Back to Journals » Journal of Pain Research » Volume 18
Programmed Intermittent Bolus versus Continuous Infusion for Regional Analgesia Following Thoracoscopic Surgery: A Systematic Review and Meta-Analysis
Authors Ren D, Liu Z, Gao Y, Xie N, Lu Y, Ge L
Received 31 March 2025
Accepted for publication 3 August 2025
Published 13 August 2025 Volume 2025:18 Pages 4073—4083
DOI https://doi.org/10.2147/JPR.S530018
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Dongqing Ren, Zhilong Liu, Yanjun Gao, Na Xie, Yu Lu, Li Ge
Department of Anesthesiology, Gansu Provincial Hospital, Lanzhou, Gansu, People’s Republic of China
Correspondence: Li Ge, Email [email protected]
Background: Continuous regional analgesia techniques have emerged as a more effective alternative for postoperative analgesia, but the clinical efficacy of infusion modes in thoracoscopic surgery remains controversial. This systematic review and meta-analysis to compare the efficacy of programmed intermittent bolus infusion (PIBI) with continuous infusion (CI) for regional analgesia in patients undergoing thoracoscopic surgery.
Methods: We searched PubMed, Embase, Web of Science, and the Cochrane Library for relevant research from inception to March 2025. Randomized controlled trials (RCTs) comparing PIBI with CI for regional analgesia following thoracoscopic surgery were included. The meta-analysis was made by using ReMan 5.4 software.
Results: We included 7 RCTs with 394 patients. For resting VAS at 6 h, there was no significant difference between PIBI and CI (MD = − 0.52, 95% CI: − 1.23 to 0.20). PIBI was more likely to reduce the resting VAS at 12 h, movement VAS at 12 h, and morphine consumption in first 24 h. PIBI had lower local anesthetic consumption and wider range of sensory blockade than CI. However, there were no significant difference between PIBI and CI in terms of the resting VAS at 24 h, resting VAS at 48 h, movement VAS at 6 h, movement VAS at 24 h, movement VAS at 48 h, morphine consumption in second 24 h, and number of people using additional analgesics.
Conclusion: PIBI provided a lower local anesthetic consumption and a wider sensory blockade compared to CI for regional analgesia following thoracoscopic surgery, although no significant clinical differences were observed in postoperative pain scores, opioid consumptions, and number of people using additional analgesics.
Limitation: The heterogeneity may influence the pooled estimates, the conclusion was only suitable for pulmonary surgery, the lack of long-term follow-up data on chronic pain outcomes.
Keywords: intermittent infusion, continuous infusion, thoracoscopic, systematic review, meta-analysis
Introduction
Thoracic surgery, including lung resection, esophagectomy, and mediastinal tumor resection, is often associated with severe postoperative pain due to the extensive dissection of intercostal nerves and pleural surfaces.1 Thoracoscopic surgery has become a mainstay for various thoracic conditions, offering advantages such as reduced pain, shorter hospital stays, and improved cosmetic outcomes compared to traditional open thoracotomy.2 However, postoperative pain management remains a significant challenge, impacting patient recovery and satisfaction.1 Effective pain management is essential not only for patient comfort but also for promoting early mobilization, reducing pulmonary complications, and improving overall recovery.3
Conventional methods, such as intravenous opioids and patient-controlled analgesia (PCA), are frequently used but are limited by their systemic side effects, including respiratory depression, nausea, vomiting, and pruritus.4 In recent years, regional analgesia techniques have gained popularity as adjuncts or alternatives to systemic analgesics.5 Among these, thoracic paravertebral block (TPVB), erector spinae plane block (ESPB), and serratus anterior plane block (SAPB) have emerged as valuable adjuncts to multimodal analgesia strategies for thoracic surgery.6–8 By selectively blocking specific nerves, regional analgesia provide targeted pain relief while minimizing systemic opioid-related side effects such as nausea, vomiting, and respiratory depression.5
Single-injection nerve blocks have been demonstrated to provide effective analgesia for patients undergoing thoracoscopic surgery, but the duration of analgesia typically does not extend through the entire acute postoperative period. Consequently, clinical practices and trials involving continuous regional analgesia (CRA) are focused on improving pain control during the 12 to 24 hours and beyond. CRA involves the placement of a catheter near specific nerves and the administration of local anesthetics (LAs) over an extended period.9 This approach offers the advantage of prolonged analgesia, allowing for sustained pain control throughout the postoperative period.10
Among the various CRA techniques, two primary infusion strategies exist: continuous infusion (CI) and programmed intermittent bolus infusion (PIBI). CI delivers a constant flow of LAs, maintaining a stable concentration at the nerve site.11 PIBI, on the other hand, involves periodic bolus injections of LAs, followed by a period of no infusion.11 While both CI and PIBI have demonstrated efficacy in postoperative pain management, their relative advantages and disadvantages remain a subject of debate. PIBI may offer improved pain control during breakthrough pain episodes due to the bolus effect.12 Conversely, CI provides more stable analgesia and it may be simpler to administer and require less frequent adjustments compared to PIBI.12
Despite their theoretical advantages, the evidence regarding their comparative effectiveness specifically in the context of thoracoscopic surgery remains limited and inconclusive. Given the increasing use of thoracoscopic surgery and the ongoing debate regarding optimal CRA strategies, a comprehensive synthesis of the available evidence is crucial to inform clinical practice. This meta-analysis aims to systematically review and quantitatively synthesize the results of randomized controlled trials (RCTs) comparing PIBI with CI for peripheral nerve block following thoracoscopic surgery.
