Back to Journals » International Journal of Women's Health » Volume 18
Position-Induced Change in Carotid Corrected Flow Time Predicts Spinal Hypotension in Cesarean Delivery
Authors Hao S, Cao Y, Zhang T, Cao Y, Wang Y ![]()
Received 12 January 2026
Accepted for publication 23 April 2026
Published 29 May 2026 Volume 2026:18 595530
DOI https://doi.org/10.2147/IJWH.S595530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Shuai Hao,1,2 Yinghao Cao,2 Tieying Zhang,3 Yu Cao,4 Yun Wang1
1Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 2Department of Anesthesiology, Beijing You’an Hospital, Capital Medical University, Beijing, 100069, People’s Republic of China; 3Department of Ultrasound, Beijing You’an Hospital, Capital Medical University, Beijing, 100069, People’s Republic of China; 4Department of Clinical Epidemiology, Beijing You’an Hospital, Capital Medical University, Beijing, 100069, People’s Republic of China
Correspondence: Yun Wang, Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, No. 95, Yong’an Road, Beijing, 100050, People’s Republic of China, Tel +86-13521611825, Email [email protected]
Background: Spinal anesthesia-induced hypotension (SAIH) complicates 50– 70% of cesarean deliveries, posing maternal-fetal risks. This prospective, single-center observational study (ClinicalTrials.gov: ChiCTR2300077480) evaluated whether pre-induction positional change in carotid corrected flow time (δcFT) predicts SAIH in term parturients.
Methods: In this single-center prospective observational study, 54 healthy term parturients (≥ 37 weeks, ASA I–II), high-resolution carotid Doppler measured corrected flow time (cFT) and respiratory variation in peak velocity (δVpeak) in supine and left-lateral positions immediately before neuraxial block. The primary outcome was SAIH incidence within 15 minutes post-induction.
Results: Of 54 participants analyzed, 34 developed SAIH (63%). The SAIH group exhibited significantly shorter supine cFT (330.30± 18.44 vs 351.14± 19.57 ms, P< 0.001) and greater positional cFT increase (δcFT: 22.55± 14.29 vs 0.23± 13.30 ms, P< 0.001). δcFT demonstrated superior discriminatory accuracy (AUC 0.872, 95% CI 0.772– 0.972, P< 0.001) compared with supine cFT (AUC 0.769) and δVpeak (AUC 0.50– 0.52). Optimal δcFT threshold was 6.49 ms (sensitivity 94.1%, specificity 75.0%). Exploratory multivariable logistic regression analysis suggested that δcFT was associated with SAIH after adjustment for prespecified covariates (OR 1.125 per 1-ms increase, 95% CI 1.049– 1.206, P=0.001), whereas higher supine cFT was associated with a lower risk (OR 0.934, P=0.002). δcFT correlated significantly with the magnitude of blood pressure decrease (r=0.437, P=0.001). Interobserver reliability was excellent (ICC 0.969).
Conclusion: Pre-induction δcFT could be a promising noninvasive predictor of SAIH. Bedside assessment of positional changes in cFT might identify high-risk parturients and guide targeted prophylactic strategies. δVpeak lacked predictive utility in spontaneously breathing patients. Further external validation studies are warranted.
Keywords: spinal anesthesia, cesarean section, hypotension, carotid ultrasound, corrected flow time, peak-velocity respiratory variation
Introduction
Spinal anesthesia (SA) is the gold-standard technique for elective cesarean delivery worldwide due to its efficacy and safety profile.1,2 However, spinal anesthesia-induced hypotension (SAIH) remains a highly prevalent and clinically significant complication, occurring in 50% to 70% of cases despite prophylactic measures such as fluid loading, vasopressors, and left uterine displacement.3–5 SAIH is primarily driven from the sympatholytic effect of spinal anesthesia, which reduces systemic vascular resistance, and from aortocaval compression by the gravid uterus, leading to a critical decrease in venous return and cardiac preload.6–8 Maternal consequences include nausea, vomiting, dizziness, and, rarely, syncope or cardiac arrest.9,10 Potential fetal complications include impaired uteroplacental perfusion, reduced Apgar scores, and umbilical artery acidemia.11–13 In addition, hemodynamic instability could also increase the risk of adverse maternal-fetal outcomes, such as emergency delivery for fetal compromise.14 While prophylactic vasopressors can reduce the incidence of hypotension, approximately 30% of patients may carry a significant risk of reactive hypertension.15–17 Therefore, accurate pre-operative prediction of SAIH susceptibility is crucial for optimizing personalized prophylaxis and improving maternal–fetal outcomes.
Noninvasive carotid artery Doppler ultrasonography has emerged as a promising tool for hemodynamic assessment.18–20 The corrected flow time (cFT), derived from the systolic ejection period normalized to a heart rate of 60 bpm, can serve as a sensitive marker for preload changes: hypovolemia shortens cFT, whereas increased preload prolongs it.21–23 In addition, respiratory variation in carotid peak velocity (δVpeak) has also been proposed as a dynamic predictor of fluid responsiveness in spontaneously breathing patients, reflecting stroke volume variation induced by changes in intrathoracic pressure.24–26 Recent prospective observational studies have shown that cFT and δVpeak can predict postinduction hypotension in patients undergoing various elective surgical procedures.27,28 A cFT-guided fluid therapy could reduce hypotension incidence from 92.3% to 35.7% in elderly patients after general anesthesia induction for surgeries.29 Unlike indices measured with respiration controlled by the mechanical ventilation, both cFT and δVpeak are potentially applicable to awake spontaneously breathing parturients and require further investigations before they can be widely accepted in the clinical practice.30,31
In addition to static carotid artery Doppler ultrasonography measurements, dynamic evaluations of these measurement changes, such as cFT changes after passive leg raising (PLR), have shown satisfactory performance in assessing volume status and predicting fluid responsiveness in critically ill patients in the intensive care unit.32,33 In obstetric patients, shifting from a supine to a left lateral position can rapidly alleviate aortocaval compression, transiently augmenting venous return by approximately 300 mL and effectively performing a “mini-PLR” test.34 In these obstetric women, while static supine cFT (SP-cFT) has shown moderate predictive value for SAIH,35 it remains unknown whether the positional change from supine to left lateral side (δcFT=Left-lateral cFT - Supine cFT), similar to PLR in non-pregnant patients, could serve as a noninvasive method to assess volume status and predict SAIH in order to guide fluid therapy. Furthermore, evidence regarding δVpeak in spontaneously breathing parturients is limited and inconsistent. While some research reported that δVpeak could predict fluid responsiveness in parturients during cesarean delivery, other studies showed a wide grey zone with low discriminative power.24,31,36
In the current study, we hypothesized that the magnitude of the cFT increase (δcFT=Left -lateral cFT - Supine cFT) in response to this positional change, as well as the δVpeak during spontaneous breathing could reflect underlying preload dependence and therefore predicts susceptibility to the significant preload reduction caused by spinal anesthesia in pregnant women undergoing elective cesarean. Our specific study aims were, 1) determine the predictive value of pre-anesthetic SP-cFT, δcFT, and δVpeak during spontaneous breathing for SAIH in cesarean delivery; 2) compare the predictive accuracy of δcFT with that of SP-cFT; 3) determine the optimal cutoff values for SP-cFT and δcFT; 4) assess the correlation between these indices (SP-cFT, δcFT, and δVpeak) and the magnitude of systolic blood pressure decrease; 5) evaluate the inter-observer reliability of cFT measurements; and 6) investigate the value of SP-cFT and δcFT in the contexts of other commonly used variables, including age, body mass index (BMI), baseline systolic blood pressure, and baseline heart rate, to predict SAIH. By exploring the use of carotid Doppler indices, particularly the dynamic changes in cFT and δVpeak, our research sought to provide accurate measures for identifying pregnant women at high risk for SAIH, thereby guiding a personalized, targeted treatment strategy to improve maternal-fetal outcomes.
