Back to Journals » International Journal of General Medicine » Volume 19
Predicting Post-Craniotomy Intracranial Infection Using Perioperative and Early Postoperative Variables: A Retrospective Machine Learning Study
Authors Zhong Z, Zhang L, Yu P, Xu B
Received 14 January 2026
Accepted for publication 14 April 2026
Published 1 May 2026 Volume 2026:19 596122
DOI https://doi.org/10.2147/IJGM.S596122
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Zian Zhong,* Liangjin Zhang,* Ping Yu, Bing Xu
Department of Neurology, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, Xiangyang, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ping Yu; Bing Xu, Email [email protected]; [email protected]
Objective: To identify perioperative clinical and surgical variables associated with intracranial infection (ICI) after craniotomy, and establish an accurate machine learning prediction model for clinical risk stratification and early intervention.
Methods: A retrospective study included 419 patients who underwent craniotomy surgery at Xiangyang Central Hospital from May 2017 to April 2024. Perioperative variables were collected. Univariate and multivariate logistic regression were used to screen for risk factors. Four models (LR, RF, XGBoost, LightGBM) were constructed and validated through AUC, sensitivity, specificity, PPV, NPV, calibration curve, and DCA were used to evaluate the performance.
Results: 53 patients (12.6%) developed ICI. Independent risk factors included prolonged surgical time, significant intraoperative bleeding, postoperative cerebrospinal fluid leakage, multiple surgeries (≥ 2), and frequent cerebrospinal fluid sampling/drug injection through drainage tubes. LightGBM achieved the best performance: training set AUC 0.873 (95% CI 0.819– 0.927), test set AUC 0.811 (95% CI 0.758– 0.924), sensitivity 81.0%, specificity 79.3%, PPV 38.6%, NPV 95.7%. Good calibration and high clinical practicality were confirmed.
Conclusion: Machine learning models, especially LightGBM, can effectively predict postoperative ICI. The identified risk factors and best models support personalized risk assessment and clinical prevention.
Keywords: craniotomy, intracranial infection, machine learning, perioperative variables, predictive model
Introduction
Intracranial infection (ICI) is a severe postoperative complication following craniotomy, encompassing meningitis, ventriculitis, brain abscess, and other illnesses posing significant threats to patient prognosis.1,2 Clinical studies indicate that the incidence of postoperative ICI ranges from 4.6% to 25% in domestic populations and from 1% to 10% in international populations, with an attributable mortality of 24% to 43%.2–4 The high incidence and mortality rates of ICI are closely linked to its nonspecific early clinical manifestations and the limitations of diagnostic methods. The diagnostic gold standard for ICI involves detecting pathogenic bacteria through postoperative cerebrospinal fluid (CSF) culture; however, the low positive rate of this method frequently leads to delayed diagnosis and treatment.5
In addition, the blood-brain barrier poses a significant challenge to antibiotic treatment, as most antibiotics struggle to reach effective concentrations in CSF.6–8 This limitation, coupled with the lack of timely pathogenic evidence for drug susceptibility testing, makes the selection of anti-infective drugs extremely difficult. Therefore, identifying high-risk patients and implementing targeted preventive measures before infection occurs is crucial for reducing the incidence of postoperative ICI and improving patient prognosis. Traditional prediction methods based on logistic regression have been widely used, but they may not fully capture the complex nonlinear relationship between multiple perioperative variables and ICI risk.
Machine learning algorithms possess the capability to handle high-dimensional data and discern concealed patterns, exhibiting significant potential in medical predictive research.9,10 In comparison to conventional statistical models, machine learning techniques, including random forest, XGBoost, and LightGBM, excel in integrating numerous clinical and surgical variables, thereby enhancing prediction accuracy. This retrospective study aims to employ perioperative clinical and surgical variables to construct and compare multiple machine learning models alongside logistic regression models for predicting postoperative ICI. The ultimate objective is to furnish clinical practice with dependable and pragmatic predictive tools, while investigating crucial risk factors linked to postoperative ICI.
Methods
Study Population
As a retrospective study, we enrolled patients who underwent craniotomy at Xiangyang Central Hospital between May 2017 and April 2024. The inclusion criteria were as follows: patients who underwent craniotomy performed by doctors with associate senior professional titles or above; complete clinical data. Exclusion criteria included: preoperative diagnosis of ICI; severe functional impairment of major organs such as the heart, lungs, liver, and kidneys; incomplete treatment due to various reasons, including discharge against medical advice, transfer to another hospital, abandonment of treatment, or death; and active infections in other parts of the body before surgery. The process of patient enrollment and prediction model construction is illustrated in Figure 1.
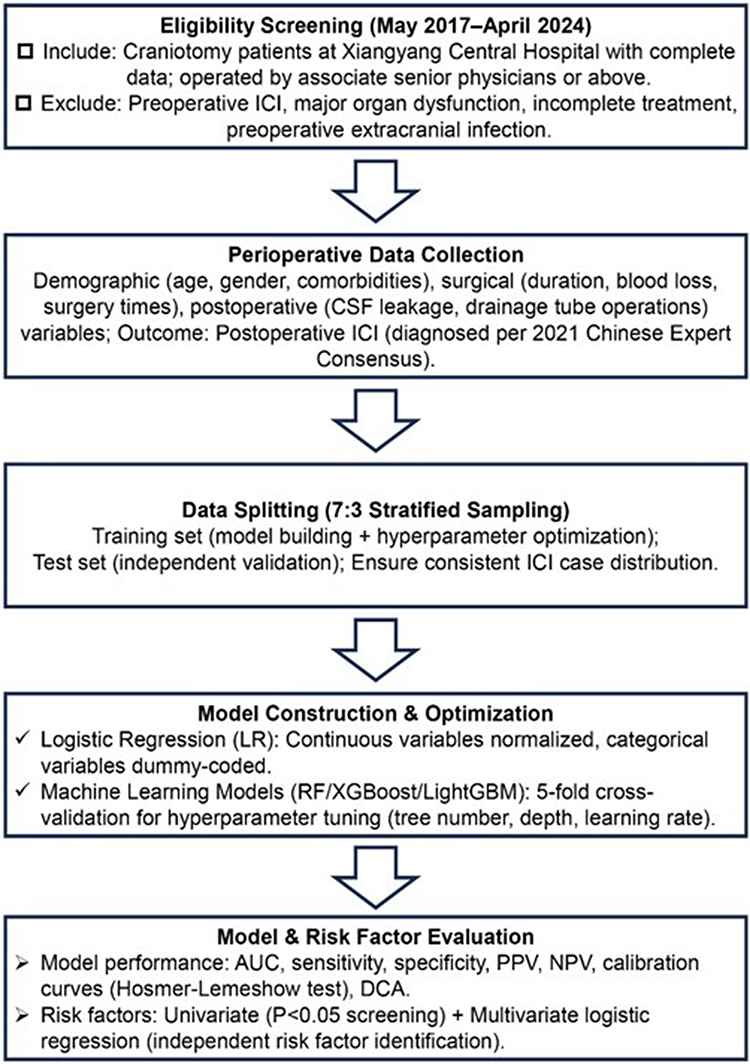 |
Figure 1 Flowchart of Study Design and Predictive Model Development for Postoperative Intracranial Infection Risk Assessment. Note: The bold black text serves as the subtitle for each section. |
Ethical Statement
This retrospective study was approved by the Ethics Committee of Xiangyang Central Hospital affiliated with Hubei University of Arts and Sciences in accordance with institutional ethical guidelines. This study was conducted in accordance with the principles of the Helsinki Declaration and relevant national ethical guidelines for medical research involving human subjects. As this is a retrospective analysis using existing electronic medical records, the ethics committee has waived the requirement for individual patients to provide written informed consent, provided that all patient data is completely anonymous to protect privacy. Prior to data analysis, identifiable information such as name, medical record number, and contact information has been deleted or encrypted to ensure confidentiality. All procedures are conducted in accordance with regulatory requirements and institutional policies regarding the use of human research data.
