Back to Journals » Journal of Inflammation Research » Volume 18
Prognostic Value of SIRI in Sepsis: A Retrospective Study and Machine Learning-Based Model Development
Authors Zhu Y, Wang Z ![]() , Li S, Xiao X, Liu Y, He J, Huang F
, Li S, Xiao X, Liu Y, He J, Huang F ![]() , Wang J
, Wang J ![]()
Received 6 June 2025
Accepted for publication 18 September 2025
Published 1 October 2025 Volume 2025:18 Pages 13609—13623
DOI https://doi.org/10.2147/JIR.S536139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Yilin Zhu,1,* Zhiyang Wang,2,* Shifeng Li,3,* Xin Xiao,3 Yujie Liu,3 Jiachen He,3 Fang Huang,3 Jun Wang3
1Department of Critical Care Medicine, Zhangjiagang Hospital Affiliated to Soochow University/The First People’s Hospital of Zhangjiagang City, Zhangjiagang, 215600, People’s Republic of China; 2Department of Emergency and Critical Care Medicine, The Second Affiliated Hospital of Soochow University, Suzhou, 215006, People’s Republic of China; 3Department of Critical Care Medicine, The First Affiliated Hospital of Soochow University, Suzhou, 215006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Wang, Department of Critical Care Medicine, The First Affiliated Hospital of Soochow University, No. 188 Shizi Street, Suzhou, 215006, People’s Republic of China, Email [email protected] Fang Huang, Department of Critical Care Medicine, The First Affiliated Hospital of Soochow University, No. 188 Shizi Street, Suzhou, 215006, People’s Republic of China, Email [email protected]
Background: In recent years, the Systemic Inflammation Response Index (SIRI) has demonstrated unique advantages in evaluating sepsis prognosis. This study aims to investigate the predictive value of SIRI for 28-day outcomes in sepsis patients, and develop and validate a prognostic model for 28-day mortality.
Methods: The demographic characteristics, disease severity, laboratory tests, treatments, and outcome measures were recorded from the adult sepsis patients. The restricted cubic splines and the ROC curve analysis were employed to evaluate the relationship and predictive capability of SIRI. Next, SIRI was categorized into tertiles, and univariate and multivariate Cox regression analyses were performed to assess its association with prognosis, supplemented by Kaplan-Meier (K-M) curves, and compare mortality differences. Patients from the First Affiliated Hospital of Soochow University were randomly allocated into training and internal validation sets at a 3:1 ratio, using the Boruta algorithm and LASSO regression and a prognostic model was constructed via logistic regression, while patients from the First People’s Hospital of Zhangjiagang City served as the external validation set. Then, the predictive performance, accuracy, and clinical utility of the model were validated using the ROC curve, Hosmer-Lemeshow test, calibration curve, and decision curve analysis (DCA).
Results: The 380 patients from the First Affiliated Hospital of Soochow University and 240 patients from the First People’s Hospital of Zhangjiagang City were enrolled for the present study. The restricted cubic spline analysis revealed a nonlinear increasing trend in mortality risk with rising SIRI levels. The ROC curve analysis demonstrated that SIRI has superior predictive capability than the APACHE II and SOFA scores. When SIRI was categorized into tertiles, both the univariate and multivariate Cox regression analyses identified SIRI as significantly associated to 28-day prognosis (p< 0.001). The K-M curves further confirmed that higher SIRI levels correlated to lower 28-day survival rates (p< 0.001). In the training set, the Boruta algorithm combined with LASSO regression selected six independent risk factors: blood urea nitrogen (BUN), age, phosphorus (P), lactate (Lac), mechanical ventilation (MV), and SIRI. These were incorporated into the predictive model through logistic regression analysis. The ROC curve analysis revealed that the model exhibited good predictive performance across the training set (AUC: 0.851), internal validation set (AUC: 0.908), and external validation set (AUC: 0.792). The calibration of the model was verified using the Hosmer-Lemeshow test and calibration curve, while DCA was performed to confirm its clinical utility.
Conclusion: SIRI is significantly correlated to the 28-day prognosis in sepsis patients, and has excellent predictive value for short-term outcomes. The prediction model that incorporated SIRI exhibited high prognostic accuracy.
Keywords: sepsis, systemic inflammation response index, prognosis, prediction model, nomogram
Introduction
Sepsis is a life-threatening acute organ dysfunction syndrome caused by a dysregulated host response to infection.1 This severe condition is associated to high mortality rates, and has far-reaching consequences for patient health, healthcare systems, and socioeconomic stability.2
Although various scoring systems such as SOFA and APACHE II are widely used in clinical practice, they have limitations in capturing dynamic immune-inflammatory changes. In recent years, immune-related composite indices have gained increasing attention for their simplicity and prognostic potential. Among them, the Systemic Inflammation Response Index (SIRI) has not yet been extensively studied in sepsis populations, and no predictive models based on SIRI have been developed to date.
The Systemic Inflammation Response Index (SIRI) is a composite biomarker that quantitatively consolidates the data of three immune cell populations via the following formula: SIRI = (absolute neutrophil count × absolute monocyte count) / absolute lymphocyte count. This index dynamically evaluates systemic inflammation and immune balance. Neutrophils, as key mediators of innate immunity, exert a profound influence on the magnitude of inflammatory responses, which is a process governed by its activation state.3 Monocytes, which are endowed with the dual capacity for phagocytic clearance and immune modulation, are well-documented participants in the pathogenesis of a spectrum of diseases.4,5 Lymphocytes, which are central orchestrators of adaptive immunity, assume indispensable roles in combating infections, managing autoimmune disorders, and combating malignant transformations that play pivotal roles in adaptive immunity, and are key regulators in infections, autoimmune diseases, and malignancies.6,7 Given the central roles of these immune cells in sepsis, SIRI provides a comprehensive reflection of both inflammation and immune suppression, which are hallmark features of sepsis pathophysiology.
