")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Psychological Impact of COVID-19 on Doctors and Medical Students of Punjab, Pakistan: A Logistic Regression Analysis
Authors Junaid Tahir M , Tariq W, Anas Tahseen Asar M, Irfan Malik M, Kamal Akhtar F , Malik M, Akhtar Q, Abbasher Hussien Mohamed Ahmed K , Talha Awan M, Ullah K , Asghar MS
Received 5 April 2022
Accepted for publication 27 May 2022
Published 8 June 2022 Volume 2022:15 Pages 1297—1308
DOI https://doi.org/10.2147/JMDH.S369452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Muhammad Junaid Tahir,1 Waleed Tariq,1 Muhammad Anas Tahseen Asar,1 Muhammad Irfan Malik,1,2 Fahd Kamal Akhtar,1 Muna Malik,3 Qirat Akhtar,4 Khabab Abbasher Hussien Mohamed Ahmed,5 Muhammad Talha Awan,1 Kaleem Ullah,6 Muhammad Sohaib Asghar7
1Lahore General Hospital, Lahore, Pakistan; 2Postgraduate Medical Institute, Lahore, Pakistan; 3Combined Military Hospital, Lahore, Pakistan; 4Army Medical College, Rawalpindi, Pakistan; 5University of Khartoum, Faculty of Medicine, Khartoum, Sudan; 6Pir Abdul Qadir Shah Jeelani Institute of Medical Sciences, Gambat, Sindh, Pakistan; 7Dow University of Health Sciences–Ojha Campus, Karachi, Pakistan
Correspondence: Khabab Abbasher Hussien Mohamed Ahmed, Faculty of Medicine, University of Khartoum, Khartoum, 11111, Sudan, Email [email protected]
Background: This study was carried out to find the awareness level, prevalence of anxiety and depression, and their associated factors among doctors and medical students during the COVID-19 pandemic in Punjab province, Pakistan.
Materials and Methods: An online questionnaire-based cross-sectional study was conducted; data were collected regarding the demographic profile, awareness of COVID-19, anxiety symptoms using a self-rating anxiety scale (SAS), and depression symptoms using a self-rating depression scale (SDS). A total of 504 responses were obtained. The Chi-square test was used to compare groups and the logistic regression model for the association of factors with anxiety and depression.
Results: A total of 504 medical students and doctors responded to the questionnaire. The mean age of participants was 25.66 ± 6.71 years. The awareness rate of COVID-19 was 97.6%. The prevalence rate of anxiety and depression was 3.4% and 15.1%, respectively. According to the logistic regression model, those with low awareness levels (≤ 6 points) and spending more time on the news (> 3 hours) had higher levels of anxiety, while higher levels of depression symptoms were reported in females, young people, and medical students.
Conclusion: Doctors and medical students had a high level of awareness of COVID-19 and a low level of anxiety and depression. However, female gender and younger age group were the most vulnerable groups significantly associated with depression.
Keywords: COVID-19, doctors, medical students, awareness, anxiety, depression, infection
Introduction
Coronavirus disease 2019 (COVID-19) belongs to a group of acute respiratory disorders, which was reported for the first time in Wuhan Hubei, China. The agent responsible for this disease was labeled as 2019-CoV. It was a newly found strain of the virus that was unknown to man.1–3 Later, it was named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by the International Committee on Taxonomy of Viruses because of its resemblance to SARS CoronaVirus. The World Health Organization (WHO) has named this respiratory disease COVID-19. On 11th March 2020, WHO declared the COVID-19 pandemic.4
SARS-CoV-2 has raised concerns due to its rapid transmission via coughing or sneezing aerosols, nasal discharge, saliva, urine and stool, and close contact with an infected person.5,6 According to WHO, COVID-19 situation report (March 7, 2022), a total of445096612cases have been confirmed including5998301deaths. In Pakistan, up till now, 1515392cases have been confirmed including30281deaths.7 COVID-19 is creating a massive effect worldwide affecting every part of human society as reducing economic activities and increasing financial insecurity and unemployment. Furthermore, adaptations to new routines such as the closure of institutes, work from home, ban on social gatherings and increase in self-dependence and application of technology have contributed to the mental health burden.8 Lower-middle-income countries (LMICS) are at major risk of economic and healthcare collapse due to scarcity of resources to support physical and mental health care, thus extending to an increase in the risk of suicide rate in North America.9
A COVID-19 pandemic is an unprecedented event with marked miscommunication leading to misconceptions that can lead to inappropriate actions regarding the prevention of disease.10,11 Adults more than 60 years of age or those with severe medical conditions such as diabetes, heart, or lung diseases are the most susceptible groups to acquiring infections.12 Pregnant women, psychiatric patients, students, and adolescents are at major risk of psychological disturbance under the lockdown situation, reducing their access to healthcare support.13–16
In the present situation, health care workers (HCWs) are directly involved in the care of COVID-19 patients. As they are in close contact with the patients, they are at greater risk of acquiring the disease.2 The rapidly increasing number of suspected and confirmed cases, extreme workload, inadequate protective equipment, shortage of drugs and hand sanitizers, widespread media coverage, and feeling of lack of support may increase the physical and mental burden for these HCWs.11,17 According to recent reports, a large number of medical staff have acquired the infection while treating the infected patients leading to their deaths.18 This insecurity and all other factors are making them more liable to develop anxiety and depression. Data acquired from previous epidemic studies show that during these situations of physical and mental overload HCWs develop a high level of stress, depression, and anxiety which have long-term psychological effects on their professional as well as personal life.19,20 It reduces their efficiency as medical professionals thus producing more burden on the healthcare departments that are suffering from the pandemic.
