Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Respiratory Muscle Strength and Mortality in Patients with COPD: A Systematic Review and Meta-Analysis
Authors Mizusawa H ![]() , Okura K, Shiraishi M
, Okura K, Shiraishi M ![]() , Noguchi M, Higashimoto Y
, Noguchi M, Higashimoto Y
Received 27 June 2025
Accepted for publication 16 December 2025
Published 31 December 2025 Volume 2025:20 Pages 4205—4216
DOI https://doi.org/10.2147/COPD.S550066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Hiroki Mizusawa,1 Kazuki Okura,2 Masashi Shiraishi,1 Masaya Noguchi,1 Yuji Higashimoto3
1Department of Rehabilitation, Kindai University Hospital, Minami-ku Sakai, Osaka Prefecture, Japan; 2Department of Rehabilitation, Akita University Hospital, Akita City, Akita Prefecture, Japan; 3Department of Rehabilitation Medicine, Kindai University, Minami-ku Sakai, Osaka Prefecture, Japan
Correspondence: Hiroki Mizusawa, Faculty of Medicine, Department of Rehabilitation Medicine, Kindai University, 1-14-1 Mihara-dai, Minami-ku, Sakai, Osaka, 590-0197, Japan, Tel +81-72-288-7222, Fax +81-72-298-1500, Email [email protected]
Purpose: Respiratory muscle weakness is common in chronic obstructive pulmonary disease (COPD), potentially carrying prognostic information beyond airflow limitation; however, clinical testing remains variably standardized, and its independent association with survival is uncertain. We evaluated whether respiratory muscle strength is associated with survival in patients with COPD, and summarized implementation-relevant evidence for other indices.
Methods: We systematically searched PubMed/MEDLINE, CENTRAL, and Web of Science from January 1, 1990 to September 30, 2025, screened observational cohorts and baseline-prognosis analyses in patients with COPD, appraised risk of bias, and meta-analyzed time-to-event estimates using random-effects where ≥ 2 comparable studies were available. Eligible studies enrolled patients with COPD with observational cohorts or baseline-prognosis analyses reporting all-cause mortality as outcome.
Results: Of the six eligible studies, two permitted pooling for inspiratory strength versus all-cause mortality. Lower inspiratory strength was associated with higher mortality (pooled hazard ratio 0.97, 95% confidence interval 0.95– 0.99; I2=58%). In severity-restricted cohorts, frequently reported cut-offs were maximal inspiratory strength (MIP) ≤ 55 cmH2O and maximal expiratory strength (MEP) ≤ 80 cmH2O; all-cause mortality in these groups was approximately 46.6– 54.4% at 42– 60 months. However, in broader-severity samples, 2-year and 12– 45-month mortality rates were 9.4– 14.7% and 8.4– 33.6%, respectively. Peak inspiratory flow rate (PIFR) < 60 L/min repeatedly aligned with exacerbations and 90-day readmission. Conversely, the prognostic signal for MEP was directionally inconsistent, and sniff nasal inspiratory pressure associations frequently attenuated after adjustment.
Conclusion: MIP shows a consistent directional association with survival in patients with COPD, although magnitude estimates vary with measurement protocols and confounder control. We propose a minimum reporting set (posture, starting lung volume, trials/repeatability, device/calibration, cmH2O units, and prespecified confounders) and immediate clinical actions: standardized MIP during stable visits for risk stratification and PIFR screening to guide inhaler selection.
Keywords: chronic obstructive pulmonary disease, respiratory muscle strength, maximal inspiratory pressure, prognosis, mortality, peak inspiratory flow rate
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality globally, ranking among the top three causes of death.1 In addition to airflow limitation, patients experience progressive functional impairment, reduced quality of life, and high healthcare utilization.1 Exercise-induced dyspnea and exercise intolerance partially reflect respiratory muscle dysfunction.2 The diaphragm, which is the primary inspiratory muscle responsible for approximately 60–80% of inspiratory work,3 exhibits reduced exercise capacity and muscle strength in COPD and is closely associated with dynamic hyperinflation.4 Therefore, respiratory muscle function possesses clear validity as a clinically meaningful concept that influences symptoms and activities of daily living.
Measuring respiratory muscle strength is one of the methods for evaluating respiratory muscle function. Standardized guidelines for respiratory muscle assessment have evolved (American Thoracic Society (ATS)/European Respiratory Society (ERS) statements in 2002 and updated in 2019),5,6 and clinical research has accumulated over more than 20 years. A recent retrospective cohort study (n=79; predominantly severe–very severe COPD) followed for 42 months identified maximum inspiratory pressure: maximal inspiratory strength (MIP) ≤55 cmH2O and maximal expiratory strength (MEP) ≤80 cmH2O as mortality risk cut-offs, with significant separation of Kaplan–Meier curves and confirmation in multivariable Cox models.7 Notably, adding MIP/MEP to forced expiratory volume in 1 second (FEV1), peak oxygen consumption (V˙O2peak), and 6-minute walking distance (6MWD) improved mortality risk discrimination, underscoring the complementary prognostic value of respiratory muscle strength beyond spirometry and exercise indices. Nevertheless, it remains uncertain whether respiratory muscle strength independently predicts survival more broadly. Despite detailed ATS/ERS recommendations on how to perform respiratory muscle testing, clinically standardized, reproducible protocols have not been established in practice or consistently implemented in research. Key aspects, including patient selection, timing (stable state vs post-exacerbation), maneuver quality control, and unit handling, remain variable across studies. Moreover, actionable prognostic thresholds have not been validated or adopted, and confounder adjustment is inconsistent, leaving the independent prognostic role of respiratory muscle strength uncertain.
Accordingly, we conducted a systematic review and meta-analysis in patients with COPD to quantify the association between baseline respiratory muscle strength and all-cause mortality, using narrative synthesis for indices or outcomes lacking compatible data. We also critically examined sources of inconsistency and outlined standards to support clinical implementation. We aimed to: (1) summarize current measurement methods and key sources of variability for respiratory muscle strength testing; (2) assess and quantify prognostic evidence, focusing on all-cause mortality in patients with COPD, while explaining observed heterogeneity; and (3) derive practical standards and research priorities to enable clinical implementation.
Methods
Protocol and Reporting
The systematic review and meta-analysis were reported and conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement.8 We prespecified eligibility, search strategy, and extraction/analysis procedures according to PRISMA 2020 guidelines (Figure 1).
