Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Prevalence of Hyperuricemia and the Relationship Between Serum Uric Acid and Hypertension in New Onset Diabetic Patients: A Cross-Sectional Indian Study
Authors Singh SK ![]() , Singh R, Singh SK, Iquebal MA, Jaiswal S, Singh A
, Singh R, Singh SK, Iquebal MA, Jaiswal S, Singh A
Received 22 February 2022
Accepted for publication 17 May 2022
Published 14 June 2022 Volume 2022:15 Pages 1809—1817
DOI https://doi.org/10.2147/DMSO.S363311
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Shailendra Kumar Singh,1,2 Rina Singh,1 Santosh Kumar Singh,3 Mir Asif Iquebal,4 Sarika Jaiswal,4 Archana Singh5
1Department of Endocrine, Endocrine Clinic, Varanasi, Uttar Pradesh, India; 2Visiting Endocrinologist, Opal Hospital, Varanasi, Uttar Pradesh, India; 3Department of Endocrinology, Endo Centre, Patna, Bihar, India; 4Center for Agricultural Bioinformatics, ICAR-IASRI, New Delhi, India; 5Department of Extension and Communication Management & Home Science, Acharya Narendra Deva University of Agriculture and Technology, Ayodhya, Uttar Pradesh, India
Correspondence: Shailendra Kumar Singh, Email [email protected]
Objective: Prevalence of hyperuricemia (HU) is increasing and it is associated with hypertension, metabolic syndrome, diabetes mellitus (DM), obesity, chronic kidney disease, gout and cardiovascular disease. Elevated level of serum uric acid (SUA) has been shown to be associated with hypertension and diabetes in many countries but there is lack of evidence from India. The aim of this study is to know the prevalence of HU and to know the relationship between SUA and hypertension in newly onset DM.
Methods: This is a cross-sectional study from a tertiary center. A total of 305 (males: 212; females: 93) newly diagnosed diabetic patients were enrolled. All patients were categorized as normotensive (< 140/90) and hypertensive (≥ 140/90) based on ADA criteria. Based on SUA level participants were grouped into 3 tertile (T1: < 4.52; T2: 4.52– 5.64; T3: > 5.64 mg/dl).
Results: The mean age, systolic blood pressure (SBP) and diastolic blood pressure (DBP) of the patients were 46.76 ± 0.61 years, 130.6± 1.06 mmHg and 84.11± 0.63 mmHg, respectively. The mean level of SUA was 5.14± 0.073 mg/dl and level was significantly higher in males compared with females (P < 0.000). Overall prevalence of HU and hypertension was 12.13% and 44.59%, respectively. There was an increase in the prevalence of hypertension across the SUA tertile. SBP and DBP significantly increased across the SUA tertile (P < 0.014 and < 0.001, respectively). A multiple logistic regression analysis revealed that SUA tertile was independently associated with presence of hypertension (P < 0.01).
Conclusion: This first report on the population of the eastern part of India indicates a significant positive relationship between SUA and hypertension among the newly onset Indian diabetic patients. Therefore, routine measurement of SUA is recommended in newly onset hypertensive diabetic patients to prevent HU and its related complications.
Keywords: serum uric acid, hypertension, newly onset diabetes mellitus, blood pressure, prevalence
Introduction
Prevalence of diabetes mellitus (DM) is increasing and so is the associated cardiovascular disease (CVD).1,2 Life expectancy is reduced by as much as 10 years in diabetics and CVD accounts for 2/3rds cause of death in these patients.3–5 CVD in DM is related to dysglycemia, hypertension, dyslipidemia, obesity, hyperuricemia and other factors.6 In DM one cannot effectively prevent CVD by controlling blood glucose only.7 So we need a multifactorial and novel way to prevent CVD in DM. Controlling hypertension, dyslipidemia, obesity, hyperuricemia are the other ways to control CVD in DM.8
Uric acid (UA) is the byproduct of purine metabolism. Its level is high in patients with obesity, insulin resistance (IR), metabolic syndrome (MS) and DM.9–11 Elevated serum level of UA is associated with various complications such as CVD, endothelial dysfunction, chronic kidney disease (CKD), incident hypertension and prediabetes.12–14 In the past few years, the relationship between serum uric acid (SUA) and the incidence of hypertension has received widespread attention. A positive association between SUA and hypertension has been reported in various epidemiological studies.15–19 But it is unclear, whether SUA is a marker for hypertension or a risk factor for development of hypertension.20 Some argue that both originate from common factors, such as a high fructose diet, which causes development of both hyperuricemia and hypertension.21 SUA induces hypertension in two steps.22 First it raises secretion of renin, reduces nitric oxide bioavailability and increases oxidative stress. This first step leads to renal vasoconstriction and a reversible uric acid (UA) dependent and salt inducible hypertension. After some weeks of persistently elevated UA, architectural vascular damage occurs with afferent arteriolopathy and mild interstitial inflammation. At this second stage hypertension becomes salt sensitive and does not respond to UA-lowering therapy. Recently a few studies with small numbers of subjects have reported that UA-lowering therapy can reduce blood pressure in hypertensive patients with hyperuricemia.23,24 This suggests that SUA might be a risk factor for development of hypertension. So, if we can reduce the uric acid with drugs (xanthine acid oxidase inhibitors) or lifestyle modification, we can prevent development of hypertension and thus CVD. A positive association has been found between SUA and hypertension in various countries. No studies have been performed until now to show an association between SUA and hypertension in newly diagnosed DM patients from the eastern part of India. Furthermore, level of SUA varies among different ethnicities due to difference in genetics, diet and lifestyle. Hence, we aimed to investigate the association of SUA with hypertension in newly diagnosed diabetic patients from the eastern part of India and further to know the prevalence of hyperuricemia and hypertension in these diabetic patients.