Data Collection
Perioperative clinical and surgical variables were collected from electronic medical records, including: (1) demographic and baseline characteristics: age, gender, hypertension, diabetes, long-term preoperative use of glucocorticoid, preoperative radiotherapy and chemotherapy, preoperative Glasgow Coma Scale (GCS), preoperative diagnosis, and open brain injury;11 (2) Surgical related variables: surgical timing (emergency or elective), surgical grade, surgical incision classification, surgical site (supratentorial, infratentorial, or combined), surgical duration (minutes), intraoperative blood loss (mL), presence of intracranial implants, and number of craniotomy attempts (≥ 2 or<2); (3) Postoperative variables: indwelling drainage tube, postoperative cerebrospinal fluid leakage, frequent collection of cerebrospinal fluid or injection of drugs through drainage tube (≥ 3 times within 24 hours of indwelling drainage tube), prolonged bed rest time after surgery; (4) Outcome variable: incidence of postoperative ICI. All included patients have complete clinical and surgical data, and there are no missing or incomplete data in the study dataset. We carefully reviewed the electronic medical records of all included patients and confirmed that all variables, such as cerebrospinal fluid leakage, drainage tube operation, and prolonged bed rest, were recorded as clinical events that occurred prior to the diagnosis of intracranial infection.
Diagnosis of Postoperative ICI
The diagnosis of postoperative ICI is based on the 2021 edition of the “Expert Consensus on Diagnosis and Treatment of Central Nervous System Infections in Chinese Neurosurgery”. If the first four criteria are met, clinical diagnosis is made, and if the fifth criterion is met, etiological confirmation is performed. All ICI diagnoses are jointly confirmed by at least two chief physicians from the diagnostic and treatment team of the department: (1) Clinical manifestations: systemic inflammatory response (body temperature >38°C or 90 beats/minute, respiratory rate >20 beats/minute), changes in consciousness (drowsiness, coma, blurred consciousness or coma), signs of elevated intracranial pressure (headache, nausea and vomiting, papillary edema), meningeal irritation symptoms (neck stiffness, positive Kernighan and Brudzinski signs); (2) Blood routine: White blood cell count >10.0 × 109/L, neutrophil ratio >0.8; (3) Lumbar puncture: intracranial pressure >200mm H2O, cloudy, yellow or purulent cerebrospinal fluid, total white blood cell count >100 × 106/L, neutrophil ratio >0.7, cerebrospinal fluid glucose <2.2 mmol/L, cerebrospinal fluid glucose/serum glucose <0.4; (4) Imaging findings: Early ICI patients have no specific signs on cranial CT or MRI; if it develops into a brain abscess in the later stage, typical brain ring enhancement will appear on enhanced CT or MRI; (5) Pathogenic examination: Positive cerebrospinal fluid culture (excluding specimen contamination) is the gold standard. It should be clarified that the intracranial infections included in this study include meningitis, ventriculitis, brain abscess, and other central nervous system infections related to craniotomy, not limited to meningitis.
Model Construction and Validation
Using stratified sampling, the dataset was randomly divided into training and testing sets at a 7:3 ratio to ensure consistent distribution of ICI cases in both groups. Four prediction models were constructed: logistic regression (LR), random forest (RF), extreme gradient boosting (XGBoost), and LightGBM. Prior to model construction, detailed data preprocessing steps were carried out, including normalization of continuous variables, conversion of categorical variables into dummy variables, and detection and handling of outliers using the interquartile range method. For the LR model, continuous variables were normalized and categorical variables were converted into dummy variables. For machine learning models (RF, XGBoost, LightGBM), 5-fold cross-validation was employed in the training set for hyperparameter optimization.12 The key hyperparameters for optimization included the number of decision trees, maximum tree depth, learning rate, and minimum sample size for each leaf node.
Statistical Analysis
All statistical analyses were conducted using R software (version 4.2.0). Continuous variables following a normal distribution are described as mean ± standard deviation (x ± s) and compared using the independent sample t-test. Continuous variables not conforming to a normal distribution are described as median and interquartile range [M (Q1-Q3)] and compared using the Mann–Whitney U-test. Categorical variables are described as counts and percentages [n (%)], and comparisons are made using chi-square tests or Fisher’s exact tests where appropriate.
