Back to Journals » International Journal of General Medicine » Volume 19
Prognostic Nutritional Index is Independently Associated with Major Adverse Cardiovascular Events in Patients with Triple - Vessel Disease: A Retrospective Cohort Study
Authors Wang M ![]() , Lei Y
, Lei Y ![]() , Xue Y
, Xue Y
Received 20 February 2026
Accepted for publication 9 April 2026
Published 18 April 2026 Volume 2026:19 603394
DOI https://doi.org/10.2147/IJGM.S603394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Mengmeng Wang,1 Yuping Lei,2 Yuzeng Xue2
1School of Clinical Medicine, Shandong Second Medical University, Weifang, Shandong, 261053, People’s Republic of China; 2Department of Cardiology, Liaocheng People’s Hospital, Liaocheng, Shandong, 252000, People’s Republic of China
Correspondence: Yuzeng Xue, Department of Cardiology, Liaocheng People’s Hospital, Liaocheng, Shandong, 252000, People’s Republic of China, Email [email protected]
Objective: Current evidence indicates that nutrition plays an important role in cardiovascular disease risk monitoring and prognosis assessment. Therefore, this study aimed to evaluate the correlation between the prognostic nutritional index (PNI) and major adverse cardiovascular events (MACE) in patients with triple - vessel coronary heart disease (TV - CHD).
Methods: In this single - center retrospective cohort study, 547 patients with TV - CHD admitted to Liaocheng People’s Hospital from January 2020 to January 2023 were enrolled. Univariate and multivariate Cox regression analyses, subgroup and sensitivity analyses, receiver operating characteristic (ROC) curve analysis, and Kaplan - Meier survival analysis were performed to assess the association between PNI and time to first MACE.
Results: During a median follow - up period of 38.5 months, 176 MACE events occurred (32.2%). Multivariate Cox regression analysis showed that after adjusting for all confounding factors, each one - unit increase in PNI was associated with a 2.9% reduction in MACE risk (HR 0.971, 95% CI 0.947– 0.997, P = 0.026). Compared with the T1 group, the T3 group had a 34.5% lower risk of MACE (HR 0.655, 95% CI 0.447– 0.960, P = 0.030). Multiple subgroup and sensitivity analyses further confirmed the robustness of the results. Time - dependent ROC analysis indicated that PNI had modest predictive value for MACE risk (overall population: time=dependent AUC at 12, 24, and 36 months were 0.588, 0.575, and 0.562). Kaplan - Meier survival curves demonstrated significant differences in cumulative MACE risk among PNI tertiles, with the T1 group having the poorest prognosis (Log - rank P = 0.010).
Conclusion: Lower PNI levels are independently associated with an increased risk of MACE in TV - CHD patients. Given its modest discriminatory ability, PNI should be considered a readily available, cost - effective supplementary biomarker that may provide adjunctive prognostic value in the comprehensive assessment of this high - risk population.
Keywords: coronary heart disease, triple - vessel disease, prognostic nutritional index, major adverse cardiovascular events, risk prediction, retrospective study
Introduction
The China Cardiovascular Health and Disease Report 2024 points out that with the development of the social economy—especially the acceleration of population aging and urbanization—cardiovascular disease (CVD) remains the leading cause of death among urban and rural residents in China, with coronary heart disease (CHD) ranking first in prevalence among these conditions.1 Preliminary survey results show that the prevalence of CHD among Chinese residents aged ≥ 18 years is 758 per 100,000, and the rate increases rapidly with age.1 The diagnosis and treatment of CHD remain challenging, particularly for patients with triple - vessel CHD (TV - CHD). Because these patients have lesions in all three major coronary arteries, they usually present with diffuse and severe atherosclerosis, often accompanied by impaired cardiac function, and are therefore classified as a high - risk group within CHD. Numerous randomized clinical trials have shown that even after coronary intervention or bypass surgery, these patients still face a high risk of major adverse cardiovascular events (MACE), such as all - cause death, cardiovascular death, non - fatal MI, non - fatal cerebral infarction, and unplanned revascularization.2–4 Therefore, identifying modifiable risk factors in patients with TV - CHD is crucial to improving prognosis in this high - risk population.
Current evidence suggests that nutrition plays an important clinical role in CVD. For example, Almuwaqqat Z et al analyzed data from the Million Veteran Program (MVP, 2011–2018) and the UK Biobank (UKB, 2006–2010), finding that higher body mass index (BMI) variability was significantly associated with adverse cardiovascular events among U.S. veterans. Each 1 - standard - deviation increase in BMI variability was associated with an 8% higher risk of cardiovascular mortality (HR 1.08, 95% CI 1.04–1.11).5 In another study, Jung E et al analyzed 14 independent reports including 1,055,309 participants and 9,457 cardiovascular events, revealing that total cholesterol (TC) and low - density lipoprotein cholesterol (LDL - C) were positively associated with cardiovascular mortality risk, while high - density lipoprotein cholesterol (HDL - C) showed a negative association.6 In recent years, the relationship between serum albumin levels and CHD risk has gained increasing attention.7,8 In a cross - sectional study evaluating adults over 45 years of age, researchers found that serum albumin levels were negatively correlated with CHD risk after adjusting for confounders (OR = 0.970, 95% CI 0.948–0.992), indicating that lower serum albumin levels were associated with a higher risk of CHD.9 However, while these studies have revealed associations between certain nutritional markers and major cardiovascular events—particularly in CHD patients—these markers are all single parameters.
In contrast, a widely used immune - nutritional measure derived from serum albumin and peripheral blood lymphocyte count—the prognostic nutritional index (PNI), calculated from serum albumin and peripheral blood lymphocyte count—has been widely used to predict adverse outcomes in various patient populations.10–13 As an immune - nutritional biomarker, PNI reflects chronic inflammation, immune function, and nutritional status. Because it is easily obtainable and integrates both nutritional and immune aspects, PNI may have greater prognostic value in CVD than single nutritional indicators. Several studies have also demonstrated the prognostic value of PNI in patients with CVD. For instance, Ma et al14 found in a cohort of over 17,000 CHD patients that PNI was closely associated with the New York Heart Association (NYHA) functional classification. Patients with lower PNI values were more likely to be in NYHA class III–V, and those who were malnourished or underweight had the poorest cardiac function, suggesting that PNI can not only predict prognosis but also serve as an auxiliary indicator of cardiac function deterioration. Focusing on the relationship between CHD and atrial fibrillation (AF), Xie et al15 retrospectively analyzed 600 patients with acute ST - segment elevation MI (STEMI) who underwent percutaneous coronary intervention (PCI). They found that the incidence of new - onset AF during hospitalization was 7.7%, and a low PNI was an independent risk factor for new - onset AF (OR = 0.824). The receiver operating characteristic (ROC) curve showed a cutoff value of 40.1 for predicting AF, with a sensitivity of 76.1% and specificity of 71.3%, indicating that PNI is related to both nutritional and immune status in CHD patients and can help predict arrhythmia risk, indirectly affecting long - term prognosis. Regarding CHD complicated with acute kidney injury (AKI), Hatem et al16 reported that among 336 patients with non - ST - elevation MI (NSTEMI), the incidence of contrast - associated AKI (CA - AKI) was 20%, and patients with CA - AKI had significantly lower PNI values. A PNI < 48.5 was identified as an independent predictor of CA - AKI. Dong et al17 further expanded the study to CHD patients with chronic kidney disease (CKD), including 4,391 patients, and found a linear negative correlation between PNI and CA - AKI, with low PNI patients showing a significantly increased risk. These findings suggest that maintaining good nutritional and immune status is crucial for preventing contrast - related complications in high - risk groups. However, the research evidence regarding the correlation between “time - to - first MACE” after discharge for patients with three - vessel coronary artery disease (TV - CHD) and PNI is still limited. Therefore, it is very necessary to explore whether PNI can provide additional prognostic value beyond the existing mature clinical and anatomical markers.
