Back to Journals » Journal of Inflammation Research » Volume 19
Preoperative Systemic Pan-Immune-Inflammation Value Predicts Posthepatectomy Liver Failure After Laparoscopic Resection for Hepatocellular Carcinoma: A Retrospective Cohort Study
Authors Wu X ![]() , Xu S, Zhang T, Xing Y, Min X, Wu J, Mao Q
, Xu S, Zhang T, Xing Y, Min X, Wu J, Mao Q
Received 13 February 2026
Accepted for publication 19 May 2026
Published 24 June 2026 Volume 2026:19 600314
DOI https://doi.org/10.2147/JIR.S600314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Felix Marsh-Wakefield
Xiuyu Wu,1,2,* Shun Xu,1,* Tianqi Zhang,3,* Ying Xing,4 Xia Min,1 Jingjing Wu,1 Qian Mao1
1Department of Hepatobiliary and Pancreatic Surgery, The Affiliated Jiangning Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2School of Clinical Medicine, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Department of Emergency Medicine, The Affiliated Jiangning Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 4School of Nursing, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Mao, Department of Hepatobiliary and Pancreatic Surgery, The Affiliated Jiangning Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Background: Post-hepatectomy liver failure (PHLF) remains a major cause of morbidity after liver resection for hepatocellular carcinoma (HCC). Routine blood-count-based inflammatory indices may complement established liver reserve assessments. This study evaluated whether preoperative systemic pan-immune-inflammation value (S-PIV) predicts PHLF after conventional laparoscopic hepatectomy for HCC.
Methods: We conducted a single-center retrospective cohort study of consecutive patients who completed conventional laparoscopic hepatectomy for liver tumors between January 2017 and December 2025. Eligible patients had pathologically confirmed HCC and complete preoperative laboratory data within 7 days before surgery. Planned open hepatectomy, conversion to open surgery, and robotic-assisted hepatectomy were outside the predefined cohort scope. S-PIV was calculated as neutrophil count × monocyte count × platelet count / lymphocyte count. The primary outcome was ISGLS-defined PHLF, analyzed as any-grade PHLF versus no PHLF. Discrimination was assessed using ROC analysis, dose-response using restricted cubic splines, and clinical utility using decision curve analysis.
Results: Among 582 screened patients, 356 were included; 68 (19.1%) developed PHLF. Preoperative S-PIV showed good discrimination for PHLF (AUC 0.873). The Youden index identified an optimal cut-off of 455.4, with sensitivity 0.726 and specificity 0.908. S-PIV showed higher AUCs than NLR (0.831) and PLR (0.848). Higher S-PIV was associated with PHLF in univariable analysis (per 100 units: OR 1.12, 95% CI 1.06– 1.45; P< 0.001) and remained independently associated after sequential adjustment for demographics/comorbidities, liver functional reserve, and tumor/operative factors (Model 3 per 100 units: OR 1.06, 95% CI 1.03– 1.13; P< 0.001). Restricted cubic splines showed a graded risk increase without evidence of nonlinearity, and decision curve analysis suggested net benefit across threshold probabilities of approximately 10%– 70%.
Conclusion: Preoperative S-PIV, derived from routine blood counts, may serve as a practical adjunct for PHLF risk stratification after conventional laparoscopic hepatectomy for HCC. External multicenter validation and calibration are urgently required before routine implementation.
Plain Language Summary: Liver surgery can help many patients with liver cancer, but some patients may have poor liver function after part of the liver is removed. This problem can slow recovery and may become serious. Doctors therefore need simple ways to identify patients who may need closer care before and after surgery.
In this study, we reviewed people with this type of liver cancer who had laparoscopic liver surgery at our hospital. We tested whether information from a routine blood test before surgery could help estimate the chance of liver failure after surgery. This blood test reflects the balance between inflammation and immune status in the body.
We found that patients with a higher inflammation-related blood score before surgery were more likely to develop liver failure after surgery. This score may help doctors discuss surgical risk with patients, plan perioperative care, and identify patients who may need closer monitoring after surgery.
These findings are promising, but they come from one hospital. More studies from multiple hospitals are needed before this blood score can be used routinely in clinical practice.
What do the terms mean?
The terms used in this article are explained in plain language as follows. Hepatocellular carcinoma refers to the most common type of primary liver cancer. Laparoscopic liver surgery refers to liver surgery performed through small cuts in the abdomen using a camera and surgical instruments. Liver failure after surgery refers to a condition in which the remaining liver does not work well enough after part of the liver has been removed. A blood inflammation score is calculated from routine blood cell counts and reflects inflammation and immune status. Liver reserve refers to the ability of the liver to keep working after surgery. Closer monitoring means more careful observation and follow-up before and after surgery. Multicenter validation means testing the findings in patients from other hospitals to confirm whether the results are reliable.
Keywords: hepatocellular carcinoma, laparoscopic hepatectomy, posthepatectomy liver failure, pan-immune-inflammation value, systemic inflammation, risk prediction
Introduction
Hepatocellular carcinoma (HCC) remains a major global health burden, accounting for substantial cancer-related incidence and mortality worldwide.1 Contemporary staging and practice guidance continue to emphasize surgical resection as a potentially curative option for appropriately selected patients, particularly when liver functional reserve and tumor biology permit safe hepatectomy.2,3 However, the clinical benefit of resection can be offset by serious postoperative complications, among which post-hepatectomy liver failure (PHLF) is the most feared because it directly drives morbidity, prolonged hospitalization, and early mortality after liver surgery.4–6 The International Study Group of Liver Surgery (ISGLS) definition has been widely adopted to standardize PHLF diagnosis and grading, facilitating comparability across surgical series and enabling more consistent perioperative risk evaluation.4
Despite progress in parenchymal-sparing techniques and perioperative care pathways, PHLF remains difficult to prevent because risk is multifactorial and not fully captured by any single preoperative test.5,6 Current strategies for preoperative risk assessment focus primarily on hepatic functional reserve and anticipated remnant liver capacity, using composite liver function scores and functional tests to estimate the ability to tolerate resection.5,6 The albumin-bilirubin (ALBI) grade was developed as an objective approach to quantify liver dysfunction in HCC and has been increasingly incorporated into perioperative decision-making frameworks.7 In addition, ALBI-based or related liver reserve models have been evaluated for predicting PHLF after major hepatectomy for HCC, yet predictive performance across cohorts is variable, reflecting heterogeneity in patient selection, cirrhosis severity, and operative complexity.8,9 Indocyanine green retention at 15 minutes (ICG-R15) is also frequently used to quantify hepatic clearance capacity, and ICG-based nomograms have been proposed to improve individualized PHLF risk estimation.10
Beyond liver reserve, systemic inflammation and immune dysregulation have gained recognition as biologically plausible contributors to impaired liver regeneration and vulnerability to postoperative decompensation after hepatectomy.5,6 Blood-derived immune-inflammation indices, such as the systemic immune-inflammation index (SII), integrate circulating leukocyte and platelet compartments and have shown prognostic relevance in HCC.11 More recently, the pan-immune-inflammation value (PIV)-a composite metric incorporating neutrophils, monocytes, lymphocytes, and platelets-was introduced and validated as a robust prognostic marker in large oncologic cohorts,12 and subsequent meta-analytic evidence has supported its association with survival across diverse malignancies.13 These findings suggest that a single, routinely available inflammatory composite may capture a clinically actionable systemic milieu that is not reflected by liver function parameters alone.