The COVID-19 pandemic has also affected education just like other human activities, leading to drastic changes in patterns of education from face-to-face, real-time interaction to online teaching. Despite the rapid advancements in information and communication technology (ICT), the world is still unknown to online teaching techniques.21 Video conferencing and social media have been popular ways for student and teacher interaction but the development of new collaboration tools is needed for teaching a course. Medical education has also shifted from traditional to digital learning. Clinical skills have been tutored through online simulations, but it has been agreed that there is no replacement for direct hands-on learning and direct interaction with the patients.22 Psychological health of the medical students has also been affected by the COVID-19 pandemic due to the changes in the learning techniques and fear of acquiring infection and lockdown situation.2
Therefore, it is necessary to assess the mental health of doctors and medical students during the COVID-19 pandemic by quantifying the symptoms of anxiety and depression and exploring the potential risk factors associated with these symptoms. We hope our study findings will serve as important evidence for the targeted interventions and promotion of psychological health among doctors and medical students.
Materials and Methods
Due to the lockdown situation in Pakistan, a web-based cross-sectional survey (Google forms) was used for the collection of data from doctors and medical students in Punjab Province, Pakistan, for the period of 4 weeks from March 30, 2020, to April 27, 2020. Data was collected through friend circle forwarding, WhatsApp sharing, and other social media platforms. This participation was completely voluntary and participants could withdraw from the survey at any moment as per their choice. Electronic informed consent was obtained from each participant before the survey.
All the participants provided their demographic data, and knowledge about COVID-19, and also filled out two standardized questionnaires, which assessed their depression and anxiety. The minimum age limit for answering the questionnaire was set at 15 years. All those with serious mental illness or diseases which affect their mental health were excluded. In total, 504 volunteers who responded to the questionnaire participants (60.6% response rate) were included in the study.
Demographic information included gender, age, and profession. Professions included two categories: (1) Doctors of all specialties and (2) Medical students, which included students of all years of MBBS.
For the section regarding the COVID-19 information, was divided into two parts: (1) Daily average time spent to acquire information regarding the COVID-19 pandemic and (2) COVID-19 related knowledge, which included twelve judgment questions: (a) Accurate incubation period of SARS-CoV-2; (b) Symptom mostly present in COVID-19 patient; (c) Mode of transmission of disease; (d) Duration of isolation of a person in contact with COVID-19 patient; (e) Severe cases can cause pneumonia, heart failure, kidney failure, and death; (f) Estimated mortality rate; (g) Diagnostic test used; (h) Any specific medication for treatment or prevention of COVID-19; (i) Currently any vaccine available; (j) COVID-19 affects only old age people and infant or not; (k) Rate of infection transmission is more in a hot and humid environment; (l) No need to wear a medical mask if not interacting with COVID-19 patient; (m) Best preventing measure is frequent hand washing. One point was given for each correct answer, and no points were for uncertain or incorrect answers. A self-structured scoring system was used. A Score of less than 6 was considered unaware, 7–10 aware and 11–13 well aware.
For quantitative analysis of anxiety, Zung Self-rating Anxiety Scale (SAS)23 and for depression Zung Self-rating Depression Scale (SDS)24 were used. SAS and SDS had been used in the previous studies11 and found to have good reliability (Cronbach’s alpha = 0.804 and 0.864 for SAS and SDS, respectively, for the present study). Both SAS and SDS have 20-item Likert and norm-referenced scales using a 4-point scale ranging from 1 (a little of the time, or none) to 4 (all of the time, or most). Based on this scoring system, a 20-item scale is asked regarding psychological and physiological symptoms that a patient felt during the previous week. The total score of SAS and SDS range from 20-to 80, the greater the score, the more the level of anxiety and depression. SAS/SDS scores of 50–59 points, 60–69 points, and 70 or more indicate mild, moderate, and severe anxiety and depression, respectively.23,24
A descriptive analysis was conducted to describe the demographic profile and awareness related to COVID-19 among doctors and medical students of Punjab Province, Pakistan. The prevalence of anxiety and depression stratified by gender, age, profession, awareness, prior knowledge about COVID-19, and time spent on the news were reported. The Chi-square test was used to compare the differences between groups. Using the logistic regression model, we explored potential influencing factors for anxiety and depression during the COVID-19 pandemic. We obtained an odds ratio (OR) with a 95% confidence interval (95% CI) from the above-mentioned logistic regression model. All the data were analyzed using SPSS version 22.0 and a p-value <0.05 was considered significant.
Results
A total of 504 doctors and medical students responded to the survey. Of 504 participants, 285 (56.5%) were females and 219 (43.5%) were males. The majority of respondents were from the age group 21–30 (66.3%) with a mean age of 26.42 ± 6.71 years (mean ± SD). Among all respondents, 243 (48.2%) were doctors and 261 (52.8%) were medical students. About 209 (41.5%) respondents were aware of the coronavirus before the COVID-19 pandemic. The majority 301 (60.5%) spent less than an hour daily on information regarding COVID-19, 274 (54.4%) were well aware of knowledge regarding COVID-19, 17 (3.4%) were having anxiety symptoms and 76 (15.1%) were suffering from symptoms of depression as shown in Table 1.
