Back to Journals » Vascular Health and Risk Management » Volume 22
Comparison of FINDRISC and the Framingham Model for Predicting CHD Risk: Results from the Kharameh Cohort Study
Authors Hamedi A ![]() , Seif M, Sharifi MH, Rezaianzadeh A, Lashkardoost H, Baberi F, Hassanzadeh J
, Seif M, Sharifi MH, Rezaianzadeh A, Lashkardoost H, Baberi F, Hassanzadeh J
Received 22 April 2026
Accepted for publication 29 June 2026
Published 14 July 2026 Volume 2026:22 619033
DOI https://doi.org/10.2147/VHRM.S619033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Konstantinos Tziomalos
Andishe Hamedi,1 Mozhgan Seif,2 Mohammad Hossein Sharifi,3 Abbas Rezaianzadeh,4 Hossein Lashkardoost,5 Fatemeh Baberi,1 Jafar Hassanzadeh6
1Student Research Committee, Department of Epidemiology, Shiraz University of Medical Sciences, Shiraz, Iran; 2Non-Communicable Diseases Research Center, Department of Epidemiology, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran; 3Research Center for Traditional Medicine and History of Medicine, Non-Communicable Diseases Research Center, Shiraz University of Medical Sciences, Shiraz, Iran; 4Colorectal Research Center, Department of Community Medicine, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran; 5Department of Public Health, North Khorasan University of Medical Sciences, Bojnurd, Iran; 6Department of Epidemiology, Research Centre for Health Sciences, Institute of Health, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence: Jafar Hassanzadeh, Department of Epidemiology, Research Centre for Health Sciences, Institute of Health, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran, Tel +989177208941, Email [email protected]
Background: Coronary heart disease is a leading cause of death worldwide, making early risk identification essential. This study compares the predictive performance of FINDRISC and the Framingham model in the Kharameh Cohort.
Methods: This prospective cohort study included 9,469 participants aged 40– 70 years from the Kharameh cohort (a branch of the PERSIAN study) who were free of CHD at baseline and were followed for 6 years to identify incident CHD events. Data on FINDRISC components, as well as laboratory and demographic variables, were collected at enrollment. Logistic regression models were developed using the total FINDRISC score and its individual items, and their predictive performance was compared with the Framingham non‑laboratory risk score using 10‑fold cross‑validation and metrics including AUC‑ROC, sensitivity, and specificity.
Results: During a six‑year follow‑up of 9,469 participants (mean age 51.6 years, 55.6% female), 540 incident CHD events (5.7%) were identified. The total FINDRISC score was significantly higher in individuals who developed CHD (11.35 vs. 9.59, P< 0.001). However, the total FINDRISC score alone showed weak discriminatory power (AUC=58.6%, 95% CI: 55.9– 61.3%). An item-based FINDRISC model demonstrated improved performance (AUC=71%, 95% CI: 68.9– 73%), and further enhancement with gender, systolic blood pressure, and total cholesterol yielded the highest predictive accuracy (AUC=75.2%, 95% CI: 73%– 77%). The non‑laboratory Framingham risk score (AUC=73.3%, 95% CI: 71.4– 75.1%) showed similar discriminatory performance compared with the enhanced item‑based FINDRISC models.
Conclusion: The enhanced item-based FINDRISC model, incorporating gender and systolic blood pressure showed comparable performance to the Framingham non-laboratory model, providing a simple, accessible screening tool for the Iranian population.
Keywords: coronary heart disease, risk prediction, FINDRISC, Framingham risk score
Introduction
Cardiovascular diseases (CVDs), particularly coronary heart disease (CHD), remain the leading cause of mortality worldwide with deaths increasing from 12.1 million in 1990 to 18.6 million in 2019.1,2 According to global reports, CVD have been responsible for about 17.7 million deaths worldwide in recent years, of which about 7.4 million cases were due to coronary artery disease.3 In Iran, the disease pattern is similar to the global trend. According to national reports, approximately 160,000 deaths from heart disease are recorded annually, and approximately 40% of the country’s total mortality is related to this group of diseases.4 Evidence also shows that Iran, as a middle-income country in the region, has a high incidence rate of cardiovascular disease mortality, and information on risk prediction models in regional populations is still limited.5 Early identification of individuals at high risk is therefore a critical component of preventive medicine and public health strategies, especially given that many major risk factors such as hypertension, smoking, dyslipidemia, and metabolic disorders are modifiable.6
Risk prediction models have been widely developed to estimate the likelihood of cardiovascular events and support clinical decision-making. Traditional approaches such as the Framingham risk model incorporate established clinical and biochemical variables to estimate long-term cardiovascular risk and have been extensively validated in diverse populations. These models rely on known determinants including blood pressure, cholesterol levels, and lifestyle behaviors, reflecting the multifactorial etiology of atherosclerosis and CHD.6 Nevertheless, their performance may vary across populations due to demographic, genetic, and environmental differences, highlighting the need for evaluation and recalibration in regional cohorts.7,8 Although the Framingham Risk Score has been widely used as a practical and clinically relevant tool for predicting cardiovascular risk, its accuracy may be limited in certain populations and it does not incorporate some established risk factors, highlighting the need for further validation and refinement in different populations.9 In Iranian populations, differences in lifestyle, prevalence of risk factors, and baseline cardiovascular risk may influence the predictive accuracy of international models, highlighting the importance of evaluating these tools in local cohort studies.10
Alongside classical cardiovascular risk models, non-invasive screening tools developed for metabolic risk assessment have gained attention for their potential utility in cardiovascular prediction.11 The Finnish Diabetes Risk Score (FINDRISC) is a questionnaire-based instrument originally designed to identify individuals at risk of type 2 diabetes using anthropometric and lifestyle indicators.12 Although FINDRISC was initially developed for diabetes risk assessment, several studies have suggested that it may also predict cardiovascular outcomes because many of its components are closely related to cardiometabolic risk.11 Since metabolic disorders share common pathophysiological pathways with cardiovascular disease, including obesity, insulin resistance, and dyslipidemia.13 Metabolic syndrome and related metabolic abnormalities have been consistently associated with a significantly higher risk of cardiovascular disease. Such tools may offer accessible and cost-effective alternatives for early risk identification, particularly in resource-limited settings. Previous longitudinal studies have shown that higher FINDRISC scores are associated not only with incident diabetes but also with increased risk of coronary heart disease, stroke, and all-cause mortality.11 Their simplicity and reliance on self-reported or easily obtainable measures make them attractive for large epidemiological studies and primary care screening programs.
Population-specific studies allow comparison of predictive tools and their applicability. However, evidence comparing a simple questionnaire-based metabolic risk score with a traditional cardiovascular prediction model in Iranian populations remains limited. This study evaluates the performance of FINDRISC versus the Framingham model for predicting CHD risk in the Iranian Kharameh Cohort, aiming to inform tailored prevention strategies.