Univariate analysis was used to screen variables related to postoperative ICI (P<0.05). Multiple logistic regression analysis was performed to identify independent risk factors. The performance of predictive models was evaluated using AUC, sensitivity, specificity, PPV, NPV, and F1 scores. The calibration curve was used to assess the consistency between predicted and actual ICI rates, and the Hosmer-Lemeshow test was employed for calibration evaluation. Discrimination capability analysis (DCA) was conducted to evaluate the clinical utility of the model by calculating net benefits at different threshold probabilities. P<0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
This study enrolled a total of 419 patients, with 53 (12.6%) experiencing postoperative ICI. The training set comprised 293 patients (including 40 ICI patients), while the testing set consisted of 126 patients (13 ICI patients). As illustrated in Table 1, no significant differences were observed between the ICI and non-ICI groups in demographic characteristics such as age, gender, and the presence of hypertension or diabetes (all P>0.05). However, notable disparities were found in surgical-related variables (surgery duration, intraoperative blood loss, and number of surgeries) and postoperative factors (cerebrospinal fluid leakage, frequent cerebrospinal fluid sampling, drug injection via drainage tubes, and prolonged bed rest) between the two groups (all P<0.05). This section identifies baseline imbalances in key clinical variables between the infected and non-infected groups, paving the way for subsequent risk factor analysis and model development.
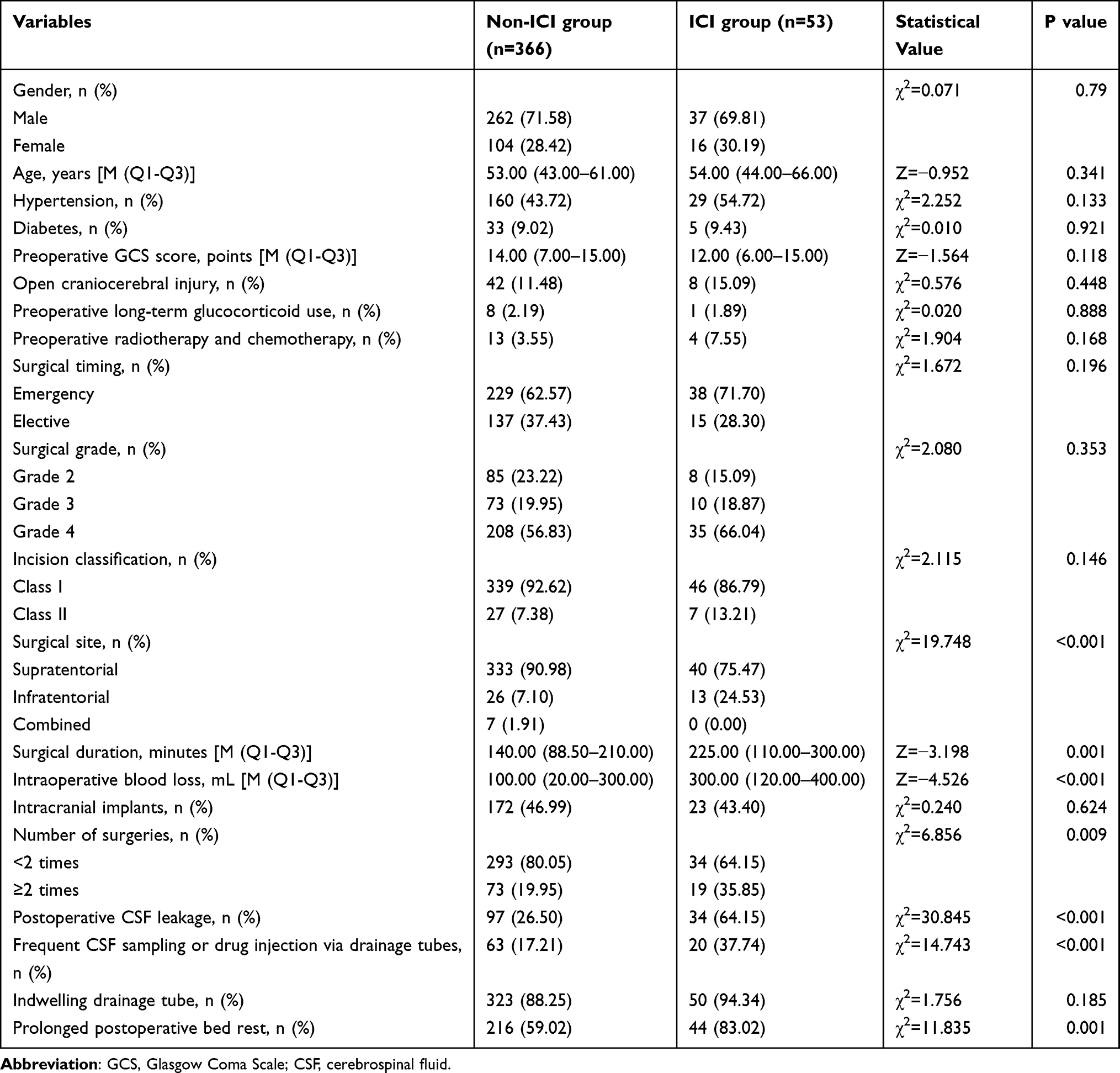 |
Table 1 Baseline Characteristics of the Study Population Stratified by Postoperative Intracranial Infection (ICI) Status |
Univariate and Multivariate Analysis of Risk Factors for Postoperative ICI
Univariate analysis revealed that factors such as surgical duration, intraoperative blood loss, surgical site, number of surgeries, postoperative cerebrospinal fluid leakage, frequent cerebrospinal fluid sampling or drug injection via drainage tubes, and prolonged postoperative bed rest time were significantly correlated with postoperative ICI (all P<0.05), as detailed in Table 2. Following adjustment for potential confounding factors, multivariate logistic regression analysis indicated that prolonged surgical duration (odds ratio [OR]=1.004, 95% CI: 1.000–1.009, P=0.045), significant intraoperative blood loss (OR=1.002, 95% CI: 1.000–1.003, P=0.038), postoperative cerebrospinal fluid leakage (OR=5.004, 95% CI: 2.570–9.744, P<0.001), surgical frequency ≥ 2 (OR=2.452, 95% CI=1.197–5.021, P=0.014), and frequent cerebrospinal fluid sampling or drug injection via drainage tubes (OR=3.941, 95% CI: 1.836–8.460, P<0.001) were identified as independent risk factors for postoperative ICI. These findings elucidate the key determinants of ICI following craniotomy and offer a significant theoretical foundation for targeted preventive measures.