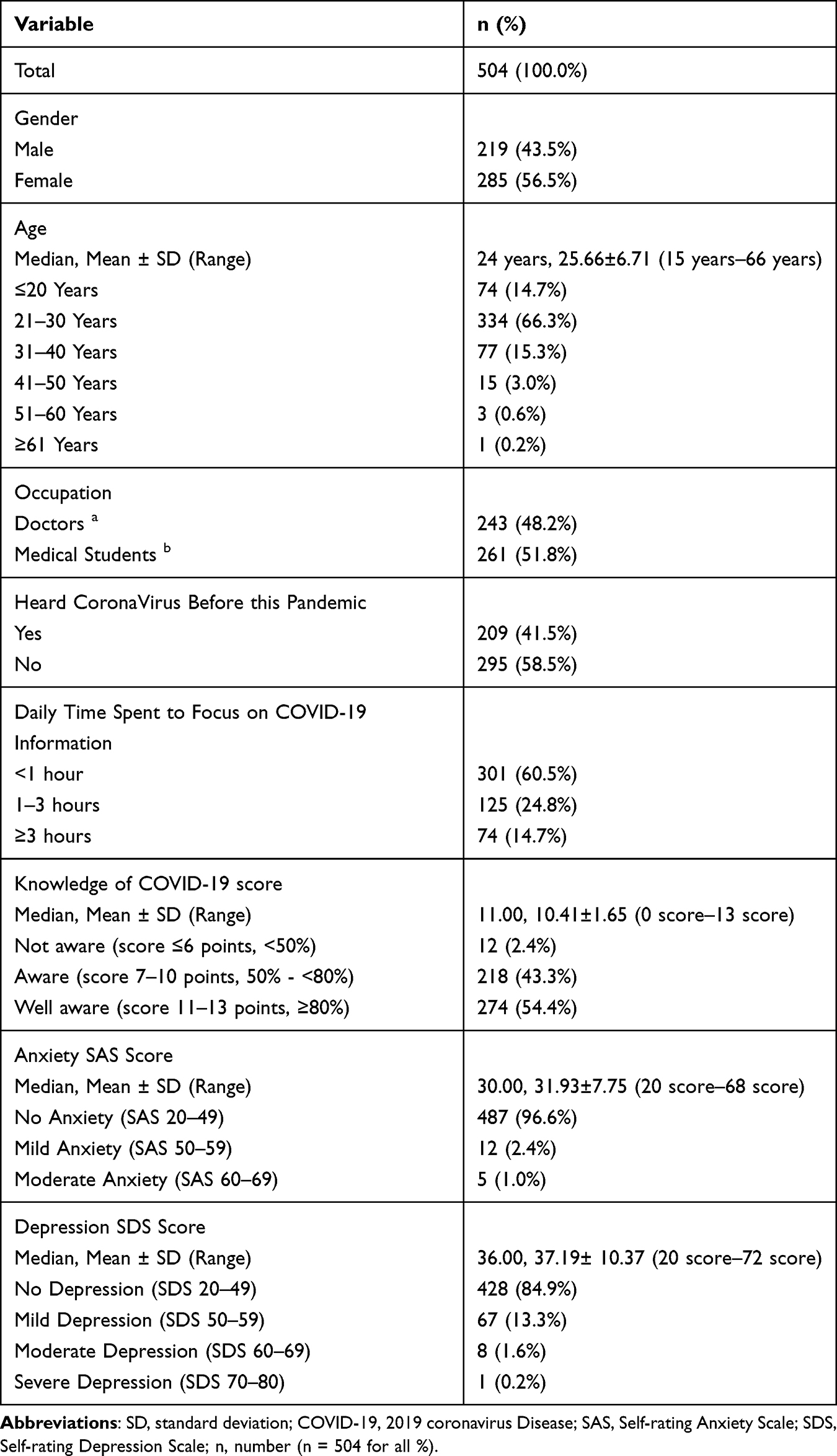 |
Table 1 Demographic Profile, Knowledge, SAS, and SDS Scores of Study Sample (n = 504) |
Table 2 shows the awareness of COVID-19 among various groups, such as gender and age group, based on previous knowledge and time spent on the news. The level of well awareness among males (27.6%) and females (26.8%) is comparable (p < 0.01). Most of the participants who were well aware (11–13 points) belong to the age group 21–30 (p<0.001). The 157 (31.2%) doctors and 117 (23.2) medical students are well aware of the COVID-19 pandemic (p < 0.01). The respondents without previous knowledge (31.2%) of SARS Corona Virus had a higher level of well awareness than those with prior knowledge (23.2%) (p > 0.05). The percentage of being well aware in participants who spend less than 1 hour, 1 to 3 hours, and more than 3 hours on news is 29.6%, 15.7%, and 9.1%, respectively (p < 0.05).