Methods
Study Design and Population
This prospective cohort study utilized data from the Kharameh cohort, a branch of the Prospective Epidemiological Research Studies in Iran (PERSIAN).14 The design and objectives of the PERSIAN cohort have been previously described. Baseline enrollment was conducted in 2014, and a total of 10,663 individuals aged 40–70 years from Kharameh, southern Iran, were recruited (participation rate: 97.3%).
For the present analysis, participants with a self‑reported history of coronary heart disease (CHD) at baseline—including prior myocardial infarction or angina—were excluded (n = 1,194). The final study population comprised 9,469 individuals free of CHD at baseline. Participants were followed for a median of 6 years, and incident CHD events were recorded over six follow-up phases. During the follow‑up period, participants were contacted annually and invited to attend follow‑up assessments. Information on hospital admissions, physician diagnoses, and major health events was collected through interviews and review of medical records. Loss to follow‑up was minimal due to the structured follow‑up system of the PERSIAN cohort. All participants had complete information for the key variables used in the analysis; therefore, no exclusions were made due to missing data.
Ethics and Inclusion Criteria
The study protocol was approved by the Ethics Committee of Shiraz University of Medical Sciences, and written informed consent was obtained from all participants. Inclusion criteria were age 40–70 years and residence in Kharameh for at least 9 months before enrollment. Exclusion criteria at baseline included diagnosed CHD, mental disorders, untreated acute illnesses, and unwillingness to participate or attend clinical examinations.
Data Collection and Measurements
Data were obtained from the Kharameh Cohort Study records. Demographic information (age, gender, marital status, occupation), lifestyle factors (smoking, opium use, alcohol consumption, physical activity, fruit/vegetable intake), and medical history (hypertension, diabetes, family history of CHD and diabetes) were extracted from standardized questionnaires completed at baseline.
Anthropometric data, including height, weight, and waist circumference, were recorded at baseline. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Blood pressure measurements, taken twice in a seated position after 10 minutes of rest, were also retrieved from the cohort records.
Fasting blood glucose (FBS), total cholesterol (CHOL), and triglycerides (TG) values were collected from baseline laboratory data. All laboratory analyses had been performed at the central laboratory of the Kharameh Cohort using standard enzymatic methods.
Definition of Outcomes and Key Variables
CHD incidence was defined as the first occurrence of coronary heart disease, including myocardial infarction or angina, during follow‑up. Incident CHD events were identified during follow‑up through participant interviews, review of hospital records, and physician diagnoses recorded in the cohort database. Reported events were verified by trained physicians based on available medical documentation, including hospital discharge summaries, diagnostic tests, and clinical records.
Diabetes mellitus was defined as a self‑reported physician diagnosis, use of antidiabetic medication, or FBS ≥ 126 mg/dL.
Hypertension was defined as SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, or use of antihypertensive medication.
FINDRISC Score and Its Components
The Finnish Diabetes Risk Score (FINDRISC) questionnaire was used to assess the baseline risk profile. This instrument comprises eight items: age, BMI, waist circumference, physical activity, daily consumption of fruits/berries/vegetables, history of antihypertensive drug treatment, history of high blood glucose, and family history of diabetes. Each item contributes a weighted score, and the total score ranges from 0 to 26. The FINDRISC score is divided into five categories:
Very low: score <7, individual predicted to have a 1% probability of developing the disease.
Low: score 7–11, individual predicted to have a 4% probability of developing the disease.
Moderate: score 12–14, individual predicted to have a 16% probability of developing the disease.
High: score 15–20, individual predicted to have a 33% probability of developing the disease.
Very high: score >20, individual predicted to have a 50% probability of developing the disease.
Two Modeling Approaches Were Employed
Model 1 (Total Score): The total FINDRISC score was used as a single predictor in logistic regression.
Model 2 (Item‑based): The eight individual FINDRISC items were entered as separate predictors in a multivariable logistic regression, allowing estimation of population‑specific coefficients.
The candidate variables considered for model extension were prespecified based on prior epidemiological evidence and clinical relevance to cardiovascular disease risk. Established cardiovascular risk factors such as systolic blood pressure, smoking status, lipid levels, and glucose have been consistently associated with CHD in previous studies. In addition, lifestyle exposures such as opium use and alcohol consumption were examined due to their relatively high prevalence in Iranian populations and previously reported associations with cardiometabolic outcomes in regional epidemiological studies. Subsequently, demographic and laboratory variables—gender, smoking, SBP, CHOL, FBS, opium use, alcohol consumption, and TG—were added one by one to both models in a stepwise manner to assess incremental predictive value. Variables that did not materially improve model performance (ie, no increase in AUC or F1‑score) were excluded from the final models. Variable selection was guided by changes in model performance metrics (particularly AUC and F1‑score) during cross‑validation in order to reduce unnecessary model complexity and minimize the risk of overfitting. Based on this process, gender, CHOL, and SBP were retained in the extended models, whereas smoking, opium use, alcohol consumption, and FBS were removed.
Framingham Non-Laboratory Risk Score
In addition to the FINDRISC-based models, we evaluated the performance of the non‑laboratory Framingham risk score for predicting incident CHD. This score is designed to estimate 10-year coronary heart disease risk without requiring blood lipid measurements and is based on the following variables: age, gender, systolic blood pressure, smoking status, BMI, diabetes status, and treatment for hypertension. The total score for each participant was calculated using the published algorithm for the non-laboratory-based Framingham model. Its predictive performance was then assessed using logistic regression, first as a total score and then by comparing its components to the enhanced FINDRISC models.
Statistical Analysis
Descriptive statistics were expressed as mean ± standard deviation for continuous variables and frequencies (percentages) for categorical variables. Comparisons between participants with and without incident CHD were performed using independent t‑tests or chi‑square tests, as appropriate.
Logistic regression analysis was used to assess the association between the total FINDRISC score and CHD incidence, with odds ratios (OR) and 95% confidence intervals (CI) reported. For the item‑based model, multiple logistic regression was applied to estimate the independent contribution of each FINDRISC component. Logistic regression was used to model the probability of incident CHD during the follow‑up period. Although Cox proportional hazards models are commonly applied in longitudinal cohort studies, the primary objective of this study was to compare the predictive discrimination of different risk scores for CHD occurrence by the end of the follow‑up period rather than to analyze time‑to‑event dynamics. Because follow‑up completion was high (~97%) and censoring was minimal, logistic regression was considered an appropriate approach for comparing the predictive performance of the evaluated risk models.