Materials and Methods
This is a cross-sectional tertiary care center-based study conducted between April 2020 and May 2021. 305 consecutive patients with newly onset diabetes (duration <1 year) were enrolled over a period of one year. Patients with history of renal, cardiac, hepatic diseases, pregnant women, drug addicts and patients on antihyperuricemic treatment were excluded from the study.
Due care was taken not to include patients having alcohol intake in the last seven days.26 Diagnosis of DM was done based on ADA criteria.27 Data regarding age, sex, height, weight, BMI (body mass index), waist circumference (WC), BP (blood pressure), uric acid, lipid profile, glycosylated hemoglobin A1c (GlyHbA1c), glomerular filtration rate (GFR) were collected from patients on a predefined format. Weight was measured by a weighing machine with precision of 0.1 kg. Height was measured by a stadiometer with precision of 0.1 cm. For height measurement patients were asked to remove footwear and stand with head kept in Frankfort position. BMI was calculated by dividing the weight (in kg) by square of height (in meter). BP was measured with the help of a digital BP machine.
7 mL venous blood was collected in the morning for FPG (fasting plasma glucose), GlyHbA1c, vitamin D, creatinine and lipid profile. Blood glucose was estimated by glucose oxidase-peroxidase method. Vitamin D level was analyzed on Siemens ADVIA centaur, standardized against ID-LC/MS/MS, as per vitamin D standardization (Thyrocare). Creatinine was measured by creatinine enzymatic method. Lipid profile was carried out by standard enzymatic procedure. Ultrasonography was done to rule out cirrhosis in suspected cases.
The present investigation defined elevated SBP (systolic blood pressure) as ≥140 mmHg and/or DBP (diastolic blood pressure) ≥90 mm Hg as per ADA criteria.28 All hypertensive patients were either on amlodipine or telmisartan as they do not influence the serum uric acid level.
Hyperuricemia was defined as SUA level >416.4 micromole/mL (>7 mg/dl) in men and >356.9 micromole/mL (>6 mg/dl) in women. All participants were divided into three tertile based on SUA levels (T1: <4.52 mg/dl; T2: 4.52–5.64 mg/dl; T3: >5.64 mg/dl). Prevalence of hypertension was estimated in each tertile separately.
Ethical Statement
All diabetic patients provided written informed consent and they agreed to participate in this study. The protocol was approved by the Ethics Committee for Research, Opal Hospital, Varanasi, India, dated February 1, 2020. The study was also conducted using good clinical practice following the Declaration of Helsinki.
Statistical Analysis
All recorded data were summarized using descriptive analyses. Mean, standard error of mean, median, range (Min–Max) were used to describe continuous variables. Frequency and percentage were used to describe categorical variables. All data were analyzed using SPSS software ver. 20.0F.25 The difference between sex groups for baseline variables was done by independent sample t-test (two-tailed). Pearson’s correlation coefficient test was performed to assess the interrelationships between BP variables and SUA levels. One-way ANOVA determined the differences for variables among the groups. Box plot was used for showing the level of SUA in normotensive and hypertensive population. The relationship between SUA and hypertension was evaluated by logistic regression modeling. In Model-1, age and GFR were adjusted and in Model-2 age, GFR and sex were adjusted. In Model-3 age, GFR, sex and BMI were adjusted. A p-value <0.05 was considered as statistically significant.
Results
Baseline and Demographic Characteristics of Study Population
Baseline characteristics of newly diagnosed diabetic patients are summarized in Table 1. 305 (male: 212, female: 93) patients with mean age 46.76±0.61 years were recruited in the study. There was no significant age difference between male and female groups. Mean BMI of patients were 26.33±0.25, with a significant difference between gender groups (P <0.04). Mean HDL (high density lipoprotein) level was 41.32±0.56 mg/dl of all patients and mean HDL level was significantly higher in females compared with males (P <0.000). Females had a lower mean level of SUA compared with males (P <0.000). Mean levels of A1c, vitamin D, TG (triglyceride), WC, SBP, DBP, GFR, total cholesterol (TC) and LDL (low density lipoprotein) were similar in the two groups. Prevalence of hyperuricemia was 12.13%, 11.79% and 12.90% in all, males and females, respectively.