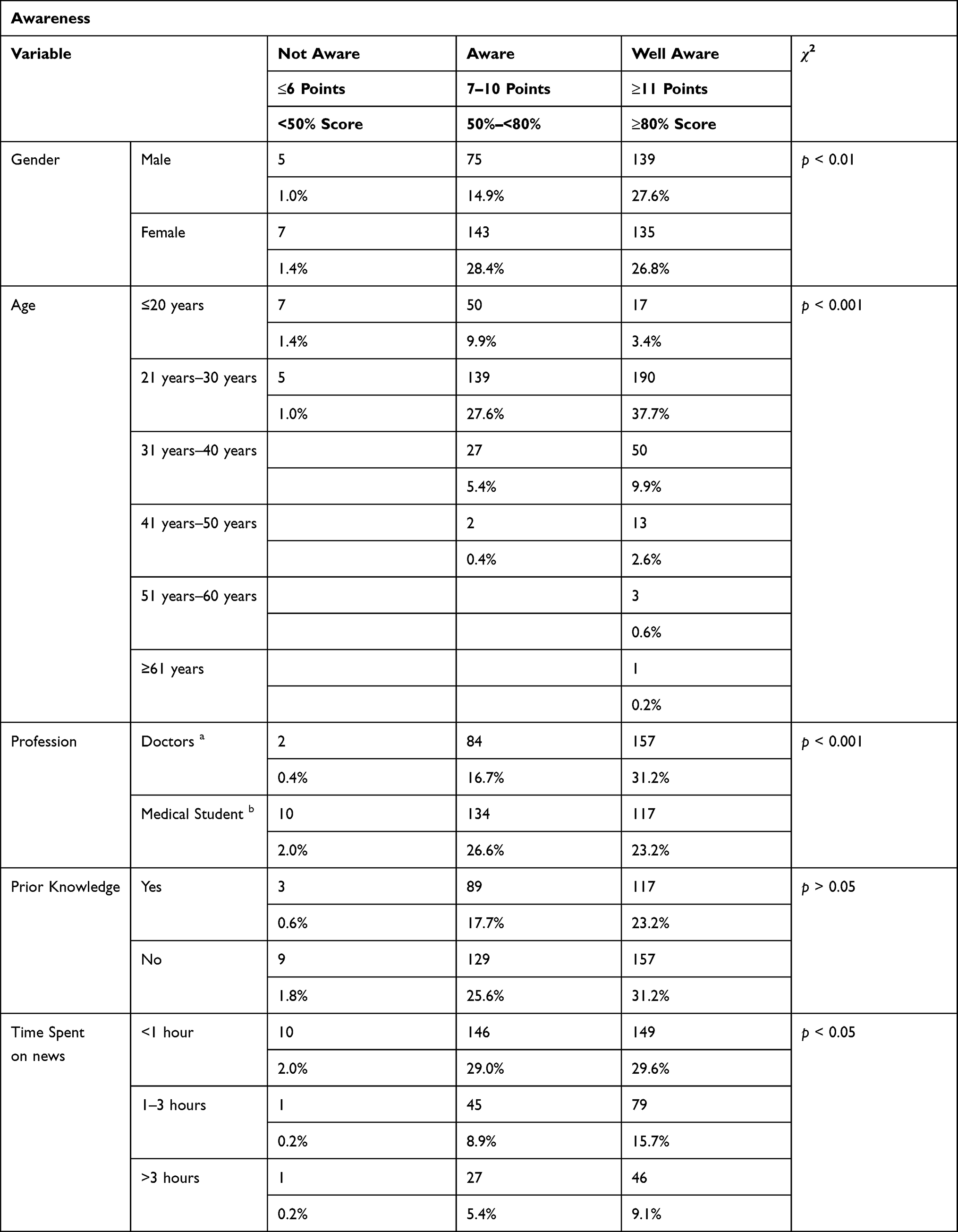 |
Table 2 Awareness of COVID-19 Pandemic in Doctors and Medical Students in Punjab Province, Pakistan, Stratified by Gender, Age, Profession, Prior Knowledge, and Time Spent on the News (n = 504) |
Table 3 shows the prevalence of anxiety according to demographics. Females 12 (2.4%) were more anxious as compared to males 5 (1%) (p>0.05). Participants belonging to the age group 21–30 are having more anxiety 12 (2.4%) than other age groups (p > 0.05). The level of anxiety in medical students 11 (2.2%) is comparable to doctors 6 (1.2%). The anxiety in respondents not aware (0.4%), aware (1.2%) and well aware (1.8%) is analogous (p > 0.05). Similarly, anxiety level on the basis of time spent on news less than 1 hour, 1–3 hours, and more than 3 hours is 1.4%, 0.6%, and 1.4%, respectively (p < 0.05).
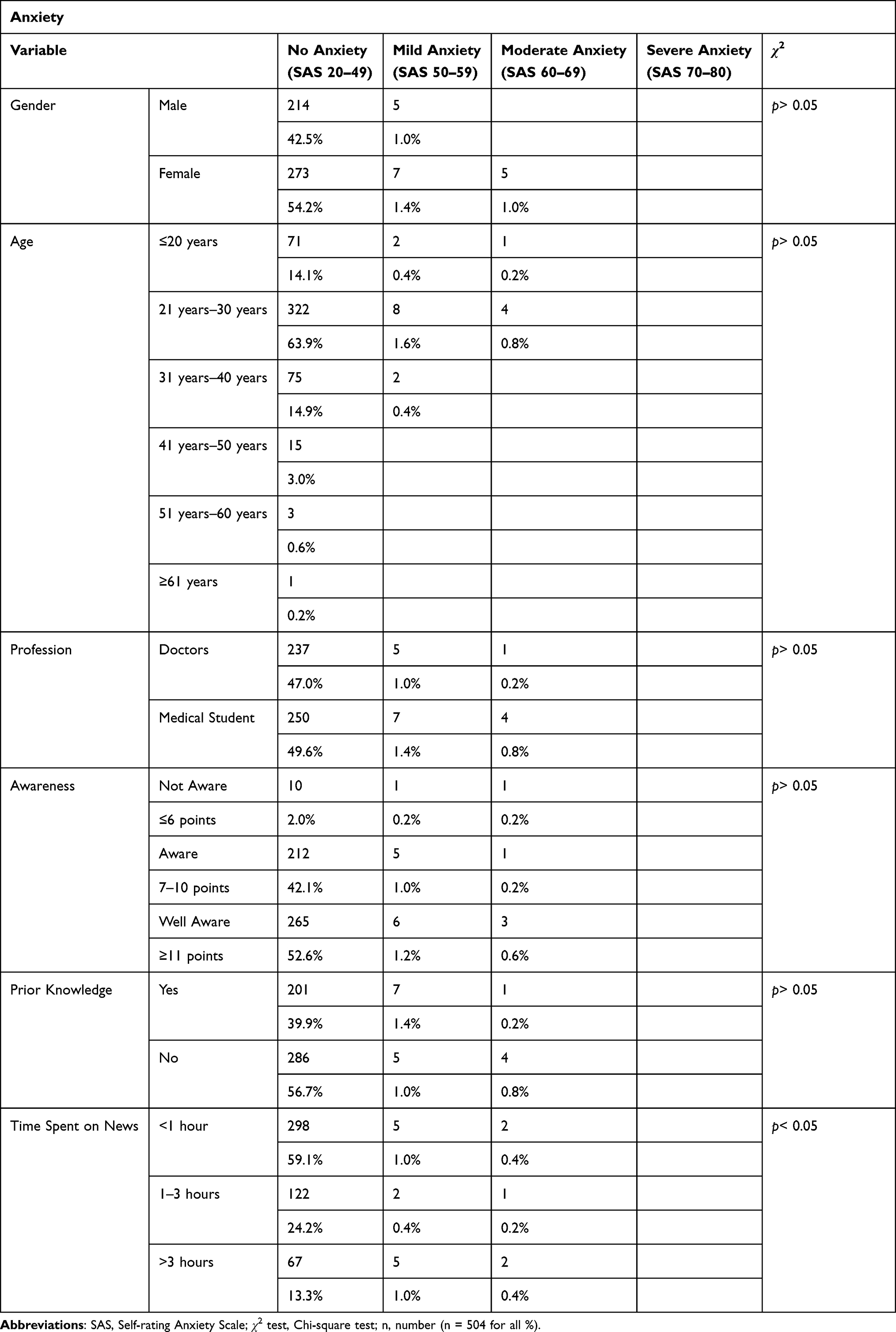 |
Table 3 Prevalence of Anxiety in Doctors and Medical Students in Lahore, Pakistan, Stratified by Gender, Age, Profession, Awareness Level, Prior Knowledge, and Time Spent on the News (n = 504) |
Table 4 depicts the prevalence of depression. Females (51, ie, 11.1%) and medical students (47, ie, 9.3%) had higher levels of depression than males (25, ie, 5%) and doctors (29, ie, 5.8%), respectively (p > 0.05). The age group less than 30 