More broadly, recent cohort-profile and retrospective cohort studies in other clinical settings have underscored the importance of explicit cohort definitions, standardized data capture, and cautious interpretation of observational findings.14,15 Recent retrospective studies have developed preoperative models incorporating liver functional reserve, inflammatory indices, ICG-R15, and clinical variables to predict PHLF after hepatectomy for HCC.16–19 Although these models have reported promising discriminatory performance, their clinical transportability remains limited by single-center derivation, heterogeneous variable selection, and insufficient external validation or calibration.20 Nevertheless, in the hepatectomy setting, existing prediction models often emphasize hepatic reserve and operative factors while underutilizing comprehensive immune-inflammation composites; moreover, many models show limited generalizability when applied across institutions and populations.20 This challenge highlights the importance of rigorous methodological evaluation and transparent reporting standards for prediction research, as emphasized by established risk-of-bias frameworks.20 In parallel, enhanced recovery after surgery (ERAS) recommendations and ERAS-based strategies for liver surgery-including evidence syntheses focused on cirrhotic populations-underscore the ongoing need for precise preoperative stratification to identify patients who may benefit from tailored perioperative optimization.21,22 Against this background, we conducted a retrospective cohort study to determine whether a preoperative systemic inflammation composite (S-PIV), calculated from routine blood counts, is associated with PHLF after hepatectomy for HCC and to evaluate its incremental discriminatory and clinical utility when integrated into perioperative risk assessment.
Methods
Study Design, Setting, and Ethics
This retrospective cohort study was conducted at the Affiliated Jiangning Hospital of Nanjing Medical University. Consecutive patients who completed conventional laparoscopic hepatectomy for liver tumors between January 2017 and December 2025 were screened. The study protocol was approved by the institutional review board (IRB No. 2026–03-026-K01), and the requirement for informed consent was waived due to the retrospective design.
Patient Selection
The selection process is presented in Figure 1. Eligible patients had postoperative pathological confirmation of hepatocellular carcinoma (HCC), completed conventional laparoscopic curative-intent hepatectomy, were aged ≥18 years, and had complete preoperative laboratory testing obtained within 7 days before surgery. Because the present study was designed to evaluate a conventional laparoscopic hepatectomy cohort, planned open hepatectomy, conversion from laparoscopic to open surgery, and robotic-assisted hepatectomy were outside the predefined scope of this study and were not included in the final analytic population. Patients were excluded for non-HCC pathology, receipt of preoperative anti-tumor therapy (eg, transarterial chemoembolization or radiofrequency ablation), recurrent disease or palliative resection, extrahepatic metastasis, active infection or inflammatory conditions, hematologic or autoimmune disorders, or incomplete key clinical data, consistent with Figure 1. During cohort construction, 14 patients were excluded because of incomplete key clinical data. Missing key variables mainly involved one or more variables required for exposure definition, covariate adjustment, or outcome ascertainment, including preoperative blood count components, liver functional reserve assessments, key operative variables, or postoperative outcome records. Active infection or inflammatory conditions were defined as a documented clinical diagnosis requiring antibiotic treatment and/or evidence of systemic infection, such as fever and/or leukocytosis, during the preoperative evaluation period. Such patients were excluded to minimize inflammatory confounding.
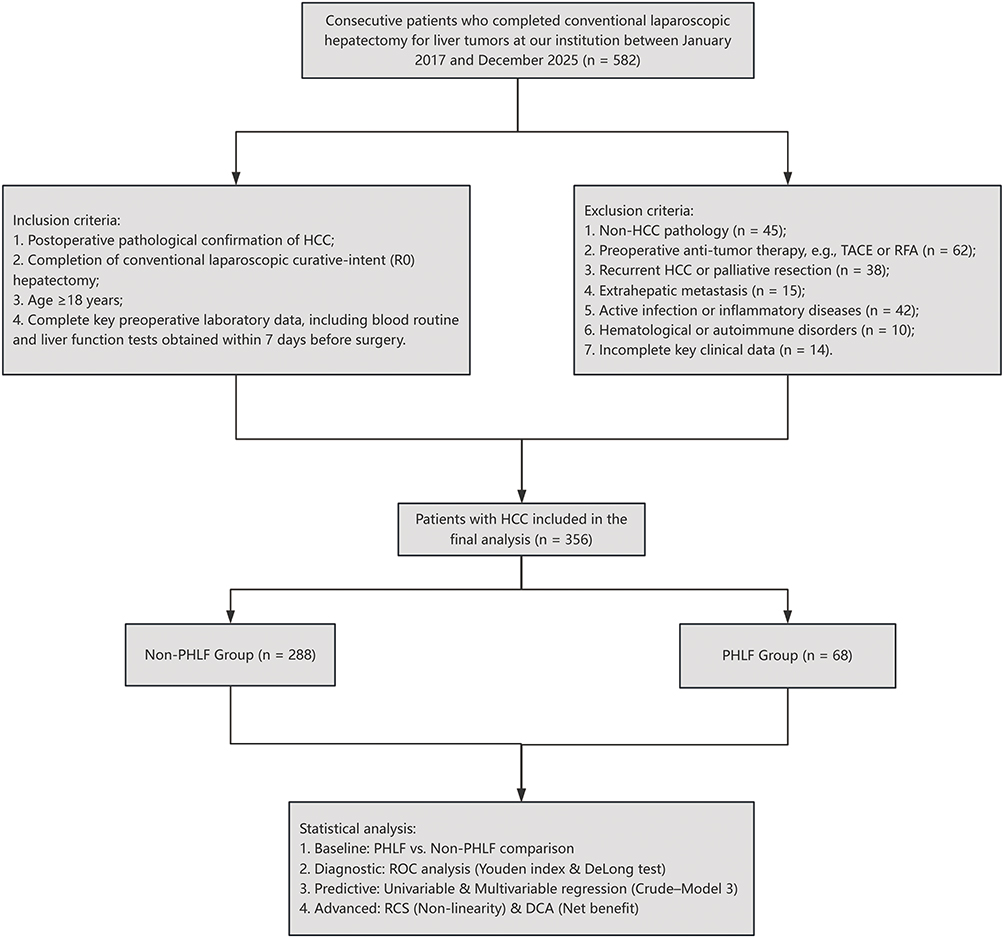 |
Figure 1 Study flow diagram. Consecutive patients who completed conventional laparoscopic hepatectomy for liver tumors between January 2017 and December 2025 were screened. Patients were included or excluded according to predefined criteria, resulting in a final analytic cohort of 356 patients with pathologically confirmed hepatocellular carcinoma. Among them, 68 patients developed post-hepatectomy liver failure (PHLF), whereas 288 patients did not. Planned open hepatectomy, conversion from laparoscopic to open surgery, and robotic-assisted hepatectomy were outside the predefined scope of this conventional laparoscopic cohort. PHLF was defined according to the International Study Group of Liver Surgery criteria. |
Data Collection, Perioperative Management, and Definitions
Clinical and laboratory variables were retrospectively abstracted from the hospital information system (HIS). Demographics, comorbidities, liver disease background, preoperative laboratory variables, tumor characteristics, and operative variables were extracted. Preoperative laboratory variables included complete blood count parameters and liver function tests obtained within 7 days before surgery. Complete blood count parameters were measured using an automated hematology analyzer (Sysmex XN-9000, Kobe, Japan) in the hospital’s central laboratory according to standardized quality-control procedures. Tumor characteristics included tumor size, tumor number, Barcelona Clinic Liver Cancer (BCLC) stage, alpha-fetoprotein (AFP), and pathological features. Operative variables included extent of hepatectomy, Pringle maneuver time, intraoperative blood loss, and transfusion. Major hepatectomy was defined as resection of ≥3 Couinaud segments. All included procedures were completed as conventional laparoscopic hepatectomies. Planned open procedures, conversion to open surgery, and robotic-assisted procedures were outside the predefined scope of this conventional laparoscopic cohort. The Pringle maneuver was routinely used for inflow control and applied in an intermittent or continuous fashion at the surgeon’s discretion. Intraoperative transfusion was defined as red blood cell (RBC) transfusion. Comorbidities were defined based on documented physician diagnoses in the medical record and/or ongoing medication use at the time of surgery. Although body mass index and serum albumin were available, detailed preoperative nutritional assessments, sarcopenia measurements, and alcohol/tobacco exposure histories were not systematically or consistently documented across the entire retrospective study period. Therefore, these variables were not included in the primary multivariable models to avoid introducing additional information bias. Data collection and verification were facilitated by trained nursing staff who abstracted variables from medical records, cross-checked key fields for consistency and completeness, and minimized transcription errors under the supervision of the study investigators.
