Back to Journals » Advances in Medical Education and Practice » Volume 17
Prevalence, Digital Tools, and Management Strategies for Depression in Medical Students: A Narrative Review
Authors Ren Y ![]() , Liang S, Wang R, Dong S, Wu Y, Su W
, Liang S, Wang R, Dong S, Wu Y, Su W
Received 4 February 2026
Accepted for publication 23 May 2026
Published 12 June 2026 Volume 2026:17 601300
DOI https://doi.org/10.2147/AMEP.S601300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Yuan Ren,1 Shikai Liang,1 Renzhi Wang,2 Sheng Dong,1 Youtu Wu,1 Wei Su1
1Department of Neurosurgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, People’s Republic of China; 2Department of Neurosurgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Youtu Wu; Wei Su, Department of Neurosurgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Medical students experience high rates of depression due to intense academic demands, challenges in identity formation, and limited support networks. Despite growing awareness, early detection and effective management remain insufficient. This narrative review synthesizes current evidence on the prevalence, recognition, and management of depression in medical students, with a focus on digital identification tools and competence-based mental health education. Included studies address prevalence, recognition, digital interventions, educational reforms, and competence development. Evidence indicates that stigma, inadequate training, and inconsistent institutional protocols hinder timely identification. Digital interventions including self-screening applications, remote counseling platforms, and predictive analytics models offer scalable and accessible solutions, though challenges remain in privacy, equitable access, and cultural adaptability. Integrating mental health competence into curricula is increasingly recognized as critical, encompassing self-awareness, help-seeking behavior, peer support, professional boundaries, and digital literacy for mental health tools. Most studies are cross-sectional, limiting understanding of longitudinal outcomes and the sustained impact of interventions. Future efforts should prioritize culturally responsive digital solutions, structured competence-based training, and system-level strategies to foster psychologically safe learning environments. We propose a conceptual framework linking prevalence, digital tools, educational interventions, and institutional policies to guide systemic improvements in depression recognition and management for medical students. This review highlights the need for coordinated strategies to reduce barriers, enhance competence, and promote well-being, ultimately supporting students’ academic success and professional development.
Keywords: depression, digital mental health, early detection, medical education reform, mental health competence, medical students, psychological safety, risk prediction
Introduction
Depression is a pervasive mental health concern among medical students, with a global pooled prevalence estimated at 27.2%, with only 15.7% seeking treatment1 The disproportionately high burden of depression among medical students, compared to age-matched peers, stems from a complex interplay of academic overload, identity conflict between student and professional roles, and pervasive emotional isolation due to inadequate peer and institutional support.2 The demanding medical curriculum, frequent assessments, and competitive environments often lead to chronic stress and sleep deprivation.3
Exacerbating these challenges is the hidden curriculum of emotional suppression and clinical detachment, which implicitly frames vulnerability as weakness and discourages help-seeking.4,5 This culture fosters maladaptive perfectionism and internalized shame, well-established predictors of depressive symptoms.6,7
Educational interventions such as structured reflection and peer support can enhance self-awareness, resilience, and emotional competence.8,9 This includes training students to recognize early signs of emotional distress in themselves and others, creating psychologically safe environments for disclosure, and integrating structured reflection and peer support into clinical training.10 Failure to address these challenges not only jeopardizes student well-being, but also compromises the development of empathic, resilient future physicians.
Yet, despite evidence of their effectiveness, integration of these interventions into medical curricula remains inconsistent, and digital support tools such as self-screening apps and remote counseling platforms are underexplored.11–13 Moreover, reported prevalence, intervention outcomes, and implementation practices vary widely across studies, highlighting fragmentation and inconsistencies in the literature.
To address these gaps, this narrative review aims to provide a structured synthesis across three interrelated domains: (1) the epidemiology and recognition of depression among medical students, (2) the potential role of digital tools in early detection and support, and (3) strategies for building mental health competence through medical education. By integrating these domains, we aim to provide a unified framework that clarifies existing evidence, identifies inconsistencies, and informs actionable strategies for medical schools to enhance early detection, foster student competence, and support the well-being and professional development of future physicians.
Method
A narrative literature review was conducted to synthesize current evidence regarding depression recognition, digital mental health tools, and educational strategies among medical students. Relevant literature was identified through searches of electronic databases, including PubMed, Web of Science, and EMBASE. Searches were performed using combinations of keywords related to “medical students”, “depression”, “mental health”, “digital tools”, “screening”, “early identification”, “telepsychiatry”, “mental health competence”, and “medical education”. Articles published between 2015 and 2025 were primarily considered.
Articles published in English were considered, with priority given to peer-reviewed studies, reviews, and educational reports relevant to the objectives of this review. Studies focusing on prevalence, recognition, digital interventions, mental health education, and institutional support strategies for medical students were included. Reference lists of relevant articles were also manually screened to identify additional studies. Literature selection was guided by relevance, methodological quality, and contribution to the thematic focus of the review.