Methods
Our study complies with the PRISMA statement and the protocol was registered in the International Prospective Register of Systematic Reviews (CRD420251002276).
Inclusion and Exclusion Criteria
We included studies according to PICOS criteria: patients undergoing thoracoscopic surgery (P); the infusion mode of peripheral nerve block is PIBI (I); the infusion mode of peripheral nerve block is CI (C); postoperative pain scores and opiates consumption within 48 hours, total LAs consumption, blocked dermatomes, and number of people using additional analgesics (O); RCTs (S). These researches would be excluded: (1) the data cannot be used for statistical analysis; (2) the data was incomplete or duplicate; (3) unpublished studies, crossover randomized design studies.
Search Strategy
We searched PubMed, Embase, Web of Science, and the Cochrane Library from inception to March, 2025. The search strategy was based on the PICOS framework and the key words, including “intermittent”, “continuous”, and “thoracoscopic”. There was no limitation on sample size, surgical types and language. The full search strategy of PubMed as representative was shown in supplementary material 1.
Data Extraction
All titles, abstracts, and full texts were reviewed by two reviewers individually. Any disagreements were resolved by the third reviewer. The data extracted from each RCT included baseline demographic information, information regarding assessment of the risk of bias, and outcomes. The primary outcome was resting pain score at 6 h. The secondary outcomes included postoperative resting and movement pain score, morphine consumption, LAs consumption, number of people using additional analgesics within 48 h, and range of sensory blockade (the number of thoracic cutaneous segments).
Certainty of Evidence
Two independent reviewers assessed the risk of bias by using the Cochrane Collaboration’s tool, which included of sequence generation, allocation sequence concealment, blinding of participants and personal, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other potential sources bias.13 The GRADE methodology was used to evaluate the quality of evidence for each outcome.
Statistical Analysis