Materials and Methods
Study Design and Patient Selection
This prospective, single-center observational cohort study was conducted at Beijing You’an Hospital, Capital Medical University, from November 13, 2023, to June 21, 2024, after approval from the Institutional Review Board (IRB No. 2023–028) and registration with ClinicalTrials.gov (ChiCTR2300077480), registration date: 09-Nov-2023. All procedures adhered to the Declaration of Helsinki (2013).37
Consecutive women scheduled for elective cesarean delivery under spinal anesthesia were screened during routine pre-operative assessment. Eligible participants were 18–40 years old, with a gestational age ≥37+0 weeks, a singleton pregnancy, and the American Society of Anesthesiologists (ASA) physical status I–II. All participants provided written informed consent prior to enrollment.
Exclusion criteria were rigorously applied to ensure patient safety and protocol integrity. Patients were excluded if they presented with severe supine hypotensive syndrome diagnosed preoperatively, contraindications to spinal anesthesia (including coagulopathy, allergy to local anesthetics, or infection at the puncture site), significant cardiovascular comorbidities (eg, congenital heart disease, coronary artery disease, severe valvulopathy, peripheral arterial disease, arrhythmias, carotid plaque, or stenosis >50%), diabetes mellitus, preeclampsia, neurological disorders, or psychiatric conditions impairing cooperation.
Additional intraprocedural exclusion criteria were applied post-enrollment: conversion to general anesthesia; inadequate (below the T8 dermatome) or excessively high (above the T4 dermatome) sensory block level after intrathecal injection; or incomplete data collection.
Ultrasound Acquisition Protocol
All the ultrasound examinations were performed by a professional ultrasound physician. After the video images were saved, offline data acquisition and collection were independently performed by two trained anesthesia nurses. All studies were performed with a Philips IntelliVue MP70 ultrasound system (Philips, Netherlands) with a 3–13 MHz linear-array transducer; cine loops were stored in native DICOM format. Upon arrival in the pre-operative holding area, parturients rested supine for 10 min while continuous noninvasive blood pressure, heart rate, and pulse oximetry were recorded. The head was rotated 30° to the left, and the neck was slightly extended. In the transverse plane, the right common carotid artery was identified 2 cm proximal to the carotid bulb; the transducer was then rotated to obtain a longitudinal view, with color Doppler confirming laminar flow. A pulsed-wave sample volume was placed centrally with an insonation angle of ≤60°, and three consecutive cardiac cycles free of maternal Valsalva were recorded. The position was then changed to full left lateral decubitus for 5 min, and the identical sequence was repeated. All acquisitions were anonymised, and the anesthesiologist initiating spinal anesthesia remained blinded. Flow time (FT) was defined from the onset of systolic upstroke to the dicrotic notch; cFT=FT + [1.29 × (HR – 60)]; δVpeak was calculated as [(Vmax – Vmin)/((Vmax + Vmin)/2)] ×100% averaged over three respiratory cycles; dynamic indices were δcFT=cFTleft-lat – cFTsupine and d-δVpeak=δVpeakleft-lat – δVpeaksupine.
Anesthetic Management
All participants underwent a standardized anesthetic protocol. Pregnant individuals fasted for a minimum of 8 h for solids and 2 h for clear fluids preoperatively. Upon arrival in the operating room, supplemental oxygen was administered via face mask at 2 L/min. Standard monitoring included noninvasive blood pressure (NIBP), three-lead electrocardiography (ECG), and pulse oximetry (SpO2), with measurements recorded at 5-min intervals. An intravenous catheter was inserted, and lactated Ringer’s solution was infused at a maintenance rate of 10 mL/kg/h.
Spinal anesthesia was performed with the patient in the right lateral decubitus position. A 25-gauge spinal needle was used to inject hyperbaric bupivacaine 0.5% (8–12 mg) into the subarachnoid space at the L3–L4 interspace over 10–15 s. All spinal procedures were performed by a single, experienced anesthesiologist with 15 years of clinical experience, thereby minimizing operator-dependent variability.
Surgery commenced 5–10 min after intrathecal injection, contingent upon achieving a sensory block to T6, as assessed by pinprick testing. Patients with inadequate block (below T8) or excessive spread (above T4) were excluded per protocol. NIBP was measured every 2 min from the induction of anesthesia until delivery, and every 5 min thereafter until the end of surgery. SAIH was defined as SBP <80% of baseline SBP. Baseline SBP was defined as the mean of the pre-anesthesia systolic blood pressure measurements obtained before spinal anesthesia. We selected a 15-minute observation window after spinal anesthesia based on the physiological characteristics of SAIH. Following spinal anesthesia, sympathetic blockade occurs rapidly, leading to a sudden decrease in systemic vascular resistance and venous return. Most hypotension episodes begin in the early phase of anesthesia. Once SAIH occurred, management included accelerated crystalloid infusion, leftward tilt of the operating table (15°–30°), and intravenous boluses of methoxamine (1–2 mg) or ephedrine (10–20 mg). Bradycardia (heart rate<50 bpm) was treated with atropine 0.5 mg IV.
Statistical Analysis
Sample size was calculated a priori using MedCalc 23.2.6. Assuming an area under the receiver operating characteristic curve (AUC) of 0.75 for δcFT versus a null AUC of 0.50, α=0.05 (two-tailed), power=0.90, and an expected SAIH incidence of 65%, a minimum of 53 analyzable patients was required. Allowing for a 15% dropout rate, we planned to enroll 63 participants.
Statistical analyses were performed with R 4.3.2 and SPSS 29.0. Continuous variables were assessed for normality (Shapiro–Wilk test); normally distributed data are expressed as mean±SD, otherwise as median [IQR]. Categorical variables are presented as n (%). Univariable comparisons used independent t tests, Mann–Whitney U, χ2, or Fisher’s exact tests, as appropriate. Pearson correlation coefficients were calculated to assess the relationships among preanesthetic SP-cFT, supine δVpeak (SP-δVpeak), δcFT, change in δVpeak (d-δVpeak), and the magnitude of systolic blood pressure decrease (δSBP) after induction of spinal anesthesia.
An exploratory multivariable logistic regression analysis was performed to evaluate the association between carotid Doppler–derived indices and SAIH after adjustment for prespecified covariates (age, BMI, baseline HR, baseline SBP, SP-cFT, and δcFT). Multicollinearity was assessed using variance inflation factors. The linearity of the logit for continuous variables was evaluated using the Box–Tidwell approach. Model discrimination was quantified using the AUC, with DeLong’s test employed for comparison against competing indices; 95% confidence intervals were derived from 1000 bootstrap replicates. Calibration was evaluated using the Hosmer–Lemeshow test and the Brier score. Internal validation was performed using bootstrap resampling. The optimal δcFT cutoff was determined by maximizing the Youden index and performing a gray-zone analysis.
Interobserver reliability was quantified by the intraclass correlation coefficient (two-way mixed-effects, absolute agreement), coefficient of variation, and Bland–Altman limits of agreement. A two-sided P<0.05 was considered significant.
Results
Patient Flow and Baseline Characteristics
Of the 72 parturients screened, 60 met eligibility criteria and provided written informed consent. Subsequently, six were excluded: four due to protocol deviations (three with block heights above T4 or below T8, one with intraoperative conversion to general anesthesia), and two due to incomplete sonographic datasets. The final analytic cohort comprised 54 women (Figure 1). Baseline demographic and obstetric variables were well balanced between patients who subsequently developed SAIH (n=34, 63%) and those who did not (n=20, 37%) (Table 1). Mean maternal age was 34±4 years, median gestational age was 38+3 weeks [37+1–41+0], and mean BMI was 28.78±4.11 kg/m2. There were no significant differences between groups in height, weight gain during pregnancy, parity, or neonatal Apgar scores. Intraoperative crystalloid volume administered prior to delivery was similar (708.82±196.36 mL vs 640±221.6 mL, P=0.241), as was estimated blood loss (333.24±103.77 mL vs 335±148.77 mL, P=0.959). Baseline heart rate and baseline systolic blood pressure did not differ significantly between the two groups (all P > 0.05).
