")
Back to Journals » International Journal of General Medicine » Volume 15
Prevalence of Hypertension and Its Associated Risk Factors Among Patients with Rheumatoid Arthritis in the Kingdom of Saudi Arabia
Authors Al-Ahmari AK
Received 15 April 2022
Accepted for publication 4 August 2022
Published 8 August 2022 Volume 2022:15 Pages 6507—6517
DOI https://doi.org/10.2147/IJGM.S370956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdullah K Al-Ahmari
Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-Kharj, Riyadh, Saudi Arabia
Correspondence: Abdullah K Al-Ahmari, Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam Bin Abdulaziz University, P.O. Box 173, Al-Kharj, 11942, Saudi Arabia, Tel +966 11 588 6082, Fax +966 11 588 6000, Email [email protected]
Purpose: Data regarding hypertension prevalence among patients with rheumatoid arthritis in Saudi Arabia are scarce. This study was aimed at estimating the prevalence of hypertension and its associated risk factors among patients with rheumatoid arthritis in Saudi Arabia.
Patients and Methods: This was a cross-sectional study of adult patients with rheumatoid arthritis who presented at the OPD of two major hospitals in Riyadh city. Patient information such as demographic characteristics, comorbidities, drug use, and other clinical data were captured through medical record review and supplemented by patient interviews. Multivariate logistic regression was used to identify the significant factors for hypertension.
Results: The prevalence of hypertension was found in 32.35% of the 1490 rheumatoid arthritis patients who participated in our study. Logistic regression analyses revealed that advanced age, female sex, low education level, unemployment, smoking, and consulting with physicians less than two times within the past 12 months were risk factors for increased hypertension prevalence among patients with rheumatoid arthritis. A significantly higher risk of hypertension was observed among RA patients with obesity, diabetes, hyperlipidemia, cancer, kidney disease, osteoporosis, and Parkinson’s disease than among patients without these comorbidities.
Conclusion: Hypertension is highly prevalent among patients with rheumatoid arthritis, and advanced age, sex, low educational level, unemployment, smoking, and comorbidities are risk factors for increased hypertension prevalence.
Keywords: blood pressure, prevalence, rheumatoid arthritis, risk factors, Saudi Arabia
Introduction
Hypertension is a chronic disorder characterized by persistently high blood pressure (BP) in the arteries.1 Most of the time, high BP does not result in any noticeable symptoms.2 However, long-term high BP is a major risk factor for coronary artery disease, stroke, heart failure, atrial fibrillation, peripheral vascular disease, vision loss, chronic kidney disease, and dementia.3
In 2008, 24% of the world’s adult population had uncontrolled hypertension, which is predicted to rise to 31% by 2025.4 A high prevalence of hypertension has been discovered among the Saudi Arabian population in several studies. Al-Nozha et al reported that hypertension affects more than one-fourth of the adult Saudi population and that its prevalence is increasing.5 In a nationwide survey conducted by El Bcheraoui et al, the prevalence of hypertension in Saudi Arabia was approximately 15.2%, whereas that of borderline hypertension was nearly 41%.6 Additionally, Al-Wabel et al reported high rates of prehypertension and hypertension among young adults and that the majority of these cases were undiagnosed.7 Elkhalifa et al showed a high prevalence of hypertension among individuals in Saudi Arabia and that diabetes, obesity, and aging were the most important determinant factors for hypertension.8
Rheumatoid arthritis (RA) is a long-term inflammatory illness that affects synovial joints and causes tissue degeneration. It typically develops in middle-aged individuals.9 It can affect extra-articular tissues, including the kidneys and heart.10,11 Charles-Schoeman stated that the prevalence of cardiovascular diseases (CVDs) increases in patients with RA.12 Furthermore, Chung et al reported that hypertension was likely more common in patients with RA than in the control subjects in their study.13 Additionally, Dessein et al reported that in patients with RA, hypertension may represent a traditional cardiovascular risk factor whose prevalence increases and alters based on the presence of the disease.14
Individuals with autoimmune rheumatic disorders, such as systemic lupus erythematosus and RA, have a higher risk of CVD and associated mortality than that in the general population.15 This high prevalence of CVD has been linked to an increased risk of hypertension in patients with autoimmune rheumatic diseases.16 Several other studies have also confirmed that cardiovascular complications, including hypertension, are common and morbid complications of RA.17–21 Therefore, individuals with RA need to be constantly monitored for CVD events and their risk factors must be effectively managed. Nevertheless, there is a gap in the literature on the prevalence of hypertension in Saudi Arabia, particularly among RA patients. Thus, this study was aimed at estimating the prevalence of hypertension and its associated risk factors in patients with RA in Saudi Arabia. Rheumatologists may find this information valuable in identifying high-risk patients and improving blood pressure control for RA patients in our area.
Materials and Methods
Study Design and Setting
This was a cross-sectional study. From October 2019 to March 2020, two clinical pharmacists, four nurses, and pharmacy interns gathered data from RA patients who visited two rheumatology clinics in two public hospitals in Riyadh, Prince Sultan Military Medical City (PSMMC) and King Khaled Hospital & Prince Sultan Center for Health Care.
