Back to Journals » Journal of Inflammation Research » Volume 19
Predictive Value of NLRP3 Inflammasome Activation for Unstable Plaques and Major Adverse Cardiovascular Events in Coronary Heart Disease
Authors Liu Y, Guo X, Pan J, Jin J, Li J ![]() , Hou Y, Wang M, Bai J, Fan Y
, Hou Y, Wang M, Bai J, Fan Y
Received 10 July 2025
Accepted for publication 28 December 2025
Published 13 January 2026 Volume 2026:19 550023
DOI https://doi.org/10.2147/JIR.S550023
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rongxue Wu
Yaping Liu,1 Xiangqian Guo,1 Jiping Pan,1 Jianjian Jin,2 Jing Li,2 Yanjun Hou,3 Mingzhen Wang,3 Jianhua Bai,3 Yan Fan2
1The First School of Clinical Medical, Gansu University of Chinese Medicine, Lanzhou, 730000, People’s Republic of China; 2Department of Cardiology, Gansu Provincial Hospital, Lanzhou, 730000, People’s Republic of China; 3Department of Cardiology, Dongxiang County Hospital, Linxia, 731400, People’s Republic of China
Correspondence: Yan Fan, Email [email protected]
Background: The role of Nod-like receptor protein 3 (NLRP3) inflammasome activation in unstable plaques remains incompletely elucidated. This study aimed to investigate whether the NLRP3 inflammasome and its downstream cytokine IL-1β serve as predictors of unstable plaques and subsequent major adverse cardiovascular events (MACE) in patients with coronary heart disease (CHD).
Methods: The study enrolled 232 patients diagnosed with CHD at Gansu Provincial Hospital between May 2023 and June 2024. Based on standardized plaque vulnerability criteria assessed by intravascular ultrasound (IVUS) or optical coherence tomography (OCT), patients were divided into a stable plaque group (n=143) and an unstable plaque group (n=89). Serum concentrations of NLRP3 and IL-1β were measured using ELISA. During a median follow-up of 14 months (IQR, 7– 20), the primary composite endpoint was MACE, defined as recurrent myocardial infarction, rehospitalization due to heart failure, or all-cause death.
Results: NLRP3 and IL-1β were identified as independent predictors of unstable plaques in CHD (OR=1.002 and 1.030, respectively), demonstrating high predictive value for plaque rupture and erosion (AUCs: 0.817 and 0.727 for rupture; 0.760 and 0.758 for erosion). Furthermore, elevated levels of these biomarkers were independently associated with an increased risk of MACE (HR=1.006 for NLRP3; HR=1.056 for IL-1β). Kaplan-Meier analysis confirmed that patients with high biomarker levels experienced a significantly higher incidence of MACE (log-rank P < 0.001). The high predictive accuracy of both biomarkers for MACE was further substantiated by AUC values of 0.874 (NLRP3) and 0.870 (IL-1β).
Conclusion: NLRP3 inflammasome activation is a key predictor of unstable plaques (including rupture and erosion) and subsequent MACE in CHD patients, highlighting its strong promise as a clinical biomarker for refining risk stratification and guiding future therapies.
Keywords: coronary heart disease, unstable plaques, NLRP3 inflammasome, IL-1β, major adverse cardiovascular events
Introduction
Despite substantial progress in the prevention and treatment of cardiovascular diseases over recent decades, acute coronary syndrome (ACS) remains one of the leading causes of morbidity and mortality worldwide.1 The central pathophysiological mechanism involves thrombosis resulting from unstable atherosclerotic plaques.2 Such vulnerable plaques are pathologically defined by the presence of one or more of the following features: rupture, erosion, or calcified nodules.3–5 These characteristics can be identified by intracoronary imaging techniques including intravascular ultrasound (IVUS) and optical coherence tomography (OCT). Patients often do not exhibit overt symptoms in the early stages, making it challenging to detect the plaques during the subclinical phase. However, screening studies have revealed a 20%–63% prevalence of atherosclerotic plaques among asymptomatic individuals aged 45 to 65.6,7 If left untreated, progressive plaque destabilization with subsequent rupture or mural thrombus formation may lead to vascular occlusion, potentially culminating in thrombotic events such as myocardial infarction or stroke. Therefore, early detection and assessment of unstable plaques hold critical clinical significance in mitigating the risk of major adverse cardiovascular events (MACE). Nevertheless, there are few non-invasive biomarkers available in clinical practice for predicting unstable plaques and MACE.
The NOD-like receptor protein 3 (NLRP3) inflammasome is a multimeric protein complex composed of three key components: NLRP3 (the NOD-like receptor family member), ACS (apoptosis-associated speck-like protein containing a CARD), and pro-caspase-1.8 In resting cells, the components as well as their substrates (pro-IL-1β and pro-IL-18) remain at non-detectable baseline levels. Upon exposure to exogenous or endogenous “danger” stimuli, NLRP3 recruits its downstream adaptor protein ACS to assemble the inflammasome complex. This interaction triggers the activation of pro-caspase-1 into active Caspase-1, which subsequently promotes the secretion of IL-1β and IL-18, the pro-inflammatory cytokines. IL-1β and IL-18 exert broad pro-inflammatory effects by inducing the expression of chemokines and adhesion molecules in various cell types. Previous studies have revealed upregulated expression of NLRP3 inflammasome components in atherosclerotic plaques and peripheral blood mononuclear cells of patients with atherosclerosis, and the expression levels may be related to disease severity.9,10 These findings implicate NLRP3 in the development of atherosclerotic plaques and link it to plaque vulnerability.
Although previous studies have demonstrated that the NLRP3 inflammasome plays a critical role in the pathogenesis of various diseases,11 there is limited clinical research on whether it can serve as a biomarker for evaluating and predicting unstable plaques. This study examined the serum levels of NLRP3 and its downstream inflammatory factor IL-1β in patients with atherosclerosis, aiming to identify new non-invasive biomarkers for unstable plaques and MACE in coronary heart disease (CHD).
Material and Methods
Patients
A total of 232 patients were enrolled in this study, who were diagnosed with CHD by coronary angiography (CAG) in the Department of Cardiology, Gansu Provincial Hospital between May 2023 and June 2024. The inclusion criteria were as follows: (1) age ≥18 years; (2) CAG-confirmed CHD with ≥50% stenosis in at least one major coronary artery; (3) CAG followed by either IVUS or OCT examination; (4) complete clinical data available. Patients with acute and chronic infectious diseases, severe liver or kidney disease, malignant tumors, or autoimmune or chronic wasting diseases were excluded. The study was approved by the Ethics Committee of Gansu Provincial Hospital (Approval No.: 2023–272) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Clinical Data Collection
Patient baseline data were obtained from the Hospital Information System of Gansu Provincial Hospital. The dataset comprised demographic information, medical history, laboratory parameters, as well as echocardiographic, coronary angiographic, and intravascular imaging (IVUS/OCT) data.