Based on the above background, we assume that a lower level of PNI is significantly associated with a higher risk of MACE. Based on this assumption, this study aims to evaluate the correlation between PNI and MACE in patients with TV - CHD. The goal is to provide new insights and theoretical evidence for risk monitoring and prognostic assessment in CHD.
Methods
Study Population
This was a single - center retrospective cohort study conducted at Liaocheng People’s Hospital from January 2020 to January 2023. A total of 700 patients with TV - CHD were initially screened. The inclusion criteria were as follows: (1) age ≥18 years; (2) diagnosis of triple - vessel disease confirmed by coronary angiography (stenosis ≥ 50% in three major coronary arteries). The exclusion criteria were as follows: (1) patients with severe hepatic or renal failure; (2) patients with malignant tumors or cachexia; (3) patients with severe hematologic or immune system diseases; (4) patients with severe infections; (5) patients currently receiving nutritional support; (6) patients currently receiving glucocorticoid or immunosuppressive therapy; (7) patients without baseline data on serum albumin and peripheral lymphocyte count; (8) patients who died during hospitalization. (9) patients lost to follow-up. Based on the above inclusion and exclusion criteria, 547 patients were finally included in the analysis. This study was reviewed and approved by the Ethics Committee of Liaocheng People’s Hospital, and the study protocol complied with the basic principles of the Declaration of Helsinki. As this was a retrospective study, and all data were anonymized, the requirement for informed consent was waived by the Ethics Committee of Liaocheng People’s Hospital.
Definition and Grouping of Prognostic Nutritional Index
In this study, the PNI was calculated as serum albumin (g/L) plus 5 times the total peripheral blood lymphocyte count (109/L).11 Furthermore, according to the tertiles of PNI, patients were divided into three groups: T1 (≤ 44.55, n = 183), T2 (44.55–49.42, n = 182), and T3 (> 49.42, n = 182).
Follow - Up and Outcome Definition
All patients were followed from the date of hospital discharge until death or September 2025. Follow - up data were obtained through multiple outpatient and emergency visit records, hospitalization records, and telephone follow-ups, with information collected from patients or their family members. For suspected adverse events reported through telephone follow-up, we further conducted cross-verification by reviewing the patients’ electronic medical records, hospitalization records and death certificates in our hospital or other medical institutions. In addition, for patients without MACE, the follow-up time was truncated at their last known contact time or the study’s follow-up deadline. A total of 50 patients were lost to follow-up in this study, with a loss to follow-up rate of 7.14%.The primary endpoint of this study was the occurrence of time - to - first MACE, including a combination of one or more of the following: all-cause death, cardiovascular death, non-fatal MI, non-fatal cerebral infarction, and unplanned revascularization. The operational definitions and adjudication criteria for each MACE component were as follows: all-cause death was defined as death from any cause during follow-up. Cardiovascular death was defined as death attributable to myocardial infarction, heart failure, sudden cardiac death, or other clearly documented cardiovascular causes. Non-fatal myocardial infarction (MI) was defined as a rise in cardiac troponin above the 99th percentile upper reference limit, accompanied by at least one of the following: ischemic symptoms, new ischemic electrocardiographic changes, development of pathological Q waves, or imaging evidence of new loss of viable myocardium. Non-fatal cerebral infarction was defined as an ischemic stroke confirmed by a neurologist based on clinical presentation and neuroimaging (CT or MRI), excluding transient ischemic attack and hemorrhagic stroke. Unplanned revascularization was defined as any urgent coronary revascularization (percutaneous coronary intervention or coronary artery bypass grafting) performed due to acute ischemic symptoms or clinical deterioration, excluding staged or elective procedures that were scheduled prior to the initial discharge as part of a planned treatment strategy.
Data Collection and Definitions
In this study, all data were obtained from the electronic medical record system of Liaocheng People’s Hospital, including demographic data, anthropometric measurements, medical history, previous medication use, laboratory biomarkers, and discharge medications. Demographic data included age, sex, family history of CHD, and smoking status. Family history of CHD18 was defined as a confirmed history of MI, angina, sudden cardiac death, and/or revascularization (including coronary artery bypass grafting or PCI) in first - degree relatives (men ≤ 55 years old or women ≤ 65 years old, including parents and siblings). Smoking was defined as a history of regular smoking in the past or at present. Anthropometric data included height, weight, BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate. BMI was calculated as body weight (kg) divided by the square of height (m2). SBP, DBP, and heart rate were obtained from the first measurements recorded upon hospital admission.
Medical history and medication data included a history of hypertension, diabetes, dyslipidemia, CHD, prior PCI, and the use of antihypertensive, hypoglycemic, lipid - lowering, and antiplatelet drugs. Hypertension19 was defined as an office blood pressure measured on three different occasions without antihypertensive treatment showing SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg, or a documented history of hypertension currently treated with antihypertensive medications even if blood pressure was < 140/90 mmHg. Diabetes20 was defined as the presence of typical clinical symptoms (polydipsia, polyphagia, polyuria, and unexplained weight loss) plus any of the following: random plasma glucose ≥ 11.1 mmol/L, fasting blood glucose (FBG) ≥ 7.0 mmol/L, 2 - hour plasma glucose during an oral glucose tolerance test ≥ 11.1 mmol/L, or glycated hemoglobin (HbA1c) ≥ 6.5%. In the absence of typical symptoms, repeated testing was required for diagnosis. Dyslipidemia, according to the Chinese Guidelines for Lipid Management (2023),21 was defined as TC ≥ 5.2 mmol/L, triglycerides ≥ 1.7 mmol/L, LDL - C ≥ 3.4 mmol/L, or HDL - C ≤ 1.0 mmol/L. A history of CHD was defined as a previous diagnosis of coronary atherosclerotic heart disease, including a history of MI, angiographically confirmed coronary stenosis, prior revascularization, hospital admission for angina with objective evidence, or a history of chronic stable angina. A history of PCI was defined as having undergone any PCI, including coronary stent implantation, percutaneous transluminal coronary angioplasty, or other related interventional techniques.
Laboratory biomarkers included white blood cell count (WBC), neutrophil count, lymphocyte count, monocyte count, hemoglobin, platelet count, C - reactive protein (CRP), triglycerides, TC, LDL - C, HDL - C, apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), lipoprotein(a), FBG, albumin, uric acid, estimated glomerular filtration rate (eGFR), fibrinogen, D - dimer, N - terminal pro brain natriuretic peptide (NT - proBNP), and cardiac troponin I (cTnI). All blood samples were collected from the antecubital vein and analyzed in the hospital’s central laboratory. Discharge medications included aspirin, clopidogrel, ticagrelor, statins, β - blockers, angiotensin - converting enzyme inhibitors (ACEI) / angiotensin receptor blockers (ARB), calcium channel blockers (CCB), furosemide, spironolactone, and hypoglycemic agents.