Statistical analysis was carried out in ReMan 5.4 software. The data expressed as median and inter-quartile range was converted to mean and standard deviations,14 and opiates consumption was converted to intravenous morphine equivalent (mg).15 For the number of people using additional analgesics within 48 h, the pooled relative risk (RR) and 95% confidential intervals (CIs) was calculated. For other outcomes, the mean differences (MD) and 95% CIs were evaluated. All analyses were initially carried out using a fixed-effects model. Heterogeneity was regarded as significant if I2 ≥ 50%, and the analyses were adopted with a random-effects model.16 Meanwhile, we performed sensitivity analysis to find the sources of heterogeneity. The funnel plot was used to exclude potential publication bias. The subgroup analysis was based on the types of nerves block. P value < 0.05 was considered as statistical significance throughout the study.
Results
The process of literature selection was shown in Figure 1. Seven studies enrolling 394 patients were included in the meta-analysis, between PIBI (n = 197 patients) and CI (n = 197 patients) groups.17–23 A summary of the characteristics, interventions, and outcomes of each study included in our analysis was shown in Table 1. The most common types of nerve block included thoracic paravertebral block (TPVB) and erector spinae plane block (ESPB).
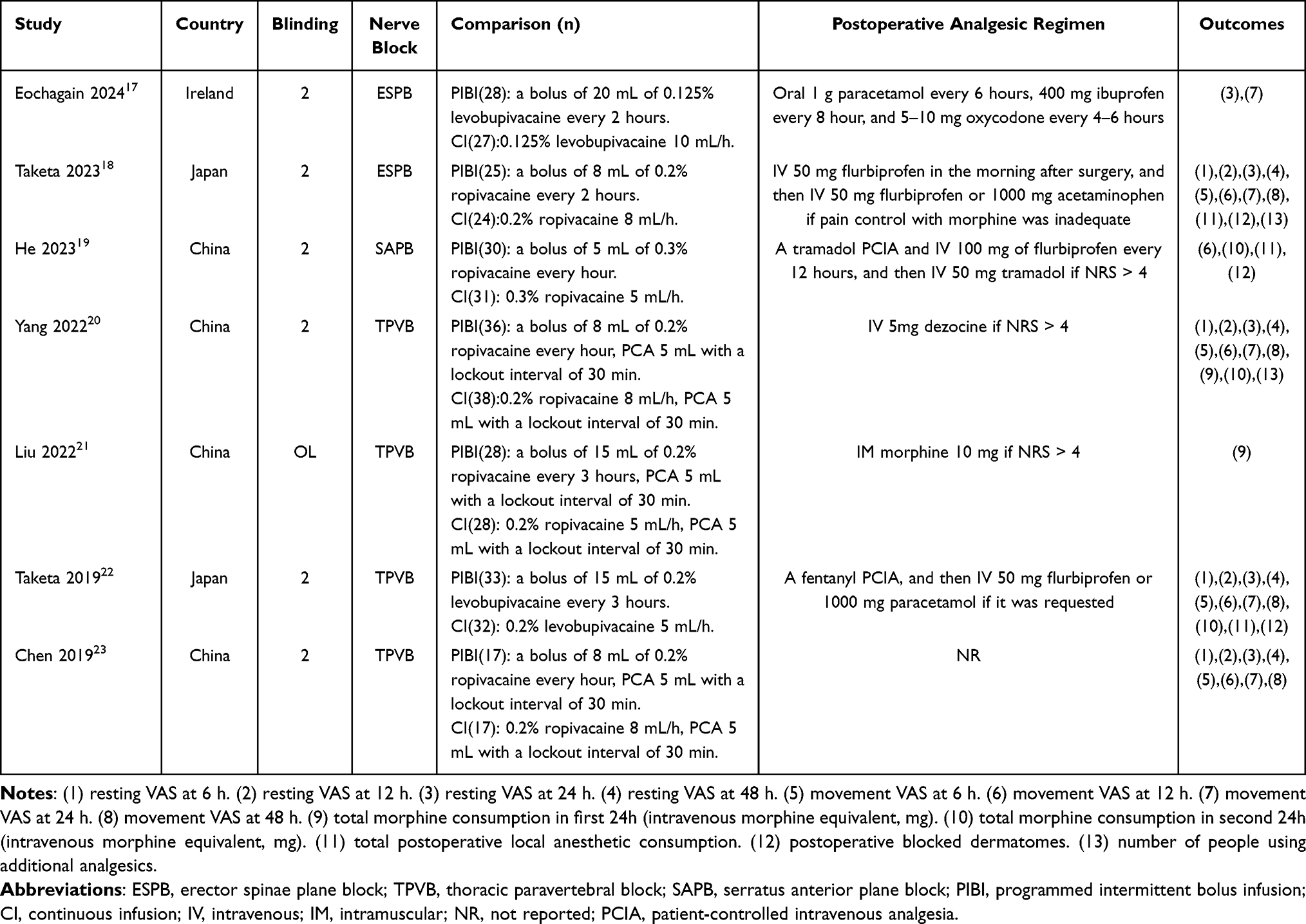 |
Table 1 Study Characteristics of Included Studies |
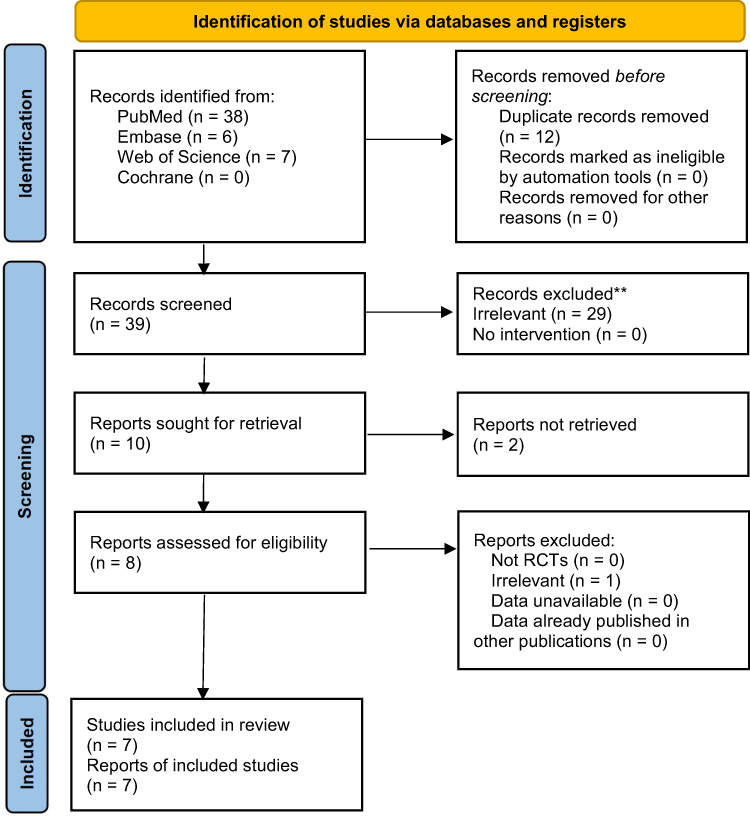 |
Figure 1 PRISMA flow diagram of study selection. PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89.24 |
Primary Outcome
The resting VAS at 6 h was reported in 4 RCTs. The risk of bias was shown in Figure 2. Figure 3 suggested a low publication bias. The pooled data did not suggest that PIBI was superior to CI (MD = −0.52, 95% CI: −1.23 to 0.20; I2 = 79%; Figure 4). The sensitivity analysis showed a similar result after deleting one RCT23 (MD = −0.00, 95% CI: −0.00 to 0.00; I2 = 49%; Figure 5). The subgroup analysis did not suggest that PIBI was superior to CI in TPVB group (MD = −0.44, 95% CI: −1.35 to 0.47; I2 = 81%; Figure 6). A summary of the evidence was presented in Table 2.