Current smokers were defined as patients who had smoked at least 100 cigarettes during their lifetime and were still smoking within the past 30 days.12 The criterion for hypertension was measured using a standard electronic sphygmomanometer after 10 min of rest in the supine position, systolic blood pressure 140 mmHg or diastolic blood pressure 90 mmHg, or the current use of antihypertensive medication.13 Hyperlipidemia was defined as total cholesterol (TC)>5.17 mmol/L, or/and low-density lipoprotein cholesterol (LDL-C)>3.12 mmol/L, or receiving antilipidemic treatment.14 Type 2 diabetes mellitus was defined as fasting plasma glucose 7.0 mmol/L, or 2-h post-load plasma glucose 11.1 mmol/L, or if a patient was receiving anti-diabetic treatment.15
Coronary angiography was performed according to the standard method. There were two specialized physicians who read the images and decided the results. The Gensini score was used to assess the severity of coronary artery stenosis due to its close correlation with lesion severity and computational convenience. IVUS or OCT was carried out in accordance with the standard operating procedures, and the images were analyzed and interpreted by two independent professional engineers. Unstable plaques are defined by IVUS/OCT by the presence of key pathological features: plaque rupture, characterized by fibrous cap disruption, cavity formation, and intraluminal thrombus; plaque erosion, identified by thrombus adhesion over an intact fibrous cap; or calcified nodule, featuring irregular protruding calcification, fracture, and surface thrombus.
Detection of NLRP3 and IL-1β Serum Levels
Fasting peripheral venous blood (10 mL) was collected from each patient within 24 hours of admission. Blood samples were centrifuged at 3000 r/min for 6 minutes at 4°C, and the supernatant serum obtained was stored in a −80°C refrigerator for subsequent analysis. Serum levels of the NLRP3 inflammasome and the cytokine IL-1β were measured using commercial enzyme-linked immunosorbent assay (ELISA) kits (NLRP3: YJ981244; IL-1β: YJ301122; YUANJU BIO, China) according to the manufacturers’ instructions.
Follow-Up
The patients were followed for a median of 14 months (IQR, 7–20 months) through telephone interviews, outpatient clinic visits, or hospital medical record reviews. The occurrence of MACE was documented, including all-cause mortality, recurrent myocardial infarction, and rehospitalization due to heart failure.
Statistical Analysis
Statistical analysis was conducted using SPSS 25.0 software. Data conforming to normal distribution,  ± SD were presented, and intergroup differences were analyzed using the independent samples t-test. Non-normally distributed data were presented as medians with interquartile ranges (Q1, Q3), and non-parametric tests were utilized for intergroup comparisons. Categorical data were expressed as percentages, with between-group differences evaluated by Pearson’s chi-square test or Fisher’s exact test. Logistic regression was employed to analyze the relationship between NLRP3 and unstable plaques, and Cox proportional hazards regression modeling was performed to identify prognostic factors influencing clinical outcomes in patients with CHD. Survival curves were plotted using the Kaplan-Meier method to examine differences in MACE incidence across different serum NLRP3 and IL-1β levels. The predictive value of NLRP3 for unstable plaque, its three specific subtypes, and MACEs was evaluated through ROC curve analysis.