By synthesizing changes in these three immune cell lineages, SIRI not only reflects the degree of inflammation and immune suppression, but also provides valuable reference for risk stratification and prognosis prediction in sepsis patients. Its clinical utility has been demonstrated in prognostic evaluation across multiple diseases.8–11 Compared to conventional inflammatory parameters, the innovation of SIRI lies in its incorporation of the interplay among three immune cell types, aligning well with sepsis pathophysiology.12–16 Consequently, SIRI offers unique advantages for prognostic assessment in sepsis patients. However, research on the application of SIRI in sepsis remains exploratory, and no SIRI-based prognostic prediction model for sepsis have been reported to date. The present study aims to investigate the evaluative and predictive value of SIRI for 28-day prognosis in sepsis patients. Furthermore, the present study embarks on the development of a predictive model that leverages machine learning algorithms. Both internal and external validations were conducted to rigorously evaluate its clinical relevance and practical utility.
Materials and Methods
Study Design and Participants
The present dual-center, retrospective observational study collected clinical data from 560 sepsis patients who were admitted to the intensive care unit (ICU) of the First Affiliated Hospital of Soochow University, and 404 sepsis patients who were admitted to the ICU of the First People’s Hospital of Zhangjiagang City between July 2022 and July 2024. All enrolled patients met the Sepsis-3.0 diagnostic criteria. Diagnostic criteria for sepsis: Sepsis diagnosis was established according to the 2016 International Guidelines for Management of Sepsis and Septic Shock (2016 Sepsis-3.0),1 Documented or suspected infection, and qSOFA OR ΔSOFA (an acute change in total SOFA score of ≥2 points from baseline).
Inclusion criteria: All adult patients (≥18 years old), who met the aforementioned diagnostic criteria for sepsis, were included for the present study.
Exclusion criteria (patients were excluded when they met any of the following criteria): (1) patients who were <18 years old; (2) patients diagnosed with malignancy or hematologic disorder; (3) patients with chronic viral infections (including hepatitis B virus); (4) patients with a history of organ transplantation; (5) pregnant or lactating patients; (6) patients with autoimmune diseases or patients who recently received immunosuppressive therapy; (7) patients with a recent history of radiotherapy or chemotherapy.
Elimination criteria: (1) hospitalization duration of <24 hours; (2) missing critical laboratory data (including complete blood count); (3) unavailable follow-up outcomes.
According to the predefined inclusion and exclusion criteria, 102 patients were excluded from the First Affiliated Hospital of Soochow University and 74 patients were excluded from the First People’s Hospital of Zhangjiagang City. At the First Affiliated Hospital of Soochow University, 102 patients were excluded due to the following reasons: 48 patients had pre-existing malignancies or hematologic disorders, 35 patients had chronic viral infections (including hepatitis B virus), five patients were organ transplant recipients, three patients were pregnant or lactating women, seven patients had autoimmune diseases or recent immunosuppressive therapy, and four patients recently underwent radiotherapy or chemotherapy. In addition, the following patients were further excluded due to the following: 30 patients had a hospitalization duration of <24 hours, 34 patients had missing critical laboratory data (including complete blood count), and 14 patients had unavailable follow-up outcomes. At the First People’s Hospital of Zhangjiagang City, 74 patients were excluded due to the following reasons: 28 patients had pre-existing malignancies or hematologic disorders, 31 patients had chronic viral infections, three patients were organ transplant recipients, five patients were pregnant or lactating women, five patients had autoimmune diseases or recent immunosuppressive therapy, and two patients recently underwent radiotherapy or chemotherapy. In addition, the following patients were further excluded due to the following: 33 patients had a hospitalization duration of <24 hours, 38 patients had missing essential laboratory data, and 19 patients had unavailable follow-up outcomes. After rigorous screening, 380 eligible patients from the First Affiliated Hospital of Soochow University and 240 eligible patients from the First People’s Hospital of Zhangjiagang City were finally included for the statistical analysis. The present study was approved by the ethics committees of the two centers (Ethics approval nos: 2025221 and ZJGYYLL-LW-2025-03-014).
Data Extraction and Preprocessing
The following variables were considered for the present study: (1) demographic characteristics: age, gender, and body mass index (BMI); (2) underlying comorbidities: hypertension (HTN), diabetes mellitus (DM), coronary heart disease (CHD), chronic obstructive pulmonary disease (COPD), chronic liver disease (CLD), chronic kidney disease (CKD), and stroke; (3) disease severity scores: Acute Physiology and Chronic Health Evaluation II (APACHE II) score and Sequential Organ Failure Assessment (SOFA) score (within 24 hours of admission); (4) baseline vital signs on admission: heart rate (HR), respiratory rate (RR), systolic blood pressure (SBP), and diastolic blood pressure (DBP); (5) laboratory parameters (worst values within 48 hours of admission): (a) blood gas analysis: PH, partial pressure of carbon dioxide (PaCO2), oxygenation index (PaO2/FiO2), and lactate; (b) complete blood count: white blood cell count (WBC), lymphocyte count (LYM), monocyte count (MON), neutrophil count (NE), hemoglobin (HB), red blood cell distribution width (RDW), and platelet count (PLT); (c) coagulation profile: prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB), and D-dimer; (d) biochemical markers: total bilirubin (TBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (ALB), blood urea nitrogen (BUN), serum creatinine (SCr), blood glucose (GLU), total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), lactate dehydrogenase (LDH), potassium (K), sodium (Na), chloride (Cl), calcium (Ca), and phosphorus (P); (6) treatment modalities: continuous renal replacement therapy (CRRT) and mechanical ventilation (MV); (7) clinical outcome: mortality at 28 days (with 28-day mortality as the primary clinical endpoint).
