Back to Journals » Open Access Emergency Medicine » Volume 14
Reasons for Emergency Department Visit, Outcomes, and Associated Factors of Oncologic Patients at Emergency Department of Jimma University Medical Centre
Authors Workina A ![]() , Habtamu A
, Habtamu A ![]() , Zewdie W
, Zewdie W ![]()
Received 10 July 2022
Accepted for publication 19 October 2022
Published 28 October 2022 Volume 2022:14 Pages 581—590
DOI https://doi.org/10.2147/OAEM.S381816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Abdata Workina,1 Asaminew Habtamu,1 Wondeson Zewdie2
1Department of Nursing, Jimma University, Jimma, Oromia, Ethiopia; 2Department of Emergency, Jimma University Medical Centre, Jimma, Oromia, Ethiopia
Correspondence: Abdata Workina, Department of Nursing, Jimma University, Jimma University, P.O. Box-378, Jimma, Oromia, Ethiopia, Tel +251923643857, Email [email protected]
Introduction: The number of oncologic patients visiting the emergency department (ED) is increasing and represent a challenge for the emergency team owing to they might have acute sign and symptoms of a still undiagnosed malignancy, management of treatment-related side effects, co-morbidities, and palliative care. Thus, this study was aimed to identify reasons for ED visits, management outcomes, and associated factors of oncologic patients.
Patients and Methods: A prospective cross-sectional study was conducted from March 11, 2021 to August 25, 2021 at the ED of Jimma University Medical Center on a total of 338 oncologic patients. Data were collected from the patient and the patient’s medical record using a questionnaire developed from up-to-date similar literatures. The questionnaire was started filled out upon diagnosis of cancer and completed during discharge from the ED. The outcomes of the patients were dichotomized into died and survived then, it was analyzed using frequency and bivariate logistic regression.
Results: The most common reasons for oncologic patients ED visit were neutropenic fever 79 (23.4%) followed by vomiting 38 (11.2%) and electrolyte abnormality 37 (10.9%) respectively. Among oncologic patients visited ED, 137 (40.5%) of them were admitted to ward and 126 (37.3%) of them were discharged with improvement while 64 (18.9%) of them were died. Based on multivariate logistic regression, those patients who had distant metastasis cancer (AOR 1.85; 95% CI 1.03– 7.21), comorbidity (AOR 2.56; 95% CI 1.20, 6.96), and ECOG > 3 (AOR 2.40; 95% CI 1.25,13.43) were more likely to die than their counterparts.
Conclusion: Most of the oncologic patients visited ED due to neutropenic fever, nausea and or vomiting, and electrolyte disorder. Amongst oncologic patients who were visited ED, most of them were admitted to ward while around one-fifth of them were died. Having distant metastasis cancer, comorbidity and ECOG > 3 were independent predictors of an oncologic patient’s outcome at the ED.
Keywords: cancer, oncology, emergency department, metastasis, ED
Introduction
Although there is a development of surgical and medical cancer management modalities, it is a major public health concern worldwide.1–5 It is estimated that cancer kills over 7.9 million people globally each year constituting about 13% of total deaths worldwide.5 The overall burden of cancer in the world is projected to continue to rise, particularly in developing countries. It is anticipated that an estimated 21 million people will be diagnosed, and 13 million will die of cancer in the year 2030 unless treatment intervention takes place.5–7
Among patients with cancer, 6.8% of them visited the emergency department (ED). Of whom, more than half of the patients were admitted to inpatient service for further management.8 Cancer patients visit EDs due to management of treatment-related side effects, oncologic emergencies, co-morbidities, and end-of-life care.9,10 These oncologic emergencies are occurring in 30–50% of cancer patients presenting to EDs. It comprises malignant spinal cord compression, increased intracranial pressure (ICP), metabolic and endocrine emergencies, cardiac emergencies, airway and pulmonary emergencies like pneumothorax, pleural effusion, radiation-induced lung injury, aspiration pneumonia, malignant airways disease, pulmonary vascular disease, diaphragmatic dysfunction; gastrointestinal (GI) emergencies like nausea and vomiting, constipation, diarrhea, ascites, hepatic encephalopathy, malignant gastroparesis, GI bleeding, nephro-urologic emergencies that take in acute kidney injury, tumor lysis syndrome, obstructive uropathy, infectious emergencies like neutropenic fever, sepsis are complications that result in an ED visit.2,8,9,11,12
Mortality due to oncologic emergency in low-income countries can range from 19.7% to 37.6%, and in the USA 13% of cancer patients who visited the ED died even though care was provided, and early recognition of the conditions at triage have a significant impact in the quality of life and mortality rate of patients.13,14 The outcome of cancer patients who visited the EDcan be predicted by region of cancer, stage of cancer, associated comorbidity, and measures taken to control cancer.4–6
Even though some studies were conducted related to ED visits of cancer patients and its outcome, there is no data in Ethiopia. Thus, this study helps to identify the reasons for oncologic patients ED visit, outcomes and related factors which will be used for further appropriate preparedness and to improve quality of healthcare provided for the patients. Furthermore, this study finding can be used as a baseline finding, especially in resource limited countries like Ethiopia.
