Back to Journals » Journal of Pain Research » Volume 19
Prevalence and Nomogram-Based Prediction Model of Neuropathic Pain After Knee Arthroplasty
Authors Xin Y, Wang C, Li J ![]() , Fang X, Huang Z, Bai G, Li W, Zhang W
, Fang X, Huang Z, Bai G, Li W, Zhang W ![]() , Zhang C
, Zhang C ![]()
Received 4 September 2025
Accepted for publication 18 January 2026
Published 29 January 2026 Volume 2026:19 565227
DOI https://doi.org/10.2147/JPR.S565227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Yishan Xin,1– 4 Chenwei Wang,5 Juncheng Li,1– 4 Xinyu Fang,1– 4 Zida Huang,1– 4 Guochang Bai,1– 4 Wenbo Li,1– 4 Wenming Zhang,1– 4 Chaofan Zhang1– 4
1Department of Orthopaedic Surgery, the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 2Department of Orthopaedic Surgery, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350212, People’s Republic of China; 3Fujian Provincial Institute of Orthopedics, the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 4Fujian Orthopaedic Bone and Joint Disease and Sports Rehabilitation Clinical Medical Research Center, Fuzhou, 350005, People’s Republic of China; 5School of Basic Medical Sciences, Fujian Medical University, Fuzhou, 350122, People’s Republic of China
Correspondence: Chaofan Zhang, Department of Orthopaedic Surgery, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, 350001, People’s Republic of China, Tel +860591-87982113, Email [email protected] Wenming Zhang, Department of Orthopaedic Surgery, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, 350001, People’s Republic of China, Tel +860591-87982113, Email [email protected]
Background: Neuropathic pain (NP) following knee arthroplasty significantly impairs patient quality of life, yet current research lacks objective predictors and predictive models. This study aimed to identify postoperative NP associated factors and develop a nomogram prediction model.
Methods: We enrolled 128 patients undergoing primary unilateral knee arthroplasty (February 2023–August 2024) with 6– 24 month follow-up. NP was assessed using PainDETECT (PDQ) and DN4 scales; pain-related quality of life was evaluated via the Oxford Knee Score pain subscale (OKS-PS). Clinical records were systematically reviewed. Variables were screened using univariate logistic regression, optimized via LASSO regression, and incorporated into a multivariate logistic regression nomogram, followed by validation analyses.
Results: NP incidence was 14.06% (18/128). OKS-PS confirmed a significant association between postoperative NP and reduced quality of life. The nomogram identified female sex, decreased preoperative range of motion (ROM), greater preoperative mechanical axis angles (pMAA) difference, and higher postoperative C-Reactive protein (CRP) as factors significantly associated with NP. Bootstrap validation yielded an AUC of 0.764 (95% CI: 0.760– 0.770), sensitivity 0.707 (0.694– 0.718), and specificity 0.737 (0.724– 0.747). 10-fold cross-validation showed comparable results: AUC 0.813 (0.721– 0.906), sensitivity 0.778 (0.5– 0.938), specificity 0.764 (0.676– 0.833). Calibration curves indicated agreement (MAE=0.037), and DCA demonstrated strong clinical utility across threshold probabilities of 0.003– 0.391.
Conclusion: Postoperative NP was significantly associated with female sex, reduced preoperative ROM, increased pMAA difference, and elevated postoperative CRP. The validated nomogram showed good predictive performance, establishing a reliable tool for early identification and risk assessment of post-arthroplasty NP.
Keywords: neuropathic pain, knee arthroplasty, associated factors, nomogram, prevalence
Introduction
Knee arthroplasty, the standard surgical treatment for end-stage osteoarthritis, significantly alleviates pain, restores function, and improves quality of life with favorable long-term outcomes.1 Nevertheless, chronic postoperative pain persists as a challenging clinical complication despite advances in surgical techniques. Most affected patients exhibit neurological symptoms such as sensory abnormalities,2,3 suggesting potential development of neuropathic pain (NP).
Studies report NP incidence in 6–15% of postoperative patients,4 with prevalence soaring to nearly 50% among those experiencing persistent pain.3,5 This rate significantly exceeds those of well-documented complications like deep vein thrombosis and surgical site infection.6 NP further demonstrates notable comorbidities with anxiety and depression,5,7 while greater NP severity correlates with more profound quality-of-life impairment.8–10
NP is defined as pain resulting from a lesion or disease of the somatosensory nervous system.11,12 Patients typically present with diffuse, poorly localized pain accompanied by characteristic symptoms including numbness, burning sensations, tingling/pricking, and electric shock-like sensations.13 A recent longitudinal study revealed complex evolutionary patterns of NP in patients with chronic postsurgical pain. Over the 15-month postoperative follow-up period, data showed that 26% of patients experienced improvement, while 56% maintained persistent NP symptoms. The remaining 18% exhibited unstable trajectories: 9% with fluctuating symptoms and 9% with new-onset NP.3
The mechanisms underlying NP following knee arthroplasty remain incompletely understood. Surgical trauma to peripheral nerves represents one potential etiology.14 Prior studies correlate previous knee surgery with NP-like symptoms in severe osteoarthritis, suggesting surgically-induced nerve injury may contribute to NP pathogenesis.15 Specifically, the procedure risks injury to cutaneous nerves critical for knee sensory innervation: the medial femoral cutaneous nerve (MFCN), intermediate femoral cutaneous nerve (IFCN), and infrapatellar branch of the saphenous nerve (IPBSN).14,16 Other studies have demonstrated postoperative differences in pain sensitivity within the MFCN and IFCN innervation zones,2 while nerve blocks targeting these nerves have shown efficacy in alleviating established neuropathic pain,14 further supporting nerve injury as a potential contributor to NP. Alternatively, inflammatory mediators serve as established biomarkers in neuropathic conditions (eg, polyneuropathy, postherpetic neuralgia)17 and osteoarthritis.18 yet their role in post-arthroplasty NP lacks clinical validation,19,20 warranting further investigation.
Recent studies have increasingly focused on identifying risk factors post-knee arthroplasty. An analysis of 14 prospective/retrospective studies indicates that postoperative acute pain severity, emotional state, and cognitive function predict NP development.21 Given the potential link between nerve injury and NP development, biomechanical factors, younger age/female sex, and lower tourniquet pressures may also confer NP risk despite limited direct evidence.22,23 Notably, unicompartmental knee arthroplasty (UKA) may reduce NP incidence relative to total knee arthroplasty (TKA) due to diminished soft tissue disruption and inflammatory response.24 The documented fluctuation in NP symptomatology further underscores postoperative time as a critical clinical variable.3 Pharmacologically, gabapentinoids alleviate symptoms in 30–40% of NP patients via calcium channel modulation,25 implying potential dysregulation of calcium signaling in NP pathogenesis.
Although existing studies have identified various factors, a persistent gap remains in objective and reliable predictive indicators, limiting clinical translation of current evidence. To bridge this gap, we retrospectively reviewed patients who underwent knee arthroplasty at our institution to determine NP occurrence and identify potential predictive factors. Based on these findings, we developed and validated a personalized risk prediction model for neuropathic pain following knee arthroplasty.
