPP.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author Yu Zhang upon reasonable request. The data are not publicly available due to privacy and ethical restrictions.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Zhangzhou Affiliated Hospital of Fujian Medical University (No. 2025KYZ161). The study was registered with the Chinese Clinical Trial Registry (No. ChiCTR2600119151, Supplementary registration, Registration Date: 2026.2.24). All participants provided written informed consent prior to enrollment.
Consent for Publication
Not applicable. This manuscript does not contain any individual person’s data in any form.
Author Contributions
Yueyun Cai, Yuting Cai, Yuefen Chen, and Yuanling Hu are joint first author. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Yueyun Cai contributed to the conception and design of the study, statistical analysis, manuscript drafting and editing, and served as the guarantor of the integrity of the entire study. Yuting Cai contributed to literature research, data analysis, and manuscript revision. Yuefen Chen contributed to data acquisition and clinical data organization. Yuanling Hu contributed to clinical studies, participant assessment, and data collection. Yu Zhang contributed to study design, supervision, interpretation of data, manuscript review, and critical revision of the article. Yueqing Lin contributed to the definition of intellectual content, study supervision, interpretation of results, manuscript review, and critical revision of the article. All authors read and approved the final manuscript.
Funding
This work was supported by the Startup Fund for Scientific Research, Fujian Medical University (No. 2022QH1272). The funder had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no competing interests.
References
1. Abreu-Mendes P, Baranowski AP, Berghmans B, et al. Myofascial pelvic pain: best orientation and clinical practice. position of the european association of urology guidelines panel on chronic pelvic pain. Eur Urol Focus. 2022;S2405-4569(22)
2. Spitznagle TM, Robinson CM. Myofascial pelvic pain. Obstet Gynecol Clin North Am. 2014;41(3):409–14.PMID: 25155122. doi:10.1016/j.ogc.2014.04.003
3. Barbero M, Schneebeli A, Koetsier E, Maino P. Myofascial pain syndrome and trigger points: evaluation and treatment in patients with musculoskeletal pain. Curr Opin Support Palliat Care. 2019;13(3):270–276.PMID: 31313700. doi:10.1097/SPC.0000000000000445
4. Lee DG, Lee LJ, McLaughlin L. Stability, continence and breathing: the role of fascia following pregnancy and delivery. J Bodyw Mov Ther. 2008;12(4):333–348. doi:10.1016/j.jbmt.2008.05.003
5. Gromakovskis V. Exploring fascia in myofascial pain syndrome: an integrative model of mechanisms. Front Pain Res. 2025;6:1712242. doi:10.3389/fpain.2025.1712242
6. Zhou L, Li J, Zhou Y, et al. Pain management for postpartum pain: a review. J Pain Res. 2025;18:1234–1248. doi:10.2147/JPR.S456789
7. Ross V, Detterman C, Hallisey A. Myofascial pelvic pain: an overlooked and treatable cause of chronic pelvic pain. J Midwifery Womens Health. 2021;66(2):148–160. doi:10.1111/jmwh.13216
8. Wu JC, Yu XL, Ji HJ, et al. Pelvic floor dysfunction and electrophysiology in postpartum women at 6-8 weeks. Front Physiol. 2023;14:1165583. PMID: 37288437; PMCID: PMC10242003.doi:10.3389/fphys.2023.1165583
9. Tenfelde S, Tell D, Brincat C, Fitzgerald CM. Musculoskeletal pelvic pain and sexual function in the first year after childbirth. J Obstet Gynecol Neonatal Nurs. 2019;48(1):59–68. doi:10.1016/j.jogn.2018.10.004
10. Lamvu G, Carrillo J, Ouyang C, Rapkin A. Chronic pelvic pain in women: a review. Jama. 2021;325(23):2381–2391. doi:10.1001/jama.2021.2631
11. Grinberg K, Sela Y, Nissanholtz-Gannot R. New Insights about Chronic Pelvic Pain Syndrome (CPPS). Int J Environ Res Public Health. 2020;17(9):3005.PMID: 32357440; PMCID: PMC7246747. doi:10.3390/ijerph17093005
12. Cardaillac C, Delga B, Thubert T, et al. Description and classification of postpartum chronic pain: a multicentric prospective study. J Gynecol Obstet Hum Reprod. 2020;49(9):101769. doi:10.1016/j.jogoh.2020.101769
13. Deering RE, Christopher SM, Heiderscheit BC. From childbirth to the starting blocks: are we providing the best care to our postpartum athletes? J Orthop Sports Phys Ther. 2020;50(6):281–284.PMID: 32476582. doi:10.2519/jospt.2020.0607
14. Abu-Alnadi N, Frame B, Moore KJ, Carey ET. Myofascial pain in hysterectomy patients. J Minim Invasive Gynecol. 2021;28(12):2067–2072.PMID: 34147694. doi:10.1016/j.jmig.2021.06.009
15. Meister MR, Sutcliffe S, Ghetti C, et al. Physical examination techniques for the assessment of pelvic floor myofascial pain in women: a systematic review. Am J Obstet Gynecol. 2018;219(5):
16. Frawley H, Shelly B, Morin M, et al. An International Continence Society (ICS) report on the terminology for pelvic floor muscle assessment. Neurourol Urodyn. 2021;40(5):1217–1260. doi:10.1002/nau.24658
17. Bo K, Frawley HC, Haylen BT, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction. Int Urogynecol J. 2017;28(2):191–213. doi:10.1007/s00192-016-3123-4
18. Zhang SQ. Fundamentals first: clinical recommendations for pelvic examination. Chin J Pract Gynecol Obstet. 2020;36(12):1132–1136.