Prevalence and Characteristics of Depression Among Medical Students
Global and Regional Prevalence
Depression is a major public health concern among medical students, with prevalence varying widely by region. In low- and middle-income countries (LMICs), rates are often higher due to limited mental health infrastructure and greater academic stress. A meta-analysis in Africa reported a pooled prevalence of 38.8% (95% CI: 29.6–48.1%)14 while a Namibian post-COVID study found 43.6%, linked to female gender and financial hardship.15 In Saudi Arabia, prevalence ranges from 30.9% to 77.6% (mean ≈ 51.5%), with first-year students and women at higher risk.16
In higher-income settings, prevalence studies typically report rates in the 20–30% range, reflecting stronger institutional mental health support and preventive frameworks.17,18 Nevertheless, outliers exist, such as Spain in 2020, which reported 41% overall prevalence, including 23.4% with moderate-severe symptoms and 10% with suicidal ideation.19 These discrepancies suggest that even in well-resourced contexts, temporal factors (eg, COVID-19), assessment methods, and local cultural factors can substantially influence reported prevalence. Overall, while regional trends are evident, caution is warranted when interpreting cross-study comparisons, highlighting the need for context-sensitive assessment and interventions tailored to local systems and cultures.
Symptomatology and Clinical Subtypes
The manifestation of depression in medical students is often atypical or subclinical, making early detection challenging. Commonly reported symptoms include emotional blunting, loss of motivation, cognitive fatigue, feelings of worthlessness, and sleep disturbances, many of which are frequently normalized or masked by academic stress. Functional depression, characterized by relatively preserved academic performance despite significant emotional distress, is particularly prevalent and often overlooked.20 However, estimates of prevalence and symptom profiles vary across studies, likely reflecting differences in assessment tools, sample characteristics, and cultural context.
Recent qualitative studies have also described “masked” or internalized depressive presentations, where students exhibit perfectionism, overcommitment, or emotional detachment as coping mechanisms. These patterns may not meet full diagnostic criteria for major depressive disorder (MDD), but are clinically relevant given their association with burnout, dropout risk, and suicidal ideation.20,21 Nevertheless, methodological limitations including small sample sizes and reliance on self-report warrant caution when generalizing findings.
Moreover, cognitive fatigue is prominent among students with elevated depressive symptoms. A broader undergrad study associated moderate to severe fatigue with greater psychiatric burden and poorer cognitive functioning, findings likely generalizable to the medical student population given the high demands and prolonged stress they endure during training.22 Given the high demands and prolonged stress of medical training, these findings are likely generalizable, yet further research with longitudinal designs is needed to clarify causal relationships and identify potential intervention targets.
Risk Factors
Multiple individual and contextual factors contribute to the high depression burden among medical students. First-year students often face academic adjustment, social isolation, and identity challenges,23 while senior students experience heavier clinical workloads and professional identity pressures.24–27 Female students consistently report higher depressive symptoms, linked to gender-specific stressors, cultural expectations, and stigma in help-seeking;28 in Malaysia, anxiety and depression were significantly more common among females.23 Minority, international, and low-income students may face acculturative stress, discrimination, religiosity-related conflict, or financial strain.28
Irregular schedules, long hours, and disrupted circadian rhythms are also common and strongly associated with depressive symptom severity.29 A study among Iraqi medical students found that poor sleep and psychological distress were common and significantly linked to lower academic performance (Pearson’s r= −0.333 to −0.437, p <0.001),30 and a review estimated 67.9% of students globally had poor sleep quality, associated with elevated depression and anxiety.31
Personality traits and coping styles such as neuroticism, perfectionism, and maladaptive coping (eg, avoidance, rumination) increase vulnerability to depression. In Malaysian undergraduates demonstrated evaluative perfectionism and avoidant coping mediated the risk of depression.32 Moreover, perfectionism is widely recognized as a persistent predictor of depressive symptoms and emotional exhaustion in medical training environments.26,33 Recent evidence suggests that medical school applicants who eventually succeeded in multiple mini-interview (MMI) assessments tend to exhibit lower need for cognitive closure and higher tolerance for ambiguity, traits considered advantageous in clinical decision-making under uncertainty.33 Overall, patterns suggest that risk is cumulative and context-dependent: personal vulnerabilities may be amplified or mitigated by environmental factors such as workload, mentorship, and institutional support. However, most studies are cross-sectional, culturally limited, and rely on self-reported measures, underscoring the need for longitudinal, multi-center research to clarify causal pathways and identify effective interventions.
Early Identification Strategies for Depression in Medical Students
Early Identification Tools
Early detection of depression is critical for timely intervention and support in medical education settings. Standardized self-report screening instruments such as the Patient Health Questionnaire-9 (PHQ-9),34 Beck Depression Inventory-II (BDI-II),35 and Depression Anxiety Stress Scales (DASS)36 are widely used due to their ease of administration and validated psychometric properties. However, these tools rely heavily on self-awareness and willingness to disclose symptoms like fatigue or sleep disturbances, which may be hindered by stigma, denial, or fear of professional consequences. Faculty observation and peer-based identification strategies offer alternative or complementary approaches, yet their effectiveness depends on training, sensitivity, and trust within the academic environment.37
Risk Prediction Models and Digital Monitoring
Emerging technologies present promising avenues for early identification of depression among students. Wearable devices, such as smartwatches, can continuously record physiological markers like heart rate variability, sleep duration, and activity levels.38 One recent study using an explainable anomaly detection framework on consumer-grade wearables demonstrated a robust ability (F1 ≈ 0.80) to detect significant symptom escalation in depression and anxiety.39 Yet, these methods have not been extensively validated in medical student populations, and factors such as privacy concerns, device adherence, and cultural adaptation may limit their practical utility.