Methods and Materials
Study Design and Setting
A prospective cross-sectional study was conducted from March 11, 2021 to August 25, 2021 at the ED of Jimma University Medical Center. Jimma University Medical Center (JUMC) was located in south-west Ethiopia and provides teaching and research services in addition to medical services. It is the only teaching and referral hospital in the south-western part of the country. The medical center provides services for more than 20 million patients with 800 beds from south-west Ethiopia. The institution is providing services for around 15,000 inpatients, 160,000 outpatient attendants, 11,000 emergency cases, and 4500 deliveries per year.16,17
Study Population
All oncologic patients who were visited the adult ED of JUMC from March 11, 2021 to August 25, 2021.
Eligibility Criteria
Cancer patients aged ≥ 14 years old who visited the ED due to cancer related cause were included in the study. Oncologic patients who seek care for another disease other than cancer, such as cancer patients who presented to the ED due to trauma or poisoning, were excluded from the study.
Sample Size Determination and Sampling Procedure
Patients presenting to the ED with a cancer-related complaint from March 11, 2021 to August 25, 2021 were triaged using South Africa triaging system. Then, after patients were diagnosed for cancer based International Classification of Disease 10th Revision Clinical Modification (ICD-10-CM) diagnoses codes, they were sequentially enrolled in the study until the expected sample size, 340, was reached.
Data Collection Tool and Procedure
A questionnaire was developed from up-to-date similar literatures which contain socio-demographic characteristics, clinical profile (chief complaint, comorbidity, primary tumor site, prior ED presentation treatment and tumor status), reasons for ED visit and outcome of the patient.6,11,15,18–21 The variables like prior cancer treatment, ED complaints, educational status, occupation, marital status and comorbidity were collected from the patient and status of cancer, oncologic complications, primary tumor location, and region of metastasis were collected from patient’s medical record. Comorbidities are those included in the Charlson comorbidity score and cancer diagnosis was categorized based on International Classification of Disease 10th Revision Clinical Modification (ICD-10-CM) diagnoses codes. The data was collected 24 hours during the data collection period and the patient was followed from histological diagnosis to discharge from the ED. The data was collected by 4 BSc nurses working at the ED of JUMC.
Data Quality Assurance
The questionnaire was pilot-tested at the study site on 26 oncologic patients three days prior to the actual data collection. The questionnaire was started upon diagnosis of cancer and completed during discharge from the ED. Data collectors were trained on the contents of the tool and the supervisor provided onsite close supervision, and technical support, and checked all filled questionnaires for completeness, accuracy, and consistency.
Data Processing and Analysis
Ethical Considerations
The ethical approval and clearance were obtained from Jimma University Institutional Review Board (IRB) and a cooperation letter was written to the CEO of the Jimma University Medical Centre to conduct the study. The adult emergency ward staff were informed and permission was obtained from them. Written informed consent was obtained from the study participants. Confidentiality of all the study participants was highly maintained throughout the data collection of the research process. For those patients under 18 years of age, parental informed consent was obtained. This study complies with the Declaration of Helsinki.
Result
Socio-Demographic Characteristics of Cancer Patients
A total of 338 oncologic patients were included in the study, out of which 202 (59.8%) were females. The mean age of the patients is 43.0±14.9SD. Regarding the educational status of the participants, 114 (33.7%), of them had learned up to high/preparatory school whereas around one-fifth, 53 (15.7%), of them had completed a diploma or above. Most of the patients were referred from other government hospitals (113; 33.4%), followed by 96 (28.4%), who were transferred from OPD of JUMC. Concerning the time of ED arrival, more than half (224; 66.3%), of them visited the ED during day time (from 6:00 AM to 6:00PM) while the rest were during the night (from 6:00 PM to 6:00 AM) (Table 1).