Eligibility Criteria
Patients with seropositive RA aged ≥18 years were eligible for participation. Patients were included if their complete medical records for the previous 6 months could be accessed at the time of data collection. Individuals recently diagnosed with RA, those with seronegative RA, mixed connective tissue disease, or other connective tissue disorders were excluded from this study. Additional exclusions included pregnant women, those who were terminally ill, or those who had cognitive impairments. Overall, 1490 RA patients met the criteria for participation.
The protocol of this study, which was conducted in compliance with the Declaration of Helsinki, was approved by the Ministry of Health’s institutional review board (number 2019–0059E) and PSMMC’s research ethics committee (project no.: 1240). All study participants were informed of the project’s rationale and aims, and interviews were voluntary. The patients had the freedom to opt-out of the study at any time and for any reason. Signed written informed consent was obtained from all participants before data collection and for the publication of this study.
Study Variables
Dependent Variable: Presence of Hypertension
According to the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, HT was defined as an SBP of 140 mmHg and an average DBP of 90 mmHg or an SBP of 130 mmHg and an average DBP of 80 mmHg (if the patient in question had a history of CVD or was diagnosed with diabetes mellitus). BP readings obtained during urgent care visits were excluded to prevent the inclusion of transiently elevated BP values caused by acute diseases.
Independent Variables
Some independent factors were also included. When determining a person’s educational level, the highest possible grade level was considered. Individuals were categorized into five groups: no formal, elementary, intermediate, secondary, and post-secondary (eg university and vocational) education. Based on their marital status at the time of study inclusion, the participants were divided into two groups: those who were married, divorced, or separated at the time of the interview and those who were not married. Based on their smoking habits, individuals were classified as smokers and non-smokers. Participants’ BMI was also assessed; they were categorized as obese or non-obese depending on whether their BMI was less or higher than 30 kg/m2. Medication-related data, including the type of BP-lowering medicine used, were gathered and documented. Furthermore, the presence or absence of comorbidities was noted (as yes or no, respectively). The comorbidities included hyperlipidemia, irritable bowel syndrome, anemia, anxiety, cancer, renal disease, asthma, liver disease, migraine, acid reflux/gastroesophageal reflux disease, osteoporosis, depression, diabetes mellitus, skin disease, and thyroid disease. Laboratory findings from previous visits were used to characterize these conditions. An acute sickness or recent medication modification (within the previous 3 months) was inapplicable; thus, related data were omitted.
Data Collection
Interviews and medical records were used to obtain individuals’ information. Semi-structured interviews were conducted with patients to obtain sociodemographic data such as age, sex, marital status, employment situation, and other lifestyle factors, such as smoking status, as well as the number of clinic visits in the past year. All eligible patients’ electronic medical data were carefully analyzed, and all comorbidities were noted.
To guarantee accuracy and avoid translation mistakes, the survey questionnaire was first prepared in English, translated into Arabic, and then translated back into English. To ensure that the data format and questionnaire used were of high quality and homogeneous, a preliminary evaluation was conducted on 5% of the total sample pool. A data abstraction tool was used to enhance the model if any flaws were found during the pretesting phase. Before beginning their assignment, data collectors were given time to prepare and get trained. The data were reviewed for consistency and correctness on the spot.
BP Measurement Procedure
BP readings were taken by nurses by using a pretested standard mercury sphygmomanometer. Patients were instructed to relax for at least 5 minutes and refrain from smoking or consuming coffee 30 minutes before the assessment. Excessive clothes were removed to avoid interference with the cuff. During BP measurement, the patients were instructed to rest and be calm. To measure BP, the cuff was inflated to the point where no sound could be heard while using a stethoscope. Thereafter, the cuff was gently deflated to assess the SBP and DBP. In 5 minutes, at the very least, two measurements were taken and recorded. The average of the two measures was calculated and used for the analysis.
Statistical Analysis
Descriptive statistics were used to determine the prevalence of hypertension among the patients. Frequencies and percentages were used to analyze how the study variables were distributed across individuals with and without a history of hypertension. Sample characteristics were described as dichotomous or polychotomous variables based on demographic and clinical information. A two-step analysis was performed to assess the association between risk factors and the prevalence of hypertension. First, a univariate logistic model was performed for each risk factor independently. Then, only the significant risk factors were included in the multivariate logistic model for further analysis. All other model variables were simultaneously adjusted, and odds ratio (OR) and 95% confidence intervals (CIs) were determined to quantify the influence of each predictor on BP control status. Data were analyzed using the SAS-9.4 program for all the analyses. A significant result was defined as one with a P-value of <0.05.
Results
Overall, 1490 patients were included in this study. The prevalence of hypertension among RA patients in our study sample was 32.35%. The mean ages of the hypertensive and non-hypertensive patients were 56.9 and 46.3 years, respectively. Most of the hypertensive patients were female, married, had a low level of education, were unemployed, and were non-smokers. Moreover, most hypertensive patients had visited a physician more than two times within the past 12 months, and the majority had visited the physician in the last 3 months. The sociodemographic characteristics of the hypertensive patients and those without a previous diagnosis of hypertension are shown in Table 1.
 |
Table 1 Sociodemographic Characteristics of Hypertensive Patients and Patients Without Hypertension |
The prevalence of hypertension and its association with other diseases are shown in Table 2. The present study showed that 42.81%, 44.26%, 40.4%, 75%, and 61.54% of the obese individuals, patients with hyperlipidemia, patients with irritable bowel syndrome, patients who had cancer, and patients with kidney disease, respectively, had hypertension. Moreover, 50%, 50.18%, 52.38%, 48.87%, and 50% of the patients with chronic obstructive pulmonary disease, osteoporosis, Parkinson’s disease, diabetes, and myocardial infarction, respectively, had hypertension.