Statistical Analysis
Since the present study was retrospective in nature, no sample size calculations were performed. Variables with a missing data rates that exceeded 30% were excluded from the analysis, while for variables with missing data rates below 30%, multiple imputation was applied. Categorical variables were presented in percentage (%). Continuous variables with non-normal distribution were presented in median and quartile, while variables with normal distribution were presented in mean and standard deviation (mean [S.E.]). Statistical comparisons between categorical variables were conducted using chi-square test, and comparisons between two groups of continuous variables were conducted using t-test or nonparametric test.
In the training cohort, feature selection was performed using the least absolute shrinkage and selection operator (LASSO) regression and Boruta analysis. Statistically significant variables (p<0.05) were identified as independent risk factors, and included in the final logistic regression model. Then, a corresponding nomogram was plotted. Model prediction accuracy was assessed using the area under the receiver operating characteristic curve (AUC), and the consistency between the predicted and actual values was evaluated via the calibration curve. Then, the clinical benefits were analyzed using the decision curve. Data description was performed using the Tableone software package, LASSO regression analysis was performed using glmnet, and Boruta analysis was performed using boruta. The nomogram and calibration curve were plotted using rms, and the receiver operating characteristic (ROC) curve was plotted using pROC. All statistical analyses were performed using R 4.3.0 (https://www.r-project.org). A two-sided p-value of <0.05 was considered statistically significant. The present study was designed and analyzed according to the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) statement.
Results
Characteristics of the study Cohort
Based on the inclusion and exclusion criteria, 380 sepsis patients from the First Affiliated Hospital of Soochow University and 240 sepsis patients from the First People’s Hospital of Zhangjiagang City were enrolled for the statistical analysis. Sepsis patients from the First Affiliated Hospital of Soochow University were divided into two groups based on the 28-day prognostic outcomes: survival group (259 patients) and