Immune–Inflammation Indices
The primary exposure was the systemic pan-immune-inflammation value (S-PIV), calculated from preoperative peripheral blood counts as follows: S-PIV = neutrophil count × monocyte count × platelet count / lymphocyte count. Neutrophil, monocyte, platelet, and lymphocyte counts were derived from the same preoperative complete blood count test obtained within 7 days before surgery. Conventional inflammatory indices, including the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), were assessed as comparators.
Liver Functional Reserve Assessment
ALBI grade was calculated using the standard formula based on serum albumin and bilirubin and categorized according to established cutoffs.7 Indocyanine green retention at 15 minutes (ICG-R15) was measured preoperatively using a standard indocyanine green dose of 0.5 mg/kg within 7 days before surgery.
Outcome Definition
The primary endpoint was post-hepatectomy liver failure (PHLF), defined according to the International Study Group of Liver Surgery (ISGLS) criteria,4 with grades A/B/C recorded for clinical characterization. For the primary analyses, PHLF was modeled as a binary outcome (any-grade PHLF vs no PHLF). PHLF diagnosis and grading were independently confirmed by two senior hepatobiliary surgeons, each with more than 10 years of experience in hepatobiliary surgery and hepatocellular carcinoma resection and holding the title of Associate Chief Physician or above, with final classification reached by consensus.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), as appropriate, and categorical variables as number (%). Data distribution was assessed by visual inspection of histograms and Q-Q plots and formally tested using the Shapiro–Wilk test. Normally distributed continuous variables were compared using Student’s t test, non-normally distributed variables using the Mann–Whitney U-test, and categorical variables using the χ2-test or Fisher’s exact test, as appropriate. Receiver operating characteristic (ROC) analysis was used to assess discrimination, with areas under the curve (AUCs) reported along with 95% confidence intervals (CIs) derived using the DeLong method. The optimal cut-off value for S-PIV was determined using the Youden index, and AUCs were compared using the DeLong test. Univariable logistic regression was performed to estimate odds ratios (ORs) and 95% CIs for PHLF. Sequentially adjusted multivariable logistic regression models were constructed as follows: Model 1 adjusted for demographics and comorbidities; Model 2 further adjusted for liver functional reserve; and Model 3 additionally adjusted for tumor and surgical factors. To explore the dose-response relationship between continuous S-PIV and PHLF risk, restricted cubic spline regression was applied using three knots at the 10th, 50th, and 90th percentiles, with nonlinearity assessed using the Wald test. Clinical utility was evaluated using decision curve analysis (DCA) by quantifying net benefit across threshold probabilities for the S-PIV-based prediction model and comparing it with “treat-all” and “treat-none” strategies.23 Missing data were handled using a complete-case approach. Patients with incomplete key variables were excluded during cohort construction before the final analytic dataset was established, as reflected in Figure 1. Therefore, no imputation was performed. Because the final analytic dataset contained complete information for the prespecified variables, formal missing-data pattern testing was not applicable to the final analytic cohort. All analyses were performed using R software (version 4.0.4). A two-sided P value <0.05 was considered statistically significant.
Results
Patient Selection and Incidence of PHLF
A total of 582 consecutive patients who completed conventional laparoscopic hepatectomy for liver tumors were screened. Planned open hepatectomy, conversion from laparoscopic to open surgery, and robotic-assisted hepatectomy were outside the predefined scope of this conventional laparoscopic cohort. After applying the predefined inclusion and exclusion criteria, 356 patients with pathologically confirmed HCC and complete key clinical data were included in the final analytic cohort. During cohort construction, 14 patients were excluded because of incomplete key clinical data, as shown in Figure 1. Among the included patients, 68 (19.1%) developed post-hepatectomy liver failure (PHLF), whereas 288 (80.9%) did not.
Baseline and Perioperative Characteristics
Baseline and perioperative characteristics stratified by PHLF status are summarized in Table 1. Patients who developed PHLF had significantly higher preoperative systemic inflammation indices, including S-PIV (median [IQR] 252.2 [160.7–411.6] vs 156.6 [97.6–263.6], P<0.001) and NLR (median [IQR] 4.3 [3.5–5.7] vs 1.9 [1.5–2.6], P<0.001), whereas PLR did not differ between groups (P=0.786). Hepatic functional reserve was less favorable in the PHLF group, including a higher proportion of ALBI grade 2/3 (85.3% vs 22.9%, P<0.001) and higher ICG-R15 (mean ± SD 12.5±5.7% vs 5.9±2.9%, P<0.001). Regarding tumor burden and operative factors, patients with PHLF had larger tumors (mean ± SD 6.5±2.6 cm vs 4.7±2.2 cm, P<0.001) and more frequently had BCLC stage B disease (80.9% vs 61.1%, P=0.002). Intraoperatively, the PHLF group experienced greater blood loss (mean ± SD 531.4±344.1 mL vs 317.8±178.2 mL, P<0.001) and a markedly higher transfusion rate (39.7% vs 5.2%, P<0.001).