Statistical Methods
All statistical analyses were performed using SPSS version 30.0 (IBM Corporation, USA) and R software (version 4.2.1, with the “survival” and “timeROC” packages). The Shapiro–Wilk test was used to assess the normality of all continuous variables before analysis. Since none of the continuous variables followed a normal distribution, they were expressed as median (interquartile range), and differences between two groups were analyzed using the Mann–Whitney U-test, while differences among three groups were compared using the Kruskal–Wallis test. Categorical variables were expressed as frequencies (percentages), and differences between groups were evaluated using the chi - square test or Fisher’s exact test.
Univariate Cox regression analysis was used to assess the association between each variable and MACE. Variables with P < 0.05 were included in three multivariate Cox regression models to further evaluate the relationship between PNI and MACE. Model 1 adjusted for age only. Model 2 adjusted for age, hypertension, CHD, PCI history, use of lipid - lowering drugs, and antiplatelet drugs. Model 3 further adjusted for age, hypertension, CHD, PCI history, lipid - lowering drugs, antiplatelet drugs, hemoglobin, eGFR, NT - proBNP, aspirin, ticagrelor, furosemide, and spironolactone. As show in Figure 1, the proportional hazards assumption was tested using Schoenfeld residuals, and no violation was detected (global P = 0.5076). As show in Figure 2, a restricted cubic spline (RCS) with four knots was used to assess non - linearity, confirming a linear negative association. Subgroup analyses were conducted based on seven variables (age, sex, smoking, hypertension, dyslipidemia, CHD, and PCI) to verify the robustness of the association between PNI and MACE. Additionally, a sensitivity analysis excluding patients with a family history of CHD was performed to reassess the multivariate relationship between PNI and MACE. The predictive value of PNI for MACE was evaluated using time - dependent ROC curve analysis (tdROC) at 12, 24, and 36 months. Finally, Kaplan - Meier survival curves were used to compare the cumulative incidence of MACE among the three PNI tertile groups. All tests were two - sided, and P < 0.05 was considered statistically significant. Given the exploratory nature of this retrospective study, no formal sample size or power calculation was performed prior to data collection; the sample size was determined by the number of eligible patients during the study period. In this study, all categorical variables were complete, except for a few continuous variables which were missing by a single digit. We performed mean imputation for these missing values.
 |
Figure 1 Use Schoenfeld residuals to verify the proportional hazards assumption of the PNI. Abbreviation: PNI, prognostic nutritional index. |
 |
Figure 2 Analysis of the relationship between PNI and the risk of MACE using restricted cubic splines. Abbreviations: PNI, prognostic nutritional index; MACE, major adverse cardiovascular events. |
Results
Baseline Characteristics by MACE Group
As shown in Table 1, a total of 547 patients were included in the study, among whom 372 (68.0%) were male, with a median age of 64 years (56.00, 71.00). According to the occurrence of MACE, patients were divided into the non - MACE group (n = 371) and the MACE group (n = 176). Compared with the non - MACE group, patients in the MACE group were older and had higher proportions of hypertension, CHD, history of PCI, and use of antihypertensive, hypoglycemic, lipid - lowering, and antiplatelet medications. They also had higher levels of D - dimer and NT - proBNP, as well as a greater use of furosemide and spironolactone, but lower levels of lymphocyte count, hemoglobin, albumin, and eGFR, and lower proportions of aspirin and ticagrelor use (P < 0.05). More importantly, the MACE group had significantly lower PNI levels (P < 0.001). Other variables showed no significant differences between the two groups (P > 0.05).
 |
Table 1 Baseline Characteristics Grouped According to MACE |
Baseline Characteristics by PNI Tertiles
As shown in Table 2, patients were divided into three groups according to PNI tertiles: T1 (≤ 44.55, n = 183), T2 (44.55–49.42, n = 182), and T3 (> 49.42, n = 182). There were significant differences in several baseline variables among the three groups, including age, SBP, DBP, WBC, lymphocyte count, hemoglobin, platelet count, CRP, triglycerides, TC, LDL - C, HDL - C, ApoA1, ApoB, lipoprotein(a), FBG, albumin, eGFR, D - dimer, NT - proBNP, cTnI, furosemide, and spironolactone (P < 0.05). Notably, the incidence of MACE differed significantly among the three PNI groups and gradually decreased with higher PNI tertiles (P = 0.012).
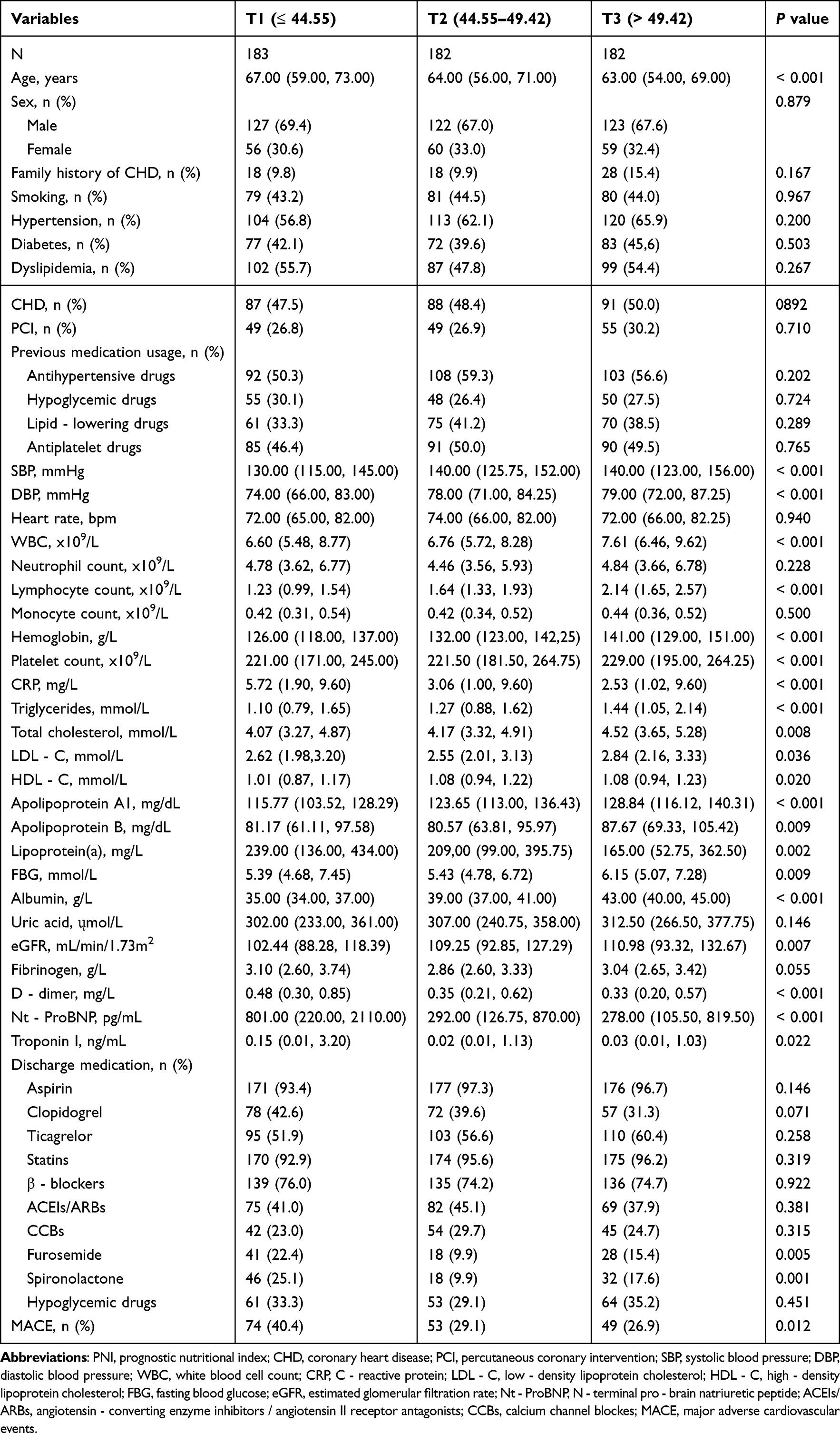 |
Table 2 Baseline Characteristics Grouped According to the PNI Tertiles |
Univariate Cox Regression Analysis for MACE
As shown in Table 3, univariate Cox regression analysis indicated that age, hypertension, CHD, history of PCI, use of lipid - lowering drugs, antiplatelet drugs, hemoglobin, albumin, eGFR, NT - proBNP, aspirin, ticagrelor, furosemide, spironolactone, and PNI were all significantly associated with MACE risk (P < 0.05). Each one - unit increase in PNI was associated with a 3.8% reduction in MACE risk (HR: 0.962, 95% CI: 0.936–0.989, P = 0.005).