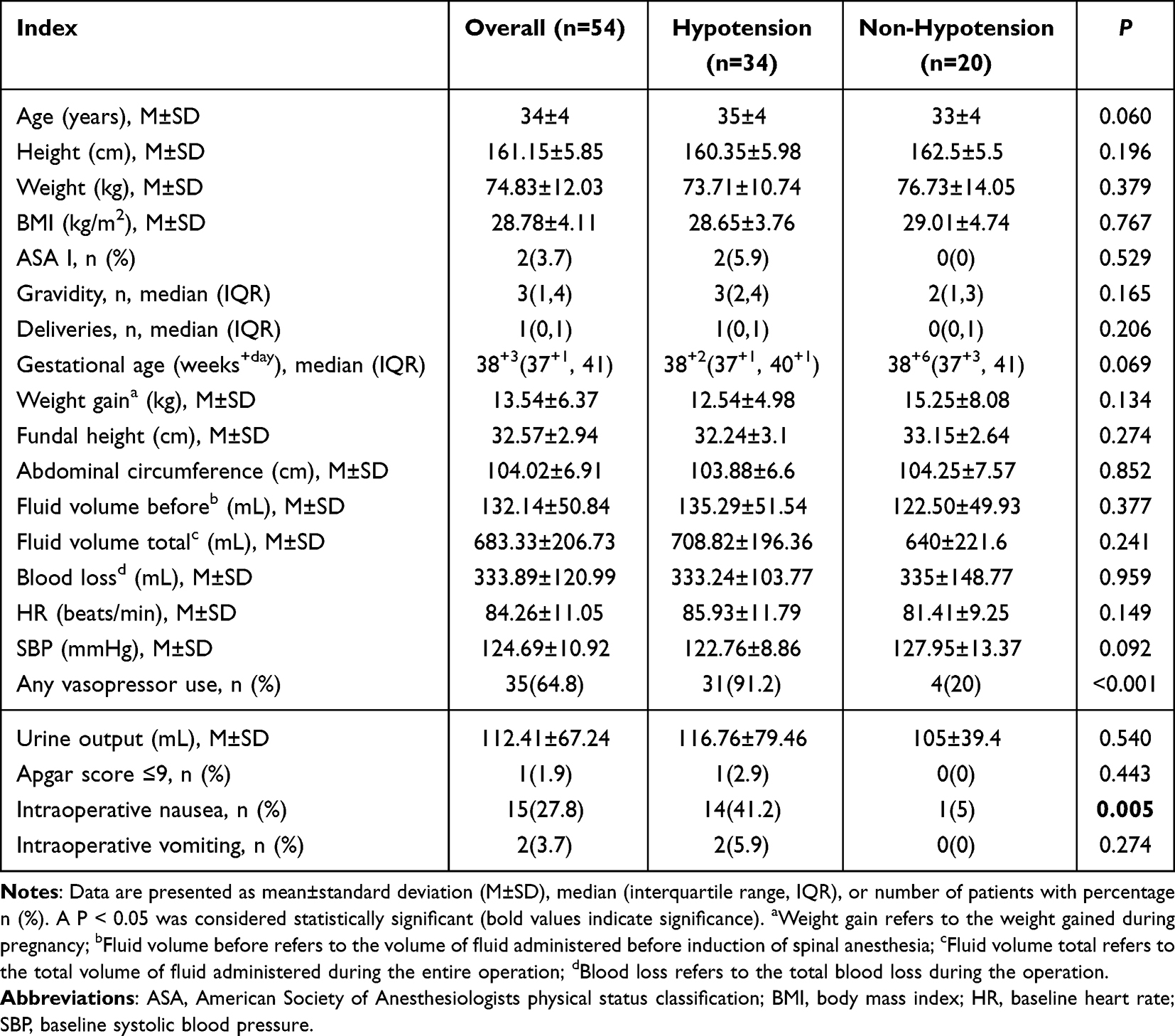 |
Table 1 Patient Characteristics and Perioperative Details |
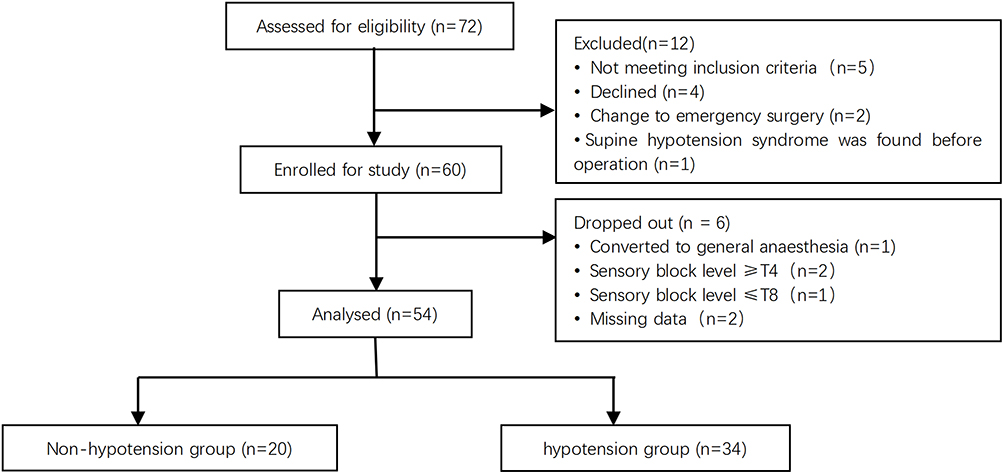 |
Figure 1 Study flow chart of patient enrolment and analysis. |
Ultrasound Indices and Positional Changes
Carotid ultrasound was successfully performed in all 54 parturients, with excellent intrasession image quality. In the supine position, baseline cFT was significantly shorter in patients who later developed SAIH than in those who remained normotensive (330.30±18.44 ms vs 351.14±19.57 ms, mean difference −20.84 ms; 95% CI −31.7 to −10.0 ms; P<0.001). After 5 min in the left -lateral position, cFT increased markedly in the SAIH group (to 352.85±21.53 ms, mean within-group change +22.55±14.29 ms; P<0.001), whereas the change was negligible in the nonhypotensive group (+0.23±13.30 ms; P=0.94), yielding a large between-group difference in δcFT (22.55±14.29 ms vs 0.23±13.30 ms; P<0.001) (Tables 2, 3 and Figure 2). In contrast, neither supine δVpeak nor left-lateral δVpeak differed significantly between groups, and the positional change in δVpeak (d-δVpeak) was also not significant (all P > 0.05).