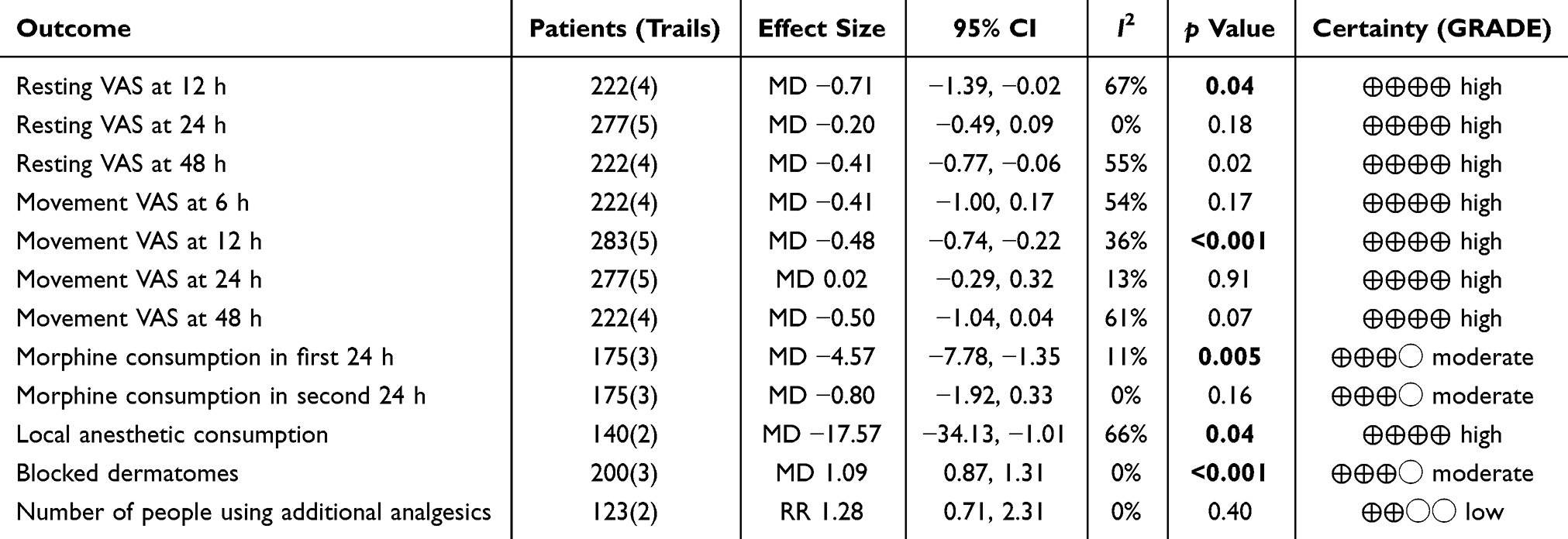 |
Table 2 Secondary Outcomes for PIBI Versus CI |
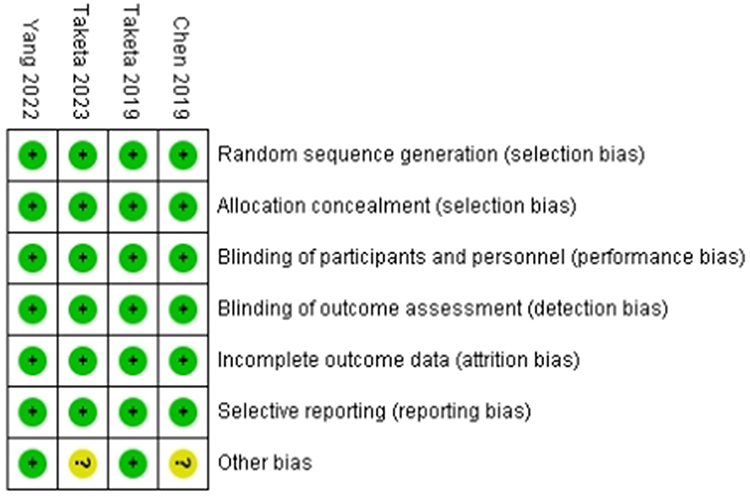 |
Figure 2 Risk of bias of resting VAS at 6 h (0–10 scale). |
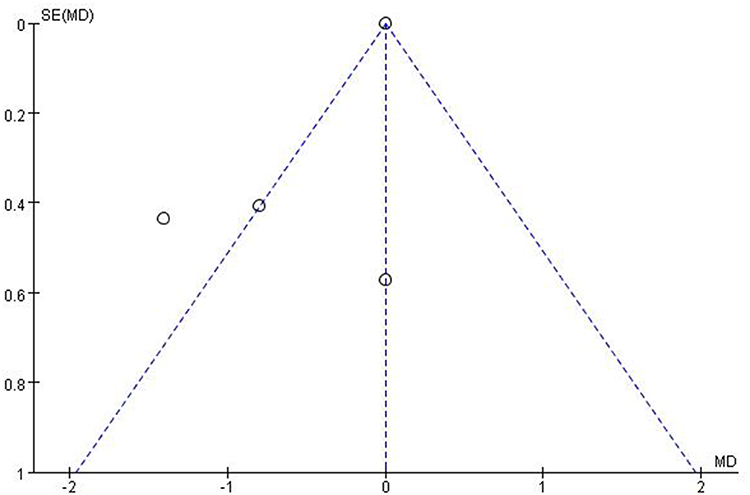 |
Figure 3 Funnel plot of resting VAS at 6 h (0–10 scale). |
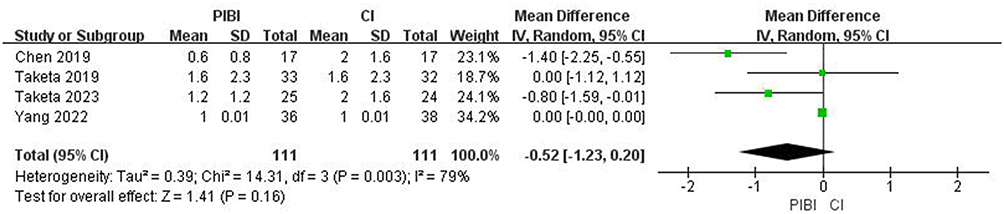 |
Figure 4 Forest plot of resting VAS at 6 h (0–10 scale). Abbreviations: PIBI, programmed intermittent bolus infusion; CI, continuous infusion. |
 |
Figure 5 Sensitivity analysis of resting VAS at 6 h (0–10 scale). Abbreviations: PIBI, programmed intermittent bolus infusion; CI, continuous infusion. |
 |
Figure 6 Subgroup analysis of resting VAS at 6 h (0–10 scale). Abbreviations: PIBI, programmed intermittent bolus infusion; CI, continuous infusion. |
Secondary Outcomes
PIBI was found to be statistically more effective than CI in resting VAS at 12 h (MD = −0.71, 95% CI: −1.39 to −0.02; I2 = 67%; Figure 7A), movement VAS at 12 h (MD = −0.48, 95% CI: −0.74 to −0.22; I2 = 36%; Figure 7B), and morphine consumption in first 24 h (MD = −4.57, 95% CI: −7.78 to −1.35; I2 = 11%; Figure 7C).