Materials and Methods
Study Design and Population Follow-Up
This study received ethical approval from our institutional review board (Approval No.: MRCTA, ECFAH of FMU [2023]308), with written informed consent obtained from all participants. This study included patients who underwent primary knee arthroplasty at the First Affiliated Hospital of Fujian Medical University between February 2023 and August 2024. Based on evidence indicating pain stabilization by 6 months postoperatively,3,26 the inclusion criteria comprised: (1) age ≥18 years; (2) UKA or TKA for osteoarthritis; (3) unilateral primary procedure with 6-months to 2-years postoperative time. Exclusion criteria included: (1) lost to follow-up or impaired communication capacity; (2) incomplete laboratory/clinical documentation; (3) postoperative infection or revision surgery.
Patients were routinely followed up at 1, 3, 6, 12 and 24 months to evaluate surgical outcomes. To assess the current pain status of patients, the follow-up was conducted in March 2025 and completed within the same month. Additional contacts served as necessary measures for instances of loss to follow-up or inadequate communication (Figure 1).
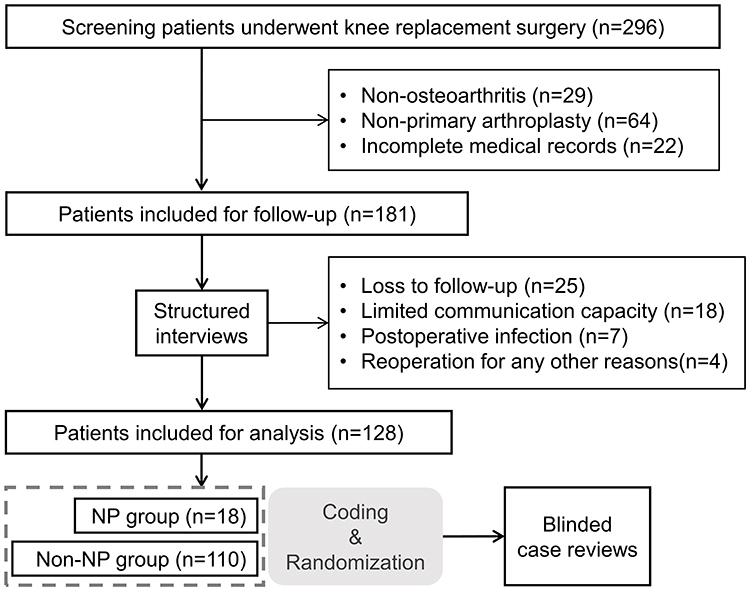 |
Figure 1 The flowchart of patient inclusion and follow-up. |
The follow-up protocol was structured around a three-part questionnaire (Supplementary questionnaire). The first part collected basic patient information including name, age. The classification of employment status followed the methodology applied by Wang et al.27 The second part assessed pain using the Oxford Knee Score pain subscale (OKS-PS), with validated scores ≤14 indicating pain significantly impacting quality of life.28,29 The third part incorporated two neuropathic pain screening tools - PainDETECT questionnaire (PDQ) and DN4,30,31 both cross-culturally validated for use in Chinese populations32,33 - to evaluate neuropathic pain prevalence and characteristics. To enhance the specificity of NP identification, We applied combined diagnostic criteria (PDQ≥11 and DN4≥3) to identify neuropathic pain cases.3,34
Clinical Characteristics and Examination Results
For patients who completed the follow-up, researchers blinded to the follow-up outcomes, retrospectively collected demographic characteristics and clinical data from the electronic medical record system, including clinical symptoms, physical signs, laboratory results, and imaging findings (Figure 1). Based on evidence demonstrating increased postoperative pain following staged bilateral TKA within 6 months,35,36 we specifically reviewed whether patients underwent contralateral knee arthroplasty within this 6-month postoperative period. Radiographic measurements of preoperative mechanical axis angles (pMAA) were performed using preoperative full-length lower limb radiographs,37 with positive values assigned to varus alignment and negative values to valgus alignment. The centers of the hip, knee (intercondylar notch), and ankle were sequentially marked and connected; the angle formed by these lines represents the pMMA. To isolate the effect of deformity magnitude independent of direction (varus/valgus), we defined pMAA difference as ABS [ABS(Right pMAA)-ABS(Left pMAA)]. Data with missing rates exceeding 5% were excluded from subsequent analyses. Postoperative inflammatory and nutritional markers were collected as part of routine testing to reflect surgical inflammation.
Statistical Analysis
All statistical analyses were performed using SPSS 29.0 and R software version 4.4.2. Spearman’s nonparametric correlation test was employed for correlation analysis of survey results. For continuous variables in clinical data: normally distributed data were presented as mean ± standard deviation (χ̅±S) and compared using independent samples t-tests; non-normally distributed data were expressed as median [P25, P75] and analyzed with rank-sum tests. Categorical data were described as frequencies (percentages) and compared using chi-square tests or Fisher’s exact probability test when chi-square assumptions were not met. A p-value < 0.05 was considered statistically significant.
This study developed the prediction model through a multi-stage feature selection and model optimization strategy with the following procedures. Stage 1: Univariate logistic regression was used for initial screening of potential predictors (significance level α=0.10). Stage 2: To prevent overfitting and ensure model robustness and interpretability, LASSO regression was applied to the prescreened variables. The optimal regularization parameter λ was determined via 10-fold cross-validation. Feature subsets were selected according to the one standard error rule (1-SE rule), favoring sparser models to enhance stability. Stage 3: Multivariate logistic regression analysis was performed on LASSO-selected variables. Final predictors were identified through bidirectional stepwise regression (entry/removal criteria: P<0.05 and P>0.10, respectively). A nomogram prediction model was developed using the finalized variables. Internal validation was conducted via the bootstrap resampling method (1000 iterations), suitable for small samples: (1) ROC curve analysis was conducted to calculate discrimination metrics including AUC, sensitivity and specificity; (2) calibration curves were plotted with Hosmer-Lemeshow test to evaluate model goodness-of-fit; (3) decision curve analysis (DCA) was performed to quantify net benefit across 0–100% threshold probabilities. To further validate model robustness, 10-fold cross-validation was implemented with corresponding ROC curves generated. The study employed stratified sampling to ensure that each fold contained NP cases. All statistical analyses were performed using R software (v4.4.2) with the packages boot, caret, glmnet, rms, ggplot2, pROC and ggDCA.
Results
Patient Characteristics and Follow-Up
This retrospective study analyzed 296 surgical records from February 2023 to August 2024. Following the exclusion of 115 cases not meeting inclusion criteria, follow-up assessments were performed on the remaining patients. Validated data from 128 patients were obtained through online questionnaires (Figure 1), resulting in a final response rate of 70.7% (128/181). This rate is consistent with those reported in prior literature.38 Reliability analysis indicated adequate internal consistency, with Cronbach’s alpha coefficients of 0.840 (Part 2) and 0.798 (Part 3) for the questionnaire, supporting the reliability of follow-up outcomes.
The prevalence of NP following knee arthroplasty was 14.06% (18/128). Follow-up assessments revealed an inverse relationship between NP severity and quality of life, as measured by declining OKS-PS with increasing scores on both the PDQ and DN4 scales. Notably, PDQ scores demonstrated a stronger negative correlation with OKS-PS reduction than DN4 scores (Figure 2A and B).
