")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Moderation Effects of Positive Core Belief and Social-Emotional Responsiveness on the Relationship Between Cyberbullying Victimization and Affective Symptoms
Authors Nisu S, Anuroj K , Wannaiampikul S, Pangsorn A, Chiencharoenthanakij R, Chongbanyatcharoen S
Received 24 May 2023
Accepted for publication 20 June 2023
Published 6 July 2023 Volume 2023:16 Pages 2545—2551
DOI https://doi.org/10.2147/PRBM.S420771
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Sansanee Nisu,1 Krittisak Anuroj,1 Sivaporn Wannaiampikul,2 Apichai Pangsorn,3 Romteera Chiencharoenthanakij,1 Siwat Chongbanyatcharoen1
1Department of Psychiatry, Faculty of Medicine, Srinakharinwirot University, Nakhon Nayok, Thailand; 2Department of Biochemistry, Faculty of Medicine, Srinakharinwirot University, Bangkok, Thailand; 3Department of Forensics, Faculty of Medicine, Srinakharinwirot University, Nakhon Nayok, Thailand
Correspondence: Krittisak Anuroj, Department of Psychiatry, Faculty of Medicine, Srinakharinwirot University, 62 Moo 7 Ongkharak Subdistrict, Ongkharak District, Nakhon Nayok, 26120, Thailand, Tel +6637385085 Ext. 60804, Email [email protected]
Introduction: Medical students are a vulnerable population. Exposure to cyberbullying can aggravate stress and lead to affective disorders. Features that moderate the influence of this stressor have been under-studied in Thai context.
Materials and Methods: An annual survey on the mental health and stressors of medical students from 2021 was analyzed. Measures on cyberbullying victimization, psychosocial stressors, self-reported resilience measures (“problem solving”, “positive core belief”, “social emotional responsiveness”, and “perseverance”), and other covariates were assessed for their effects on affective symptoms using linear regression. Interaction analyses were then performed.
Results: A total of 303 cyberbullied respondents were included. In a linear regression model controlled for cyberbullying victimization score, perceived psychosocial difficulties, age, and academic year, positive core belief significantly predicted lower affective symptoms, while social-emotional responsiveness showed a trend toward predicting lower affective symptoms. Trend toward negative interaction was found for positive core belief, whereas an opposite trend was found for social-emotional responsiveness. Implications in the context of medical schools are also discussed.
Discussion: Positive core belief appears to be a resilience feature toward cyberbullying victimization in the studied population. Its effects were discussed from the perspective of cognitive-behavioral therapy. In the context of medical school, the belief could be fostered by creating a safe learning environment with readily available guidance. Social-emotional responsiveness is a protective factor toward cyberbullying victimization, although its trend toward negative interaction with cyberbullying victimization implies that this feature’s protective effect declines as intensity of the bullying increases.
Conclusion: Positive core belief is a potential resilience feature of cyberbullying victimization. On the other hand, the protective effect of social-emotional responsiveness appeared to decline with greater intensity of cyberbullying.
Keywords: depression, anxiety, irritability, online bullying, medical students
Plain Language Summary
In an effort to explore whether certain personal characteristics protect medical students from mental health adversities from experiencing cyberbullying, a survey was conducted. It was found that traits related to positive beliefs about oneself, society, and the world (so-called positive core belief) reduced the effects of cyberbullying on emotional disturbances. Traits related to social-emotional responsiveness also reduced the effects of cyberbullying on emotional disturbances, although their effects waned with a greater intensity of cyberbullying. Promotion of these protective traits in the context of medical school has been discussed.