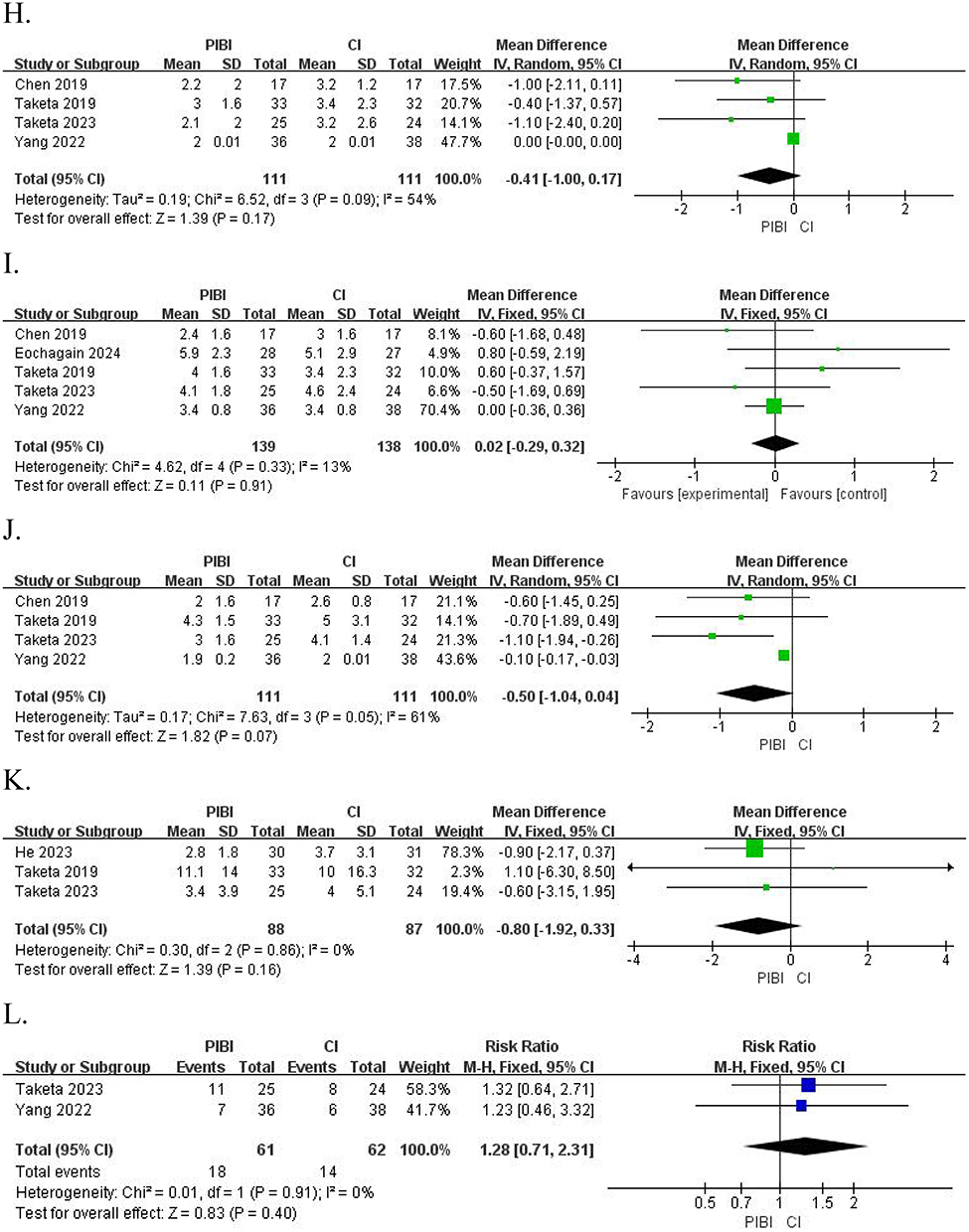
Figure 7 Continued. Figure 7 (A). Forest plot of resting VAS at 12 h (0–10 scale). (B) Forest plot of movement VAS at 12 h (0–10 scale). (C) Forest plot of total morphine consumption in first 24 h (intravenous morphine equivalent, mg). (D) Forest plot of total postoperative local anesthetic consumption. (E) Forest plot of postoperative blocked dermatomes. (F) Forest plot of resting VAS at 24 h (0–10 scale). (G). Forest plot of resting VAS at 48 h (0–10 scale). (H) Forest plot of movement VAS at 6 h (0–10 scale). (I). Forest plot of movement VAS at 24 h (0–10 scale). (J) Forest plot of movement VAS at 48 h (0–10 scale). (K) Forest plot of total morphine consumption in second 24h (intravenous morphine equivalent, mg). (L) Forest plot of number of people using additional analgesics. Abbreviations: PIBI, programmed intermittent bolus infusion; CI, continuous infusion.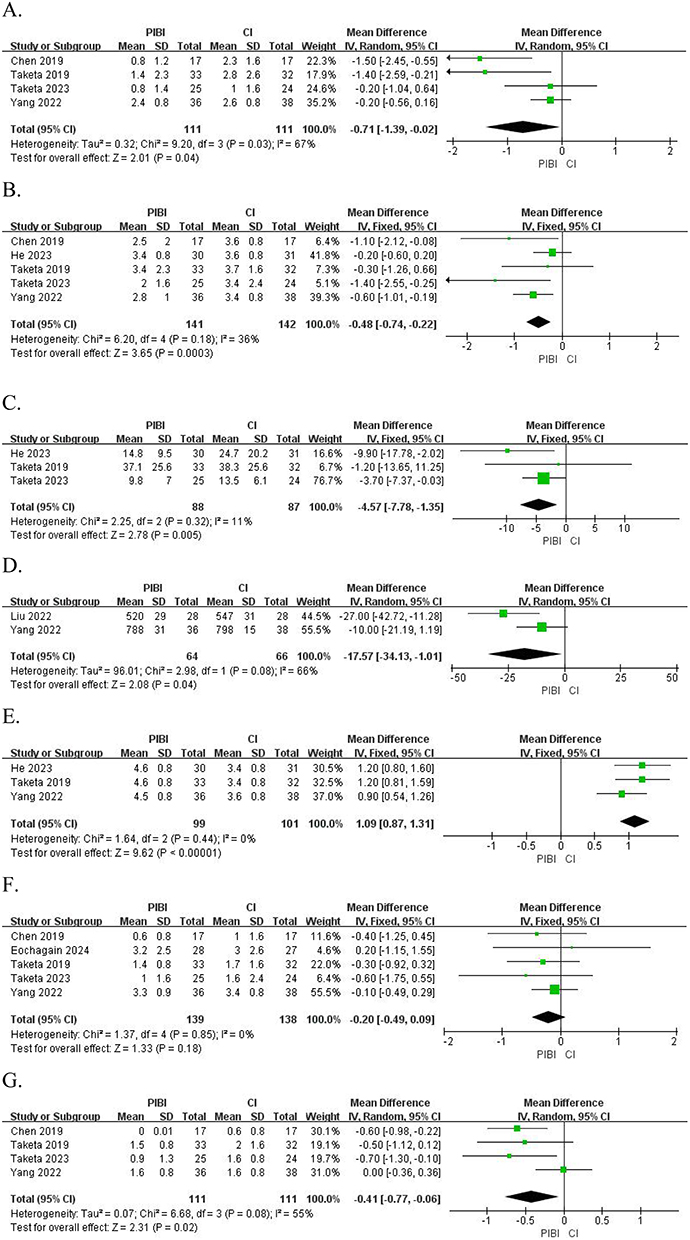
PIBI was found to have significantly lower LAs consumption (MD = −17.57, 95% CI: −34.13 to −1.01; I2 = 66%; Figure 7D) and wider range of sensory blockade than CI (MD = 1.09, 95% CI: 0.87 to −11.31; I2 = 0%; Figure 7E).
However, there were no significant difference between PIBI and CI in terms of the resting VAS at 24 h (MD = −0.20, 95% CI: −0.49 to 0.09; I2 = 0%; Figure 7F), resting VAS at 48 h (MD = −0.41, 95% CI: −0.77 to −0.06; I2 = 55; Figure 7G), movement VAS at 6 h (MD = −0.41, 95% CI: −1.00 to 0.17; I2 = 54; Figure 7H), movement VAS at 24 h (MD = 0.02, 95% CI: −0.29 to 0.32; I2 = 13%; Figure 7I), movement VAS at 48 h (MD = −0.50, 95% CI: −1.04 to 0.04; I2 = 61%; Figure 7J), morphine consumption in second 24 h (MD = −0.80, 95% CI: −1.92 to 0.33; I2 = 0%; Figure 7K), and number of people using additional analgesics (RR = 1.28, 95% CI: 0.71 to 2.31; I2 = 0%; Figure 7L).
Discussion
The findings of this meta-analysis provide compelling evidence for the role of PIBI in CRA following thoracic surgery. By synthesizing data from multiple studies, we have demonstrated that PIBI significantly reduces LAs consumption and provided a wider sensory blockade compared to CI. These results underscore the potential of PIBI as a more effective infusion mode for CRA following thoracoscopic surgery. Existing meta-analyses have focused on comparing CI and PIBI in labour analgesia and upper or lower limb surgeries.12,25 However, these analyses may not be directly applicable to thoracoscopic surgery due to differences in surgical technique, pain mechanisms, and patient characteristics. We consider that the different mechanisms between PIBI and CI is the main reason for the difference in results.