± SD were presented, and intergroup differences were analyzed using the independent samples t-test. Non-normally distributed data were presented as medians with interquartile ranges (Q1, Q3), and non-parametric tests were utilized for intergroup comparisons. Categorical data were expressed as percentages, with between-group differences evaluated by Pearson’s chi-square test or Fisher’s exact test. Logistic regression was employed to analyze the relationship between NLRP3 and unstable plaques, and Cox proportional hazards regression modeling was performed to identify prognostic factors influencing clinical outcomes in patients with CHD. Survival curves were plotted using the Kaplan-Meier method to examine differences in MACE incidence across different serum NLRP3 and IL-1β levels. The predictive value of NLRP3 for unstable plaque, its three specific subtypes, and MACEs was evaluated through ROC curve analysis.
Results
Comparison of Baseline Characteristics Between Stable and Unstable Plaque Groups
According to their IVUS or OCT results, the 232 CHD patients were classified into two groups: the stable plaque group (n=143) and the unstable plaque group (n=89). The baseline characteristics of the patients in the stable and unstable plaque groups are shown in Tables 1 and 2. The unstable plaque group had significantly higher hypertension prevalence, white blood cell (WBC) count, blood urea nitrogen level, high-sensitivity troponin I (hs-TnI) level, Gensini score, NLRP3 level, and IL-1β level. Other clinical characteristics showed no statistically significant differences between the two groups.
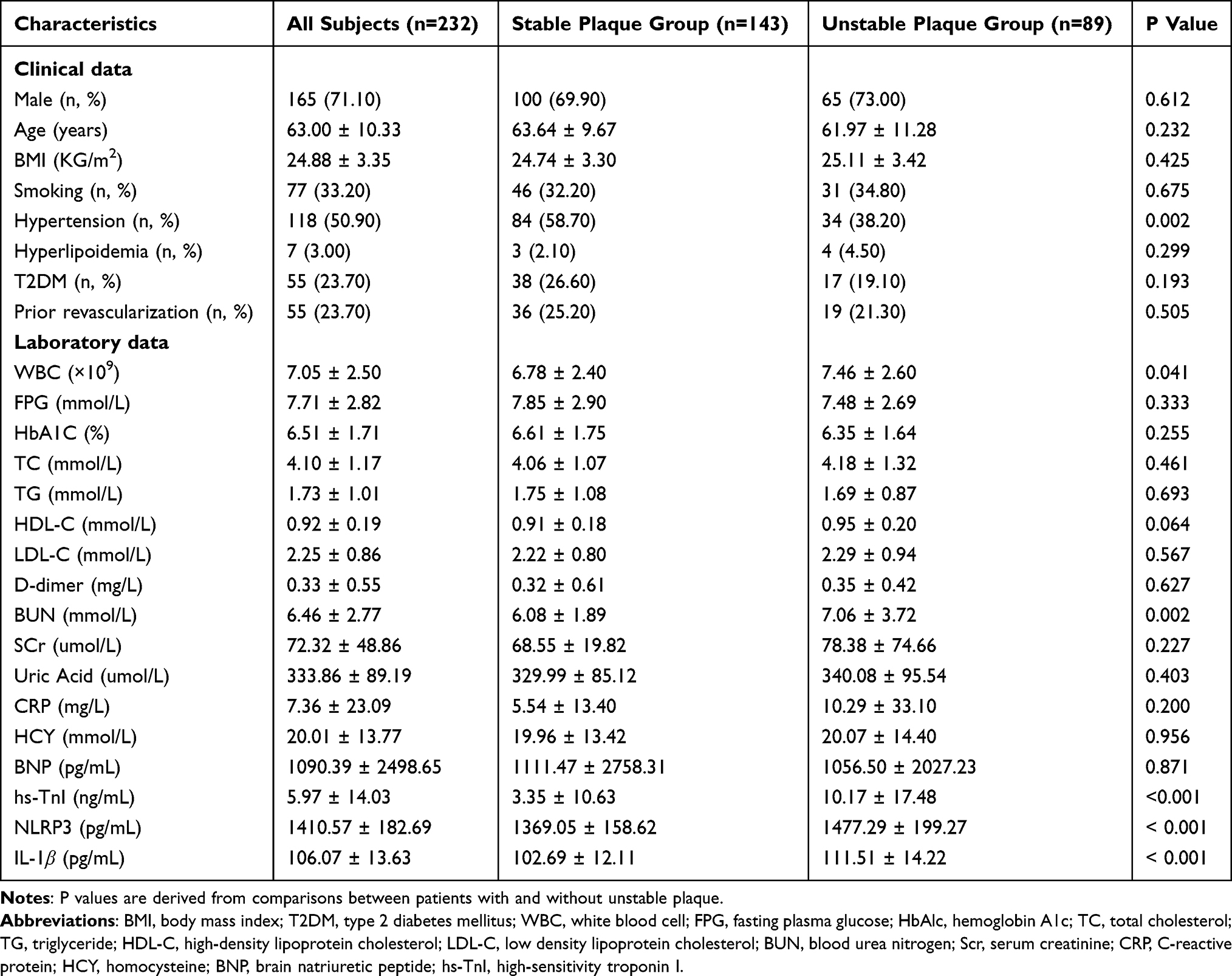 |
Table 1 Comparison of Clinical and Laboratory Data Between the Stable Plaque and Unstable Plaque Groups |
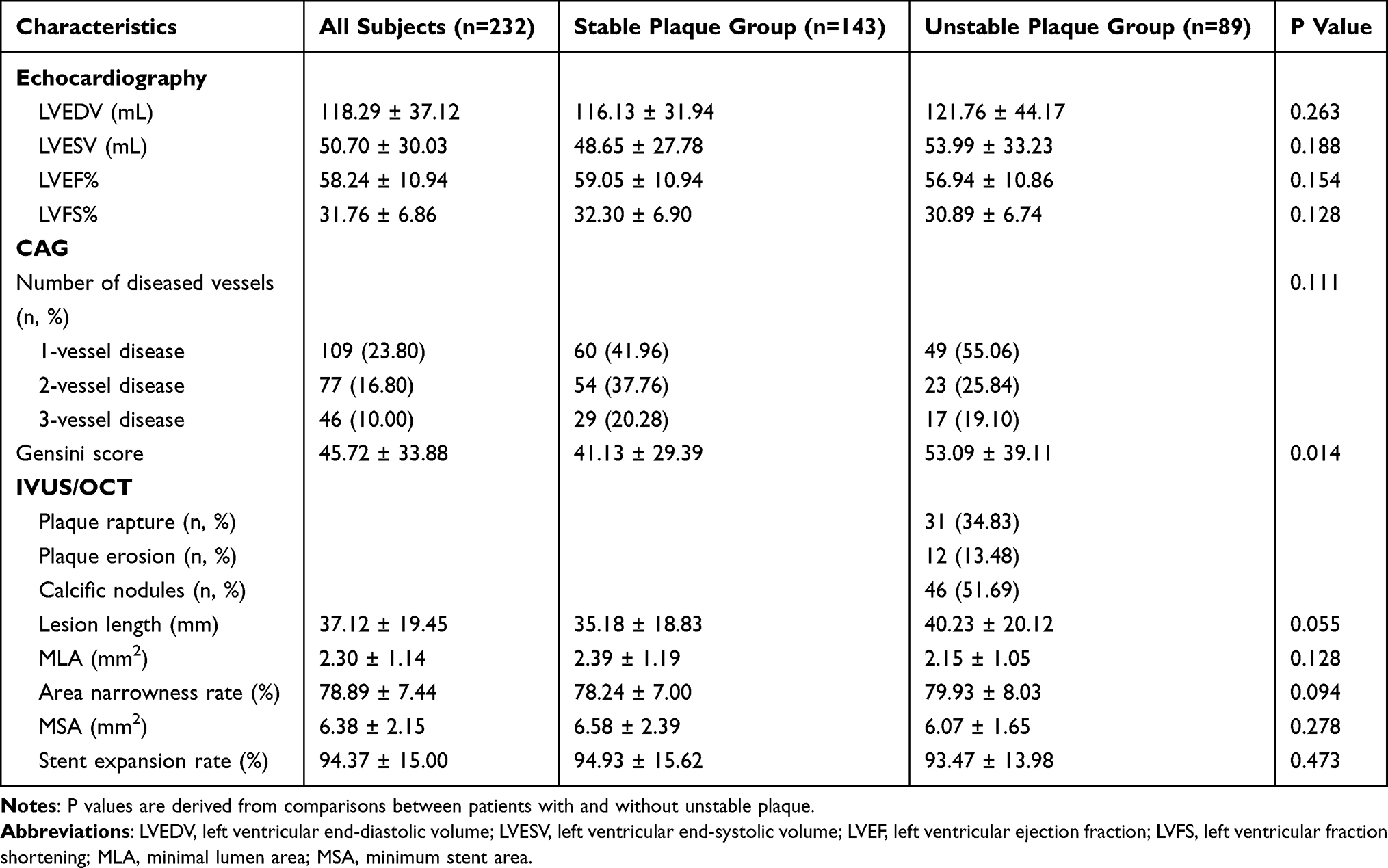 |
Table 2 Comparison of Imaging Characteristics Between the Stable Plaque Group and the Unstable Plaque Group |
Factors Associated with Unstable Plaques
Spearman’s rank correlation analysis revealed a moderate-to-strong positive correlation between the serum IL-1β level and NLRP3 inflammasome activity in CHD patients (ρ=0.570, P<0.001, 95% CI :0.483–0.647). Binary logistic regression analysis was performed to identify factors associated with unstable plaques. Occurrence of unstable plaques (no=0, yes=1) was set as the dependent variable, and the covariates included the characteristics with statistically significant differences in the baseline data analysis, namely, history of hypertension, WBC count, BUN level, hs-TnI level, Gensini score, NLRP3 level, and IL-1β level, as covariates. After adjusting for the aforementioned risk factors, NLRP3 (OR=1.002, 95% CI:1.000–1.004, P<0.05) and IL-1β (OR=1.030, 95% CI:1.002–1.058, P<0.05) remained independent risk factors for the development of unstable plaques in CHD patients. Table 3 summarizes the results of the univariate and multivariate logistic regression analyses.