years has more prevalence of depression (13.9%) than more than 30 years (1.2%) (p > 0.05). The depression in those being well aware (7.6%) and aware (6.6%) is more than in those not aware (0.8%). The depression level in those having prior knowledge (7.3%) and no prior knowledge (7.7%) is comparable (p>0.05). The depression in those time spent on news less than an hour (9.3%) is higher than those who spend 1 to 3 hours (3.6%) and more than 3 hours (2.2%) on news (p>0.05).
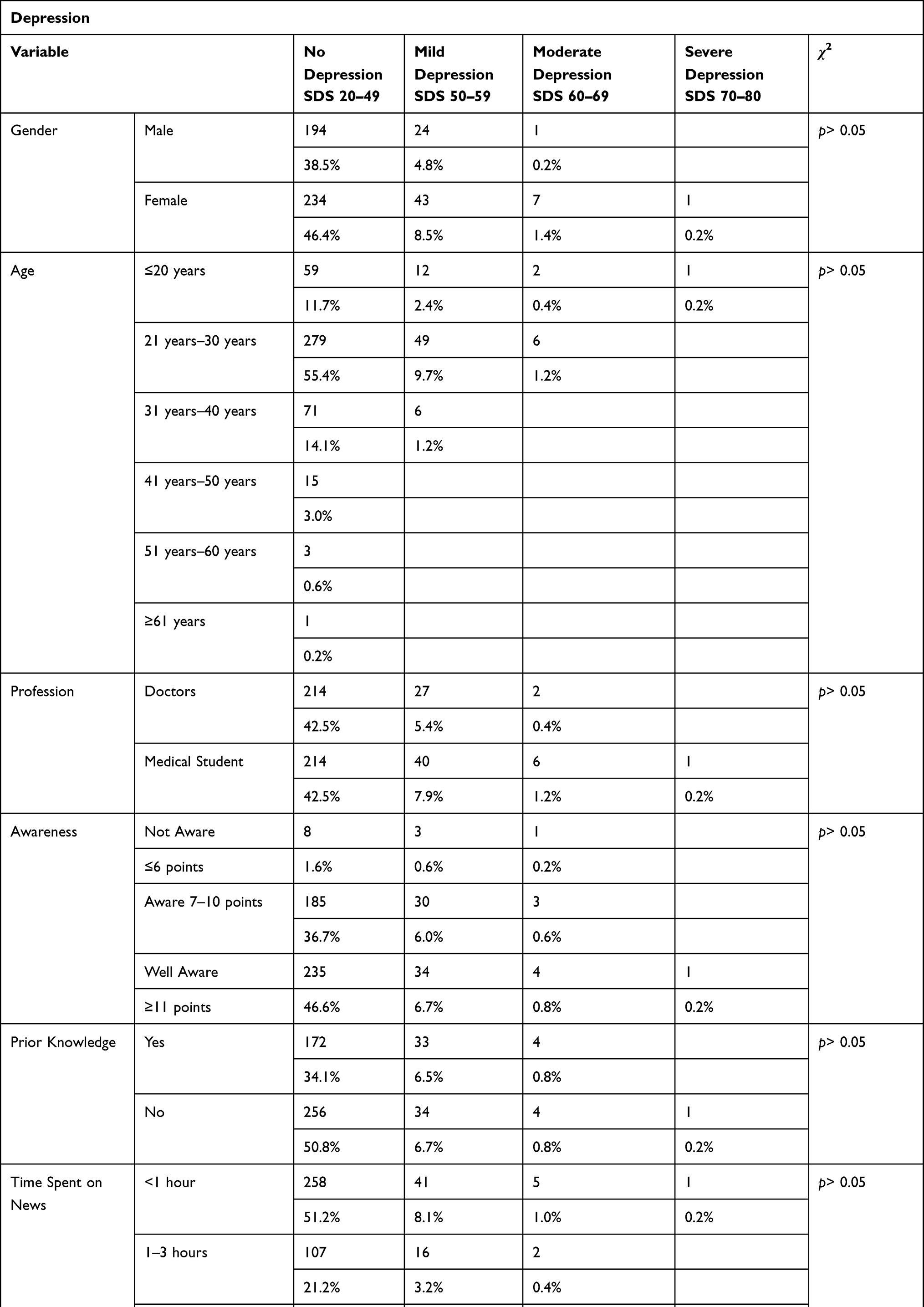 |
Table 4 Prevalence of Depression in Doctors and Medical Students in Punjab Province, Pakistan, Stratified by Gender, Age, Profession, Awareness Level, Prior Knowledge, and Time Spent on the News (n = 504) |
The associations of different influencing factors with anxiety and depression studied in this survey are shown in Table 5. In logistic regression models, gender (ie female) was significantly associated with anxiety (OR = 1.88, 95% CI = 0.65–5.43) and depression (OR = 1.69, 95% CI = 1.01–2.83). Medical students showed significant association with anxiety (OR = 1.74, 95% CI = 0.63–4.78) and depression (OR = 1.62, 95% CI = 0.98–2.67). Low awareness level (not aware) also had a significant association with both anxiety (OR = 6.37, 95% CI = 1.28–31.25) and depression (OR = 2.91, 95% CI = 0.86–9.90).