Model Development and Validation
All models were developed using logistic regression. To address class imbalance (only 5.7% incident cases), the Synthetic Minority Over‑sampling Technique (SMOTE) was applied to the training data during cross‑validation. SMOTE was applied only to the training datasets within each cross‑validation fold to address class imbalance while preserving the original distribution of the validation data. This approach helps reduce potential bias and limits overfitting that could occur if oversampling were applied to the entire dataset. Model performance was always evaluated using the original non‑resampled validation folds. This strategy was used to prevent information leakage between training and validation datasets and to ensure that model performance estimates were not artificially inflated by oversampling procedures. Model performance was evaluated using 10‑fold stratified cross‑validation repeated on the entire dataset. In each fold, the model was trained on the balanced training set and tested on the original (imbalanced) validation fold.
For the item‑based model, the linear predictor (logit score) for each individual was calculated as:

The predicted probability of CVD was then obtained via the logistic function:

Model Evaluation Metrics
For each model, we computed the confusion matrix elements (true positives [TP], true negatives [TN], false positives [FP], false negatives [FN]), accuracy, precision (positive predictive value), recall (sensitivity), specificity, F1‑score, and the area under the receiver operating characteristic curve (AUC‑ROC). The 95% confidence intervals for AUC were estimated using 1,000 bootstrap resamples of the cross‑validated predictions. Pairwise comparisons of AUC values between competing models were conducted using bootstrap resampling based on the cross‑validated prediction probabilities, and statistical significance was assessed using two‑sided tests.
Software
All analyses were performed using Python version 3.9 (Anaconda Navigator, Jupyter Lab) with the library’s pandas, NumPy, scikit‑learn, imbalanced‑learn, matplotlib, and seaborn.
Results
Among the 9,469 participants free of CHD at baseline, 542 incident CHD events occurred during the six‑year follow‑up period, corresponding to an incidence of 5.7%. The mean age of participants was 51.56 ± 8.05 years, and 55.6% were women. Compared with participants who remained free of CHD, those who developed CHD were older, had a larger waist circumference, higher blood glucose and lipid levels, higher blood pressure, a higher prevalence of diabetes, and a more frequent family history of cardiovascular disease. High‑risk behaviors such as smoking, opium use, and alcohol consumption were also more common among CHD cases, whereas physical activity was less frequent in this group. The demographic and clinical characteristics of the participants are presented in Table 1.
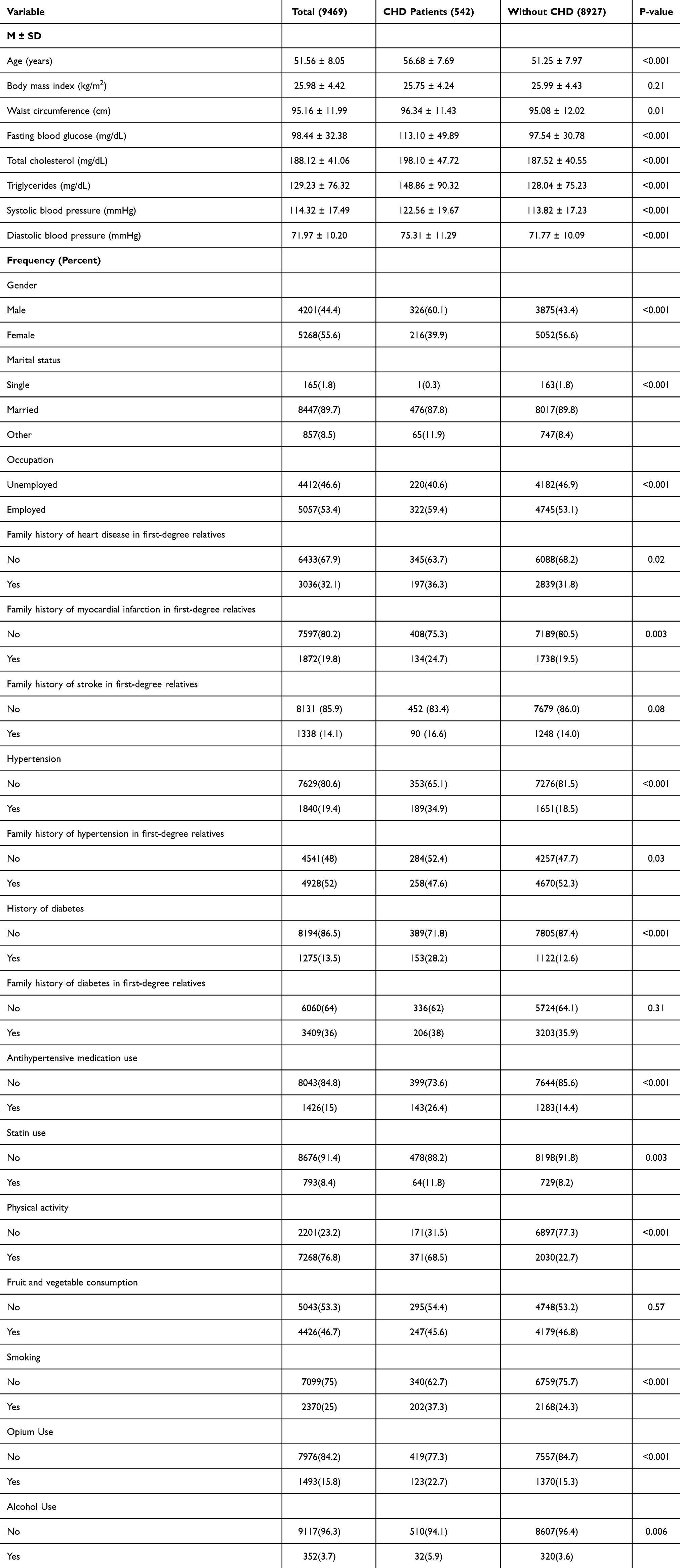 |
Table 1 Demographic and Clinical Characteristics of Participants with and without CHD |
The mean FINDRISC score in the overall population was 9.69 ± 4.90. Among participants free of CHD, the mean FINDRISC score was 9.59 ± 4.84 (n = 8927), whereas among those who developed CHD, it was 11.35 ± 5.55 (n = 542); this difference was statistically significant (P < 0.001).
The distribution of CHD across FINDRISC risk categories is illustrated in Figure 1. The results clearly show that as the FINDRISC score increases, the proportion of individuals developing CHD also rises, with a markedly different distribution pattern between affected and unaffected individuals. In the group without CHD, the frequency was concentrated in the lower score categories. Specifically, 35.3% of individuals had a score below 7, and 31.2% had scores between 7 and 11. In contrast, only 2% of those without CHD fell into the highest risk category (score >20), indicating a low probability of disease in these groups. Among participants who developed CHD, the distribution was completely different. The highest percentages were observed in the higher score categories: 21.2% of cases had scores between 15 and 20, and 19.9% had scores between 12 and 14. Only 25.8% of cases had a score below 7.