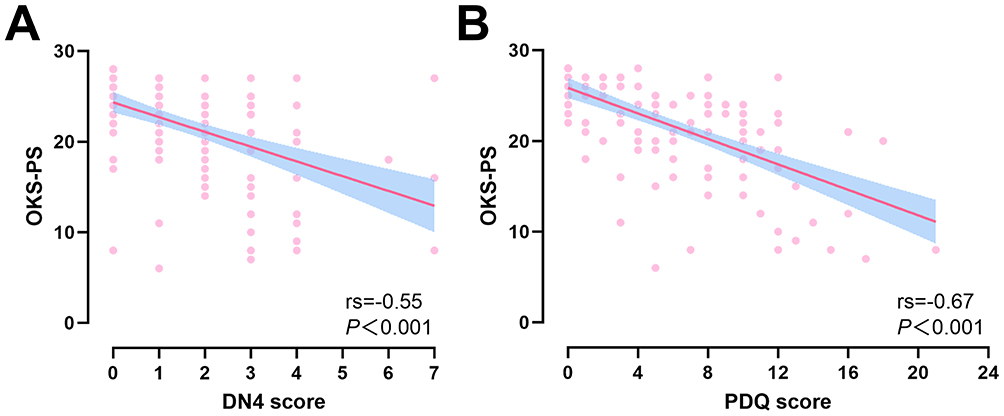 |
Figure 2 Correlation analysis of NP scores with OKS-PS. (A) The association between DN4 score and OKS-PS, with a negative correlation (rs=−0.55, p<0.001). (B) The association between PDQ score and OKS-PS, with a negative correlation (rs=−0.67, p<0.001). Abbreviations: OKS-PS, Oxford Knee Score-Pain Subscale; DN4, Douleur Neuropathique 4; PDQ, PainDETECT Questionnaire. |
Through medical record review, no statistically significant difference was observed between the two groups in surgical procedure selection (TKA vs UKA). Regarding preoperative characteristics, the NP group demonstrated significantly smaller preoperative range of motion (ROM) (p = 0.003), higher pMAA on the surgical side (p = 0.029), pMAA [abs.] (p = 0.045), and pMAA difference (p = 0.008). No significant differences were identified in age, gender, employment status, surgical side, symptom duration, or BMI (Table 1).
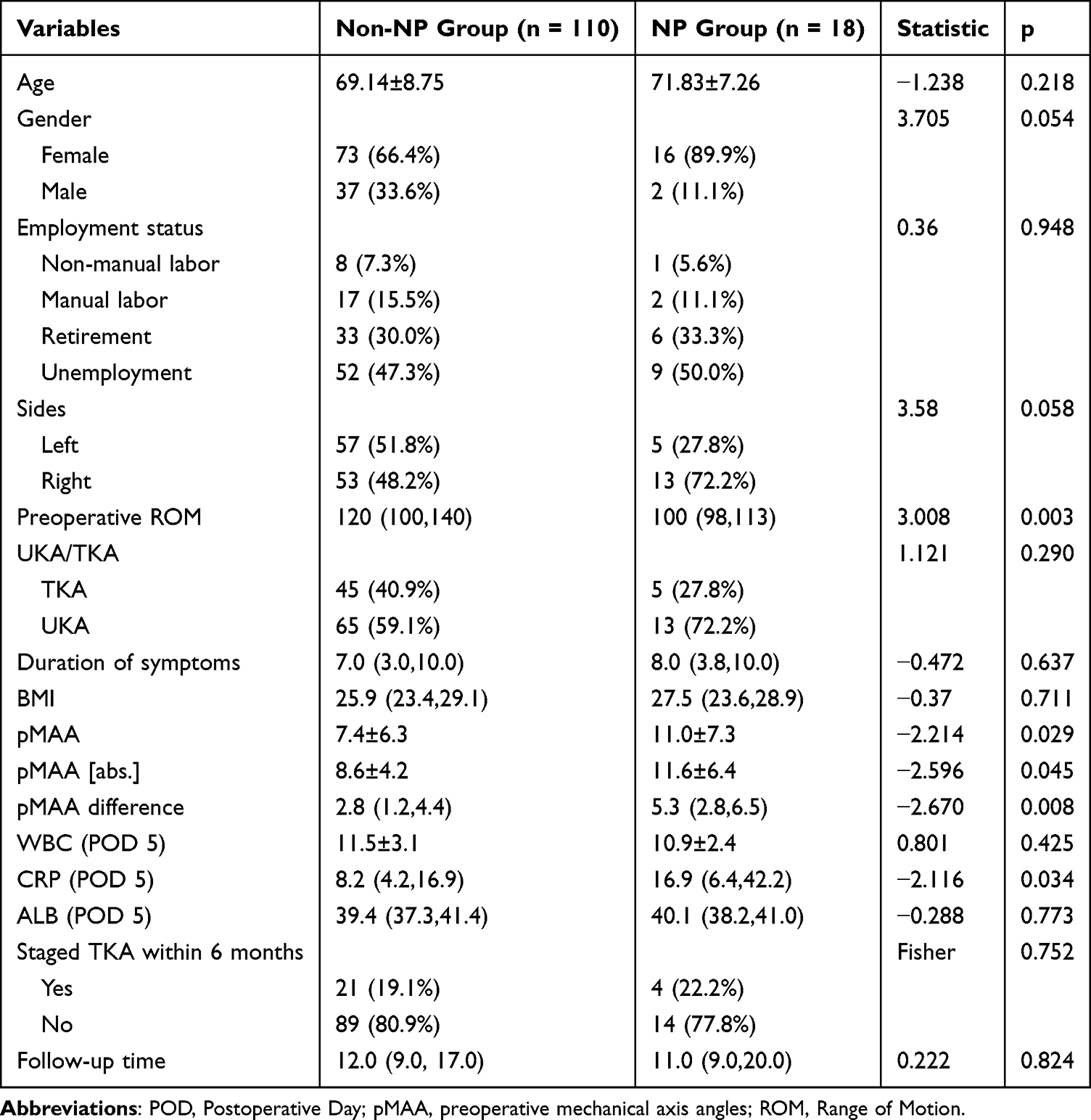 |
Table 1 Clinical Characteristics of Patients [n (%) or Mean±SD or Medians (IQRs)] |
Analysis of postoperative inflammatory and nutritional markers revealed that the NP cohort demonstrated elevated postoperative C-Reactive protein (CRP) (p = 0.034). In contrast, no significant intergroup differences were observed in WBC or albumin during this period. Additionally, neither follow-up duration nor the incidence of staged contralateral knee arthroplasty within the 6-month postoperative period differed significantly between groups (Table 1).
Exploration of Potential Predictors
Using α=0.10 as the significance threshold, univariate regression analysis identified several predictors of NP occurrence: gender (OR=4.055, p=0.071), preoperative ROM (OR=0.962, p=0.004), pMAA (OR=1.104, p=0.031), pMAA[abs.] (OR=1.125, p=0.022), pMAA difference (OR=1.233, p=0.008), and postoperative CRP (OR=1.034, p=0.033) (Table 2). The analysis revealed that female, poorer preoperative ROM, more severe preoperative mechanical axis angles, and elevated postoperative CRP were associated with NP development.