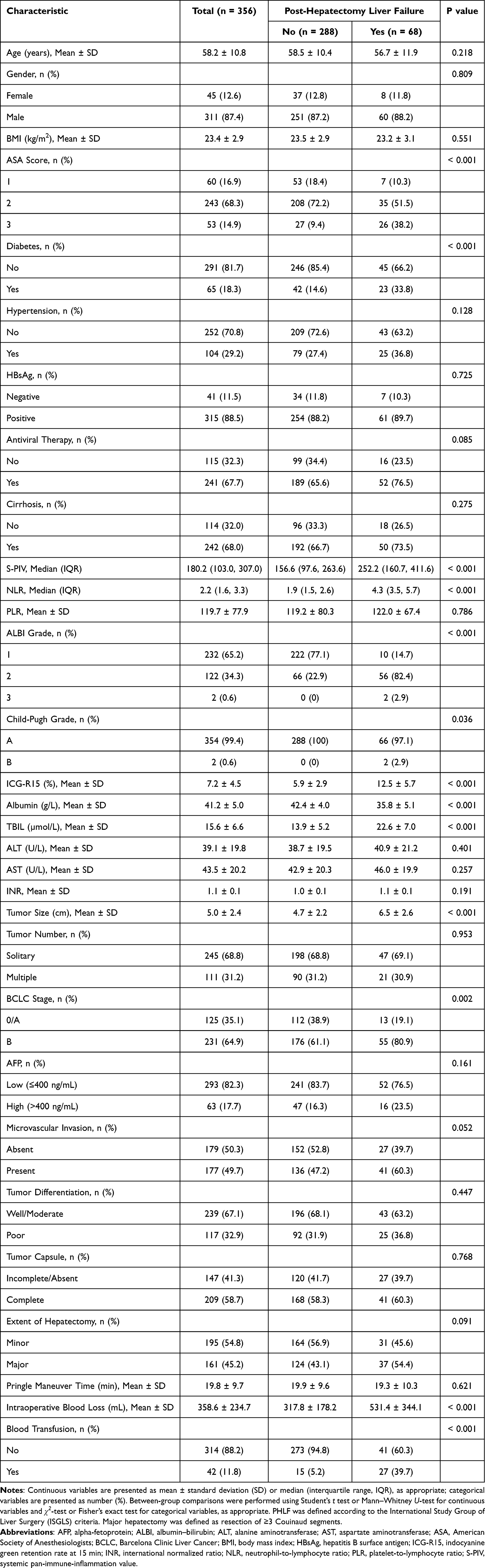 |
Table 1 Baseline and Perioperative Characteristics of Patients Stratified by Post-Hepatectomy Liver Failure (PHLF) |
Discrimination of S-PIV for Predicting PHLF
On receiver operating characteristic (ROC) analysis, preoperative S-PIV demonstrated good discrimination for PHLF, with an AUC of 0.873. The optimal cut-off value determined by the Youden index was 455.4, yielding a sensitivity of 0.726 and specificity of 0.908 (Figure 2). Compared with conventional inflammatory indices, S-PIV showed higher discrimination than NLR (AUC 0.831) and PLR (AUC 0.848) for predicting PHLF (Figure 3).
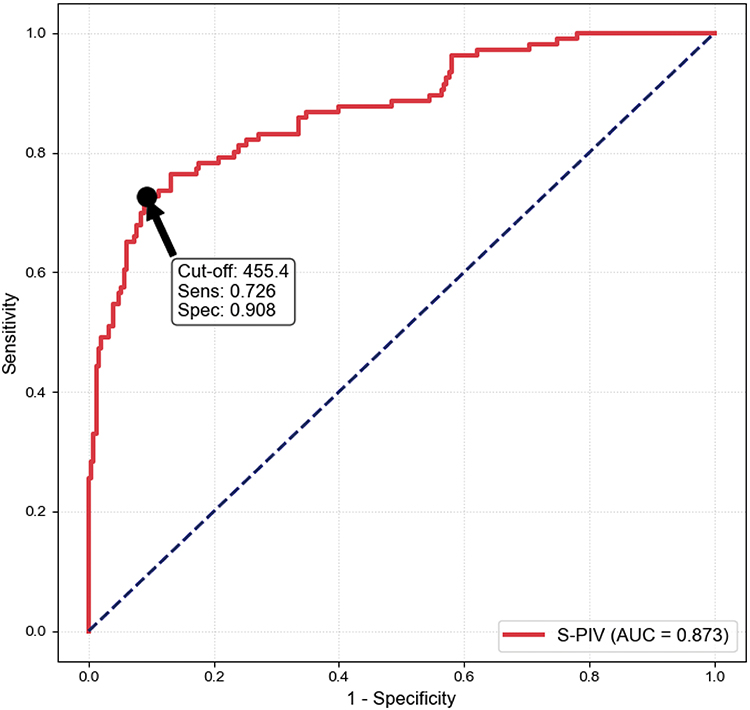 |
Figure 2 Receiver operating characteristic curve of preoperative S-PIV for predicting post-hepatectomy liver failure. The discriminative performance of preoperative systemic pan-immune-inflammation value (S-PIV) for predicting PHLF was evaluated using receiver operating characteristic analysis. The optimal cut-off value was determined using the Youden index and is indicated on the curve. Sensitivity, specificity, and area under the curve are shown in the figure. |
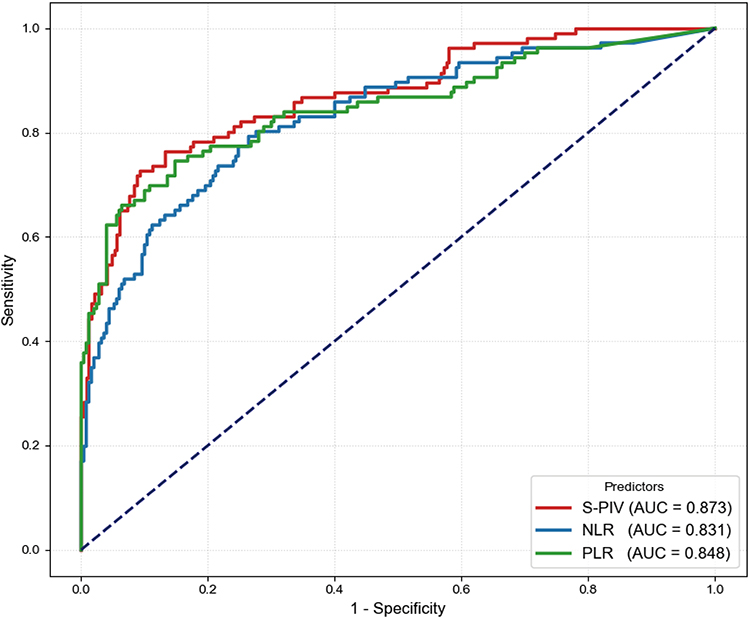 |
Figure 3 Comparison of receiver operating characteristic curves for inflammatory indices. Receiver operating characteristic curves were used to compare the discriminative performance of preoperative systemic pan-immune-inflammation value (S-PIV), neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR) for predicting post-hepatectomy liver failure. Areas under the curve are shown for each inflammatory index. |
Univariable Predictors of PHLF
In univariable logistic regression analysis (Table 2), higher S-PIV was significantly associated with PHLF (per 100 units: OR 1.12, 95% CI 1.06–1.45, P<0.001). Additional factors associated with PHLF included ASA class 3 (OR 7.29, 95% CI 2.81–18.94, P<0.001), diabetes (OR 2.99, 95% CI 1.64–5.45, P<0.001), ALBI grade 2/3 (OR 8.84, 95% CI 3.11–18.96, P<0.001), ICG-R15 (per 1%: OR 1.51, 95% CI 1.36–1.67, P<0.001), tumor size (per 1 cm: OR 1.40, 95% CI 1.23–1.58, P<0.001), and BCLC stage B (OR 2.69, 95% CI 1.41–5.15, P=0.003).