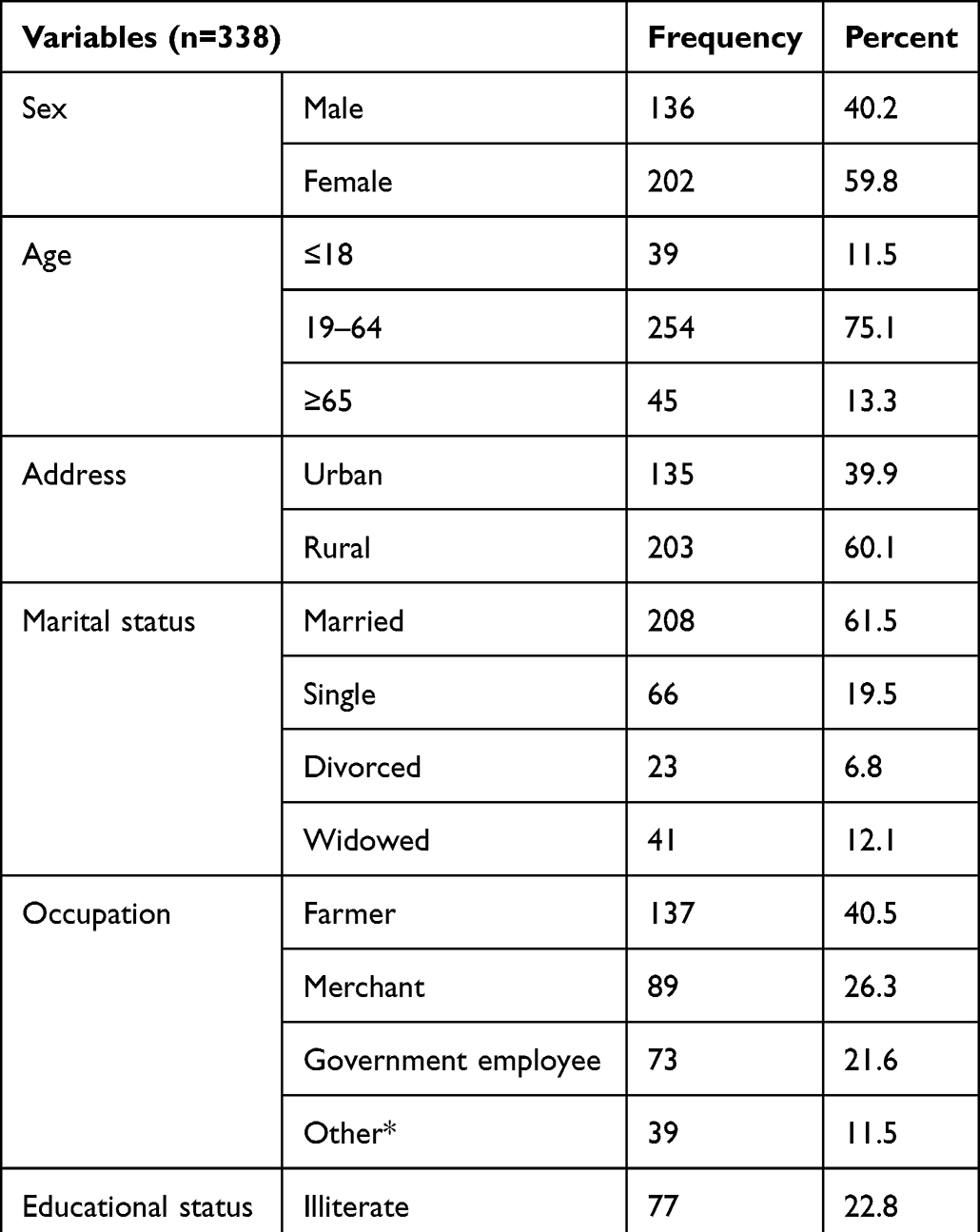 |
Table 1 Socio-Demographic Characteristics of Patients with Cancer at the ED of JUMC, Jimma, Ethiopia, 2021 |
Clinical Profile of Oncologic Patients Who Visited ED
The most major complaint of the oncologic patients was easy fatigability (50; 14.8%) followed by shortness of breath (5; 19.2%) and vomiting (39; 11.5%) respectively. Almost around one-third (144; 42.6%), of the oncologic patients had comorbidity, out of which 45 (13.3%), 32 (9.5%) and 29 (8.6%) had a retroviral infection, diabetes mellitus and hypertension, respectively. Concerning primary cancer sites, one-third (117; 34.6%), accounted for blood cancer followed by cervical cancer (53; 15.7%) and breast cancer (39; 11.5%) respectively. Amongst the patients who visited ED, more than half (193; 57.1%), of them had locally advanced cancer while the rest had distant metastases (Table 2).
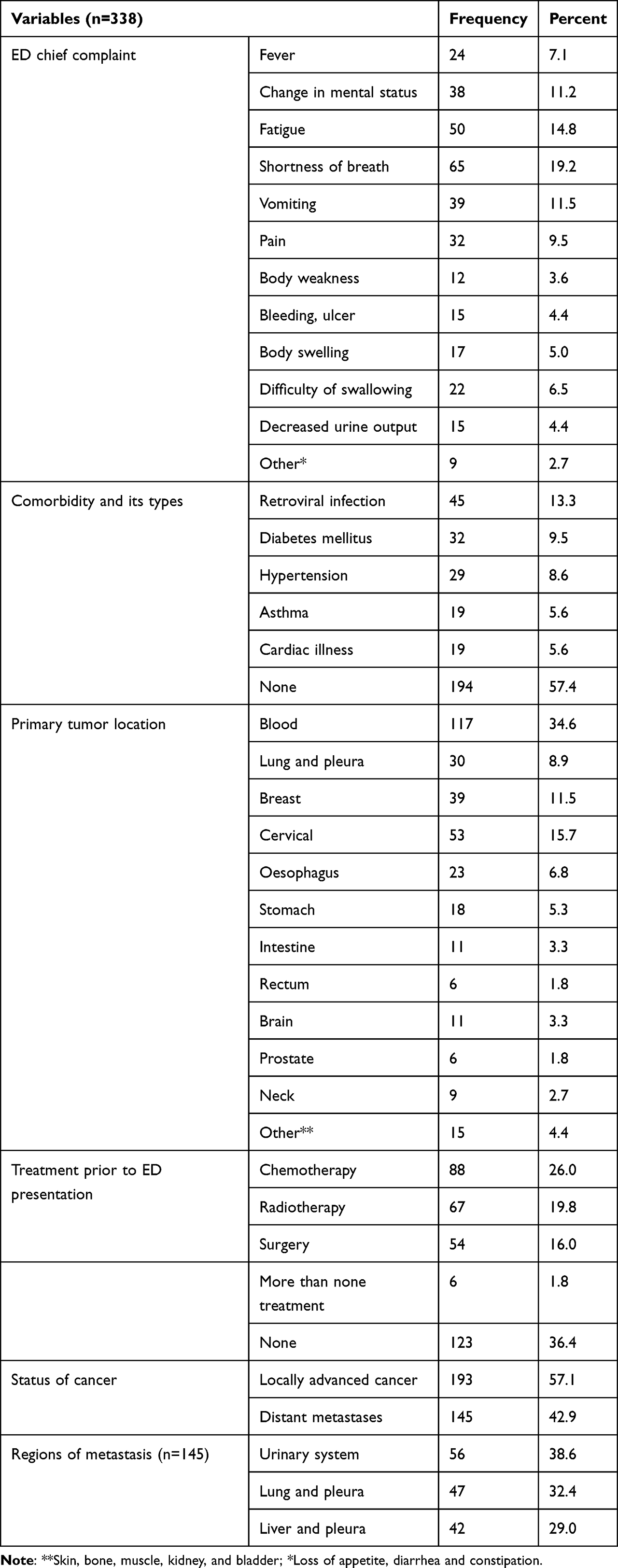 |
Table 2 Clinical Characteristics of Oncologic Patients Who Visited ED of JUMC, Jimma, Ethiopia, 2021 |
Reasons for ED Visit, and Outcome of Oncologic Patients Who Visited ED
The most common reason for oncologic ED visits was neutropenic fever (79; 23.4%) followed by nausea/and vomiting (38; 11.2%) and electrolyte abnormality (37; 10.9%). Among the study participants, around one-third (105; 31.1%) of them were categorized under eastern cooperative oncology group (ECOG) category one whereas, 62 (18.3%) of them were categorized under ECOG4. Regarding the outcomes of patients at the ED, 137 (40.5%) of them were admitted to ward and 126 (37.3%) of them were discharged with improve while 64 (18.9%) of the oncologic patients died (Table 3).
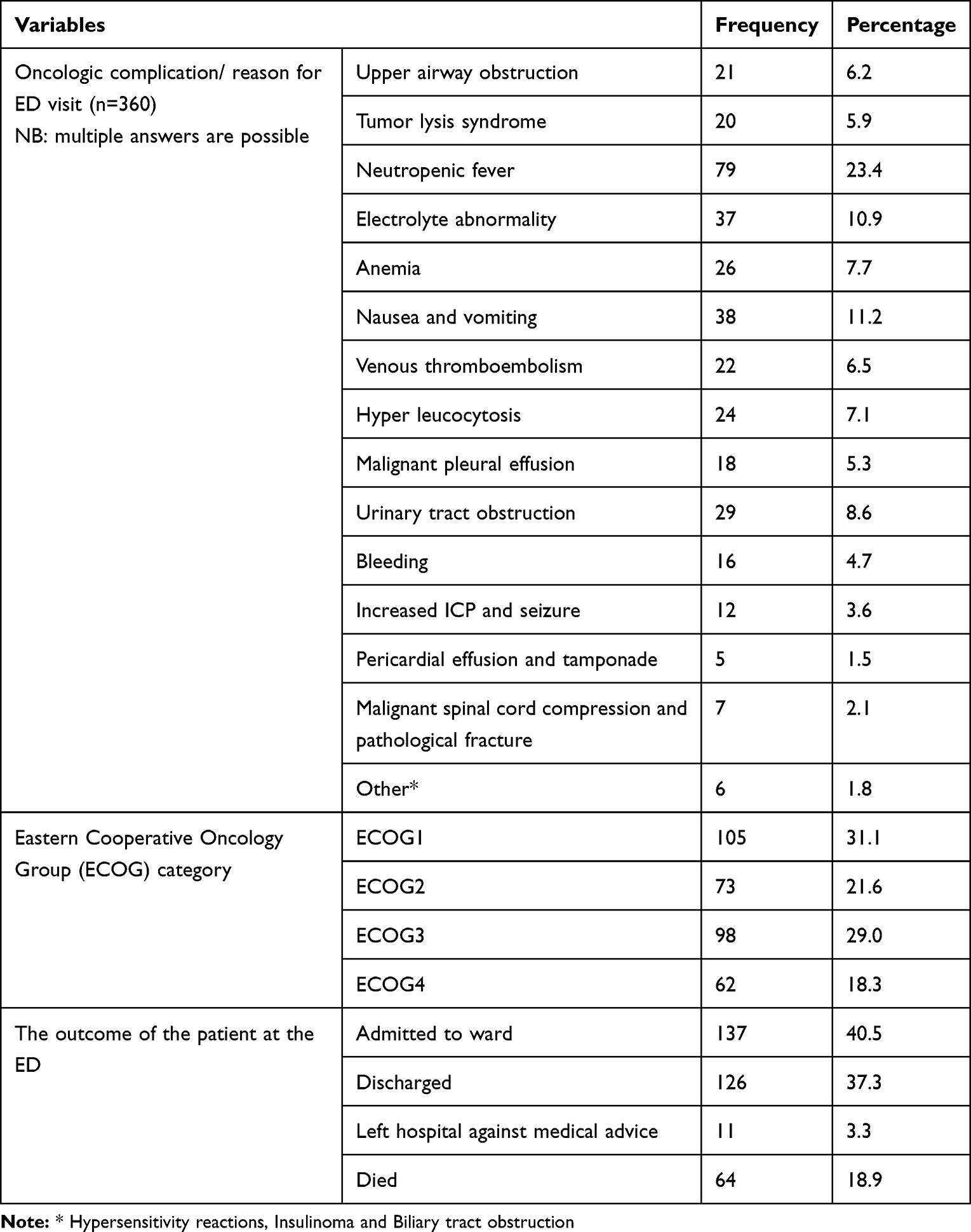 |