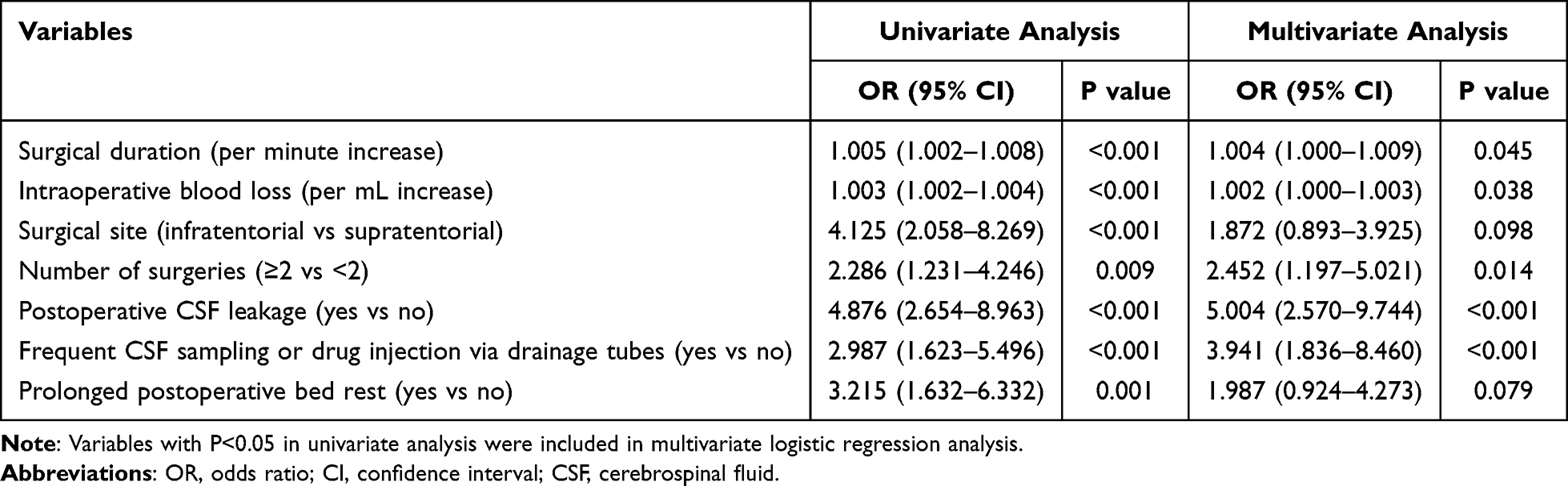 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Risk Factors for Postoperative Intracranial Infection |
Performance Comparison of Predictive Models
As shown in Table 3, the performance of four prediction models in the training and testing sets is summarized. In the training set, the LightGBM model had the highest AUC of 0.873 (95% CI: 0.819–0.927), followed by the XGBoost model (AUC=0.856, 95% CI: 0.798–0.914), RF model (AUC=0.832, 95% CI: 0.771–0.893), and LR model (AUC: 0.826, 95% CI: 0.768–0.884). In the test set, the LightGBM model still maintained the best performance with an AUC of 0.841 (95% CI: 0.758–0.924), higher than the XGBoost model (AUC=0.815, 95% CI: 0.723–0.907), RF model (AUC=0.798, 95% CI=0.701–0.895), and LR model (AUC: 0.789, 95% CI: 0.690–0.888). As shown in Figure 2, the ROC curve of the LightGBM model is consistently higher than the other three models in the two groups. In addition, the LightGBM model showed the highest sensitivity (81.0%) and specificity (79.3%) in the test set, as well as good PPV (38.6%) and NPV (95.7%). To further validate the superiority of the LightGBM model, we used the DeLong test to compare the AUC differences between LightGBM and three other models (XGBoost, RF, LR) in the training and testing sets. The statistical results show that the AUC of the LightGBM model is significantly higher than the other three models (P<0.05), which provides statistical support for the conclusion that the LightGBM model has the best predictive performance. These findings indicate that machine learning models, especially LightGBM models, have superior predictive capabilities compared to traditional LR models, highlighting the value of integrating complex nonlinear relationships between variables.
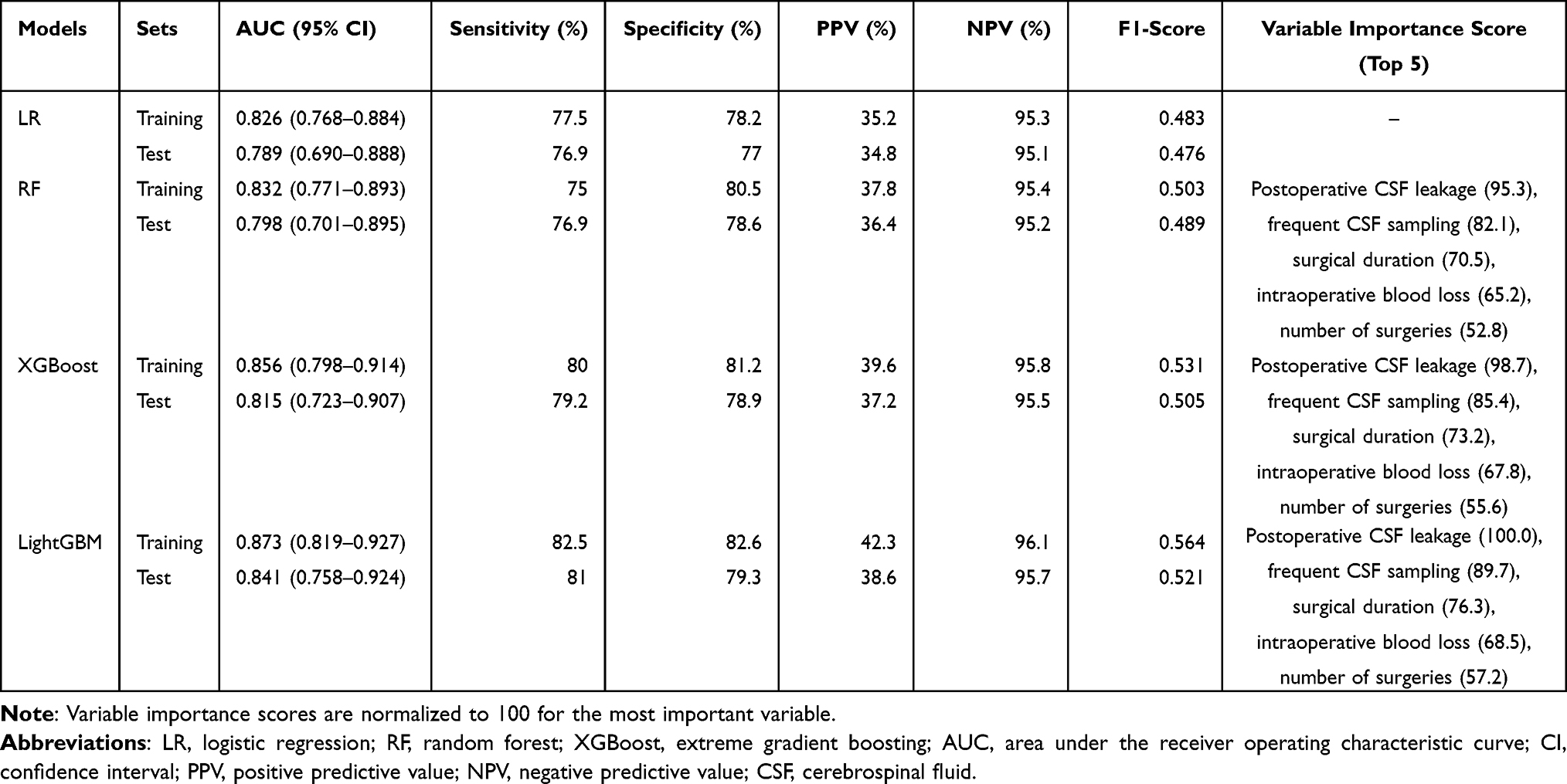 |
Table 3 Performance of Predictive Models in the Training and Test Sets |
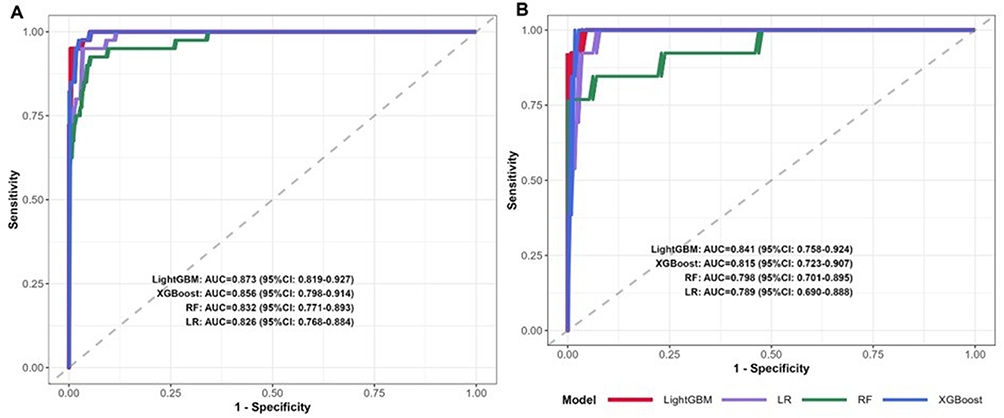 |
Figure 2 Receiver operating characteristic (ROC) curves of four predictive models for postoperative intracranial infection (ICI). Notes: ROC curves of logistic regression (LR), random forest (RF), XGBoost, and LightGBM models in the training set (A) and test set (B). The LightGBM model exhibits the highest area under the ROC curve (AUC) in both sets, indicating superior discriminative ability compared to the other three models. |
Calibration and Clinical Utility of the Optimal Model
As shown in Figure 3, the calibration curve of the LightGBM model demonstrates remarkable consistency between the predicted ICI rate and the actual observed rates in both the training and testing sets. The Hosmer-Lemeshow test result for the LightGBM model yields χ2=8.763 with P=0.363, indicating no significant difference between the predicted and actual values, thus confirming the model’s excellent calibration. DCA (refer to Figure 4) reveals that, across a broad threshold probability range (0–0.90), the LightGBM model offers superior net benefits compared to the “treat all” and “no treat” strategies. Specifically, within the threshold probability range of 0.10 to 0.80, the net benefit of the LightGBM model significantly surpasses that of the other three models, highlighting its strong clinical applicability in guiding decision-making. This section verifies that the optimal model not only exhibits high prediction accuracy but also possesses excellent clinical applicability, effectively assisting clinicians in risk assessment.
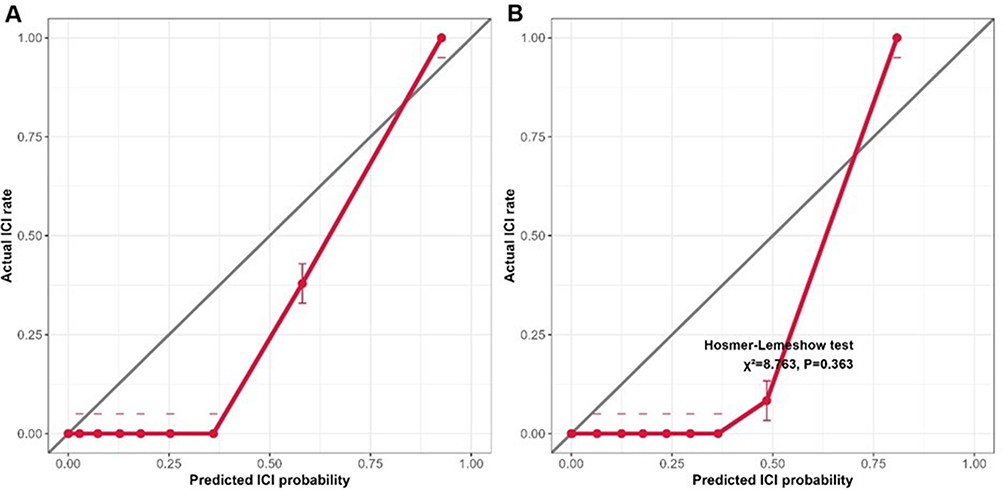 |