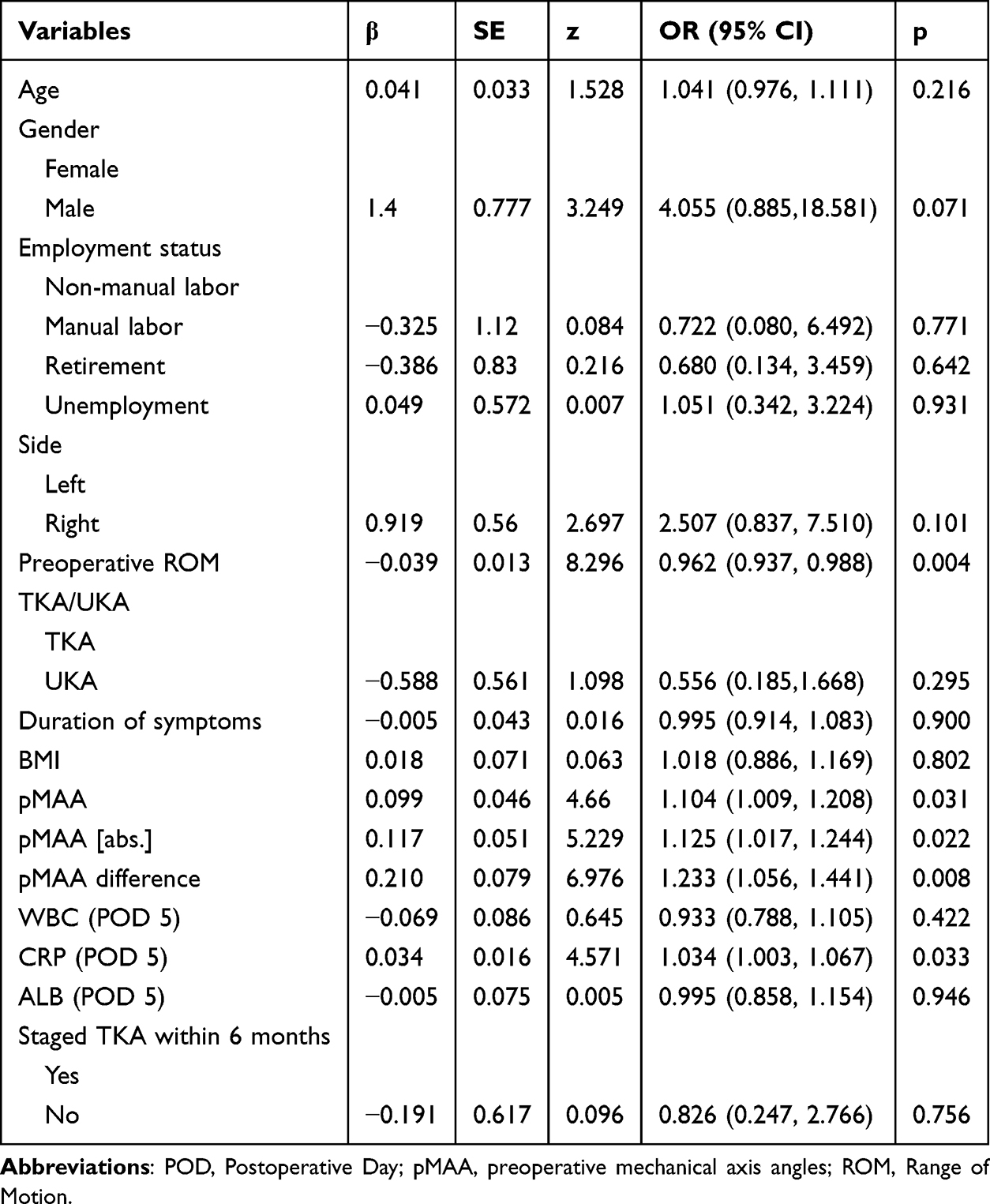 |
Table 2 Univariate Logistic Regression for NP |
The LASSO regression excluded pMAA[abs.] to prevent overfitting (Figure 3A, B and Supplementary Table 1). Subsequent multivariate logistic regression was performed on the 5 retained variables identified 4 independent factors for postoperative neuropathic pain: gender (OR=0.13, p=0.025), preoperative ROM (OR=0.97, p=0.023), pMAA difference (OR=1.32, p=0.007) and postoperative CRP (OR=1.04, p=0.017). The pMAA was excluded from the final (Figure 4).
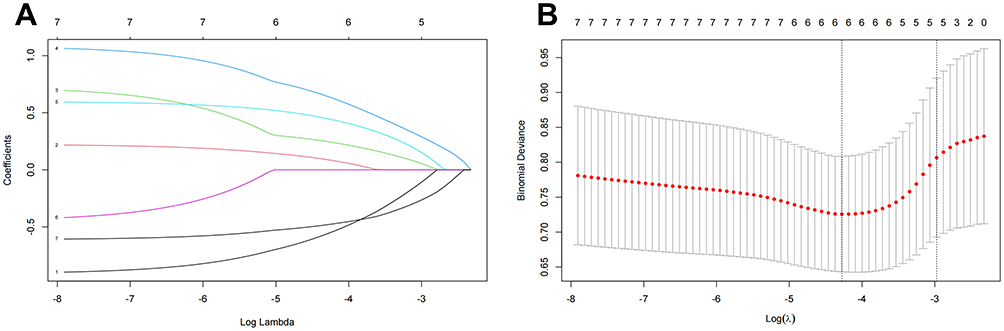 |
Figure 3 LASSO regression analysis for variable selection. (A) LASSO coefficient curve for the six variables. (B) Determination of the optimal regularization parameter (λ) in LASSO regression via 10-fold cross-validation using the minimum criterion. |
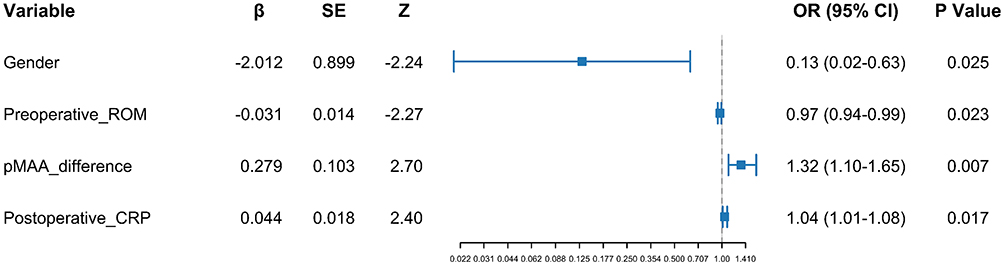 |
Figure 4 Multivariable logistic regression forest plot. Abbreviations: pMAA, preoperative mechanical axis angles; ROM, Range of Motion. |
Nomogram Development and Validation
Based on the multivariate analysis, an individualized nomogram for NP risk prediction was constructed (Figure 5). Collinearity diagnostics indicated no significant multicollinearity among predictors (Supplementary Table 2). The nomogram incorporated 4 independent predictors with a total scoring range of 0–200 points.