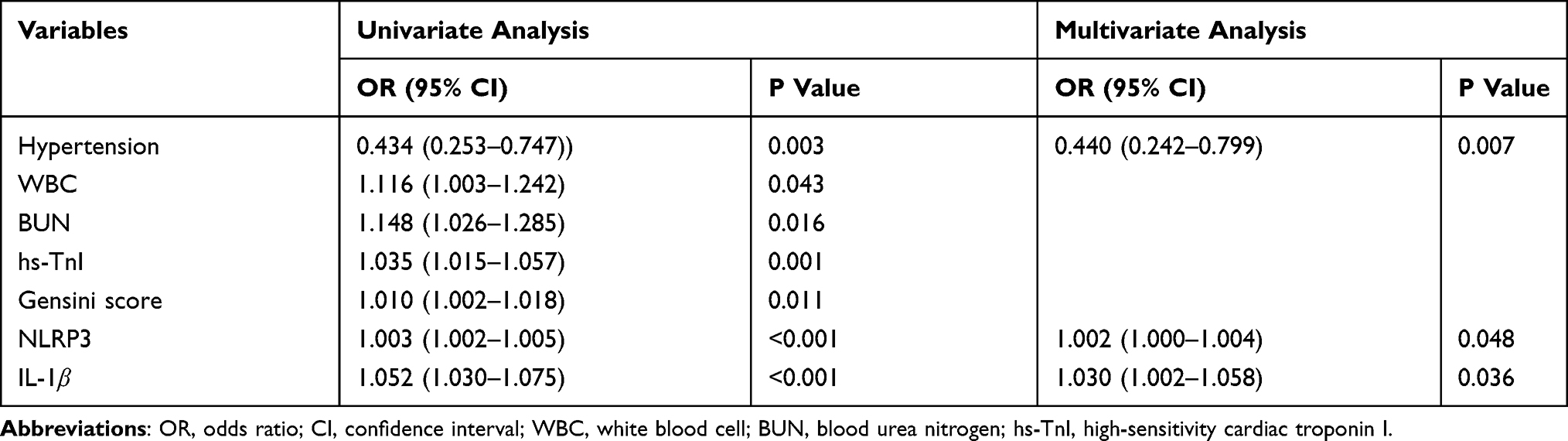 |
Table 3 Association of Risk Factors with Unstable Plaque in CHD Patients |
Predictive Value of NLRP3 and IL-1β for Unstable Plaques
The ROC curve analysis demonstrated that both NLRP3 and IL-1β showed predictive capacity for unstable plaques, with AUC values of 0.662 and 0.680, sensitivities of 36.00% and 61.80%, specificities of 98.60% and 71.30%, and the optimal cutoff values of 1608.31 pg/mL and 111.30 pg/mL, respectively (Figure 1A). For the prediction of plaque rupture, NLRP3 and IL-1β exhibited AUC values of 0.817 and 0.727, respectively. The corresponding sensitivities were 71.00% and 93.50%, the specificities were 90.50% and 43.80%, and the cutoff values were 1671.81 pg/mL and 115.20 pg/mL, respectively (Figure 1B). For predicting plaque erosion, the two factors showed AUC values of 0.760 and 0.758, sensitivities of 58.30% and 75.00%, specificities of 93.02% and 74.10%, and cutoff values of 1583.13 pg/mL and 109.05 pg/mL (Figure 1C). In terms of calcified nodules, the AUC values of NLRP3 and IL-1β were 0.430 and 0.523, respectively (Figure 1D). These results demonstrate that both NLRP3 and IL-1β serve as independent risk factors for plaque rupture and plaque erosion, suggesting their potential clinical utility in evaluating atherosclerotic plaque vulnerability.
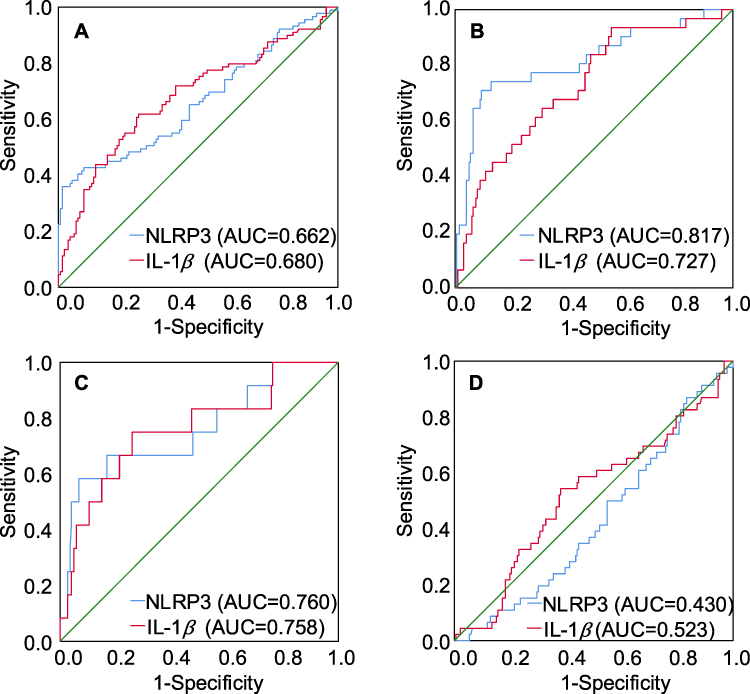 |
Figure 1 ROC curves of NLRP3 and IL-1β for predicting unstable plaques and specific subtypes. (A) All unstable plaques, (B) Plaque rupture, (C) Plaque erosion, (D) Calcified nodules. |
Comparison of Clinical Characteristics Between Patients with and without MACE
Over a median follow-up of 14 months (IQR 7–20 months), 25 (10.78%) patients had MACE, including 4 cases of all-cause death, 13 cases of recurrent myocardial infarction and 8 cases of heart failure readmission. The baseline characteristics of the patients with or without MACE are demonstrated in Tables 4 and 5. The patients with MACE were older, higher WBC, SCr, BNP, hs-TnI, multivessel lesions, Gensini score, LVEDV and LVESV. Moreover, the level of LVEF and LVFS was lower in patients with MACE. It should be noted that a significantly higher unstable plaque distribution as well as NLRP3 and IL-1β level was observed in the patients with MACE as compared with those without MACE.