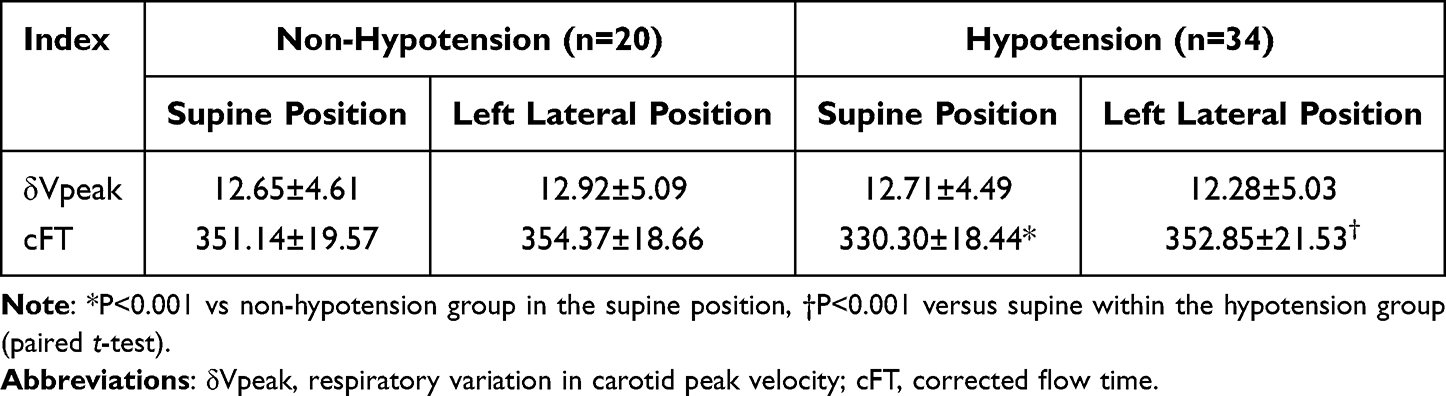 |
Table 2 Changes in δVpeak and cFT by Position |
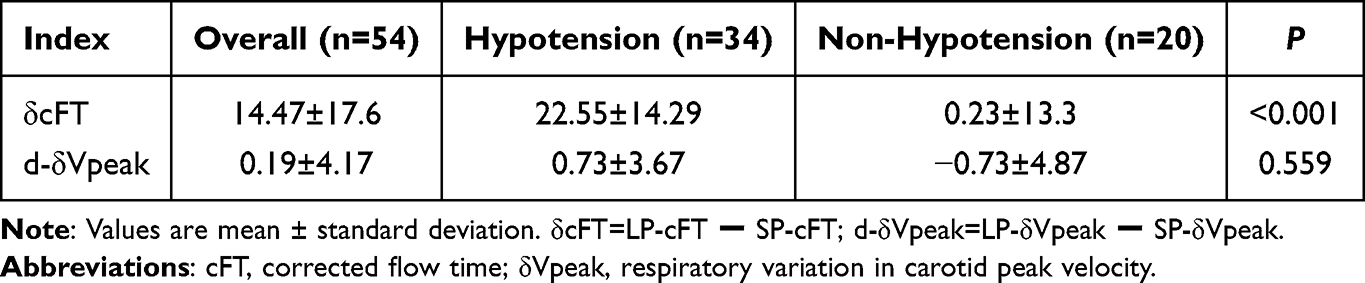 |
Table 3 Comparisons of Positional Change Indices (δcFT and d-δVpeak) Between Hypotension and Non-Hypotension Groups |
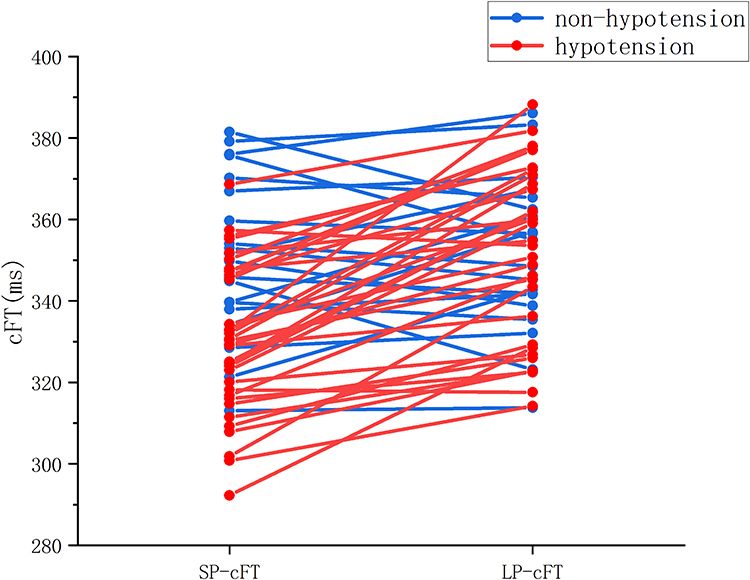 |
Figure 2 Change in carotid corrected flow time (cFT) from supine to left-lateral position in parturients who did or did not develop hypotension. Data are mean±SD. Red line=hypotension group, blue line=non-hypotension group. Abbreviations: cFT, corrected flow time; LP, left-lateral position; SP, supine position. |
Diagnostic Performance of Ultrasound Indices
Receiver operating characteristic analysis demonstrated that δcFT had a higher discriminatory ability for SAIH (AUC 0.872; 95% CI 0.772–0.972) compared with supine cFT (AUC 0.769; 95% CI 0.639–0.899) (Figure 3). However, the difference between the two correlated ROC curves did not reach statistical significance according to DeLong’s test (P=0.152). The optimal δcFT cutoff determined by the maximum Youden index was 6.49 ms, yielding a sensitivity of 94.1%, and a specificity of 75.0% (Table 4). A supine cFT<334.24 ms provided sensitivity of 85.0% and specificity of 64.7% (Table 4). Gray-zone analysis indicated that δcFT values between 6.71 and 19.97 ms constituted an inconclusive range for 28% of patients, which was narrower than the gray zone for supine cFT (328.52–354.06 ms, 48%) (Table 4 and Figure 4).
 |
Table 4 Receiver-Operating Characteristic Analysis of Supine cFT and Posture-Induced Change in cFT for Predicting Post-Spinal Hypotension |
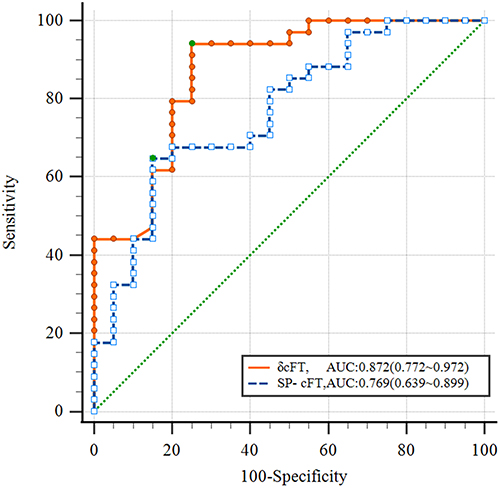 |
Figure 3 Receiver-operating characteristic curves of supine cFT (SP-cFT) and posture-induced change in cFT (δcFT) for predicting hypotension after spinal anesthesia. Dotted blue line=SP-cFT (AUC=0.769); solid Orange line =δcFT (AUC=0.872); dotted green line=chance (AUC= 0.5). Green dots mark optimal cut-off values determined by the maximal Youden index. Abbreviations: ROC, receiver-operating characteristic; AUC, area under the curve; cFT, corrected flow time; SP, supine position; δcFT, LP-cFT – SP-cFT; LP, left-lateral position. |
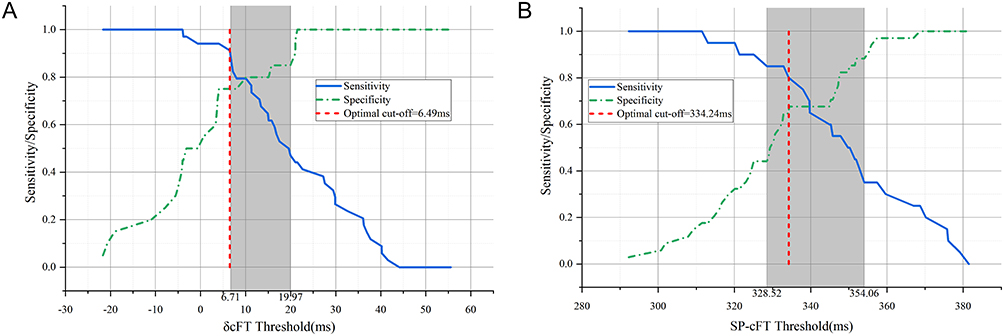 |
Figure 4 Grey-zone analysis of posture-induced change in cFT (δcFT) (A) and supine cFT (SP-cFT) (B) for predicting post-spinal hypotension. Solid blue line=sensitivity; dotted green line=specificity. The shaded region represents the inconclusive “grey zone” defined by 95% confidence intervals around the optimal threshold; the dashed red line indicates that threshold. Abbreviations: cFT, corrected flow time; SP, supine position; δcFT, LP-cFT – SP-cFT; LP, left-lateral position. |
Secondary Outcomes and Correlation Analysis
Pearson correlation analysis revealed significant relationships between δSBP after spinal anesthesia and ultrasound indices. Specifically, δSBP was negatively correlated with SP-cFT (r=−0.429, P=0.001) and positively correlated with δcFT (r=0.437, P=0.001) (Figure 5A and B). In contrast, δSBP did not show significant correlations with supine δVpeak (r=0.001, P=0.96) or d-δVpeak (r=0.081, P=0.559). These findings suggest that SP-cFT and δcFT are more reliable predictors of the magnitude of blood pressure decrease following spinal anesthesia, whereas δVpeak does not provide additional predictive value in this context.