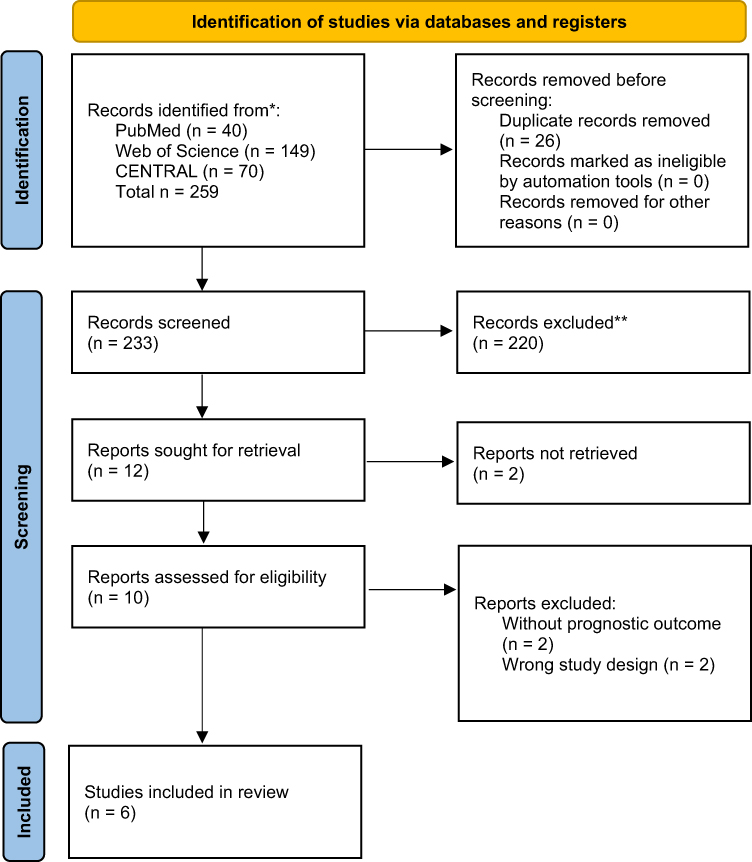 |
Figure 1 PRISMA 2020 study selection flow. Flow diagram of record identification, screening, eligibility assessment, and inclusion, prepared in accordance with PRISMA 2020. The numbers in each box indicate the records identified and excluded and the studies included in the qualitative and quantitative syntheses. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and automation tools. Abbreviations: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. |
Eligibility Criteria
We included studies involving adults with COPD. Index tests included respiratory muscle strength/flow measures (MIP, MEP, PImax/PEmax, sniff nasal inspiratory pressure (SNIP), peak inspiratory flow rate (PIFR), peak expiratory flow rate (PEFR), and cough peak flow (CPF)); diaphragm ultrasound was excluded as an index but considered in the background. The outcome was all-cause mortality, and eligible designs included observational cohort studies. We included baseline-prognosis analyses of trials (published from January 1, 1990 to September 30, 2025 in English/Japanese). Full operational criteria and edge-case rules are detailed in Supplementary Methods. We excluded letters, editorials, congress abstracts, case reports, reviews, cross-sectional studies, and animal studies.
Information Sources and Search Strategy
Two reviewers conducted an online search in parallel and independently. PubMed/MEDLINE, CENTRAL, and Web of Science were searched from January 1, 1990 to September 30, 2025 using controlled vocabulary and free-text terms (“Chronic Obstructive Pulmonary Disease” OR COPD OR “chronic obstructive pulmonary disease” OR emphysema) AND ((“maximal inspiratory pressure” OR MIP OR “maximal expiratory pressure” OR MEP OR “Sniff Nasal Inspiratory Pressure” OR SNIP OR “Peak Inspiratory Flow Rate” OR PIFR OR “Peak Expiratory Flow Rate” OR PEFR OR “Cough Peak Flow” OR CPF) AND (mortality OR survival OR prognosis OR “end of life” OR “overall mortality” OR “hazard ratio” OR “12 month” OR “1 year” OR “long-term” OR “long term”), with no device-brand filter. Complete strategies are presented in Supplementary Table S1.
Study Selection
Two reviewers conducted the study selection in parallel and independently. A third, more experienced reviewer resolved any conflicts concerning the inclusion of a study after a group discussion where the perspectives of both initial reviewers were considered. The study selection was conducted in stages: initially based on title evaluation, then abstract, and later by full-text analysis, following the predefined eligibility criteria.
Data Extraction
We used a standardized form to capture study design, setting/country, sample size, population characteristics (age, male, and % pred. FEV1), index definition (unit, posture, trials, and repeatability), outcomes and follow-up, effect estimates (hazard ratio (HR)/odds ratio (OR)/risk ratio (RR) with 95% confidence interval (95% CI), adjustment covariates, and risk-of-bias items, as summarized in Table 1.