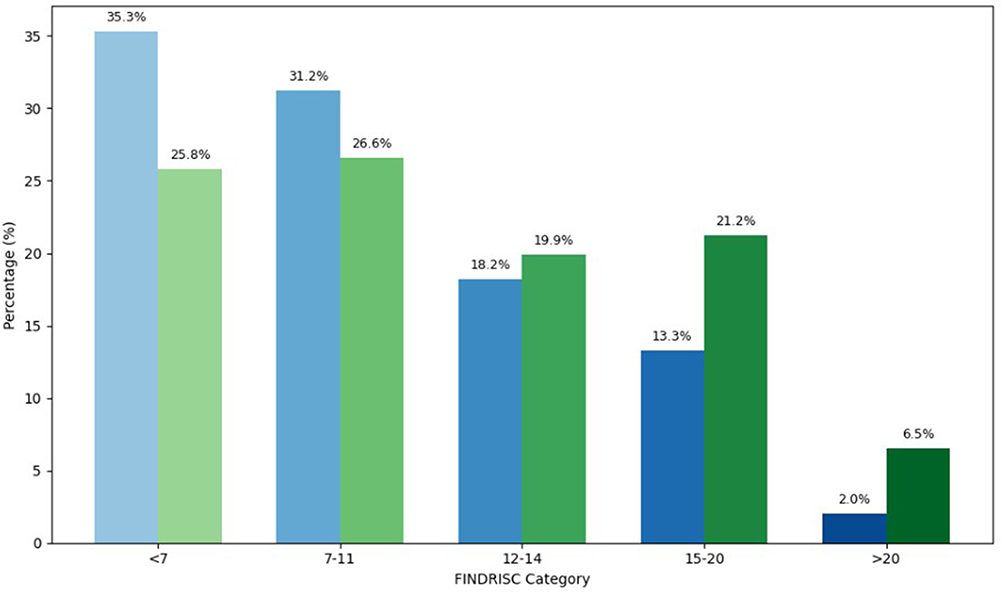 |
Figure 1 Distribution of CHD Incidence by FINDRISC Score Categories. Green bars represent participants with CHD (Yes CHD), while blue bars represent participants without CHD (No CHD). |
To investigate the contribution of each component of the FINDRISC tool in predicting CHD, multiple logistic regression analysis was performed. The results are presented as odds ratios (OR) with 95% confidence intervals (Table 2). Overall, variables such as age, increased waist circumference, use of antihypertensive medication, and a history of high blood glucose were identified as independent risk factors for CHD. In contrast, certain behavioral factors, including physical activity and vegetable consumption, as well as BMI and family history of diabetes, showed non-significant trends toward increased risk.
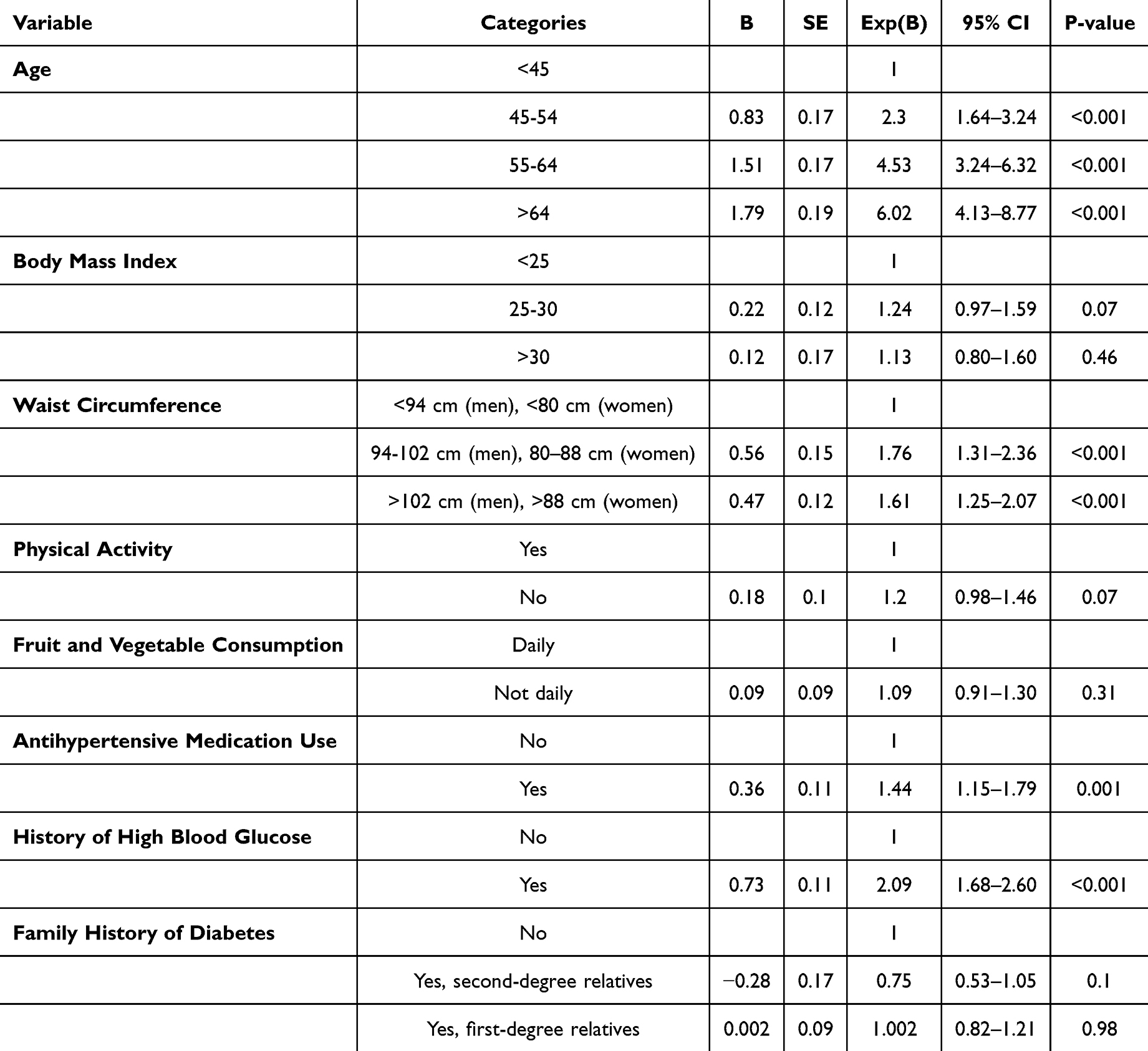 |
Table 2 Results of Multiple Logistic Regression Analysis for FINDRISC Tool Components in Predicting CHD Incidence |
The model’s overall accuracy based on the FINDRISC score was 59.31%. The area under the ROC curve (AUC-ROC) was 58.81%, indicating that the discriminative power of the model was only marginally better than random guessing. We then incorporated demographic and laboratory variables to predict CHD. The results are presented in Table 3.