In parallel, speech-based machine learning (ML) models speech-based machine learning and AI/ML models using behavioral or textual data, offer innovative avenues for early depression detection. Voice biomarkers have demonstrated moderate predictive performance (AUC ~0.77, sensitivity ~0.78), comparable to traditional self-report tools such as PHQ-9.40–42 Similarly, smartphone-based models integrating passive usage and social engagement metrics have shown meaningful associations with depressive symptoms.43,44
Despite this promise, these methods currently slightly lag behind traditional screening in robustness and require rigorous validation in medical student populations. Challenges such as privacy concerns, adherence, and cultural adaptation may limit practical implementation. Overall, these findings suggest that hybrid strategies combining traditional and digital approaches could enhance early identification, but further research is needed to confirm effectiveness, feasibility, and acceptability in real-world educational settings.
Challenges
Despite growing enthusiasm for digital mental health tools in medical education, several barriers hinder their effective implementation. Students have reported technical difficulties, frequent and distracting notifications, the requirement for constant internet access, and burdensome registration procedures as major obstacles to consistent use.13 Additionally, concerns over anonymity, time demands, and cost further reduce engagement. Interestingly, most students did not favor interventions specifically tailored to medical students but preferred general-purpose interventions applicable to all student populations, potentially to avoid stigma and maintain privacy.13
Privacy concerns remain paramount, particularly when monitoring sensitive psychological states such as depression.45 Students may fear that sharing mental health data, whether through apps, wearable devices, or AI-based assessments, could compromise confidentiality or be accessed by faculty in ways that affect academic standing.45–47 Additionally, user adherence is a common challenge; even well-designed tools may suffer from low engagement. One study found that although over half of college students had installed a mental health app, only ~19% used it consistently over time, citing concerns about privacy, complexity, and relevance to immediate needs.48 The risk of unintended labeling is also non-negligible: identified “at-risk” students may experience social isolation, altered perceptions by peers or instructors, or pressure to seek support before they are ready. This aligns with concerns from broader educational settings, where AI-based surveillance tools designed to detect mental health risks have been shown to disproportionately flag marginalized students and lead to unintended harms including disciplinary consequences.49 From a technical perspective, ensuring the security and ethical use of sensitive data demands robust encryption, secure storage, and clear limitations on access and data sharing.49,50 Furthermore, without transparent governance frameworks and institutional oversight, students may remain skeptical of the intent behind such initiatives. Thus, successful integration of digital screening or prediction systems into medical education must prioritize informed consent, ensure voluntary participation, and adopt student-centered design principles that respect autonomy, promote trust, and align with existing support services.51–53
Digital Mental Health Interventions
Digital mental health interventions for medical students range from Cognitive Behavioral Therapy-based (CBT-based) mobile apps to online counseling, virtual peer support, and blended approaches combining digital and in-person support (Table 1). Overall, these interventions demonstrate moderate improvements in depressive and anxiety symptoms, self-reflection, coping skills, mindfulness, empathy, and psychological resilience. For instance, CBT-based apps such as Woebot and an asynchronous digital cognitive behavioral intervention platform (DCE GAMA-AIMS) reduced depressive and anxiety symptoms, with effect sizes ranging from moderate (Hedges’ g ≈ 0.32) to large (effect size 1.32).54,55 Blended interventions, combining apps with institutional or in-person counseling, further enhanced coping and self-reflection, although some participants reported screen fatigue and time demands.56
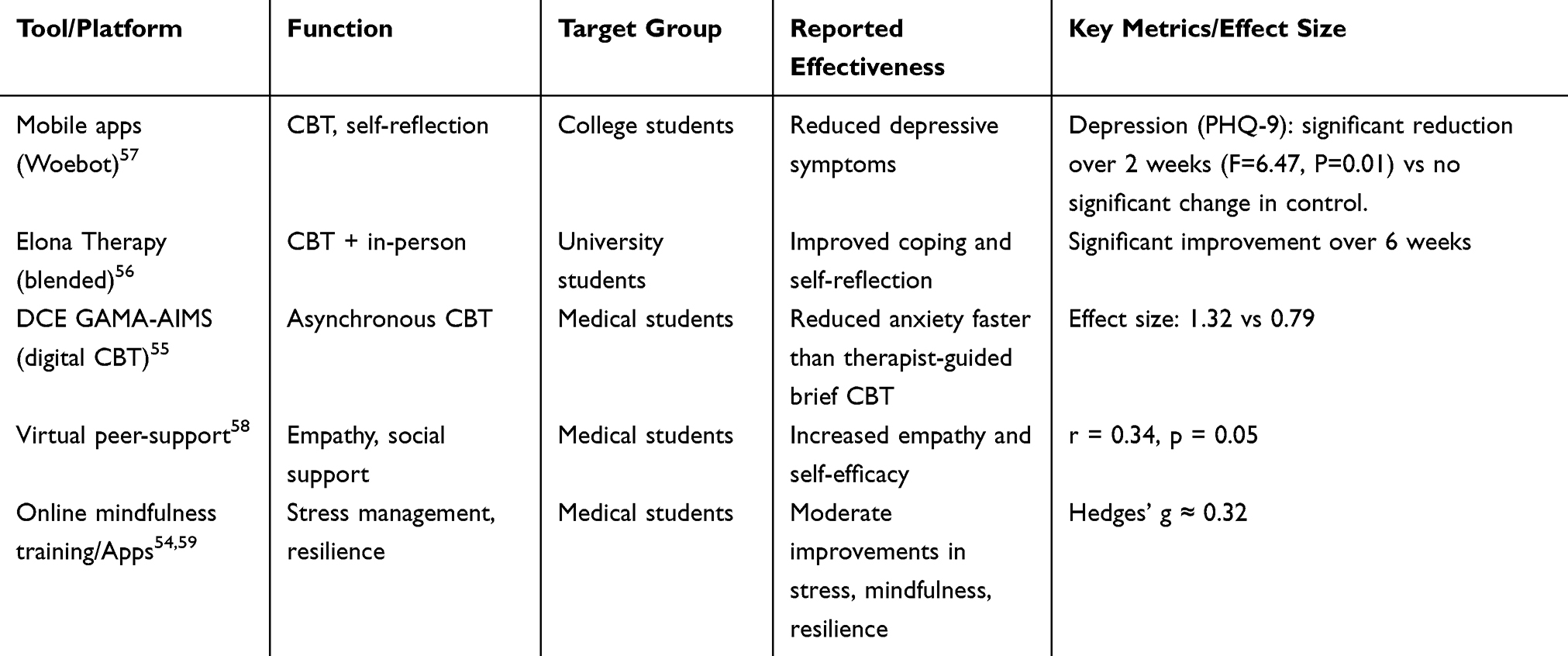 |
Table 1 Digital Tools for Managing Depression in Medical Students |