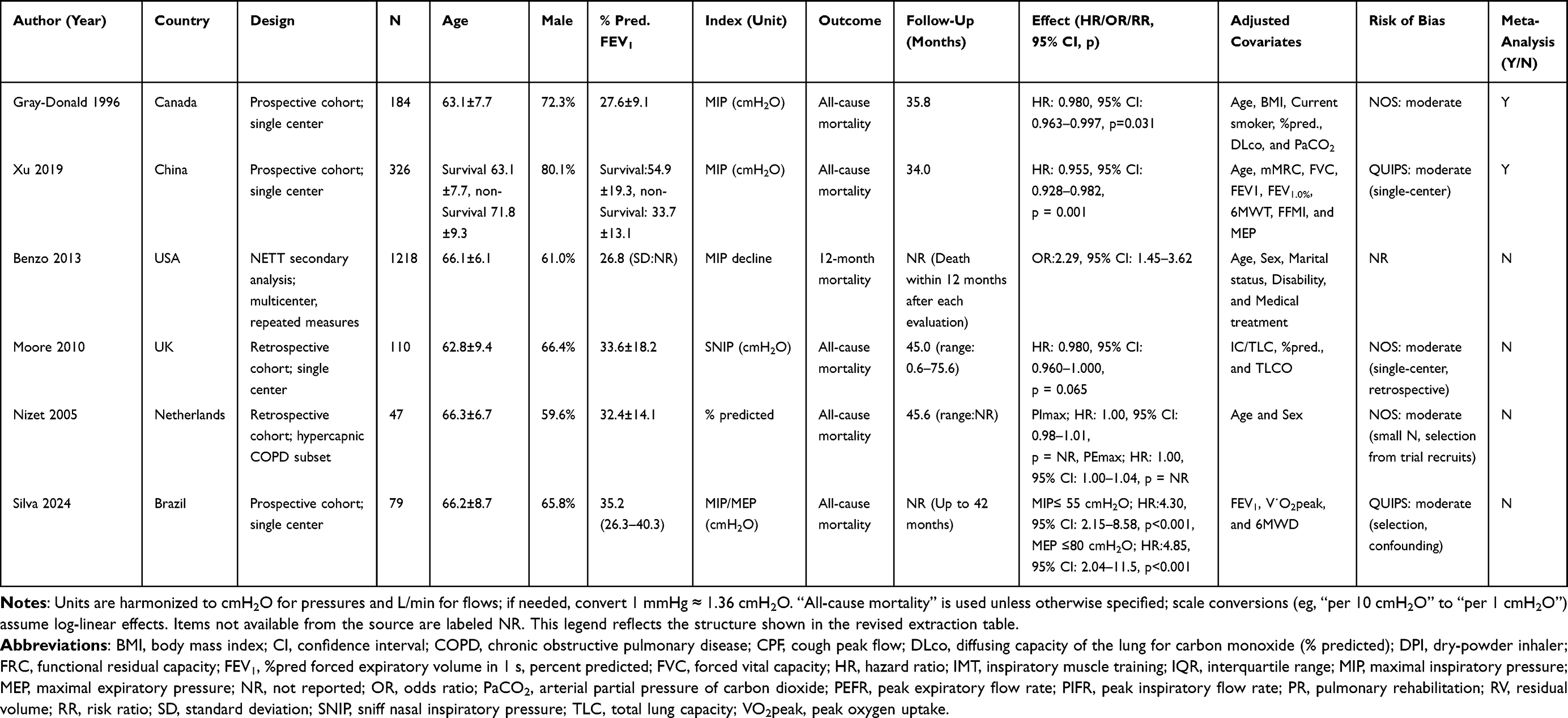 |
Table 1 Study Characteristics and Effect Estimates |
Statistical Analysis and Data Synthesis
All statistical analyses were performed using EZR v.1.41 (Saitama Medical Center, Jichi Medical University, Saitama, Japan). When two or more studies reported comparable time-to-event estimates for the same index–outcome pair, we pooled HRs using an inverse-variance random-effects model. Between-study heterogeneity was quantified using I2, τ2, and the Cochran Q test (p-value). All estimates are presented with 95% CI, and results are displayed using forest plots. Where required, effect measures were harmonized to a common metric before synthesis, and units for respiratory pressure indices were standardized to cmH2O.
Risk of Bias (RoB) Assessment
Cohort studies were assessed using the Newcastle–Ottawa Scale, while prognostic studies were further evaluated with the Quality In Prognosis Studies domains. For randomized controlled trials involving baseline-prognosis analyses, RoB-2 was used for selection/measurement domains. A summary of RoB is presented alongside effect estimates in Table 1.
Synthesis
When two or more studies reported comparable effect metrics for the same index–outcome pair, we conducted random-effects meta-analysis, reporting the pooled effect with 95% CI, between-study heterogeneity (I2, τ2). Otherwise, results were narratively synthesized based on the index (MIP/MEP/SNIP/PIFR/PEFR) and mortality outcome. PRISMA flow diagram and forest plots are provided. Studies that could not be meta-analyzed because of incompatible outcomes, effect metrics, or insufficient data were synthesized narratively.
Results
Study Selection and Characteristics
As detailed in the selection flow diagram (Figure 1), the initial search yielded 259 results. After removing duplicate records and ineligible studies, 12 remained and were subjected to full-text review. Of these, six were included. The studies included outpatient COPD cohorts with variable severity and follow-up (12–60 months), predominantly reporting all-cause mortality. Extracted variables and adjustment sets are summarized in Table 1.
Quantitative Synthesis (Mortality)
Two cohorts reported comparable effect metrics for inspiratory strength and all-cause mortality, permitting quantitative pooling. The random-effects model indicated that lower inspiratory strength was associated with higher mortality (pooled HR 0.97 [95% CI 0.95–0.99]), with moderate heterogeneity (I2 58%, τ2 = 0.0002, p = 0.12), consistent with between-study differences (Figure 2).
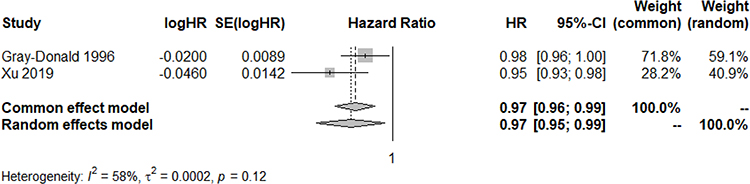 |
Figure 2 Association between inspiratory muscle strength and all-cause mortality in COPD: forest plot. Forest plot displaying study-specific hazard ratios (HR) with 95% confidence intervals (CI) for the association between inspiratory muscle strength and all-cause mortality. Square markers are proportional to inverse-variance weights; diamonds denote pooled estimates. The vertical solid line indicates the line of no effect (HR=1). The random-effects model yielded a pooled HR of 0.97 (95% CI, 0.95–0.99), with heterogeneity I2=58%, τ2=0.0002, and Cochran’s Q p=0.12. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; MIP, maximal inspiratory pressure. |
Other Indices/Outcomes (Narrative)
Several studies were not eligible for quantitative pooling and are therefore summarized narratively in Table 1; their findings informed the qualitative interpretation but were not part of the sensitivity analyses. For MEP, results were directionally inconsistent across studies, with a prognostic signal weaker than that of MIP. SNIP showed univariate associations, which were often attenuated after adjustment. For PIFR, values <60 L/min were repeatedly associated with exacerbations and near-term readmission in stable/discharge cohorts (implementation relevance for inhaler choice). For PEFR, lower values aligned with worse inpatient or exacerbation outcomes in selected settings. A literature search identified no studies evaluating CPF as a prognostic marker in COPD. To aid interpretation and implementation, a concise, index-by-outcome summary of pros and cons is provided in Table 2. Furthermore, this table collates key measurement features (posture, trials, and repeatability), typical clinical use-cases, and the principal strengths/limitations of each index alongside a qualitative appraisal of evidence consistency.