CRA have long been utilized to provide sustained analgesia by delivering LAs via catheters. Traditionally, CI has been the standard method, where a constant rate of LAs is administered to maintain a stable analgesic effect.23 The mechanism of CI is based on maintaining a stable and continuous blockade of nerve conduction.23 PIBI is a technique that involves the periodic administration of a bolus dose of LAs, allowing for rapid increases in LAs concentration at the nerve site during each bolus administration.23 This can result in a more extensive and even coverage of the nerve fibers, enhancing the overall efficacy of the block.23 Based on the above evidences, it is not difficult to explain why the sensory blockade range of PIBI is wider than CI.
Additionally, the popular CRA include TPVB, ESPB, and SAPB in thoracic surgery. The primary reasons for their popularity are the demonstrated effectiveness following a single injection, as well as the ease and safety of the ultrasound-guided puncture and catheterization techniques. For TPVB, the LAs diffuse within the thoracic paravertebral space, effectively blocking the ventral and dorsal rami of the spinal nerves, as well as the sympathetic chain.26 For ESPB, the LAs are injected into the fascial plane between the erector spinae muscle and the transverse processes of the vertebrae, allowing the LAs to spread and block the branches of the spinal nerves.27 For SAPB, the LAs is injected into the fascial plane either superficial or deep to the serratus anterior muscle, blocking the lateral cutaneous branches of the intercostal nerves, which innervate the anterolateral and lateral aspects of the thoracic wall.28 Based on the evidence from the previous paragraph, the paravertebral space and these fascial planes have a more significant obstruction to the diffusion of LAs for CI. Additionally, the difference of LAs consumption and postoperative pain scores show that the efficacy attenuation rate of PIBI is slightly better than that of CI.