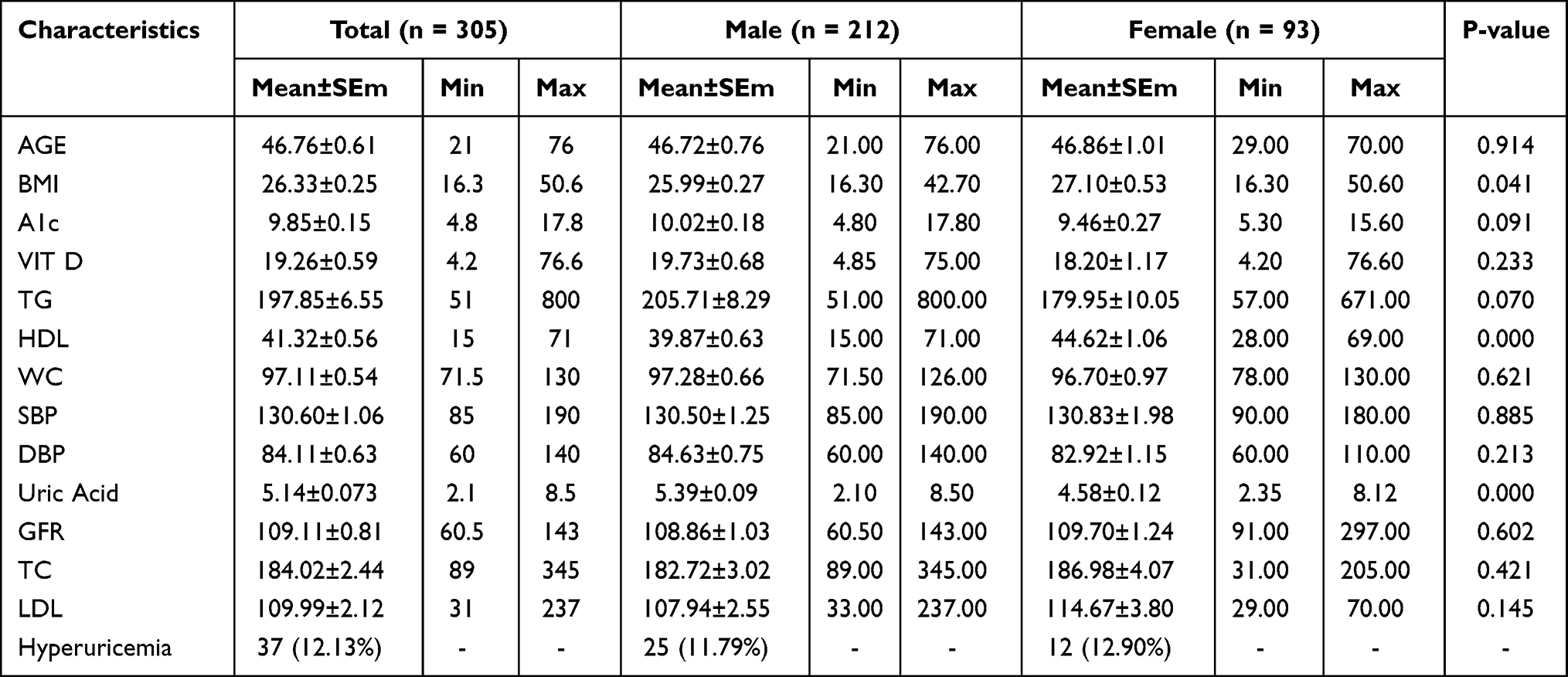 |
Table 1 Baseline Characteristics of the Study Participants by Gender. P-values are Obtained from Independent Sample t-test in Comparison Between the Gender Groups |
SUA Tertile and Baseline Characteristics of Patients
Baseline characteristics of patients with different SUA tertile are presented in Table 2. Number of patients in tertile 1, tertile 2 and tertile 3 were 102, 102 and 101, respectively. Increasing trends for mean level of SUA were found across tertile (P <0.000). Mean value of SBP increases with increasing SUA tertile (P <0.014). With increasing SUA level, mean value of DBP also increased significantly (P <0.001). The mean values for BMI, A1c, HDL WC and GFR were significantly increased with increasing concentration of SUA (P <0.05). Mean values for age, vitamin D, TG, total cholesterol and LDL was not significantly increased with increasing concentration of SUA.
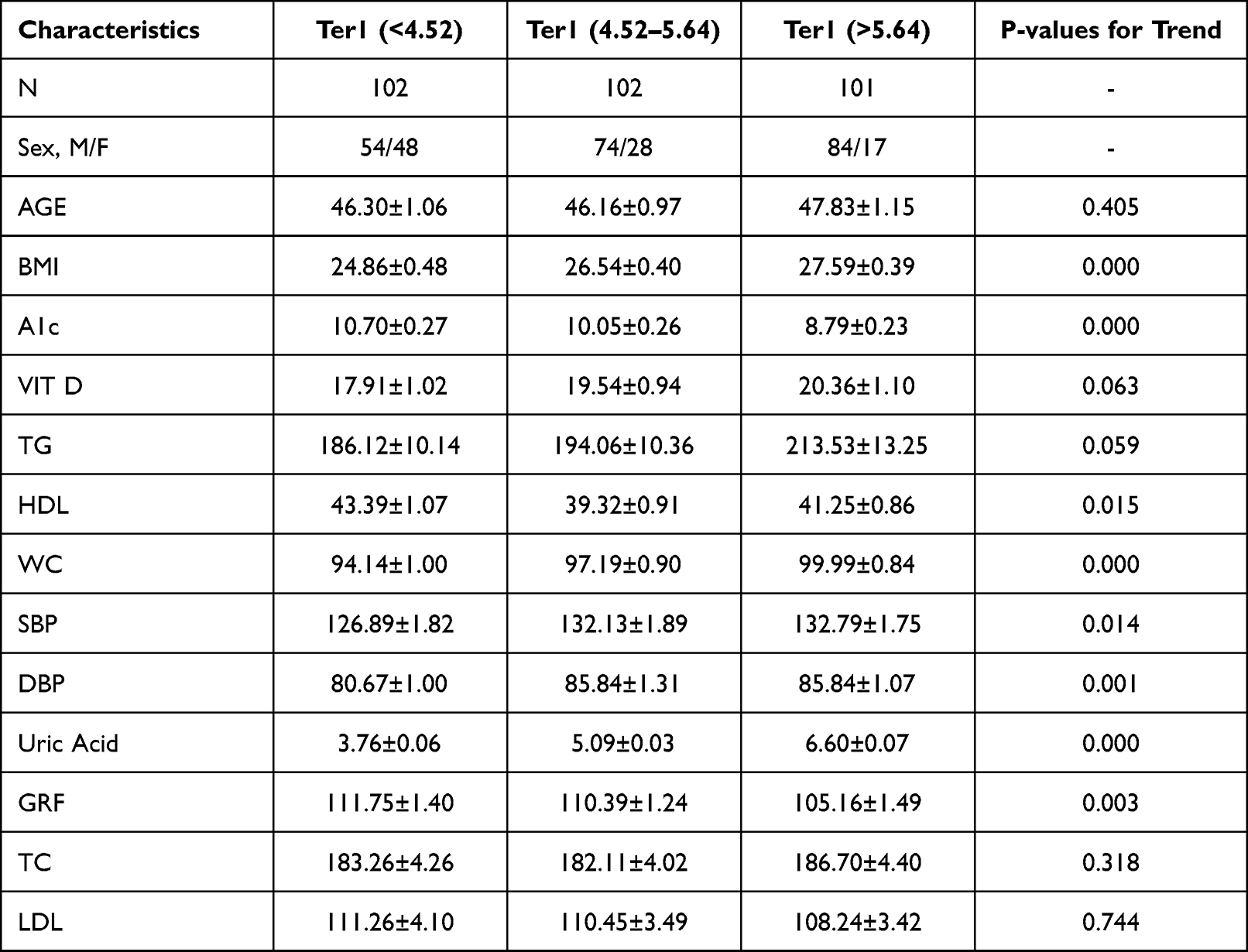 |
Table 2 Baseline Characteristics of the Study Participants According to UA Tertile. Values are Presented as Mean ± SE. P-values are Obtained from One-Way ANOVA |
SUA Tertile and Prevalence of Hypertension
Prevalence of hypertension in each tertile is presented in Table 3. Prevalence of hypertension was 44.59%. 44.34% and 45.16% in all, males and females, respectively. Prevalence of hypertension was similar in males and females, however it increased with increasing concentration of SUA but more in females than males (P <0.05 for trends).
 |
Table 3 Prevalence of Hypertension. Blood Pressure (mmHg) Was Categorized as Normal (SBP < 140; DBP < 90) and Hypertensive (SBP ≥ 140; DBP ≥ 90) |
Association of SUA Tertile with Blood Pressure