Virtual peer-support programs complement app-based interventions by fostering empathy and self-efficacy, reinforcing a help-seeking culture among medical students.58 While not purely digital, such near-peer models often complement anonymous or app-based platforms, reinforcing help-seeking culture59 While engagement and acceptability are generally high, challenges remain, including variable adherence, potential screen fatigue, and limited evidence for long-term effects. These findings suggest that multi-modal, blended digital approaches may be most effective in addressing the mental health needs of medical students.
Mental Health Competence in Medical Education
Mental Health Competence Concept
Our review highlights that medical students frequently experience psychological distress, yet current educational and digital interventions demonstrate variable effectiveness. Mental health competence, encompassing the ability to recognize distress, communicate empathetically, and manage sensitive clinical situations, aligns closely with competency-based medical education (CBME) frameworks and Entrustable Professional Activities (EPA).60 Tasks such as assessing distress or responding to distressed patients require integration of communication, clinical reasoning, and professional judgment. Evidence indicates that CBME-aligned programs can improve communication skills, confidence, and attitudes toward mental illness,61 with longitudinal mentorship and repeated reflective practice showing more sustained benefits than short-term interventions.62 These findings suggest that mental health competence develops gradually through repeated clinical and interpersonal experiences and is shaped by curriculum design, faculty role-modeling, and institutional culture.
Based on these findings, mental health competence should be considered a developmental process rather than a single educational outcome. Figure 1 illustrates an integrated framework encompassing early identification, competency-based education, and supportive learning environments.
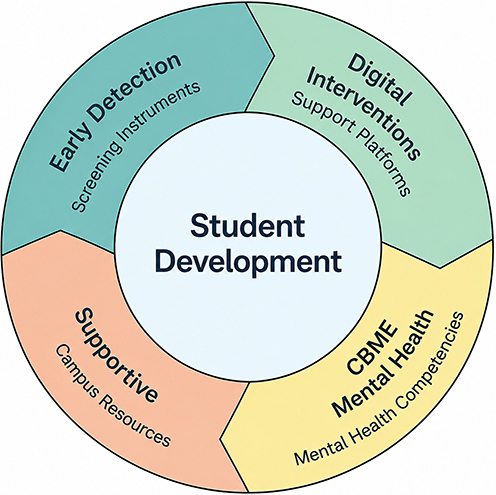 |
Figure 1 A Conceptual Framework for Promoting Mental Health Competence in Medical Education. Note: This figure was created by the authors. |
Education Strategies
Experiential teaching strategies are increasingly used in mental health education because they allow students to engage with the emotional and interpersonal aspects of patient care rather than focusing solely on theoretical knowledge. Methods such as case-based learning (CBL), role-playing, reflective writing, and narrative medicine are commonly incorporated into competency-based curricula to strengthen communication skills, empathy, and clinical preparedness.
Case-based learning facilitates integration of psychiatric knowledge with clinical reasoning, yet most studies report only short-term gains in academic performance or case-analysis ability.63 This suggests that while CBL may enhance cognitive understanding, it does not automatically translate into sustained clinical behavior or empathic patient interactions. Differences in intervention duration, facilitation quality, and cultural context likely contribute to inconsistent outcomes across studies, highlighting the importance of context-sensitive implementation.
Role-playing and simulation-based approaches may be particularly valuable in mental health training because students are required to respond to emotionally challenging situations in real time. Reviews report improvements in self-efficacy, emotional insight, and empathy,64 with cohort studies showing sustained increases in empathy scores after immersive simulation training.65 Critically, the magnitude and durability of these effects appear to depend on intervention intensity and structured reflective debriefing: brief workshops may provide immediate emotional engagement, whereas longitudinal programs are more likely to reinforce enduring behavioral change. This pattern underscores the importance of both repeated exposure and guided reflection in developing mental health competence.
Reflective writing and narrative medicine enhance self-awareness and professional identity formation. Evidence from guided reflection and patient storytelling interventions indicates improvements in empathy and patient-centered thinking,66–68 outcomes are largely self-reported, leaving uncertainty about translation into observable clinical behavior. This points to a recurring gap in the literature: the need for objective, longitudinal assessment of competence beyond immediate self-perceived gains.