 |
Table 3 Univariate Cox Regression Analysis of MACE |
Multivariate Analysis of the Association Between PNI and MACE
As shown in Table 4, in Model 1 (adjusted for age only), each one - unit increase in PNI was associated with a 3.1% reduction in MACE risk (HR: 0.969, 95% CI: 0.943–0.996, P = 0.026). Compared with the T1 group, MACE risk decreased by 31.9% (HR: 0.681, 95% CI: 0.478–0.970, P = 0.033) in T2 and by 32.9% (HR: 0.671, 95% CI: 0.465–0.969, P = 0.033) in T3. In Model 2 (adjusted for age, hypertension, CHD, PCI, lipid - lowering drugs, and antiplatelet drugs), each one - unit increase in PNI reduced MACE risk by 4.2% (HR: 0.958, 95% CI: 0.932–0.985, P = 0.002). Compared with the T1 group, MACE risk decreased by 37.8% in T2 (HR: 0.622, 95% CI: 0.437–0.885, P = 0.008) and by 42.5% in T3 (HR: 0.575, 95% CI: 0.400–0.826, P = 0.003). In Model 3 (further adjusted for hemoglobin, eGFR, NT - proBNP, aspirin, ticagrelor, furosemide, and spironolactone), each one - unit increase in PNI still reduced MACE risk by 2.9% (HR: 0.971, 95% CI: 0.947–0.997, P = 0.026). Compared with T1, MACE risk decreased by 34.5% in T3 (HR: 0.655, 95% CI: 0.447–0.960, P = 0.030).
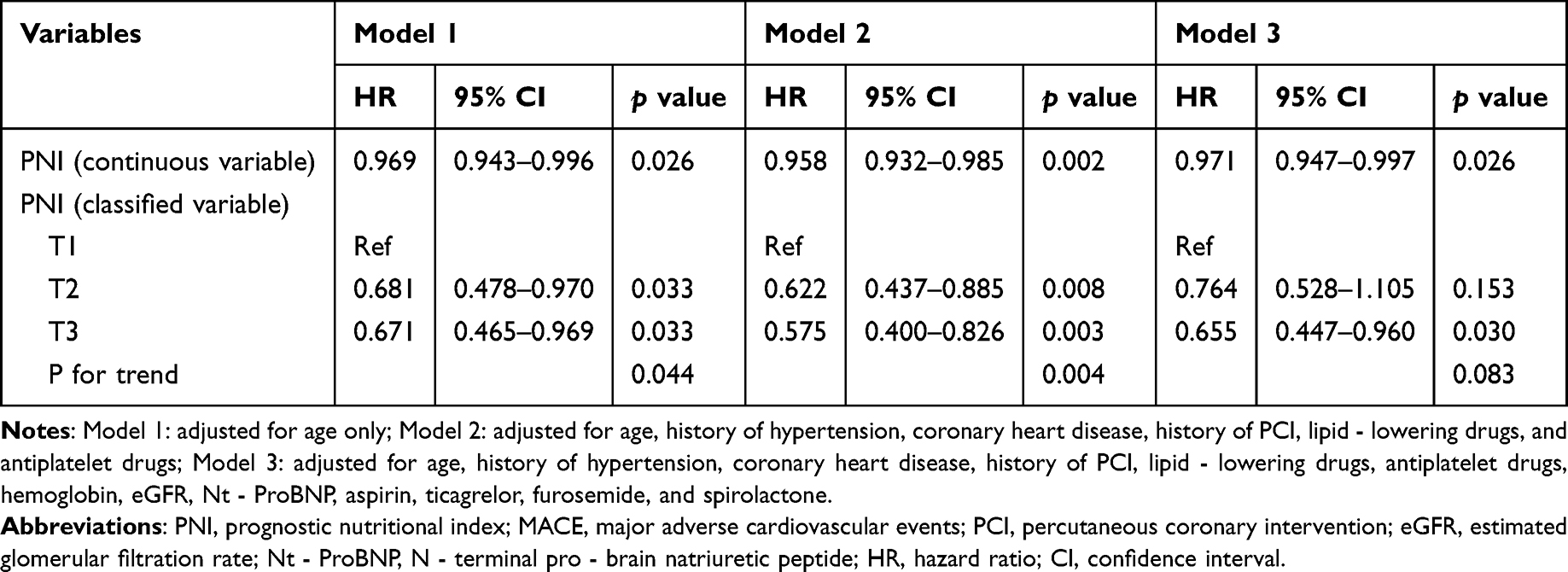 |
Table 4 Multivariate Correlation Between PNI and MACE |
Subgroup Analysis of PNI and MACE
As shown in Table 5, in the fully adjusted multivariate Cox regression model, among females, each one - unit increase in PNI was associated with a 6.8% reduction in MACE risk (HR: 0.932, 95% CI: 0.881–0.987, P = 0.016). In the subgroup aged ≥ 65 years, compared with T1, MACE risk was 40.4% lower in T3 (HR: 0.596, 95% CI: 0.367–0.969, P = 0.037). In non - smokers, compared with T1, MACE risk decreased by 46.5% in T3 (HR: 0.535, 95% CI: 0.334–0.858, P = 0.010), and each one - unit increase in PNI reduced MACE risk by 5.7% (HR: 0.943, 95% CI: 0.909–0.978, P = 0.002). In the subgroup without hypertension, compared with T1, MACE risk decreased by 54.3% in T2 (HR: 0.457, 95% CI: 0.217–0.962, P = 0.039). In patients without dyslipidemia, each one - unit increase in PNI reduced MACE risk by 4.7% (HR: 0.953, 95% CI: 0.919–0.989, P = 0.010). In patients with CHD, compared with T1, MACE risk decreased by 50.4% in T2 (HR: 0.496, 95% CI: 0.303–0.812, P = 0.005) and by 49.4% in T3 (HR: 0.506, 95% CI: 0.321–0.798, P = 0.003), with each one - unit increase in PNI reducing MACE risk by 4.5% (HR: 0.955, 95% CI: 0.924–0.987, P = 0.006). In patients with a history of PCI, compared with T1, MACE risk decreased by 46.8% in T2 (HR: 0.532, 95% CI: 0.296–0.955, P = 0.035) and by 69.2% in T3 (HR: 0.308, 95% CI: 0.167–0.569, P < 0.001), and each one - unit increase in PNI reduced MACE risk by 7.2% (HR: 0.928, 95% CI: 0.887–0.970, P < 0.001).