A significant positive correlation was found between SUA levels and SBP and DBP. Pearson’s correlation coefficient test indicates that SUA level was significantly positively associated with SBP (r = 0.135, P <0.018) and DBP (r = 0.181, P <0.001) (Figure 1). In hypertensive patients SUA was elevated compared with normotensive patients (Figure 2). Mean level of SUA in normotensive and hypertensive males was 5.29+0.114 and 5.53+0.131 with median (interquartile range) of 5.26 (2.06) and 5.49 (2.19) mg/dl, respectively. In females mean levels of SUA in normotensive and hypertensive patients were 4.37+0.126 and 4.82+0.182 with median (interquartile range) of 4.26 (1.80) and 4.87 (1.88) mg/dl respectively. The association of hypertension and SUA tertile for all diabetic patients is presented in Table 4 after applying logistic regression analysis. Hypertension was positively correlated with SUA tertile (P <0.01 for trends) in the present study. After adjusting age and GFR (model 1), the odds ratios (95% CI) were 1.092 (1.000–1.294) and 1.153 (1.048–1.436), respectively for T2 and T3 compared with T1. In model 2, after adjustment for age, sex and GFR, the odds ratios (ORs) were 0.980 (0.893–1.077) and 1.040 (1.001–1.336) for T2 and T3, respectively compared with T1. In model 3 after adjustment for age, sex, GFR and BMI, the ORs were 1.114 (0.994–1.248) and 1.287 (1.057–1.592), respectively for T2 and T3 compared with T1. This shows that SUA tertile was independently associated with increased prevalence of hypertension.
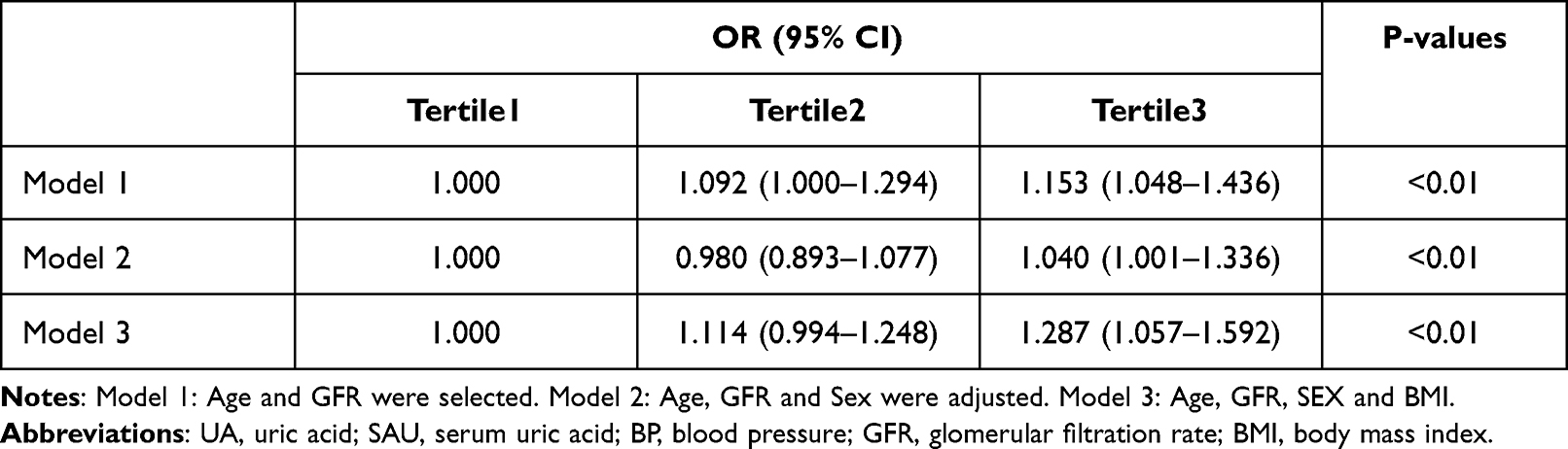 |
Table 4 Association of UA Quartiles with Hypertension. The Logistic Regressions Were Applied to Evaluate the Association Between SUA Quartiles and BP-Class |
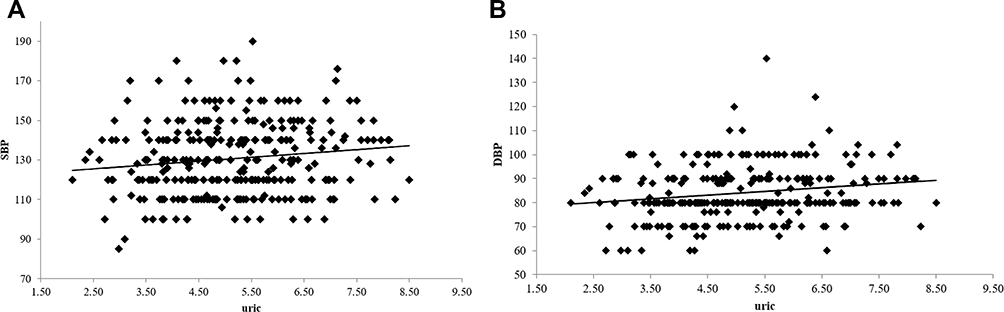 |
Figure 1 Association of SUA levels with (A) SBP and (B) DBP. The scale in the Y-axis is not similar between the figures. |