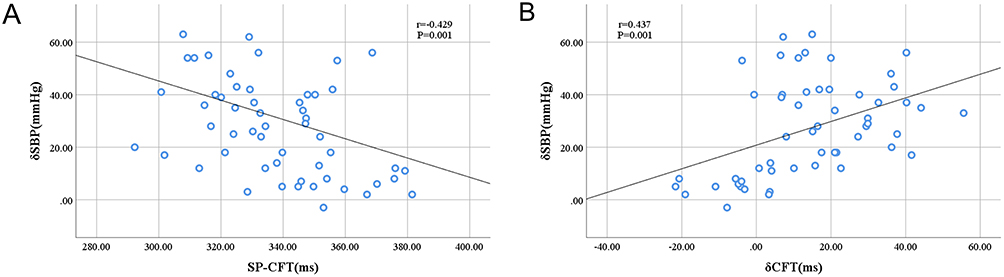 |
Figure 5 Relationship between the maximum systolic blood pressure decrease (δSBP) after spinal anaesthesia and (A) supine cFT (SP-cFT) or (B) posture-induced change in cFT (δcFT). The solid line shows the least-squares fit. Pearson correlation coefficients and p-values are shown in each panel. Abbreviations: δSBP, maximum percentage drop in systolic blood pressure; cFT, corrected flow time; SP, supine position; LP, left-lateral position; δcFT, LP-cFT – SP-cFT. |
Exploratory Multivariable Prediction Model
Exploratory multivariable logistic regression analyses were performed to assess whether carotid Doppler–derived indices remained associated with SAIH after adjustment for prespecified covariates. In the δcFT-based model, δcFT remained significantly associated with SAIH (per 1-ms increase; OR 1.125; 95% CI 1.049–1.206; P=0.001). In the SP-cFT-based model, higher supine cFT was associated with a lower risk of SAIH (per 1-ms increase; OR 0.934; 95% CI 0.895–0.975; P=0.002) (Table 5). Age, BMI, baseline heart rate, and the remaining adjusted covariates were not significantly associated with hypotension in either model (all P>0.05) (Table 5).
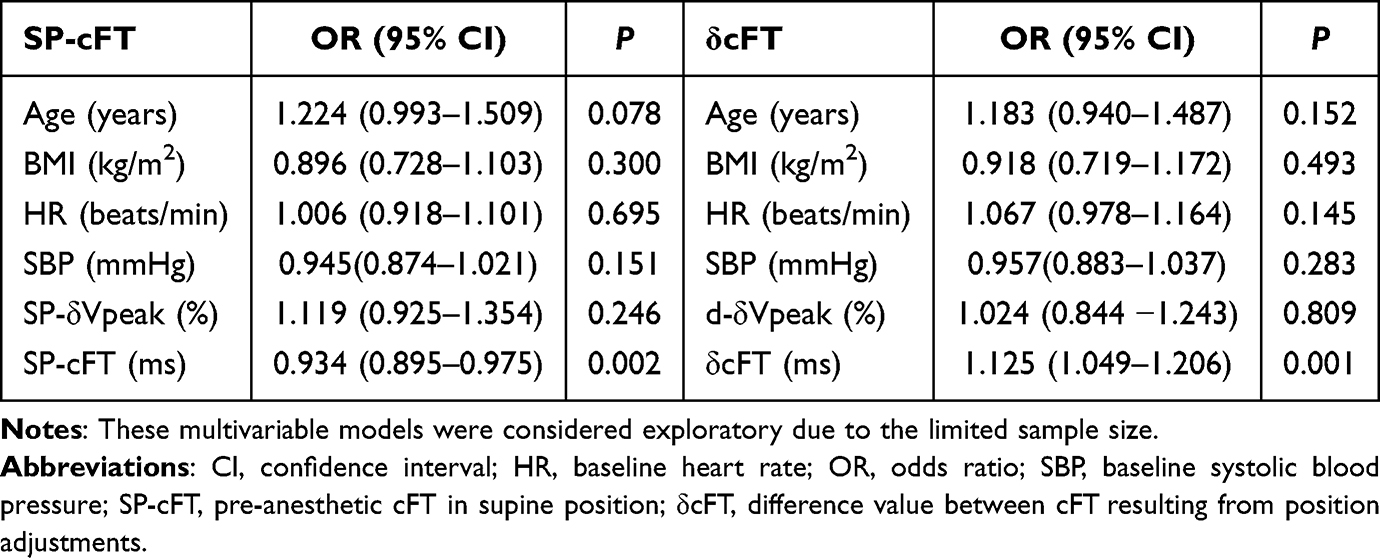 |
Table 5 Exploratory Multivariable Logistic Regression Models for Spinal-Anesthesia-Induced Hypotension |
No evidence of problematic multicollinearity was observed, with all variance inflation factors close to 1. In addition, no significant deviation from the linearity of the logit was detected for any continuous predictor.
For the SP-cFT-based model, the apparent discrimination was acceptable, with an AUC of 0.847. Calibration was also acceptable, with a Hosmer–Lemeshow test of χ2 = 8.394 (df = 8, P=0.396) and a Brier score of 0.150. Bootstrap internal validation indicated some optimism, with an optimism-corrected AUC of 0.779 and an optimism-corrected calibration slope of 0.663 (Supplementary Table S1 and Figure S1). For the δcFT-based model, discrimination was better, with an apparent AUC of 0.897. Calibration was satisfactory, with a Hosmer–Lemeshow test of χ2 = 6.764 (df = 8, P = 0.562) and a Brier score of 0.115. Bootstrap internal validation demonstrated an optimism-corrected AUC of 0.848 and an optimism-corrected calibration slope of 0.682, indicating better overall predictive performance than the SP-cFT model, although some degree of overfitting remained (Supplementary Table S1 and Figure S1).
Observer Reliability and Measurement Quality
Intrasession repeatability was evaluated by having two trained anesthesiology nurses measure the same set of ultrasound images for each patient. Each nurse performed three separate measurements per patient, resulting in six datasets per patient (three from Nurse A and three from Nurse B). The coefficient of variation for supine cFT was 3.1% (95% CI 2.5–3.7%) with an intraclass correlation coefficient (ICC) of 0.89 (95% CI 0.83–0.93); for left-lateral cFT, the CV was 3.0% (2.4–3.6%) and the ICC was 0.86 (0.78–0.92). In a second intrasession series, CVs were 3.2% (2.6–3.8%) and 3.2% (2.5–3.9%), respectively, with ICCs of 0.86 (0.79–0.92) and 0.88 (0.81–0.93). These results demonstrate the consistency of measurements within each nurse’s datasets.
Inter-operator agreement was assessed using 54 paired datasets from the full cohort. Bland–Altman analysis (Figure 6) revealed a mean bias of 0.8 ms (95% limits of agreement, −13.8 to 15.4 ms) for supine cFT and 1.9 ms (−12.6 to 16.4 ms) for left lateral cFT. The inter-operator ICCs were 0.969 (95% CI, 0.947–0.982) and 0.967 (95% CI, 0.943–0.981), respectively, with a pooled coefficient of variation of 1.1%. Although formal inter-operator variability assessment was not conducted for δVpeak, both nurses adhered to the same protocol for calculating δVpeak and reviewed the recordings together to minimize the influence of subjectivity.