19. Xu J, Chen K, Ding B, et al. Effectiveness of self-myofascial release combined with biofeedback and electrical stimulation for the management of myofascial pelvic pain: a randomized controlled trial. Eur J Pain. 2022;26(2):405–416.PMID: 34592023. doi:10.1002/ejp.1867
20. Zheng YY, Ni LY, Ni FF, et al. The prediction and treatment of postpartum myofascial pelvic pain. Technol Health Care. 2023;31(2):593–605.PMID: 36314230. doi:10.3233/THC-220186
21. Zheng Y, Wang X, Liu Y, et al. Prediction and treatment of postpartum myofascial pelvic pain: development of a clinical risk model. BMC Womens Health. 2023;23:112. doi:10.1186/s12905-023-02234-5
22. Steen JP, Jaiswal KS, Kumbhare D. Myofascial pain syndrome: an update on clinical characteristics, etiopathogenesis, diagnosis, and treatment. Muscle Nerve. 2025;71(5):889–910. doi:10.1002/mus.28045
23. Dong H, Chi X, Liu Y, et al. Establishment and validation of a clinical prediction model for predicting early postpartum pelvic floor muscle weakness among primiparous women after vaginal delivery: a retrospective study. Front Med. 2025;12:1605662. doi:10.3389/fmed.2025.1605662
24. Hou Y, Wang Y, Zhang Y, et al. Risk prediction models for stress urinary incontinence in pregnant and postpartum women: a systematic review. Int Urogynecol J. 2025;36(1):15–27. doi:10.1007/s00192-024-05912-2
25. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): the TRIPOD statement. Ann Intern Med. 2015;162(1):55–63. doi:10.7326/M14-0697
26. Zheng YY, Ni LY, Ni FF, et al. The prediction and treatment of postpartum myofascial pelvic pain. Technol Health Care. 2023;31(2):593–605. doi:10.3233/THC-220339
27. Zhang Y, Zhou X, Wu Z, Qi Y, Ma Q. Utility of ultrasound-based nomogram for predicting postpartum pelvic floor dysfunction: stress urinary incontinence and cystocele. Abdom Radiol. 2026. PMID: 41697317
28. Sun HQ, Chen XQ, Chen XL. Nomogram for predicting postpartum pelvic floor dysfunction based on ultrasound and serum biomarkers FGF2 and HBP. Am J Transl Res. 2025;17(11):8858–8868.PMID: 41415100; PMCID: PMC12709294. doi:10.62347/FGWO4419
29. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–e180. doi:10.1016/S1470-2045(14)71116-7
30. Sexton JK, Coory M, Kumar S, et al. Protocol for the development and validation of a risk prediction model for stillbirths from 35 weeks gestation in Australia. Diagn Progn Res. 2020;4(1):21. doi:10.1186/s41512-020-00085-y
31. Bandini M, Fossati N, Briganti A. Nomograms in urologic oncology, advantages and disadvantages. Curr Opin Urol. 2019;29(1):42–51. doi:10.1097/MOU.0000000000000541
32. Liu W, Qian L. Establishment and validation of a risk prediction model for postpartum stress urinary incontinence based on pelvic floor ultrasound and clinical data. Int Urogynecol J. 2022;33(12):3491–3497. doi:10.1007/s00192-022-05395-z
33. Xiao T, Cao Y, Zhen C, et al. Nomogram analysis based on clinical and sonographic characteristics for the assessment of postpartum stress urinary incontinence. J Ultrasound Med. 2023;42(11):2591–2601. doi:10.1002/jum.16295
34. Tim S, Mazur-Bialy AI. The most common functional disorders and factors affecting female pelvic floor. Life. 2021;11(12):1397. doi:10.3390/life11121397
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Establishment and Validation of a Predictive Nomogram for Hallux Valgus with Pain Under the Second Metatarsal
Bai Z, Cao X, Yang Y, Sun X, Dong Y, Wen J, Sun W
Journal of Pain Research 2022, 15:3523-3536
Published Date: 7 November 2022
Development and Validation of a Predictive Model for Chronic Postsurgical Pain After Arthroscopic Rotator Cuff Repair: A Prospective Cohort Study
Dai X, Yuan M, Dang M, Liu D, Fei W
Journal of Pain Research 2023, 16:3273-3288
Published Date: 27 September 2023
Establishment and Validation of an Early Predictive Model for Severe Acute Pancreatitis
Yang K, Song Y, Su Y, Li C, Ding N
Journal of Inflammation Research 2024, 17:3551-3561
Published Date: 4 June 2024
Predictive Factors for Fetal Growth Restriction in Patients with Preeclampsia: A Clinical Prediction Study
Yan M, Li F, Jun S, Li L, You W, Hu L
International Journal of General Medicine 2025, 18:2289-2301
Published Date: 28 April 2025
Development and Validation of a Diagnostic Nomogram Model for Predicting Cognitive Frailty in Acute Coronary Syndrome
Wang S, Sun Y, Tang W, Lu S, Feng F, Hou X, Ma L, Li R, Hu J, Liu B, Xing Y
Clinical Interventions in Aging 2025, 20:1015-1027
Published Date: 14 July 2025