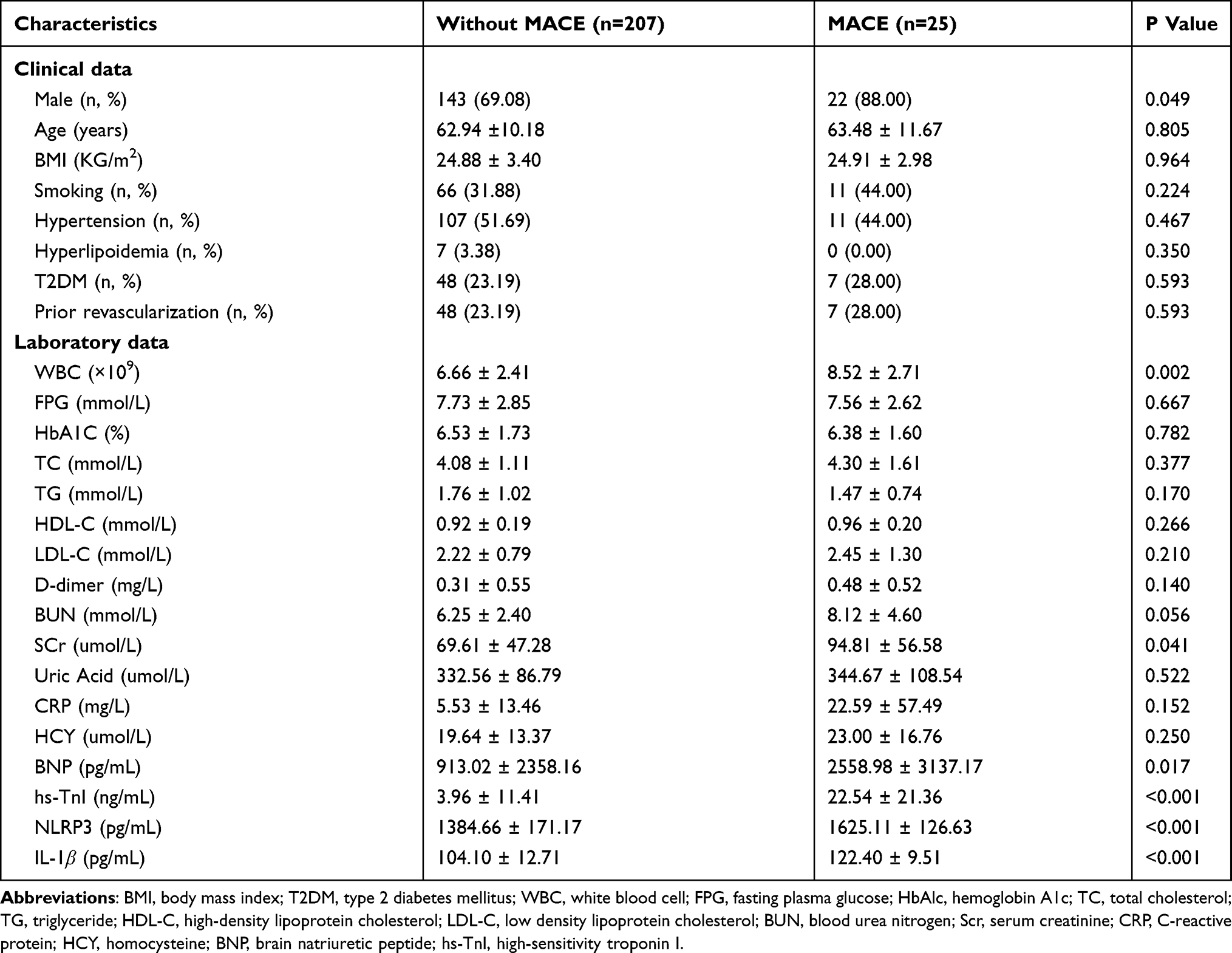 |
Table 4 Comparison of Clinical and Laboratory Data Between Patients with and without MACE |
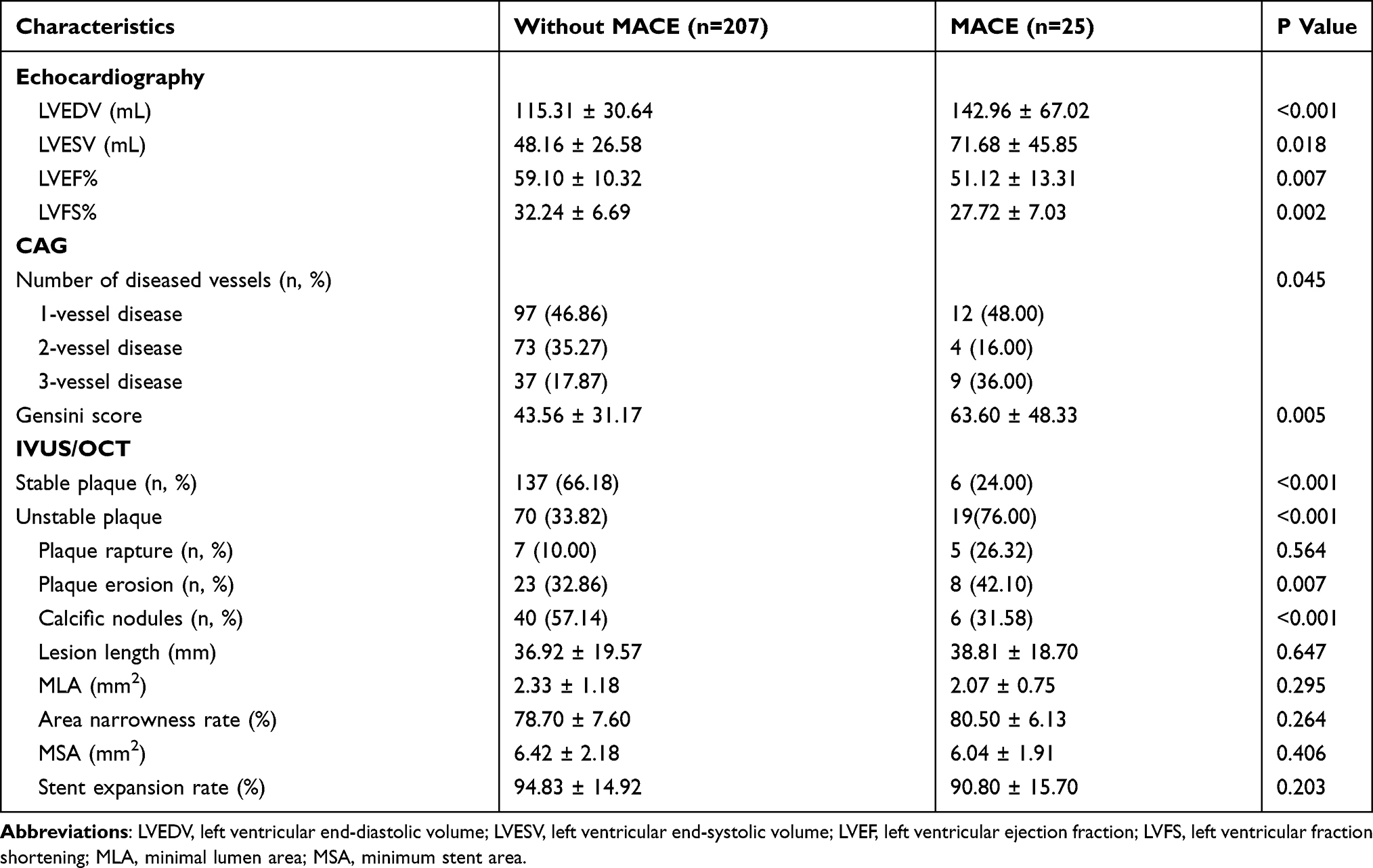 |
Table 5 Comparison of Imaging Characteristics Between Patients with and without MACE |
Factors Associated with MACE
Cox regression analysis was performed to identify predictive factors for MACE. Table 6 summarizes the results of univariate and multivariate Cox proportional-hazard regression analyses. Significant predictors included WBC, SCr, hs-TnI, CK-MB, LVEDV, LVEF, NLRP3, and IL-1β. After adjusting for the aforementioned risk factors, NLRP3 (HR=1.006, 95% CI:1.002–1.011, P<0.05) and IL-1β (HR=1.056, 95% CI:1.011–1.104, P<0.05) remained to be independent risk factors for the occurrence of MACE.