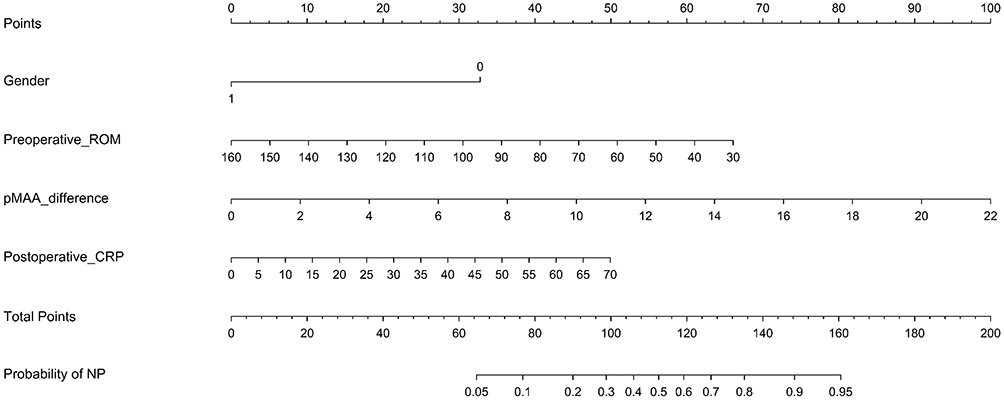 |
Figure 5 Nomogram Model for Predicting Risk of Postoperative NP. For clinical application, the patient’s clinical characteristics are used to locate their position on the corresponding axis for each variable. A vertical line is drawn upwards from this point to determine the assigned points for that variable. The points for all variables are then summed to calculate the Total Points (ranging from 0 to 200). Finally, a vertical line is projected downward from the Total Points to the “Prob of NP” axis to determine the predicted probability of postoperative neuropathic pain for that patient. |
Using 1000 bootstrap resamples, we evaluated model performance via ROC analysis, calibration curves, and DCA. The ROC curve demonstrated discriminative capacity with an AUC of 0.764 (95% CI 0.760–0.770), sensitivity 0.707 (95% CI 0.694–0.718), and specificity 0.737 (95% CI 0.724–0.747) (Figure 6A and Supplementary Table 3). Calibration curves indicated close agreement between predicted and observed outcomes (mean absolute error [MAE] = 0.037; Figure 6C). DCA showed net benefit across threshold probabilities of 0.003–0.391 (Figure 6D).
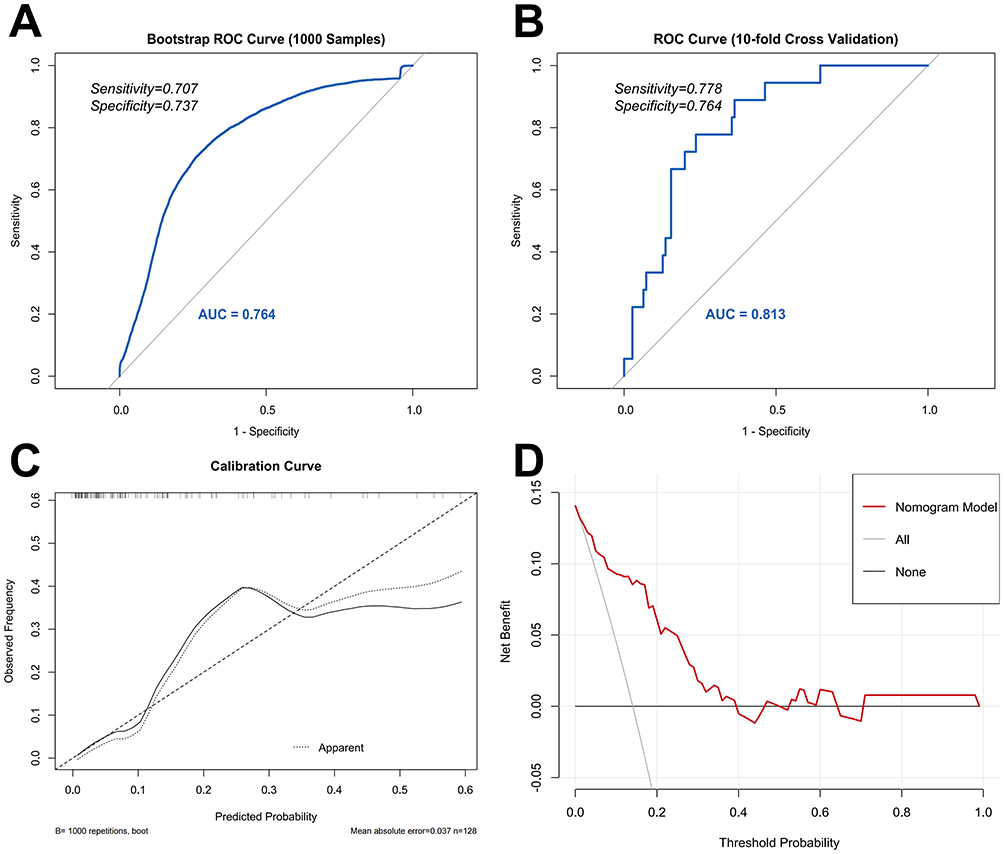 |
Figure 6 Validation of nomogram models. (A and B) The ROC curves of the nomogram after bootstrap sampling validation and ten-fold cross-validation. (C) The calibration curves of the nomogram. (D) The DCA curve showing the net benefit obtained at different decision thresholds. Abbreviations: ROC, Receiver Operating Characteristic; DCA, Decision Curve Analysis. |
Additional validation through 10-fold cross-validation yielded an AUC of 0.813 (95% CI 0.721–0.906), sensitivity 0.778 (95% CI 0.5–0.938), and specificity 0.764 (95% CI 0.676–0.833) (Figure 6B and Supplementary Table 3), confirming sustained discriminatory performance.
Discussion
Neuropathic pain (NP), a significant complication impairing long-term quality of life after knee arthroplasty, has received increasing clinical attention concerning its pathogenesis and risk factors. This study demonstrating a significant association between NP and deterioration in the pain dimension of quality of life. Furthermore, this study represents one of the first investigations into potential associations between objective clinical indicators and postoperative NP development. Notably, we identified 4 independent factors for postoperative NP: gender, preoperative ROM, pMAA difference, and postoperative CRP. Based on these factors, a predictive nomogram model was developed to assist clinicians in identifying patients at high risk for NP.
Postoperative pain interference following knee arthroplasty is a prevalent clinical issue that adversely affects patients’ quality of life.8 Previous studies have assessed NP using comprehensive quality-of-life assessment scales.39 However, the overlap between pain and functional domains within these scales may introduce confounding factors, potentially obscuring the specific association between pain intensity and physical function measurements.9 Pinedo-Villanueva et al found that patients in the high-pain group reported significantly worse outcomes in dimensions such as “pain,” “night pain,” and “limping,” and these pain dimensions were highly correlated with various aspects of quality of life.28 Consequently, the OKS-PS was developed, encompassing seven pain-related items to form a pain-specific instrument. As highlighted by Harris et al, the OKS-PS focuses on assessing “how pain limits function”.29 It thereby provides a more direct reflection of the limitations in quality of life experienced by patients from the perspective of pain. In contrast to comprehensive quality of life assessment tools like the EQ-5D, the OKS-PS aligns more closely with patients’ actual experiences and holds greater clinical relevance.28 Through this perspective, our findings confirm that greater NP severity is associated with diminished quality of life. This is evidenced by higher scores on NP-specific scales (PDQ & DN4) and lower OKS-PS scores. However, as established in prior research,40 both PDQ and DN4 exhibit inherent limitations in characterizing NP. The PDQ demonstrates relatively low diagnostic accuracy and cannot reliably distinguish between pain types. While the DN4 shows high sensitivity, its specificity is notably low, leading to a significant increase in false-positive rates. Consequently, future newly developed NP detection models should not only validate their correlation with neurophysiological and pathological manifestations, but also further verify the association between their detection results and outcomes from both pain-specific dimensional assessments and comprehensive quality-of-life scale.