Introduction
Resilience, in psychiatric context, refers to one’s capacity to mentally adapt well under adverse psychosocial circumstances.1 Factors that conferred resilience are multidimensional and may include coping behaviors, efficacious cognitive features, personal integrity, sense of control, and social supports.2–6 Only some resilience features become active upon encountering a specific stressor, meaning that different stressors require different traits for the person to successfully adapt.4 Cyberbullying refers to the act of harassing, intimidating, or psychologically harming someone through online means.7 The situation is becoming a common adverse psychosocial experience in the current era and is a relatively understudied phenomenon in Thailand.8 Since it is known that medical students have elevated psychiatric symptoms owing to stressful learning environment, responsibility, and time constraints,9–15 any further added stresses that are amenable to intervention can be a crucial topic. Resilience features toward cyberbullying therefore warrant an exploration. Measures of overall resilience features have been associated with lower odds of being cyberbullied,16 and were also shown to moderate their effects on depression and life satisfaction.7 Studies that analyzed the features individually have found protective effects of adaptive coping strategies, social skills, social support, self-perception, and optimism.17–21 These findings are yet to be evaluated in Thai medical school context. Identifying and reinforcing intrapersonal resilience features would complement parallel efforts to reduce the occurrence of cyberaggression and minimize emotional sequelae among medical students.22
Materials and Methods
Objective
Explore the moderation effects of resilience features effects of cyberbullying victimization on affective symptoms.
Design, Participants, and Settings
This was a retrospective review of annual mental health surveillance data collected by the preclinical medical student affairs division of the authors’ faculty in January 2021. The surveillance included students’ demographic data, measures on psychosocial stressors and affective symptoms, which are elaborated in the following section. All the questionnaires were self-rated online. As the system was designed to monitor individual students and provide individualized support, the data collection was not anonymous. The data were anonymized prior to retrieval for this analysis. All medical students from academic years 1 to 3 (preclinical studies) were invited to complete the surveillance questionnaires; however, their participation was voluntary.
Measurements and Variables
Demographic data on gender, age, and academic year were collected. Participants were then asked to recall their cyberbullying victimization experience in the past month using the victimization subscale of cyber-aggression and victimization scale: Thai version. The instrument was validated in Thai adolescents, had a good internal consistency, with Cronbach’s alpha of 0.89, had the same construct as the original version, and displayed convergence with depressive symptoms.23,24 Participants rated frequencies of bullying experiences such as “I found hateful comments toward my videos online” on 5-point Likert scales, with higher score indicating more victimization experience. Participants were included in this study by rating at least 2 (“rarely”) in at least one item. The summed score from these items, which indicates the intensity of cyberbullying experience, was entered as an independent variable.
The Suanprung Stress Test—20 is a measure published by the Thai Department of Mental Health and has been made available for public use. It consists of 20 items, 6 of which inquired about the presence of psychosocial difficulties with everyday stressors (such as goal-related or financial problems), 14 of which queried affective symptoms (depression, anxiety, irritability, and associated cognitive and somatic symptoms), all of which were convergently validated with electromyography. Items were queried on a 5-point Likert scale.25 The first six items were summed and entered as an independent variable as a covariate (psychosocial stressor), and the remaining 14 were summed and entered as the dependent variable (affective symptoms).
Resilience features were assessed using items from the resilience quotient questionnaire and emotional quotient questionnaire. Both were developed by the Thai Department of Mental Health, validated in representative sample of Thai population, and made available for public use.26,27 Items were compiled based on their relevance to the reviewed concept of resilience features.7,16–20 A total of 32 items from the following categories were compiled: (1) problem solving, which queried problem-focused coping and attitudes toward problems; (2) positive core belief, which contained statements related to worldview, hope, and optimism; (3) social-emotional responsiveness, which queried participants’ perceived emotional sensitivity and response in social situations; and (4) perseverance, which queried grids and attitudes toward hardships. These items were phrased such as “I feel strengthened as I successfully solved problems.” The participants rated their agreement on a 4-point Likert scale. The sums of the scores from each category were entered into the statistical analysis.
Statistical Analysis
Cyberbullying victimization, psychosocial difficulties, resilience features, and demographic data were visualized in scatterplots for potential linear relationships with affective symptoms and were subjected to simple linear regression. Those with potential associations with affective symptoms were entered into a multivariable linear regression; results from the saturated and reduced models are presented. Resilience factors were then examined for their interaction with cyberbullying victimization using another model. All final regression models were tested for independence of errors, normal distribution of residuals, homoscedasticity, and linearity. No imputation or substitution was performed as there were no missing data. Statistical analyses were performed using SPSS version 27 (ICN 793700).