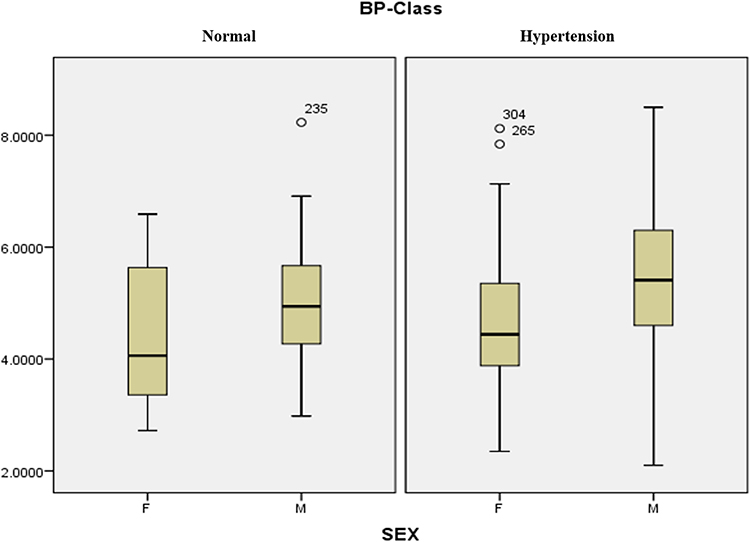 |
Figure 2 Box plot showing level of SUA in normal and hypertensive population by gender. |
Discussion
Hypertension is a leading cause of CVD and premature death.29,30 Worldwide prevalence of hypertension is rapidly increasing and this increase is more significant in low- and middle-income countries compared with developed countries.31 Various reasons such as high sodium intake, obesity, hyperuricemia, alcohol intake, stress, physical inactivity, older age and unhealthy diet may explain the regional heterogeneity in prevalence of hypertension. Despite high prevalence, treatment and control of hypertension is low in developing countries. However various trials show that if we can control blood pressure we can reduce CVD. Meta-analysis shows that a 2 mmHg reduction in SBP can reduce stroke mortality by 10% and death from ischemic heart disease and other CVD by about 7% and a further 2 mmHg reduction in DBP in mean of population distribution can result in 6% decrease in occurrence of CHD and 15% risk reduction of stroke and transient ischemic attack.32,33 Hyperuricemia has been reported to be commonly present in patients with primary hypertension and especially in malignant hypertension.34 Recently a systematic review and meta-analysis by Agrawal et al reported that treatment with urate lowering drug reduces SBP by 3.3 mmHg and DBP by 1.3 mmHg.35 Therefore, reduction of SUA can help in lowering of blood pressure and thus CVD. In the present study we tried to explore the prevalence of hypertension and hyperuricemia and potential association of SUA and hypertension. This is the first study from the eastern part of India that has evaluated the relationship between SUA and hypertension in new-onset DM.