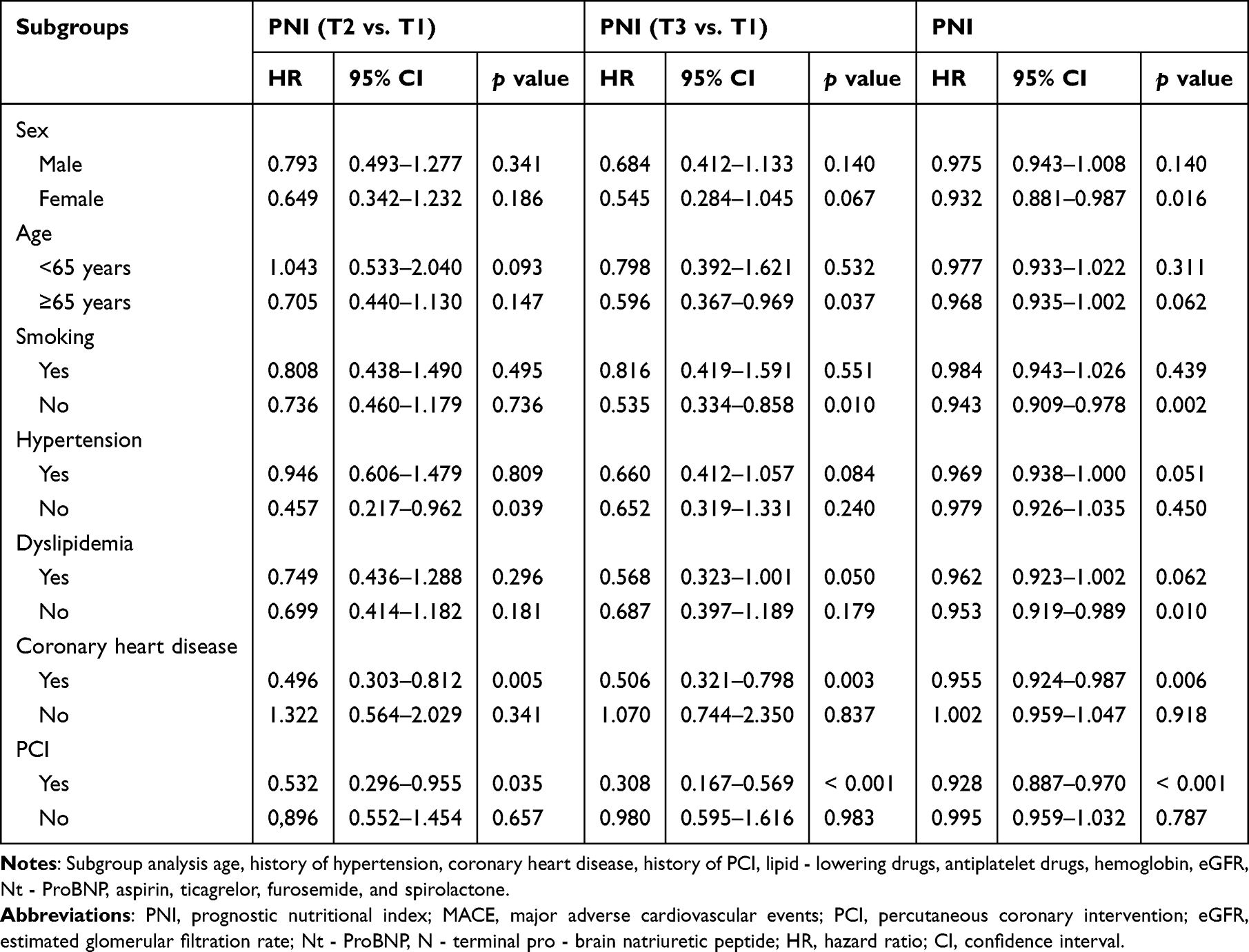 |
Table 5 Multivariate Subgroup Analysis of PNI and MACE |
Sensitivity Analysis
As shown in Table 6, in the sensitivity analysis excluding patients with a family history of CHD, higher PNI levels remained significantly associated with a lower risk of MACE in both Model 1 (adjusted for age) and Model 2 (partially adjusted). In Model 2, each one - unit increase in PNI reduced MACE risk by 3.8% (HR: 0.962, 95% CI: 0.934–0.991, P = 0.010), and compared with T1, MACE risk decreased by 37.6% in T2 (HR: 0.624, 95% CI: 0.429–0.909, P = 0.014) and by 41.8% in T3 (HR: 0.582, 95% CI: 0.389–0.871, P = 0.008). In the fully adjusted Model 3, although the HR and 95% CI for PNI were not statistically significant (P = 0.059), MACE risk was still 37.5% lower in T3 compared with T1 (HR: 0.625, 95% CI: 0.412–0.948, P = 0.027).