A post-hoc analysis of the achieved statistical power was performed using G*Power version 3.1. With an alpha of 0.05, a sample size of 303 participants, and eight predictors (as in the final interaction model), a power value approaching 1.0 was achieved for variables with medium effect size.
Results
Of the 333 students who participated in the survey, 303 reported having experienced cyberbullying and were included. Their characteristics are presented in Table 1. The proportions of subjects who reported perceived difficulties (rated higher than “1: none” or “2: minimally”) in each item are presented for illustrative purposes. The dependent affective symptoms assumed a right-skewed distribution.
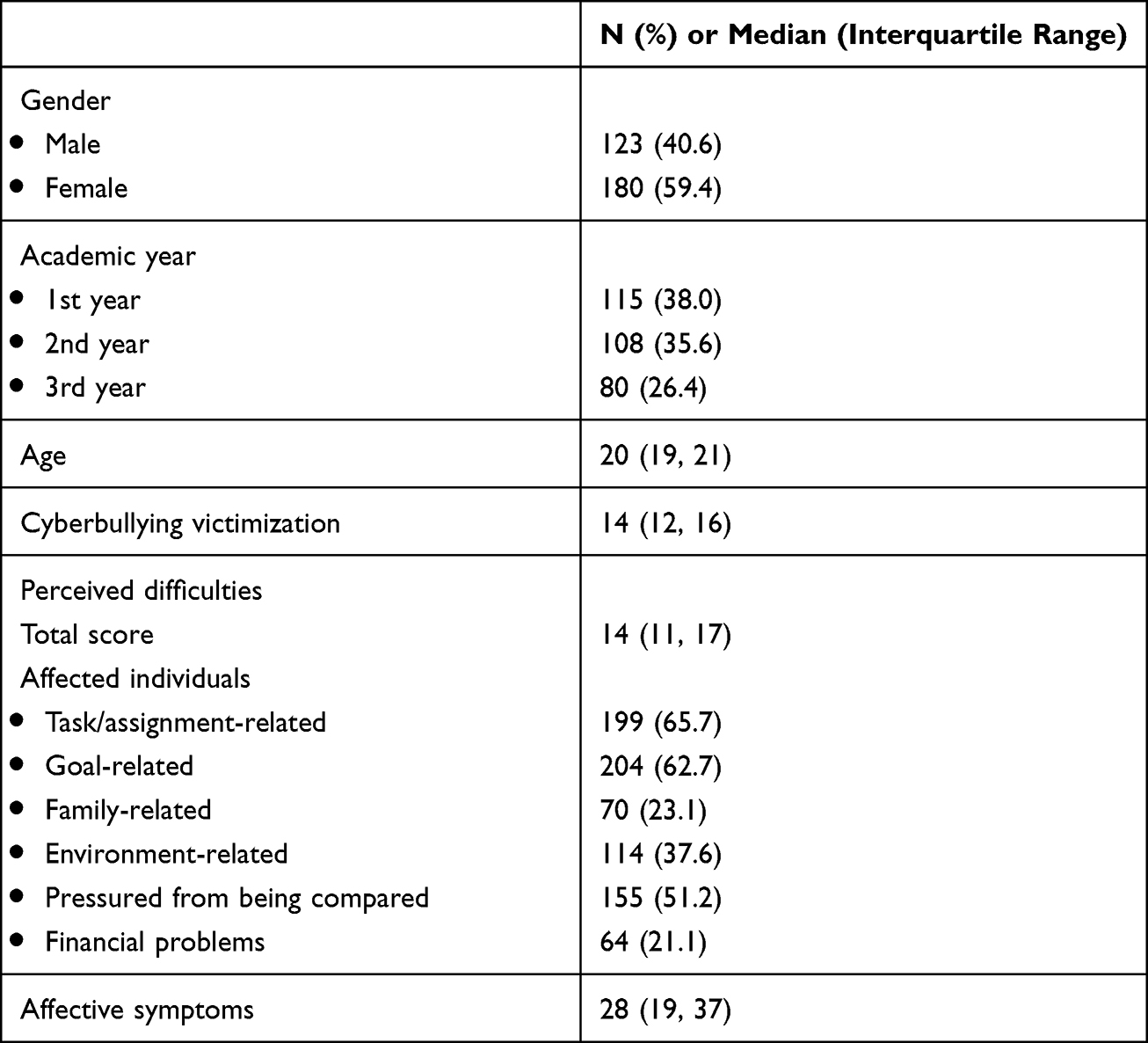 |
Table 1 Demographic Data of Included Participants |
Scatterplots and subsequent simple regression revealed a potential linear relationship between affective symptoms and age (B = 0.60, p = 0.15), academic year (B = 9.50, p < 0.01 for year 2, and B = 3.02, p-value = 0.11 for year 3), psychosocial difficulties (B = 1.7, p < 