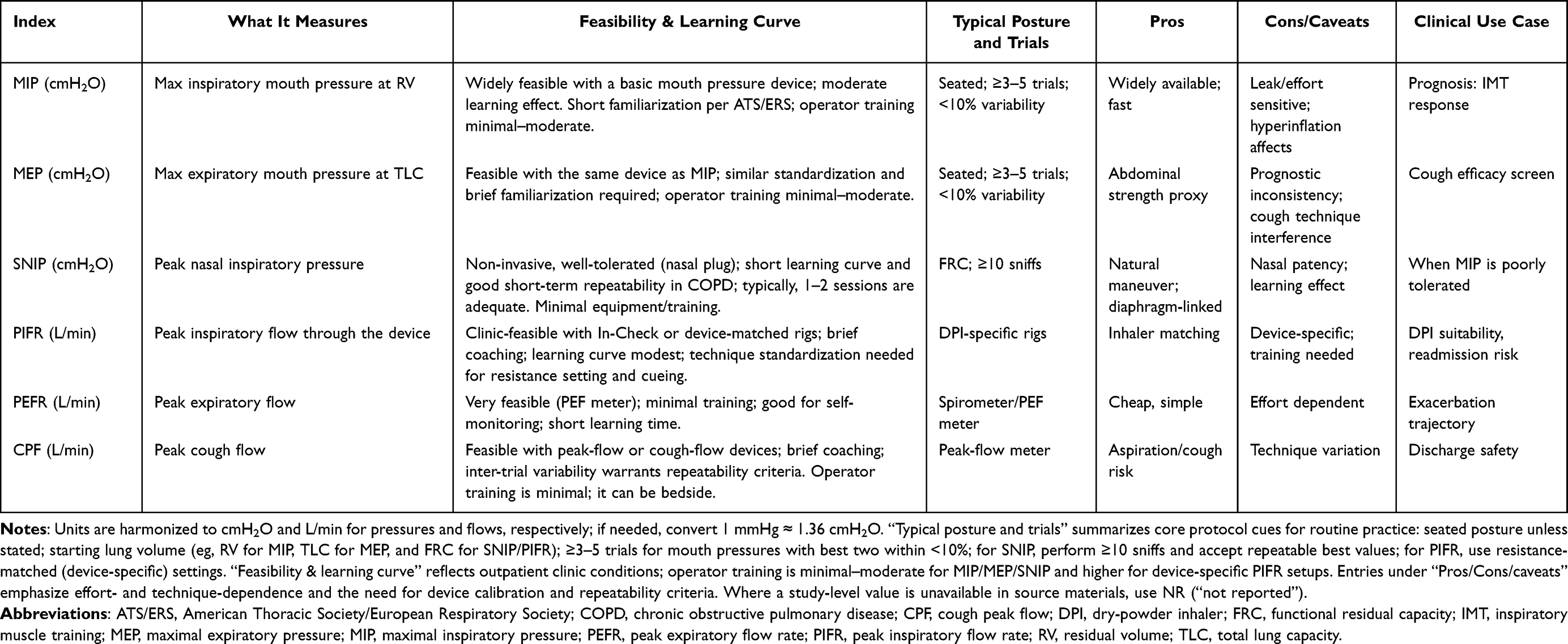 |
Table 2 Respiratory Muscle and Flow Indices (“Index at a Glance”): What Each Measures, Feasibility/Learning Curve, Protocol Cues, and Clinical Use Cases |
RoB
Overall, RoB was predominantly moderate, primarily due to confounding and measurement variability. Many studies lacked simultaneous adjustment for key covariates or relied on univariable models without a prespecified selection strategy, limiting internal validity. Protocols for MIP/SNIP/MEP/PIFR/CPF varied in posture, trial number, repeatability criteria, and units (mmHg vs cmH2O); device details and PIFR device context were frequently unclear, likely increasing heterogeneity. Domain-level judgments are summarized in Table 1. For data synthesis, we harmonized units to cmH2O and prioritized adjusted estimates.
Sensitivity and Small-Study Considerations
Qualitative sensitivities yielded consistent conclusions. Restricting adjusted HR to cohorts with clear measurement protocols (posture and repeatability) did not alter the direction of the observed effects. Given the small number of pooled studies, we did not perform small-study bias tests or funnel-plot assessments, which are unreliable with <10 studies.
Discussion
In this systematic review with meta-analysis, lower inspiratory muscle strength, which is primarily MIP, was consistently associated with higher mortality independent of airflow limitation. The pooled estimate favored a protective effect of greater inspiratory strength, although moderate heterogeneity was observed. Lower MIP was associated with higher all-cause mortality in patients with COPD in our quantitative synthesis; the direction of effect was consistent, although heterogeneity in measurement and adjustment warrants caution in magnitude interpretation. These findings refine prior single-center signals and align with contemporary task-force guidance,6 emphasizing standardized respiratory muscle testing and interpretation. However, only a few studies reported MEP or other respiratory muscle strength indicators as outcomes, making a statistical approach impossible. Through a narrative review, we could present the usefulness of these other indicators as currently reported prognostic predictors for patients with COPD. Finally, Figure 3 presents a conceptual causal framework integrating inspiratory muscle weakness, mediators, clinical outcomes, and potential interventions. In subsequent paragraphs, each pathway is described narratively to contextualize the meta-analysis findings.
 |
Figure 3 Conceptual framework linking inspiratory muscle weakness to clinical outcomes and modifiable interventions. Schematic overview of proposed pathways from inspiratory muscle weakness (MIP ↓) to downstream consequences—including impaired cough mechanics (CPF ↓/MEP ↓), dynamic hyperinflation and ventilatory limitation (IC ↓), reduced exercise tolerance (VO2peak ↓), and heightened risk of exacerbation and mortality—mediated by skeletal-muscle dysfunction, nutritional status, and baseline pulmonary function. Potential intervention nodes include device matching using peak inspiratory flow and pulmonary rehabilitation augmented with inspiratory muscle training. Abbreviations: CPF, cough peak flow; IC, inspiratory capacity; IMT, inspiratory muscle training; MEP, maximal expiratory pressure; MIP, maximal inspiratory pressure; PIFR, peak inspiratory flow rate; PR, pulmonary rehabilitation; VO2peak, peak oxygen uptake. |
Respiratory muscle strength in COPD is typically quantified by MIP, reflecting the coordinated force generation of the diaphragm, intercostal and scalene muscles, and accessory muscles—the sternocleidomastoid and parietal muscles—during maximal inspiration.9 MEP captures expiratory muscle performance driven by the abdominal wall and internal intercostals.6,10 Beyond loss of mass or geometry, qualitative abnormalities—reduced force generation and decreased myosin heavy chain content per sarcomere—are evident in diaphragmatic fibers, which is the primary inspiratory muscle,11 aligning with the “respiratory muscle dysfunction” node in Figure 3. This dysfunction, influenced by clinical confounders and sarcopenia, plausibly contributes to lower inspiratory muscle strength, which subsequently leads to hyperinflation, cough/clearance inefficiency, and the respiratory muscle metaboreflex.