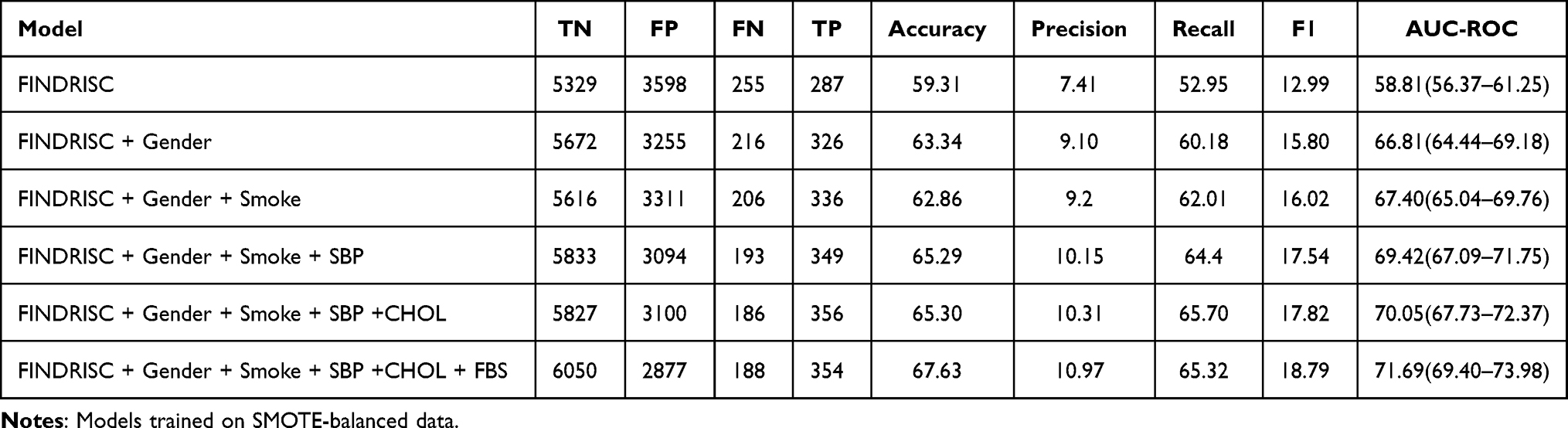 |
Table 3 Performance of FINDRISC Score and Extended Risk Models |
In this stepwise process, other demographic and laboratory variables such as opium use, alcohol consumption, and triglycerides were also evaluated; however, adding them to the model did not significantly improve any of the performance metrics. Notably, the AUCs of these models did not increase compared to the previous step and, in some cases, even decreased slightly. Therefore, these variables were excluded from the final model.
A second model was developed based on the individual components of the FINDRISC questionnaire using logistic regression with population‑specific coefficient estimation. Overall, the item‑based model demonstrated substantially better performance compared to the model based on the total FINDRISC score. Nevertheless, the model required further improvement or combination with other variables for screening applications. Therefore, we incorporated demographic and laboratory variables to predict CHD incidence. The variables were added sequentially in a stepwise manner to evaluate both non‑laboratory and laboratory‑enhanced models. Particular attention was given to models that relied solely on easily obtainable non‑laboratory variables to enable a fair comparison with the non‑laboratory Framingham risk score. In this framework, the model including FINDRISC questionnaire items plus gender and systolic blood pressure (SBP) was considered the primary non‑laboratory enhanced FINDRISC model. The results are presented in Table 4. Based on this analysis, variables that had a positive and significant impact on predicting CHD were retained in the final model, including gender, systolic blood pressure (SBP), and total cholesterol (CHOL). However, it should be noted that the cholesterol‑containing model represents a laboratory‑enhanced version of the FINDRISC‑based model. The improvement in discrimination compared with the non‑laboratory model (Questions + Gender + SBP) was relatively modest. In contrast, smoking, opium use, alcohol consumption, and fasting blood glucose (FBS) were excluded from the final model due to a lack of substantial improvement in evaluation metrics (particularly AUC) (Table 4).
 |
Table 4 Performance of Questions Included in the FINDRISC Risk Assessment Score and Extended Risk Models |
In addition to the FINDRISC-based models, we evaluated the performance of the non‑laboratory‑based Framingham risk score (based on BMI) for predicting incident CHD. The mean Framingham risk score in the overall population was 8.92 ± 4.70. Among participants free of CHD, the mean score was 8.69 ± 4.60 (n = 8927), whereas among those who developed CHD, it was 12.70 ± 4.58 (n = 542); this difference was statistically significant (P < 0.001).
The performance of the logistic regression model based on the non‑laboratory Framingham score shows 68% accuracy. The area under the ROC curve (AUC) was 0.73 (95% CI 0.71–0.75), indicating moderate discriminative ability. These findings indicate that the non‑laboratory Framingham risk score (AUC = 0.73, 95% CI 0.71–0.75) shows a discrimination capacity comparable to that of the non‑laboratory enhanced FINDRISC model consisting of questionnaire items plus gender and systolic blood pressure (AUC = 0.74). The similarity in predictive performance is largely attributable to the presence of systolic blood pressure as a key predictor in both models (Figure 2). The non‑laboratory Framingham model, therefore, performs very similarly to the FINDRISC + Gender + SBP model, both of which rely exclusively on non‑laboratory variables (AUC 0.73 vs. 0.74). This similarity is largely due to the presence of blood pressure as a common variable in both models.