Figure 3 Calibration Curves of the LightGBM Model in the Training and Test Sets. Notes: The diagonal line represents the ideal calibration (perfect agreement between predicted and actual intracranial infection [ICI] rates). The solid lines denote the observed calibration of the LightGBM model in the training set (A) and test set (B), respectively. Both curves closely align with the ideal diagonal, indicating excellent consistency between the predicted ICI risks and actual observed ICI rates. The Hosmer-Lemeshow test result (χ2=8.763, P=0.363) further confirms that there is no significant difference between the predicted and actual values, verifying the reliable calibration performance of the LightGBM model. |
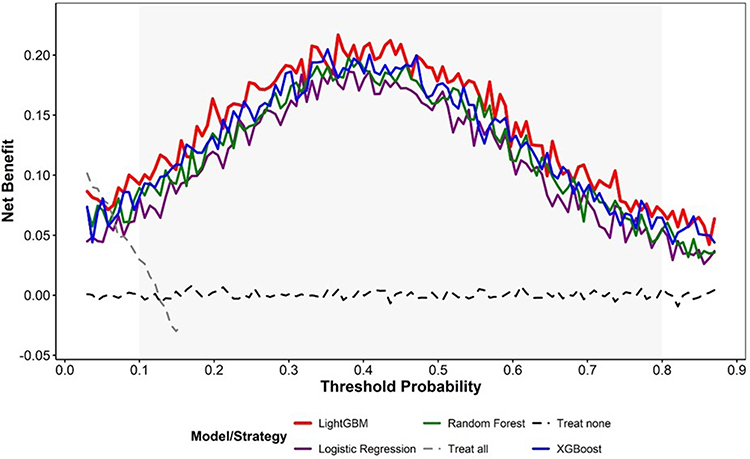 |
Figure 4 Decision Curve Analysis (DCA) of the Four Predictive Models for Postoperative Intracranial Infection. Notes: The x-axis represents the threshold probability, and the y-axis represents the net benefit. The colored solid lines correspond to different predictive models: LightGBM (red), XGBoost (blue), random forest (RF, green), and logistic regression (LR, purple). The gray dashed line denotes the “treat all” strategy, and the black dashed line denotes the “treat none” strategy. The LightGBM model provides a higher net benefit than the other three models and the two benchmark strategies across a wide range of threshold probabilities (0–0.90). Specifically, between the threshold probabilities of 0.10 and 0.80, the net benefit of the LightGBM model is significantly superior, highlighting its strong clinical utility in guiding individualized risk stratification and early intervention for postoperative ICI. |
Variable Importance in the LightGBM Model
The variable importance ranking in the LightGBM model (Supplementary Table 1) reveals that postoperative cerebrospinal fluid leakage is the most significant predictor (importance score=100.0), followed by frequent cerebrospinal fluid sampling or drug injection through drainage tubes (importance score=89.7), surgical duration (importance score=76.3), intraoperative bleeding (importance score=68.5), and surgical frequency ≥ 2 (importance score=57.2). These findings align with those obtained from multiple logistic regression analysis, further underscoring the pivotal role of these five variables in predicting postoperative ICI. The ranking of variable importance offers clear guidance for clinicians in prioritizing preventive measures, such as enhancing the management of cerebrospinal fluid leakage and standardizing drainage tube procedures.
Discussion
Postoperative ICI is a key complication affecting the prognosis of craniotomy patients, and accurate risk prediction and targeted prevention are crucial for improving clinical outcomes. This study constructed and compared four predictive models using perioperative clinical and surgical variables, identified independent risk factors for postoperative ICI, and validated the superior performance of the LightGBM model. The following discussion focuses on key findings, comparisons with previous studies, and clinical significance.
In this study, we identified five independent risk factors for postoperative ICI through multivariate analysis, namely: prolonged surgical time, significant intraoperative blood loss, postoperative cerebrospinal fluid leakage, ≥2 surgeries, and frequent cerebrospinal fluid sampling or drug injection through drainage tubes. Consistent with previous studies, prolonged surgical time has been confirmed as a key risk factor.13–15 Potential mechanisms may include long-term exposure of brain tissue to external environments and surgical instruments, increasing the risk of pathogen invasion; prolonged surgery and anesthesia drugs lead to a decline in the body’s immune function; and the cumulative damage to