death group (121 patients). At a 3:1 ratio, sepsis patients from the First Affiliated Hospital of Soochow University were randomly allocated into two sets: training set and internal validation set. There were no statistically significant differences in baseline characteristics between the two groups (Table 1). Sepsis patients from the First People’s Hospital of Zhangjiagang City served as the external validation set. A flowchart is presented in Figure 1.
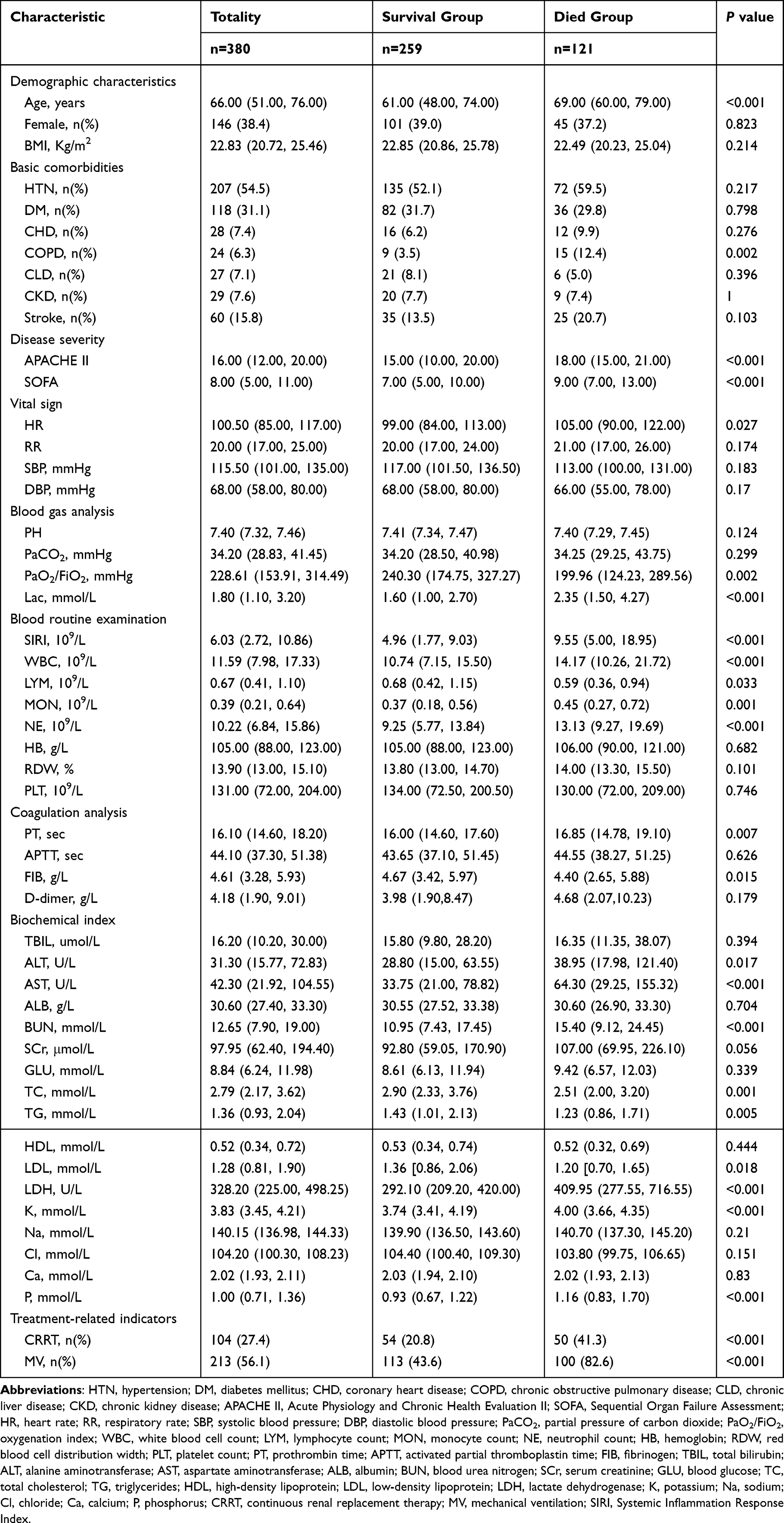 |
Table 1 Comparison of Baseline Characteristics Between Survival and Non-Survival Groups |
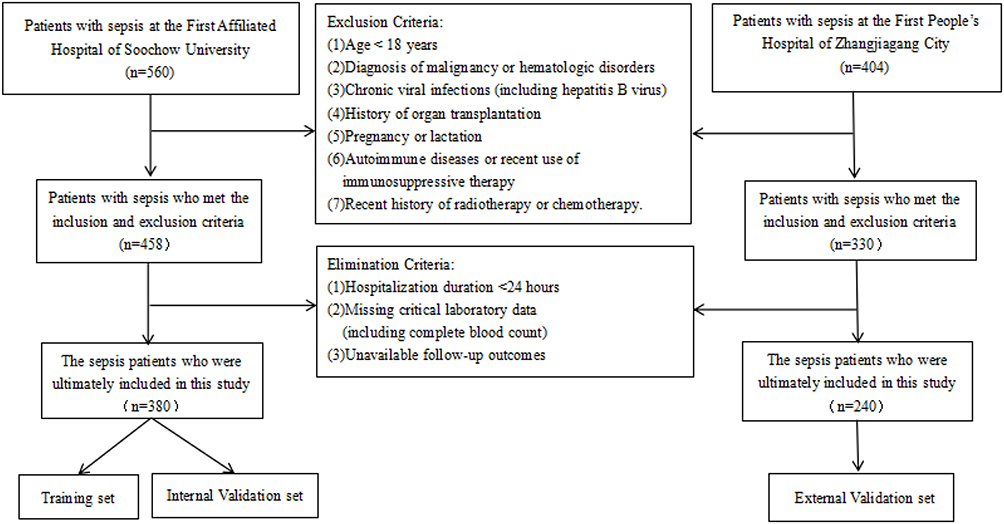 |
Figure 1 The study flowchart. |
The Relationship Between SIRI and Prognosis of Sepsis
The restricted cubic spline analysis (Figure 2) revealed a non-linear increasing trend in mortality risk with elevated SIRI levels in sepsis patients.
 |
Figure 2 The relationship between SIRI and mortality in sepsis patients. The solid line represents the hazard ratio, and the shaded area represents the 95% confidence interval (CI). The vertical axis indicates the mortality risk of sepsis patients. |
Predictive Value of SIRI for the Prognosis of Sepsis
The ROC curve analysis revealed that the AUC values for the SIRI, APACHE II score, and SOFA score were 0.732 (95% CI: 0.680–0.785), 0.647 (95% CI: 0.592–0.702), and 0.647 (95% CI: 0.588–0.706), respectively. Notably, SIRI had a significantly higher predictive accuracy, when compared to both the APACHE II (p=0.026) and SOFA (p=0.037) scores, indicating its superior prognostic performance (Figure 3).
 |
Figure 3 Comparison of areas in the ROC curve for the SIRI, APACHE II score, and SOFA score. |
Correlation Between SIRI Levels and Clinical Outcomes in Sepsis
Patients were stratified into three groups according to SIRI tertiles: Q1 group (SIRI <33%, SIRI <3.72 × 109/L; n = 126), Q2 group (33% ≤ SIRI < 67%, 3.72 × 109/L ≤ SIRI < 9.04 × 109/L; n = 128), and Q3 group (SIRI ≥ 67%, SIRI ≥ 9.04 × 109/L; n = 126). The baseline characteristics across these three groups are presented in Supplementary Table 1.
In Model 1, the mortality risk of sepsis patients significantly increased with the increase in SIRI levels. After progressively adjusting for covariates in Model 2 and Model 3, SIRI remained as an independent predictor of mortality, with a persistent dose-dependent increase in death risk (all, p<0.05) (Table 2).