Table 3 Oncologic Complications (Reason for ED Visit) and Outcome of Oncologic Patients at the ED of JUMC, Jimma, Ethiopia, 2021 |
Factors Associated with the Outcome of Oncologic Patients
Outcomes of oncologic patients at the ED were dichotomized into died and survived to compute bivariate logistic regression. Those predictor variables having p-value <0.25 were transferred into multivariate logistic regression to overcome the effect of cofounding variable. In the multivariate logistic regression variables having p-value <0.05 were considered statistically significant associations.
In bivariate logistic regression, those patients aged ≤18 years (COR 1.82; 95% CI, 0.64–5.19) and ≥65 years (COR 22.42; 95% CI, 8.11–31.07) were more likely to die than those aged 18 to 64 years old patients. Furthermore, predictor variables night time ED arrival (COR 3.81; 95% CI, 2.17–6.70), distant metastasis of cancer (COR 2.91; 95% CI, 1.66–5.13), having comorbidity (COR 4.19(); 95% CI, 2.32, 7.55), Poor ECOG (COR 5.93; 95% CI, 3.08, 11.44), and primary tumor site were the factors which predict the outcomes of oncologic patients at the ED (Table 4).
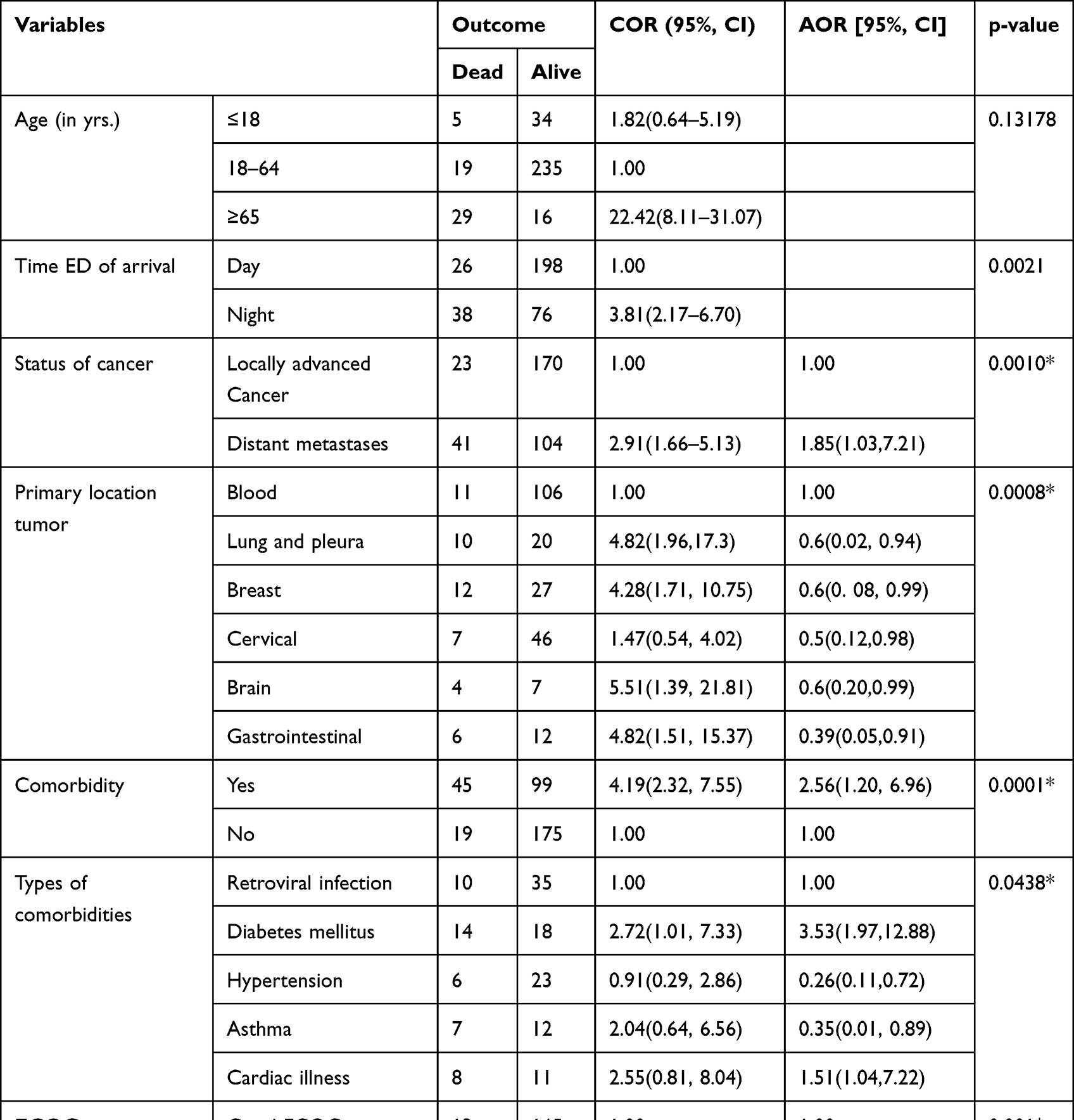 |
Table 4 Bivariate and Multivariate Logistic Regression Analysis of Oncologic Patients’ Outcome Who Visited ED of JUMC, Jimma, Ethiopia, 2021 |
Based on multivariate logistic regression, those patients with distant metastasis cancer were 1.85 times more likely to die than locally advanced cancer types (AOR 1.85; 95% CI 1.03–7.21, P=0.0010). Additionally, having comorbidity (AOR 2.56; 95% CI 1.20, 6.96), and ECOG >3 (AOR 2.40; 95% CI 1.25,13.43) were independent predictors of patient outcomes (Table 4).
Discussion