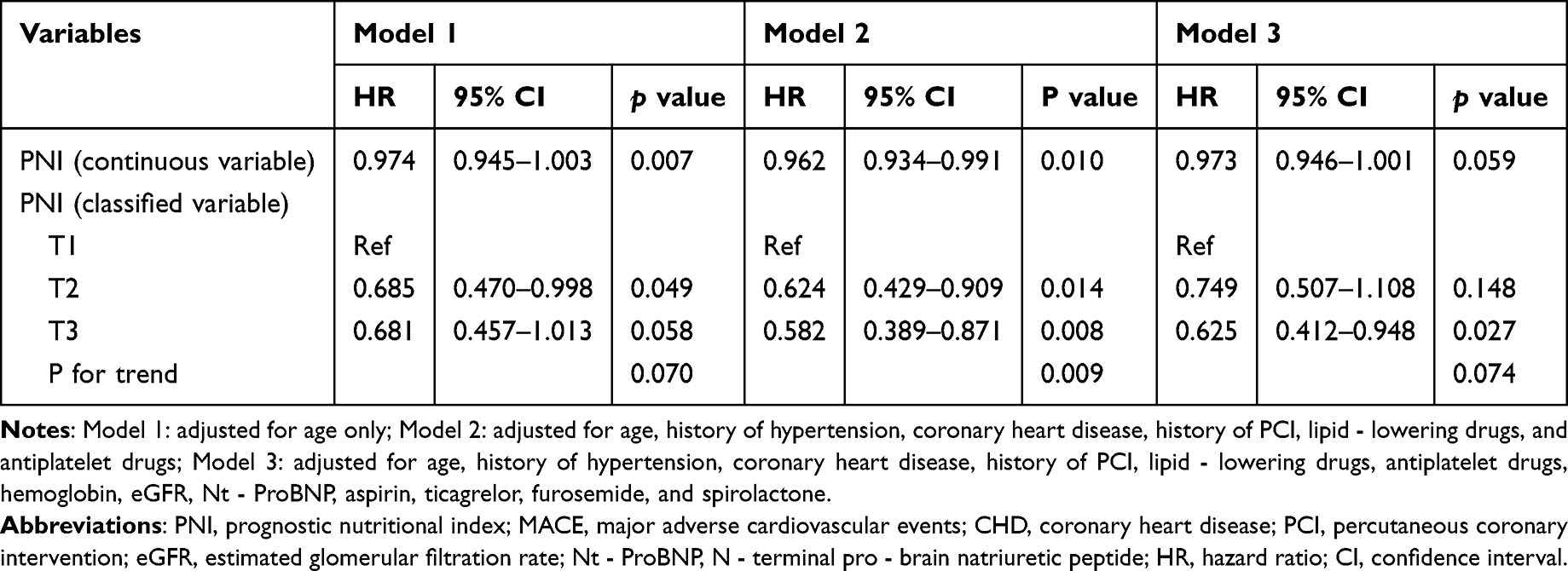 |
Table 6 Multivariate Correlation Between PNI and MACE: Exclude Patients with CHD Family History |
Visualization of PNI and MACE Risk
As shown in Figure 3, time - dependent ROC curve analysis demonstrated that PNI had modest predictive value for MACE at 12, 24, and 36 months post - discharge. The time - dependent AUC values were 0.5875, 0.5751, and 0.5622, respectively.
 |
Figure 3 Time - dependent ROC curves assessing the predictive value of PNI for MACE. Abbreviations: AUC, area under the curve; CI, confidence interval; ROC, receiver operating characteristic curve; PNI, prognostic nutritional index; MACE, major adverse cardiovascular events. |
As shown in Figure 4, Kaplan - Meier survival analysis revealed significant differences in the cumulative incidence of MACE among different PNI groups (Log - rank P = 0.010), with patients in the T1 group showing a faster increase in cumulative MACE risk and a poorer prognosis. The curve includes numbers at risk and censoring marks, with time origin defined as discharge.
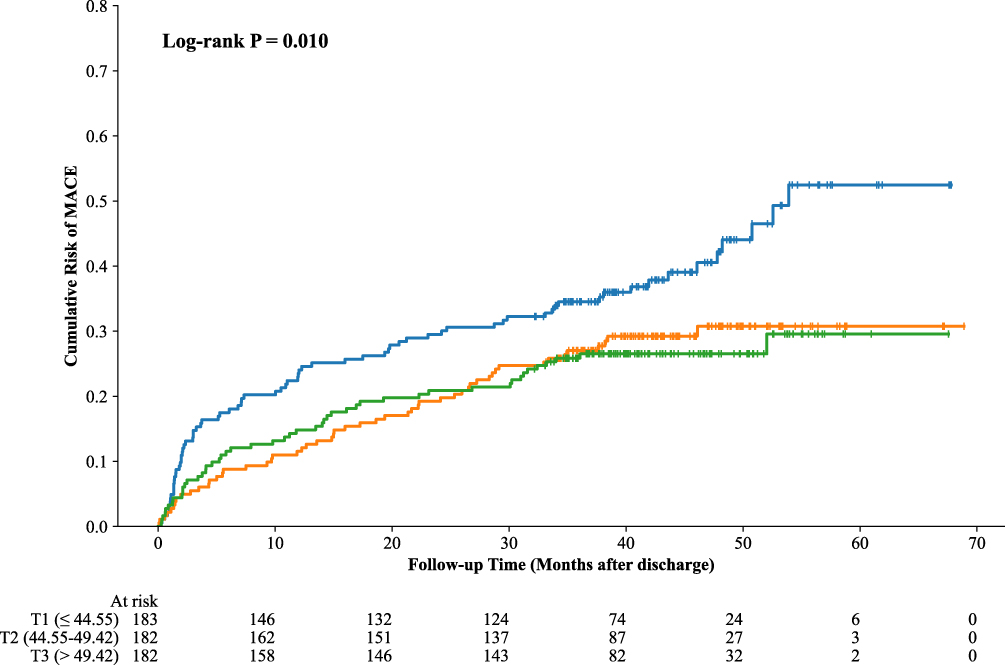 |
Figure 4 Kaplan - Meier survival curve assessing the differences in the cumulative risk of MACE among the PNI tertile groups. Abbreviations: PNI, prognostic nutritional index; MACE, major adverse cardiovascular events. |
Discussion
In this study, we analyzed 547 patients with TV - CHD). During a median follow - up period of 38.5 months, 176 patients (32.2%) experienced MACE. Multivariate Cox regression analysis showed that after adjusting for all confounding factors, each one - unit increase in the PNI was associated with a 2.9% reduction in MACE risk, and compared with the T1 group, the T3 group had a 34.5% lower MACE risk. Multiple subgroup and sensitivity analyses further confirmed the stability of these results. Time - dependent ROC curve analysis demonstrated that PNI had modest predictive value for MACE risk in both the overall population and gender subgroups. Kaplan - Meier survival curves revealed significant differences in cumulative MACE risk among PNI tertiles, with the T1 group showing the poorest prognosis. These findings suggest that lower PNI levels are significantly associated with a higher risk of MACE in patients with TV - CHD, and that PNI may have potential adjunctive clinical value for prognostic evaluation in this population.
In recent years, numerous studies in China and abroad have confirmed that PNI plays an important role in assessing nutritional, inflammatory, and immune status in patients with CHD, and may be closely related to disease severity, complication rate, and long - term prognosis. For example, in a large cohort of PCI patients, Liu et al22 included 3,561 CHD patients with an average follow - up of 37.6 months and found that higher PNI levels were significantly associated with reduced risks of all - cause and cardiac mortality. Kaplan - Meier analysis showed that patients with higher PNI had better long - term survival, and multivariate Cox regression confirmed that PNI was an independent predictor. Similarly, Wu et al,23 in a prospective cohort study involving over 15,000 CHD patients, found a “J - shaped” relationship between PNI and all - cause mortality—both extremely low and extremely high PNI levels were associated with increased mortality, while moderate PNI levels predicted the best outcomes. This suggests that clinicians should be aware of bidirectional risks when interpreting PNI. In our study, patients in the highest PNI tertile (T3) had the lowest MACE risk, which aligns with the protective left‑hand side of the J‑shaped curve. However, the prevalence of extremely high PNI values in our TV‑CHD cohort was relatively low, and we did not observe an increased risk in the T3 group. This may reflect differences in population characteristics or the composite endpoint used; further studies with larger sample sizes are needed to explore potential non‑linear effects of PNI specifically in patients with triple‑vessel disease. Compared with traditional single nutritional markers, PNI is more comprehensive, universal, and easy to implement in clinical practice, making it a promising tool for cardiovascular disease risk stratification and personalized treatment.