0.01), and cyberbullying victimization (B = 0.70, p < 0.01). These variables were examined in standardized residual plots, all of which met the assumptions of linearity and homogeneity of variance. Multivariable linear regression was performed; the reduced model was adjusted for academic year, psychosocial difficulties, and cyberbullying victimization. In the main effect models (Table 2, upper section), positive core belief significantly predicted lower affective symptoms, whereas social-emotional responsiveness had a trend toward predicting lower affective symptoms. Problem solving and perseverance failed to predict affective symptoms.
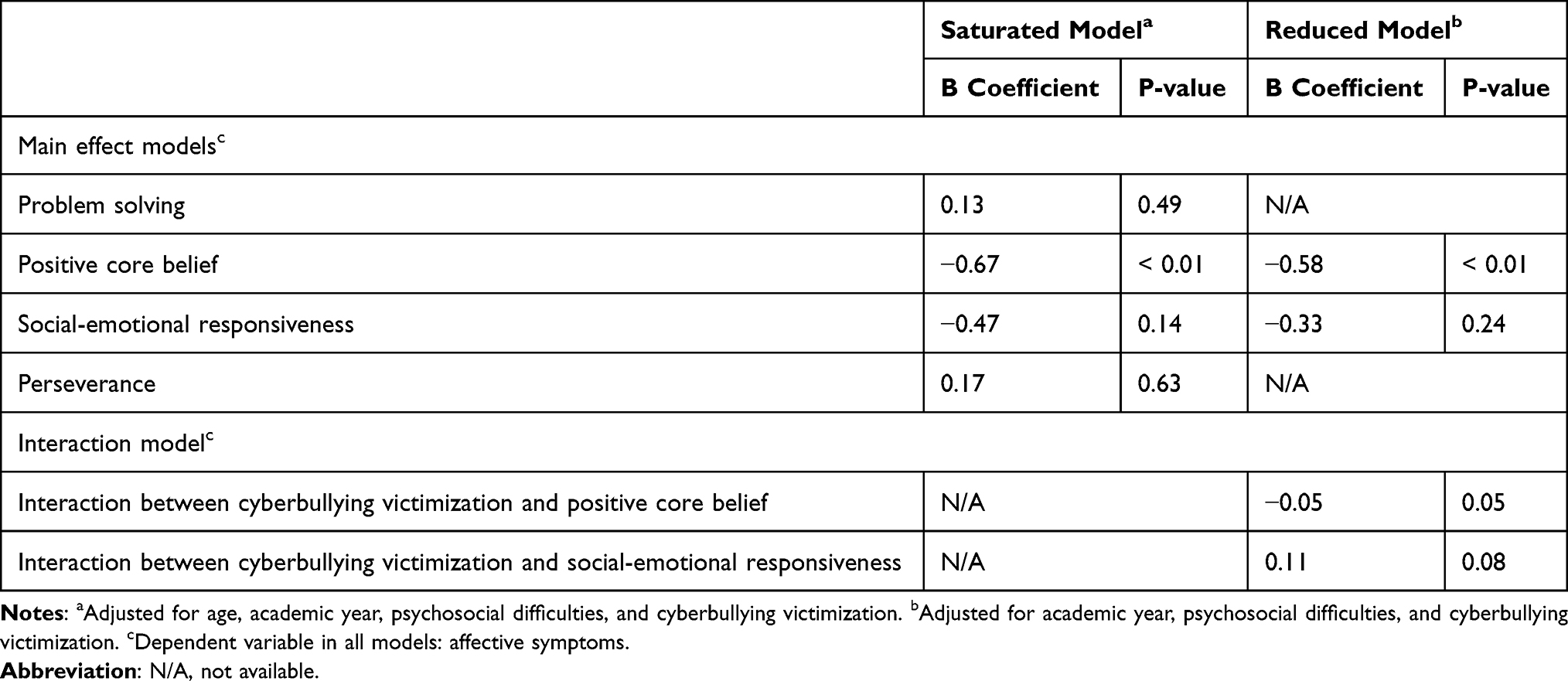 |
Table 2 Results from Linear Regression Examining the Effects of Resilience Features on Affective Symptoms |
Subsequent analysis of the interaction between the two categories of resilience features found a trend toward negative interaction for positive core belief and an opposite trend for social-emotional responsiveness. The coefficients are listed in the lower part of Table 2.