 |
Table 2 Univariable Logistic Regression Analysis for Predictors of Post-Hepatectomy Liver Failure (PHLF) |
Independent Association Between S-PIV and PHLF
In sequentially adjusted models (Table 3), S-PIV remained independently associated with PHLF after adjustment for demographics and comorbidities (Model 1: OR 1.10, 95% CI 1.03–1.57, P<0.001), additional liver functional reserve variables (Model 2: OR 1.08, 95% CI 1.02–1.19, P<0.001), and further tumor and surgical factors, including tumor size, extent of hepatectomy, and blood transfusion (Model 3: OR 1.06, 95% CI 1.03–1.13, P<0.001). ORs are reported per 100-unit increase in S-PIV.
 |
Table 3 Association Between S-PIV and Post-Hepatectomy Liver Failure (PHLF) Across Sequentially Adjusted Logistic Regression Models |
Dose–Response Relationship and Clinical Utility
Restricted cubic spline analysis demonstrated a graded increase in predicted PHLF probability with increasing S-PIV, with no evidence of significant nonlinearity (P for nonlinearity >0.05) (Figure 4). On decision curve analysis, the S-PIV-based prediction model provided greater net benefit than the treat-all and treat-none strategies across threshold probabilities of approximately 10%–70%, supporting its clinical utility for preoperative risk stratification (Figure 5).
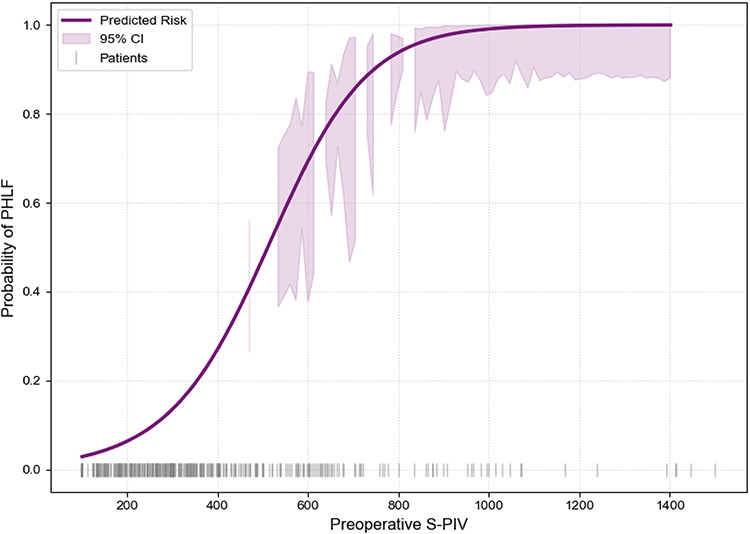 |
Figure 4 Restricted cubic spline analysis of preoperative S-PIV and the probability of post-hepatectomy liver failure. Restricted cubic spline regression was used to evaluate the dose–response relationship between preoperative systemic pan-immune-inflammation value (S-PIV) and the predicted probability of post-hepatectomy liver failure. The spline model used three knots located at the 10th, 50th, and 90th percentiles of S-PIV. The solid line represents the predicted probability, the shaded area represents the 95% confidence interval, and rug marks indicate the distribution of patients. There was no evidence of significant nonlinearity. |
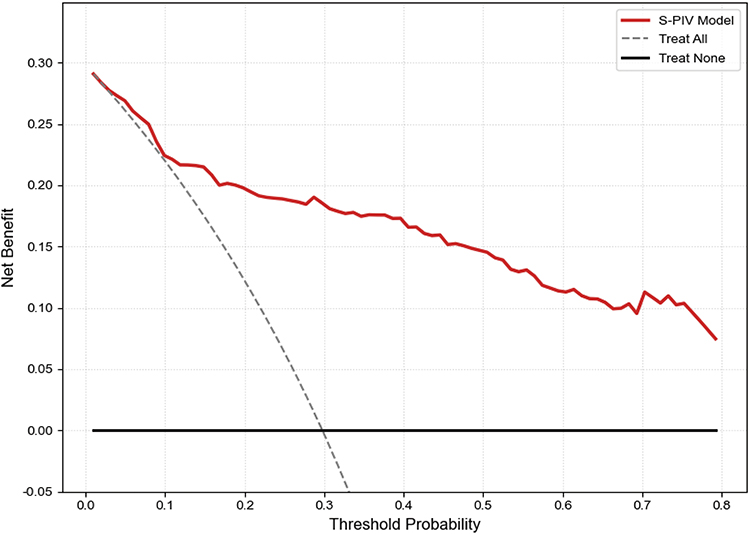 |
Figure 5 Decision curve analysis of the S-PIV-based prediction model for post-hepatectomy liver failure. Decision curve analysis was performed to evaluate the clinical utility of the S-PIV-based prediction model by estimating net benefit across a range of threshold probabilities. The model was compared with treat-all and treat-none strategies. The S-PIV-based model showed higher net benefit across clinically relevant threshold probabilities. |
Discussion
Principal Findings
Post-hepatectomy liver failure (PHLF) remains a major driver of morbidity and mortality after liver resection, and accurate preoperative risk stratification is still challenging despite advances in operative technique and perioperative care.5,6,24–26 In this single-center retrospective cohort of patients undergoing conventional laparoscopic hepatectomy for hepatocellular carcinoma (HCC), we found that the preoperative systemic pan-immune-inflammation value (S-PIV) was strongly associated with PHLF and demonstrated good discrimination. S-PIV remained independently associated with PHLF after sequential adjustment for comorbidity burden, hepatic functional reserve, and tumor/surgical factors, suggesting that it may provide information beyond conventional variables routinely considered during preoperative assessment of HCC candidates for liver resection.2,3,5 The observed dose-response pattern further supports the clinical relevance of S-PIV, as the predicted probability of PHLF increased progressively with higher S-PIV without evidence of significant nonlinearity. In addition, decision curve analysis suggested that the S-PIV-based prediction model may provide net clinical benefit across a range of threshold probabilities.23 Taken together, these findings support S-PIV as a practical adjunctive marker for preoperative risk communication and perioperative planning in patients undergoing laparoscopic hepatectomy for HCC. However, S-PIV should be interpreted as a complementary risk-stratification tool rather than a stand-alone determinant of surgical eligibility.