However, although we found an association between PNI and MACE in TV - CHD patients, the underlying biological mechanisms remain unclear. Based on the literature, several mechanisms may be involved: (1) PNI as a marker of immune - nutritional and inflammatory status: Studies have shown that malnutrition may trigger acute coronary syndromes.24 Patients with low PNI levels often suffer from malnutrition, which reduces their ability to cope with cardiovascular stress.25 Malnutrition can impair myocardial repair and remodeling, increase cardiac burden, and eventually lead to HF or other adverse cardiovascular events.26 (2) Role of serum albumin: Experimental and clinical evidence indicates that atherosclerosis is a chronic inflammatory disease driven primarily by monocytes and macrophages, with involvement of adaptive immunity and autoimmune components.27 Serum albumin may influence the pathogenesis of CHD through its anti - inflammatory, antioxidant, and antiplatelet aggregation properties.28–30 Moreover, albumin protects against endothelial dysfunction induced by inflammation and oxidative stress during sepsis31 and has antiplatelet and anticoagulant effects, preventing histone - induced platelet aggregation in a charge - dependent manner.32,33 These findings suggest that serum albumin plays a protective role against the development of CHD. (3) Role of lymphocytes: A decreased absolute lymphocyte count indicates malnutrition and impaired immune defense, which can exacerbate atherosclerotic burden.34 Reduced lymphocyte ratios reflect physiological stress responses, which activate the hypothalamic - pituitary - adrenal axis and induce cellular and molecular changes in platelet function, coagulation, endothelial integrity, redox balance, and sterile inflammation—all of which are associated with systemic deterioration of cardiovascular health.35 Although these mechanisms may partially explain the link between PNI and MACE, further cellular and animal studies are needed to verify these biological pathways.
Despite yielding meaningful results, this study has several limitations that may affect its generalizability. First, this was a single - center study with a relatively small sample size, which may limit the representativeness of the findings; larger multicenter studies are needed for validation. Second, as a retrospective observational study, it did not include genetic or genomic data, preventing causal inference between PNI and MACE. Third, although we adjusted for many confounders, unmeasured factors such as environmental influences, diet, socioeconomic status, and genetic predisposition might still have affected the results. Fourth, PNI was calculated from baseline serum albumin and lymphocyte counts measured only once, without evaluating dynamic changes or long - term exposure, which may also influence outcomes.Fifth, the exclusion of patients who died during hospitalization (criterion 8) may have introduced survival bias, as the sickest patients were excluded from the analysis. Sixth, we acknowledge that adjusting for discharge medications, particularly furosemide and spironolactone, may have introduced confounding by indication, as these medications are often prescribed as a proxy for underlying heart failure severity. Such adjustment may represent over-adjustment for mediators rather than baseline risk factors, potentially underestimating the true prognostic effect of PNI. Seventh, the composite MACE endpoint used in this study, which includes non‑fatal cerebral infarction and unplanned revascularization, is broader than definitions used in some other studies; this may limit direct comparability of event rates across different cohorts. Finally, MACE was used as a composite endpoint, and we did not analyze its individual components (eg., all - cause mortality, cardiovascular death, non - fatal MI, non - fatal stroke, or unplanned revascularization). Thus, the specific associations between PNI and individual cardiovascular events remain unclear. External validation in large-scale, prospective, multicenter cohorts is therefore essential before considering clinical translation. Despite these limitations, the present findings may provide new insights and theoretical evidence for future research.
Conclusion
In this single - center retrospective cohort study, lower PNI levels were significantly associated with a higher risk of MACE among patients with TV - CHD. This suggests that nutritional status may have important clinical value in the prognostic assessment of CHD. Therefore, PNI can be combined with other traditional risk prediction models and integrated into the routine risk stratification process, thereby enhancing the predictive value for the risk of MACE in patients with TV-CHD. Future large - scale prospective randomized controlled trials, combined with cellular and animal experiments as well as artificial intelligence and bioinformatics analyses, are warranted to further elucidate the potential mechanisms underlying this association.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Ethics Committee of Liaocheng People’s Hospital (ethics approval number2025292), and the study protocol complied with the basic principles of the Declaration of Helsinki. As this was a retrospective study, and all data were anonymized, the requirement for informed consent was waived by the Ethics Committee of Liaocheng People’s Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Liaocheng Key Research and Development Program Policy Guidance Project (2025YD13) and the Shandong Province Traditional Chinese Medicine Science and Technology Project (M20241403).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Liu MB, He XY, Yang XH, et al. Key points interpretation of the China cardiovascular health and disease report 2024. Chin J Cardiovasc Med. 2025;30(4):384–16.
2. Park S-J, Ahn J-M, Kim Y-H, et al. Trial of everolimus-eluting stents or bypass surgery for coronary disease. N Engl J Med. 2015;372(13):1204–1212. doi:10.1056/NEJMoa1415447
3. Mäkikallio T, Holm NR, Lindsay M, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective, randomised, open-label, non-inferiority trial. Lancet. 2016;388(10061):2743–2752. doi:10.1016/S0140-6736(16)32052-9
4. Hueb WA, Lopes N, Gersh BJ, et al. Ten-year follow-up survival of the Medicine, Angioplasty, or Surgery Study (MASS II): a randomized controlled clinical trial of 3 therapeutic strategies for multivessel coronary artery disease. Circulation. 2010;122(10):949–957. doi:10.1161/CIRCULATIONAHA.109.911669
5. Almuwaqqat Z, Hui Q, Liu C, et al. Long-term body mass index variability and adverse cardiovascular outcomes. JAMA Network Open. 2024;7(3):e243062. doi:10.1001/jamanetworkopen.2024.3062
6. Jung E, Kong SY, Ro YS, Ryu HH, Shin SD. Serum cholesterol levels and risk of cardiovascular death: a systematic review and a dose-response meta-analysis of prospective cohort studies. Int J Environ Res Public Health. 2022;19(14):8272. doi:10.3390/ijerph19148272
7. Arques S. Serum albumin and cardiovascular disease: does low serum albumin contribute to the emergence and worsening of some cardiovascular diseases? Eur J Intern Med. 2020;80:122–123. doi:10.1016/j.ejim.2020.07.019
8. Manolis AA, Manolis TA, Melita H, Mikhailidis DP, Manolis AS. Low serum albumin: a neglected predictor in patients with cardiovascular disease. Eur J Intern Med. 2022;102:24–39. doi:10.1016/j.ejim.2022.05.004
9. Hou XZ, Liu EQ, Liu SQ, Lv H, Cui HF, Han J. The negative association between serum albumin levels and coronary heart disease risk in adults over 45 years old: a cross-sectional survey. Sci Rep. 2023;13(1):672. doi:10.1038/s41598-023-27974-w
10. Chen QJ, Qu HJ, Li DZ, et al. Prognostic nutritional index predicts clinical outcome in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Sci Rep. 2017;7(1):3285. doi:10.1038/s41598-017-03364-x
11. Cheng YL, Sung SH, Cheng HM, et al. Prognostic nutritional index and the risk of mortality in patients with acute heart failure. J Am Heart Assoc. 2017;6(6):e004876. doi:10.1161/JAHA.116.004876
12. Wada H, Dohi T, Miyauchi K, et al. Relationship between the prognostic nutritional index and long-term clinical outcomes in patients with stable coronary artery disease. J Cardiol. 2018;72(2):155–161. doi:10.1016/j.jjcc.2018.01.012
13. Sun K, Chen S, Xu J, Li G, He Y. The prognostic significance of the prognostic nutritional index in cancer: a systematic review and meta-analysis. J Cancer Res Clin Oncol. 2014;140(9):1537–1549. doi:10.1007/s00432-014-1714-3
14. Ma M, Liu Y, Liu F, et al. Relationship between prognostic nutrition index and New York Heart Association classification in patients with coronary heart disease: a RCSCD-TCM study. J Inflamm Res. 2022;15:4303–4314.