brain tissue and blood vessels during prolonged surgery can impair local defense mechanisms.16,17 Similarly, significant intraoperative blood loss has been found to be an independent risk factor, which may be due to the disruption of the integrity of cerebral blood vessels and blood-brain barrier, thereby promoting the entry of pathogens into the cranial cavity; blood accumulation in the surgical area provides a favorable medium for pathogen colonization; vascular traction injury leads to reduced local cerebral blood flow, resulting in cerebral ischemia and hypoxia, and increased susceptibility to infection.18,19
Postoperative cerebrospinal fluid leakage has been identified as the most significant predictive factor in the LightGBM model, aligning with the consensus in clinical practice.19–21 Cerebrospinal fluid leakage establishes a direct pathway between the cranial cavity and the external environment, enabling pathogens to invade in a retrograde manner. The causes of cerebrospinal fluid leakage encompass inadequate closure of the dura mater during surgery, increased intracranial pressure affecting incision healing, and failure to effectively seal the opened mastoid airbags or sinuses during surgery.22,23 Therefore, enhancing intraoperative dural repair and postoperative cerebrospinal fluid leakage monitoring are crucial for preventing ICI. Additionally, it has been found that undergoing ≥ 2 surgeries increases the risk of ICI, potentially due to repeated exposure of brain tissue to the external environment, increased surgical trauma, and impaired local tissue healing and immune function during multiple surgeries. This discovery underscores the necessity for careful evaluation of reoperation and thorough preoperative preparation to minimize the risk of infection.
Frequent cerebrospinal fluid sampling or medication injection through drainage tubes represents another significant risk factor. Indwelling drainage tubes, such as extracranial drainage tubes, are extensively utilized in neurosurgery; however, due to the direct communication between the cranial cavity and the external environment, they can also elevate the risk of intracranial infection.24,25 Frequent sampling or drug injection may result in improper aseptic procedures, displacement, or contamination of drainage tubes, ultimately leading to retrograde infection.26,27 This underscores the importance of standardized drainage tube procedures, encompassing strict aseptic techniques, minimizing unnecessary sampling and drug injection, and promptly removing drainage tubes when clinically necessary.
In terms of predictive models, this study found that machine learning models (LightGBM, XGBoost, RF) outperformed traditional LR models, with the LightGBM model exhibiting the best overall performance. The advantage of machine learning models lies in their ability to handle complex nonlinear relationships and interactions between multiple variables, which traditional linear models cannot fully capture.28,29 For instance, LR models only consider the linear contribution of each independent risk factor, whereas machine learning models can identify potential synergistic effects between variables such as surgical duration and intraoperative blood loss. The LightGBM model possesses advantages such as high efficiency, low overfitting, and strong capability in handling high-dimensional data. It achieved the highest AUC in both the training and testing sets, indicating its superior generalization ability. This is consistent with recent research indicating that gradient boosting algorithms such as LightGBM and XGBoost have significant advantages in medical prediction tasks.