Discussion
This study is among the first to investigate the issue of cyberbullying and related resilience factors in the context of medical students in Thailand. The findings confirmed clinically observed presence of cyberbullying problems in Thai medical students. The noted effect of cyberbullying victimization on affective symptoms adds to the array of factors predicting mental health problems in this vulnerable population,9–15,28 and is consistent with previous observations of cyberbullying’s negative impacts on mental health.29–33 As of the present, literatures on predictors of Thai medical student’s mental health problems are still limited. Dated measures of psychosocial difficulties (including one employed to control for covariate: the Suanprung Stress Test) do not inquire into problems encountered online. Unless this study explicitly tackles the issue, cyberbullying victimization can be an overlooked covariate. As the present study suggests that cyberbullying significantly predicts affective symptoms, future studies, not limited to those in medical students, should incorporate these online difficulties into the array of control variables. An updated general questionnaire for psychosocial difficulties may be required to ensure consistency and ease of interpretation in Thai mental health research. For future studies on cyberbullying among Thai medical students, it would be worthwhile to investigate the coping patterns utilized in this particular population. Although technologically adept as a generation, some medical students can still be befuddled by cyberbullying. In particular, when emotion get the better of rational judgment, they may be barred from utilizing effective coping strategies (eg, referring to adults when problems get out of hand) or may be inclined to choose self-destructive strategies (such as substance misuse, escapism, or avoidant strategies).24,34 Coping strategies are therefore potential targets for specific interventions. Additionally, addressing resilience features would help buffer the impact on mental health.
As observed in the interaction model, positive core belief predicted lower affective symptoms. It also displayed a trend toward negative interaction with cyberbullying victimization, meaning that the effects of cyberbullying victimization on affective symptoms decreased as the rating of positive core belief increased. These results indicate that positive core belief is a resilience feature to cyberbullying victimization. Viewed from cognitive-behavioral therapy’s perspective, core belief is congregated from past experience that subsequently serve from the shadows to influence the person’s view on himself, others, and the world through the translation into intermediate beliefs and automatic thoughts.35 In a way, it affects how the victims view the problem and their ensuant actions. For example, viewing being bullied as an occasional occurrence in social life sounds less disheartening than viewing it as a recurring misfortune, a menacing threat, or a confirmation that the world is a cruel place. Positive core beliefs could sound something like “I am capable”, “the world is fine”, “society is not that threatening.” These beliefs can be translated to relatively functional intermediate beliefs (rules and assumptions), such as “problems are meant to be dealt with” or “being bullied cannot change who I am”. With these attitudes, the hardship of bullying can become more bearable. Fostering positive core belief among medical students could be protective in various stressful situations not limited to cyberbullying. However, even with the most intensive individual therapy, positive core belief cannot be developed in one or two sessions. Different backgrounds also mean different starting points for different students. An emerging approach is to gradually evolve the medical school into a safe and mentally secure learning environment, a difficult feat owing to the complex organizational structure and requirements of compliance from a broad range of staff.36,37 Curbing the mental trauma experienced from medical school is a good start, as development of negative beliefs can be deterred. Creating an organizational culture of mentally sound medical instructors would promote social learning (through imitation, or adoption of role models) of healthy behaviors and belief. Buffers such as readily available guidance systems and mental health support may also play a role; for example, by conferring experience that someone is there to help, that solutions can be obtained from consultation, or that a safe place still exists despite the threat faced. Aside from being able to view problems in a more positive light, such situations will promote help-seeking behaviors should students feel that any problem, including bullying, is beyond their control. However, this approach requires long and dedicated efforts to bear fruit. This effect may only be evident in retrospect, such as through a trend analysis.