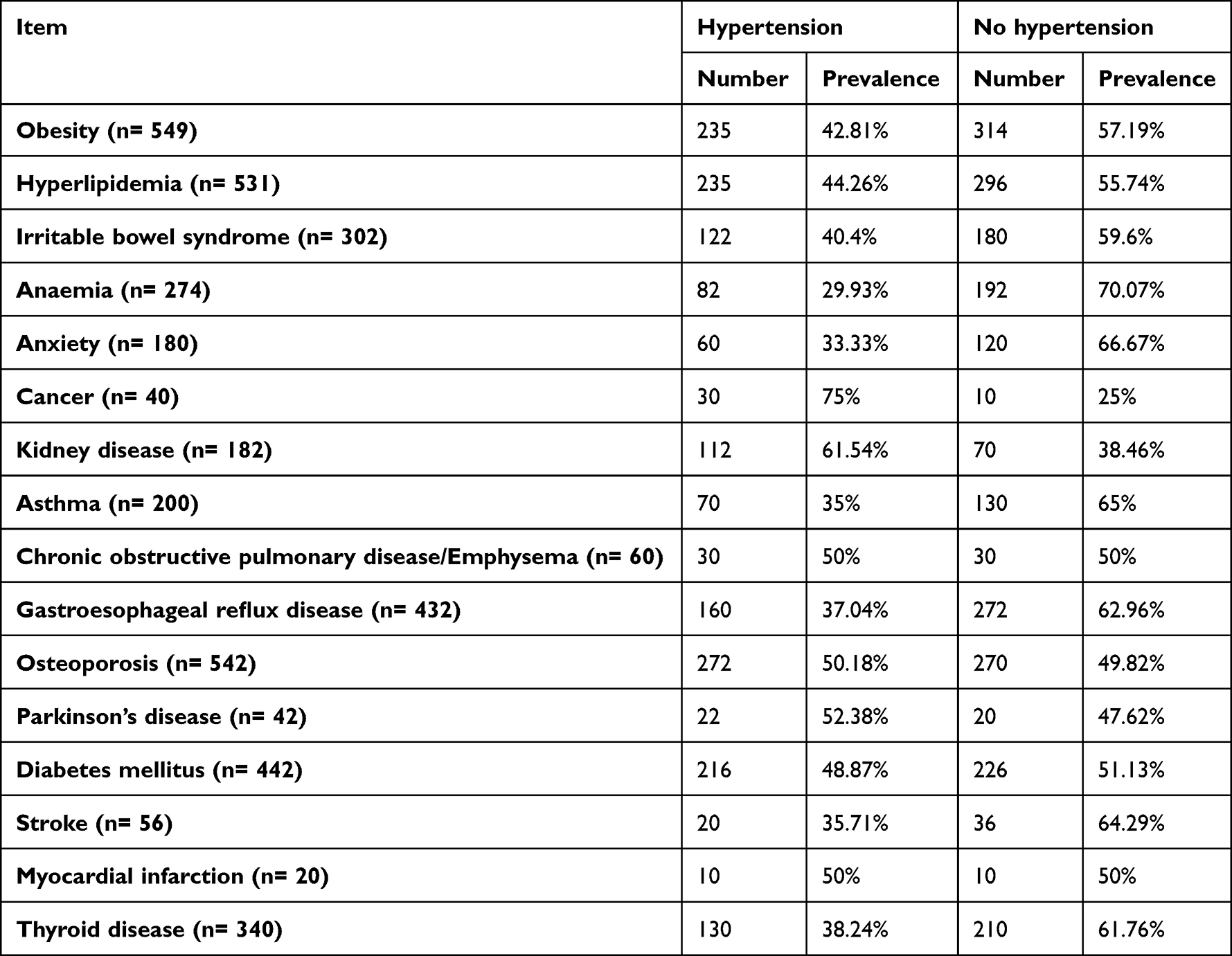 |
Table 2 The Prevalence of Hypertension Among Patients with Different Comorbidities |
Logistic regression analyses revealed that advanced age, female sex, a low level of education, unemployment, smoking, and visiting physicians less than two times within the past 12 months were risk factors for the increased prevalence of hypertension among patients with RA. The risk of hypertension was higher in people with advanced age (>60 years; OR: 9.981, 95% CI, 6.679–14.915) and a low level of education, including those with primary education alone (OR: 4.183, 95% CI: 2.827–6.191) and no formal education (OR: 2.821, 95% CI: 1.92–4.143). Compared to female patients, the risk of hypertension was lower in males (OR: 0.34, 95% CI: 0.263–0.44). Additionally, the present study also found that the risk of hypertension among unemployed persons was higher than that among employed persons (OR: 6.818, 95% CI: 5.191–8.954) and that smoking was a risk factor for hypertension (OR: 1.521, 95% CI: 1.168–1.979). The results of the logistic regression analysis to evaluate risk factors for hypertension among sociodemographic characteristics are shown in Table 3.