The clinical practicality of predictive models is a key factor determining their practical application. The DCA in this study indicates that within a wide range of threshold probabilities, the LightGBM model provides higher net benefits than the “all treat” and “no treat” strategies, suggesting that the model can effectively help clinicians identify high-risk patients and develop personalized prevention strategies. For example, patients with predicted ICI risk higher than the threshold probability can receive enhanced preventive measures, such as strict aseptic procedures during surgery, active management of cerebrospinal fluid leakage, rational use of prophylactic antibiotics, and increased postoperative monitoring frequency. In addition, the model can be used for patient education to improve compliance with treatment and nursing measures.
Compared with previous studies predicting postoperative ICI, this study has several advantages. Firstly, various machine learning models were constructed and compared with traditional LR models to comprehensively evaluate the predictive value of different algorithms. Secondly, the study included a wide range of perioperative variables, ensuring the comprehensiveness of the predictive model. Thirdly, the performance of the model was comprehensively evaluated using multiple indicators such as AUC, sensitivity, specificity, calibration curve, and DCA. However, previous studies have reported different risk factors, such as preoperative GCS scores and open traumatic brain injury, which were not significant in this study. This difference may be due to differences in patient population, sample size, and surgical techniques. For example, the proportion of patients with severe traumatic brain injury in this study was relatively low, which may have affected the statistical significance of preoperative GCS scores.
This study inevitably has certain limitations. Firstly, this is a single-center retrospective study, which may limit the generalizability of the results to other institutions with different patient populations and clinical practices. We plan to conduct multicenter prospective studies in the future to complete external validation of the model and improve the generalizability of the model results to a wider population. Secondly, due to incomplete data collection, some potential confounding variables, such as the type of antibiotic used and the duration of indwelling drainage tubes, were not included in the model. Especially, due to inconsistent clinical application standards for prophylactic antibiotics during the study period, there is a lack of complete and unified data on the type, dosage, and duration of prophylactic antibiotics in electronic medical records, and this variable has not been included in the current model; We plan to collect standardized data on the use of prophylactic antibiotics in future multicenter prospective studies to explore their role in reducing the risk of intracranial infections. Thirdly, the sample size of ICI cases is relatively small (n=53), which may affect the stability and generalization ability of the model. Future research should conduct multicenter prospective studies with larger sample sizes, including more comprehensive variables, and further validate and optimize predictive models to improve their clinical applicability.
Conclusion
In summary, our retrospective study confirms that prolonged surgical duration, significant intraoperative bleeding, postoperative cerebrospinal fluid leakage, ≥2 surgeries, and frequent cerebrospinal fluid sampling or drug injection through drainage tubes are independent risk factors for intracranial infection after craniotomy. Machine learning models, particularly LightGBM models, can effectively integrate perioperative clinical and surgical variables to predict the risk of postoperative intracranial infection, demonstrating superior performance compared to traditional logistic regression. The LightGBM model exhibits good predictive performance in the current single-center dataset, and its clinical applicability requires further validation through multicenter prospective studies with larger sample sizes and external verification. It provides a practical and reliable tool for clinical risk stratification and early intervention, which is of great significance in reducing the incidence of postoperative intracranial infections and improving patient prognosis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Grose E, Xiao JB, Fang E, Routhier-Chevrier B, Siu JM, Wolter NE. The impact of endoscopic sinus surgery in pediatric patients with sinogenic intracranial infection: a systematic review and meta-analysis. Int J Pediatr Otorhinolaryngol. 2024;187:112176. doi:10.1016/j.ijporl.2024.112176
2. Liu Y, Tang J, Wang Y, Cui F, Yang Y. Intracranial infection caused by mycoplasma hominis after neurosurgical operation: an easily overlooked but serious condition. J Infect Developing Countries. 2025;19(9):1425–12. doi:10.3855/jidc.20729
3. Hu Y, He W, Yao D, Dai H. Intrathecal or intraventricular antimicrobial therapy for post-neurosurgical intracranial infection due to multidrug-resistant and extensively drug-resistant gram-negative bacteria: a systematic review and meta-analysis. Int J Antimicrob Agents. 2019;54(5):556–561. doi:10.1016/j.ijantimicag.2019.08.002
4. Kobets AJ, Goodrich JT. The history of intracranial infections. Child’s nervous system. ChNS. 2018;34(10):1849–1857. doi:10.1007/s00381-018-3888-5
5. Kameda-Smith MM, Mendoza M, Brown LA, et al. Comparison of endoscopic sinus sampling versus intracranial sampling for microbiological diagnosis of intracranial infection in children: a case series and literature review. Child’s Nerv Syst. 2023;39(12):3561–3570. doi:10.1007/s00381-023-06038-4
6. Zhai T, Fu ZL, Qiu YB, Chen Q, Luo D, Chen K. Application of combined cerebrospinal fluid physicochemical parameters to detect intracranial infection in neurosurgery patients. BMC Neurol. 2020;20(1):213. doi:10.1186/s12883-020-01781-6
7. Zhang Y, Zhou Y, Hou M, Zhang S. Analysis of cerebrospinal fluid routine biochemical level, pathogenic bacteria distribution, and risk factors in patients with secondary intracranial infection after brain tumor surgery. Evid Based Complement Alternat Med. 2022;2022:7716205. doi:10.1155/2022/7716205