Regarding social-emotional responsiveness, although the main effect pointed toward an overall protective trend against affective symptoms, the interaction analysis indicated a positive trend, meaning that the effect of cyberbullying victimization increased as the rating on this feature increased (which sounds rather confusing). Explaining this from another perspective provides a clearer statement: the protective effect of this feature declined with increasing intensity of bullying. In general, this feature helps to establish working relationships with others, which adds to the social support inventory of the person. This feature may also allow for an empathic understanding of others and the subsequent ability to tolerate minor or unintended offenses in favor of maintaining relationships, thus explaining its overall protective effect. On the other hand, the inherent emotional sensitivity within this feature can be a vulnerability when the intensity of bullying goes beyond mild, becoming too difficult to overlook or resolve mentally with empathy.38–40 The rising use of social media could subsequently affect social sensitivity and subsequent affective disturbance in this generation of students.41,42 The increasing intensity of cyberbullying also challenges a person’s perception of the self as socially capable, creating cognitive dissonance and confusion. A challenging task for medical schools is to broaden their students’ repertoire of activities so that they are less affected by social stress, particularly due to excessive media exposure, considering the limited free time available in the context. Nevertheless, upon experiencing cyberbullying and struggling to socially adapt or equilibrating one’s scale of social sensitivity, the previously discussed systems of guidance and mental health support would also aid medical students in this regard. When guidance medical instructors or advisors are consulted by their students on the problems of bullying, they could begin by empathically listening to the problem, looking to impart healthy coping strategies, reinforcing positive core beliefs and social skills (including emotional responsiveness, where appropriate), and be ready to refer students with more severe symptoms to mental health services.
Limitations
Measures of resilience relied on self-reports of perceived aspects or behavioral tendency of oneself, which is subject to recall bias, norm (or politically correct) conformity, and even distorted self-perception in participants with poor personality functioning. Non-anonymity at the time of collection further added the risk of norm conformity (or barred nonconformers from participating altogether). Longitudinal data on affective symptoms (and subsequently, relationships with resilience features) were lacking. Participants drawn from a single, limited environment (medical school) prompted caution in generalizability. The sample size and power were sufficient only for variables with medium or large effect sizes.
Conclusion
In the present study of 303 medical students who had experienced cyberbullying, self-reported measures of positive core belief and social-emotional responsiveness were potentially protective against affective symptoms. Trends toward moderation by these two features in the relationship between cyberbullying victimization and affective symptoms were also found. Clinical and organizational implications are discussed.
Ethics Approval and Informed Consent
The study protocol was approved by the Srinakharinwirot University Ethical Committee for Human Research (identification number SWUEC/X-022/2564). The requirement for written informed consent was waived because the study reviewed anonymized survey data.
Funding
This study was supported by a research grant from the Faculty of Medicine, Srinakharinwirot University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farber E, Egeland B. Invulnerability among abused and neglected children. In: Anthony E, Cohler B, editors. The Invulnerable Child. Guilford Press; 1987:253–288.
2. Cowen EL, Work WC. Resilient children, psychological wellness, and primary prevention. Am J Community Psychol. 1988;16(4):591–607. doi:10.1007/BF00922773
3. Cowen EL, Wyman PA, Work WC. Resilience in highly stressed urban children: concepts and findings. Bull N Y Acad Med. 1996;73(2):267–284.
4. Rutter M. Resilience: concepts, findings, and clinical implications. In: Thapar A, editor. Rutter’s Child and Adolescent Psychiatry.