In relation to acute exacerbations, available data, though still limited, support a link between respiratory muscle performance and exacerbation risk. An outpatient study reported a strong association between lower respiratory muscle strength and exacerbations in COPD.12 While direct evidence for SNIP and exacerbations is lacking, several flow-based indices map onto the “exacerbations” pathway in our framework. Declines in PEFR precede both gradual- and sudden-onset events (beginning approximately 4 and 2 days prior, respectively).13 Suboptimal PIFR (<60 L/min) is associated with more frequent exacerbations and early re-exacerbations after discharge.14–17 In patients with severe COPD, lower CPF characterizes frequent exacerbators, accompanied by lower PaO2.18 These observations align with the conceptual framework, linking inspiratory weakness to impaired secretion clearance and highlighting how inhaler technique and device selection influence exacerbation risk. Drug emission from dry-powder inhalers (DPIs) is strongly flow-dependent; patients should generate sufficient PIF through the device to ensure adequate de-aggregation and dispersion.19,20 Measuring PIFR—for example, with an In-Check device matched to the target DPI’s internal resistance—helps determine device suitability.19,21 As noted above, a pragmatic threshold of approximately 60 L/min is widely cited; values below this are linked to suboptimal aerosolization and have been proposed as a predictive therapeutic biomarker to guide device selection.19–22 In practice, when PIFR is inadequate for a DPI, clinicians should consider less flow-dependent options (eg, pMDI + spacer, soft-mist inhaler, or nebulizer) and reinforce technique; contemporary guidance recommends reassessing inhaler technique and device suitability at each visit and after clinical changes.1,23
Pulmonary rehabilitation is situated within the diagram as an intervention acting primarily on inspiratory strength and ventilatory mechanics. Across studies, respiratory muscle strength is a central rehabilitation outcome, with responders displaying higher baseline MIP and greater diaphragmatic excursion than non-responders.24,25 Meta-analyses have indicated that rehabilitation improves both MIP and MEP, even when limited to aerobic training,26 and the minimal clinically important difference in MIP has been estimated at 17.2 cmH2O.27 Adding inspiratory muscle training (IMT) to standard programs augments gains in MIP and diaphragm excursion,28,29 consistent with an effect pathway that strengthens inspiratory capacity and mitigates hyperinflation, thereby improving symptoms and functional performance. Trial data in lung-transplant candidates further underscore this pattern: pulmonary rehabilitation plus IMT yielded larger improvements in 6MWD and MIP than rehabilitation alone, with dyspnea improvement in both arms,30 consistent with the intervention nodes depicted in Figure 3.
Sarcopenia is integrated into the framework as an upstream determinant of respiratory muscle dysfunction and strength. Age-related and disease-specific myocellular changes—including selective type II fiber loss, myosteatosis, and reduced type II satellite cells—are prominent.9,31,32 Diaphragmatic and global respiratory muscle forces decline with aging and sarcopenia, with transdiaphragmatic pressure reduced in older adults and individuals with sarcopenia experiencing approximately 30% overall respiratory muscle strength.33–35 Beyond age-related changes, COPD involves disease-specific fiber remodeling. In peripheral limb muscles, multiple biopsy studies have demonstrated a shift from oxidative type I fibers toward more glycolytic type II/IIx fibers, accompanied by reduced oxidative capacity and greater fatigability.36–38 In contrast, the diaphragm shows endurance-like adaptation with an increased proportion of type I fibers and reduced type II content in severe COPD, although single-fiber studies also reveal intrinsic contractile impairments.11,39,40 This divergence between limb and diaphragm helps explain why global respiratory muscle strength may decline even as diaphragmatic fatigue resistance increases, and it supports targeted interventions (eg, peripheral muscle reconditioning and IMT) tailored to distinct phenotypes.41
Emerging consensus defines respiratory sarcopenia as the coexistence of reduced respiratory muscle strength and low respiratory muscle mass, with ultrasound and computed tomography recommended for assessing respiratory muscle morphology (diaphragm thickness, thickening fraction, and excursion);9 however, cut-off values for low respiratory muscle mass remain insufficiently standardized.42–44 In parallel, diaphragm ultrasound shows practical utilities. Its structural/functional measures are reproducible and help predict extubating/reintubation risk in critical illness, highlighting prognostic relevance.42,45,46 Importantly, lower inspiratory muscle strength has been associated with increased COPD exacerbations, while low respiratory muscle area is linked to adverse outcomes, including mortality.12,44–47 Beyond device matching, routine nutritional assessment is clinically pertinent because low nutritional status is associated with higher mortality in COPD.48,49 Targeted nutritional supplementation can improve body weight, skeletal muscle mass, 6MWD, and health-related quality of life, and in malnourished patients with COPD, it may also enhance inspiratory/expiratory muscle strength.50–52 When combined with exercise/pulmonary rehabilitation, nutrition support has further improved quadriceps strength and MIP. This pattern suggests a pragmatic, multimodal approach to mitigate respiratory and whole-body sarcopenia and potentially downstream readmission risk.50,53–55 Contemporary guidance further recommends providing nutritional support in malnourished patients with COPD and reassessing their needs over time.23
Exercise tolerance sits at the nexus of ventilatory limitation and muscle reflex biology in COPD. MIP correlates strongly with 6MWD,56,57 and diaphragmatic function at baseline relates to gains in 6MWD,25 echoing the path from inspiratory weakness to hyperinflation to functional capacity. The respiratory muscle metaboreflex provides a mechanistic bridge: fatigue of the respiratory muscles can trigger sympathetically mediated vasoconstriction that diverts blood flow from locomotor muscles,58 a connection depicted from inspiratory weakness and dysfunction to the metaboreflex and then to reduced exercise tolerance. Quantitative assessments reinforce this chain: diaphragmatic excursion correlates with VO2peak and with changes in inspiratory capacity during exercise.4 Furthermore, higher diaphragmatic domes on radiographs indicate less dynamic hyperinflation and greater VO2 peak.59 Accessory respiratory muscles contribute meaningfully; increased sternocleidomastoid muscle thickness and its inspiratory change correlate with exercise tolerance.60 Respiratory muscle training studies align with these pathways: home-based expiratory muscle training improved endurance time in patients with COPD,61 and IMT within rehabilitation enhances inspiratory pressures and diaphragm excursion,29 indicating modifiable links at the intervention nodes.