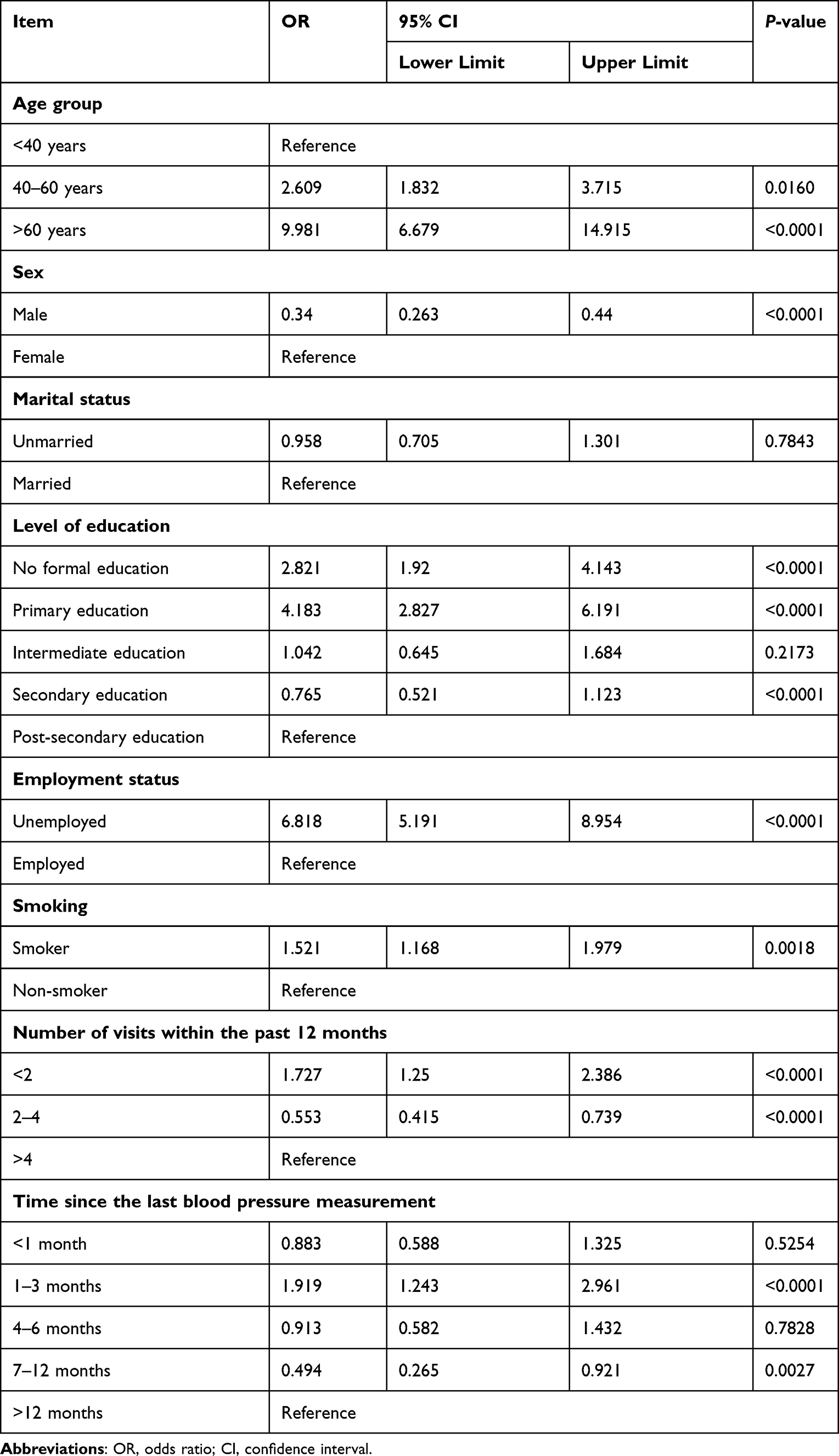 |
Table 3 Association of Hypertension with Sociodemographic Characteristics |
Table 4 shows the results of logistic regression analysis to evaluate the risk factors for hypertension associated with other diseases. Logistic regression analysis revealed a strong relationship between hypertension and most diseases. The risk of hypertension was higher among obese patients (OR: 2.456, 95% CI: 1.902–3.171), patients with hyperlipidemia (OR: 2.658, 95% CI: 2.055–3.438), cancer patients (OR: 6.497, 95% CI: 3.141–13.439), patients with kidney disease (OR: 4.186, 95% CI: 2.843–6.162), patients with asthma (OR: 1.487, 95% CI: 1.042–2.122), osteoporosis patients (OR: 2.876, 95% CI: 2.121–3.898), Parkinson’s disease patients (OR: 2.166, 95% CI: 1.025–4.578), patients with diabetes mellitus (OR: 2.699, 95% CI: 2.013–3.618), stroke patients (OR: 3.042, 95% CI: 1.619–5.715), and patients with myocardial infarction (OR: 2.85, 95% CI: 1.12–7.254).