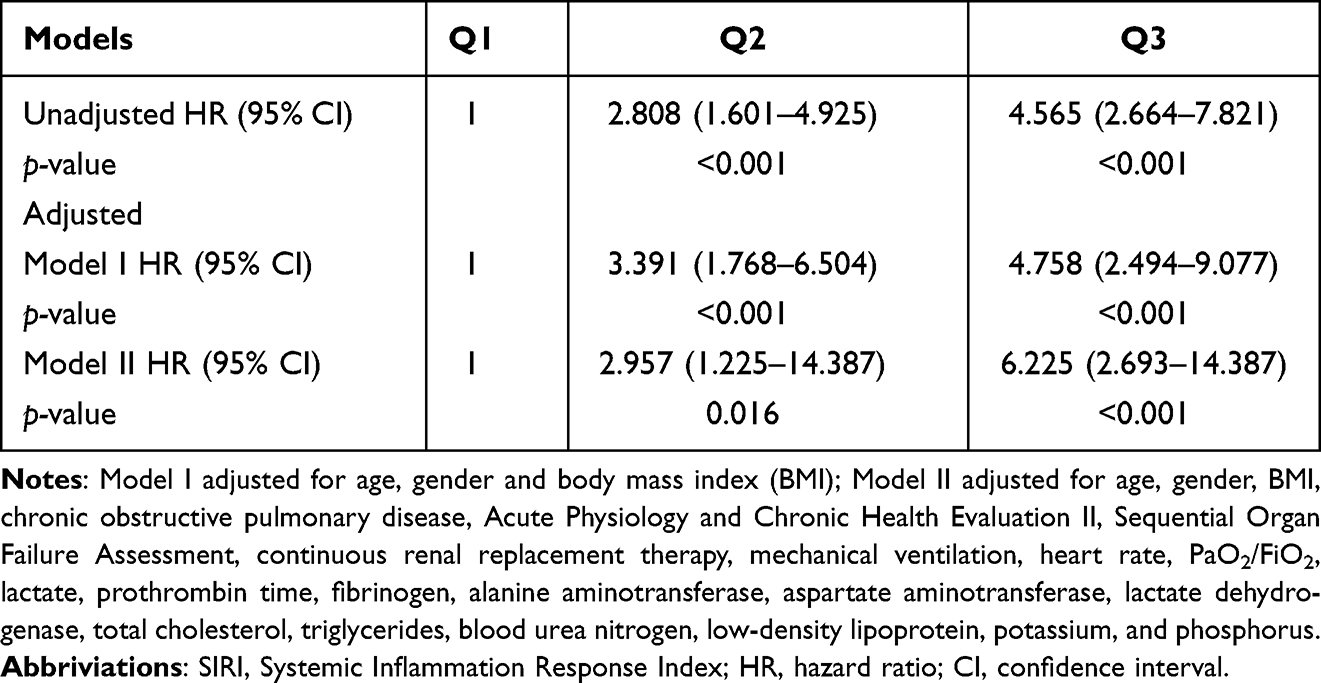 |
Table 2 Univariate and Multivariate Regression Analyses of the Association Between SIRI and 28-Day Mortality in Sepsis Patients |
The Kaplan-Meier (K-M) survival analysis (Figure 4) further revealed that patients in higher SIRI tertiles had progressively elevated 28-day in-hospital mortality (p<0.001), confirming the graded association between SIRI levels and poor clinical outcomes.
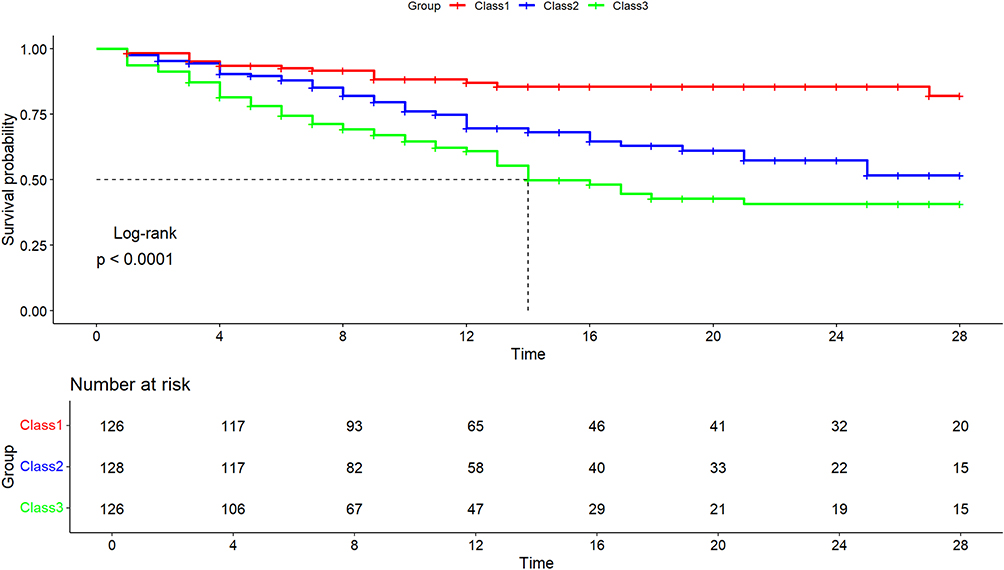 |
Figure 4 Kaplan–Meier survival curve for 28-day mortality according to different groups of SIRI (Class 1 = Q1 (n = 126), Class 2 = Q2 (n = 128), and Class 3 = Q3 (n = 126)). |
Selection of Predictive Variables, Model Construction, and Evaluation of the Predictive Model
Selection of Predictive Variables and Model Construction
Sepsis patients from the First Affiliated Hospital of Soochow University were randomly allocated into two sets at a 3:1 ratio: training set (n=284) and internal validation set (n=96). Sepsis patients from the First People’s Hospital of Zhangjiagang City served as the external validation set. In the training set, the Boruta algorithm initially identified 12 significant predictive variables: TC, AST, FIB, BUN, Age, K, WBC, LDH, P, Lac, MV and SIRI (Figure 5).