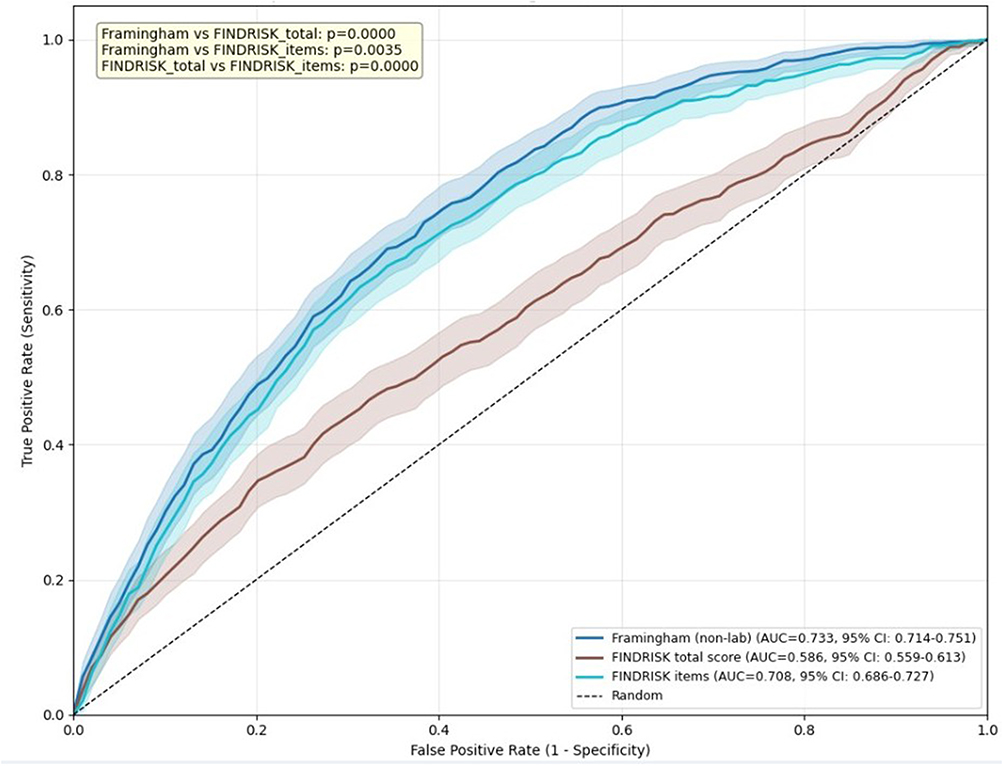 |
Figure 2 Comparison of Predictive Performance: Framingham Non-Laboratory Score vs. FINDRISC Total Score and Its Components. |
Discussion
The present cohort-based analysis evaluated the performance of the FINDRISC tool and compared it with the non-laboratory Framingham model for predicting incident CHD. Over six years of follow-up, the cumulative incidence of CHD reached 5.7%, and individuals who developed CHD were characterized by an adverse metabolic and behavioral profile, including older age, higher central adiposity, dysglycemia, dyslipidemia, hypertension, and unhealthy lifestyle behaviors. These findings are consistent with the established multifactorial risk profile of coronary disease, in which metabolic, hemodynamic, and behavioral factors commonly cluster and are associated with higher CHD risk.15
Age and waist circumference emerged as strong independent predictors in the FINDRISC component analysis, consistent with extensive epidemiologic evidence showing that vascular aging and visceral adiposity are strongly associated with cardiometabolic risk. The observed associations between antihypertensive medication use, elevated glucose history, and CHD incidence further underscore the predictive relevance of cardiometabolic dysregulation-related variables in this cohort. Machine-learning analyses derived from large cardiovascular datasets have similarly identified glycemia and blood pressure variables as dominant contributors to mortality and coronary outcomes prediction, highlighting their consistent predictive relevance across analytical approaches.16
Additionally, lifestyle exposures such as smoking and physical inactivity were more prevalent among CHD cases in our cohort, supporting the importance of behavioral risk modification. Evidence from population-scale cohorts shows that adherence to healthy lifestyle factors markedly reduces cardiovascular mortality, particularly when combined with pharmacologic prevention strategies, reinforcing the clinical relevance of behavioral risk profiling in prediction models.17 Although FINDRISC was originally developed for type 2 diabetes screening, its components overlap with cardiometabolic risk determinants; hence, its extension to cardiovascular prediction has been explored in several settings. In our analysis, score distribution patterns demonstrated clear risk stratification across categories. However, discrimination was modest (AUC ≈ 0.59), indicating limited standalone screening utility. This is not unexpected because FINDRISC was not calibrated for cardiovascular outcomes and omits key hemodynamic and lipid parameters. Studies examining the application of diabetes and cardiovascular risk scores across populations similarly emphasize that instruments developed for one outcome or population often show reduced predictive value when transferred without recalibration.18
Importantly, when demographic and laboratory variables were incorporated, predictive performance improved substantially (AUC ≈ 0.72). This improvement illustrates the importance of integrating metabolic and clinical measurements with questionnaire-based tools. Comparable research shows that hybrid or machine-learning–enhanced models consistently outperform simple score-based tools in cardiovascular prediction due to their capacity to incorporate nonlinear relationships and multi-dimensional risk features.19 Importantly, when restricting the comparison to models that rely exclusively on non‑laboratory variables, the FINDRISC‑based model, including questionnaire items, gender, and systolic blood pressure, demonstrated a discrimination ability that was very similar to that of the non‑laboratory Framingham model. This finding suggests that a simplified FINDRISC‑based approach using readily obtainable clinical variables may provide predictive performance comparable to established non‑laboratory risk scores.
Within the framework of predictive performance evaluation, the area under the receiver operating characteristic curve (ROC–AUC) serves as a key measure of discrimination, enabling comparison between clinically based and questionnaire-based risk assessment tools. Evidence indicates that classical risk-factor–based models such as the Framingham score generally demonstrate moderate to good discriminative ability across diverse populations, and they retain acceptable performance even after recalibration in non-Western settings.20 Furthermore, studies developing CHD prediction models have reported that multivariable clinical models typically yield AUC values around 0.70; for example, a nomogram-based CHD prediction model reported AUCs ranging from 0.703 to 0.706, indicating moderate discrimination comparable to standard approaches.21 These observations are consistent with the findings of the present study, in which the Framingham model exhibited superior discrimination compared with the crude FINDRISC score. It should also be noted that the Framingham model was originally developed to estimate 10-year CHD risk, whereas the outcome in the present study was assessed over approximately 6 years of follow-up. Therefore, the comparison presented here should be interpreted as a comparison of discriminative performance within this cohort rather than a direct validation of equivalent absolute risk predictions across identical time horizons. External validation studies have similarly reported AUC ranges of approximately 0.63–0.83 for the Framingham model.22 Nevertheless, research has shown that Framingham models may overestimate cardiovascular risk in certain populations and therefore require population-specific recalibration.23 Heterogeneity in predictive performance across outcome types and gender has also been documented, with discrimination often stronger for fatal than nonfatal events.24 This observation aligns with the present findings, where incorporating gender and systolic blood pressure into FINDRISC-based models substantially improved discriminative performance.