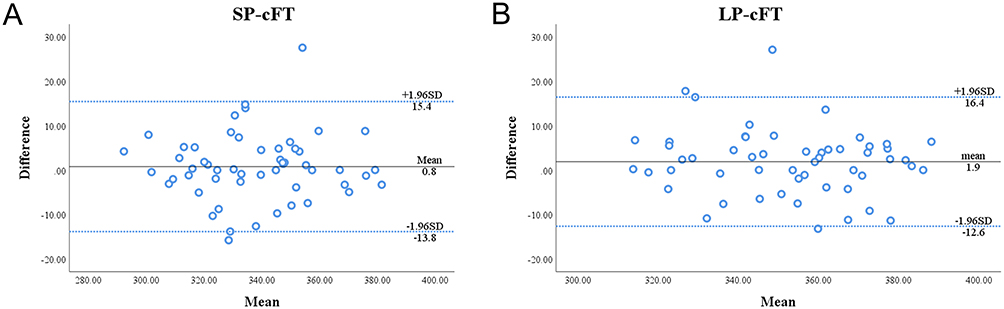 |
Figure 6 Bland-Altman plots showing inter-observer agreement for supine (SP-cFT) (A) and left-lateral (LP-cFT) (B) carotid corrected flow time measurements. Solid black line=mean bias; dashed blue lines=± 1.96 SD limits of agreement. Abbreviations: cFT, corrected flow time; SP, supine position; LP, left-lateral position; SD, standard deviation. |
Discussion
Our study demonstrated that δcFT induced by a controlled preload challenge (ie, shifting from the supine to the left lateral position) may be a promising predictor of SAIH in cesarean delivery and showed better discriminative performance than static indices such as supine cFT in this dataset. Specifically, δcFT exhibited superior discriminatory accuracy for predicting SAIH, with an AUC of 0.872, compared with 0.769 for supine cFT. The optimal δcFT threshold was 6.49 ms, with a sensitivity of 94.1% and a specificity of 75.0%. Additionally, we found that higher supine cFT values were protective against SAIH. In contrast, δVpeak did not show significant predictive value in either the supine or left lateral positions, highlighting its limitations in spontaneously breathing parturients.
Compared with previous studies that primarily focused on static hemodynamic parameters to predict SAIH,38 our study introduces a dynamic measure that overcomes the limitations of single-point measurements. For instance, Kim et al reported an AUC of 0.75 for static cFT in predicting SAIH, demonstrating its moderate predictive value.39 Similarly, other studies have explored static parameters, such as stroke volume variation and pulse pressure variation, in mechanically ventilated patients; however, these indices are less applicable to spontaneously breathing parturients.8,40 Our findings suggest that δcFT may offer a more physiologically relevant assessment of preload dependence than a single static measurement. This dynamic characteristic may be useful for perioperative risk stratification, although confirmation in larger external cohorts is required. Our study builds on these findings by introducing δcFT, a dynamic measure that captures the cardiovascular response to a controlled preload challenge. Consistent with this, δcFT showed a numerically higher AUC for predicting SAIH than supine cFT (0.872 [95% CI 0.772–0.972] vs 0.769 [95% CI 0.639–0.899]); however, the between-curve difference was not statistically significant on DeLong’s test (P=0.152). The optimal δcFT threshold was 6.49 ms, providing a sensitivity of 94.1% and a specificity of 75.0% for predicting SAIH. This enhanced predictive accuracy, together with the strong correlation between δcFT and the magnitude of systolic blood pressure decrease (r=0.437, P=0.001), highlights its clinical utility and offers a more physiologically relevant assessment of preload dependence.
The concept of using dynamic indices to predict fluid responsiveness and hypotension has been explored in various clinical settings.41–43 For example, PLR has been used to assess preload dependence by transiently increasing venous return.44–46 Our δcFT measure can be considered a noninvasive, mini–PLR test specifically tailored for the obstetric population. This method effectively simulates a reversible preload challenge by shifting the patient from the supine to the left lateral position, thereby providing valuable insights into the cardiovascular response to changes in venous return.
Consistent with prior variability, previous studies have reported inconsistent results regarding the predictive value of δVpeak in spontaneously breathing patients. Some studies suggest that δVpeak may help predict fluid responsiveness, whereas others have reported limited reliability.24,31,47 In our cohort, δVpeak did not show significant predictive value for SAIH in either the supine or left-lateral position, supporting concerns about its reliability in spontaneously breathing parturients.
The strengths of our study include its prospective design, standardized anesthesia protocol, rigorous ultrasound acquisition protocol, and the addition of model calibration and internal validation analyses. The use of high-resolution carotid Doppler imaging, combined with strict adherence to a predefined ultrasound protocol, ensured the collection of high-quality data. Additionally, inclusion of exploratory multivariable logistic regression analyses enabled us to evaluate whether carotid Doppler–derived indices remained associated with SAIH after adjusting for potential confounders. Our study aligns with the broader trend in anesthesia research toward developing personalized, noninvasive predictive tools. The integration of advanced imaging techniques, such as high-resolution carotid Doppler ultrasound, allows for real-time assessment of hemodynamic changes, which is crucial for timely intervention and improved patient outcomes.48–50 This approach is particularly relevant in obstetric care, where rapid changes in cardiovascular status can have significant implications for both the mother and the fetus.
However, our study also has limitations. The single-center design and a small sample size may limit the generalizability of our findings. Additionally, the upper limit of BMI in our study population may reduce the applicability of our findings to patients with morbid obesity. The poor predictive value of δVpeak might be attributed to the complex interplay between respiratory and cardiovascular dynamics in spontaneously breathing parturients, which could limit the accuracy of δVpeak measurements. In our study, the measurement of δVpeak was further compromised by two technical limitations. First, the Doppler technique used to measure δVpeak was technically demanding and prone to error. Minor changes in the angle of incidence or the position of the ultrasound beam could significantly affect the recorded velocities, introducing substantial measurement error and inter-observer variability.51 Second, the ultrasound equipment used in our study lacked a respiratory-trigger function. We had to manually determine respiratory cycles from M-mode peaks and troughs, likely reducing the precision of δVpeak measurements. Given these technical challenges, our findings highlighted the need for more robust, well-validated dynamic indices in this patient population.
To further enhance the prediction of SAIH and optimize maternal–fetal outcomes, several areas for improvement are proposed. First, continuous cFT monitoring using wireless neck Doppler patches could enable early detection and timely intervention for SAIH. Second, multicenter external prospective studies with larger cohorts are needed to validate the δcFT threshold identified in our study and to assess the impact of individualized management strategies on maternal and fetal outcomes. Additionally, respiratory-synchronized ultrasound should be explored to improve the reliability of δVpeak measurements in spontaneously breathing parturients. The development and validation of machine learning models integrating δcFT, heart rate variability, and other hemodynamic parameters could further enhance prediction accuracy. Ultimately, individualized prevention strategies based on risk stratification should be developed to optimize anesthesia care during cesarean delivery. Future research should focus on addressing current limitations and exploring innovative approaches to improve the accuracy and clinical applicability of SAIH prediction.
Conclusion
This study demonstrated that δcFT could be a promising noninvasive marker for predicting SAIH during cesarean delivery. An optimal δcFT threshold of 6.49 ms achieved high sensitivity (94.1%) and specificity (75.0%) for predicting SAIH, providing an easy, rapid method to identify high-risk patients and guide targeted prophylactic interventions. δcFT demonstrated better overall predictive performance than supine cFT in the present dataset, although without statistically significant superiority. Therefore, δcFT can be considered for early risk stratification. However, future external multicenter research with large sample sizes and consideration of other management variables (such as vasopressor use, tilt, and fluid loading) should validate its predictive value across diverse patient populations to confirm its generalizability.