5. Shean M. Current theories relating to resilience and young people: a literature review. Victorian Health Promotion Foundation; 2015. Available from: https://evidenceforlearning.org.au/assets/Grant-Round-II-Resilience/Current-theories-relating-to-resilience-and-young-people.pdf.
6. Auttama N, Seangpraw K, Ong-Artborirak P, Tonchoy P. Factors associated with self-esteem, resilience, mental health, and psychological self-care among university students in northern Thailand. JMDH. 2021;14:1213–1221. doi:10.2147/JMDH.S308076
7. Santos D, Mateos-Pérez E, Cantero M, Gámez-Guadix M. Cyberbullying in adolescents: resilience as a protective factor of mental health outcomes. Cyberpsychol Behav Soc Netw. 2021;24(6):414–420. doi:10.1089/cyber.2020.0337
8. Weerarit L. Cyberbullying among secondary school students: prevalence, problem-solving and risk behaviors. NEU Acad Res J. 2021;11(1):275–289.
9. Dahlin M, Joneborg N, Runeson B. Stress and depression among medical students: a cross-sectional study. Med Educ. 2005;39(6):594–604. doi:10.1111/j.1365-2929.2005.02176.x
10. Goebert D, Thompson D, Takeshita J, et al. Depressive symptoms in medical students and residents: a multischool study. Acad Med. 2009;84(2):236–241. doi:10.1097/ACM.0b013e31819391bb
11. Sidana S, Kishore J, Ghosh V, Gulati D, Jiloha R, Anand T. Prevalence of depression in students of a medical college in New Delhi: a cross-sectional study. Australas Med J. 2012;5(5):247–250. doi:10.4066/AMJ.2012.750
12. Limsricharoen K, Handee N, Chulakdabba S. Prevalence and associated factors of depression in second to sixth years medical students, faculty of medicine in Thailand. J Psychiatr Assoc Thailand. 2014;59(1):29–40.
13. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214–2236. doi:10.1001/jama.2016.17324
14. Mao Y, Zhang N, Liu J, Zhu B, He R, Wang X. A systematic review of depression and anxiety in medical students in China. BMC Med Educ. 2019;19(1):327. doi:10.1186/s12909-019-1744-2
15. Anuroj K. Cross-sectional study of vitamin D deficiency in medical students during COVID-19 pandemic: high prevalence but without association with depression. East Asian Arch Psychiatry. 2022;32:51–56. doi:10.12809/eaap2209
16. Hinduja S, Patchin JW. Cultivating youth resilience to prevent bullying and cyberbullying victimization. Child Abuse Negl. 2017;73:51–62. doi:10.1016/j.chiabu.2017.09.010
17. Ttofi MM, Farrington DP. Risk and protective factors, longitudinal research, and bullying prevention. New Dir Youth Dev. 2012;2012(133):85–98. doi:10.1002/yd.20009
18. Worsley JD, McIntyre JC, Corcoran R. Cyberbullying victimisation and mental distress: testing the moderating role of attachment security, social support, and coping styles. Emot Behav Diffic. 2019;24(1):20–35. doi:10.1080/13632752.2018.1530497
19. Brailovskaia J, Teismann T, Margraf J. Cyberbullying, positive mental health and suicide ideation/behavior. Psychiatry Res. 2018;267:240–242. doi:10.1016/j.psychres.2018.05.074
20. Jaureguizar J, Garaigordobil M, Bernaras E. Self-concept, social skills, and resilience as moderators of the relationship between stress and childhood depression. School Ment Health. 2018;10(4):488–499. doi:10.1007/s12310-018-9268-1
21. Rodelli M, De Bourdeaudhuij I, Dumon E, Portzky G, DeSmet A. Which healthy lifestyle factors are associated with a lower risk of suicidal ideation among adolescents faced with cyberbullying? Prev Med. 2018;113:32–40. doi:10.1016/j.ypmed.2018.05.002
22. Yosep I, Hikmat R, Mardhiyah A. Nursing intervention for preventing cyberbullying and reducing its negative impact on students: a scoping review. JMDH. 2023;16:261–273. doi:10.2147/JMDH.S400779
23. Anuroj K, Pittayaratstian N. Validity and reliability of cyber-aggression perpetration and victimization scale: Thai version. J Psychiatr Assoc Thailand. 2019;64(1):45–60.