The role of educators is equally critical. Compassionate faculty and emotionally supportive supervisors consistently serve as influential role models,69,70 suggesting that formal teaching alone is insufficient. Faculty development in trauma-informed care, anti-stigma communication, and emotionally responsive teaching may enhance students’ clinical skills and professional attitudes.71,72 In summary, patterns across the literature suggest that multi-faceted, longitudinal, and contextually adapted interventions, supported by reflective practice and engaged faculty, are most likely to foster durable mental health competence. Nevertheless, heterogeneity in study design, short follow-up periods, reliance on self-reported outcomes, and variable cultural adaptation limit generalizability and highlight clear directions for future research.
Assessment Approaches
Assessment of mental health competence remains challenging because the construct involves not only knowledge acquisition, but also empathy, communication, emotional responsiveness, and professional behavior. For this reason, no single assessment tool appears sufficient, and most educational programs rely on multiple complementary approaches.
Common methods include self-efficacy scales, Objective Structured Clinical Examinations (OSCEs), reflective exercises, and direct observation during clinical placements. Self-report measures can provide insight into students’ perceived confidence in managing mental health concerns, although confidence does not always correspond to actual clinical performance. Similarly, OSCE scenarios may be useful for assessing communication skills and recognition of psychological distress in simulated settings, but they may not fully capture the complexity of real patient interactions over time.
Direct observation during clinical training may offer a more authentic evaluation of students’ interpersonal and professional behaviors, particularly when managing emotionally sensitive situations. However, assessment practices remain highly variable across institutions, and few studies have examined whether improvements in educational settings translate into sustained behavioral change in clinical practice. Standardized assessment frameworks specific to mental health competence are still limited.
Limitations of Current Evidence and Future Directions
Current evidence on mental health interventions for medical students is limited by short-term or cross-sectional designs, reliance on self-reported outcomes, and a predominance of studies in high-income settings. These factors constrain understanding of sustained impact, real-world effectiveness, and cultural generalizability. Ethical considerations and faculty readiness for implementing digital or AI-assisted tools are rarely assessed, despite their potential influence on outcomes.
Future research should focus on longitudinal, culturally adapted studies using objective measures, with attention to ethical implications and faculty support. Such approaches are essential to ensure interventions are both effective and implementable across diverse educational contexts.
Conclusion
Addressing depression among medical students requires a comprehensive, multi-level approach, integrating both technological tools and educational strategies. Evidence suggests that combining early identification with competency-based training, longitudinal mentorship, and reflective practice may more effectively develop students’ ability to manage psychological distress. Consequently, fostering mental health literacy should be regarded as a core component of medical education, essential for preparing physicians who are both compassionate and resilient in real-world clinical practice.
Funding
BTCH 1st Young Talent Enlightenment Program (2024-2026) and The National Natural Science Foundation of China (8217053406).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214–10. doi:10.1001/jama.2016.17324
2. Al-Najdi S, Mansoor A, Al Hayk O, Al-Hashimi N, Ali K, Daud A. Silent struggles: a qualitative study exploring mental health challenges of undergraduate healthcare students. BMC Med Educ. 2025;25(1):157. doi:10.1186/s12909-025-06740-8
3. Phomprasith S, Karawekpanyawong N, Pinyopornpanish K, et al. Prevalence and associated factors of depression in medical students in a Northern Thailand University: a cross-sectional study. Healthcare. 2022;10(3). doi:10.3390/healthcare10030488
4. Boer C, Daelmans HEM. Team up with the hidden curriculum in medical teaching. Br J Anaesth. 2020;124(3):e52–e54. doi:10.1016/j.bja.2019.12.031
5. Howick J, Dudko M, Feng SN, et al. Why might medical student empathy change throughout medical school? A systematic review and thematic synthesis of qualitative studies. BMC Med Educ. 2023;23(1):270. doi:10.1186/s12909-023-04165-9
6. Dorevitch B, Buck K, Fuller-Tyszkiewicz M, Phillips L, Krug I. Maladaptive perfectionism and depression: testing the mediating role of self-esteem and internalized shame in an australian domestic and asian international university sample. Front Psychol. 2020;11:1272. doi:10.3389/fpsyg.2020.01272