By administering the LAs in intermittent doses, PIBI reduces the continuous systemic absorption of the drug.29 However, PIBI cannot avoid fluctuations in LAs concentration and may lead to side effects associated with high plasma levels of LAs.29 Conversely, CI allows for a more predictable pharmacodynamic profile, as the LAs concentration remains relatively constant.23 This can be advantageous in situations where a consistent level of analgesia is required over an extended period.23 However, CI can lead to the accumulation of LAs in the tissues, potentially increasing the risk of systemic toxicity and side effects.23 At present, the included studies do not reported any side effects and adverse reactions related to LAs, which only shows that these PIBI strategies are safe. Future studies should standardized strategy for PIBI to improve safety and reliability. Additionally, the movement VAS scores gradually increased between 24 and 48 hours, indicating that the severity of inflammatory pain was gradually intensifying, and regional analgesic techniques did not significantly alleviate inflammatory pain.
Limitations
Despite the promising results, this meta-analysis has several limitations that warrant consideration. First, the heterogeneity among studies, particularly in terms of catheter placement techniques, concentration and dosage of LAs, postoperative analgesia protocols, and patient populations, may have influenced the pooled estimates. Future studies should adopt standardized definitions for CRA and report outcomes in a uniform manner to improve comparability. Second, the majority of included studies were conducted in pulmonary surgery, limiting the generalizability of our findings to esophagus, mediastinum, and pleura surgeries. Further research is needed to evaluate the feasibility and effectiveness of two infusion strategies in diverse clinical environments. Another critical limitation is the lack of long-term follow-up data on chronic pain outcomes. Post-thoracotomy chronic pain is a significant complication, and CRA may play a role in its prevention. However, none of the included studies assessed the incidence of chronic pain beyond the immediate postoperative period. Future research should incorporate long-term follow-up to determine whether PIBI or CI reduces the risk of chronic pain and improves quality of life in thoracic surgery patients. Finally, the optimal concentration and dosage of LAs for PIBI remains uncertain. While existing studies have not reported the occurrence of side effects and adverse reactions related to LAs, concerns about safety may limit the clinical application of PIBI. Pharmacodynamic and pharmacokinetic evaluations are needed to determine the optimal infusion regimen for PIBI.
Conclusions
In conclusion, there was no significant clinical differences between PIBI and CI for resting VAS at 6 h. Meanwhile, the same results were observed in other pain scores, opioid consumptions, and number of people using additional analgesics. However, PIBI provided a lower LAs consumption and a wider sensory blockade compared to CI for CRA following thoracoscopic surgery. Further research is required to address the current gaps in the literature, including the need for standardized protocols, long-term follow-up, and pharmacodynamic and pharmacokinetic evaluations. As the field of regional anesthesia continues to evolve, CRA has the potential to become a cornerstone of postoperative pain management in thoracic surgery, ultimately enhancing patient care and recovery.
Funding
This work was supported by the Gansu Provincial Anesthesia and Brain Function Clinical Medical Research Center project (21JR7RA675) and the Gansu Provincial Health Industry project (GSWSKY2023-12).
Disclosure
The authors declare that they have no competing interests.
References
1. Wang L, Yang M, Meng W. Prevalence and characteristics of persistent postoperative pain after thoracic surgery: a systematic review and meta-analysis. Anesth Analg. 2023;137(1):48–57. doi:10.1213/ANE.0000000000006452
2. Matsuura Y, Ichinose J, Nakao M, et al. Outcomes of nodal upstaging comparing video-assisted thoracoscopic surgery versus open thoracotomy for lung cancer. Lung Cancer. 2021;152:78–85. doi:10.1016/j.lungcan.2020.12.017
3. Feray S, Lemoine A, Aveline C, et al. Pain management after thoracic surgery or chest trauma. Minerva Anestesiol. 2023;89(11):1022–1033. doi:10.23736/S0375-9393.23.17291-9
4. Yan H, Chen W, Chen Y, et al. Opioid-free versus opioid-based anesthesia on postoperative pain after thoracoscopic surgery: the use of intravenous and epidural esketamine. Anesth Analg. 2023;137(2):399–408. doi:10.1213/ANE.0000000000006547
5. Zhang Y, Liu M, He J, et al. Peripheral nerve block and cognitive impairment after thoracic surgery: a systematic review and meta-analysis. Minerva Anestesiol. 2024;90(5):417–426. doi:10.23736/S0375-9393.23.17669-3
6. D’Ercole F, Arora H, Kumar PA. Paravertebral block for thoracic surgery. J Cardiothorac Vasc Anesth. 2018;32(2):915–927. doi:10.1053/j.jvca.2017.10.003
7. Koo CH, Lee HT, Na HS, et al. Efficacy of erector spinae plane block for analgesia in thoracic surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2022;36(5):1387–1395. doi:10.1053/j.jvca.2021.06.029