Finally, notwithstanding the consistent directional signal, these prognostic findings warrant cautious interpretation due to potential confounding, reverse causation, and measurement error. As summarized in Table 1, only a subset of cohorts reported multivariable models, and the covariate sets were frequently incomplete. Key factors, including body mass index/sarcopenia, smoking exposure, % predicted FEV1 or severity strata, prior exacerbations or hospitalizations, cardiovascular comorbidity, and treatment intensity (pharmacotherapy and PR/IMT exposure), were seldom adjusted simultaneously; several reports provided univariable estimates only. Such incomplete control enables residual and unmeasured confounding to inflate or attenuate observed associations. Reverse causation is also plausible: low MIP may mark pre-terminal decline or advanced disease burden, rather than exerting a direct causal effect on survival. Additionally, non-uniform measurement protocols (posture, starting lung volume, number of trials, and repeatability thresholds), device and unit inconsistencies, and variable reporting of quality control likely introduced non-differential error. This may have biased estimates toward the null and contributed to the between-study heterogeneity evident in Figure 2. Finally, single-center sampling and incompletely characterized follow-up in several cohorts raise concerns about selection and attrition bias. To mitigate these issues in our synthesis, we prioritized adjusted estimates where available, harmonized units to cmH2O, and summarized non-pooled studies narratively with domain-level risk-of-bias judgments reported alongside effect estimates.
Conclusion
Baseline inspiratory muscle strength, as measured by MIP, is consistently linked to all-cause mortality in patients with COPD. Our synthesis quantifies this association and explains heterogeneity due to protocol variability and residual confounding. For other indices, we clarify why signals diverge: weaker/inconsistent MEP, attenuation for SNIP, and the implementation relevance of PIFR. In practice, clinicians should measure and report MIP with a minimum reporting set, use PIFR (~60 L/min for DPIs) to match inhalers, and pair nutrition/protein support with pulmonary rehabilitation. Key priorities for enhancing clinical practice include standardizing test protocols and thresholds, establishing well-adjusted multicenter cohorts, and conducting pragmatic trials focused on MIP or SNIP screening, PIFR-guided device selection, and nutrition and rehabilitation bundles. Collectively, these steps aim to shift the field from description to actionable decision-support at the bedside.
Summary
Respiratory muscle strength indices are vital clinical tools in managing COPD. Their integration into daily practice can improve patient outcomes, and future multicenter studies are needed to develop standardized and reproducible methodologies for broader clinical implementation.
Data Sharing Statement
The references that support the findings of this study are available on reasonable request from the corresponding author.
Acknowledgments
This study was supported by a Grant-In-Aid for Scientific Research from the Ministry of Education, Science and Culture of the Japanese Government (no. 24K20485).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Grant-In-Aid for Scientific Research from the Ministry of Education, Science and Culture of the Japanese Government (no. 24K20485).
Disclosure
The authors have no conflicts of interest.
References
1. Agustí A, Celli BR, Criner GJ. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
2. Charususin N, Dacha S, Gosselink R, et al. Respiratory muscle function and exercise limitation in patients with chronic obstructive pulmonary disease: a review. Expert Rev Respir Med. 2018;12(1):67–79. doi:10.1080/17476348.2018.1398084
3. Mu H, Zhang Q. The application of diaphragm ultrasound in chronic obstructive pulmonary disease: a narrative review. COPD. 2024;21(1):2331202. doi:10.1080/15412555.2024.2331202
4. Shiraishi M, Higashimoto Y, Sugiya R, et al. Diaphragmatic excursion correlates with exercise capacity and dynamic hyperinflation in COPD patients. ERJ Open Res. 2020;6(4):00589–2020. doi:10.1183/23120541.00589-2020
5. American Thoracic Society/European Respiratory Society ATS/ERS. Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624. doi:10.1164/rccm.166.4.518
6. Laveneziana P, Albuquerque A, Aliverti A, et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur Respir J. 2019;53(6):01214–2018. doi:10.1183/13993003.01214-2018
7. Silva RN, Goulart CDL, de Oliveira CR, et al. Respiratory muscle strength can improve the prognostic assessment in COPD. Sci Rep. 2024;14(1):12360. doi:10.1038/s41598-024-54264-w
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
9. Sato S, Miyazaki S, Tamaki A, et al. Respiratory sarcopenia: a position paper by four professional organizations. Geriatr Gerontol Int. 2023;23(1):5–15. doi:10.1111/ggi.14519
10. Aslan SC, McKay WB, Singh G, Ovechkin AV. Respiratory muscle activation patterns during maximum airway pressure efforts are different in women and men. Respir Physiol Neurobiol. 2019;259:143–148. doi:10.1016/j.resp.2018.09.004
11. Ottenheijm CA, Heunks LM, Dekhuijzen RP. Diaphragm adaptations in patients with COPD. Respir Res. 2008;9(1):12. doi:10.1186/1465-9921-9-12
12. Furukawa Y, Miyamoto A, Asai K, et al. Respiratory muscle strength as a predictor of exacerbations in patients with chronic obstructive pulmonary disease. Respirology. 2025;30(5):408–416. doi:10.1111/resp.70003
13. Cen J, Ma H, Chen Z, Weng L, Deng Z. Monitoring peak expiratory flow could predict COPD exacerbations: a prospective observational study. Respir Med. 2019;148:43–48. doi:10.1016/j.rmed.2019.01.010
14. Mahler DA, Niu X, Deering KL, Dembek C. Prospective evaluation of exacerbations associated with suboptimal peak inspiratory flow among stable outpatients with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:559–568. doi:10.2147/COPD.S353441