7. Thomas M, Bigatti S. Perfectionism, impostor phenomenon, and mental health in medicine: a literature review. Int J Med Educ. 2020;11:201–213. doi:10.5116/ijme.5f54.c8f8
8. Heydari S, Beigzadeh A. Medical students’ perspectives of reflection for their professional development. BMC Med Educ. 2024;24(1):1399. doi:10.1186/s12909-024-06401-2
9. Pointon-Haas J, Waqar L, Upsher R, Foster J, Byrom N, Oates J. A systematic review of peer support interventions for student mental health and well-being in higher education. BJPsych Open. 2023;10(1):e12. doi:10.1192/bjo.2023.603
10. Hunt DF, Bailey J, Lennox BR, Crofts M, Vincent C. Enhancing psychological safety in mental health services. Int J Ment Health Syst. 2021;15(1):33. doi:10.1186/s13033-021-00439-1
11. Kurki M, Gilbert S, Mishina K, et al. Digital mental health literacy -program for the first-year medical students’ wellbeing: a one group quasi-experimental study. BMC Med Educ. 2021;21(1):563. doi:10.1186/s12909-021-02990-4
12. Sahan F, Guthardt L, Panitz K, et al. Enhancing digital health awareness and mhealth competencies in medical education: proof-of-concept study and summative process evaluation of a quality improvement project. JMIR Med Educ. 2024;10:e59454. doi:10.2196/59454
13. Dederichs M, Weber J, Pischke CR, Angerer P, Apolinário-Hagen J. Exploring medical students’ views on digital mental health interventions: a qualitative study. Internet Interv. 2021;25:100398. doi:10.1016/j.invent.2021.100398
14. Mekonnen CK, Abate HK, Beko ZW, Zegeye AF, Azagew AW. Prevalence of depression among medical students in Africa: systematic review and meta-analysis. PLoS One. 2024;19(12):e0312281. doi:10.1371/journal.pone.0312281
15. Mhata NT, Ntlantsana V, Tomita AM, Mwambene K, Saloojee S. Prevalence of depression, anxiety and burnout in medical students at the University of Namibia. S Afr J Psychiatr. 2023;29:2044. doi:10.4102/sajpsychiatry.v29i0.2044
16. AlJaber MI. The prevalence and associated factors of depression among medical students of Saudi Arabia: a systematic review. J Family Med Prim Care. 2020;9(6):2608–2614. doi:10.4103/jfmpc.jfmpc_255_20
17. Dhanoa S, Oluwasina F, Shalaby R, et al. Prevalence and correlates of likely major depressive disorder among medical students in Alberta, Canada. Int J Environ Res Public Health. 2022;19(18):11496. doi:10.3390/ijerph191811496
18. Paz DC, Bains MS, Zueger ML, et al. COVID-19 and mental health: a systematic review of international medical student surveys. Front Psychol. 2022;13:1028559. doi:10.3389/fpsyg.2022.1028559
19. Capdevila-Gaudens P, García-Abajo JM, Flores-Funes D, García-Barbero M, García-Estañ J. Depression, anxiety, burnout and empathy among Spanish medical students. PLoS One. 2021;16(12):e0260359. doi:10.1371/journal.pone.0260359
20. Silva V, Costa P, Pereira I, et al. Depression in medical students: insights from a longitudinal study. BMC Med Educ. 2017;17(1):184. doi:10.1186/s12909-017-1006-0
21. Jestin M, Sharma S, Jhaveri D, et al. Mental health differences in medical students based on curriculum and gender. BMC Med Educ. 2023;23(1):971. doi:10.1186/s12909-023-04946-2
22. Nyer M, Mischoulon D, Alpert JE, et al. College students with depressive symptoms with and without fatigue: differences in functioning, suicidality, anxiety, and depressive severity. Ann Clin Psychiatry. 2015;27(2):100–108. doi:10.1177/104012371502700204
23. Shah P, Sapkota A, Depression CA. Anxiety, and stress among first-year medical students in a tertiary care hospital: a descriptive cross-sectional study. JNMA J Nepal Med Assoc. 2021;59(236):346–349. doi:10.31729/jnma.6420
24. Ludwig AB, Burton W, Weingarten J, Milan F, Myers DC, Kligler B. Depression and stress amongst undergraduate medical students. BMC Med Educ. 2015;15(1):141. doi:10.1186/s12909-015-0425-z
25. Iorga M, Dondas C, Zugun-Eloae C. Depressed as freshmen, stressed as seniors: the relationship between depression, perceived stress and academic results among medical students. Behav Sci. 2018;8(8):70. doi:10.3390/bs8080070
26. Bußenius L, Harendza S. The relationship between perfectionism and symptoms of depression in medical school applicants. BMC Med Educ. 2019;19(1):370. doi:10.1186/s12909-019-1823-4
27. Neufeld A, Malin G. How medical students cope with stress: a cross-sectional look at strategies and their sociodemographic antecedents. BMC Med Educ. 2021;21(1):299. doi:10.1186/s12909-021-02734-4
28. Moutinho IL, Maddalena NC, Roland RK, et al. Depression, stress and anxiety in medical students: a cross-sectional comparison between students from different semesters. Rev Assoc Med Bras. 2017;63(1):21–28. doi:10.1590/1806-9282.63.01.21
29. Shafiee A, Teymouri Athar MM, Seighali N, et al. The prevalence of depression, anxiety, and sleep disturbances among medical students and resident physicians in Iran: a systematic review and meta-analysis. PLoS One. 2024;19(8):e0307117. doi:10.1371/journal.pone.0307117
30. Al Ani HM, Al Shawi AF, Lafta RK, Abdulqadir O, Nadhim S, Abdulkarim S. Influence of stress, anxiety, and depression on sleep quality and academic performance of medical students in Fallujah University, Iraq. Int J Soc Psychiatry. 2024;70(4):772–777. doi:10.1177/00207640241229381