In this research, the questionnaire-based FINDRISC model demonstrated measurable predictive capacity for incident CHD, and its performance improved substantially when individual components and limited clinical variables were incorporated. Importantly, the predictive performance of the item-based FINDRISC model approached that of the non-laboratory Framingham risk score. The Framingham risk score has long been regarded as a benchmark cardiovascular prediction model because it was explicitly designed around coronary endpoints and incorporates hemodynamic and demographic determinants such as blood pressure, age, and gender. Consequently, its stronger odds ratio and moderate discrimination in this study were expected. Nevertheless, the enhanced FINDRISC item-based model achieved comparable AUC values after incorporating key demographic and clinical parameters, suggesting that much of the predictive advantage of Framingham stems from shared core variables rather than structural differences in modeling approach. This interpretation aligns with validation studies demonstrating that simplified non-laboratory cardiovascular risk models relying on anthropometric and behavioral variables can achieve discrimination comparable to classical scores when applied to large community populations and appropriately calibrated.25 Importantly, questionnaire-based tools offer several practical advantages. They require minimal resources, are suitable for primary screening, and allow rapid implementation in population-level epidemiologic surveillance. Evidence from comparative risk-score research indicates that non-invasive screening instruments can function effectively as first-stage stratification tools, identifying higher-risk individuals who may then undergo more comprehensive clinical assessment. This tiered approach is particularly relevant in low-resource or large-scale cohort contexts where laboratory testing may not be feasible for all participants. Our findings further suggest that predictive convergence between FINDRISC and Framingham arises from overlapping cardiometabolic constructs embedded in both tools. Variables such as age, central adiposity, and blood pressure likely capture overlapping cardiometabolic processes that are closely associated with both diabetes and coronary disease.26 When these constructs are explicitly modeled rather than aggregated into a single summary score, their predictive signal becomes more apparent, improving discrimination and narrowing the performance gap with cardiovascular-specific models.
Collectively, these findings suggest that while FINDRISC may provide an accessible preliminary screening approach in resource-limited settings, its use alone for CHD prediction is insufficient. Incorporating blood pressure, lipid measures, and demographic factors substantially enhances predictive accuracy and brings performance closer to established cardiovascular models. The comparable performance observed between the enhanced FINDRISC and non-laboratory Framingham models highlights an important practical implication: population-specific recalibration of simple tools may achieve acceptable discrimination without full reliance on complex laboratory-based frameworks.
This study has several notable strengths. First, it is based on a prospective cohort design with longitudinal follow-up, allowing temporal assessment of baseline risk factors in relation to incident CHD and strengthening the validity of the predictive analysis. Second, the simultaneous evaluation of two conceptually distinct risk assessment approaches—a questionnaire-based tool (FINDRISC) and a non-laboratory clinical model (Framingham)—enabled a comprehensive comparison of prediction strategies relevant to both community screening and clinical settings. Third, predictive performance was assessed not only through ROC–AUC but also using the F1 score, which is particularly informative in datasets with class imbalance. Because incident CHD events represented a minority outcome in this cohort, reliance on AUC alone could overestimate model utility; incorporating the F1 metric provided a more application-oriented evaluation by balancing precision and recall and better reflecting classification performance in real-world screening scenarios.
Despite these strengths, several limitations should be acknowledged. The follow-up duration, although sufficient to capture incident cases, may still be relatively short for fully characterizing long-term cardiovascular risk trajectories. Residual confounding remains possible, especially from unmeasured socioeconomic or behavioral determinants. Some predictors were derived from self-reported questionnaire data, introducing potential reporting bias that may have attenuated effect estimates. In addition, fasting glucose did not remain statistically significant in the final multivariable model and was excluded during model selection. This finding should be interpreted cautiously rather than as evidence of a lack of biological relevance. Several methodological and epidemiologic factors may explain this result, including collinearity with related metabolic variables, mediation through anthropometric or blood pressure parameters, limited variability within the study population, or insufficient statistical power to detect independent effects after adjustment. Moreover, glycemic status is partly captured indirectly through other cardiometabolic constructs embedded in both FINDRISC and Framingham variables. Similar observations have been reported in risk modeling studies where glucose-related predictors lose independent significance once correlated metabolic factors are included. Future analyses incorporating repeated glycemic measurements, alternative glycemic markers, or larger event counts may clarify its independent contribution.
In addition, model evaluation in the present study primarily focused on discrimination metrics, and calibration assessment and external validation in independent populations were beyond the scope of the current analysis, which may limit the generalizability of the findings. Another methodological consideration is that logistic regression was used to evaluate predictive performance, whereas survival analysis methods such as Cox proportional hazards models may provide additional insights into time‑to‑event relationships in longitudinal cohort data. Furthermore, although several models demonstrated acceptable predictive performance, the discriminative ability of some models was moderate, which should be considered when interpreting their clinical applicability. Future studies incorporating calibration analyses, external validation in independent cohorts, survival‑based modeling approaches, and longer follow‑up periods or pooled multi‑cohort datasets could enhance the robustness, generalizability, and clinical utility of these prediction models.
Conclusion
The total FINDRISC score alone demonstrated limited predictive value for CHD risk in the Iranian population. However, modeling the individual FINDRISC questionnaire components substantially improved predictive performance. Notably, a simplified non‑laboratory FINDRISC‑based model that incorporated questionnaire items together with gender and systolic blood pressure achieved a discriminative ability comparable to that of the non‑laboratory Framingham model. The addition of laboratory variables such as total cholesterol provided only modest further improvement in model performance. These findings suggest that a simplified non‑laboratory FINDRISC‑based approach using readily obtainable clinical variables may have potential as a preliminary CHD risk assessment strategy, particularly in settings with limited access to laboratory testing. However, because calibration assessment and external validation were not performed in the present study, further research in independent populations is required before considering broader clinical or public health implementation of the proposed model.
Data Sharing Statement
Data are available by request to corresponding author.
Ethics Approval and Consent to Participate
The PERSIAN Cohort Study is being conducted across 18 geographical regions in Iran. The study was approved by the Ethics Committee of the Ministry of Health and Medical Education. All procedures were carried out in accordance with the Helsinki Declaration and the Iranian national guidelines for research ethics. This research is part of a Ph.D. dissertation in Epidemiology conducted under the supervision of Dr. Jafar Hassanzadeh. Additionally, the Ethics Committee of Shiraz University of Medical Sciences has approved this study (IR.SUMS.SCHEANUT.REC.1403.056).
Consent for Publication
Not applicable. This manuscript does not contain any individual person’s data, images, or identifying information requiring consent for publication.
Acknowledgment
The authors would like to express their sincere gratitude to the participants of the Kharameh Cohort Study for their invaluable contribution and commitment. We also acknowledge the dedicated efforts of the research staff, field workers, and data management team, whose support made this study possible. Special thanks are extended to the Shiraz University of Medical Sciences for providing institutional support and to the local health authorities in Kharameh for their collaboration in facilitating data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares they have no conflict of interest.