15. Xie X, Chen Y, Gan W, et al. Relationship between prognostic nutritional index and new-onset atrial fibrillation in patients with acute ST-elevation myocardial infarction following percutaneous coronary intervention. Int Heart J. 2023;64(4):543–550. doi:10.1536/ihj.22-555
16. Hatem E, Aslan O, Demirci EE, et al. Relationship between prognostic nutritional index and contrast-associated acute kidney injury in patients with non-ST segment elevation myocardial infarction undergoing coronary angiography. Angiology. 2023;74(7):672–679. doi:10.1177/00033197221131920
17. Dong X, Wang B, Chen S, et al. Association between prognostic nutritional index and contrast-associated acute kidney injury in patients complicated with chronic kidney disease and coronary artery disease. J Interv Cardiol. 2021;2021:2274430. doi:10.1155/2021/2274430
18. Yang WT, Yin L, Xu HY, et al. Analysis of risk factors in acute myocardial infarction patients with a family history of coronary heart disease in China and its relationship with early-onset myocardial infarction. Chin Circ J. 2025;40(4):367–373.
19. National Health Commission of the People’s Republic of China. Dietary and nutritional guidelines for adults with hypertension (2023 edition). Gen Pract Clin Educ. 2023;21(6):484–485,507.
20. Ge JB, Xu YJ, Wang C, editors.. Internal Medicine.
21. Joint Expert Committee on the Revision of the Chinese Guidelines for Lipid Management. Chinese Guidelines for Lipid Management. Beijing: People’s Medical Publishing House; 2023:92.
22. Liu TD, Zheng YY, Tang JN, et al. Prognostic nutritional index as a novel predictor of long-term prognosis in patients with coronary artery disease after percutaneous coronary intervention. Clin Appl Thromb Hemost. 2022;28:10760296221103271. doi:10.1177/10760296221103271
23. Wu TT, Pan Y, Zhi XY, et al. Association between extremely high prognostic nutritional index and all-cause mortality in patients with coronary artery disease: secondary analysis of a prospective cohort study in China. BMJ Open. 2024;14(6):e079954. doi:10.1136/bmjopen-2024-079954
24. Raposeiras Roubín S, Abu Assi E, Cespón Fernandez M, et al. Prevalence and prognostic significance of malnutrition in patients with acute coronary syndrome. J Am Coll Cardiol. 2020;76(7):828–840. doi:10.1016/j.jacc.2020.06.058
25. Clark AL, Sze S. Impact of malnutrition using geriatric nutritional risk index in heart failure with preserved ejection fraction. JACC Heart Fail. 2019;7(8):676–677. doi:10.1016/j.jchf.2019.05.007
26. Chien SC, Chandramouli C, Lo CI, et al. Associations of obesity and malnutrition with cardiac remodeling and cardiovascular outcomes in Asian adults: a cohort study. PLoS Med. 2021;18(6):e1003661. doi:10.1371/journal.pmed.1003661
27. Wolf D, Ley K. Immunity and inflammation in atherosclerosis. Circ Res. 2019;124(2):315–327. doi:10.1161/CIRCRESAHA.118.313591
28. Roche M, Rondeau P, Singh NR, Tarnus E, Bourdon E. The antioxidant properties of serum albumin. FEBS Lett. 2008;582(13):1783–1787. doi:10.1016/j.febslet.2008.04.057
29. Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8–12. doi:10.1016/j.ejim.2018.04.014
30. Arques S. Serum albumin and cardiovascular disease: state-of-the-art review. Ann Cardiol Angeiol. 2020;69(4):192–200. doi:10.1016/j.ancard.2020.07.012
31. Kremer H, Baron-Menguy C, Tesse A, et al. Human serum albumin improves endothelial dysfunction and survival during experimental endotoxemia: concentration-dependent properties. Crit Care Med. 2011;39(6):1414–1422. doi:10.1097/CCM.0b013e318211ff6e
32. Lam FW, Cruz MA, Parikh K, Rumbaut RE. Histone induced platelet aggregation is inhibited by normal albumin. Thromb Res. 2013;132(1):69–76. doi:10.1016/j.thromres.2013.04.018
33. Paar M, Rossmann C, Nusshold C, et al. Anticoagulant action of low, physiologic, and high albumin levels in whole blood. PLoS One. 2017;12(8):e0182997. doi:10.1371/journal.pone.0182997
34. Cohen S, Danzaki K, MacIver NJ. Nutritional effects on T-cell immunometabolism. Eur J Immunol. 2017;47(2):225–235. doi:10.1002/eji.201646423
35. Sandrini L, Ieraci A, Amadio P, et al. Impact of acute and chronic stress on thrombosis in healthy individuals and cardiovascular disease patients. Int J Mol Sci. 2020;21(21):7818. doi:10.3390/ijms21217818
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Combined Effect of the Systemic Immune-Inflammation Index and Aortic Valve Calcification on Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease
Li M, Li M, Wang Z, Zhang Y
Journal of Inflammation Research 2024, 17:8375-8384
Published Date: 7 November 2024
A Machine Learning Model Integrating Tongue Image Features and Myocardial Injury Markers Predicts Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease
Zhou M, Li J, Lim J, Xiao X, Xia Y, Wang Q, Xu Z
International Journal of General Medicine 2025, 18:3739-3765
Published Date: 5 July 2025
Machine Learning Models for Identifying the Risk of Chronic Kidney Disease in Patients with Coronary Heart Disease: A Retrospective Study
He T, Zhao J, Hou L, Su K, Li Y
International Journal of General Medicine 2025, 18:7327-7340
Published Date: 5 December 2025
Predictive Value of NLRP3 Inflammasome Activation for Unstable Plaques and Major Adverse Cardiovascular Events in Coronary Heart Disease
Liu Y, Guo X, Pan J, Jin J, Li J, Hou Y, Wang M, Bai J, Fan Y
Journal of Inflammation Research 2026, 19:550023
Published Date: 13 January 2026
Comparison of FINDRISC and the Framingham Model for Predicting CHD Risk: Results from the Kharameh Cohort Study
Hamedi A, Seif M, Sharifi MH, Rezaianzadeh A, Lashkardoost H, Baberi F, Hassanzadeh J
Vascular Health and Risk Management 2026, 22:619033
Published Date: 14 July 2026