Due to the increasing prevalence of cancer alongside cancer survival rates, the number of oncologic patients visiting ED may increase.22 These oncologic patients may visit the ED because of signs and symptoms of the disease itself, treatment complications and palliative care services. The increasing burden of ED visits of oncologic patients might be considered as poor quality of cancer.1,11,18,23 Therefore, this study aimed to identify the reasons for oncologic patients ED visits, their treatment outcomes and associated factors.
This study showed that the most common reason for oncologic ED visit was neutropenic fever (79; 23.4%) followed by nausea and or vomiting (38; 11.2%) and electrolyte abnormality (37 10.9%) respectively. This study finding was consistent with the study conducted at Asan medical centre which revealed, that among cancer patients visited emergency room infection (22.8%) of them had neutropenic fever.19 Furthermore, this study findings were consistent with studies in conducted Turkey, Japan, USA and Korea which elucidated, the main reason for ED visit were, nausea and vomiting (40; 16.5%) and fever (29; 11.9%), febrile neutropenia is the most common cause of ED visit, vomiting (13.8%), is commonest reason of ED visit and one of primary reasons of ED visit was febrile neutropenia respectively.2,3,22,23
On the other hand, our study finding was in contrast with study conducted in California, Ohio, Jordan and India which elucidated the most common ED diagnoses among cancer patient were pain (10.4%), sepsis (5.7%) and nausea/vomiting (2.3%), the most common patients visited the ED due to pain 62.1%, pain is the most common reason for cancer-related ED visits and the main reason for ED visits was mental confusion (24%), respectively.1,5,24,25 The reasons for this inconsistency might be