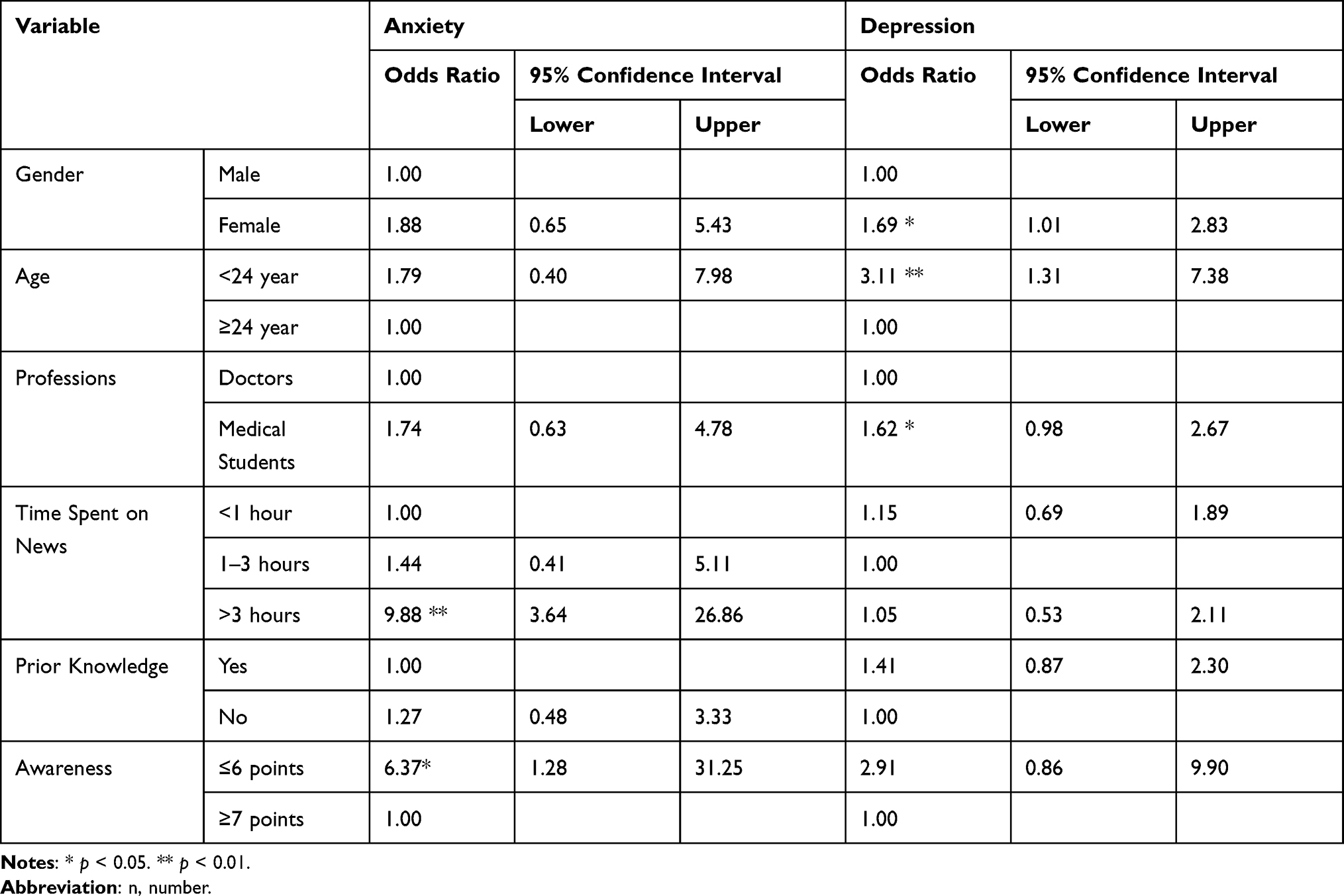 |
Table 5 Results of Logistic Regression Analyses (n = 504) |
Discussion
The effect of COVID-19 on the world had been considered significant, causing fear, anxiety, and depression particularly due to the uncertainty of the prognosis of the disease, and the absence of significant and distinct signs and symptoms to differentiate it from common illnesses. Changes in social lifestyles, lockdown restrictions, and educational disruptions had put a halt to a healthy lifestyle.5 Due to COVID-19 being a highly contagious disease and an increase in the number of reported cases, health care workers being front-line warriors were at more risk of getting the infection. Increased occupational burden and fear of acquiring infection could lead to an increased level of stress among them.19
In our study, awareness in participants was 97.6%, comparable to the awareness level of 90% reported by a survey conducted by Hussain et al5 Higher awareness levels in our study could be due to our sample population, which included only doctors and medical students that usually had more knowledge regarding health issues. In this study, the level of awareness among doctors was 99.1%, and medical students were 96.1%. That was significantly higher than reported in Mumbai, India, by Modi et al 72.1% and 74.1%, respectively.2 This difference could be due to a gap in the time of study conduction. As COVID-19 pandemic is progressing day by day, making them concerned about their personal and family health as well as patient well-being. Thus, expanding their knowledge related to COVID-19. It had been seen in previous studies that health professionals often had more awareness, and positive attitudes towards epidemics, and they often experience low levels of anxiety.25
According to our survey, females suffered more from anxiety and depression due to COVID-19 than males. This result was consistent with the previous studies that females had more psychological disorders, such as stress, anxiety, and depression during the pandemic.26 Lim et al had reported that the women had the higher rates of point prevalence of depression (14%).27
The anxiety was more pronounced in the age group of less than 40 as it was reported by Hyang and Zhao, in which the age group was less than 35 was more anxious.1 As young people became more socially active, excessive coverage of the COVID-19 pandemic had made it nearly impossible to avoid anxiety and depression related to COVID-19. Social distancing and reduction in social activities were also considerable factors further contributing to this condition.28
The levels of anxiety and depression in doctors were 2.4% and 11.9%, respectively, while the levels of anxiety and depression reported by Zhu et al were lesser, ie, 11.1% and 45.6%, respectively.19 This could be attributed to the increase in the knowledge about COVID-19 as more time had passed since the pandemic started, gaining more experience by dealing with the patients, and the low number of locally reported cases and mortality rate in Punjab, Pakistan. Previous epidemics such as the SARS outbreak in 2003 had also created various psychological manifestations similar to traumatic events such as PTSD (Post Traumatic Stress Disorder), anxiety, and depression.20
The level of anxiety reported in medical students was 4.2%, which was lower than that reported by Sadik et al, ie, 26%. A higher level of awareness consisting of accurate information reduces anxiety.29 Similarly, the depression level found was 18%, which was also low as compared to Bhattacharya et al, ie, 40%.30 The disturbance in the educational patterns and fear of uncertainty of future in this stressful era of COVID-19 raises the risk of psychological disturbance in students.26,28 The risk of acquiring infection and transmission to their family members and friends also raised concerns.30,31
Awareness about COVID-19 was significantly associated with the level of anxiety. A higher level of anxiety was found among those with low awareness of COVID-19. During distressing periods, people try to obtain information from multiple sources that lead to both true and fake stories. A rapid increase in the spread of infection had disseminated the information worldwide. It also includes myths and irrelevant facts, especially when information is inaccurate and inconsistent.32 These factors could lead people to panic. In contrast, the availability of satisfying and authentic health information could enhance awareness, produce less psychological impact and reduce stress, anxiety, and depression.26