In the present study, prevalence of hypertension was 44.59%, 44.34% and 45.16% in all, male and females, respectively. Similar trends in prevalence of hypertension were seen in previous studies also.36,37 Prevalence of hyperuricemia was 12.13%, 11.79% and 12.90% in all, males and females, respectively. Similar results were found in other studies.38–40 SUA was lower in females compared with males. Reasons for low SUA in females is due to high estrogen level.41 Estrogen is known to have uricosuric properties.41 Other reasons for high SUA in males are different eating habits, exercise and commuting methods.42
Our present finding confirms a strong association between SUA and hypertension. We observed that SBP and DBP increased progressively across the SUA tertile. We also found that prevalence of hypertension steadily increased across the SUA tertile even after adjusting the confounders such as age, sex, BMI and GFR. This proves that SUA is independently associated with hypertension. Consistent with present study, several epidemiological studies have also found a positive association between SUA and hypertension.15–19 In a Japanese study hypertension OR was 1.2 for each 1 mg/dl increase in SUA concentration after adjusting of multiple confounders. In the same study OR in the highest quartile was 1.58 in male and 1.60 in females, compared with lowest SUA quartile.15 Another study found that men with hyperuricemia had a higher risk of incident hypertension, with each unit increase in SUA associated with a 9% increase in the risk of incident hypertension.43 Other studies also found elevated SUA common in subjects with new-onset hypertension, with prehypertension and with gestational hypertension.44–46 SUA increases blood pressure through various mechanisms, such as activation of RASS, induction of oxidative stress, decrease in NO availability, smooth muscle cell proliferation, and induces inflammation and salt sensitivity.22
We also observed a relatively stronger relationship between SUA level and hypertension in females as compared to male diabetic patients. Other studies have also found the same. Gender-related differences were also reported in the association of SUA and MACE (major adverse cardiovascular event), arterial stiffness, metabolic syndrome, CAVI (cardio-ankle vascular index) and cardiac diastolic dysfunction.47 Although the reason for these gender differences is still unclear, sex hormones may have a role. Further studies are required to investigate the exact role of sex hormones in development of hypertension and other related disorders in hyperuricemic patients.
Though vitamin D deficiency has been found associated with hyperuricemia in some reports the causal association has been always a point of enigma. In the present investigation no significant association was found between uric acid level and vitamin D level. Such observations are also reported.48,49 Alcohol is known to increase serum uric acid level in blood. In the present study, patients were non-alcoholic except very few patients that too were not having alcohol consumption in last seven days while collecting the samples. Since effect of alcohol vanishes after 3 days, thus it has not influenced the statistical analysis.25
There are three primary limitations of this study. First, its cross-sectional nature prevents assessing cause–effect relationship. Second, sample size was moderate and from single center so there could be some bias. Third, we were not able to analyze dietary pattern in these patients as SUA level is also dependent upon diet.
The present investigation demonstrates that hypertension is strongly and independently associated with serum uric acid level thus early and aggressive treatment of hyperuricemia will be beneficial in prevention of the complication.
Conclusion
The results of the present study show a significant positive association between SUA and hypertension. Prevalence of hypertension and hyperuricemia is high in new-onset DM. Multiple logistic regression analysis proves that there is an independent relationship between SUA and hypertension. Therefore, routine measurement and treatment of SUA and blood pressure in diabetic patients is recommended to prevent development of related complications.
Abbreviations
HU, hyperuricemia; DM, diabetes mellitus; SUA, serum uric acid; SBP, systolic blood pressure; DBP, diastolic pressure; CVD, cardiovascular disease; UA, uric acid; IR, insulin resistance; MS, metabolic syndrome; CKD, chronic kidney disease; BMI, body mass index; WC, waist circumference; BP, blood pressure; GlyHbA1c, glycosylated hemoglobin A1c; GFR, glomerular filtration rate; FPG, fasting plasma glucose; HDL, high density lipoprotein; TG, triglyceride; TC, total cholesterol; LDL, low density lipoprotein; CHD, coronary heart disease; RASS, renin-angiotensin- aldosterone system; NO, nitric oxide; MACE, major adverse cardiovascular event; CAVI, cardio-ankle vascular index.
Acknowledgments
The authors gratefully acknowledge Vanshika Singh, Praveer Anand and Yogender Singh for their critical comments. Authors also wish to thank Prof Dinesh Kumar, Department of Biotechnology, Central University of Haryana, for his constant motivation and critical comments.
Author Contributions
SKS contributed in conceptualization, designing, acquisition of data and execution of the work. MAI and SJ analyzed the data. All authors made a significant contribution in interpretation. SKS took part in initial drafting, all authors contributed in revising the article and gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted and further agreed to be accountable for all aspects of the work.
Disclosure
Authors have no conflicts of interest related to this work to disclose.
References
1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. doi:10.2337/diacare.27.5.1047
2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diab Res Clin Practice. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
3. Leung MY, Pollack LM, Colditz GA, Chang SH. Life years lost and lifetime health care expenditures associated with diabetes in the US, National Health Interview Survey, 1997–2000. Diabetes Care. 2015;38:460–468. doi:10.2337/dc14-1453
4. Wright AK, Kontopantelis E, Emsley R, et al. Life expectancy and cause-specific mortality in type 2 diabetes: a population-based cohort study quantifying relationships in ethnic subgroups. Diabetes Care. 2017;40(3):338–345. doi:10.2337/dc16-1616
5. Geiss LS, Herman WH, Smith PJ; National Diabetes Data Group. Diabetes in America. Bethesda, Md: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 1995:233–257.