that some of the studies even included suspected cancer cases and included cancer patients even the patients visited ED due to other causes like trauma whereas our study did not it. Besides, the ED presentation of oncologic patients may be differed significantly by cancer type.
Regarding the outcomes of patients at the ED, 137 (40.5%) of them were admitted to ward and 126 (37.3%) of them were discharged with improve while 64 (18.9%) of the oncologic patients were died. This study finding was relatively consistent with study conducted in South Korea which was explicated, 16.1% of cancer patients who visited the ED died.8 Moreover, this study finding was consistent with the study conducted in Turkey and Korea which showed 39% (40) of oncologic patients were hospitalized and 54.8% of cancer-related ED visits were hospitalized.9,22
However, our study finding was inconsistent with study conducted in the USA showed that among cancer patients who visited the ED, 13% of them died.14 This variance might be due to the quality of patient care gap among developing and developed countries. Conversely, our study finding in terms of oncologic patients’ death at the ED was lower relative to study conducted at Chapel Hill, USA which revealed that 81 (28.6%) patients died.12 The possible explanation for this variability was the study conducted at Chapel Hill included death on arrival while our study only included confirmed oncologic cases who visited the ED. Additionally, this study finding is incomparable with the study conducted in Japan that explained that 67% of oncologic patients were admitted to hospital.2 The possible reason for this inconsistency might be that this study included only 45 patients, unlike our study which may cause bias.