 |
Figure 5 Feature selection based on the Boruta algorithm. Green, clinically significant features retained in the final model to enhance predictive performance; Red, statistically insignificant features excluded from further consideration; Yellow, features with borderline importance requiring additional investigation; Blue, shadow features (permuted variables) used for comparative benchmarking, but not included in model training. |
In order to minimize model bias, the LASSO regression further refined the selection to eight key factors: BUN, Age, K, Lac, WBC, P, MV and SIRI (Supplementary Figure 1). Then, these eight variables were analyzed using stepwise logistic regression, finally identifying six independent risk factors: BUN, Age, P, Lac, MV and SIRI. The multivariable logistic regression that incorporated these six factors (Figure 6) was used to construct the final prediction model, which was visually represented in a nomogram (Figure 7).
 |
Figure 6 Multivariable logistic regression analysis of 28-day mortality in sepsis patients. |
 |
Figure 7 Nomogram for predicting the 28-day mortality in sepsis patients. |
Predictive Performance, Accuracy, and Clinical Utility of the Model
The ROC curve analysis revealed that the model had an AUC of 0.851 (95% CI: 0.804–0.898), 0.908 (95% CI: 0.850–0.967), and 0.792 (95% CI: 0.732–0.852) for predicting 28-day mortality in sepsis patients in the training set, internal validation set, and external validation set, respectively, indicating its robust predictive value for short-term prognosis in sepsis patients (Figure 8). The Hosmer-Lemeshow test revealed an excellent agreement between the predicted 28-day mortality and actual observed outcomes of the model (Figure 9)(training cohort: X2 = 5.5997, degrees of freedom = 8, p = 0.6920 > 0.05; internal validation cohort: X2 = 5.9355, degrees of freedom = 8, p = 0.6545 > 0.05; external validation cohort: X2 = 6.4204, degrees of freedom = 8, p = 0.6002 > 0.05). The decision curve analysis (DCA) revealed that this prediction model provided greater net benefit, when compared to both the APACHE II and SOFA scores, confirming its clinical utility (Figure 10).
 |
Figure 8 ROC curves for the prediction model for 28-day mortality in sepsis across the training set, internal validation set, and external validation set. |
 |
Figure 9 Calibration curves for the prediction model, APACHE II score and SOFA score for the 28-day mortality prediction for sepsis across the training set (A), internal validation set (B), and external validation set (C). |
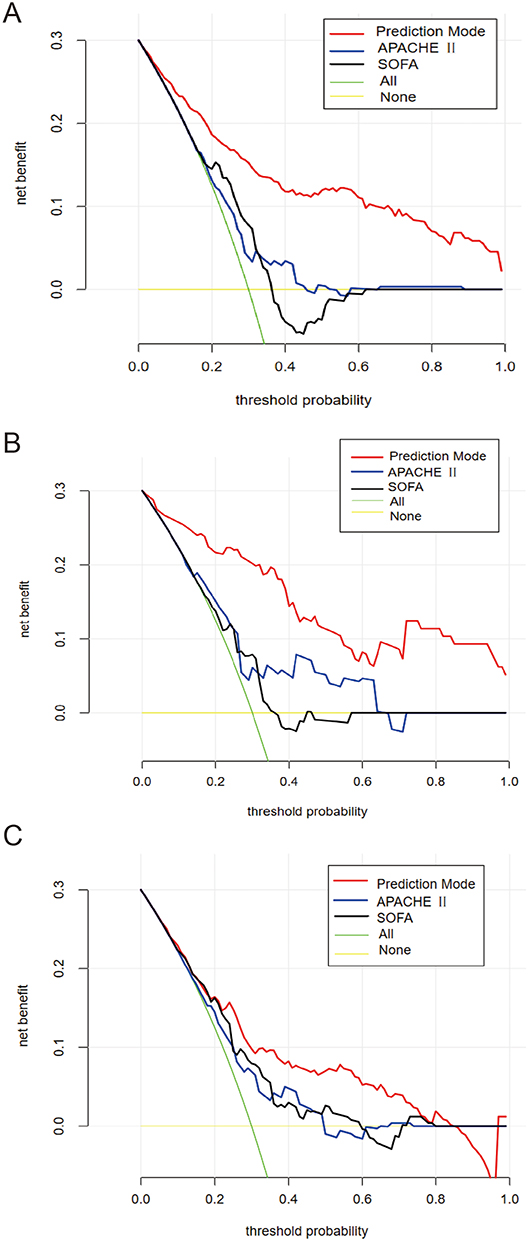 |
Figure 10 DCA of the prediction model, APACHE II score, and SOFA score for the 28-day mortality prediction for sepsis across the training set (A), internal validation set (B), and external validation set (C). |
Discussion
Despite the advances in medical technology and widespread use of antibiotics, sepsis remains a the leading cause of morbidity and mortality worldwide. In 2017, there were approximately 48.90 million sepsis cases globally, resulting in 11 million deaths,17 A meta-analysis conducted by Michael et al reported an in-hospital 28-day mortality rate of 24.40% for sepsis patients.18 Given these staggering statistics, the early identification and prognostic assessment of sepsis remains as critical research priorities. The present study revealed that SIRI has a strong correlation with 28-day mortality in sepsis patients, and possesses high predictive value. Furthermore, the SIRI-based prediction model developed in the present study exhibited a robust prognostic performance.