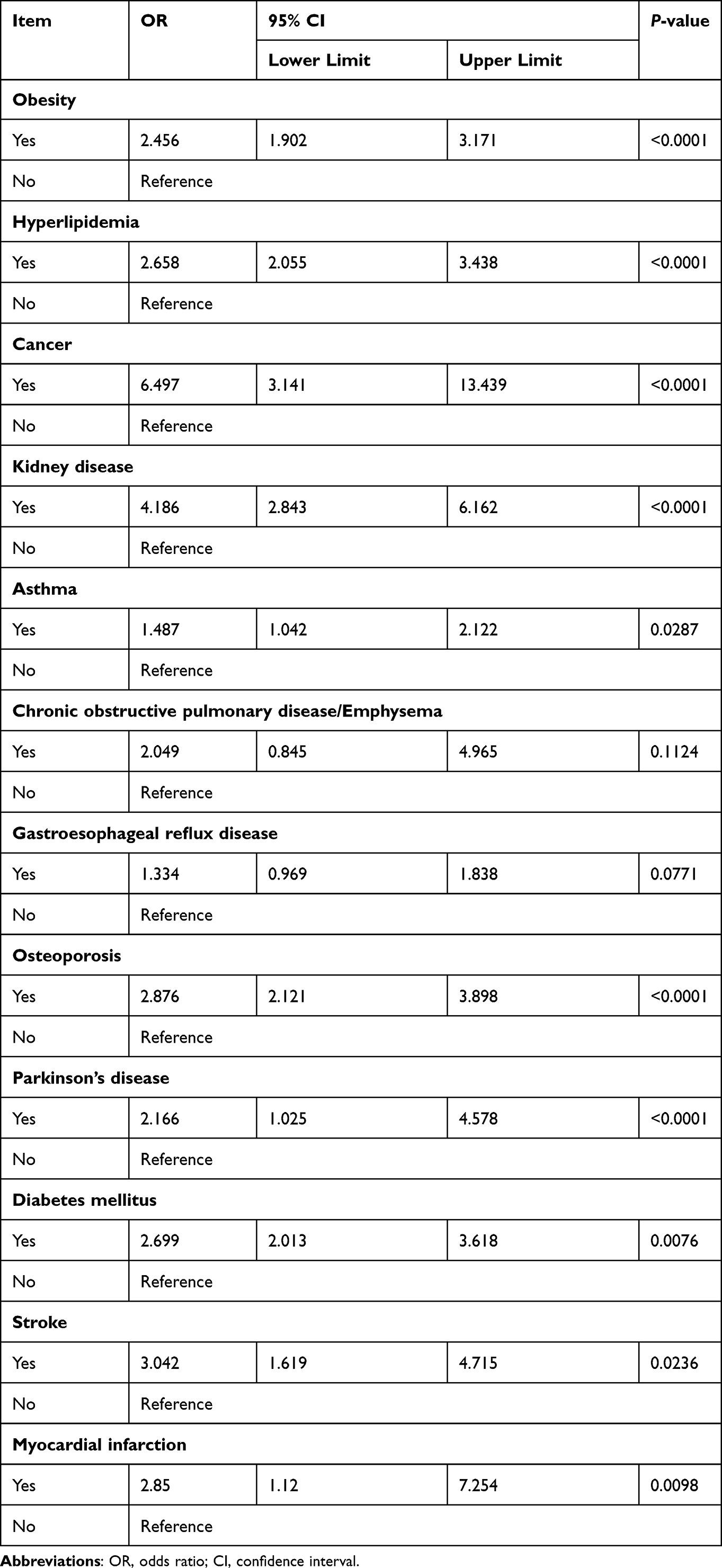 |
Table 4 Association of Hypertension with Different Comorbidities |
Discussion
In this study, the prevalence of hypertension among patients with RA in Saudi Arabia was investigated. The study showed a high prevalence of hypertension (32.35%) in patients with RA in Saudi Arabia. Similar to our findings, Al-Bishri et al conducted a cross-sectional study using data from three western hospitals and found that the prevalence of hypertension among RA patients was 35.9%.22 Several previous studies worldwide have found that hypertension is common in patients with rheumatic diseases.23–31 Akhtar et al stated that hypertension is common in patients with rheumatic diseases and that it is one of the most common risk factors for cardiovascular events in these patients, which increases morbidity and mortality rates.32 Moreover, several studies have found that hypertension is a primary risk factor that causes a high rate of negative outcomes in patients with rheumatic diseases.33–36 This study established a substantial link between hypertension in patients with RA and a variety of disorders, including hyperlipidemia, stroke, heart attack, diabetes mellitus, renal disease, irritable bowel syndrome, Parkinson’s disease, osteoporosis, and cancer. The risk of hypertension increased in individuals with RA who were obese or had chronic illnesses.