Interpretation and Biological Plausibility
The association between elevated S-PIV and PHLF is biologically plausible. PHLF reflects an imbalance between the metabolic demands placed on the remnant liver and its capacity for regeneration, synthetic function, and immune-metabolic homeostasis.24–26 Systemic inflammation may aggravate microcirculatory dysfunction, amplify perioperative stress responses, and increase susceptibility to hepatocyte injury, particularly in HCC patients with chronic liver disease and limited functional reserve.5,6,25 S-PIV integrates neutrophils, monocytes, platelets, and lymphocytes into a single composite index. Neutrophil- and monocyte-predominant states may reflect activation of innate inflammatory pathways and cytokine signaling, whereas relative lymphopenia may indicate impaired adaptive immune status or physiological stress. Platelet activation may further contribute to thromboinflammatory activity and microcirculatory disturbance.27 Therefore, a higher S-PIV may reflect a systemic inflammatory and immune-disrupted state in which surgical stress is more likely to be followed by postoperative hepatic dysfunction. This interpretation is consistent with the conceptual framework shown in Figure 6, in which elevated S-PIV may reflect inflammatory activation, relative immune suppression, and microcirculatory disturbance. Nevertheless, this proposed mechanism should be regarded as hypothesis-generating. The present retrospective study was designed to evaluate prediction and association rather than to prove a direct causal pathway between systemic inflammation and PHLF.
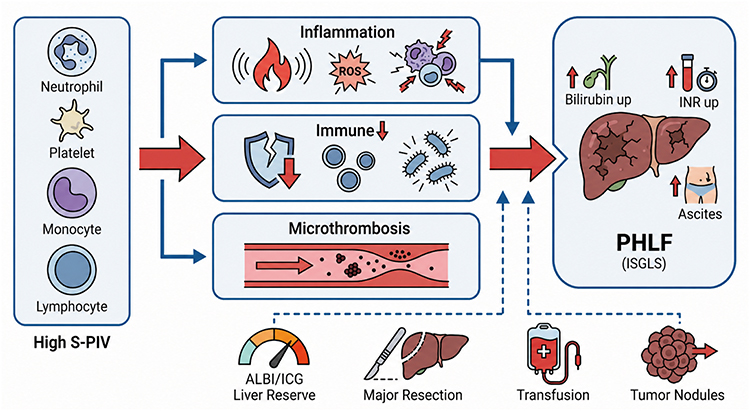 |
Figure 6 Conceptual framework linking elevated S-PIV to post-hepatectomy liver failure. Elevated systemic pan-immune-inflammation value (S-PIV) may reflect a systemic state characterized by inflammatory activation, relative immune suppression, platelet-related thromboinflammatory activity, and potential microcirculatory disturbance. In patients with impaired liver functional reserve, greater tumor burden, larger extent of hepatectomy, or perioperative transfusion, this systemic inflammatory milieu may contribute to postoperative hepatic dysfunction and increase the risk of post-hepatectomy liver failure. This figure illustrates a conceptual framework and does not imply a proven causal pathway. |
Comparison with Existing Prediction Approaches
A variety of approaches have been proposed to predict PHLF, including liver function scores, dynamic liver function tests, imaging-based assessments of future liver remnant volume or function, and models incorporating operative complexity.5,10,16–19,28 These tools have improved the understanding of PHLF risk, but no single metric fully captures the interaction among host inflammatory status, baseline liver reserve, tumor burden, and surgical stress. In HCC patients, this interaction is particularly important because underlying chronic liver disease, cirrhosis, and variable hepatic reserve may modify the response to liver resection.5,29,30
Current prediction models for PHLF often emphasize hepatic reserve and operative variables.28 However, some models require specialized measurements, complex calculations, or intraoperative parameters that may not be available at the time of early preoperative counseling.16–19,31 In contrast, S-PIV is derived from routine preoperative blood counts and can be obtained before surgery without additional cost or specialized testing. This feature makes it potentially useful as an early “host-inflammation layer” that complements established liver reserve assessments such as ALBI grade and ICG-R15, rather than replacing them.7–10,29,30
The present findings are also consistent with growing interest in inflammatory indices for perioperative risk prediction in HCC.10,11,32 Our study extends this line of research by focusing on S-PIV, a broader immune-inflammation composite incorporating neutrophils, monocytes, platelets, and lymphocytes, and by evaluating its association with PHLF using discrimination analysis, multivariable adjustment, restricted cubic splines, and decision curve analysis.
Clinical Implications for Perioperative Decision-Making
From a clinical perspective, S-PIV may be useful because it is simple, inexpensive, and available before surgery. In routine HCC surgical pathways, an elevated S-PIV could help clinicians identify patients who may benefit from more detailed risk discussion, closer perioperative monitoring, and individualized optimization before laparoscopic hepatectomy. The decision curve analysis further suggests that an S-PIV-based prediction approach may have practical value across clinically relevant risk thresholds, where different clinicians or institutions may adopt different action thresholds depending on liver reserve, planned extent of hepatectomy, and available perioperative resources.23
Importantly, S-PIV should not be used in isolation to approve or deny surgery. Instead, it may be incorporated into a broader assessment that includes liver functional reserve, tumor burden, operative complexity, comorbidities, and the expected future liver remnant.5,33 For patients considered to be at higher risk, S-PIV may help prompt multidisciplinary discussion and perioperative risk-mitigation strategies, including careful evaluation of liver reserve, optimization of comorbidities, nutritional support when indicated, blood conservation strategies, and enhanced postoperative surveillance.21,22,34
Although detailed nutritional status, sarcopenia, and alcohol/tobacco exposure were not consistently documented in the present retrospective cohort, these factors remain clinically relevant to perioperative risk assessment.21,34,35 In future prospective studies, systematic assessment of nutritional status, body composition, functional capacity, and lifestyle exposures should be incorporated to determine whether S-PIV provides incremental value beyond these established or emerging risk factors.