6. Wilson PW. Diabetes mellitus and coronary heart disease. Am J Kidney Dis. 1998;32:S89–S100. doi:10.1053/ajkd.1998.v32.pm9820468
7. Skyler JS, Bergenstal R, Bonow RO, et al. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Association and a Scientific Statement of the American College of Cardiology Foundation and the American Heart Association. J Am Coll Cardiol. 2009;53(3):298–304. doi:10.1016/j.jacc.2008.10.008
8. Gæde P, Oellgaard J, Carstensen B, et al. Years of life gained by multifactorial intervention in patients with type 2 diabetes mellitus and microalbuminuria: 21 years follow-up on the Steno-2 randomised trial. Diabetologia. 2016;59(11):2298–2307. doi:10.1007/s00125-016-4065-6
9. Chen L, Zhu W-H, Chen Z-W, et al. Relationship between hyperuricemia and metabolic syndrome. J Zhejiang Univ Sci. 2007;B8:593–598. doi:10.1631/jzus.2007.B0593
10. Modan M, Halkin H, Karasik A, Lusky A. Elevated serum uric acid: a facet of hyperinsulinaemia. Diabetologia. 1987;30:713–718. doi:10.1007/BF00296994
11. Schmidt MI, Watson RL, Duncan BB, et al. Clustering of dyslipidemia, hyperuricemia, diabetes, and hypertension and its association with fasting insulin and central and overall obesity in a general population. Metabolism. 1996;45:699–706. doi:10.1016/S0026-0495(96)90134-1
12. Nakanishi N, Okamoto M, Yoshida H, et al. Serum uric acid and risk for development of hypertension and impaired fasting glucose or type II diabetes in Japanese male office workers. Eur J Epidemiol. 2003;18:523–530. doi:10.1023/A:1024600905574
13. Li L, Yang C, Zhao Y, et al. Is hyperuricemia an inde- pendent risk factor for new-onset chronic kidney disease? A systematic review and meta-analysis based on observational cohort studies. BMC Nephrol. 2014;15:122. doi:10.1186/1471-2369-15-122
14. Desai RJ, Franklin JM, Spoendlin-Allen J, et al. An evaluation of longitudinal changes in serum uric acid levels and associated risk of cardio-metabolic events and renal function decline in gout. PLoS One. 2018;13(2):e0193622. doi:10.1371/journal.pone.0193622
15. Kuwabara M, Niwa K, Nishi Y, et al. Relationship between serum uric acid levels and hypertension among Japanese individuals not treated for hyperuricemia and hypertension. Hypertens Res Off. 2014;37:785–789.
16. Cheng W, Wen S, Wang Y, et al. The association between serum uric acid and blood pressure in different age groups in a healthy Chinese cohort. Medicine. 2017;96(50):e8953. doi:10.1097/MD.0000000000008953
17. Loeffler LF, Navas-Acien A, Brady TM, et al. Uric acid level and elevated blood pressure in US adolescents: national health and nutrition examination survey, 1999–2006. Hypertension. 2012;59(4):811–817. doi:10.1161/HYPERTENSIONAHA.111.183244
18. Cui L, Shi H-J, Wu S-L, et al. Association of serum uric acid and risk of hypertension in adults: a prospective study of Kailuan Corporation cohort. Clin. Rheumatol. 2017;36:1103–1110. doi:10.1007/s10067-017-3548-2
19. Sundström J, Sullivan L, D’Agostino RB, et al. Relations of serum uric acid to longitudinal blood pressure tracking and hypertension incidence. Hypertens. 2005;45:28–33. doi:10.1161/01.HYP.0000150784.92944.9a
20. Johnson RJ, Sánchez-Lozada LG, Mazzali M, et al. What are the key arguments against uric acid as a true risk factor for hypertension? Hypertens. 2013;61(5):948–951. doi:10.1161/HYPERTENSIONAHA.111.00650
21. Perez-Pozo SE, Schold J, Nakagawa T, et al. Excessive fructose intake induces the features of metabolic syndrome in healthy adult men: role of uric acid in the hypertensive response. Int J Obes. 2010;34(3):454–461. doi:10.1038/ijo.2009.259
22. Feig DI. Serum uric acid and the risk of hypertension and chronic kidney disease. Curr Opin Rheumatol. 2014;26:176–185. doi:10.1097/BOR.0000000000000033
23. Feig DI, Soletsky B, Johnson RJ. Effect of allopurinol on blood pressure of adolescents with newly diagnosed essential hypertension: a randomized trial. JAMA. 2008;300:924. doi:10.1001/jama.300.8.924
24. Soletsky B, Feig DI. Uric acid reduction rectifies prehypertension in obese adolescents. Hypertension. 2012;60:1148–1156. doi:10.1161/HYPERTENSIONAHA.112.196980
25. IBM Corp. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp; 2011.
26. Newcombe DS. Ethanol metabolism and uric acid. Metabolism. 1972;1(12):1193–1203. doi:10.1016/0026-0495(72)90115-1
27. American Diabetes Association. 9. Cardiovascular disease and risk management: standards of medical care in diabetes—2018. Diabetes Care. 2018;41(Supplement_1):S86–S104. doi:10.2337/dc18-S009
28. American Diabetes Association. Standards of medical care for patients with diabetes mellitus. Diabetes Care. 2003;26(Suppl 1):S33–50. doi:10.2337/diacare.26.2007.s33
29. Fields LE, Burt VL, Cutler JA, et al. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension. 2004;44(4):398–404. doi:10.1161/01.HYP.0000142248.54761.56
30. Sarki AM, Nduka CU, Stranges S, et al. Prevalence of hypertension in low- and middle-income countries: a systematic review and meta-analysis. Medicine. 2015;94:e1959. doi:10.1097/MD.0000000000001959
31. Chowdhury MAB, Uddin MJ, Haque MR, et al. Hypertension among adults in Bangladesh: evidence from a national cross-sectional survey. BMC Cardiovasc Disord. 2016;16:16. doi:10.1186/s12872-016-0192-8
32. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. doi:10.1016/S0140-6736(02)11911-8
33. Cook NR, Cohen J, Hebert PR, et al. Implications of small reductions in diastolic blood pressure for primary preven- tion. Arch Intern Med. 1995;155:701–709. doi:10.1001/archinte.1995.00430070053006
34. Cannon PJ, Stason WB, Demartini FE, et al. Hyperuricemia in primary and renal hypertension. N Engl J Med. 1966;275(9):457–464. doi:10.1056/NEJM196609012750902
35. Agarwal V, Hans N, Messerli FH. Effect of allopurinol on blood pressure: a systematic review and meta-analysis. J Clin Hypertens. 2013;15:435–442. doi:10.1111/j.1751-7176.2012.00701.x
36. Ramachandran A, Snehalatha C, Vishwanath V. Burden of type 2 diabetes and its complications - The Indian scenario. Curr Sci. 2002;83:1471–1476.