Abbreviations
ASA, American Society of Anesthesiologists physical status classification; AUC, Area Under the Curve; BMI, Body Mass Index; cFT, Corrected Flow Time; CI, Confidence Interval; d-δVpeak, Difference in Respiratory Variation of Peak Velocity (left-lateral minus supine); δcFT, Difference in Corrected Flow Time (left-lateral minus supine); δSBP, Decrease in Systolic Blood Pressure; δVpeak, Respiratory Variation in Peak Velocity; HR, Heart Rate; IQR, Interquartile Range; LP, Left-lateral Position; OR, Odds Ratio; ROC, Receiver Operating Characteristic Curve; SD, Standard Deviation; SAIH, Spinal Anesthesia-Induced Hypotension; SP Supine Position; SP-cFT, Supine Corrected Flow Time; SP-δVpeak, Supine Respiratory Variation in Peak Velocity; Vmin, Minimum Velocity; Vmax, Maximum Velocity.
Data Sharing Statement
The datasets generated and analyzed in the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Beijing You’an Hospital, Capital Medical University (IRB No. 2023-028) and adhered to the principles outlined in the Declaration of Helsinki. All participants provided written informed consent prior to enrollment.
Acknowledgments
We would like to thank Medjaden Inc. for scientific editing of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Carvalho B, Sultan P. Spinal prilocaine for caesarean section: walking a fine line. Anaesthesia. 2021;76(6):740–14. doi:10.1111/anae.15341
2. Clyburn P. Spinal anaesthesia for caesarean section: time for re-appraisal? Anaesthesia. 2005;60:633–635. doi:10.1111/j.1365-2044.2005.04282.x
3. Ferre F, Martin C, Bosch L, Kurrek M, Lairez O, Minville V. Control of spinal anesthesia-induced hypotension in adults. Local Reg Anesth. 2020;13:39–46. doi:10.2147/LRA.S240753
4. Lee JE, George RB, Habib AS. Spinal-induced hypotension: incidence, mechanisms, prophylaxis, and management: summarizing 20 years of research. Best Pract Res Clin Anaesthesiol. 2017;31:57–68. doi:10.1016/j.bpa.2017.01.001
5. Knigin D, Avidan A, Weiniger CF. The effect of spinal hypotension and anesthesia-to-delivery time interval on neonatal outcomes in planned cesarean delivery. Am J Obstet Gynecol. 2020;223:747e741–747e713. doi:10.1016/j.ajog.2020.08.005
6. Assen S, Jemal B, Tesfaye A. Effectiveness of leg elevation to prevent spinal anesthesia-induced hypotension during cesarean delivery in the resource-limited area: open randomized controlled trial. Anesthesiol Res Pract. 2020;2020:5014916. doi:10.1155/2020/5014916
7. Lirk P, Haller I, Wong CA. Management of spinal anaesthesia-induced hypotension for caesarean delivery: a European survey. Eur J Anaesthesiol. 2012;29(9):452–453. doi:10.1097/EJA.0b013e328352ab10
8. Du EW, Tan HS, Tan CW, Sultana R, Sng BL. Heart rate variability and haemodynamic factors associated with hypotension during spinal anaesthesia for caesarean delivery: a case-control study. Eur J Anaesthesiol. 2022;39:219–226. doi:10.1097/EJA.0000000000001551
9. Hu LJ, Mei Z, Shen YP, et al. Comparative dose-response study of phenylephrine bolus for the treatment of the first episode of spinal anesthesia-induced hypotension for cesarean delivery in severe preeclamptic versus normotensive parturients. Drug Des Devel Ther. 2022;16:2189–2198. doi:10.2147/DDDT.S368480
10. Sklebar I, Bujas T, Habek D. Spinal anaesthesia-induced hypotension in obstetrics: prevention and therapy. Acta Clin Croat. 2019;58:90–95. doi:10.20471/acc.2019.58.s1.13
11. Habib AS. A review of the impact of phenylephrine administration on maternal hemodynamics and maternal and neonatal outcomes in women undergoing cesarean delivery under spinal anesthesia. Anesth Analg. 2012;114:377–390.
12. Reynolds F, Seed PT. Anaesthesia for Caesarean section and neonatal acid-base status: a meta-analysis. Anaesthesia. 2005;60:636–653. doi:10.1111/j.1365-2044.2005.04223.x
13. Laudenbach V, Mercier FJ, Roze JC, et al. Anaesthesia mode for caesarean section and mortality in very preterm infants: an epidemiologic study in the EPIPAGE cohort. Int J Obstet Anesth. 2009;18:142–149. doi:10.1016/j.ijoa.2008.11.005
14. Cavoretto PI, Silvani P, Farina A. Does intrapartum epidural analgesia influence rate of emergency delivery for fetal compromise? Ultrasound Obstet Gynecol. 2023;62:621–623. doi:10.1002/uog.27494
15. Saunders H, Khadka S, Shrestha R, Baig HZ, Helgeson SA. A systematic review and meta-analysis of prophylactic vasopressors for the prevention of peri-intubation hypotension. Diseases. 2024;12:13. doi:10.3390/diseases12010013
16. Zhang C, Qiu J, Huang Y, Tan R. Prophylactic norepinephrine infusion to treat hypotension after spinal anaesthesia during caesarean section: a meta-analysis. J Obstet Gynaecol. 2024;44:2393379. doi:10.1080/01443615.2024.2393379
17. Liu P, He H, Zhang SS, et al. Comparative efficacy and safety of prophylactic norepinephrine and phenylephrine in spinal anesthesia for cesarean section: a systematic review and meta-analysis with trial sequential analysis. Front Pharmacol. 2022;13:1015325.
18. van der Graaf AM, Zeeman GG, Groen H, Roberts C, Dekker GA. Non-invasive assessment of maternal hemodynamics in early pregnancy. Pregnancy Hypertens. 2013;3:261–269. doi:10.1016/j.preghy.2013.07.005
19. Collins HE, Alexander BT, Care AS, et al. Guidelines for assessing maternal cardiovascular physiology during pregnancy and postpartum. Am J Physiol Heart Circ Physiol. 2024;327:H191–H220.
20. de Boer EC, van Houte J, Fernandes CD, et al. Exploring the predictive value of carotid doppler ultrasound and clinical features for spinal anesthesia-induced hypotension: a prospective observational study. Perioper Med. 2025;14:26. doi:10.1186/s13741-025-00508-w
21. Kerrebijn I, Atwi S, Horner C, et al. Correlation between changing carotid artery corrected flow time and ascending aortic doppler flow velocity. Br J Anaesth. 2023;131:e192–e195. doi:10.1016/j.bja.2023.09.016
22. Mackenzie DC, Khan NA, Blehar D, et al. Carotid flow time changes with volume status in acute blood loss. Ann Emerg Med. 2015;66:277–282e271. doi:10.1016/j.annemergmed.2015.04.014
23. Jung S, Kim J, Na S, Nam WS, Kim DH. Ability of carotid corrected flow time to predict fluid responsiveness in patients mechanically ventilated using low tidal volume after surgery. J Clin Med. 2021;10:2676.
24. Abbasi A, Nayeemuddin M, Azab N, et al. Respiratory variation in carotid artery peak systolic velocity is unable to predict fluid responsiveness in spontaneously breathing critically ill patients when assessed by novice physician sonologists. J Intensive Care Med. 2021;36:885–892.
25. Kim EH, Lee JH, Song IK, Kim HS, Jang YE, Kim JT. Respiratory variation of internal carotid artery blood flow peak velocity measured by transfontanelle ultrasound to predict fluid responsiveness in infants: a prospective observational study. Anesthesiology. 2019;130:719–727.
26. Yao B, Liu JY, Sun YB. Respiratory variation in peripheral arterial blood flow peak velocity to predict fluid responsiveness in mechanically ventilated patients: a systematic review and meta-analysis. BMC Anesthesiol. 2018;18:168.