Strengths, Limitations, and Future Directions
Several strengths of this study deserve emphasis. First, S-PIV is derived from routine preoperative blood counts and can be calculated easily without additional testing, supporting its feasibility for real-world preoperative assessment. Second, the study focused on a clinically homogeneous population of patients undergoing conventional laparoscopic hepatectomy for HCC, which reduced heterogeneity related to surgical approach. Third, PHLF was defined using the International Study Group of Liver Surgery criteria,4 and diagnosis and grading were confirmed by experienced hepatobiliary surgeons. Fourth, we evaluated not only discrimination but also dose-response and clinical utility, which provides a more comprehensive assessment of the potential value of S-PIV as a prediction marker.23
Several limitations should also be acknowledged. First, this was a retrospective, single-center study. Although the cohort was clinically focused, center-specific surgical expertise, perioperative management, patient selection, and laboratory practice may limit generalizability. In addition, because planned open hepatectomy, conversion from laparoscopic to open surgery, and robotic-assisted hepatectomy were outside the predefined scope of this conventional laparoscopic cohort, the findings should not be directly extrapolated to open, converted, or robotic liver resections without further validation. Second, the study used a complete-case approach. Patients with incomplete key variables were excluded during cohort construction before establishment of the final analytic dataset. Although only a small number of patients were excluded because of incomplete key clinical data, complete-case analysis may introduce selection bias if the missingness mechanism is not completely random. Because the final analytic cohort contained complete information for the prespecified variables, formal missing-data pattern testing was not applicable to the final analytic dataset. Future prospective studies should prespecify core variables, minimize missingness, and evaluate missing-data mechanisms more rigorously. Third, several clinically relevant factors were not fully evaluated. Detailed nutritional status, sarcopenia, alcohol exposure, and tobacco exposure were not systematically and consistently documented across the entire retrospective study period and therefore were not included in the primary multivariable models. Their omission may have resulted in residual confounding. Future studies should incorporate standardized nutritional assessment, body composition analysis, functional status evaluation, and lifestyle exposure data to clarify whether S-PIV remains independently predictive after adjustment for these factors.21,34,35 Fourth, the S-PIV cut-off was derived from ROC optimization in the present cohort and may not be directly transferable to other populations. Differences in HCC etiology, cirrhosis severity, surgical strategy, perioperative care, and laboratory platforms may affect the optimal threshold and model calibration. Therefore, external multicenter validation and calibration are urgently required before S-PIV can be recommended for routine clinical implementation.20,28 Future work should also evaluate calibration performance, decision-analytic benefit, and incremental value over established liver reserve assessments in independent cohorts. Finally, this study evaluated association and prediction rather than causality. Although the biological rationale linking systemic inflammation, immune dysregulation, microcirculatory disturbance, and PHLF is plausible, mechanistic studies are needed to clarify whether modulation of systemic inflammation can reduce PHLF risk. Combining S-PIV with objective measures of remnant liver volume or function, fibrosis burden, nutritional status, and imaging-based body composition may further improve individualized risk stratification.31,33,35
Conclusion
In this single-center retrospective cohort of patients undergoing conventional laparoscopic hepatectomy for HCC, preoperative S-PIV demonstrated strong discrimination for PHLF and remained independently associated with PHLF after sequential adjustment for comorbidities, hepatic functional reserve, and tumor/operative factors. The graded dose–response pattern and favorable decision-analytic profile suggest that S-PIV may function as a practical adjunct to established preoperative assessments for risk communication and perioperative planning, rather than as a stand-alone criterion for surgical decision-making. These findings should be interpreted in the context of the study’s retrospective, single-center design, complete-case analysis, and predefined laparoscopic cohort scope. External multicenter validation and calibration are urgently required before routine clinical implementation.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy considerations and institutional restrictions. Data are available from the corresponding author upon reasonable request and with permission of the relevant institution.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of The Affiliated Jiangning Hospital of Nanjing Medical University (IRB No. 2026-03-026-K01). Owing to the retrospective design of the study, the requirement for written informed consent was waived by the IRB.
Author Contributions
Xiuyu Wu: Investigation, Data curation, Writing – original draft. Shun Xu: Data curation, Formal analysis, Methodology, Writing – original draft. Tianqi Zhang: Data curation, Formal analysis, Methodology, Writing – review & editing. Ying Xing: Data curation, Investigation, Writing – review & editing. Xia Min: Data curation, Investigation, Writing – review & editing. Jingjing Wu: Data curation, Validation, Writing – review & editing. Qian Mao: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Nanjing Medical University Science and Technology Development Fund (NMUB20230112). The funder had no role in study design, data collection, analysis, interpretation, article preparation, or the decision to submit for publication.
Disclosure
The authors declare that they have no competing interests relation to this study.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–18. doi:10.3322/caac.21660
2. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
3. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
4. Rahbari NN, Garden OJ, Padbury R, et al. Posthepatectomy liver failure: a definition and grading by the international study group of liver surgery (ISGLS). Surgery. 2011;149(5):713–724. doi:10.1016/j.surg.2010.10.001
5. Nishio T, Taura K, Koyama Y, Ishii T, Hatano E. Current status of preoperative risk assessment for posthepatectomy liver failure in patients with hepatocellular carcinoma. Ann Gastroenterol Surg. 2023;7(6):871–886. doi:10.1002/ags3.12692
6. Sparrelid E, Olthof PB, Dasari BVM, et al. Current evidence on posthepatectomy liver failure: comprehensive review. BJS Open. 2022;6(6):zrac142. doi:10.1093/bjsopen/zrac142
7. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