Those people who spent more time acquiring COVID-19-related information on news, social media, and other sources, had more symptoms of anxiety. The same pattern was reported by Huang and Zhao in China.1 In this age of social media which had become a major source of information, the news spreads rapidly without verifying its authenticity. The splendid headlines and self-serving coverage of the news frighten their viewers.33 The fear of self-infection induces the adoption of dreadful behaviors. It is a natural response of humans to develop anxiety in response to stressful situations.1,34
Immediate interventions are required to prevent the development of psychological effects of the COVID-19 pandemic. Special attention is needed to reduce the workload of health care professionals. To cope with the mental effects of the outbreak, the use of the internet has to be promoted for psychotherapeutic interventions such as internet cognitive behavioral therapy (I-CBT) and mindfulness-based cognitive therapy (MBCT) that has proved to be useful and efficient. Efforts should be made to limit the time spent on receiving information related to COVID-19.35 The focus had to be on facts only, and the spread of rumors and fake news should be prevented. Effective policies should be made on the national level to improve the psychological health of vulnerable groups. Further studies should be carried out to assess the response and willingness of the healthcare workers and medical students toward the COVID-19 vaccine.
This study has some limitations. First, it was an online cross-sectional study, so we could not establish causal inferences. Second, our sample size was smaller. Third, we did not know about the pre-existing psychiatric issues of the participants. Fourth, the psychiatric diagnosis was through a self-reported questionnaire that should have been done through structured interviews and neuroimaging. Finally, there was a possibility of selection bias due to voluntary sampling through the online system using different social media platforms.
Conclusions
This study was conducted to assess the impact of the COVID-19 on the psychological health of doctors and medical students in Punjab, Pakistan. A good level of knowledge about COVID-19 was reported. They had sufficient knowledge about different perspectives of COVID-19. Female gender and younger age were the most vulnerable groups significantly associated with depression. Those who were not well aware of COVID-19 and spent more time on the news were associated with increased levels of anxiety. Special attention should be paid to the undergraduate medical students to improve their mental health affected by the pandemic. Accurate knowledge about the virus should be made available to prevent conspiracies. Targeted therapy in the form of CBT and other stress alleviating activities such as relaxation exercises should be promoted to reduce the level of anxiety and depression among doctors and medical students.
Data Sharing Statement
The data that support the findings of this study are available to the corresponding author on reasonable request.
Ethical Approval
This study was approved by the IRB committee at Pir Abdul Qadir Shah Jeelani Institute of Medical Sciences, reference number is PASQJIMS/IRB/87. The study complies with the declaration of Helsinki.
Funding
This survey did not receive any funding from public, commercial or non-profit organizations.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954. doi:10.1016/j.psychres.2020.112954
2. Modi PD, Nair G, Uppe A, et al. COVID-19 awareness among healthcare students and professionals in Mumbai metropolitan region: a questionnaire-based survey. Cureus. 2020;12(4). doi:10.7759/cureus.7514
3. Zhao D, Yao F, Wang L, et al. A comparative study on the clinical features of coronavirus 2019 (COVID-19) pneumonia with other pneumonias. Clin Infect Dis. 2020;71(15):756–761. doi:10.1093/cid/ciaa247
4. Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic.. Acta Bio-Medica: Atenei Parmensis. 2020;91(1):157. doi:10.23750/abm.v91i1.9397
5. Khan S, Gilani US, Raza SMM, Hussain T. Evaluation of general awareness among professionals regarding COVID-19: a survey based study from Pakistan; 2020.
6. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
7. World Health Organization. WHO Coronavirus (COVID-19) dashboard. Avialable from: https://covid19.who.int/table.
8. Lee Y, Lui LM, Chen-Li D, et al. Government response moderates the mental health impact of COVID-19: a systematic review and meta-analysis of depression outcomes across countries. J Affect Disord. 2021;290:364–377. doi:10.1016/j.jad.2021.04.050
9. Wang C, Tee M, Roy AE, et al. The impact of COVID-19 pandemic on physical and mental health of Asians: a study of seven middle-income countries in Asia. PLoS One. 2021;16(2):e0246824. doi:10.1371/journal.pone.0246824
10. Mukhtar F, Mukhtar N. Coronavirus (COVID-19): let’s prevent not panic. J Ayub Med Coll Abbottabad. 2020;32(1):141–144.
11. Guo J, Liao L, Wang B, et al. Psychological effects of COVID-19 on hospital staff: a national cross-sectional survey of China mainland. SSRN 3550050; 2020.
12. World Health Organization. COVID-19: vulnerable and high risk groups. Available from: https://www.who.int/westernpacific/emergencies/covid-19/information/high-risk-groups.
13. Nguyen LH, Nguyen LD, Ninh LT, et al. COVID-19 and delayed antenatal care impaired pregnant women’s quality of life and psychological well-being: what supports should be provided? Evidence from Vietnam. J Affect Disord. 2022;298:119–125. doi:10.1016/j.jad.2021.10.102
14. Hao F, Tan W, Jiang L, et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav Immun. 2020;87:100–106. doi:10.1016/j.bbi.2020.04.069
15. Ren Z, Xin Y, Ge J, et al. Psychological impact of COVID-19 on college students after school reopening: a cross-sectional study based on machine learning. Front Psychol. 2021;12:1346. doi:10.3389/fpsyg.2021.641806
16. Ren Z, Xin Y, Wang Z, Liu D, Ho RC, Ho CS. What factors are most closely associated with mood disorders in adolescents during the COVID-19 pandemic? A cross-sectional study based on 1771 adolescents in Shandong Province, China. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.728278
17. Nguyen AN, Le XTT, Ta NTK, et al. Knowledge and self-protective practices against COVID-19 among healthcare workers in Vietnam. Public Health Front. 2021;9. doi:10.3389/fpubh.2021.658107
18. Khader Y, Al Nsour M, Al-Batayneh OB, et al. Dentists’ awareness, perception, and attitude regarding COVID-19 and infection control: cross-sectional study among Jordanian dentists. JMIR Public Health Surveill. 2020;6(2):e18798. doi:10.2196/18798
19. Zhu J, Sun L, Zhang L, et al. Prevalence and influencing factors of anxiety and depression symptoms in the first-line medical staff fighting against COVID-19 in Gansu. Front Psychiatry. 2020;11. doi:10.3389/fpsyt.2020.00386
20. Maunder R, Hunter J, Vincent L, et al. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. Cmaj. 2003;168(10):1245–1251.
21. Singh J, Steele K, Singh L. Combining the best of online and face-to-face learning: hybrid and blended learning approach for COVID-19, post vaccine, & post-pandemic world. J Educ Technol Syst. 2021;50(2):140–171. doi:10.1177/00472395211047865
22. Chatterjee I, Chakraborty P. Use of information communication technology by medical educators amid COVID-19 pandemic and beyond. J Educ Technol Syst. 2021;49(3):310–324. doi:10.1177/0047239520966996
23. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
24. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
25. Mishra P, Bhadauria US, Dasar PL, et al. Knowledge, attitude and anxiety towards pandemic flu a potential bio weapon among health professionals in Indore City. Przegl Epidemiol. 2016;70(1):41–45.
26. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
27. Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, Ho RC. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci Rep. 2018;8(1):1–10. doi:10.1038/s41598-018-21243-x
28. Cao W, Fang Z, Hou G, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020;287:112934. doi:10.1016/j.psychres.2020.112934
29. Saddik B, Hussein A, Sharif-Askari FS, et al. Increased levels of anxiety among medical and non-medical university students during the COVID-19 pandemic in the United Arab Emirates. Risk Manag Healthc Policy. 2020;13:2395. doi:10.2147/RMHP.S273333
30. Baruah A, Das S, Dutta A, Das B, Sharma T, Hazarika M. Prevalence of depression among undergraduate medical students: a cross sectional study conducted at Midnapore medical college and hospital, Paschim Midnapore district WB, India. Int j Sci Res. 2019;8(12):41–45. doi:10.15373/22778179
31. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
32. Wolf MS, Serper M, Opsasnick L, et al. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the US outbreak: a cross-sectional survey. Ann Intern Med. 2020;173(2):100–109. doi:10.7326/M20-1239
33. Shaw SC. Hopelessness, helplessness and resilience: the importance of safeguarding our trainees’ mental wellbeing during the COVID-19 pandemic. Nurse Educ Pract. 2020;44:102780. doi:10.1016/j.nepr.2020.102780
34. Mak IWC, Chu CM, Pan PC, Yiu MGC, Chan VL. Long-term psychiatric morbidities among SARS survivors. Gen Hosp Psychiatry. 2009;31(4):318–326. doi:10.1016/j.genhosppsych.2009.03.001
35. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singapore. 2020;49(1):1–3.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.