Although the APACHE II and SOFA scores are widely used in emergency departments and ICUs to assess disease severity and predict outcomes in critically ill patients, these have notable limitations.19 The APACHE II score, which is based on 12 physiological parameters measured within the first 24 hours of admission, is cumbersome to calculate, and lacks real-time applicability. The SOFA score focuses primarily on organ dysfunction, but fails to incorporate key factors, such as age and comorbidities, and is relatively insensitive to dynamic changes in immune-inflammatory responses. In contrast, SIRI offers distinct advantages in reflecting inflammatory and immune status. The present SIRI-based prediction model incorporated multidimensional factors, enabling the early and effective prognostic assessment of sepsis patients. Notably, SIRI can be calculated in real-time using routine complete blood count data, making it simple, cost-effective, and easily implementable in clinical practice, particularly in resource-limited settings. Furthermore, recent studies have extended the application of SIRI to early identification and ICU outcome prediction in conditions, such as pancreatitis, cancer, and heart failure,13,14,20–22 highlighting its broad clinical utility.
Given the multifactorial nature of sepsis progression, identifying key risk factors is essential. Using the Boruta algorithm, LASSO regression, and logistic regression analysis, six independent risk factors for 28-day mortality were identified in sepsis patients: BUN, Age, P, Lac, MV and SIRI. These factors were incorporated into the present prediction model, which quantifies the individual contributions to outcomes. The model exhibited excellent predictive performance upon internal and external validation. Previous studies support the present findings: advanced age has been independently associated to sepsis mortality,23 serum lactate is a well-established prognostic marker in sepsis,24 elevated BUN levels are linked to acute kidney injury in sepsis patients,25 mechanical ventilation is required in over 20% of sepsis cases, reflecting disease severity,26 and dysregulated phosphorus metabolism (both hypophosphatemia and hyperphosphatemia) correlates to disease severity and ICU mortality.27–29 These consistent findings underscore the reliability of the present SIRI-based prediction model.
In summary, the present study confirms that SIRI is a simple yet reliable biomarker for assessing sepsis severity, and guiding risk stratification and prognostic evaluation. The elevated SIRI values indicated a state of severe inflammation and immunosuppression, which was associated to increased risk of organ dysfunction and mortality. Thus, SIRI may facilitate the early identification of high-risk patients, informing timely interventions, such as anti-inflammatory therapy, immunomodulation, and organ support, in order to improve outcomes. However, the present study has limitations. First, merely SIRI values at admission were analyzed without dynamic monitoring, which might have provided more accurate prognostic information. Second, the 28-day follow-up period was relatively short. Extended observations (such as 60 or 90 days) could better elucidate the long-term predictive value of SIRI. Therefore, future multi-center prospective studies with a larger sample size are needed to further validate the clinical utility of SIRI. In conclusion, SIRI represents as a promising inflammatory and immune marker for sepsis prognosis. Future research should focus in optimizing its clinical application strategies, in order to enhance precision in prognostic assessment and therapeutic decision-making for sepsis patients.
Conclusion
In conclusion, sepsis remains as a major global health challenge with high morbidity and mortality rates. The present study highlights SIRI as a simple and reliable biomarker for assessing sepsis severity and predicting 28-day mortality. Compared to traditional scores, such as APACHE II and SOFA, SIRI offers advantages in real-time applicability, and reflects the inflammatory and immune status. Through rigorous analyses, six independent risk factors were identified for sepsis mortality, which includes SIRI. Then, a prediction model was developed, which exhibited excellent performance. However, there were limitations in the present study, such as the single-time-point SIRI measurement, and relatively short follow-up period. Future research should focus on dynamic SIRI monitoring, longer-term outcomes, and large-scale multi-center studies, in order to further validate and optimize its clinical application. Overall, SIRI holds great potential as an inflammatory and immune marker for sepsis prognosis, serving as a promising approach to improve early risk stratification, and guide timely interventions to enhance patient outcomes.
Data Sharing Statement
The datasets presented in the study were obtained from the electronic medical record system of the First Affiliated Hospital of Soochow University and the First People’s Hospital of Zhangjiagang City. The datasets generated during and/or analysed during the current study are available from the corresponding author and the first author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University (Approval No. [2025] Lunshenpi No. 221) and the First People’s Hospital of Zhangjiagang City (Approval No: ZJGYYLL-LW-2025-03-014). As this was a retrospective, non-interventional study involving only the review of existing medical records, the requirement for obtaining individual patient informed consent was waived by the Ethics Committee. The waiver was granted on the grounds that the study posed no additional risk to the patients and could not practicably be carried out without the waiver. All patient data were anonymized to ensure confidentiality. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We would like to thank hospital staff, patients, and medical staff who cared for patients. We also thank Medjaden Inc. for scientific editing and proofreading of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Science Foundation of Jiangsu Commission of Health (M2022086), Suzhou Basic Research Project (SSD2024053) and Natural Science Foundation of Jiangsu Province (BK20241798).
Disclosure
The authors declare no competing interests in this work.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801–10.
2. Fleischmann-Struzek C, Mellhammar L, Rose N, et al. Incidence and mortality of hospital- and ICU-treated sepsis: results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. 2020;46:1552–1562. doi:10.1007/s00134-020-06151-x
3. Bellomo R, Kellum JA, Ronco C, et al. Acute kidney injury in sepsis. Intensive Care Med. 2017;43:816–828. doi:10.1007/s00134-017-4755-7
4. Cato LD, Wearn CM, Bishop JRB, et al. Platelet count: a predictor of sepsis and mortality in severe burns. Burns. 2018;44:288–297. doi:10.1016/j.burns.2017.08.015
5. Lai H, Wu G, Zhong Y, et al. Red blood cell distribution width improves the prediction of 28-day mortality for patients with sepsis-induced acute kidney injury: a retrospective analysis from MIMIC-IV database using propensity score matching. J Intensive Care Med. 2023;3:275–282. doi:10.1016/j.jointm.2023.02.005
6. Jia L, Li C, Bi X, et al. Prognostic value of systemic immune-inflammation index among critically Ill patients with acute kidney injury: a retrospective cohort study. J Clin Med. 2022;12:11. doi:10.3390/jcm12010011
7. Seyit M, Avci E, Nar R, et al. Neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio and platelet to lymphocyte ratio to predict the severity of COVID-19. Am J Emerg Med. 2021;40:110–114. doi:10.1016/j.ajem.2020.11.058
8. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122:2158–2167. doi:10.1002/cncr.30057