Several previous studies have reported similar findings. In a multi-center cross-sectional study, Guimaraes et al found that the observed risk factors among RA patients included hypertension, dyslipidemia, type-2 diabetes, and a family history of premature CVD.21 Al-Ghamdi found that the most common comorbidities in patients with RA were hypertension, diabetes mellitus, and obesity.20 Namas et al reported that the most frequent comorbidities observed in patients with RA were dyslipidemia, hypertension, diabetes mellitus, and gastroesophageal reflux disease.37 Bawazir reported that hypertension and diabetes mellitus are the main comorbidities among patients with RA in their study.38 Furthermore, Wolf and Ryan stated that the high prevalence of chronic kidney disease in patients with autoimmune rheumatic diseases hinders BP control.15 Al-Bishri et al reported that hypertension and diabetes mellitus were the most common comorbidities, followed by osteoporosis and dyslipidemia, among patients with RA in three centers in Saudi Arabia.22
Our study found that patients with advanced age, females, and obesity had significantly higher odds of hypertension prevalence among RA patients. Several previous studies have shown that advanced age is a risk factor for hypertension in RA.36,39–41 The majority of the patients in the present study were elderly and were females. Reckelhoff reported that BP is higher in men than in women of similar ages; however, after menopause, BP increases in women to levels even higher than those in men.42 Similarly, Yoichi et al reported that among individuals aged 30–45 years, the prevalence of hypertension is higher in men than in women. However, after this age, the prevalence of hypertension in women increases to levels similar to or higher than those in men.43 Similar to our findings, NaserAbed et al reported that the rate of hypertension in patients with arthritis was high in older age groups and women.44 On the other hand, some previous studies have concluded that obesity was a major risk factor for hypertension in RA patients.40,41
Patients who were smokers, in our study, exhibited a significantly higher risk for hypertension. Smoking has been previously linked with blood pressure elevation as well as hypertension development.45 In a meta-analysis study, Baghdadi et al concluded that smoker RA patients had a significant risk for MI compared to non-smokers (RR 1.50, 95% CI 1.15, 1.84).46 Rheumatoid arthritis patients with osteoporosis in our study showed a higher prevalence of hypertension. Similarly, a higher prevalence of hypertension among osteoporosis patients compared to non-osteoporosis patients was reported by Chai et al.47 Halperin et al conducted a study on healthy men and found that high levels of hyperlipidemia were associated with a significantly increased risk of developing incident hypertension.48 Such findings are consistent with the results of the present study.
Although a large sample size was used to achieve reliable research findings, there are still some study limitations worth addressing. First, the author was unable to acquire information on some lifestyle factors that are known to influence BP control (eg physical activity and salt consumption). Second, despite the author’s best efforts, the impact of several drugs known to increase BP could not be specifically examined. The results may have been impacted by the use of drugs such as corticosteroids, cyclosporine, caffeine, estrogens, and several over-The-counter medications. Third, it is possible that information on the use of hypertension medication, such as brand name, doses and duration of therapy, or other relevant data that indicate treatment adherence, clinical inertia, regimen complexity, and medication cost might markedly influence the incidence of uncontrolled BP. However, this information could not be obtained in this study. Finally, due to the “white coat” effect, BP readings in this study may have overestimated the number of individuals with uncontrolled hypertension. However, to ensure that the BP readings were representative, two BP measurements were obtained for each patient to verify whether their BP was uncontrolled.
The use of a bigger cohort and propensity score matching in future studies examining the incidence of hypertension in RA patients is highly suggested. Additionally, future studies should include other variables such as physical activity, salt consumption, and medication used to draw a comprehensive conclusion. Finally, a comparative effectiveness study on the impact of patient education and involvement in disease and risk factors management would be of great interest.
Conclusion
The findings of this study suggest that hypertension is highly prevalent in patients with RA and that advanced age, sex, low level of education, unemployment, and smoking are risk factors for its increased prevalence. This study also found a significant association between hypertension and numerous chronic diseases. The findings of this study highlight the need for early diagnosis and effective treatment of hypertension in patients with RA to prevent its damaging consequences. It is recommended that programs be implemented to increase awareness about hypertension and its associated risk factors.
Abbreviations
BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; RA, rheumatoid arthritis; CVD, cardiovascular disease; PSMMC, Prince Sultan Military Medical City; OR, odds ratio; CI, confidence interval.
Data Sharing Statement
The datasets used in this study are available from the corresponding author on reasonable request.
Acknowledgments
The author would like to thank the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia, for supporting this study. The author would also like to thank the PSMMC’s administration and personnel for their support and cooperation in this study. Finally, the author is grateful to Dr. Ziyad S. AlMalki, Ph.D., and Mr. Nehad J. Ahmed, MS, for their assistance in reviewing the final draft of the manuscript.
Funding
This study received no external funding.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Sariyanti EN, Hanim D, Anantanyu S. The relationship between income and nutritional status with the incidence of hypertension in elderly. Int J Hum Health Sci. 2020;5(1):81–84. doi:10.31344/ijhhs.v5i1.238
2. Martín-Fernández M, Vinyoles E, Real J, et al. The prognostic value of blood pressure control delay in newly diagnosed hypertensive patients. J Hypertens. 2019;37(2):426–431. doi:10.1097/HJH.0000000000001896
3. Lau DH, Nattel S, Kalman JM, Sanders P. Modifiable risk factors and atrial fibrillation. Circulation. 2017;136(6):583–596. doi:10.1161/CIRCULATIONAHA.116.023163
4. Sharma P, Beria H, Gupta PK, Manokaran S, Reddy AM. Prevalence of hypertension and its associated risk factors. J Pharm Sci Res. 2019;11(6):2161–2167. doi:10.1155/2017/5491838