37. Priya D, Dudhal K, Khakse GM, et al. Prevalence of hypertension among type 2 diabetes patients. Int J Sci Environ Technol. 2013;2:1401–1406.
38. Uaratanawong S, Suraamornkul S, Angkeaw S, Uaratanawong R. Prevalence of hyperuricemia in Bangkok population. Clin Rheumatol. 2011;30(7):887–893. doi:10.1007/s10067-011-1699-0
39. Lohsoonthorn V, Dhanamun B, Williams MA. Prevalence of hyperuricemia and its relationship with metabolic syndrome in Thai adults receiving annual health exams. Arch Med Res. 2006;37(7):883–889. doi:10.1016/j.arcmed.2006.03.008
40. Sari I, Akar S, Pakoz B, et al. Hyperuricemia and its related factors in an urban population, Izmir, Turkey. Rheumatol Int. 2009;29(8):869–874. doi:10.1007/s00296-008-0806-2
41. Antón FM, García Puig J, Ramos T, et al. Sex differences in uric acid metabolism in adults: evidence for a lack of influence of estradiol- 17 beta (E2) on the renal handling of urate. Metabolism. 1986;35(4):343–348. doi:10.1016/0026-0495(86)90152-6
42. Liu L, Lou S, Xu K, et al. Relationship between lifestyle choices and hyperuricemia in Chinese men and women. Clin Rheumatol. 2013;32(2):233–239. doi:10.1007/s10067-012-2108-z
43. Krishnan E, Kwoh CK, Schumacher HR, et al. Hyperuricemia and incidence of hypertension among men without metabolic syndrome. Hypertension. 2007;49(2):298–303. doi:10.1161/01.HYP.0000254480.64564.b6
44. Feig DI, Johnson RJ. Hyperuricemia in childhood primary hypertension. Hypertension. 2003;42:247–252. doi:10.1161/01.HYP.0000085858.66548.59
45. Syamala S, Li J, Shankar A. Association between serum uric acid and prehypertension among US adults. J Hypertens. 2007;25:1583–1589. doi:10.1097/HJH.0b013e32813aeb6c
46. Powers RW, Bodnar LM, Ness RB, et al. Uric acid concentrations in early pregnancy among preeclamptic women with gestational hyperuricemia at delivery. Am J Obstet Gynecol. 2006;194:160. doi:10.1016/j.ajog.2005.06.066
47. Zheng X, Wei Q, Long J, et al. Gender specific association of serum uric acid level and cardio-ankle vascular index in Chinese adults. Lipids Health Dis. 2018;17:80. doi:10.1186/s12944-018-0712-x
48. Peng H, Li H, Li C, et al. Association between vitamin D insufficiency and elevated serum uric acid among middle-aged and elderly Chinese Han women. PLoS One. 2013;8:e61159. doi:10.1371/journal.pone.0061159
49. Takir M, Solak Y, Erek A, et al. Association between elevated serum uric acid and vitamin D insufficiency among the middle-aged and elderly population. Turk Nephrol Dial Transplant J. 2016;25:182–186. doi:10.5262/tndt.2016.1002.10
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hypertension and Its Associated Factors Among Long-Distance Truck Drivers in Ethiopia
Rike ME, Diress M, Dagnew B, Getnet M, Hasano Kebalo A, Sinamaw D, Solomon D, Akalu Y
Integrated Blood Pressure Control 2022, 15:67-79
Published Date: 21 June 2022
Prevalence of Hypertension and Its Associated Risk Factors Among Patients with Rheumatoid Arthritis in the Kingdom of Saudi Arabia
Al-Ahmari AK
International Journal of General Medicine 2022, 15:6507-6517
Published Date: 8 August 2022
Patterns of Dyslipidemia in the Anemic and Nonanemic Hypertensive Saudi Population: A Cross-Sectional Study
Alfhili MA, Alsughayyir J, Basudan AM, Ghneim HK, Alfaifi M, Alamri HS, Awan ZA, Algethami MR
International Journal of General Medicine 2022, 15:7895-7906
Published Date: 21 October 2022
Prevalence of Undiagnosed Hypertension and Its Predictors in Jordan: A Cross-Sectional Study
Alhawari H, AlShelleh S, Alhawari H, AlRyalat SA, Khanfar AN, Alzoubi O
International Journal of General Medicine 2022, 15:7919-7928
Published Date: 25 October 2022
Trends and Comparisons of Blood Pressure and Fasting Plasma Glucose in Patients with Hypertension, Diabetes, and Comorbidity: 4-Year Follow-Up Data
Xu L, Wen X, Yang Y, Cui D
Risk Management and Healthcare Policy 2022, 15:2221-2232
Published Date: 25 November 2022