15. Alqahtani JS, Aldabayan YS, Aldhahir AM, Al Rajeh AM, Mandal S, Hurst JR. Predictors of 30- and 90-day COPD exacerbation readmission: a prospective cohort study. Int J Chron Obstruct Pulmon Dis. 2021;16:2769–2781. doi:10.2147/COPD.S328030
16. Loh CH, Peters SP, Lovings TM, Ohar JA. Suboptimal inspiratory flow rates are associated with chronic obstructive pulmonary disease and all-cause readmissions. Ann Am Thorac Soc. 2017;14(8):1305–1311. doi:10.1513/AnnalsATS.201611-903OC
17. Clark B, Wells BJ, Saha AK, et al. Low peak inspiratory flow rates are common among COPD inpatients and are associated with increased healthcare resource utilization: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2022;17:1483–1494. doi:10.2147/COPD.S355772
18. El Batrawy S, Elassal G. Is there a role for cough peak flow in assessment of patients with severe COPD? Egypt J Chest Dis Tuberc. 2014;63(4):837–841. doi:10.1016/j.ejcdt.2014.06.001
19. Ohar JA, Ferguson GT, Mahler DA, et al. Measuring peak Inspiratory flow in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:79–92. doi:10.2147/COPD.S319511
20. Ohar JA, Mahler DA, Davis GN, Lombardi DA, Moran EJ, Crater GD. Clinical burden of chronic obstructive pulmonary disease in patients with suboptimal peak inspiratory flow. Can Respir J. 2024;2024:8034923. doi:10.1155/2024/8034923
21. Amirav I, Newhouse MT, Mansour Y. Measurement of peak inspiratory flow with in-check dial device to simulate low-resistance (Diskus) and high-resistance (Turbohaler) dry powder inhalers in children with asthma. Pediatr Pulmonol. 2005;39(5):447–451. doi:10.1002/ppul.20180
22. Mahler DA, Halpin DMG. Peak inspiratory flow as a predictive therapeutic biomarker in COPD. Chest. 2021;160(2):491–498. doi:10.1016/j.chest.2021.03.049
23. Agusti A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Am J Respir Crit Care Med. 2023;207(7):819–837. doi:10.1164/rccm.202301-0106PP
24. Iwakura M, Wakasa M, Okura K, et al. Functionally relevant threshold of inspiratory muscle strength in patients with chronic obstructive pulmonary disease. Respir Med. 2021;188:106625. doi:10.1016/j.rmed.2021.106625
25. Shiraishi M, Higashimoto Y, Sugiya R, et al. Diaphragmatic excursion is correlated with the improvement in exercise tolerance after pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Respir Res. 2021;22(1):271. doi:10.1186/s12931-021-01870-1
26. Lee EN, Kim MJ. Meta-analysis of the effect of a pulmonary rehabilitation program on respiratory muscle strength in patients with chronic obstructive pulmonary disease. Asian Nurs Res. 2019;13(1):1–10. doi:10.1016/j.anr.2018.11.005
27. Iwakura M, Okura K, Kubota M, et al. Estimation of minimal clinically important difference for quadriceps and inspiratory muscle strength in older outpatients with chronic obstructive pulmonary disease: a prospective cohort study. Phys Ther Res. 2021;24(1):35–42. doi:10.1298/ptr.E10049
28. Ammous O, Feki W, Lotfi T, et al. Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2023;1(1):CD013778.
29. Shiraishi M, Higashimoto Y, Sugiya R, et al. Enhanced diaphragm excursion and exercise tolerance in COPD patients through inspiratory muscle training after standardised pulmonary rehabilitation: randomised controlled trial. ERJ Open Res. 2024;10(6):00035–2024. doi:10.1183/23120541.00035-2024
30. Pehlivan E, Mutluay F, Balci A, Kilic L. The effects of inspiratory muscle training on exercise capacity, dyspnea and respiratory functions in lung transplantation candidates: a randomized controlled trial. Clin Rehabil. 2018;32(10):1328–1339. doi:10.1177/0269215518777560
31. Wang Y, Pessin JE. Mechanisms for fiber-type specificity of skeletal muscle atrophy. Curr Opin Clin Nutr Metab Care. 2013;16(3):243–250. doi:10.1097/MCO.0b013e328360272d
32. Goncalves DA, Silveira WA, Manfredi LH, et al. Insulin/IGF1 signalling mediates the effects of beta(2) -adrenergic agonist on muscle proteostasis and growth. J Cachexia, Sarcopenia Muscle. 2019;10(2):455–475. doi:10.1002/jcsm.12395
33. Polkey MI, Harris ML, Hughes PD, et al. The contractile properties of the elderly human diaphragm. Am J Respir Crit Care Med. 1997;155(5):1560–1564. doi:10.1164/ajrccm.155.5.9154857
34. Ohara DG, Pegorari MS, Oliveira Dos Santos NL, et al. Respiratory muscle strength as a discriminator of sarcopenia in community-dwelling elderly: a cross-sectional study. J Nutr Health Aging. 2018;22(8):952–958. doi:10.1007/s12603-018-1079-4
35. Bordoni B, Morabito B, Simonelli M. Ageing of the diaphragm muscle. Cureus. 2020;12(1):e6645. doi:10.7759/cureus.6645
36. Gosker HR, van Mameren H, van Dijk PJ, et al. Skeletal muscle fibre-type shifting and metabolic profile in patients with chronic obstructive pulmonary disease. Eur Respir J. 2002;19(4):617–625. doi:10.1183/09031936.02.00762001
37. Gosker HR, Zeegers MP, Wouters EF, Schols AM. Muscle fibre type shifting in the vastus lateralis of patients with COPD is associated with disease severity: a systematic review and meta-analysis. Thorax. 2007;62(11):944–949. doi:10.1136/thx.2007.078980
38. Maltais F, Simard AA, Simard C, Jobin J, Desgagnés P, LeBlanc P. Oxidative capacity of the skeletal muscle and lactic acid kinetics during exercise in normal subjects and in patients with COPD. Am J Respir Crit Care Med. 1996;153(1):288–293. doi:10.1164/ajrccm.153.1.8542131
39. Levine S, Kaiser L, Leferovich J, Tikunov B. Cellular adaptations in the diaphragm in chronic obstructive pulmonary disease. N Engl J Med. 1997;337(25):1799–1806. doi:10.1056/NEJM199712183372503
40. Levine S, Nguyen T, Kaiser LR, et al. Human diaphragm remodeling associated with chronic obstructive pulmonary disease: clinical implications. Am J Respir Crit Care Med. 2003;168(6):706–713. doi:10.1164/rccm.200209-1070OC
41. Jaitovich A, Barreiro E. Skeletal muscle dysfunction in chronic obstructive pulmonary disease. What we know and can do for our patients. Am J Respir Crit Care Med. 2018;198(2):175–186. doi:10.1164/rccm.201710-2140CI