Based on multivariate logistic regression, those patients who had distant metastasis cancer (AOR 1.85; 95% CI 1.03–7.21), comorbidity (AOR 2.56; 95% CI 1.20, 6.96), and ECOG >3 (AOR 2.40; 95% CI 1.25,13.43) were more likely to die than their counterparts while, age of patient and time of ED arrival were not associated with outcomes oncologic patients at the ED. This study's finding was consistent with the study conducted in Hungarian which revealed that the presence of comorbidity (AOR: 7.14) was associated with outcomes of emergency cancer outcomes. However, this finding was in contrast to the other side that showed age of patients affects treatment outcomes.26 Besides, our finding was comparable with other studies that explicated cancer metastasis (AOR 1.64, CI 1.41–1.92), and having diabetes (AOR 1.11, CI 1.00–1.24) were predictors of patient outcome at the ED and the highest mortality was recorded among patients with distant metastasis (AOR 2.227; 95% CI, 2.124–2.335; P < 0.001), respectively.6,8
Nevertheless, this study’s finding was not consistent with other studies.4,27 This dissimilarity might be due to patients may present ED with varied types of signs and symptoms’ severity.
Limitations of the Study
The limitation of this study were; the management outcome of patients was followed until discharge from the ED. Thus, following ED discharge more patients might die. Moreover, the confidence intervals in bivariate and multivariate logistic regression was very wide and the results were interpreted in light of this limitation.
Conclusion
Most oncologic patients visited ED due to febrile neutropenia, nausea and or vomiting, and electrolyte disorder. Amongst oncologic patients who visited ED, most of them were admitted to ward while around one-fifth of them died. Therefore, improve quality of care at the ED is a fundamental to improve outcome of oncologic patients. Having distant metastasis cancer, comorbidity and ECOG >3 were independent predictors of oncologic patient’s outcome at the ED. Even though, this study finding can be used as baseline especially from low income countries, further multicenter study is needed.
Acknowledgments
We would like to thank Jimma University Medical Centre staff for their technical support during data collection.
Disclosure
The authors declare no competing interest in this research work.
References
1. Nene RV, Brennan JJ, Castillo EM, Tran P, Hsia RY, Coyne CJ. Cancer-related emergency department visits: comparing characteristics and outcomes. West J Emerg Med. 2021;22(5):1117–1123. doi:10.5811/westjem.2021.5.51118
2. Kotajima F, Kobayashi K, Sakaguchi H, Nemoto M. Lung cancer patients frequently visit the emergency room for cancer-related and -unrelated issues. Mol Clin Oncol. 2014;2(2):322–326. doi:10.3892/mco.2014.241
3. Gallaway MS, Idaikkadar N, Tai E, et al. Emergency department visits among people with cancer: frequency, symptoms, and characteristics. J Am Coll Emerg Physicians Open. 2021;2(3):e12438. doi:10.1002/emp2.12438
4. Ilit T, Bar-Sela G. Effective patient selection for an oncology-dedicated emergency service: a retrospective study. JCO Oncol Pract. 2021;17(10):e1567–e1575. doi:10.1200/OP.20.01081
5. Caterino JM, Adler D, Durham DD, et al. Analysis of diagnoses, symptoms, medications, and admissions among patients with cancer presenting to emergency departments. JAMA Netw Open. 2019;2(3):e190979. doi:10.1001/jamanetworkopen.2019.0979
6. Westley T, Syrowatka A, Henault D, et al. Patterns and predictors of emergency department visits among older patients after breast cancer surgery: a population-based cohort study. J Geriatr Oncol. 2018;9(3):204–213. doi:10.1016/j.jgo.2017.10.003
7. Reyes-Gibby CC, Melkonian SC, Hanna EY, et al. Cohort study of oncologic emergencies in patients with head and neck cancer. Head Neck. 2017;39(6):1195–1204. doi:10.1002/hed.24748
8. Kim YJ, Seo DW, Kim WY. Types of cancer and outcomes in patients with cancer requiring admission from the emergency department: a nationwide, population-based study, 2016–2017. Cancer. 2021;127(14):2553–2561. doi:10.1002/cncr.33534
9. Tanriverdi O, Beydilli H, Yildirim B, Karagoz U. Single center experience on causes of cancer patients visiting the emergency department in southwest Turkey. Asian Pac J Cancer Prev. 2014;15(2):687–690. doi:10.7314/apjcp.2014.15.2.687
10. Scarborough B, Goldhirsch S, Chai E. Building a supportive oncology practice that impacts emergency department visits, hospice utilization, and hospital admission. J Palliat Med. 2018;21(10):1499–1503. doi:10.1089/jpm.2017.0709
11. Yang Z, Yang R, Kwak MJ, et al. Oncologic emergencies in a cancer center emergency department and in general emergency departments countywide and nationwide. PLoS One. 2018;13(2):e0191658. doi:10.1371/journal.pone.0191658
12. Leak A, Mayer DK, Wyss A, Travers D, Waller A. Why do cancer patients die in the emergency department?: an analysis of 283 deaths in NC EDs. Am J Hosp Palliat Care. 2013;30(2):178–182. doi:10.1177/1049909112445306
13. Yang Z, Qdaisat A, Hu Z, et al. Cardiac troponin is a predictor of septic shock mortality in cancer patients in an emergency department: a retrospective cohort study. PLoS One. 2016;11(4):e0153492. doi:10.1371/journal.pone.0153492
14. Elsayem AF, Elzubeir HE, Brock PA, Todd KH. Integrating palliative care in oncologic emergency departments: challenges and opportunities. World J Clin Oncol. 2016;7(2):227–233. doi:10.5306/wjco.v7.i2.227
15. Nirenberg A, Mulhearn L, Lin S, Larson E. Emergency department waiting times for patients with cancer with febrile neutropenia: a pilot study. Oncol Nurs Forum. 2004;31(4):711–715. doi:10.1188/04.ONF.711-715