5. Al-Nozha MM, Abdullah M, Arafah MR, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77–84.
6. El Bcheraoui C, Memish ZA, Tuffaha M, et al. Hypertension and its associated risk factors in the Kingdom of Saudi Arabia, 2013: a national survey. Int J Hypertens. 2014;2014:564679. doi:10.1155/2014/564679
7. AlWabel AH, Almufadhi MA, Alayed FM, Aloraini AY, Alobaysi HM, Alalwi RM. Assessment of hypertension and its associated risk factors among medical students in Qassim University. Saudi J Kidney Dis Transpl. 2018;29(5):1100–1108. doi:10.4103/1319-2442.243959
8. Elkhalifa AM, Kinsara AJ, Almadani DA. Prevalence of hypertension in a population of healthy individuals. Med Princ Pract. 2011;20(2):152–155. doi:10.1159/000321217
9. Mjaavatten MD, Bykerk VP. Early rheumatoid arthritis: the performance of the 2010 ACR/EULAR criteria for diagnosing RA. Best Pract Res Clin Rheumatol. 2013;27(4):451–466. doi:10.1016/j.berh.2013.09.001
10. Firestein GS. Evolving concepts of rheumatoid arthritis. Nature. 2003;423(6937):356–361. doi:10.1038/nature01661
11. Silman AJ, Pearson JE. Epidemiology and genetics of rheumatoid arthritis. Arthritis Res. 2002;4(Suppl 3):S265– S272. doi:10.1186/ar578
12. Charles-Schoeman C. Cardiovascular disease and rheumatoid arthritis: an update. Curr Rheumatol Rep. 2012;14(5):455–462. doi:10.1007/s11926-012-0271-5
13. Chung CP, Giles JT, Petri M, et al. Prevalence of traditional modifiable cardiovascular risk factors in patients with rheumatoid arthritis: comparison with control subjects from the multi-ethnic study of atherosclerosis. Semin Arthritis Rheum. 2012;41(4):535–544. doi:10.1016/j.semarthrit.2011.07.004
14. Dessein PH, Joffe BI, Veller MG, et al. Traditional and nontraditional cardiovascular risk factors are associated with atherosclerosis in rheumatoid arthritis. J Rheumatol. 2005;32(3):435–442.
15. Wolf VL, Ryan MJ. Autoimmune disease-associated hypertension. Curr Hypertens Rep. 2019;21(1):10. doi:10.1007/s11906-019-0914-2
16. Taylor EB, Wolf VL, Dent E, Ryan MJ. Mechanisms of hypertension in autoimmune rheumatic diseases. Br J Pharmacol. 2019;176(12):1897–1913. doi:10.1111/bph.14604
17. Assous N, Touzé E, Meune C, Kahan A, Allanore Y. Cardiovascular disease in rheumatoid arthritis: single-center hospital-based cohort study in France. Jt Bone Spine. 2007;74(1):66–72. doi:10.1016/j.jbspin.2006.10.001
18. Monk HL, Muller S, Mallen CD, Hider SL. Cardiovascular screening in rheumatoid arthritis: a cross-sectional primary care database study. BMC Fam Pract. 2013;14(1):150. doi:10.1186/1471-2296-14-150
19. Serelis J, Panagiotakos DB, Mavrommati M, Skopouli FN. Cardiovascular disease is related to hypertension in patients with rheumatoid arthritis: a Greek cohort study. J Rheumatol. 2011;38(2):236–241. doi:10.3899/jrheum.100564
20. Al-Ghamdi AA. The co-morbidities and mortality rate among rheumatoid arthritis patients at the western region of Saudi Arabia: a retrospective cross-sectional study. J King Saud Univ Sci. 2009;16(3):15–29. doi:10.4197/Med.16-3.2
21. de Resende Guimarães MFB, Rodrigues CEM, Gomes KWP, et al. High prevalence of obesity in rheumatoid arthritis patients: association with disease activity, hypertension, dyslipidemia and diabetes, a multi-center study. Adv Rheumatol. 2019;59(1):44. doi:10.1186/s42358-019-0089-1
22. Al-Bishri J, Attar S, Bassuni N, et al. Comorbidity profile among patients with rheumatoid arthritis and the impact on prescriptions trend. Clin Med Insights Arthritis Musculoskelet Disord. 2013;6:11–18. doi:10.4137/CMAMD.S11481
23. Han C, Robinson DW, Hackett MV, Paramore LC, Fraeman KH, Bala MV. Cardiovascular disease and risk factors in patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. J Rheumatol. 2006;33(11):2167–2172.