24. Anuroj K. Effects of cyberbullying and coping strategies on depression. J Med Assoc Thai. 2022;105(Suppl.1):S58–67. doi:10.35755/jmedassocthai.2022.S01.00024
25. Mahatnirunkul S, Poompaisarnchai W, Tapunya P. Development of suanprung stress test. J Suan Psych Hospital. 1997;13(3):1–20.
26. Inthasit S, Julkeeree S. RQ: Resilience Quotient.
27. Thai Department of Mental Health. The Development of Thai Emotional Intelligence Screening Test for Age 12 to 60. Division of mental health promotion; 2001.
28. Auchayasawat S. Prevalence and factor affecting depression in clinical medical students from a medical school in Northeastern Thailand. Srinagarind Med J. 2021;36(2):200–208.
29. Kowalski RM, Giumetti GW, Schroeder AN, Lattanner MR. Bullying in the digital age: a critical review and meta-analysis of cyberbullying research among youth. Psychol Bull. 2014;140(4):1073–1137. doi:10.1037/a0035618
30. Hu Y, Bai Y, Pan Y, Li S. Cyberbullying victimization and depression among adolescents: a meta-analysis. Psychiatry Res. 2021;305:114198. doi:10.1016/j.psychres.2021.114198
31. Tran HGN, Thai TT, Dang NTT, Vo DK, Duong MHT. Cyber-victimization and its effect on depression in adolescents: a systematic review and meta-analysis. Trauma Violence Abuse. 2021;23:152483802110505. doi:10.1177/15248380211050597
32. Molero MM, Martos Á, Barragán AB, Pérez-Fuentes MC, Gázquez JJ. Anxiety and depression from cybervictimization in adolescents: a metaanalysis and meta-regression study. Eur J Psychol Appl Leg Context. 2022;14(1):42–50. doi:10.5093/ejpalc2022a5
33. Dorol-Beauroy-Eustache O, Mishara BL. Systematic review of risk and protective factors for suicidal and self-harm behaviors among children and adolescents involved with cyberbullying. Prev Med. 2021;152:106684. doi:10.1016/j.ypmed.2021.106684
34. Siah PC, Tee XY, Tan JTA, et al. Cybervictimization and depression among adolescents: coping strategies as mediators. Int J Environ Res Public Health. 2022;19(7):3903. doi:10.3390/ijerph19073903
35. Beck JS. Cognitive Therapy: Basics and Beyond. Guilford Press; 1995.
36. Rigaudy M, Elmqvist K, Vink J. Creating a no-blame culture through medical education: a UK perspective. JMDH. 2016;9:345–346. doi:10.2147/JMDH.S111813
37. Leman MA, Claramita M, Rahayu GR. Defining a “healthy role-model” for medical schools: learning components that count. JMDH. 2020;13:1325–1335. doi:10.2147/JMDH.S279574
38. Murray L, Halligan SL, Adams G, Patterson P, Goodyer IM. Socioemotional development in adolescents at risk for depression: the role of maternal depression and attachment style. Develop Psychopathol. 2006;18(02). doi:10.1017/S0954579406060263
39. Sun J, Zhang X, Wang Y, Wang J, Li J, Cao F. The associations of interpersonal sensitivity with mental distress and trait aggression in early adulthood: a prospective cohort study. J Affect Disord. 2020;272:50–57. doi:10.1016/j.jad.2020.03.161
40. Jiang Y, Ren Y, Liu T, You J. Rejection sensitivity and adolescent non-suicidal self-injury: mediation through depressive symptoms and moderation by fear of self-compassion. Psychol Psychother. 2021;94(2):481–496. doi:10.1111/papt.12293
41. Weinstein AM. Problematic social networking site use-effects on mental health and the brain. Front Psychiatry. 2022;13:1106004. doi:10.3389/fpsyt.2022.1106004
42. Rajeshwari S, Meenakshi S. The age of doom scrolling - Social media’s attractive addiction. J Educ Health Promot. 2023;12:21. doi:10.4103/jehp.jehp_838_22
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.