8. Meng J, Zhao HY, Zhuo XJ, et al. Postoperative analgesic effects of serratus anterior plane block for thoracic and breast surgery: a meta-analysis of randomized controlled trials. Pain Physician. 2023;26(2):E51–E62. doi:10.36076/ppj.2023.26.E51
9. Chelly JE, Ghisi D, Fanelli A. Continuous peripheral nerve blocks in acute pain management. Br J Anaesth. 2010;105 Suppl 1:i86–96. doi:10.1093/bja/aeq322
10. Bingham AE, Fu R, Horn JL, et al. Continuous peripheral nerve block compared with single-injection peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Reg Anesth Pain Med. 2012;37(6):583–594. doi:10.1097/AAP.0b013e31826c351b
11. Eochagain AN, Moorthy A, O’Gara Á, et al. Ultrasound-guided, continuous erector spinae plane (ESP) block in minimally invasive thoracic surgery-comparing programmed intermittent bolus (PIB) vs continuous infusion on quality of recovery and postoperative respiratory function: a double-blinded randomised controlled trial. Trials. 2022;23(1):792. doi:10.1186/s13063-022-06726-7
12. Chong MA, Wang Y, Dhir S, et al. Programmed intermittent peripheral nerve local anesthetic bolus compared with continuous infusions for postoperative analgesia: a systematic review and meta-analysis. J Clin Anesth. 2017;42:69–76. doi:10.1016/j.jclinane.2017.08.018
13. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343(d5928):d5928–d5928. doi:10.1136/bmj.d5928
14. Luo D, Wan X, Liu J, et al. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
15. Nielsen S, Degenhardt L, Hoban B, et al. A synthesis of oral morphine equivalents (OME) for opioid utilisation studies. Pharmacoepidemiol Drug Saf. 2016;25(6):733–737. doi:10.1002/pds.3945
16. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
17. Eochagain AN, Moorthy A, Shaker J, et al. Programmed intermittent bolus versus continuous infusion for catheter-based erector spinae plane block on quality of recovery in thoracoscopic surgery: a single-centre randomised controlled trial. Br J Anaesth. 2024;133(4):874–881. doi:10.1016/j.bja.2024.05.041
18. Taketa Y, Takayanagi Y, Irisawa Y, et al. Programmed intermittent bolus infusion vs. continuous infusion for erector spinae plane block in video-assisted thoracoscopic surgery: a double-blinded randomised controlled trial. Eur J Anaesthesiol. 2023;40(2):130–137. doi:10.1097/EJA.0000000000001788
19. He K, Meng Y, Zhu Y, et al. Comparing continuous and intermittent infusion effects on serratus anterior plane blocks in video-assisted thoracoscopic surgery: a randomized clinical trial. J Pain Res. 2023;16:4015–4024. doi:10.2147/JPR.S431453
20. Yang L, Huang X, Cui Y, et al. Combined programmed intermittent bolus infusion with continuous infusion for the thoracic paravertebral block in patients undergoing thoracoscopic surgery: a prospective, randomized, and double-blinded study. Clin J Pain. 2022;38(6):410–417. doi:10.1097/AJP.0000000000001037
21. Liu W, Wang F, Luo T, et al. The effects of programmed intermittent paravertebral bolus infusion on postoperative analgesia in patients undergoing video-assisted thoracoscopic surgery: a prospective, randomized, controlled study. J Cardiothorac Vasc Anesth. 2022;36(9):3637–3644. doi:10.1053/j.jvca.2022.05.006
22. Taketa Y, Irisawa Y, Fujitani T. Programmed intermittent bolus infusion versus continuous infusion of 0.2% levobupivacaine after ultrasound-guided thoracic paravertebral block for video-assisted thoracoscopic surgery: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(4):272–278. doi:10.1097/EJA.0000000000000945
23. Chen L, Wu Y, Cai Y, et al. Comparison of programmed intermittent bolus infusion and continuous infusion for postoperative patient-controlled analgesia with thoracic paravertebral block catheter: a randomized, double-blind, controlled trial. Reg Anesth Pain Med. 2019;44(2):240–245. doi:10.1136/rapm-2018-000031
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89. doi:10.1186/s13643-021-01626-4
25. Ni F, Wu Z, Zhao P. Programmed intermittent epidural bolus in maintenance of epidural labor analgesia: a literature review. J Anesth. 2023;37(6):945–960. doi:10.1007/s00540-023-03253-w
26. Wu W, Wang D, Liu Y, et al. Comparison of ultrasound-guided subtransverse process interligamentary plane block with paravertebral block for postoperative analgesia in thoracic surgery: protocol for a randomised non-inferiority trial. BMJ Open. 2024;14(3):e082135. doi:10.1136/bmjopen-2023-082135
27. Cui Y, Wang Y, Yang J, et al. The effect of single-shot erector spinae plane block (ESPB) on opioid consumption for various surgeries: a meta-analysis of randomized controlled trials. J Pain Res. 2022;15:683–699. doi:10.2147/JPR.S346809
28. Finnerty DT, McMahon A, McNamara JR, et al. Comparing erector spinae plane block with serratus anterior plane block for minimally invasive thoracic surgery: a randomised clinical trial. Br J Anaesth. 2020;125(5):802–810. doi:10.1016/j.bja.2020.06.020
29. Hida K, Murata H, Ichinomiya T, et al. Effects of programmed intermittent thoracic paravertebral bolus of levobupivacaine on the spread of sensory block: a randomized, controlled, double-blind study. Reg Anesth Pain Med. 2019;44(3):326–332. doi:10.1136/rapm-2018-100021
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
Chen Y, Gao Y
Therapeutics and Clinical Risk Management 2023, 19:783-799
Published Date: 11 October 2023