42. Turton P, AL S, Welters I. A narrative review of diaphragm ultrasound to predict weaning from mechanical ventilation: where are we and where are we heading? Ultrasound J. 2019;11(1):2. doi:10.1186/s13089-019-0117-8
43. McDonald ML, Diaz AA, Ross JC, et al. Quantitative computed tomography measures of pectoralis muscle area and disease severity in chronic obstructive pulmonary disease. A cross-sectional study. Ann Am Thorac Soc. 2014;11(3):326–334. doi:10.1513/AnnalsATS.201307-229OC
44. Tanimura K, Sato S, Fuseya Y, et al. Quantitative assessment of erector spinae muscles in patients with chronic obstructive pulmonary disease. Novel chest computed tomography-derived index for prognosis. Ann Am Thorac Soc. 2016;13(3):334–341. doi:10.1513/AnnalsATS.201507-446OC
45. Alam MJ, Roy S, Iktidar MA, et al. Diaphragm ultrasound as a better predictor of successful extubation from mechanical ventilation than rapid shallow breathing index. Acute Crit Care. 2022;37(1):94–100. doi:10.4266/acc.2021.01354
46. Eksombatchai D, Sukkratok C, Sutherasan Y, Junhasavasdikul D, Theerawit P. The ratio of respiratory rate to diaphragm thickening fraction for predicting extubation success. BMC Pulm Med. 2023;23(1):109. doi:10.1186/s12890-023-02392-w
47. Tudorache V, Oancea C, Mladinescu OF. Clinical relevance of maximal inspiratory pressure: determination in COPD exacerbation. Int J Chron Obstruct Pulmon Dis. 2010;5:119–123. doi:10.2147/copd.s9194
48. Tenda ED, Henrina J, Setiadharma A, et al. The impact of body mass index on mortality in COPD: an updated dose-response meta-analysis. Eur Respir Rev. 2024;33(174):0261–2023. doi:10.1183/16000617.0261-2023
49. Schols AM, Ferreira IM, Franssen FM, et al. Nutritional assessment and therapy in COPD: a European Respiratory Society statement. Eur Respir J. 2014;44(6):1504–1520. doi:10.1183/09031936.00070914
50. Sugawara K, Takahashi H, Kasai C, et al. Effects of nutritional supplementation combined with low-intensity exercise in malnourished patients with COPD. Respir Med. 2010;104(12):1883–1889. doi:10.1016/j.rmed.2010.05.008
51. van de Bool C, Rutten EPA, van Helvoort A, Franssen FME, Wouters EFM, Schols A. A randomized clinical trial investigating the efficacy of targeted nutrition as adjunct to exercise training in COPD. J Cachexia, Sarcopenia Muscle. 2017;8(5):748–758. doi:10.1002/jcsm.12219
52. Hsieh MJ, Yang TM, Tsai YH. Nutritional supplementation in patients with chronic obstructive pulmonary disease. J Formos Med Assoc. 2016;115(8):595–601. doi:10.1016/j.jfma.2015.10.008
53. Aldhahir AM, Rajeh AMA, Aldabayan YS, et al. Nutritional supplementation during pulmonary rehabilitation in COPD: a systematic review. Chron Respir Dis. 2020;17:1479973120904953. doi:10.1177/1479973120904953
54. Oyama Y, Tatsumi H, Takikawa H, Taniguchi N, Masuda Y. Combined effect of early nutrition therapy and rehabilitation for patients with chronic obstructive pulmonary disease exacerbation: a prospective randomized controlled trial. Nutrients. 2024;16(5):739. doi:10.3390/nu16050739
55. Moore E, Palmer T, Newson R, Majeed A, Quint JK, Soljak MA. Pulmonary rehabilitation as a mechanism to reduce hospitalizations for acute exacerbations of COPD: a systematic review and meta-analysis. Chest. 2016;150(4):837–859. doi:10.1016/j.chest.2016.05.038
56. Phillips DB, James MD, O’Donnell CD, et al. Physiological predictors of morbidity and mortality in COPD: the relative importance of reduced inspiratory capacity and inspiratory muscle strength. J Appl Physiol. 2022;133(3):679–688. doi:10.1152/japplphysiol.00352.2022
57. de Souza Y, Suzana ME, Medeiros S, Macedo J, da Costa CH. Respiratory muscle weakness and its association with exercise capacity in patients with chronic obstructive pulmonary disease. Clin Respir J. 2022;16(2):162–166. doi:10.1111/crj.13449
58. Derchak PA, Sheel AW, Morgan BJ, Dempsey JA. Effects of expiratory muscle work on muscle sympathetic nerve activity. J Appl Physiol. 2002;92(4):1539–1552. doi:10.1152/japplphysiol.00790.2001
59. Shiraishi M, Higashimoto Y, Sugiya R, et al. Diaphragm dome height on chest radiography as a predictor of dynamic lung hyperinflation in COPD. ERJ Open Res. 2023;9(3):00079–2023. doi:10.1183/23120541.00079-2023
60. Shiraishi M, Higashimoto Y, Sugiya R, et al. Sternocleidomastoid muscle thickness correlates with exercise tolerance in patients with COPD. Respiration. 2023;102(1):64–73. doi:10.1159/000527100
61. Miki K, Tsujino K, Fukui M, et al. Laryngeal widening and adequate ventilation by expiratory pressure load training improve aerobic capacity in COPD: a randomised controlled trial. Thorax. 2023;79(1):23–34. doi:10.1136/thorax-2022-219755
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Derivatives of Reactive Oxygen Metabolites are Associated with Severity of Chronic Obstructive Pulmonary Disease and Affected by a p53 Gene Polymorphism
Yamamura K, Nojiri M, Nishiki K, Kato R, Shinomiya S, Takahara Y, Oikawa T, Ishizaki T, Toga H, Mizuno S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1589-1600
Published Date: 13 July 2022
Development and Validation of a Multivariable Prediction Model to Identify Acute Exacerbation of COPD and Its Severity for COPD Management in China (DETECT Study): A Multicenter, Observational, Cross-Sectional Study
Yin Y, Xu J, Cai S, Chen Y, Chen Y, Li M, Zhang Z, Kang J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2093-2106
Published Date: 5 September 2022
The Influence of Influenza Virus Infections in Patients with Chronic Obstructive Pulmonary Disease
Liao KM, Chen YJ, Shen CW, Ou SK, Chen CY
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2253-2261
Published Date: 14 September 2022
Analyses of Factors Associated with Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Review
Qian Y, Cai C, Sun M, Lv D, Zhao Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2707-2723
Published Date: 24 November 2023
Impact of Nutritional Status and Sarcopenia on Acute Exacerbation Risk in Stable Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study
Pan H, Wang M, Chen X, Wang Y
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:605988
Published Date: 13 May 2026