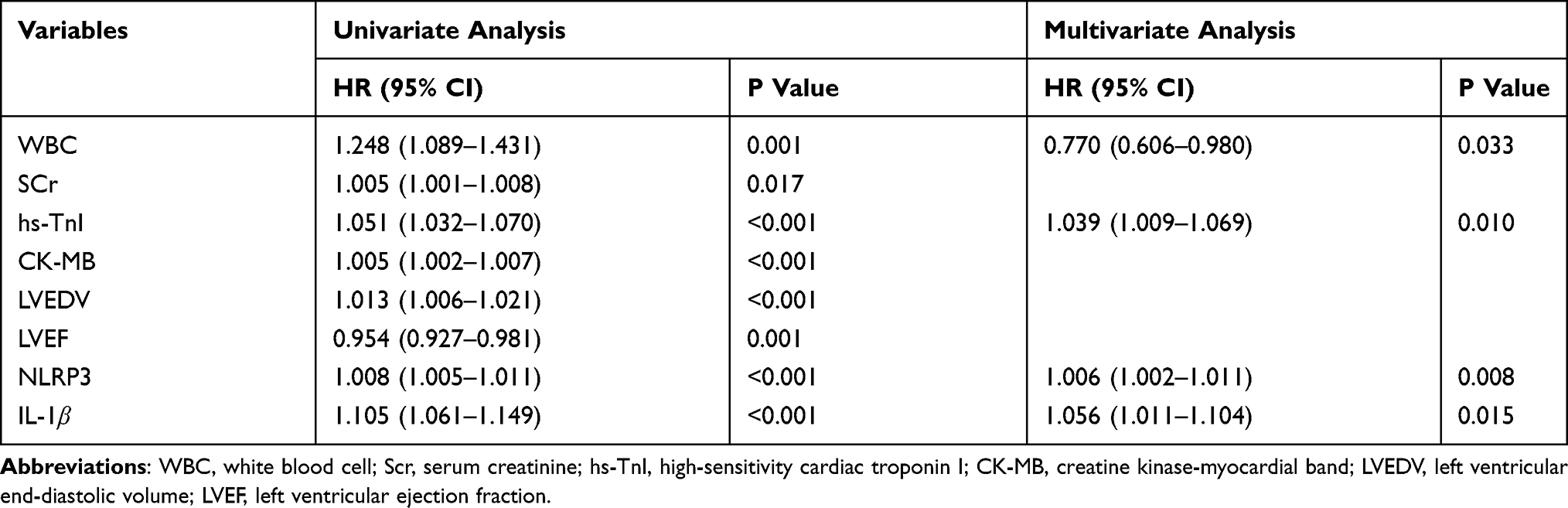 |
Table 6 Association of Risk Factors with MACE in CHD Patients |
Event-Free Survival
Based on the median serum NLRP3 level, patients were divided into two groups: the low NLRP3 group (≤1521.51 pg/mL) and the high NLRP3 group (>1521.51 pg/mL). Kaplan-Meier survival curves demonstrated significant differences between the groups. The cumulative risk of MACE increased with the increase of serum NLRP3 level (Figure 2A). Likewise, the patients were divided into a low IL-1β group (≤112.30 pg/mL) and a high IL-1β group (>112.30 pg/mL). The survival curves showed a similar tendency: an increased risk of MACE with the rise of the IL-1β level (Figure 2B). Log-rank test showed a highly significant difference between the curves for different NLRP3 levels (log-rank χ2 = 37.67, P<0.001) and those for different IL-1β levels (log-rank χ2 = 32.45, P<0.001), suggesting that these two inflammatory markers are significantly associated with the cumulative risk of MACE.
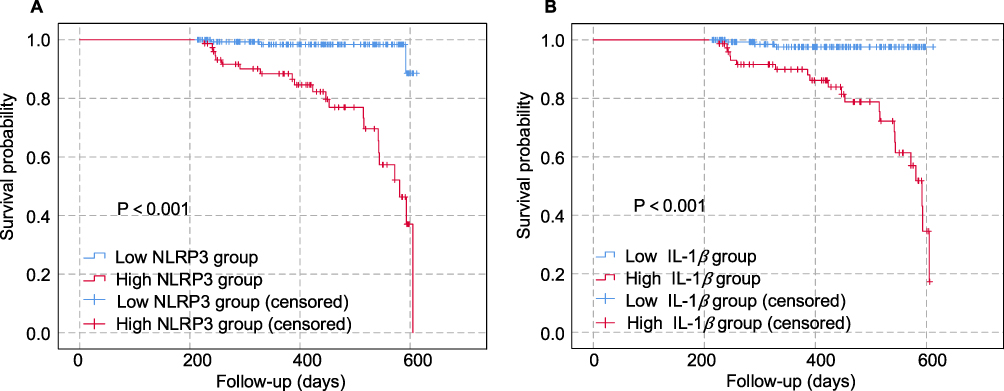 |
Figure 2 Kaplan–Meier analysis of MACE by serum levels of (A) NLRP3 and (B) IL-1β. |
Prognostic Value of NLRP3 and IL-1β for MACE
The predictive value of NLRP3 and IL-1β for clinical prognosis of patients with CHD was assessed by ROC curve analysis. The AUC values for NLRP3 and IL-1β were 0.874 and 0.870, respectively. The sensitivities were 0.800 and 0.880, the specificities were 0.860 and 0.821, and the cutoff values were 1563.98 pg/mL and 116.39 pg/mL, respectively (Figure 3). These findings indicate that both NLRP3 and IL-1β exhibit predictive value for MACE in CHD patients.
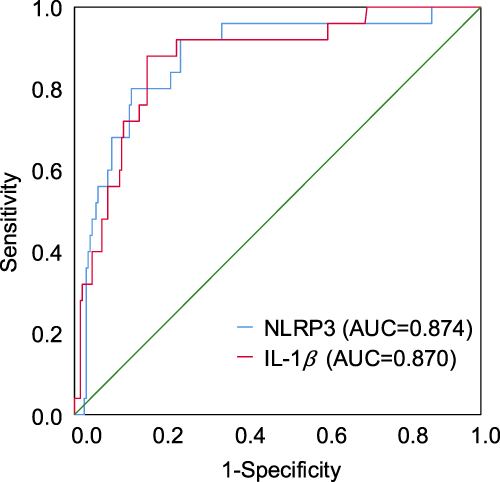 |
Figure 3 ROC curve analysis of serum NLRP3 and IL-1β for predicting MACE in CHD patients. |
Discussion
To our knowledge, this is the first study to demonstrate the predictive value of the NLRP3 inflammasome and its downstream inflammatory factor IL-1β for clinical outcomes in CHD patients with unstable plaques. NLRP3 and IL-1β are independent risk factors for unstable plaques, especially plaque rupture and plaque erosion. Moreover, elevated NLRP3 and IL-1β serum levels result in a significant increase in the risk of MACE in CHD patients.