31. Vidović S, Rakić N, Kraštek S, et al. Sleep quality and mental health among medical students: a cross-sectional study. J Clin Med. 2025;14(7):2274. doi:10.3390/jcm14072274
32. Abdollahi A, Hosseinian S, Asmundson GJG. Coping styles mediate perfectionism associations with depression among undergraduate students. J Gen Psychol. 2018;145(1):93–105. doi:10.1080/00221309.2017.1421137
33. Gärtner J, Bußenius L, Prediger S, Vogel D, Harendza S. Need for cognitive closure, tolerance for ambiguity, and perfectionism in medical school applicants. BMC Med Educ. 2020;20(1):132. doi:10.1186/s12909-020-02043-2
34. Costantini L, Pasquarella C, Odone A, et al. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473–483. doi:10.1016/j.jad.2020.09.131
35. Hasan MT, Khan MHA. Psychometric properties of the bangla version of the Beck Depression Inventory-II (BDI-II) with university students in bangladesh: a cross-sectional study. Health Sci Rep. 2025;8(1):e70280. doi:10.1002/hsr2.70280
36. Ramón-Arbués E, Gea-Caballero V, Granada-López JM, Juárez-Vela R, Pellicer-García B, Antón-Solanas I. The prevalence of depression, anxiety and stress and their associated factors in college students. Int J Environ Res Public Health. 2020;17(19):7001. doi:10.3390/ijerph17197001
37. Graves J, Flynn E, Woodward-Kron R, WCY H. Supporting medical students to support peers: a qualitative interview study. BMC Med Educ. 2022;22(1):300. doi:10.1186/s12909-022-03368-w
38. Guo X, Su T, Xiao H, Xiao R, Xiao Z. Using 24-h heart rate variability to investigate the sleep quality and depression symptoms of medical students. Front Psychiatry. 2021;12:781673. doi:10.3389/fpsyt.2021.781673
39. Zhang Y, Folarin AA, Stewart CL, et al. An explainable anomaly detection framework for monitoring depression and anxiety using consumer wearable devices. CoRR. 2025;05:
40. Wei Y, Qin S, Liu F, et al. Acoustic-based machine learning approaches for depression detection in Chinese university students. Original Research. Frontiers in Public Health. 2025. doi:10.3389/fpubh.2025.1561332
41. Menne F, Dörr F, Schräder J, et al. The voice of depression: speech features as biomarkers for major depressive disorder. BMC Psychiatry. 2024;24(1):794. doi:10.1186/s12888-024-06253-6
42. Donaghy P, Ennis E, Mulvenna M, et al. A review of studies using machine learning to detect voice biomarkers for depression. J Tech Behav Sci. 2024:1-5.doi:10.1007/s41347-024-00454-2
43. Lehtimaki S, Martic J, Wahl B, Foster KT, Schwalbe N. Evidence on digital mental health interventions for adolescents and young people: systematic overview. JMIR Ment Health. 2021;8(4):e25847. doi:10.2196/25847
44. Borelli JL, Wang Y, Li FH, et al. Detection of depressive symptoms in college students using multimodal passive sensing data and light gradient boosting machine: longitudinal pilot study. JMIR Form Res. 2025;9:e67964. doi:10.2196/67964
45. Montagni I, Tzourio C, Cousin T, Sagara JA, Bada-Alonzi J, Horgan A. Mental health-related digital use by university students: a systematic review. Telemed e-Health. 2020;26(2):131–146. doi:10.1089/tmj.2018.0316
46. Gulliver A, Bennett K, Bennett A, Farrer LM, Reynolds J, Griffiths KM. Privacy issues in the development of a virtual mental health clinic for university students: a qualitative study. JMIR Ment Health. 2015;2(1):e9. doi:10.2196/mental.4294
47. Parker L, Halter V, Karliychuk T, Grundy Q. How private is your mental health app data? An empirical study of mental health app privacy policies and practices. Int J Law Psychiatry. 2019;64:198–204. doi:10.1016/j.ijlp.2019.04.002
48. Melcher J, Camacho E, Lagan S, Torous J. College student engagement with mental health apps: analysis of barriers to sustained use. J Am Coll Health. 2022;70(6):1819–1825. doi:10.1080/07448481.2020.1825225
49. Koh J, Tng GYQ, Hartanto A. Potential and pitfalls of mobile mental health apps in traditional treatment: an umbrella review. J Personal Med. 2022;12(9):1376. doi:10.3390/jpm12091376
50. Palmer KM, Burrows V. Ethical and safety concerns regarding the use of mental health-related apps in counseling: considerations for counselors. J Technol Behav Sci. 2021;6(1):137–150. doi:10.1007/s41347-020-00160-9
51. Nock MK, Kleiman EM, Abraham M, et al. Consensus statement on ethical & safety practices for conducting digital monitoring studies with people at risk of suicide and related behaviors. Psychiatric Res Clin Pract. 2021;3(2):57–66. doi:10.1176/appi.prcp.20200029
52. McInnis BJ, Pindus R, Kareem D, Nebeker C. Considerations for the design of informed consent in digital health research: participant perspectives. J Empir Res Hum Res Ethics. 2024;19(4–5):175–185. doi:10.1177/15562646241290078
53. Yusof MYPM, Teo CH, Ng CJ. Electronic informed consent criteria for research ethics review: a scoping review. BMC Med Ethics. 2022;23(1):117. doi:10.1186/s12910-022-00849-x
54. Ferrari M, Allan S, Arnold C, et al. Digital interventions for psychological well-being in university students: systematic review and meta-analysis. J Med Internet Res. 2022;24(9):e39686. doi:10.2196/39686