9. Chen J, Wei H. Immune intervention in sepsis. Front Pharmacol. 2021;12:718089.
10. Boomer JS, To K, Chang KC. Immunosuppression in patients who die of sepsis and multiple organ failure. JAMA. 2011;306(23):2594–2605. doi:10.1001/jama.2011.1829
11. Nedeva C, Neff LS, Broughton P, Bradshaw AD, DeLeon-Pennell KY. Inflammation and cell death of the innate and adaptive immune system during sepsis. Biomolecules. 2021;12:11. doi:10.3390/biom12010011
12. Huang M, Cai S, Su J. The pathogenesis of sepsis and potential therapeutic targets. Int J Mol Sci. 2019;21:20. doi:10.3390/ijms21010020
13. Zhou Y, Zhang Y, Cui M, et al. Prognostic value of the systemic inflammation response index in patients with acute ischemic stroke. Brain Behav. 2022;12:e2619.
14. Wang X, Ni Q, Wang J, et al. Systemic inflammation response index is a promising prognostic marker in elderly patients with heart failure: a retrospective cohort study. Front Cardiovasc Med. 2022;9:871031.
15. Li Q, Ma X, Shao Q, et al. Prognostic impact of multiple lymphocyte-based inflammatory indices in acute coronary syndrome patients. Front Cardiovasc Med. 2022;9:811790.
16. Chao B, Ju X, Zhang L, et al. A novel prognostic marker Systemic Inflammation Response Index (SIRI) for operable cervical cancer patients. Front Oncol. 2020;10:10. doi:10.3389/fonc.2020.00010
17. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395:200–211. doi:10.1016/S0140-6736(19)32989-7
18. Bauer M, Gerlach H, Vogelmann T, et al. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019— results from a systematic review and meta-analysis. Critical Care. 2020;24:24. doi:10.1186/s13054-019-2723-z
19. Yu S, Leung S, Heo M. Comparison of risk prediction scoring systems for ward patients: a retrospective nested case-control study. Crit Care. 2014;18(3):R132. doi:10.1186/cc13947
20. Chen L, Kong X, Wang Z, et al. Pretreatment systemic inflammation response index in patients with breast cancer treated with neoadjuvant chemotherapy as a useful prognostic indicator. Cancer Manag Res. 2020;Volume 12:1543–1567. doi:10.2147/CMAR.S235519
21. Jin Z, Hao D, Song Y, et al. Systemic inflammatory response index as an independent risk factor for ischemic stroke in patients with rheumatoid arthritis: a retrospective study based on propensity score matching. Clin Rheumatol. 2021;40(10):3919–3927. doi:10.1007/s10067-021-05762-z
22. He W-Z, Jiang C, Liu -L-L, et al. Association of body composition with survival and inflammatory responses in patients with non-metastatic nasopharyngeal cancer. Oral Oncol. 2020;108:104771. doi:10.1016/j.oraloncology.2020.104771
23. Weng L, Zeng X-Y, Yin P, et al. Sepsis-related mortality in China: a descriptive analysis. Intensive Care Med. 2018;44:1071–1080. doi:10.1007/s00134-018-5203-z
24. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49:e1063–e1143. doi:10.1097/CCM.0000000000005337
25. Harazim M, Tan K, Nalos M, et al. Blood urea nitrogen - independent marker of mortality in sepsis. Biomedical Papers. 2023;167(1):24–29. doi:10.5507/bp.2022.015
26. Dhital R, Basnet S, Poudel DR. Predictors and outcome of invasive mechanical ventilation in hospitalized patients with sepsis: data from National Inpatient Sample. J Community Hosp Intern Med Perspect. 2018;8:49–52. doi:10.1080/20009666.2018.1450592
27. Fang Y, Zhang Y, Zhang X. Serum phosphate levels and the development of sepsis associated acute kidney injury: evidence from two independent databases. Front Med. 2024;11:1367064.
28. Al Harbi SA, Al-Dorzi HM, Al Meshari AM, et al. Association between phosphate disturbances and mortality among critically ill patients with sepsis or septic shock. BMC Pharmacol Toxicol. 2021;22:22. doi:10.1186/s40360-021-00492-z
29. S R, H A, R S, et al. Severe hypophosphatemia in sepsis as a mortality predictor. Ann Clin Lab Sci. 2006;36(1):67–72.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
A Nomogram Based on SEER Database for Predicting Prognosis in Patients with Mucinous Ovarian Cancer: A Real-World Study
Zhang K, Feng S, Ge Y, Ding B, Shen Y
International Journal of Women's Health 2022, 14:931-943
Published Date: 26 July 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022
Development and Validation of a Novel Nomogram Integrated with Hypoxic and Lactate Metabolic Characteristics for Prognosis Prediction in Hepatocellular Carcinoma
Qiu X, Dong L, Wang K, Zhong X, Xu H, Xu S, Guo H, Wei X, Chen W, Xu X
Journal of Hepatocellular Carcinoma 2024, 11:241-255
Published Date: 2 February 2024