The role of the NLRP3 inflammasome in coronary atherosclerosis was first reported by Duewell et al in 2010.16 Subsequent research further confirmed the association between NLRP3 inflammasome and the disease. The studies of Afrasyab et al10 and Zhu et al17 demonstrated a significant positive correlation between the level of NLRP3 and the severity of coronary atherosclerosis, and they revealed a markedly elevated NLRP3 expression in peripheral blood monocytes of patients with ACS. Currently, the role of local and systemic inflammation in the development of atherosclerosis is well acknowledged.18 Immune-inflammatory responses and oxidative stress are recognized as the primary drivers for atherosclerotic plaque formation and instability.19–21 The NLRP3 inflammasome plays a pivotal role in atherosclerosis and is associated with the severity of coronary artery disease.10,22 However, there is no published evidence establishing NLRP3 as a biomarker for predicting vulnerable plaques in CHD patients. This cohort study demonstrates the prognostic value of NLRP3 for vulnerable plaque phenotypes in CHD. Using predefined thresholds, levels ≥1583.13 pg/mL and ≥1671.81 pg/mL effectively identified patients at significantly increased risk for plaque erosion and rupture, respectively.
The exact mechanism through which the NLRP3 inflammasome promotes coronary plaque vulnerability has not yet been fully understood. Existing literature indicates that NLRP3 inflammasome activation triggers the secretion of pro-inflammatory cytokines IL-1β and IL-18, thereby markedly exacerbating endothelial cell inflammation and oxidative stress.23 Following endothelial cell dysfunction, monocytes adhere to the lesion sites and differentiate into macrophages. These activated macrophages secrete proteolytic enzymes and matrix metalloproteinases, which degrade the fibrous cap, thus contributing to plaque destabilization and rupture.24 The fact that both the upstream sensor NLRP3 and the downstream effector IL-1β remained independently significant after extensive adjustment provides strong evidence that the “NLRP3–IL-1β” axis is an independent driver of plaque instability in coronary artery disease. Therefore, we speculate that the NLRP3 inflammasome exacerbates plaque vulnerability by augmenting oxidative stress in atherosclerotic lesions.
Recent clinical trials have demonstrated that patients harboring such unstable atherosclerotic plaques exhibit a significantly elevated risk of future MACE.4,25 Autopsy reports on cardiogenic death and acute myocardial infarction have demonstrated that acute thrombosis within coronary atherosclerotic plaques is predominantly caused by three distinct types of plaque pathology: plaque rupture, plaque erosion, and calcified nodules.26 Among the three, plaque rupture is the most common (60%–75% of fatal cases), followed by plaque erosion (25%–40%), and calcified nodules are the least common (approximately 5%).27,28 Clinically, unstable plaques are more prone to rupture compared to stable ones, posing a higher risk for cardiovascular events. In our study, the NLRP3 and IL-1β are identified as independent predictive indicators for MACE in CHD patients, and a high level of serum NLRP3 (≥1563.98 pg/mL in our study) correlates with a significantly elevated MACE risk. In addition, studies have confirmed that activation of the NLRP3 inflammasome and its downstream signaling pathways induces inflammatory responses and oxidative stress, promoting macrophage lipid deposition, migration, and foam cell formation. These processes lead to dysfunction of vascular endothelial cells, thereby promoting platelet activation, aggregation, and subsequent thrombus formation.29–31 All these are closely related to the occurrence, progression, and prognosis of CHD.
Our study establishes a novel, quantifiable biomarker for identifying high-risk coronary plaques, based on a defined serum NLRP3 cut-off level of 1583.13 pg/mL. This finding provides a potential tool for the early detection of plaque vulnerability in clinical practice. The integration of NLRP3 into cardiovascular risk models could enhance precision medicine strategies, enabling targeted early interventions, such as the use of NLRP3 inhibitors. Based on these findings, we propose the implementation of serial serum NLRP3 monitoring in high-risk individuals. For those with elevated levels, a multi-faceted, intensive management strategy should be considered to stabilize plaques and ultimately reduce the risk of major adverse cardiovascular events.
The present study has some limitations. First, the sample size was moderate, with samples all from a single center. Second, the study only tentatively explored the predictive value of the NLRP3 inflammasome in CHD at the serum level. Third, the dynamic trends of inflammatory markers and their long-term relationship with plaque stability still require further elucidation through longitudinal studies. In our future work, we will expand sample size and coverage, and delve into the underlying mechanisms from various perspectives, such as proteomics, genomics and cell biology to further verify the prognostic value of the NLRP3 inflammasome for the long-term risk of cardiovascular adverse events in CHD patients.
Conclusions
Our study demonstrated a significant association between NLRP3 inflammasome activation and the presence of unstable coronary atherosclerotic plaques. Both NLRP3 and IL-1β were identified as independent risk factors for plaque instability and MACE in patients with CHD. These biomarkers exhibit considerable clinical utility in predicting plaque rupture, plaque erosion, and subsequent MACE. These findings may facilitate early identification of high-risk individuals, thereby contributing to improved clinical prognosis.
Data Sharing Statement
The data presented in this study will be provided by the corresponding author upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the scientific research project of Gansu Provincial Hospital (23GSSYD-29).
Disclosure
The authors declare no conflicts of interest.