The nomogram visually integrates multiple objective predictive factors for quantitative risk calculation, thereby reducing subjective bias in clinical assessment.41 Its application has shown significant clinical value. For example, Chen et al developed a nomogram incorporating key clinical and laboratory indicators to predict severe COVID-19 and mortality risk. Their model achieved AUC values of 0.771 and 0.748 in the training and validation sets, respectively—comparable to our results—confirming this predictive tool’s discriminative capacity.42 In oncology, nomogram is similarly widely adopted for prognostic evaluation, frequently outperforming conventional TNM staging systems.43
Current Research on post knee arthroplasty NP predominantly focuses on isolated risk factor exploration or conventional regression analyses, often lacking comprehensive multifactorial predictive models.19,20 This study advances the field by applying a nomogram to predict postoperative NP, which integrating diverse factors using objective metrics to minimize subjective bias. The DCA curve indicates that this model is suitable for using a lower threshold probability for clinical decision making. Given the potential negative impact of postoperative NP on patient outcomes and doctor-patient relationships, clinicians are advised to proactively communicate with patients exhibiting high predicted risk scores according to this model. Early intervention is necessary in the meantime. Regarding the evolution of NP diagnostic criteria—from reliance on single questionnaires to the incorporation of dual-questionnaire approaches—isolated assessment tools remain clinically limited. Future studies should therefore focus on developing additional diagnostic instruments and validating their combined utility.
Collectively, our findings provide direct support for the concept that the development of postoperative NP is not only clearly associated with nerve injury related risk factors, such as female sex and deformity severity, but also correlates with elevated postoperative CRP, which reflect heightened inflammatory responses. Based on this evidence, we propose that postoperative NP in the knee joint arises from the combined effects of nerve injury and inflammation.
Female sex constitutes a significant risk factor for various NP conditions.44,45 Our study demonstrates that this association persists in the context of postoperative NP, with female patients exhibiting both higher incidence rates and greater pain severity.44,45 Females are more likely to suffer from psychological problems, such as depression and pain catastrophizing, which are frequent risk factors for many kinds of NP.21 Additionally, biologically mediated sex differences, including hormonal influences on pain modulation pathways,46 may contribute to this observed disparity.
pMAA, quantified by the difference in femoral-tibial mechanical axis angles between the operative and contralateral limbs, served as an independent predictor of NP. Whereas no statistically significant results were obtained for the mechanical axis angles on the operated side. This observation suggests that the magnitude of deformity, as reflected by the inter-limb discrepancy in alignment, holds greater predictive value than unilateral measurements. This finding underscores the potential role of individual biomechanical variations in NP pathogenesis. pMMA serves as a key imaging indicator for assessing the degree of knee joint deformity.37 Previous research indicates that joint deformity may elevate NP risk through two primary mechanisms: First, severe deformity necessitates more extensive soft tissue releases during surgery. For instance, correcting a varus deformity often requires release of the deep medial collateral ligament and the posteromedial joint capsule.47 These structures are in close proximity to nerves such as the medial femoral cutaneous nerve (MFCN) and the infrapatellar branch of the saphenous nerve (IFCN),14 consequently increasing the risk of intraoperative nerve injury. Second, chronic nerve entrapment due to pre-existing deformity may impede full postoperative nerve recovery.48 An example is common peroneal nerve entrapment associated with genu varum deformity,49 which can predispose to NP. These findings affirm the value of preoperative radiographic evaluation, specifically assessing inter-limb alignment discrepancies, in predicting NP risk. Nevertheless, it is crucial to acknowledge that NP is a multifactorial outcome influenced by diverse biopsychosocial aspects,50 Consequently, relying solely on imaging parameters for NP prediction has inherent limitations.51
Among the potential mechanisms contributing to NP following knee arthroplasty, the inflammatory response warrants specific consideration. Elevated postoperative CRP were significantly associated with NP development (p=0.017), implicating inflammation in its pathogenesis. Previous research has established inflammation’s critical role in diverse NP states (eg, polyneuropathy, osteoarthritis), primarily through enhanced neuronal excitability and glial cell activation.52,53 While this association is recognized in other contexts, the specific inflammatory mechanisms operating after arthroplasty necessitate further investigation. Another studies indicate that neuropathic features in patients with sciatica are associated not only with psychological factors such as depression, anxiety, and alexithymia but also with elevated serum CRP levels.17 The identification of objective biomarkers to complement subjective psychological assessments is therefore a key objective of the present work. Furthermore, inflammatory mediators (eg, cytokines and chemokines) might contribute to the NP pathological process by inducing sensitization pathways within both the peripheral and central nervous systems. This potential role represents a promising avenue for future research on NP following knee arthroplasty.18
Several limitations warrant consideration in this study. First, its single-center retrospective design entails inherent constraints, including a limited sample size, potential data incompleteness, and possible recall bias. Consequently, the current study design may not adequately capture the occurrence of late onset neuropathic pain.3 Second, there is probability of model overfitting due to less NP event and there is lack of external validation, to compensate for this, we strengthened the analytical rigor by applying LASSO regression and performed two internal validation procedures—bootstrapping and 10-fold cross-validation. Third, although the results demonstrate good internal consistency and are authentic and reliable, the number of included patients was limited by challenges in following up with discharged participants. The response rate of 70.7% may also introduce selection bias. While this return rate is predictable,38 it should be acknowledged that it impacts the exploration of prevalence and predictive factors. Future research should address these limitations through large-scale prospective studies with extended follow-up periods, which would better control confounding variables and further elucidate risk factors for postoperative NP.
Conclusion
Firstly, the prevalence of postoperative NP was 14.06%, and it can significantly impair quality of life. Secondly, factors independently associated with postoperative NP included gender, preoperative ROM, pMAA difference, and postoperative CRP. Furthermore, this study developed a nomogram prediction model demonstrating good predictive efficacy, providing a quantitative tool for individualized assessment. However, prospective, multicenter validation is required before the model can be widely applied in clinical practice.
Abbreviation
NP, neuropathic pain; MFCN, medial femoral cutaneous nerve; IFCN, intermediate femoral cutaneous nerve; IPBSN, infrapatellar branch of the saphenous nerve; UKA, unicompartmental knee arthroplasty; TKA, total knee arthroplasty; OKS-PS, Oxford Knee Score pain subscale; PDQ, Pain DETECT questionnaire; pMAA, preoperative mechanical axis angles; ROM, range of motion; DCA, decision curve analysis; BMI, body mass index; CRP, C-reactive protein.
Data Sharing Statement
The data that support the findings of this study available from the corresponding author, upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and received ethical approval from our institutional review board (Approval No.: MRCTA, ECFAH of FMU [2023]308, Branch for Medical Research and Clinical Technology Application, Ethics Committee of the First Affiliated Hospital of Fujian Medical University). Informed consent was obtained from all participants, ensuring they understood and agreed to their responses being used in this research project. They were assured of their right of anonymity, respect for their dignity, and the freedom to withdraw from the study at any point.