References
1. Shi A, Tao Z, Wei P, Zhao J. Epidemiological aspects of heart diseases. Exp Ther Med. 2016;12(3):1645–15. doi:10.3892/etm.2016.3541
2. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
3. Moradi-Joo E, Nabavi SS, Gholizadeh B, et al. Estimation of the economic burden of cardiovascular diseases in Iran. Comprehens Health Biomed Studies. 2025;3(3):e164904. doi:10.5812/chbs-163797
4. Sarrafzadegan N, Mohammmadifard N. Cardiovascular disease in Iran in the last 40 years: prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. Arch Iran med. 2019;22(4):204–210.
5. Fahimfar N, Fotouhi A, Mansournia MA, et al. Prediction of cardiovascular disease mortality in a Middle Eastern country: performance of the Globorisk and score functions in four population-based cohort studies of Iran. Int J Health Policy Manag. 2020;11(2):210.
6. Miah J, Ca DM, Sayed MA, Lipu ER, Mahmud F, Arafat SY, editors. Improving cardiovascular disease prediction through comparative analysis of machine learning models: a case study on myocardial infarction. In:
7. Artigao-Rodenas LM, Carbayo-Herencia JA, Divison-Garrote JA, et al. Framingham risk score for prediction of cardiovascular diseases: a population-based study from Southern Europe. PLoS One. 2013;8(9):e73529. doi:10.1371/journal.pone.0073529
8. Selvarajah S, Kaur G, Haniff J, et al. Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population. Int J Cardiol. 2014;176(1):211–218. doi:10.1016/j.ijcard.2014.07.066
9. Hemann BA, Bimson WF, Taylor AJ. The Framingham Risk Score: an appraisal of its benefits and limitations. Am Heart Hospit J. 2007;5(2):91–96. doi:10.1111/j.1541-9215.2007.06350.x
10. Mirzaei M, Mirzaei M. Agreement between Framingham, IraPEN and non-laboratory WHO-EMR risk score calculators for cardiovascular risk prediction in a large Iranian population. J Cardiovasc Thoracic Res. 2019;12(1):20. doi:10.34172/jcvtr.2020.04
11. Silventoinen K, Pankow J, Lindström J, Jousilahti P, Hu G, Tuomilehto J. The validity of the Finnish Diabetes Risk Score for the prediction of the incidence of coronary heart disease and stroke, and total mortality. Eur J Prevent Cardiol. 2005;12(5):451–458.
12. Hamedi A, Seif M, Sharifi MH, Rezaianzadeh A, Hassanzadeh J. Performance of the finnish diabetes risk score in screening for undiagnosed type 2 diabetes among adults without prior diagnosis: a Kharameh Cohort Study, Iran. Primary Care Diabetes. 2025;19:517–521. doi:10.1016/j.pcd.2025.07.001
13. Silveira Rossi JL, Barbalho SM, Reverete de Araujo R, Bechara MD, Sloan KP, Sloan LA. Metabolic syndrome and cardiovascular diseases: going beyond traditional risk factors. Diabetes/Metab Res Rev. 2022;38(3):e3502. doi:10.1002/dmrr.3502
14. Poustchi H, Eghtesad S, Kamangar F, et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Am J Epidemiol. 2018;187(4):647–655. doi:10.1093/aje/kwx314
15. Achim A, Péter OÁ, Cocoi M, et al. Correlation between coronary artery disease with other arterial systems: similar, albeit separate, underlying pathophysiologic mechanisms. J Cardiovasc Develop Dis. 2023;10(5):210. doi:10.3390/jcdd10050210
16. Yuda E, Kaneko I, Hirahara D. Machine-learning insights from the Framingham Heart Study: enhancing cardiovascular risk prediction and monitoring. Appl Sci. 2025;15(15):8671. doi:10.3390/app15158671
17. Peng W, Bai X, Yang Y, et al. Healthy lifestyle, statin, and mortality in people with high CVD risk: a nationwide population-based cohort study. Am J Prevent Cardiol. 2024;17:100635. doi:10.1016/j.ajpc.2024.100635
18. Ssekubugu R, Makumbi F, Enriquez R, et al. Cardiovascular (Framingham) and type II diabetes (Finnish Diabetes) risk scores: a qualitative study of local knowledge of diet, physical activity and body measurements in rural Rakai, Uganda. BMC Public Health. 2022;22(1):2214. doi:10.1186/s12889-022-14620-9
19. Mallya P, Henao R, Hong C, et al. Automated data harmonization in clinical research: natural language processing approach. JMIR Format Res. 2025;9:e75608.
20. Sun C, Xu F, Liu X, et al. Comparison of validation and application on various cardiovascular disease mortality risk prediction models in Chinese rural population. Sci Rep. 2017;7(1):43227. doi:10.1038/srep43227
21. Wang M, Wang M, Zhu Q, et al. Development and validation of a coronary heart disease risk prediction model in snorers with hypertension: a retrospective observed study. Risk Manag Healthcare Policy. 2022;Volume 15:1999–2009. doi:10.2147/RMHP.S374339
22. Al-Shamsi S. Performance of the Framingham coronary heart disease risk score for predicting 10-year cardiac risk in adult United Arab Emirates nationals without diabetes: a retrospective cohort study. BMC Fam Pract. 2020;21(1):175. doi:10.1186/s12875-020-01246-2
23. Damen JA, Pajouheshnia R, Heus P, et al. Performance of the Framingham risk models and pooled cohort equations for predicting 10-year risk of cardiovascular disease: a systematic review and meta-analysis. BMC Med. 2019;17(1):109. doi:10.1186/s12916-019-1340-7
24. Motamed N, Khoonsari M, Karbalaie Niya MH, et al. External validity of cardiovascular risk assessment tools in individuals with MASLD (NAFLD): a cohort study. Sci Rep. 2025;15(1):33462. doi:10.1038/s41598-025-07775-z
25. Alemu YM, Alemu SM, Bagheri N, Wangdi K, Chateau D. Discrimination and calibration performances of non-laboratory-based and laboratory-based cardiovascular risk predictions: a systematic review. Open Heart. 2025;12(1):e003147. doi:10.1136/openhrt-2024-003147
26. Klaus JR, Hurwitz BE, Llabre MM, et al. Central obesity and insulin resistance in the cardiometabolic syndrome: pathways to preclinical cardiovascular structure and function. J Cardiometabolic Syndrome. 2009;4(2):63–71. doi:10.1111/j.1559-4572.2008.00038.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Machine Learning Models for Identifying the Risk of Chronic Kidney Disease in Patients with Coronary Heart Disease: A Retrospective Study
He T, Zhao J, Hou L, Su K, Li Y
International Journal of General Medicine 2025, 18:7327-7340
Published Date: 5 December 2025
Prognostic Nutritional Index is Independently Associated with Major Adverse Cardiovascular Events in Patients with Triple - Vessel Disease: A Retrospective Cohort Study
Wang M, Lei Y, Xue Y
International Journal of General Medicine 2026, 19:603394
Published Date: 18 April 2026