References
1. Bhatt DL, Lopes RD, Harrington RA. Diagnosis and Treatment of Acute Coronary Syndromes: a Review. JAMA. 2022;327(7):662–12. doi:10.1001/jama.2022.0358
2. Collet JP, Thiele H, Barbatom E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42:1289–1367. doi:10.1093/eurheartj/ehaa575
3. Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-history study of coronary atherosclerosis. New Engl J Med. 2011;364(3):226–235. doi:10.1056/NEJMoa1002358
4. Erlinge D, Maehara A, Ben-Yehuda O, Bøtker HE, Maeng M. Identification of vulnerable plaques and patients by intracoronary near-infrared spectroscopy and ultrasound (PROSPECT II): a prospective natural history study. Lancet. 2021;397(10278):985–995. doi:10.1016/S0140-6736(21)00249-X
5. Prati F, Romagnoli E, Gatto L, et al. Relationship between coronary plaque morphology of the left anterior descending artery and 12 months clinical outcome: the CLIMA study. Eur Heart J. 2020;41(3):383–391. doi:10.1093/eurheartj/ehz520
6. Lloyd-Jones DM, Lewis CE, Schreiner PJ, Shikany JM, Sidney S, Reis JP. The Coronary Artery Risk Development In Young Adults (CARDIA) Study. J Am College Cardiol. 2021;78(3):260–277. doi:10.1016/j.jacc.2021.05.022
7. Fernández-Friera L, Peñalvo JL, Fernández-Ortiz A, et al. Prevalence, Vascular Distribution, and Multiterritorial Extent of Subclinical Atherosclerosis in a Middle-Aged Cohort. Circulation. 2015;131(24):2104–2113. doi:10.1161/circulationaha.114.014310
8. Henao-Mejia J, Elinav E, Strowig T, Flavell RA. Inflammasomes: far beyond inflammation. Nat Immunol. 2012;13(4):321–324. doi:10.1038/ni.2257
9. Paramel Varghese G, Folkersen L, Strawbridge RJ, et al. NLRP3 Inflammasome Expression and Activation in Human Atherosclerosis. J Am Heart Assoc. 2016;5(5):e003031. doi:10.1161/jaha.115.003031
10. Afrasyab A, Qu P, Zhao Y, et al. Correlation of NLRP3 with severity and prognosis of coronary atherosclerosis in acute coronary syndrome patients. Heart Vessels. 2016;31(8):1218–1229. doi:10.1007/s00380-015-0723-8
11. Vandanmagsar B, Youm Y-H, Ravussin A, et al. The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nature Med. 2011;17(2):179–188. doi:10.1038/nm.2279
12. Ryan N, Rinku S, Yao Z, Wodchis W, Rosella L. Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int J Epidemiol. 2020;49(1):113–130. doi:10.1093/ije/dyz078
13. Hypertension RCoCGftPaTo, (China) HA, Care HBoCIEaPAfMaH, et al. Chinese Guidelines for the Prevention and Treatment of Hypertension (2024 revision). Chin J Hypertens. 2024;32(7):603–700. doi:10.16439/j.issn.1673-7245.2024.07.002
14. Yuanlin G, Jianjun L. Highlights of the guidelines for prevention and treatment of dyslipidemia in Chinese adults (Revised Edition 2016). Chin J Front Med Sci. 2017;9(6):12–14. doi:10.12037/YXQY.2017.06-04
15. Society CD. Guideline for the prevention and treatment of diabetes mellitus in China (2024 edition). Chin J Diabetes Mellitus. 2025;17(1):16–139. doi:10.3760/cma.j.cn115791-20241203-00705
16. Duewell P, Kono H, Rayner KJ, et al. NLRP3 inflammasomes are required for atherogenesis and activated by cholesterol crystals. Nature. 2010;464(7293):1357–1361. doi:10.1038/nature08938
17. Zhu J, Wu S, Hu S, et al. NLRP3 inflammasome expression in peripheral blood monocytes of coronary heart disease patients and its modulation by rosuvastatin. Mol Med Rep. 2019;20(2):1826–1836. doi:10.3892/mmr.2019.10382
18. Gallo A, Le Goff W, Santos RD, et al. Hypercholesterolemia and inflammation—Cooperative cardiovascular risk factors. Eur J Clin Invest. 2024;55(1):e14326. doi:10.1111/eci.14326
19. Oikonomou EK, Williams MC, Kotanidis CP, et al. A novel machine learning-derived radiotranscriptomic signature of perivascular fat improves cardiac risk prediction using coronary CT angiography. Eur Heart J. 2019;40(43):3529–3543. doi:10.1093/eurheartj/ehz592
20. Libby P. Inflammation during the life cycle of the atherosclerotic plaque. Cardiovascular Research. 2021;117(13):2525–2536. doi:10.1093/cvr/cvab303
21. Peluso I, Morabito G, Urban L, Ioannone F, Serafi M. Oxidative Stress in Atherosclerosis Development: the Central Role of LDL and Oxidative Burst. Endocrine Metabolic Immune Disorders. 2012;12(4):351–360. doi:10.2174/187153012803832602
22. Zheng F, Xing S, Gong Z, Xing Q. NLRP3 Inflammasomes Show High Expression in Aorta of Patients with Atherosclerosis. Heart Lung & Circulation. 2013;22(9):746–750. doi:10.1016/j.hlc.2013.01.012
23. Syed SN, Weigert A, Brüne B. Sphingosine Kinases are Involved in Macrophage NLRP3 Inflammasome Transcriptional Induction. Int J Mol Sci. 2020;21(13):4733. doi:10.3390/ijms21134733
24. Ajoolabady A, Pratico D, Vinciguerra M, Lip GYH, Franceschi C, Ren J. Inflammaging: mechanisms and role in the cardiac and vasculature. Trends Endocrinol Metab. 2023;34(6):373–387. doi:10.1016/j.tem.2023.03.005
25. Li M, Li M, Wang Z, Zhang Y. The Combined Effect of the Systemic Immune-Inflammation Index and Aortic Valve Calcification on Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease. J Inflamm Res. 2024;17:8375–8384. doi:10.2147/jir.S493735
26. Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons From Sudden Coronary Death. Arteriosclerosis Thrombosis Vasc Biol. 2000;20(5):1262–1275. doi:10.1161/01.ATV.20.5.1262
27. Yahagi K, Kolodgie FD, Otsuka F, et al. Pathophysiology of native coronary, vein graft, and in-stent atherosclerosis. Nat Rev Cardiol. 2016;13(2):79–98. doi:10.1038/nrcardio.2015.164
28. Torii S, Sato Y, Otsuka F, et al. Eruptive Calcified Nodules as a Potential Mechanism of Acute Coronary Thrombosis and Sudden Death. J Am College Cardiol. 2021;77(13):1599–1611. doi:10.1016/j.jacc.2021.02.016
29. Meyers AK, Zhu X. The NLRP3 Inflammasome: metabolic Regulation and Contribution to Inflammaging. Cells. 2020;9(8):1808. doi:10.3390/cells9081808
30. Khoury MK, Yang H, Liu B. Macrophage Biology in Cardiovascular Diseases. Arteriosclerosis Thrombosis Vasc Biol. 2021;41(2):e77–e81. doi:10.1161/atvbaha.120.313584
31. Burger F, Baptista D, Roth A, et al. NLRP3 Inflammasome Activation Controls Vascular Smooth Muscle Cells Phenotypic Switch in Atherosclerosis. Int J Mol Sci. 2021;23(1):340. doi:10.3390/ijms23010340
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Combined Effect of the Systemic Immune-Inflammation Index and Aortic Valve Calcification on Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease
Li M, Li M, Wang Z, Zhang Y
Journal of Inflammation Research 2024, 17:8375-8384
Published Date: 7 November 2024
A Machine Learning Model Integrating Tongue Image Features and Myocardial Injury Markers Predicts Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease
Zhou M, Li J, Lim J, Xiao X, Xia Y, Wang Q, Xu Z
International Journal of General Medicine 2025, 18:3739-3765
Published Date: 5 July 2025
Prognostic Nutritional Index is Independently Associated with Major Adverse Cardiovascular Events in Patients with Triple - Vessel Disease: A Retrospective Cohort Study
Wang M, Lei Y, Xue Y
International Journal of General Medicine 2026, 19:603394
Published Date: 18 April 2026