Consent for Publication
All authors gave final approval of the version to be published.
Funding
This work was supported by Natural Science Foundation of Fujian Province (2025J01111), the First Affiliated Hospital of Fujian Medical University Excellent Talent Program (YXRQN-ZCF2023) and the First Affiliated Hospital of Fujian Medical University Excellent Talent Program (YJCRC-B-ZWM2024).
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter discussed in this manuscript.
References
1. Madry H. Surgical therapy in osteoarthritis. Osteoarthritis Cartilage. 2022;30:1019–13. doi:10.1016/j.joca.2022.01.012
2. Şahin F, Beyaz SG, Karakuş N, Inanmaz ME. Total knee arthroplasty postsurgical chronic pain, neuropathic pain, and the prevalence of neuropathic symptoms: a prospective observational study in Turkey. J Pain Res. 2021;14:1315–1321. doi:10.2147/JPR.S293856
3. Bertram W, Howells N, White SP, et al. Prevalence and patterns of neuropathic pain in people with chronic post-surgical pain after total knee arthroplasty. Bone Joint J. 2024;106-B(6):582–588. doi:10.1302/0301-620X.106B6.BJJ-2023-0889.R1
4. Hasegawa M, Tone S, Naito Y, Wakabayashi H, Sudo A. Prevalence of persistent pain after total knee arthroplasty and the impact of neuropathic pain. J Knee Surg. 2019;32(10):1020–1023. doi:10.1055/s-0038-1675415
5. Priol R, Pasquier G, Putman S, Migaud H, Dartus J, Wattier J-M. Trajectory of chronic and neuropathic pain, anxiety and depressive symptoms and pain catastrophizing after total knee replacement. Results of a prospective, single-center study at a mean follow-up of 7.5 years. Orthop Traumatol Surg Res. 2023;109:103543. doi:10.1016/j.otsr.2022.103543
6. Richardson MK, Liu KC, Mayfield CK, Kistler NM, Christ AB, Heckmann ND. Complications and safety of simultaneous bilateral total knee arthroplasty: a patient characteristic and comorbidity-matched analysis. J Bone Joint Surg. 2023;105(14):1072–1079. doi:10.2106/JBJS.23.00112
7. Vieira WF, Coelho DRA, Litwiler ST, et al. Neuropathic pain, mood, and stress-related disorders: a literature review of comorbidity and co-pathogenesis. Neurosci Biobehav Rev. 2024;161:105673. doi:10.1016/j.neubiorev.2024.105673
8. Lee N-K, Won SJ, Lee J-Y, Kang S-B, Yoo SY, Chang CB. Presence of night pain, neuropathic pain, or depressive disorder does not adversely affect outcomes after total knee arthroplasty: a prospective cohort study. J Korean Med Sci. 2022;37(43):e309. doi:10.3346/jkms.2022.37.e309
9. Jensen MP, Chodroff MJ, Dworkin RH. The impact of neuropathic pain on health-related quality of life: review and implications. Neurology. 2007;68(15):1178–1182. doi:10.1212/01.wnl.0000259085.61898.9e
10. Melikoglu MA, Celik A. Does neuropathic pain affect the quality of sleep? Eurasian J Med. 2017;49(1):40–43. doi:10.5152/eurasianjmed.2017.16261
11. Finnerup NB, Kuner R, Jensen TS. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021;101(1):259–301. doi:10.1152/physrev.00045.2019
12. Haanpää M, Attal N, Backonja M, et al. NeuPSIG guidelines on neuropathic pain assessment. Pain. 2011;152(1):14–27. doi:10.1016/j.pain.2010.07.031
13. Scholz J, Finnerup NB, Attal N, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–59. doi:10.1097/j.pain.0000000000001365
14. B S, Td N, Ae J, et al. The anterior branch of the medial femoral cutaneous nerve innervates the anterior knee: a randomized volunteer trial. Minerva Anestesiologica. 2023;89. doi:10.23736/S0375-9393.22.16910-5
15. Valdes AM, Suokas AK, Doherty SA, Jenkins W, Doherty M. History of knee surgery is associated with higher prevalence of neuropathic pain-like symptoms in patients with severe osteoarthritis of the knee. Semin Arthritis Rheum. 2014;43(5):588–592. doi:10.1016/j.semarthrit.2013.10.001
16. Peng MS, Clendenen SR, Shi GG, Tsui BCH. Infrapatellar branch of saphenous nerve: from anatomy, sonoanatomy to its clinical implications. Reg Anesth Pain Med. 2025;rapm–2025–106383. doi:10.1136/rapm-2025-106383
17. Sommer C, Leinders M, Üçeyler N. Inflammation in the pathophysiology of neuropathic pain. Pain. 2018;159(3):595. doi:10.1097/j.pain.0000000000001122
18. Dainese P, Mahieu H, De Mits S, Wittoek R, Stautemas J, Calders P. Associations between markers of inflammation and altered pain perception mechanisms in people with knee osteoarthritis: a systematic review. RMD Open. 2023;9(2):e002945. doi:10.1136/rmdopen-2022-002945
19. Maeda K, Sonohata M, Kitajima M, Kawano S, Mawatari M. Risk factors of neuropathic pain after total hip arthroplasty. Hip & Pelvis. 2018;30(4):226–232. doi:10.5371/hp.2018.30.4.226
20. Ashoorion V, Sadeghirad B, Wang L, et al. Predictors of persistent post-surgical pain following total knee arthroplasty: a systematic review and meta-analysis of observational studies. Pain Med. 2023;24(4):369–381. doi:10.1093/pm/pnac154
21. Drosos GI, Triantafilidou T, Ververidis A, Agelopoulou C, Vogiatzaki T, Kazakos K. Persistent post-surgical pain and neuropathic pain after total knee replacement. World J Orthop. 2015;6(7):528–536. doi:10.5312/wjo.v6.i7.528
22. Christ AB, Chiu Y-F, Joseph A, Westrich GH, Lyman S. Incidence and risk factors for peripheral nerve injury after 383,000 total knee arthroplasties using a New York state database (SPARCS). J Arthroplasty. 2019;34(10):2473–2478. doi:10.1016/j.arth.2019.05.008
23. Shetty T, Nguyen JT, Sasaki M, et al. Risk factors for acute nerve injury after total knee arthroplasty. Muscle Nerve. 2018;57(6):946–950. doi:10.1002/mus.26045
24. Hao Y, Li J, Feng Y, Huang H, Dong W, Liu G. Clinical outcomes of unicompartmental knee arthroplasty and total knee arthroplasty in the same patient. Arch Orthop Trauma Surg. 2024;144(11):4791–4800. doi:10.1007/s00402-024-05564-3
25. Petzke F, Tölle T, Fitzcharles M-A, Häuser W. Cannabis-Based medicines and medical cannabis for chronic neuropathic pain. CNS Drugs. 2022;36(1):31–44. doi:10.1007/s40263-021-00879-w
26. Wylde V, Beswick A, Bruce J, Blom A, Howells N, Gooberman-Hill R. Chronic pain after total knee arthroplasty. EFORT Open Reviews. 2018;3(8):461–470. doi:10.1302/2058-5241.3.180004
27. Wang S, Shen B, Wu M, Chen C, Wang J. Effects of socioeconomic status on risk of ischemic stroke: a case-control study in the Guangzhou population. BMC Public Health. 2019;19(1):648. doi:10.1186/s12889-019-6998-4