24. Gonzalez A, Maradit Kremers H, Crowson CS, et al. Do cardiovascular risk factors confer the same risk for cardiovascular outcomes in rheumatoid arthritis patients as in non-rheumatoid arthritis patients? Ann Rheum Dis. 2008;67(1):64–69. doi:10.1136/ard.2006.059980
25. Chung CP, Oeser A, Solus JF, et al. Prevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosis. Atherosclerosis. 2008;196(2):756–763. doi:10.1016/j.atherosclerosis.2007.01.004
26. Panoulas VF, Metsios GS, Pace AV, et al. Hypertension in rheumatoid arthritis. Rheumatology. 2008;47(9):1286–1298. doi:10.1093/rheumatology/ken159
27. Manavathongchai S, Bian A, Rho YH, et al. Inflammation and hypertension in rheumatoid arthritis. J Rheumatol. 2013;40(11):1806–1811. doi:10.3899/jrheum.130394
28. Protogerou A, Zampeli E, Konstantonis GD, et al. SAT0073 arterial hypertension in rheumatoid arthritis without cardiovascular disease: high prevalence, low awareness, poor control and increased vascular damage-associated ‘white coat’ phenomenon. Ann Rheum Dis. 2013;72(Suppl 3):
29. Gerli R, Sherer Y, Vaudo G, et al. Early atherosclerosis in rheumatoid arthritis: effects of smoking on thickness of the carotid artery intima media. Ann N Y Acad Sci. 2005;1051(1):281–290. doi:10.1196/annals.1361.069
30. Panoulas VF, Toms TE, Metsios GS, et al. Target organ damage in patients with rheumatoid arthritis: the role of blood pressure and heart rate. Atherosclerosis. 2010;209(1):255–260. doi:10.1016/j.atherosclerosis.2009.08.047
31. Paffenbarger RS
32. Akhtar MM. Rheumatoid arthritis and hypertension: literature review of the last ten years. EC Microbiol. 2019;15:43–49.
33. Barra LJ, Pope JE, Hitchon C, et al. The effect of rheumatoid arthritis–associated autoantibodies on the incidence of cardiovascular events in a large inception cohort of early inflammatory arthritis. Rheumatology. 2017;56(5):768–776. doi:10.1093/rheumatology/kew474
34. Pappas DA, Nyberg F, Kremer JM, et al. Prevalence of cardiovascular disease and major risk factors in patients with rheumatoid arthritis: a multinational cross-sectional study. Clin Rheumatol. 2018;37(9):2331–2340. doi:10.1007/s10067-018-4113-3
35. Avina-Zubieta JA, Thomas J, Sadatsafavi M, Lehman AJ, Lacaille D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies. Ann Rheum Dis. 2012;71(9):1524–1529. doi:10.1136/annrheumdis-2011-200726
36. Midtbø H, Gerdts E, Kvien TK, et al. The association of hypertension with asymptomatic cardiovascular organ damage in rheumatoid arthritis. Blood Press. 2016;25(5):298–304. doi:10.3109/08037051.2016.1172867
37. Namas R, Joshi A, Ali Z, Al Saleh J, Abuzakouk M. Demographic and clinical patterns of rheumatoid arthritis in an Emirati cohort from United Arab Emirates. Int J Rheumatol. 2019;2019:3057578. doi:10.1155/2019/3057578
38. Bawazir YM. Clinicodemographic profiles of rheumatoid arthritis patients from a single center in Saudi Arabia. Open Access Rheumatol. 2020;12:267–275. doi:10.2147/OARRR.S277956
39. Bartels CM, Johnson H, Voelker K, et al. Impact of rheumatoid arthritis on receiving a diagnosis of hypertension among patients with regular primary care. Arthritis Care Res. 2014;66(9):1281–1288. doi:10.1002/acr.22302
40. Panoulas VF, Douglas KM, Milionis HJ, et al. Prevalence and associations of hypertension and its control in patients with rheumatoid arthritis. Rheumatology. 2007;46(9):1477–1482. doi:10.1093/rheumatology/kem169
41. Abebe SM, Berhane Y, Worku A, Getachew A. Prevalence and associated factors of hypertension: a crossectional community based study in Northwest Ethiopia. PLoS One. 2015;10(4):e0125210. doi:10.1371/journal.pone.0125210
42. Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. 2001;37(5):1199–1208. doi:10.1161/01.hyp.37.5.1199
43. Izumi Y, Matsumoto K, Ozawa Y, et al. Effect of age at menopause on blood pressure in postmenopausal women. Am J Hypertens. 2007;20(10):1045–1050. doi:10.1016/j.amjhyper.2007.04.019
44. NaserAbed SN, Abed WT, Ali J. Prevalence of hypertension and associated factors in arthritis patients attending the rheumatology department in Al-Zahraa teaching hospital in Kut city, Iraq. Ann Trop Med Public Health. 2020;23(7):392–398. doi:10.36295/ASRO.2020.23718
45. Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2007;28(12):1462–1536. doi:10.1093/eurheartj/ehm236
46. Baghdadi LR, Woodman RJ, Shanahan EM, Mangoni AA. The impact of traditional cardiovascular risk factors on cardiovascular outcomes in patients with rheumatoid arthritis: a systematic review and meta-analysis. PLoS One. 2015;10(2):e0117952. doi:10.1371/journal.pone.0117952
47. Chai H, Ge J, Li L, Li J, Ye Y. Hypertension is associated with osteoporosis: a case-control study in Chinese postmenopausal women. BMC Musculoskelet Disord. 2021;22(1):1–7. doi:10.1186/s12891-021-04124-9
48. Halperin RO, Sesso HD, Ma J, Buring JE, Stampfer MJ, Michael Gaziano J. Dyslipidemia and the risk of incident hypertension in men. Hypertension. 2006;47(1):45–50. doi:10.1161/01.HYP.0000196306.42418.0e
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.