8. Cai Y, Zhou L, Wang H, Zhang L, Wang J, Zhang K. Comparation of vancomycin penetration into cerebrospinal fluid in postoperative intracranial infection and community-acquired meningitis patients. J Clin Pharm Ther. 2019;44(2):216–219. doi:10.1111/jcpt.12770
9. MacEachern SJ, Forkert ND. Machine learning for precision medicine. Genome. 2021;64(4):416–425. doi:10.1139/gen-2020-0131
10. Handelman GS, Kok HK, Chandra RV, Razavi AH, Lee MJ, Asadi H. eDoctor: machine learning and the future of medicine. J Internal Med. 2018;284(6):603–619. doi:10.1111/joim.12822
11. Bodien YG, Barra A, Temkin NR, et al. Diagnosing level of consciousness: the limits of the glasgow coma scale total score. J Neurotrauma. 2021;38(23):3295–3305. doi:10.1089/neu.2021.0199
12. Handorf E, Yin Y, Slifker M, Lynch S. Variable selection in social-environmental data: sparse regression and tree ensemble machine learning approaches. BMC Med Res Method. 2020;20(1):302. doi:10.1186/s12874-020-01183-9
13. Xiong X, Xie Y, Li B, Yin C, Hu K. Treatment of intracranial infection by extensively drug-resistant acinetobacter baumannii after craniocerebral surgery. J Craniofac Surg. 2024;35(7):e673–e5. doi:10.1097/SCS.0000000000010542
14. Wang J, Yang JB, Wang XL, Ding WL. Pseudomeningocele following posterior cranial fossa surgery significantly increases the risk of intracranial infection: a 10-year retrospective analysis. Surg Infect. 2024;25(8):598–605. doi:10.1089/sur.2024.071
15. Cao D, Shen D, Shi Z, et al. A study on the effectiveness of multiple intraoperative disinfections and bacteriological monitoring in reducing postoperative intracranial infection rates in transnasal endoscopic skull base surgery. Acta neurochirurgica. 2025;167(1):91. doi:10.1007/s00701-025-06498-4
16. Suryaningtyas W, Sabudi I, Parenrengi MA. The extracranial versus intracranial approach In frontoethmoidal encephalocele corrective surgery: a meta-analysis. Neurosurg Rev. 2022;45(1):125–137. doi:10.1007/s10143-021-01582-6
17. Wang X. Mechanism and application of hyperbaric oxygen therapy in neurosurgery. Med Gas Res. 2026;16(2):156–160. doi:10.4103/mgr.MEDGASRES-D-24-00164
18. Tan AP, Svrckova P, Cowan F, Chong WK, Mankad K. Intracranial hemorrhage in neonates: a review of etiologies, patterns and predicted clinical outcomes. Eur J Paediatr Neurol. 2018;22(4):690–717. doi:10.1016/j.ejpn.2018.04.008
19. Fu P, Zhang Y, Zhang J, Hu J, Sun Y. Prediction of intracranial infection in patients under external ventricular drainage and neurological intensive care: a multicenter retrospective cohort study. J Clin Med. 2022;11(14):3973. doi:10.3390/jcm11143973
20. Wei Z, Han S, Hou S, Yu D, Wu YG. A predictive model for postoperative intracranial infection in patients following spontaneous intracranial aneurysm rupture. J Craniofac Surg. 2025;36(6):e804–e9. doi:10.1097/SCS.0000000000011637
21. Yue Z, Zhi X, Bi L, Zhao L, Ji J. Treatment and prognostic risk factors for intracranial infection after craniocerebral surgery. Neurosurg Rev. 2023;46(1):199. doi:10.1007/s10143-023-02106-0
22. Guo X, Fang J, Wu Y. Risk factors of intracranial infection in patients after intracranial aneurysm surgery: implication for treatment strategies. Medicine. 2021;100(48):e27946. doi:10.1097/MD.0000000000027946
23. Huang X, Zhang X, Zhou J, et al. Analysis of risk factors and preventive strategies for intracranial infection after neuroendoscopic transnasal pituitary adenoma resection. BMC Neuro. 2022;23(1):1. doi:10.1186/s12868-021-00688-3
24. Chen L, Li X, Li D, Dong X, Chen H. Efficacy and safety of intraventricular polymyxin B plus continuous ventricular drainage for the treatment of intracranial infection caused by drug-resistant Acinetobacter baumannii. Ann palliat Med. 2022;11(2):490–497. doi:10.21037/apm-21-3149
25. Deleu T, Bruyninckx D, Fieuws S, et al. A comparison between proximal and distal cerebrospinal fluid sampling sites in patients with external ventricular drains. Neurosurgery. 2025;97(4):786–792. doi:10.1227/neu.0000000000003482
26. Rahimi J, Woehrer A. Overview of cerebrospinal fluid cytology. Handbook Clin Neurol. 2017;145:563–571. doi:10.1016/B978-0-12-802395-2.00035-3
27. Zhu Y, Wen L, You W, et al. Influence of ward environments on external ventricular drain infections: a retrospective risk factor analysis. Surg Infect. 2021;22(2):211–216. doi:10.1089/sur.2019.355
28. Lv R, Wang Z, Ma Y, Li W, Tian J. Machine learning enhanced optical spectroscopy for disease detection. J Phys Chem Lett. 2022;13(39):9238–9249. doi:10.1021/acs.jpclett.2c02193
29. Ngiam KY, Khor IW. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019;20(5):e262–e73. doi:10.1016/S1470-2045(19)30149-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prediction of Acute Kidney Injury in Intracerebral Hemorrhage Patients Using Machine Learning
She S, Shen Y, Luo K, Zhang X, Luo C
Neuropsychiatric Disease and Treatment 2023, 19:2765-2773
Published Date: 11 December 2023
A Machine-Learning Model Based on Clinical Features for the Prediction of Severe Dysphagia After Ischemic Stroke
Ye F, Cheng LL, Li WM, Guo Y, Fan XF
International Journal of General Medicine 2024, 17:5623-5631
Published Date: 28 November 2024
Development and Validation of a Neonatal Hypothermia Prediction Model for In-Hospital Transport Using Machine Learning Algorithms: A Single-Center Retrospective Study
Zhang W, Gu X, Gu C, Yao L, Zhang Y, Wang K
Journal of Multidisciplinary Healthcare 2025, 18:3205-3217
Published Date: 4 June 2025
Using Machine Learning and the HAMD-24 Scale to Predict Suicide Ideation in Depressed Patients
Chen Y, Jiang ZY, Dong GZ, Zhang WY, Wang K, Yang HY
Psychology Research and Behavior Management 2025, 18:2153-2165
Published Date: 12 October 2025
Predictions of Small Intracranial Aneurysms’ Rupture Risk with Ensemble Machine Learning Model (Super Learner): A Retrospective Study in Two Tertiary Hospitals in China
Hu X, Ye S, Qi D, Li S, Tang X, Fang Y
International Journal of General Medicine 2025, 18:6637-6649
Published Date: 3 November 2025