55. Kusumadewi AF, Marchira CR, Widyandana D, Wirasto RT. Randomized clinical trial comparing the effects of an asynchronous mobile application to guided brief cognitive behavioral therapy for managing anxiety among medical students. Trends Psychiatry Psychother. 2025;47:e20230713. doi:10.47626/2237-6089-2023-0713
56. Braun P, Atik E, Guthardt L, Apolinário-Hagen J, Schückes M. Barriers to and facilitators of a blended cognitive behavioral therapy program for depression and anxiety based on experiences of university students: qualitative interview study. JMIR Form Res. 2023;7(e45970):e45970. doi:10.2196/45970
57. Fitzpatrick KK, Darcy A, Vierhile M. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (woebot): a randomized controlled trial. JMIR Ment Health. 2017;4(2):e19. doi:10.2196/mental.7785
58. Abrams MP, Salzman J, Espina Rey A, Daly K. Impact of providing peer support on medical students’ empathy, self-efficacy, and mental health stigma. Int J Environ Res Public Health. 2022;19(9):5135. doi:10.3390/ijerph19095135
59. Moore S, Mavaddat N, Auret K, et al. The Western Australian medical schools mindfulness project: a randomised controlled trial. BMC Med Educ. 2024;24(1):1182. doi:10.1186/s12909-024-06128-0
60. Ten Cate O. Competency-based postgraduate medical education: past, present and future. GMS J Med Educ. 2017;34(5):Doc69. doi:10.3205/zma001146
61. Sethuraman B, Chari U, Perugu S, Salazar LJ, Students’ SP. Perspectives of competency-based medical education in undergraduate psychiatry clinical training: a qualitative evaluation. Indian J Psychol Med. 2024;46(5):400–407. doi:10.1177/02537176241265484
62. Goel A, Sethi Y, Moinuddin A, Deepak D, Gupta P. Competency-based medical education (CBME) curriculum and its effect on prevalence of anxiety, depression and stress amongst medical undergraduates. J Educ Health Promot. 2022;11:380. doi:10.4103/jehp.jehp_564_22
63. Rønning SB, Bjørkly S. The use of clinical role-play and reflection in learning therapeutic communication skills in mental health education: an integrative review. Adv Med Educ Pract. 2019;10:415–425. doi:10.2147/amep.S202115
64. Mavis B. Self-efficacy and OSCE performance among second year medical students. Adv Health Sci Educ Theory Pract. 2001;6(2):93–102. doi:10.1023/a:1011404132508
65. Avlogiari E, Maria Karagiannaki S, Panteris E, Konsta A, Diakogiannis I. Improvement of medical students’ empathy levels after an intensive experiential training on empathy skills. Psychiatry Clin Psychopharmacol. 2021;31(4):392–400. doi:10.5152/pcp.2021.21098
66. Lim JY, Ong SYK, CYH N, et al. A systematic scoping review of reflective writing in medical education. BMC Med Educ. 2023;23(1):12. doi:10.1186/s12909-022-03924-4
67. Charon R. Narrative Medicine: Honoring the Stories of Illness. Oxford University Press; 2006; doi:10.1093/oso/9780195166750.001.0001
68. Kagawa Y, Ishikawa H, Son D, et al. Using patient storytelling to improve medical students’ empathy in Japan: a pre-post study. BMC Med Educ. 2023;23(1):67. doi:10.1186/s12909-023-04054-1
69. Bogerd R, Silkens MEWM, Boerebach B, Henriques JPS, KMJMH L. Compassionate behavior of clinical faculty: associations with role modelling and gender specific differences. Perspect Med Educ. 2025;14:118–128. doi:10.5334/pme.1481
70. Ahmadian Yazdi N, Bigdeli S, Soltani Arabshahi SK, Ghaffarifar S. The influence of role-modeling on clinical empathy of medical interns: a qualitative study. J Adv Med Educ Prof. 2019;7(1):35–41. doi:10.30476/jamp.2019.41043
71. Chokshi B, Walsh K, Dooley D, Falusi O, Deyton L, Beers L. Teaching trauma-informed care: a symposium for medical students. MedEdPORTAL. 2020;16:11061. doi:10.15766/mep_2374-8265.11061
72. Omid A, Haghani F, Toufan N. Developing a model for clinical teaching with emotional intelligence. BMC Med Educ. 2024;24(1):1404. doi:10.1186/s12909-024-06349-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Impact of COVID-19 on Doctors and Medical Students of Punjab, Pakistan: A Logistic Regression Analysis
Junaid Tahir M, Tariq W, Anas Tahseen Asar M, Irfan Malik M, Kamal Akhtar F, Malik M, Akhtar Q, Abbasher Hussien Mohamed Ahmed K, Talha Awan M, Ullah K, Asghar MS
Journal of Multidisciplinary Healthcare 2022, 15:1297-1308
Published Date: 8 June 2022
Moderation Effects of Positive Core Belief and Social-Emotional Responsiveness on the Relationship Between Cyberbullying Victimization and Affective Symptoms
Nisu S, Anuroj K, Wannaiampikul S, Pangsorn A, Chiencharoenthanakij R, Chongbanyatcharoen S
Psychology Research and Behavior Management 2023, 16:2545-2551
Published Date: 6 July 2023
Prevalence and Associations of Night Eating Syndrome Among Medical Students in Saudi Arabia
Haneef S, Almuammar S
Psychology Research and Behavior Management 2024, 17:529-535
Published Date: 14 February 2024
A Study on the Association Between Risk Factors and Psychosocial Factors of Non-Cardiac Chest Pain (NCCP) in Adults Aged 40 and Above Based on 2013-2018 US NHANES Data
Chen Y, Li S, Guo F
Journal of Pain Research 2025, 18:7245-7259
Published Date: 30 December 2025