28. Pinedo-Villanueva R, Khalid S, Wylde V, Gooberman-Hill R, Soni A, Judge A. Identifying individuals with chronic pain after knee replacement: a population-cohort, cluster-analysis of Oxford knee scores in 128,145 patients from the English National Health Service. BMC Musculoskelet Disord. 2018;19(1):354. doi:10.1186/s12891-018-2270-9
29. Harris K, Dawson J, Doll H, et al. Can pain and function be distinguished in the Oxford Knee Score in a meaningful way? An exploratory and confirmatory factor analysis. Qual Life Res. 2013;22(9):2561–2568. doi:10.1007/s11136-013-0393-x
30. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1):29–36. doi:10.1016/j.pain.2004.12.010
31. Freynhagen R, Baron R, Gockel U, Tölle TR. Pain DETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006;22(10):1911–1920. doi:10.1185/030079906X132488
32. Zhang Y, Zhang S, Pan L, et al. Painful Diabetic Peripheral Neuropathy Study of Chinese Outpatients (PDNSCOPE): a multicentre cross-sectional registry study of clinical characteristics and treatment in Mainland China. Pain Ther. 2021;10(2):1355–1373. doi:10.1007/s40122-021-00281-w
33. Chang X, Yao S, Wei J, Shang L, Xu C, Ma J. The validation and cross-cultural adaptation of the pain DETECT questionnaire in osteoarthritis-related pain. J Orthop Surg Res. 2025;20(1):94. doi:10.1186/s13018-025-05510-y
34. Epping R, Verhagen AP, Hoebink EA, Rooker S, Scholten-Peeters GGM. The diagnostic accuracy and test-retest reliability of the Dutch PainDETECT and the DN4 screening tools for neuropathic pain in patients with suspected cervical or lumbar radiculopathy. Musculoskelet Sci Pract. 2017;30:72–79. doi:10.1016/j.msksp.2017.05.010
35. Sun J, Li L, Yuan S, Zhou Y. Analysis of early postoperative pain in the first and second knee in staged bilateral total knee arthroplasty: a retrospective controlled study. PLoS One. 2015;10:e0129973. doi:10.1371/journal.pone.0129973
36. Kim M-H, Nahm FS, Kim TK, Chang MJ, Do S-H. Comparison of postoperative pain in the first and second knee in staged bilateral total knee arthroplasty: clinical evidence of enhanced pain sensitivity after surgical injury. Pain. 2014;155:22–27. doi:10.1016/j.pain.2013.08.027
37. Moon YW, Kim JG, Han JH, Do KH, Seo JG, Lim HC. Factors Correlated with the Reducibility of varus deformity in knee osteoarthritis: an analysis using navigation guided TKA. Clin Orthop Surg. 2013;5:36–43. doi:10.4055/cios.2013.5.1.36
38. Meyer VM, Benjamens S, Moumni ME, Lange JFM, Pol RA. Global overview of response rates in patient and health care professional surveys in surgery: a systematic review. Ann Surg. 2022;275:e75. doi:10.1097/SLA.0000000000004078
39. Allison DJ, Ahrens J, Mirkowski M, Mehta S, Loh E. The effect of neuropathic pain treatments on pain interference following spinal cord injury: a systematic review. J Spinal Cord Med. 2023;47:465–476. doi:10.1080/10790268.2023.2218186
40. Dunker Ø, Grotle M, Kvaloy M, et al. Accuracy of neuropathic pain measurements in patients with symptoms of polyneuropathy: validation of painDETECT, S-LANSS, and DN4. Pain. 2022;164(5):991–1001. doi:10.1097/j.pain.0000000000002793
41. Lee W, Lam S-K, Zhang Y, Yang R, Cai J. Review of methodological workflow, interpretation and limitations of nomogram application in cancer study. Radiat Med Protect. 2022;3(4):200–207. doi:10.1016/j.radmp.2022.08.004
42. Chen J, Hu Q, Zhong R, et al. Development and validation of nomogram models for severe and fatal COVID-19. Sci Rep. 2024;14(1):29146. doi:10.1038/s41598-024-80310-8
43. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology – more than meets the eye. Lancet Oncol. 2015;16(4):e173–80. doi:10.1016/S1470-2045(14)71116-7
44. Baskozos G, Hébert HL, Pascal MM, et al. Epidemiology of neuropathic pain: an analysis of prevalence and associated factors in UK Biobank. Pain Rep. 2023;8:e1066. doi:10.1097/PR9.0000000000001066
45. Smith BH, Hébert HL, Veluchamy A. Neuropathic pain in the community: prevalence, impact, and risk factors. Pain. 2020;161(Supplement 1):S127. doi:10.1097/j.pain.0000000000001824
46. Luo X, Chen O, Wang Z, et al. IL-23/IL-17A/TRPV1 axis produces mechanical pain via macrophage-sensory neuron crosstalk in female mice. Neuron. 2021;109:2691–2706.e5. doi:10.1016/j.neuron.2021.06.015
47. Abdalla Abusenna MD, Hany El-Bardesy MS. Total knee replacement in genu valgum. Med J Cairo Univ. 2018;86(March):223–229. doi:10.21608/mjcu.2018.55081
48. Gutkowska O, Martynkiewicz J, Mizia S, Bąk M, Gosk J. Results of operative treatment of brachial plexus injury resulting from shoulder dislocation: a study with a long-term follow-up. World Neurosurg. 2017;105:623–631. doi:10.1016/j.wneu.2017.06.059
49. Puijk R, Rassir R, Kok LM, Sierevelt IN, Nolte PA. Common peroneal nerve palsy after TKA in valgus deformities; a systematic review. J Exp Orthop. 2022;9:12. doi:10.1186/s40634-021-00443-x
50. Forstenpointner J, Ruscheweyh R, Attal N, et al. No pain, still gain (of function): the relation between sensory profiles and the presence or absence of self-reported pain in a large multicenter cohort of patients with neuropathy. PAIN. 2021;162:718. doi:10.1097/j.pain.0000000000002058
51. Pegreffi F, Di Leo MT, Costa G, et al. Kellgren-Lawrence vs. outerbridge classifications: shedding light on the weak correlation to reaffirm the value of knee clinical examination. Arthroscopy. 2025. doi:10.1016/j.arthro.2025.05.036
52. de Oliveira Júnior JO, Portella Junior CSA, Cohen CP. Inflammatory mediators of neuropathic pain. Rev Dor. 2016;17:35–42. doi:10.5935/1806-0013.20160045
53. Liu F, Zhang L, Su S, et al. Neuronal C-Reactive protein/FcγRI positive feedback proinflammatory signaling contributes to nerve injury induced neuropathic pain. Adv Sci. 2023;10:e2205397. doi:10.1002/advs.202205397
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Anaemia, Morphological Classification and Its Associated Risk Factors Among Lactating Mothers at Mbarara City Council Health Centre IV, Southwestern Uganda
Clinton O, Micheal K, Namyalo Angella K, Mary M, Mike M, Muwanguzi E, Okongo B, Wagubi R
Journal of Blood Medicine 2022, 13:473-481
Published Date: 2 September 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023