16. JIMMA. Aslan. Available from: https://www.aslanproject.org/jumc.
17. Hordofa DF, Daba KT, Mengesha AA. Clinical presentation of retinoblastoma in Ethiopia: a case of Jimma university medical center pediatric oncology unit, Southwest Ethiopia. Ethiop J Health Sci. 2021;31(5):963–968. doi:10.4314/ejhs.v31i5.7
18. Torigoe T, Imanishi J, Yazawa Y, et al. Oncologic emergency in patients with skeletal metastasis of unknown primary. Acute Med Surg. 2021;8(1):e600. doi:10.1002/ams2.600
19. Ahn S, Lee YS, Lim KS, Lee JL. Emergency department cancer unit and management of oncologic emergencies: experience in Asan Medical Center. Support Care Cancer. 2012;20(9):2205–2210. doi:10.1007/s00520-012-1478-8
20. Pettit N, Boadu D, Bischof JJ. Emergency department management of chemotherapy related febrile neutropenia: an opportunity to improve care. Am J Emerg Med. 2021;50:5–9. doi:10.1016/j.ajem.2021.07.008
21. Cimpoeşu D, Dumea M, Durchi S, et al. [Oncological emergencies in the emergency department]. Rev Med Chir Soc Med Nat Iasi. 2011;115(4):1073–1079. Romanian
22. Lee SY, Ro YS, Shin SD, Moon S. Epidemiologic trends in cancer-related emergency department utilization in Korea from 2015 to 2019. Sci Rep. 2021;11(1):21981. doi:10.1038/s41598-021-01571-1
23. Bayrak E, Kitiş Y. The main reasons for emergency department visits in cancer patients. Haseki Tip Bül. 2018;56(1):6–13. doi:10.4274/haseki.83997
24. Alsharawneh A, Hasan AAH. Cancer related emergencies with the chief complaint of pain: incidence, ED recognition, and quality of care. Int Emerg Nurs. 2021;56:100981. doi:10.1016/j.ienj.2021.100981
25. Amado JP, Vasquez R, Huari RW, Sucari AS, Oscanoa TJ. Patients with end-stage oncologic and nononcologic disease in emergency service of an Urban Tertiary Hospital. Indian J Palliat Care. 2018;24(1):25–27. doi:10.4103/IJPC.IJPC_108_17
26. Koch M, Varga C, Soós V, et al. Main reasons and predictive factors of cancer-related emergency department visits in a Hungarian tertiary care center. BMC Emerg Med. 2022;22(1):114. doi:10.1186/s12873-022-00670-0
27. Klotz AD, Caterino JM, Durham D, et al. Observation unit use among patients with cancer following emergency department visits: results of a multicenter prospective cohort from CONCERN. Acad Emerg Med. 2022;29(2):174–183. doi:10.1111/acem.14392
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Burden of Metastatic Cancer–Induced Bone Pain: A Narrative Review
Colosia A, Njue A, Bajwa Z, Dragon E, Robinson RL, Sheffield KM, Thakkar S, Richiemer SH
Journal of Pain Research 2022, 15:3399-3412
Published Date: 25 October 2022
The Use of Chatbots in Oncological Care: A Narrative Review
Wang A, Qian Z, Briggs L, Cole AP, Reis LO, Trinh QD
International Journal of General Medicine 2023, 16:1591-1602
Published Date: 1 May 2023
Psychometric Properties of the Peruvian Version of the MOS Scale for Social Support in Cancer Patients and Convergent Network with Quality of Life
Ramos-Vera C, Calle D, Collacso Fiesta H, Lamilla LL, Serpa-Barrientos A, Saintila J
Patient Preference and Adherence 2023, 17:1999-2011
Published Date: 14 August 2023
Evaluating the Outcomes in Patients with Colorectal Cancer Using the Malnutrition Universal Screening Tool: A Systematic Review
Muntean C, Blidari AR, Faur AM, Curca RO, Feier CVI
Journal of Multidisciplinary Healthcare 2024, 17:4277-4289
Published Date: 3 September 2024
Analysis of Risk Factors and Risk Prediction for Cervical Lymph Node Metastasis in Thyroid Papillary Carcinoma
Tian D, Li X, Jia Z
Cancer Management and Research 2024, 16:1571-1585
Published Date: 11 November 2024