8. Zhang ZQ, Xiong L, Zhou JJ, et al. Ability of the ALBI grade to predict posthepatectomy liver failure and long-term survival after liver resection for different BCLC stages of HCC. World J Surg Oncol. 2018;16(1):208. doi:10.1186/s12957-018-1517-0
9. Guo G, Lei Z, Tang X, et al. External validation of six liver functional reserve models to predict posthepatectomy liver failure after major resection for hepatocellular carcinoma. J Cancer. 2021;12(17):5260–5267. doi:10.7150/jca.58726
10. Fang T, Long G, Wang D, et al. A nomogram based on preoperative inflammatory indices and ICG-R15 for prediction of liver failure after hepatectomy in HCC patients. Front Oncol. 2021;11:667496. doi:10.3389/fonc.2021.667496
11. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
12. Fuca G, Guarini V, Antoniotti C, et al. The pan-immune-inflammation value is a new prognostic biomarker in metastatic colorectal cancer: results from a pooled-analysis of the Valentino and TRIBE first-line trials. Br J Cancer. 2020;123(3):403–409. doi:10.1038/s41416-020-0894-7
13. Guven DC, Sahin TK, Erul E, Kilickap S, Gambichler T, Aksoy S. The association between the pan-immune-inflammation value and cancer prognosis: a systematic review and meta-analysis. Cancers. 2022;14(11):2675. doi:10.3390/cancers14112675
14. Li Y, Mei Y, Zhao J, et al. Cohort profile: precision environmental health cohort of healthy undergraduates. Phenomics. 2025;5(3):301–310. doi:10.1007/s43657-024-00215-4
15. Chen LL, Zhai WJ, Bao J, et al. Efficacy and safety of Jinhua Qinggan granule, a compound Chinese herbal medicine, in oldest-old patients with COVID-19: a retrospective cohort study. J Integr Med. 2025. doi:10.1016/j.joim.2025.10.005
16. Lei Z, Cheng N, Si A, et al. A novel nomogram for predicting postoperative liver failure after major hepatectomy for hepatocellular carcinoma. Front Oncol. 2022;12:817895. doi:10.3389/fonc.2022.817895
17. Lin S, Song Z, Peng H, et al. A novel nomogram based on preoperative parameters to predict posthepatectomy liver failure in patients with hepatocellular carcinoma. Surgery. 2023;174(4):865–873. doi:10.1016/j.surg.2023.06.025
18. Santol J, Kim S, Gregory LA, et al. An APRI+ALBI-based multivariable model as a preoperative predictor for posthepatectomy liver failure. Ann Surg. 2025;281(5):861–871. doi:10.1097/SLA.0000000000006127
19. Zhang D, Pan Y, Yang Z, et al. A nomogram based on preoperative lab tests, BMI, ICG-R15, and EHBF for the prediction of post-hepatectomy liver failure in patients with hepatocellular carcinoma. J Clin Med. 2023;12(1):324. doi:10.3390/jcm12010324
20. Moons KGM, Wolff RF, Riley RD, et al. PROBAST: a tool to assess risk of bias and applicability of prediction model studies: explanation and elaboration. Ann Intern Med. 2019;170(1):W1–W33. doi:10.7326/M18-1377
21. Joliat GR, Kobayashi K, Hasegawa K, et al. Guidelines for perioperative care for liver surgery: enhanced recovery after surgery (ERAS) society recommendations 2022. World J Surg. 2023;47(1):11–34. doi:10.1007/s00268-022-06732-5
22. Delabays C, Demartines N, Joliat GR, Melloul E. Enhanced recovery after liver surgery in cirrhotic patients: a systematic review and meta-analysis. Perioper Med. 2024;13(1):24. doi:10.1186/s13741-024-00375-x
23. Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006;26(6):565–574. doi:10.1177/0272989X06295361
24. Soreide JA, Deshpande R. Post hepatectomy liver failure (PHLF)-recent advances in prevention and clinical management. Eur J Surg Oncol. 2021;47(2):216–224. doi:10.1016/j.ejso.2020.09.001
25. Bekheit M, Grundy L, Salih AK, et al. Post-hepatectomy liver failure: a timeline centered review. Hepatobiliary Pancreat Dis Int. 2023;22(6):554–569. doi:10.1016/j.hbpd.2023.03.001
26. Merath K, Tiwari A, Court C, et al. Postoperative liver failure: definitions, risk factors, prediction models and prevention strategies. J Gastrointest Surg. 2023;27(11):2640–2649. doi:10.1007/s11605-023-05834-2
27. Starlinger P, Ubl DS, Hackl H, et al. Combined APRI/ALBI score to predict mortality after hepatic resection. BJS Open. 2021;5(1):zraa043. doi:10.1093/bjsopen/zraa043
28. Yoshino K, Yoh T, Taura K, Seo S, Ciria R, Briceno-Delgado J. A systematic review of prediction models for post-hepatectomy liver failure in patients undergoing liver surgery. HPB. 2021;23(9):1311–1320. doi:10.1016/j.hpb.2021.05.002
29. Marasco G, Alemanni LV, Colecchia A, et al. Prognostic value of the albumin-bilirubin grade for the prediction of post-hepatectomy liver failure: a systematic review and meta-analysis. J Clin Med. 2021;10(9):2011. doi:10.3390/jcm10092011
30. Wang YY, Zhong JH, Su ZY, et al. Albumin-bilirubin versus Child-Pugh score as a predictor of outcome after liver resection for hepatocellular carcinoma. Br J Surg. 2016;103(6):725–734. doi:10.1002/bjs.10095
31. Luo N, Huang X, Ji Y, et al. A functional liver imaging score for preoperative prediction of liver failure after hepatocellular carcinoma resection. Eur Radiol. 2022;32(8):5623–5632. doi:10.1007/s00330-022-08656-z
32. Silva JPM, Coelho FF, Cassenote AJF, et al. Preoperative inflammatory markers as prognostic predictors after hepatocellular carcinoma resection: data from a western referral center. BMC Surg. 2022;22(1):329. doi:10.1186/s12893-022-01764-1
33. Chansangrat J, Keeratibharat N. Portal vein embolization: rationale, techniques, outcomes and novel strategies. Hepatol Oncol. 2021;8(4):HEP42. doi:10.2217/hep-2021-0006
34. Hao S, Reis HL, Quinn AW, Snyder RA, Parikh AA. Prehabilitation for older adults undergoing liver resection: getting patients and surgeons up to speed. J Am Med Dir Assoc. 2022;23(4):547–554. doi:10.1016/j.jamda.2022.01.077
35. Higashi T, Hayashi H, Taki K, et al. Sarcopenia, but not visceral fat amount, is a risk factor of postoperative complications after major hepatectomy. Int J Clin Oncol. 2016;21(2):310–319. doi:10.1007/s10147-015-0898-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Indocyanine Green Retention Test as a Predictor of Postoperative Complications in Patients with Hepatitis B Virus-Related Hepatocellular Carcinoma
Mai RY, Bai T, Luo XL, Wu GB
Therapeutics and Clinical Risk Management 2022, 18:761-772
Published Date: 2 August 2022
Laparoscopic Hepatectomy versus Open Hepatectomy After Conversion Therapy Using Transarterial Chemoembolization or Hepatic Arterial Infusion Chemotherapy for Patients with Initially Unresectable Hepatocellular Carcinoma
Yang Z, Hu Z, Fu Y, Hu D, Zhou Z, Chen M, Pan Y, Zhang Y
Journal of Hepatocellular Carcinoma 2023, 10:1157-1167
Published Date: 21 July 2023
Predicting Postoperative Pneumonia in ESCC After Neoadjuvant Chemo-Immunotherapy: Combined Use of ARISCAT Score and Inflammatory Biomarkers
Ding J, Zhao J, Qin T, Liu C, Yang Y, Xu D, Chen Y, Xu Z
Journal of Inflammation Research 2025, 18:12855-12868
Published Date: 16 September 2025
Development and Validation of an Interpretable Machine Learning Model Based on Peripheral Blood Biomarkers for Esophageal Cancer Risk Prediction
Wang Q, Shen L, Qiu W, Shi Q, Zhang Y, Shen K, Zhang J, Qiu H
International Journal of General Medicine 2026, 19:617852
Published Date: 26 June 2026