27. Wang J, Li Y, Su H, Zhao J, Tu F. Carotid artery corrected flow time and respiratory variations of peak blood flow velocity for prediction of hypotension after induction of general anesthesia in elderly patients. BMC Geriatr. 2022;22:882. doi:10.1186/s12877-022-03619-x
28. Maitra S, Baidya DK, Anand RK, Subramanium R, Bhattacharjee S. Carotid artery corrected flow time and respiratory variations of peak blood flow velocity for prediction of hypotension after induction of general anesthesia in adult patients undergoing elective surgery: a prospective observational study. J Ultrasound Med. 2020;39:721–730. doi:10.1002/jum.15151
29. Huang S, Liao Z, Chen A, Wang J, Xu X, Zhang L. Effect of carotid corrected flow time combined with perioperative fluid therapy on preventing hypotension after general anesthesia induction in elderly patients: a prospective cohort study. Int J Surg. 2024;110:799–809. doi:10.1097/JS9.0000000000000863
30. Singla D, Gupta B, Varshney P, Mangla M, Walikar BN, Jamir T. Role of carotid corrected flow time and peak velocity variation in predicting fluid responsiveness: a systematic review and meta-analysis. Korean J Anesthesiol. 2023;76:183–193.
31. Kim DH, Shin S, Kim N, Choi T, Choi SH, Choi YS. Carotid ultrasound measurements for assessing fluid responsiveness in spontaneously breathing patients: corrected flow time and respirophasic variation in blood flow peak velocity. Br J Anaesth. 2018;121:541–549. doi:10.1016/j.bja.2017.12.047
32. Cheong I, Otero Castro V, Sosa FA, et al. Passive leg raising test using the carotid flow velocity-time integral to predict fluid responsiveness. J Ultrasound. 2024;27:97–104. doi:10.1007/s40477-023-00824-1
33. Barjaktarevic I, Toppen WE, Hu S, et al. Ultrasound assessment of the change in carotid corrected flow time in fluid responsiveness in undifferentiated shock. Crit Care Med. 2018;46:e1040–e1046. doi:10.1097/CCM.0000000000003356
34. Kundra P, Velraj J, Amirthalingam U, et al. Effect of positioning from supine and left lateral positions to left lateral tilt on maternal blood flow velocities and waveforms in full-term parturients. Anaesthesia. 2012;67:889–893. doi:10.1111/j.1365-2044.2012.07164.x
35. Juri T, Suehiro K, Yasuda S, Kimura A, Fujimoto Y, Mori T. Changes in the corrected carotid flow time can predict spinal anesthesia-induced hypotension in patients undergoing cesarean delivery: an observational study. J Anesth. 2024;38:105–113.
36. Xu L, Dai S, Shen J, Lv C, Tang Y, Chen X. The predictive ability of carotid artery corrected flow time and respirophasic variation in blood flow peak velocity measured by ultrasonography for fluid responsiveness in parturients for cesarean delivery. Minerva Anestesiol. 2020;86:1039–1046.
37. World Medical A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–2194.
38. Yu C, Gu J, Liao Z, Feng S. Prediction of spinal anesthesia-induced hypotension during elective cesarean section: a systematic review of prospective observational studies. Int J Obstet Anesth. 2021;47:103175. doi:10.1016/j.ijoa.2021.103175
39. Kim HJ, Cho AR, Lee H, et al. Ultrasonographic carotid artery flow measurements as predictors of spinal anesthesia-induced hypotension in elderly patients: a prospective observational study. Med Sci Monit. 2022;28:e938714.
40. Boisselle ME, Zaphiratos VV, Fortier A, Richebe P, Loubert C. Comparison of carbetocin as a bolus or an infusion with prophylactic phenylephrine on maternal heart rate during Cesarean delivery under spinal anesthesia: a double-blinded randomized controlled trial. Can J Anaesth. 2022;69:715–725.
41. Monnet X, Marik PE, Teboul JL. Prediction of fluid responsiveness: an update. Ann Intensive Care. 2016;6:111.
42. Guarracino F, Bertini P. Dynamic indices of preload and fluid responsiveness: some certainty in the midst of the uncertain. Minerva Anestesiol. 2019;85:460–461.
43. Douglas IS, Alapat PM, Corl KA, et al. Fluid response evaluation in sepsis hypotension and shock: a randomized clinical trial. Chest. 2020;158:1431–1445.
44. Monnet X, Jabot J, Maizel J, Richard C, Teboul JL. Norepinephrine increases cardiac preload and reduces preload dependency assessed by passive leg raising in septic shock patients. Crit Care Med. 2011;39:689–694. doi:10.1097/CCM.0b013e318206d2a3
45. Honore PM, Spapen HD. Passive leg raising test with minimally invasive monitoring: the way forward for guiding septic shock resuscitation? J Intensive Care. 2017;5:36. doi:10.1186/s40560-017-0232-1
46. De Backer D. Can passive leg raising be used to guide fluid administration? Crit Care. 2006;10:170. doi:10.1186/cc5081
47. Shen J, Dai S, Tao X, Chen X, Xu L. Corrected flow time and respirophasic variation in blood flow peak velocity of radial artery predict fluid responsiveness in gynecological surgical patients with mechanical ventilation. BMC Anesthesiol. 2022;22:299. doi:10.1186/s12871-022-01837-9
48. Suriani I, van Houte J, de Boer EC, et al. Carotid doppler ultrasound for non-invasive haemodynamic monitoring: a narrative review. Physiol Meas. 2023;43. doi:10.1088/1361-6579/ac96cb
49. de Souza TB, Rubio AJ, Carioca FL, et al. Carotid doppler ultrasonography as a method to predict fluid responsiveness in mechanically ventilated children. Paediatr Anaesth. 2022;32:1038–1046. doi:10.1111/pan.14513
50. Lipszyc AC, Walker SCD, Beech AP, Wilding H, Akhlaghi H. Predicting fluid responsiveness using carotid ultrasound in mechanically ventilated patients: a systematic review and meta-analysis of diagnostic test accuracy studies. Anesth Analg. 2024;138:1174–1186. doi:10.1213/ANE.0000000000006820
51. Di Mario C, Madretsma S, Linker D, et al. The angle of incidence of the ultrasonic beam: a critical factor for the image quality in intravascular ultrasonography. Am Heart J. 1993;125:442–448.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Dose-Response Study of Phenylephrine Bolus for the Treatment of the First Episode of Spinal Anesthesia-Induced Hypotension for Cesarean Delivery in Severe Preeclamptic versus Normotensive Parturients
Hu LJ, Mei Z, Shen YP, Sun HT, Sheng ZM, Chen XZ, Qian XW
Drug Design, Development and Therapy 2022, 16:2189-2198
Published Date: 8 July 2022
Effectiveness of Leg-Elevation to Prevent Post-Spinal Hypotension in Elective Cesarean Section: A Systematic Literature Review of Randomized Controlled Trial
Besha Desta A, Alemu B, Mossie A, Abebe M, Shiferaw A, Girma B, Ilala TT, Tamrat Yilma K, Mohamed K
Open Access Surgery 2023, 16:61-68
Published Date: 9 October 2023
Effects of Hyperbaric and Isobaric Bupivacaine on Hemodynamic Profiles and Block Characteristics Among Parturients Undergoing Elective Cesarean Section Under Spinal Anesthesia: A Randomized Controlled Trial
Besha A, Zemedkun A, Tadesse M, Hailu S, Mossie A, Shiferaw A, Angasa D, Adamu Y
Journal of Pain Research 2023, 16:3545-3558
Published Date: 20 October 2023
Low-Dose Ropivacaine-Fentanyl Spinal Anesthesia Combined with Carbetocin for Cesarean Section: A Randomized Double-Blind Non-Inferiority Trial
Li M, Xie G, Chu L, Lu Y, Xu T, Li Y
Journal of Pain Research 2025, 18:4539-4550
Published Date: 2 September 2025
The Median Effective Dose of Phenylephrine Infusion for Prevention of Spinal-Induced Hypotension During Cesarean Delivery in the 15° Left-Tilt vs. Supine Positions: A Randomised Control Study
Yu XQ, Drzymalski DM, Qian J, Hu HJ, Xiao F, Yu L
Drug Design, Development and Therapy 2026, 20:591446
Published Date: 8 May 2026